class factors modifying drug action
TRANSCRIPT

Dr. RAGHU PRASADA M SMBBS,MDASSISTANT PROFESSORDEPT. OF PHARMACOLOGYSSIMS & RC.
1

1. Alteration in concentration of drug that reaches thereceptor-age, weight, sex, disease states,MDR(Multi-Drug Resistance genes)
2. Variation in concentration of an endogenousreceptor ligand-pharmacological antagonists-propranolol, Saralasin
3. Alteration in number and function of receptor-thyroid hormone and β receptor, agonist(DR),antagonist(UR)
4. Changes in the components of response distal tothe receptor-vasodilator drugs

1. Body size2. Age – pediatric &
geriatric3. Sex4. Species and race5. Genetics –P’genomics
and P’genetics6. Routes of drug
administration7. Pregnancy & Lactation
8. Physiological states– GIdiseases,congestive heartdisease, thyroid disease,kidney & liver disease
9. Diet &Environmentalfactors
10. Psychological factors11. Cumulation12. Tolerance & resistance
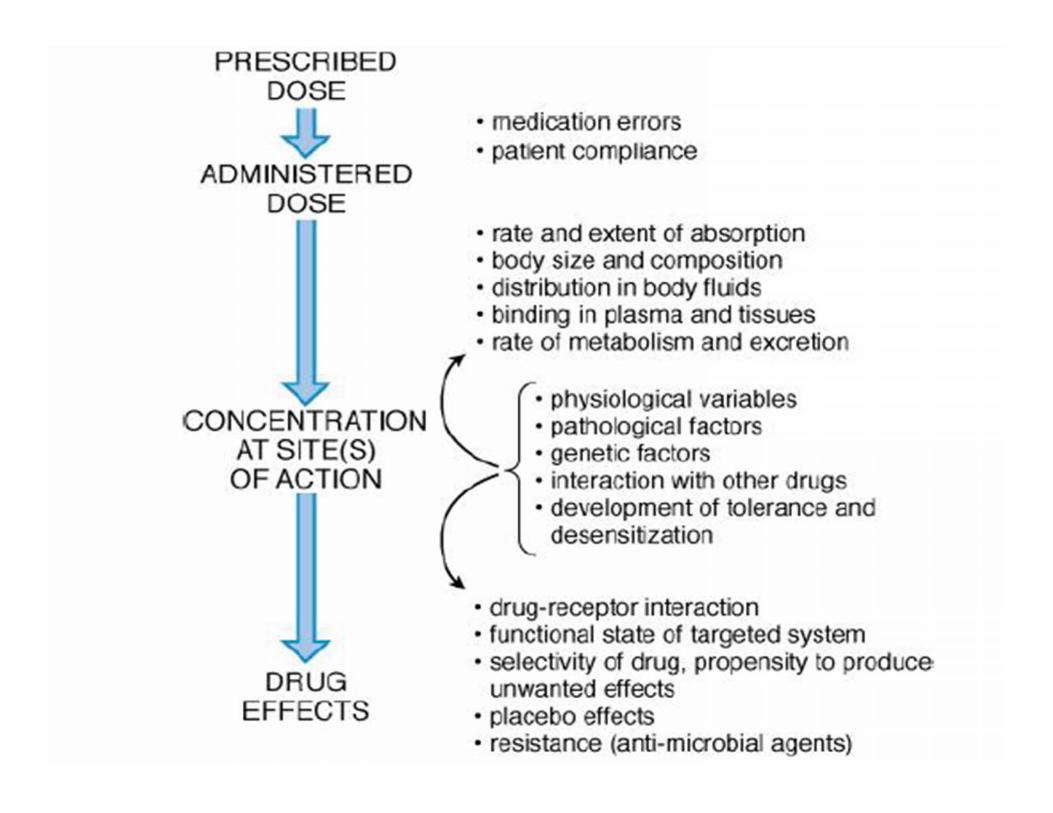

Influences the concentration of drugAttained at the site of actionAverage adult dose for – medium builtFor ext. Obese or lean individual –individual dose = bw(kg)/70 χ averageAdult dose
Body surface area (BSA) provides a moreAccurate basis for dose calculationIndividual dose = BSA (m2)/1.7 χ av. Adult Dose
BSA(m2) = bw(kg)0.425 χ height(cm)0.725 χ 0.007184
Obtained from chart form or slideRule nomograms based on bw andHeight. Avail. For some drugs

Solid dosage forms and aerosol inhalation are difficultto administer to young children .Many drugs prepared for children are in the form ofelixirs or suspensions.Elixirs are alcoholic solutions in which the drugmolecules are dissolved and evenly distributednoshaking is required.Suspensions contain dissolved particles of drug thatmust be distributed throughout the vehicle by shaking

Dose calculationYoung’s formula –child dose = age /age + 12 χ adult doseDilling’s formula –child dose = age/20 χ adult doseBody surface area
Chloramphenicol-gray baby syndromeRectal diazepamTheophylline, phenytoin, carbamazepine- shorter t1/2
Elderly- renal functionslower absorptionLesser plasma protein bindingDecrease in the volume of distribution

Females- lesser body surface areaDigoxin in womenAntihypertensives- clonidine, methyl dopa, betablocker and diuretics

Pharmacogenetics –the study of genetic basis forvariability in drug responseHuman genome projectPharmacogenomics-it is the use of genetic informationto guide the choice of drug and dose on individualbasisSpecific gene defectscan lead to variation in drug responses ‐e.g. Atypical pseudo‐cholinesterase ‐ prolongedsuccinylcholine induced apnoea

G‐6 pd deficiency – Hemolysis with primaquine andother oxidizing drugs like sulphonamides, Dapsone,quinine, chloroquine, Nalidixic acid, nitrofurantoinAcute intermittent porphyria- precipitated bybarbiturates is due to genetic defect in repression ofporphyrin synthesisDose of a drug to produce the same effect may vary by4‐6 fold among different individuals because of ‐different rate of metabolism‐ due to difference inthe amount and isoform pattern of drug metabolizingenzymes which is genetically controlled.

Differences in target organ sensitivityThe low activity of CYP2C9 variants metabolizewarfarin at a slow rate and are at higher risk ofbleedingSlow acetylators- polymorphism at NAT2 (N-acetyltransfrase 2) gene results in rapid and slow acetylatorstatus

GENE PRODUCT DRUGS RESPONSES AFFECTED
N-Acetyl transferase(NAT2) Isoniazid, hydralazine,sulfonamides,procainamide, dapsone
Hypersensitivity tosulfonamides, hydralazineinduced lupus, isoniazidneurotoxicity
Glutathionetransferases(GSTM1)
Anticancer agents Decreased response in breastcancer, more toxicity in AML
Thiopurine MethylTransferase(TPMT)
Mercaptopurine,Azathioprine
Thiopurine toxicity
COMT Levodopa Enhanced drug effect
Organic cation transporter(OCT1, OCT2)
Metformin Pharmacokinetic, renalclearance
Novel organic cationtranporter(OCTN1)
Gabapentin Renal clearance
CYP2B6 Cyclophosphamide Ovarian failure
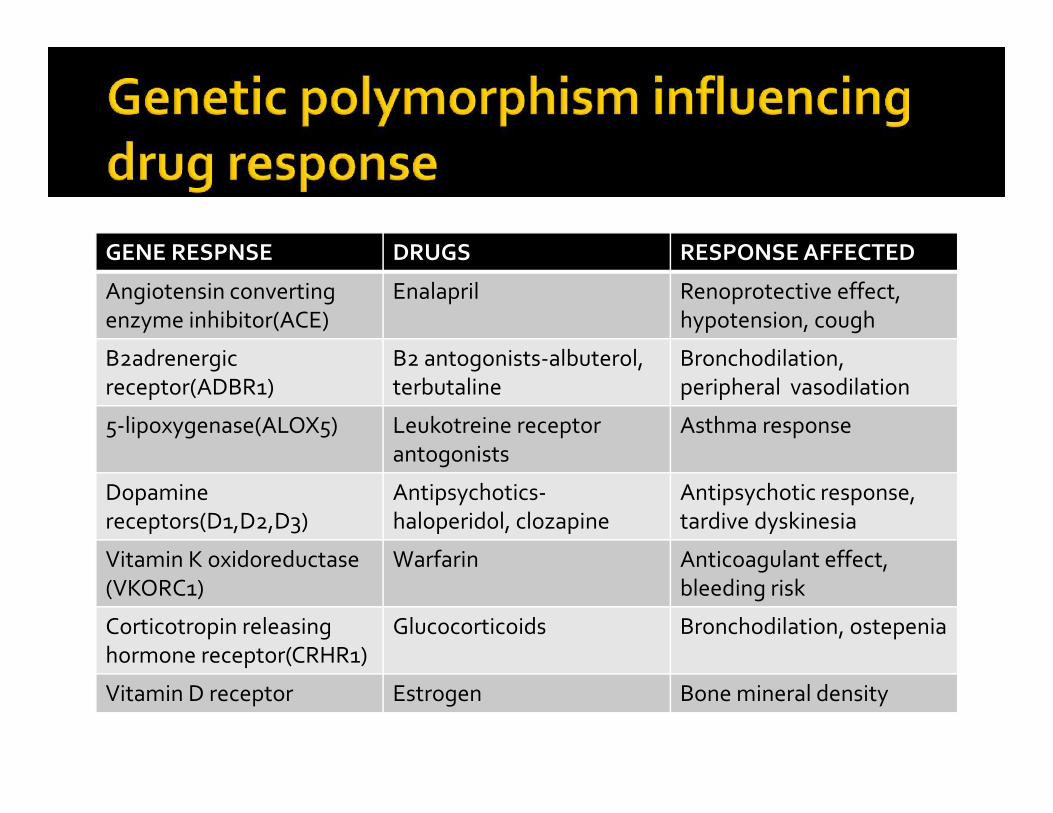
GENE RESPNSE DRUGS RESPONSE AFFECTED
Angiotensin convertingenzyme inhibitor(ACE)
Enalapril Renoprotective effect,hypotension, cough
Β2adrenergicreceptor(ADBR1)
B2 antogonists-albuterol,terbutaline
Bronchodilation,peripheral vasodilation
5-lipoxygenase(ALOX5) Leukotreine receptorantogonists
Asthma response
Dopaminereceptors(D1,D2,D3)
Antipsychotics-haloperidol, clozapine
Antipsychotic response,tardive dyskinesia
Vitamin K oxidoreductase(VKORC1)
Warfarin Anticoagulant effect,bleeding risk
Corticotropin releasinghormone receptor(CRHR1)
Glucocorticoids Bronchodilation, ostepenia
Vitamin D receptor Estrogen Bone mineral density

Differences in responsiveness to drugsAmong different species ‐Rabbits are resistant to atropineRats & mice to digitalisImp. to know while extrapolating results fromexperimental animals to manRacial differences in human beings ‐Blacks require higher andMongols require lower conc. of atropine & Ephedrineto dilate the pupil

Governs the speed and intensity of drugresponse.Use & action may vary with route,e.g. magnesium sulfate ‐given orally causes purgationApplied on inflamed areas - ↓ses swellingI.V. – produces CNS depression and hypotension

Exposure to insecticides , carcinogens, tobacco smoke ,charcoal broiled meat induce drug metabolism.
Type of diet can alter drug absorption set up in whichdrug is taken – hypnotics work better when taken atnight in quiet surroundings
Most drugs can cross the placenta andExpose the developing embryo and fetusto their pharmacologic and teratogenic effects .As a rule we try to avoid drugs during pregnancy, ifpossible. Factors affecting placental drug transfer anddrug effects on fetus
The physicochemical properties of drug.Rate at which drug crosses the placentaAnd amount of drug reaching the fetus.Duration of exposure to drug

Distribution characteristics in different Fetal tissues.Stage of placental and fetal development at the time ofexposure to drug.Drug passage across the placenta is dependent onLipid solubility and Degree of drug ionization .Lipophilic drugs diffuse readily acrossThe placenta and enter the fetal circulationFor example‐ thiopental , drug used forCesarean Section (CS) crosses the placenta almostimmediately and can produce sedation or apnea innewborn
Drug’s efficacy can be affected by Patient’sexpectations and attitude .Anxious patient requires more general anestheticPLACEBO “I will please”- relieves symptoms of illnessby creating expectations for the goodNOCEBO “I will harm” harms by creating a panic orfear for nothing, nocebo reactors are usuallypessimistic persons whose symptoms of illness do notrespond to medications
Placebo- this is an inert substance which is given in thegarb of medicine.MOA-It works by psychodynamic rather thanpharmacodynamic means and produces responseequal to active drugUSES-As a control device in clinical trial of drugsTo treat a patient who, in the opinion of physician doesnot require active drug

GI disease- in coeliac disease the absorption ofamoxicillin is decreased but that of cephalexin andcotrimoxazole is increasedAclorohydria decreases aspirin absorption by favoringits ionizationNSAIDs can aggravate peptic ulcer diseaseLiver disease-liver disease can influence drugdisposition in several ways-Bioavailability of drugs having high first passmetabolism is increased due to loss of hepatocellularfunction and portocaval shunting

Protein binding of acidic drugs-if serum albumin isreduced then more drug is present in free formMetabolism and elimination of some drugs- morphine,lidocaine and propranololProdrugs needing hepatic metabolism for activation –bacampicillin are less effectiveCirrhotics –sensitivity of brain to depressant action ofmorphine and barbiturates is markedly increasedLow clotting factors- increased prothrombin time
Aminoglycoside, phenobarbitone, digoxin –clearance ofdrugs primarily excreted unchanged in urine is reducedparallel to decrease in creatinine clearancePermeability of blood brain barrier is increased in renalfailure-opiates, barbirturates, phenothiazines,benzodiazepines, produce more CNS depressionTetracyclines have an anti-anabolic effect and accentuateuraemiaNSAIDs cause more fluid retentionNeprotoxic drugs-aminoglycosides, tetracyclines,sulfonamides, vancomycin, nitrofurantoin, cyclosporine,amphotericin-B- should be avoided

Decreasing drug absorption from GIT due to mucosaledema and splanhnic vasoconstriction.Ex-Procainamide, hydrochlorthiazideVolume of distribution is altered –loading dose oflignocaine should be reducedRetarding drug elimination as a result of decreasedperfusion and congestion of liver-dosing of drugsshould be reduced in lignocaine, theophylline
Hypo thyroid patients are more sensitive to digoxin,morphine and CNS depressantsHyperthyroid patients are more sensitive to arrhythmicaction of digoxin and less sensitive to inotropic action
Antipyretic drugs can lower body temperature onlywhen it is raisedThiazides induce more marked diuresis in edematouspatientsMyocardial infarction patients are more sensitive toadrenaline and digitalis induced cardiac arrhythmiasMyasthenics are very sensitive to curare, and in themweakness is aggravated by quinineSchizophrenics tolerate large doses of phenothizines
Head injury patients are prone to go into respiratoryfailure with normal doses of morphineAtropine, imipramine, furosemide, can cause urinaryretention in individuals with prostatic hypertrophyHypnotics given to a patient in severe pain may causemental confusion and deliriumCotrimoxazole produces a higher incidence of adversereactions in AIDS patients
Any drug can accumulate in the body if the rate ofadministration is more than the rate of eliminationA course of emetine should not be repeated within 6weeksLoading dose of digoxin is not needed with in oneweek
Requirement of higher dose of a drug to produce a givenresponse.Natural ‐ inherently less sensitive to the drug
rabbits are tolerant to atropineblack races are tolerant to mydriatics
Acquired – by repeated use of a drug in an individualwho was initially responsive. A continuous presence ofdrug in the body leads to toleranceExceptions –atropine, cocaine, sodium nitroprusside
Tolerance develops to sedative action ofchlorpromazine but not to its antipsychotic actionTolerance occurs to the sedative action ofphenobarbitone but not as much to antiepilepticactionTolerance occurs to analgesic and euphoric action ofmorphine, but not to constipating and miotic actions

Pharmacokinetic/drug disposition- the effectiveconcentration of the drug at the site of action isdecreased, mostly due to enhancement of drugelimination on chronic use- barbiturates andcarbamazepine induce their own metabolism, whilerenal excretion of amphetamine is accelerated afterregular intakePharmacodynamic/cellular tolerance- drug action islessened, cell of target organ become less responsiveEg- morphine, barbiturates, nitrates—desensitization/down regulation of receptors
Development of tolerance to pharmacologicallyrelated drugs.Alcoholics to barbiturates.Closer the drugs, more complete is the tolerancePartial tolerance between morphine and barbituratesBut complete tolerance between morphine andpethidine

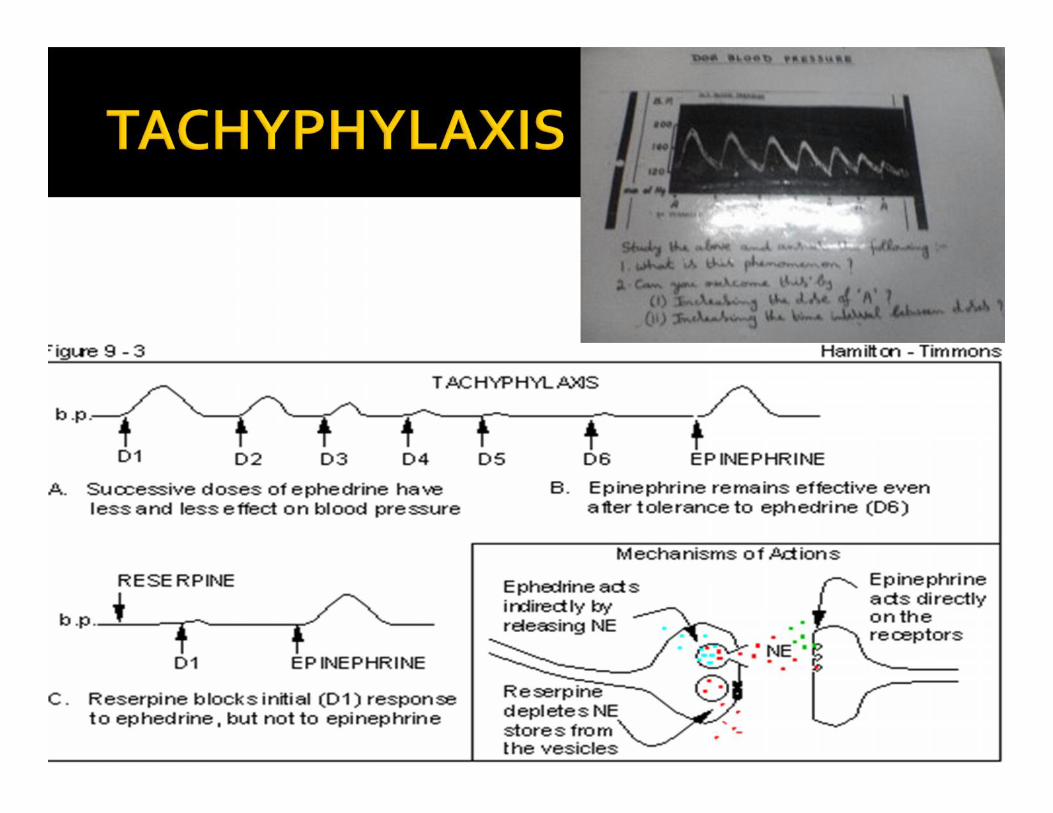
Rapid development of tolerance ‐ doses of a drugrepeated in quick succession result in markedreduction in response.Usually seen with indirectly actingdrugs e.g. Ephedrine , tyramine -which actby releasing catecholamines in the body ,Synthesis can’t match release when doses given inquick succession, stores get depleted

Therapeutic methods Tachyphylaxis –acute Tolerance -chronic
Clinical practice Rarely seen, as thedrug administration isnever done in quicksuccession
Can be seenTolerance developsslowly and is seen withintermittent dosingschedule
Original effect of is notpossible as there isexhaustion ofmediators or due tofaster desensitizationof the receptors
Effect can still beobtained by increasingthe dose

Natural-mycobacterium tuberculi are insensitive totetracyclinesAcquired-Tolerance of micro‐organisms toInhibitory action of antimicrobials.E.g. Staphylococcus to penicillin GCross tolerance- sulfonamides
