classifying your thyroid fna specimens using...
TRANSCRIPT

Classifying Your Thyroid FNA Specimens
Using Bethesda Terminology: Use of
Adjunct Molecular Reflex Testing
Constantine Theoharis, MD
Assistant Professor
David Chhieng, MD, MBA, MSHI
Professor
Director of Cytology
Department of Pathology
Yale University
New Haven CT

Overall Objectives
� To apply the Bethesda Thyroid FNA Classification
System in the evaluation of thyroid FNA.
� To utilize molecular testing as an adjunctive test in
thyroid FNA. thyroid FNA.
� To advise clinicians on the implications of the each
diagnostic category of the Bethesda Classification
system and the results of molecular testing.

Overview
� Usage and clinical implications of the Bethesda Thyroid
Fine Needle Aspiration Classification System
� Indications and implications of molecular testing in thyroid
FNA
3

The Utilization of the Bethesda
System & BRAF Molecular
Adjunct Testing on Thyroid
Cytologic Samples Cytologic Samples
Part I of II
4
Constantine Theoharis, MDAssistant Professor
Department of PathologyYale School of Medicine
ASCP 2011

Objectives
� Review the Bethesda Thyroid FNA Classification System
� Describe its utilization at Yale & the questions it raises
Cellularityraises
� Posit molecular testing as prequel to part 2
� Challenge our view of the modern cytopathologist/surgical pathologist
5
Architecture Cytology
The Art of Cytopathology

Background� Thyroid Cancer
� Most common endocrine malignancy
� Incidence increasing
� Problematic clinically� Nodules
� ~7% of the population
� But TFNA is Compromised
� 60% benign
� 10% malignant
� 20% equivocal
� 10% non-diagnostic/unsatisfactory
� Lack of Uniformity� ~7% of the population� Only 5% are malignant
� Thyroid FNA (TFNA) = � the keystone modality� Diagnostic test*� Screening test *
*more in a moment6
� Lack of Uniformity
� Terminology
� Criteria
� Clinical Implications
� Bethesda Classification
� Resolutions?
� Molecular Diagnostics
� Not expressly advocated in the Bethesda System

The Bethesda System
1. Nondiagnostic or
Unsatisfactory
� Cyst fluid only
� Virtually acellular specimen
� Obscuring factors
4. Follicular neoplasm or
suspicious for a follicular
neoplasm
� Specify if Hürthle cell type
5. Suspicious for malignancy
2. Benign
� Benign follicular nodule e.g. adenomatoid nodule, colloid nodule
� Lymphocytic thyroiditis
3. Atypia of undetermined
significance
5. Suspicious for malignancy
6. Positive for malignancy
� PTC
� Medullary carcinoma
� Anaplastic carcinoma
� Lymphoma
� Metastatic neoplasm
� Other
7Ali and Cibas (Ed): The Bethesda System for Reporting Thyroid Cytopathology. Springer. 2009

Audience ResponseHow many thyroid FNAs do you see at your
institution?
� Answer choice #1: 1-100 cases/year.
� Answer choice #2: 101-500 cases/year.
� Answer choice #3: 501-1000 cases/year.� Answer choice #3: 501-1000 cases/year.
� Answer choice #4: 1001-3000 cases/year.
� Answer choice #5: >3000 cases/year.

Yale Endocrine Cytopathology
and Surgical Pathology
� Endocrine Surgery Referral Center
�Over 3,200 Thyroid FNAs annuallyFNAs annually
� Representing 2,500 patients seen in clinic per year
� Approximately 400 operations performed annually
9
Yale Smilow Cancer Center

Audience ResponseDo you utilize the Bethesda Thyroid FNA
Classification at your institution?
� Answer choice #1: No. We don’t have a
classification system per se.
� Answer choice #2: No. We have our own
departmental system.departmental system.
� Answer choice #3: Yes. We use TBS as it has been
described in the literature.
� Answer choice #4: Yes, however, we’ve modified it
somewhat to fit our needs.

The Bethesda System (Yale Version)
1. Nondiagnostic/ Unsatisfactory� Insufficient cellularity
� Poor preservation
� Obscuring factors
2. Benign � Benign mixed macro/micro-
follicular hyperplastic nodule i.e. goiter
� Lymphocytic thyroiditis/
4. Follicular neoplasm� Microfollicular pattern
� S/O Follicular Variant of PTC
5. Hürthle cell neoplasm
6. Suspicious for malignancy� Papillary Thyroid Carcinoma
� Medullary carcinoma� Lymphocytic thyroiditis/ Hashimoto thyroiditis
� Cyst Contents or Colloid Nodule-if USG matches
3. Indeterminate [AUS/FLUS]� Low cellularity with
predominance of microfollicles and absence of colloid
� Atypical nuclear features
� Medullary carcinoma
� Anaplastic carcinoma
� Lymphoma
� Metastatic malignancy
7. Positive for malignancy� Papillary Thyroid Carcinoma
� Medullary carcinoma
� Anaplastic carcinoma
� Lymphoma
� Metastatic malignancy
11Theoharis et al. Thyroid 2009;19:1215

Is Thyroid FNA a Diagnostic or a
Screening Test?
� Diagnostic�Positive for PTC/MTC/ATC
�Suspicious for…
�Negative for Malignancy
AUS/Indeterminate?
� Screening
�Follicular Neoplasm
�Hürthle Cell Neoplasm
�AUS/Indeterminate?
12
�AUS/Indeterminate?
� Architecture�Group Cell Features
�Single Cell Features
� Cytology�Nucleus v.s. Cytoplasm
�AUS/Indeterminate?
� Architecture
�Group Cell Features
�Single Cell Features
� Cytology
�Nucleus v.s. Cytoplasm?
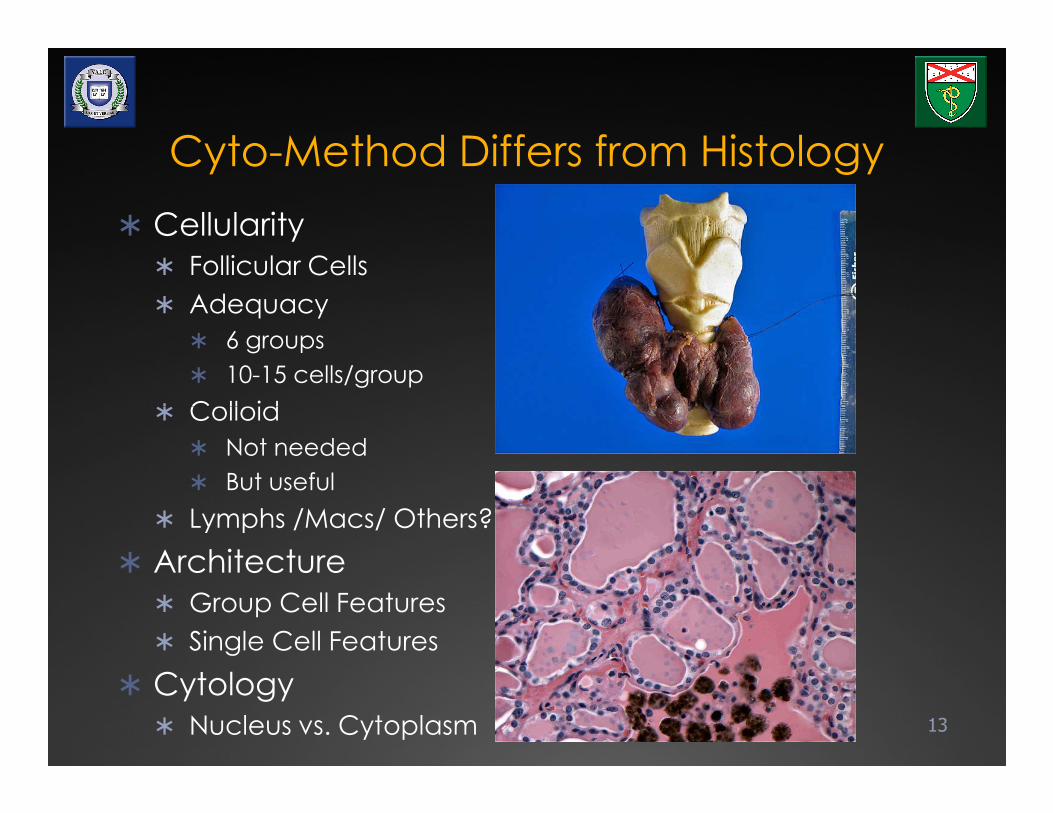
Cyto-Method Differs from Histology
� Cellularity
� Follicular Cells
� Adequacy
� 6 groups
� 10-15 cells/group
� Colloid
13
� Colloid
� Not needed
� But useful
� Lymphs /Macs/ Others?
� Architecture
� Group Cell Features
� Single Cell Features
� Cytology
� Nucleus vs. Cytoplasm


NegativeUSG: Hyperechoic nodule(s), capsular calcifications, bordering vessels…non-specific
15

Papillary Thyroid Carcinoma� Ultrasound
� Hypoechoic
� Microcalcifications
� Increased Vascularity
� Cellularity
� Follicular Cells!
16
� Follicular Cells!
� Architecture
� +/- Papillae, sheets,
caps
� Cytology
� Irregular Nuclear
Membranes & Grooves
� Intra-Nuclear
Cytoplasmic Invaginations (INCI’s)

Papillary Thyroid Carcinoma -
Papillae
17

Papillary Thyroid Carcinoma -
Inclusion (INCI)
18

Psammoma Body (Calcospherite)
19

Papillary Thyroid Carcinoma-
Papillae
20

Papillary Thyroid Carcinoma –
Inclusion (INCI)
21Does a classic positive PTC need molecular testing? BRAF? For Dx? for Pgx?

PTC Papillae & Psammoma
22

PTC with Oncocytic Features
23

Papillary Thyroid Carcinoma
to LN
24

Papillary Thyroid Carcinoma
to LN
25Often, few if any lymphocytes are present

Follicular & Hürthle Cell
Thyroid Neoplasms� Architecture
�Microfollicles
�NO Papillae
�Capsule & Vessel?
26
�Capsule & Vessel?
� Cytoplasm
�Amount v.s. Nucleus
� Nuclei�Smooth
�Enlarged
�+/- Nucleoli
�+/- Scant Colloid
�NO INCI’s
USG: Isoechoic nodule, no calcifications, no central vascularity…non-specific findings

Follicular Adenoma Capsule
27

Follicular Thyroid Carcinoma
� CAPSULAR INVASION
� VASCULAR INVASION
� Architecture�Microfollicles
28
�Microfollicles
�NO Papillae
� Nuclei�Smooth
�Enlarged
�+/- Nucleoli
�+/- Scant Colloid
�NO INCI’s

FTC Capsular Mushrooming
29

Follicular Thyroid Carcinoma
30

Follicular Neoplasm >
Follicular Adenoma
31

Follicular Neoplasm >
Follicular Carcinoma
32

Hürthle Cell Carcinoma
33Vascular Invasion

Hürthle Cell Neoplasm
34

Hürthle Cell Neoplasm >
Hürthle Cell Carcinoma
Normal sized cells
35Rarely, the degree of atypia is so great…
Massive cell with atypia

Indeterminate/FLUS/AUS
� For specimens that contain cells (follicular, lymphoid, or
other) with architectural and/or nuclear atypia
insufficient to be classified as suspicious for a follicular
neoplasm, suspicious for malignancy, or malignancy
� Criteria� Criteria
� Borderline cellularity with predominance of follicular cells
and absence/scant colloid
� Borderline cellularity with predominance of Hürthle cells
� Focal nuclear atypia s/o PTC (nuclear enlargement with
pale chromatin, nuclear grooves) particularly in patients
with lymphocytic thyroiditis or cystic changes
� Atypical lymphoid population
� Atypia with obscuring factors and/or air drying artifacts
36

AUS/FLUS/Indeterminate
(Yale Version)
� Architectural Atypia�Low Cellularity
�Microfollicles
�Absent/Scant Colloid
37
� Incipient Changes of
Neoplasia?
Indeterminate-Architectural Atypia

Follicular Adenoma with
intact capsule on resection
38

AUS/FLUS/Indeterminate
(Yale Version)
� Nuclear Atypia�Elongation/Enlargement
�Nuclear Membrane Irregularities/Grooves
�Rare possible(?)
39
�Rare possible(?) pseudoinclusions
� Incipient Changes of
Neoplasia?
Indeterminate-Nuclear Atypia

Mixed Classic and Follicular
variant PTC on resecton
40

� “At our institution, the term ‘indeterminate,’ corresponds to the NCI 2007 guidelines category “Follicular cells of undetermined significance.” Lesions designated as such my benefit from re-aspiration in the appropriate clinical context.”
Repeat FNA in 3- 6 months
Indeterminate/FLUS/AUS
� Repeat FNA in 3- 6 months
� ~20% of nodules are repeatedly diagnosed as “indeterminate”
� Surgery indicated if worrisome clinical and/or US findings
� Can we do better?
� Reflex BRAF mutational analysis?*
41*more on this coming in part 2!

Suspicious for
malignancy
� GOAL: � Maintain high PPV of
malignancy on f/u but w/o compromising sensitivity
� USUAL SUSPECTS:� Suspicious for PTC
� Most common
� Lobectomy ± frozen section (completion subsequently)subsequently)
� Suspicious MTC, ATC, NHL
� Compromised:� Quantity
� Quality
� Can we do better?
� Reflex BRAF mutational analysis?*
42*more on this coming in part 2!
Quantity Quality
The Need for Compromise

Suspicious for malignancy
Papillary group Nuclear atypia
43Overstained, obscuring blood, low cellularity, compromise dsample

What’s the difference?
Is it Atypical?
� Rule of Thumb:
� “I’m not certain it’s
negative”
Is it Suspicious
� Rule of Thumb:
� “I’m not certain it’s positive”
� You the cytopathologist
are communicating:
� “Don’t lose this patient to
follow-up”
� Malignant risk should be
low: <30%
� You the cytopathologist
are communicating:
� “Consider lobectomy
based upon this sample”
� Malignant risk should be
high: >60%
44

Medullary Thyroid Carcinoma
� Cellularity
� Cellular
� Architecture
� SINGLE Cells
� Cytology
45
� Cytology� Spindled
� Plasmacytoid
� Nuclei
� Smooth
� Salt & Pepper
� Small nucleoli
� +/- INCI’s� Ancillary Test?
� Calcitonin

Medullary Thyroid Carcinoma
46

Medullary Thyroid Carcinoma
47

Anaplastic Thyroid Carcinoma� History
� Older patient
� Rapid, recent growth
� Gross� Hemorrhage
� Necrosis
48
� Necrosis
� Architecture� SINGLE/Cellular
� Giant/Spindled
� Pleomorphic
� PMN’s� Nuclei
� Dark/Irregular
� Mitoses
� INCI’s
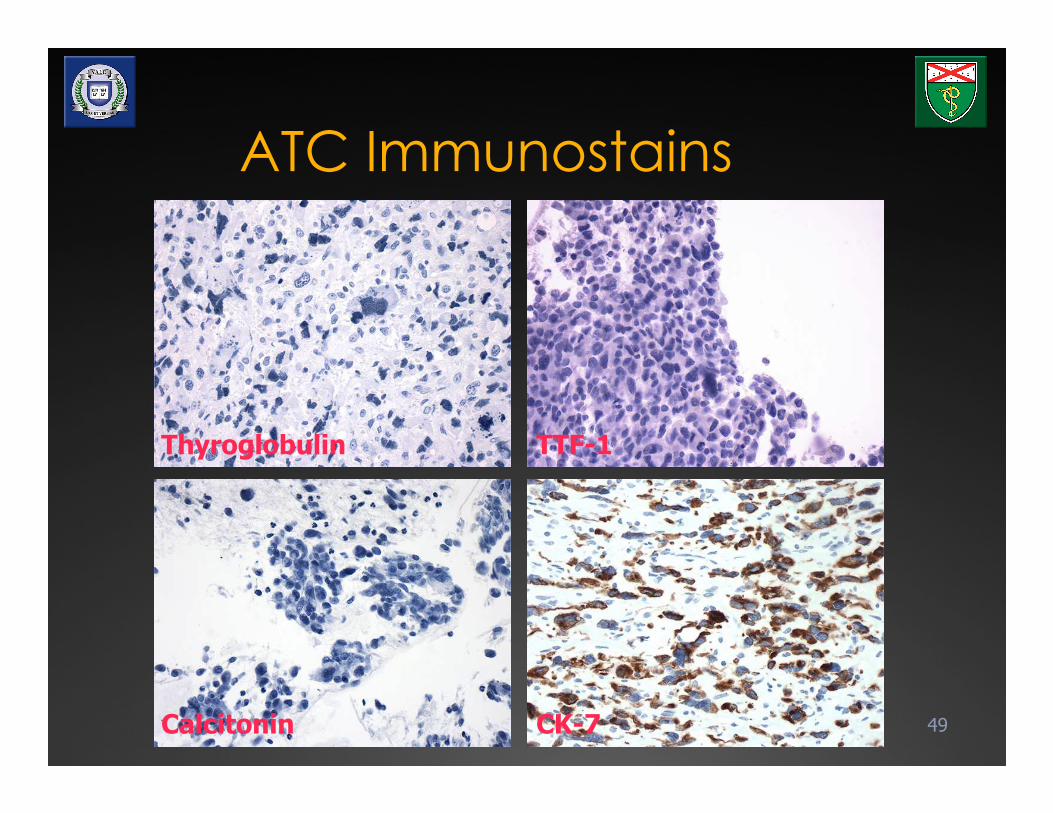
ATC Immunostains
49
Thyroglobulin TTF-1
Calcitonin CK-7

Anaplastic Thyroid
Carcinoma
50

Anaplastic Thyroid
Carcinoma
51

Non-Hodgkin Lymphoma
� Large B-Cell
� Hashimoto association
� Architecture�Monotypic/Cellular
52
�Monotypic/Cellular
�Cytoplasmic vacuoles
� Nuclei�Immature chromatin
�Multi-Nucleoli

Thyroid NHL
53Liquid Monolayer pseudo-groups

Thyroid NHL +CD45
54

Distribution of cytologic categories
Cytologic Category By Nodules
2008
By Patients
2008
Expected frequency
Unsatisfactory 357 (11.7%) 230 (9.0%) 10% to 15%
Benign/Negative for
Malignancy
2368 (78.0%) 1799 (72.8%) 70% to 80%
Indeterminate/Atypia of
Undetermined
Significance
95 (3.0%) 89 (3.6%) 3% to 18%
55
Significance
Follicular /Hürthle Cell
Neoplasm
176 (5.8%) 166 (6.7%) 5% to 8%
Suspicious for
Malignancy*
43 (1.4%) 39 (1.6%) 2.5% to 8%
Malignancy* 168 (5.5%) 145 (5.9%) 4% to 8%
Total 3207 2468
* Majority of them were PTC Modified from Theoharis et al. Thyroid 2009;19:1215

Comparison before and after TBS
Cytologic Category By Nodules
2008
By Patients
2008
By Nodules
2007
By Patients
2007
Unsatisfactory* 357 (11.7%) 230 (9.0%) 293 (14.4%) 197 (12%)
Benign/Negative for
Malignancy*
2368 (78.0%) 1799 (72.8%) 1361 (66.9%) 1053 (65.9%)
Indeterminate/AUS 95 (3.0%) 89 (3.6%) Susp FN 48
(2.3%)
Susp FN 45
(2.8%)
56
Follicular /Hürthle Cell
Neoplasm*
176 (5.8%) 166 (6.7%) 174 (8.3%) 156 (9.8%)
Suspicious for
Malignancy
43 (1.4%) 39 (1.6%) 29 (1.4%) 26 (2%)
Malignancy 168 (5.5%) 145 (5.9%) 119 (6%) 112 (7%)
Total 3207 2468 2035 1596
* Differences were statistically significant Theoharis et al. USCAP 2010

Cytologic-Histologic Correlation
Cytologic category
(% surgery)
MNG/HT FA CA Total
Unsatisfactory (11%) 9 8 8 25
Benign/Negative for
Malignancy (0.3%)
61 13 8* 82
Indeterminate (30%) 7 7 13 27
Follicular / Hürthle Cell
Neoplasm (61%)
33 34 35** 102
Suspicious for
Malignancy (77%)
2 2 26 30
Malignancy (77%) 0 0 112 112
Total 112 64 202 378
57
*The false negatives were micro PTC (≤ 1cm), not initially sampled by FNA** included both follicular CA and FV PTC

Operating Characteristic
As a Screening test
for NEOPLASM
As a Diagnostic test
for MALIGANCY
Sensitivity NA NA
Specificity 68% 93%
58
Specificity 68% 93%
Positive predictive
value
NA NA
Negative predictive
value
83% 91%
Theoharis et al. Thyroid 2009;19:1215

Risk of malignancy per Dx
Diagnostic Category Incidence of
malignancy at Yale
NCI recommended
rate of malignancy
Benign/Negative for
Malignancy10%* (0.3%) 0%-3%
Indeterminate 30%* (14%) 5%-15%
Follicular /Hürthle Cell 33% 20%-30%Follicular /Hürthle Cell
Neoplasm33% 20%-30%
Suspicious for Malignancy 87% 60%-75%
Malignancy 100% 97%-99%
59
* Only a selected subset of patients underwent surgery
Modified from Theoharis et al. Thyroid 2009;19:1215

� 171 nodules diagnosed as indeterminate/FLUS/AUS
between Jan 2008 to Jun 2009;
� Accounting for 2.8% of all cases
Indeterminate/FLUS/AUS
Category Number of
cases
Case with Follow-Up
(Surgery/Repeat FNA)
Malignant
Follow-Up
60
cases (Surgery/Repeat FNA) Follow-Up
Low cellularity/
microfollicular
pattern
104 (61%) 59(59%/41%) 7%
Nuclear atypia 67 (39%) 45(73%/27%) 56%
Total 171 104 (65%/35%) 20%
Adeniran et al USCAP 2010

Problems with equivocation� On Re-FNA
� <10% of Indeterminates were re-dx’d as Indeterminate
� Majority are PTC; most classified as having “nuclear atypia” cytologically
Re-FNA benign?� Re-FNA benign?
� Hyperplastic nodules in both groups with Hashimoto thyroiditis more prevalent in the 2nd group
� Suspicious Category less problematic (87% CA risk)
� Adjunct testing?� Immunostaining?
� Molecular testing?61

Molecular Diagnostics?
primum non nocere*
62MAPK SIGNALING PATHWAY
* From the Greek: ὠφελέειν, ἢ µὴ βλάπτειν

Audience ResponseDo you utilize molecular testing on thyroid FNAs at
your institution?
� Answer choice #1: No.
� Answer choice #2: BRAF only.
Answer choice #3: BRAF, RET only.� Answer choice #3: BRAF, RET only.
� Answer choice #4: BRAF, RAS only.
� Answer choice #5: Panel of BRAF, RET, RAS, PAX
etc.

A Possible Guideline to Molecular
Thyroid FNA Testing
64Theoharis C, Hui P. Surgery of the Thyroid and Parathyroid Glands 2nd Ed. (in press)

Pathologist
OUTCOME
Proteomics
Novel Tech
Electron
Microscopy
Immuno &
Chem Stains
Gross
Pathology
Practice
Management
Epidemiology
Somatic
Genomics
Gene
Arrays
Pharmaco-
genomics
Image
Analysis
Molecular
Diagnostics
Knowledge
Databases
Histology
Cytology
Flow
Cytometry
Electronic Data Layer
Decision Support
Pathologist/Cytopathologist as
Diagnostic Specialist
• Pathology develops and
adopts tools to leverage
data from emerging
technologies
• We become diagnostic
65
Dx
Diagnostic
ImagingMedical
Record
Medical
Literature
Medical Rx
Options
Surgical
Techniques
Social
Environment
Patient
Health
Patient
Rx
Clinical
Laboratory
TreatingClinician(s)
• We become diagnostic
consultants, providing
outcomes based treatment
recommendations to
treating clinicians
• We become the
Department of Diagnostic
Medicine
Sinard JH, Practical Pathology Informatics, used with permission

Summary� The Bethesda 6-tier classification system
� Conveys different levels of risk of malignancy
� Excellent screening test for follicular/Hürthle cell
neoplasm
� Superb diagnostic test for identifying PTC with a
specificity of 93%
� Sub-classifying indeterminate category into 2
descriptive groups conveys different levels of risk
� Molecular Testing may have a role especially in
equivocal cases
� Part 2 follows shortly…
� Thank you!
66

Acknowledgements�Cytopathologists
�David Chhieng
�Adebowale Adeniran
�Diane Kowalski
�Malini Harigopal
�Guoping Cai
�Angelique Levi
Surgical Pathologist�Surgical Pathologist
�Manju Prasad
�Molecular Pathologist
�Pei Hui
�Surgeons
�Robert Udelsman
�Sanziana Roman
�Julie Ann Sosa
�Tobias Carling
�Radiologist
�Lynwood Hammers67

Molecular Testing in Thyroid FNA
David Chhieng, MD, MBA, MSHI
Professor
Director of Cytology
Department of Pathology
Yale University
New Haven CT

Objectives� To apply the Bethesda Thyroid FNA Classification
System in the evaluation of thyroid FNA.
� To utilize molecular testing as an adjunctive test in
thyroid FNA.
� To advise clinicians on the implications of the each
diagnostic category of the Bethesda Classification
system and the results of molecular testing.

Overview� Introduction
� BRAF testing as a diagnostic marker
� RAS mutational analysis
� Use of a molecular panel
� BRAF testing as a prognostic marker
3

Adjunctive Testing� Immunocytochemistry
� Flow cytometry
� Lymphocytic thyroiditis vs lymphoma
� Molecular testing� Molecular testing
4

Immunocytochemistry� Primary vs secondary
� TTF-1 and thyroglobulin
� Medullary carcinoma
� Calcitonin, chromogranin, synaptophysin, and mCEA� Calcitonin, chromogranin, synaptophysin, and mCEA
� PTC vs other follicular-derived lesions
� CK 19, HBME-1, Galectin-3
� None specific enough
� False positive staining in Non-neoplastic lesions such
as lymphocytic thyroiditis and post FNA reactive foci

An example of medullary carcinoma staining positive
for calcitonin (ThinPrep preparation)

Immunohistochemistry for cytokeratin 19 in a fine needle aspirate of papillary
carcinoma (Giemsa preparation with immunohistochemistry performed after
removal of the coverslip).
Anderson C E , McLaren K M J Clin Pathol 2003;56:401-405

Expression of various makers in
thyroid lesions
Diagnosis Galactin -3 HBME 1 CK 19
Carcinoma (n=85) 92% 87% 72%
PTC (n=67) 94% 85% 72%
Follicular (n=6) 66% 50% 50%
Hurthle cell (n=8) 88% 13% 50%
Anaplastic (n=4) 100% 0% 25%
Adenoma (n=21) 10% 10% 5%
Non neoplastic thyroid (n=102) 17% 7% 13%
Nodular goiter (n=29) 55% 24% 31%
Thyrotoxicosis (n=14) 7% 0% 0%
Normal (n=59) 0% 0% 7%
Prasad et al. Mod Pathol. 2005:14:169.

Molecular TestingMolecular Testing
9

1. None
2. BRAF only
Audience Response
What molecular testing does your laboratory offer for
thyroid FNA?
3. BRAF and Ras
4. A panel of markers (i.e. BRAF, Ras, RET/PTC, PAX8-PPRϒϒϒϒ)

Revised Management Guidelines for
Patients with Thyroid Nodules and
Differentiated Thyroid Cancer
American Thyroid Association, 2009

MAPK Signaling pathway� >70% of PTC found
to have mutations
involving one of
the genes in the
MAPK signaling
pathway
� Especially RET/PTC,
RAS, and BRAF
� Usually mutually
exclusive
Nikiforov Y. Mod Path. 2008:2: S37

Other mutations
� Follicular carcinoma
� RAS mutation
� PAX8-PPARγ rearrangement
� Medullary carcinoma
� RET point mutation

Molecular alterations—frequency
Abnormality FA F CA PTC Comments
BRAF -- -- 40-60% •Classic and Tall cell
•Extranodal extension
and LN metastatsis
RET/PTC -- -- 20% •Classic
•Young onset and post
radiationradiation
•Type 1 (70%)
•Type 3 (30%)
RAS 20-40% 40-50% 10-20% •5% in goiter
•FV PTC
•Distant > LN metastasis
PAX8-PPARϒ
(t2,3)(q13;p25)
2-10% 20-40% 5-10% •FV PTC
•Younger age
•Aggressive behavior
Modified from Gillian CP. ANZ J Surg. 2010; 80: 33

BRAF � Found in ~45% (40-60%) of PTC
� Virtually all point mutations result in a valine-to-
glutamate at residue 600 (V600E)
� Highly prevalent in classical and tall cell variant� Highly prevalent in classical and tall cell variant
� Rare in follicular variant

Specificity of BRAF Detection in Thyroid FNA
Nature of studies No of
samples
BRAF
positive
Final diagnosis in
BRAF-positive samples
Prospectives 1814 159 100%
Retrospectives 685 291 100%
Research FNA of
surgically
removed thyroid
267 131 99.2%*
removed thyroid
Total 2766 581 99.8%
•The false positive is hyperplastic nodule with atypical nodular hyperplasia
Nikiforova & Nikiforov. Thyroid. 2009;19:1351

BRAF � Using SSCP, BRAF detected in 76% (28/37)
classical PTC (Yale data)
� Compared to direct sequencing, BRAF detected
in 65% (24/37)
� SSCP had an analytical sensitivity of 5% tumor cells
for a definite identification of BRAFfor a definite identification of BRAF
� Implemented reflex BRAF testing for equivocal
and positive thyroid FNA since Sept 09
� A total of 157 thyroid FNAs tested between Sept
2009 and Nov 2010
� 156 (99.4%) had sufficient DNA for BRAF testing

Demographic and characteristics of
patients and thyroid nodules
� ^10 patients had two nodules biopsied
� * the case with insufficient DNA was excluded
� # According to nodules
^10 patients had two nodules biopsied * the case with insufficient DNA was excluded# According to nodules
Adeniran et al. Thyroid 2011; 21:717

Histologic follow up results of thyroid
nodules with equivocal cytologic diagnosis
Adeniran et al. Thyroid 2011; 21:717
Over 50% of suspicious cases found to be follicular variant of PTC

Tissue follow up of thyroid nodules with
positive cytologic diagnosis according to
BRAF status
Adeniran et al. Thyroid 2011; 21:717

Histologic follow up with indeterminate
FNA and BRAF testing
Cytologic
diagnosis
(n=84)
BRAF
results
Surgical Follow up Total P value
PTC Benign
Indeterminate
w/ MF pattern
Positive
(n=0)
0 0 0
w/ MF pattern
(INa)
(n=0)
< 0.001
Negative
(n=28)
2* 8 10
Indeterminate
w/ nuclear
atypia (INb)
Positive
(n=19)
16 0 16
Negative
(n=36)
9* 13 22
• These cases were follicular variant and diffuse sclerosing variant PTC
Adenirian et al. Acta Cytologica. In press

Performance of BRAF testing in
indeterminate FNA
Sensitivity Specificity PPV NPV
59% 100% 100% 66%
~ 20% increase in positive identification of PTC
Adenirian et al. Acta Cytologica. In press

Algorithm for managing patients with
thyroid FNA and BRAF testing

Ras Mutations
� Point mutations found in many human cancers and in most types of thyroid tumors
� K-RAS, H-RAS, N-RAS genes may be involved
� Hot spots - codons 12, 13 and 61� Hot spots - codons 12, 13 and 61
� N-RAS codon 61 mutations most common in thyroid tumors

Mechanism of RAS Activation by Point Mutation
RASGDP Mutations
codons
• 12/13 in exon 1
Inactive
RASGTP
DownstreamEffectors
• 12/13 in exon 1 affecting GTP binding domains
• 61 in exon 2 affecting GTPase domain
Active

Molecular Pathways Activated by RAS
RASGRB2
SOS
Y1062
SHC
FRS2
RET
P
P
P
P
PLC Ral /Cdc42
DAG
PKC
AKT
Rho
Rac
B-RAF
MEK
ERK
PI3K
JNK
P70S6K
MEKK1
BCL
BAD
Apoptosisc-Jun, Fos ,
c-Myc , Elk-1

Incidences of Ras Mutations in Thyroid
Lesions
Thyroid Lesions Incidence of Ras Mutations
Follicular Carcinoma 40-50%
Papillary Carcinoma 10-20%*Papillary Carcinoma 10-20%*
Follicular Adenoma 20-40%
Goiter (Adenomatous Hyperplasia) 0-3%
•Almost exclusively in follicular variantLiu et al. Thyroid 2004: 14: 616
Nikiforvoa and Nikiforvoa. Thyroid 2009: 19: 1351

RAS mutations and
indeterminate FNA
� 64 Indeterminate thyroid FNAs (including FLUS, FN,
and suspicious) with positive RAS mutation and
surgical follow up
� Results of surgical follow up� Results of surgical follow up
Malignant 84%
PTC 52
Follicular carcinoma 4
Neoplastic Follicular Adenoma 11 16%
Non-neoplastic 0 0%
Nikiforov et el. JCEM. 2009;94:2092

Our Approach
Positive BRAF (regardless of RAS mutation)
Total thyroidectomy
� Perform RAS mutation in addition to BRAF mutation analysis for all indeterminate cases
IndeterminatePositive
RAS/Negative BRAF
Lobectomy
Negative BRAF + Negative RAS
Repeat FNA

Our Approach� Not recommended for cases with the diagnosis of
“Follicular Neoplasm”
� Up to 20% of RAS positive cases are Follicular
Adenoma and occasionally Adenomatous
HyperplasiaHyperplasia
� Current approach is lobectomy +/- intraoperative
consultation—No significant impact on patient
management

Alternate approach to molecular testing
in thyroid FNA
� Performing a panel of mutations on ALL thyroid FNAs
� The panel includes
� BRAF (V600E)
� RAS (k-,n-, & h-)
� RET/PTC rearrangement (RET/PTC 1 & RET/PTC 3)
ϒ
� RET/PTC rearrangement (RET/PTC 1 & RET/PTC 3)
� PAX8-PPRϒ

Performance of Molecular
testing using a panelReference Number of FNA
Samples
Specimens
types
Number of mutations
identified
1 470 All types 32 (7%)
2 400 All types 50 (13%)
3 285 Only those with
surgical FU
67 (29%)
4 432 All types 61 (14%)
1. Nikiforov et el. JCEM. 2009;94:2092.
2. Moses et al. WJ Surg. 2010;34:2589.
3. Cantara et al. JCEM. 2010;95:1365.
4. Mathur et al. Surgery. 2010; 148:1170.

Diagnostic
category
Numbers Mutation status Follow up
Malignant Follicular
Adenoma
Negative
Positive 79 Positive 26 26 0 0
Negative 53 53 0 0
Suspicious 81 Positive 52 50 0 2
Negative 29 10 4 15
Indeterminate 115 Positive 22 21 1 0
Negative 93 29 29 35
Negative 99 Positive 13 9 4 0Negative 99 Positive 13 9 4 0
Negative 86 5 10 71
Non-diangostic 53 Positive 14 12 2 0
Negative 39 4 11 24
Total 427 Positive 127
(30%)
118
(93%)
7
(6%)
2
(1%)
Negative 300
(70%)
101
(34%)
54
(18%)
145
(48%)
1. Nikiforov et el. JCEM. 2009;94:2092.
2. Moses et al. WJ Surg. 2010;34:2589.
3. Cantara et al. JCEM. 2010;95:1365.

Performance of Molecular
testing using a panelReference Sensitivity Specificity PPV NPV
1 62% 100% 97% 95%
2 38% 65% 42% 65%
3 80% 100% 100% 90%
1. Nikiforov et el. JCEM. 2009;94:2092.
2. Moses et al. WJ Surg. 2010;34:2589.
3. Cantara et al. JCEM. 2010;95:1365.

Prognostic Molecular
Markers

BRAF and Prognosis� Correlate with aggressive tumor characteristic
� Extrathyroidal extension
� Nodal metastases
� Resistant to radioiodine
� Tumor recurrence� Tumor recurrence

BRAF: Invasion and LNs

BRAF: Recurrence
Kaplan-Meier estimate of recurrence-free probability of PTC in patients with or without BRAF
mutation.
A, Analysis of a multicenter series consisting of 219 cases, mainly Caucasian patients. Log-rank
test: �2 O 4.0, P O 0.04. [Xing et al., 2005 (83).]
B, Analysis of a Korean series consisting of 203 patients. Log-rank test: �2 O 4.60, P O 0.037.
[Kim et al., 2006 (71), with permission from Wiley–Blackwell.]

BRAF: Higher Stage Disease
� BRAF is an
Independent
Prognostic Factor
associated with
Worse Disease and
Poorer Outcomes
Xing, M: BRAF Mutation
in Thyroid Cancer

BRAF mutation analysis and FNA
BRAF +ve BRAF –ve
Histologic subtype
Follicular variant 7% 51% p<0.05
Classic 22% 11% p<0.05
Tall cell variant 30% 6% p<0.05 Tall cell variant 30% 6% p<0.05
Extrathyroidal extension 56% 15% p<0.05
Mean size (cm) 1.9 2.3 p<0.05
LN involvement (Level VI) 47% 19% p<0.05
Yip et al. Surgery 2009; 146: 1215

Pathologic features of 60 papillary thyroid
carcinomas
Adeniran et al. Thyroid 2011; 21:717

Histologic Features of Papillary Thyroid
Carcinoma with and without BRAF Mutation
Morphologic features BRAFmutation
Positive
BRAFmutation
Negative
P Value
Tumor Capsule (intact or
infiltrated)
12 (35%)1 15 (68%)2 0.02
Infiltrative Growth 32 (94%) 13 (59%) 0.002
Stromal fibrosis, sclerosis or
desmoplasia
33 (97%) 15 (68.1%) <0.001
Plump tumor cells with 22 (65%) 6 (27%) 0.01Plump tumor cells with
moderate amount of
eosinophilic cytoplasm
22 (65%) 6 (27%) 0.01
Classic fully developed nuclear
features
33 (97%) 5 (22.7%) 0.0001
Lymphovascular invasion 4 (11.7%) 4 (18%) NS
Psammoma bodies 17 (50%) 5 (22.7) 0.05
Stromal calcifications 24 (70%) 10 (45%) 0.09
Cystic change 8 (23.5%) 3 (13.6%) NS
Extrathyroidal Extension 4 (11.7%) 4 (18%) NS
Finklestein et al. Presented at the 2011 USCAP meeting

Potential impact of BRAF status
on patient management
� Initial surgical management
� Total thyroidectomy
� Possible central lymph node dissection
� Initial radioiodine treatment� Initial radioiodine treatment
� Higher does of radioactive iodine

1. Archival slides with or without microdissection
2. Lavage fluid from needles washing after direct preparing direct smears
Audience Response
What kind of specimen does your laboratory used
for molecular testing for thyroid FNA?
preparing direct smears
3. Cell block
4. Obtaining additional pass to be collected in preservative solution

Specimen types for molecular testing
Specimen types Comments
Scraping all cellular
materials from archival
slides
• Ability to select slides containing optimal numbers
of tumor cells
• Destruction of diagnostic materials on the original
slides
• Labor intensive with microdissectionMicrodissecting from
archival slides archival slides
Lavage fluid from
washing the needles
after preparing direct
smears
• Quantity and composition of cellular materials
unknown—Compromise sensitivity
• Discordance of BRAF mutation status between
matched FNA and FFPE samples
• Storage up to 3 weeks after collection
Obtaining additional
pass to be collected in
preservative sol’n
• Quantity and composition of cellular materials
unknown—Compromise sensitivity
• Discordance of BRAF mutation status between
matched FNA and FFPE samples
• Required different collection protocol

Conclusions & Future Directions
� Molecular testing improved diagnostic accuracy for
thyroid FNA
� High PPV for cancer except RAS
� Need to define algorithms of patient management based
on cytology and molecular testing
� Prognostic markers
� BRAF mutation signifies more aggressive tumor
behavior—different therapeutic regime
� Therapeutic targets
� Novel inhibitors of MAP kinase pathway