cl-'2~ immunolog¡c/assocfations of keloidsedculos/c… · more often than those with fair...
TRANSCRIPT
Cl-'2"~
IMMUNOLOG¡C/ASSOCfATIONS OF KELOIDS
Placik,
M.D., and Victor L. l,ewis,Jr.~M.D., F.A.C.S., Chicago, Illinoisatto]
lih99dof having keloids (7). The reported ratiosof black to Asian to white as well as male tofemale val-Y considerably (5, 8,9). A family historyof keloids is frequently elicited (10) and auto-somal recessive (11), autosomal dominant (12)and cross-linked recessive (13) patterns of inher-itance have been proposed.
WOUND~AIR resultSinaspectrumof lesions rang-ingfrom nearly "~arI.ess" healing to pathologicscars...Keloids are the seque.Iae of abnormal heal-ingprocesses. Keloids cortsist of scar tissue thatext~nds beyond fue confines of the originalwound O). Keloids tend to form within fue firstyear afrerthe mciting skin wound. In many sit-uations, fue historyfails to identify any precedinginjury. The presence of foreign material, hem~.toma, imection, inflammatory changes (2) or in-creased skin tension (3) are associated with asusceptibility to keloid formation. Keloids havea marked tendency to recur after excision. Keloidsmar become pruritic, tender and paimul. Thesymptoms and clinical behavior of keloids aresuggestive of an ongomg inflammatory process.
Despite extensive research, fue epidemiologic,histologic, endocrinologic and biochemical find-ings are not readiIy applicable to the diagnosisor management of keloids at the present time.The cause of keloids remainsan enigma; however,there is evidence to suppott a role for immunemechanisms in the pathogenesis of keloids. Anunderstanding of fue inflammatory changes con-tributing to keloid formation mar be essentialto understanding 'sca~less wound healing.
HISfOLOGIC FAcrORS
Keloids are likely to occur on the upper one-~ofthe body-the head, neck, chest, shouldersand arms (14). The most commonlv affected are asare fue }2re§tergal, lateral cheek in females andskin overlying the mandible, neckand ear. Skin,vith modified dermallavers (eyelids, areola, penisand scrotum) (15), in addition to skins lacking:sebaceous glands (16) and melanocytes (palmsand soles) (17), are rarelv affected by keloids.Melanocytes are absent. or present in only trace~ounts in fibrotic lesions (including keloid)(18). There are no known reports of keloids in.albinos.
There are no standardized criteria in estab-lishing the histopathologic diagnosis of keloids.Histologic definitions are vague and subjective{p, 19-21). A few communications suggest a con-tinuum of disease progressing from hypertrophicscar to keloid (1, 2, 20). Several authors nowbelieve that they can use the electron microscopeto distinguish keloids from hypertl-ophic scars(22-24).
EPlDEMIOLOGIC FACTORS
Humans are the onlv creatures affected by Fe-loids (4). Patlents .oetween tne aQ"es ot ten and20 xears demonstrate the highest ínCldence oikeloid development (5). They occur in all agegroups but are rarely found in newborns (6).The prevalence in the general population is un-known. Darkly pigmented individ~alsare affectedmore often than those with fair skin. Europeansresiding in the tropics acquire an increased like-
From the Division oí PIastic, Reconstructive and MaxillofacialSurgery, Deparnnent of Sut'gCry, Northwestern University MedicalSchool, Chi~o.
Reprint requests: Dr. Victor L. Lewis, Jr" 107 N. Fairbanks Ct,Suite 121O, Chicago, Illiriois 60611.
~DOCRINOLOGIC FACTORS
Endocrine factors have been implicated in thecause of keloids (25, 26). The ages of the greatestincidence of keloid corre late ,vith the periodsof physical (puberty) (27) and pituitary growth(28,29). The predisposition for kel~i~ for~atio~has been associated with abnormal nmction ofthe hypothalamus and eituit~~ (17,29, 30), ~!2M. (28, 29) and parathyroid (31). To date, no
~
185

~
186 SURGERY; gynecQúJ~&Obstetrics. August 1992. Volume 175
~fj»,¡~J
one hasverifiedapath"ogeli~tic mechanism""dem::"" "", ~""' """, c '"
onstrating"an endocflqologic cause of k~loids¡""""""" " "" ," """,
the preceding hypotlj~~" are conjecture""bas~dprimarily on clinicalpbservations. "
Keloids frequently,"gl'ow 1'apidly during preg-nancy (27) andtiiayregre~s wit~ menopa~se (5,28, 32, 33). A causal" relatlonsh1p of kel01d f01'-mation and estrogen(:Qntentration has not be endocumeI1ted despitei#u:tiple investig~tio~1S,(2",3"4), Reports of elevated testosterone bmd11'Ig bykeloid fibroblasts"have be en published; th~"~.creasedandroQ"eu"metabolism i_s_"believed to'<:on;;trigute,tQ keJoi~ patholrenesis (35)
" "" ""
BIOCI:IEt.llSTRY
'1 "1 ; el ~¡ ¡I,
~.!!¡4,
¡til'jl !"r ,¡ltt, J
and an increased (37,57) vel-SUS an unchanged(50) ratio of collagen type 1 to type III. hl,'es-tigators have attempted to con-oborate the afore-mentioned l"esults with findings of increasedquantities of fibronectin messenger ribonucleicacid (mRNA) (45); increased (37, 57) ,'ersus nor-mal amounts of type 1 procollagen specific mRNA(50) and normal values of type III aIld V Pl"O-collagen specific mRNA (50, 57) and type IVproc.ollagen specific mRNA (50) levels in keloid
speclmens.One author noted that there was no difference
in total (type 1, 11 and V) procollagen specificmRNA betlveen keloid and control fibroblasts ofall patients exaInined. However, the cultured fi-broblasts of keloid tissue exhibited an acceleratedl-ate of t)'Pe 1 and III procollagen specific mRNAwhen compared with the fibroblasts from thenormal appearing skin of the same patient (50).This would suggest that basal rates of collagens)'llthesis mar have heretofore been inappropri-ately assumed to be standal-dized '\~thin a controlpopulation. Future studies mar need to conu-astthe levels of collagen production of keloid tissuesrelative to the skin that is normal looking fromthe same patient. Despite the increased metabolicactivity, the growth charactel-istics (mean popu-lation doubling time, confluent density, cellularvolume or karyotype) of the cultured keloid fi-broblasts are no different than that of normaltissue fibroblasts (59). The accelerated rate ofcollagen synthesis by keloid fibroblasts returnsto normal if the cells are harvested from lesionsthat are greater than two to three years of age(60).
Several hypotheses based on the biochemicalfindings ha,'e been advanced to account for theaccumulation of collagen by interference withcollagen breakdown or by enhancement of col-lagen production. As mentioned previously, thereis an abundance of alpha-globulins (alpha-one-antitrypsin and alpha-tlvo-macroglobulin) in ke-loid tissue when compared with normal skin orscar fibroblast strains (44). Alpha-globulins inhibitcollagenase and mar result in decreased collagendegradation. However, the collagenase contentof keloids is ,'ariable and alpha-globulins do notexclusivel)' accumulate in keloids; they are alsofound in hypertrophic scars. lndividuals have hadatypical keloids after dermabrasion while on orafter l"eceiving isotretinoin (61), which is knownto reduce the production of collagenase (62).
l~esults of other studies have ShO'Vll that thedeposition of collagen, measured in terms of the
Keloid rissues con~~ itJicreased .qllan,titiesofwater (20, 36, 37), calclUm(38), hlstamme (20,39, 40), acid phosphatase (41), alanine trattsam-inase, lactatedehydrógenase (42, 43), alpha~lo~ulins (44), fibronectin (45) elastin and glyc~saminoglycans (37) andproteogl)'cans su~h aschondroitin four sulfate: (16). An additionaI find-ing that has be en repeatedly confirmedis thatexcessive collagen deposition is a hallmark ofkeloids (20, 47-50). Keloid deri,'ed fibroblasts,in vitro, produce incr<:;ased amounts of coll~enper cell in compari~n with normal skin andscar fibroblast strains (~1--53). The keloid fibro-blasts s tlIesize excessive amounts of colla enthroughou! the in vitro lifespan (when replatedbeyond four passages). It is believed that thefibroblasts are functioning autonomously becauserepeated subculturing techniques isolate tlIe fi-broblasts from the influence of any in vivo factors,that is, in fue absenceof any humoral subst~ces.
The explanation for the exuberant productionof collagen obseIVed in keloid is unknown. Theconcentrations of galactosylhydroxylysyl glucosyl-transferase (50), proline hy<Jroxylase (20, 39, 47,48, 50), soluble collagen{20, 36) and abnormalcollagen cross link~s {54) are also increasedin keloid tissue. Furthenl1ore, increased (20), de-creased (55) and unchanged (49, 56) amountsof collagenase have been cited in keloidal versusnormal skin tissue colIagenase assays. The deg-radation of newly syntl1esized procollagen poly-e tides is decreased in fibroblast cultures de-
rived from keloid tissue when compared witnnormal sk1n (37).
Reportedchanges in the collagen content °.rkeloids il1cludeabund3nt type 1 collagen (57)versus unaltered quantities of typeIcollagel1 {50,58), excessive type I.H collagen (~7,58)versusnormal amounts of type III collag~ (57, 58)
¡~
rJ!
Placik and Lewis: IMMUNOLOGIC ASSOCIAnONSOF KELOIDS 187
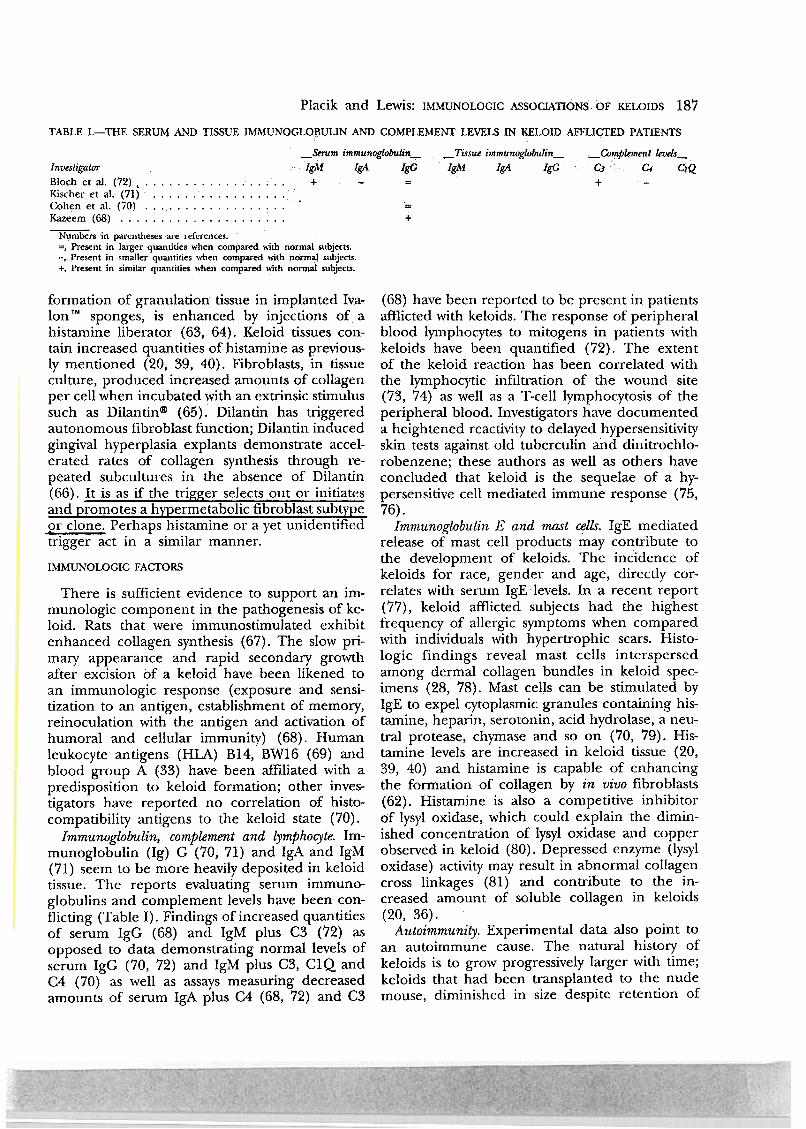
TABLE I.,-".THE SERUM AND TISSUE IMMUNOGLO~ULIN A.~D COMPLEMENT LEVELS IN KELOID AFFLICTED PATIENTS
_Serom immunogú>bulin- ~Tissue i7nmunoglQbulin- _OJmplement levels-lnvestigator IgM 19A IgG 19M 19A 19G CJ C4 cIQBloch et al. (72) , '.. ..+ -= + -Kischeretal.(71) """""""'"Cohen et al. (70) ,..Kazeem(68) Numben in parentlleses are references.
=,Present in larger quantities when compared "ith normal subjects.-, Present in smaller quantities,,'hell compared 'fÍlh n()rm3:J subjecr...+, Present in similar qualuities ,,'hen compared "ith normal subjecr...
+
formation of granulation tissue in implanted Iva-Ion TM sponges, is enhanced by injections of a
histamine liberator (63, 64). Keloid tissues con-tain increased quantities of histamine as previous-ly mentioned (20, 39, 40). Fibroblasts, in tissueculture, produced increased amounts of collagenper cell when incubated with an extrinsic stimulussuch as Dilantin@ (65). Dilantin has triggeredautonomous fibroblast function; Dilantin inducedgingival hyperplasia explants demonstrate accel-erated rates of collagen syntllesis through re-peated subcultures in fue absence of Dilantin(66). It is as if the trigger selectsout 01' initiatesaIld promotes a hypermetabolic fibroblast subtyp~91' clone. Perhaps histamine or a yet unidentifiedtrigger act in a similar manner.
IMMUNOLOGIC FACTORS
There is sufficient evidence to support an im-munologic component in the pathogenesis of ke-laido Rats that were immunostimulated exhibirenhanced collagen synthesis (67). The slow pri-mary appearance and rapid secondary growthafter excision bf a keloid have been likened toan immunologic response (exposure and sensi-tization to an antigen, establishment of memory,reinoculation with the antigen and activation ofhumoral and cellular immunity) (68). Humanleukocyte antigens (HLA) B14, BW16 (69) andblood group A (33) have been affiliated with apredisposition to keloid formation; other inves-tigators have reported no correlation of histo-compatibility antigens to the keloid state (70).
Immunoglobulin, complement and lympho~te. Im-munoglobulin (Ig) G (70, 71) and IgA and IgM(71) seem to be more heavily deposited in keloidtissue. The reports evaluating serum immuno-globulins and complement levels have been con-flicting (Table 1). Findings of increased quantitiesof serum IgG (68) and IgM plus C3 (72) asopposed to data demonstrating normal levels ofserum IgG (70, 72) and IgM plus C3, C1Q andC4 (70) as well as assays measuring decreasedamounts of serum IgA plus C4 (68, 72) and C3
(68) have been reported to be present in patientsafl1icted \vith keloids. The response oí peripheralblood lymphocytes to mitogens in patients withkeloids have been quantified (72). The extentof the keloid reaction has been correlated withthe lymphocytic infiltration of fue wound site(73, 74) as "lell as a T-cell lymphocytosis of theperipheral blood. Investigators have documenteda heightened reactivity to delayed hypersensitivityskin tests against old tuberculin and dinitrochlo-robenzene; these authors as well as others haveconcluded that keloid is the sequelae of a hy-persensitive cell mediated immune response (75,76).
Immunoglobulin E and mast cells. IgE mediatedrelease of mast cell products mar contribute tofue development of keloids. The incidence ofkeloids for race, gender and age, directly cor-relates with serum IgE levels. In a recent report(77), keloid afl1icted subjects had the highestfrequency of allergic symptoms \'lhen compared"lith individuals with hypertrophic scars. Histo-logic findings l-eveal mast cells interspersedamong dermal collagen bundles in keloid spec-imens (28, 78). Mast cells can be stimulated byIgE to expel cytoplasmic granules containing his-tamine, heparin, serotol-rin, acid hydrolase, a neu-tral protease, chymase and so on (70, 79). His-tamine levels are increased in keloid tissue (20,39, 40) and histamine is capable of enhancingthe formation of collagen by in vivo fibroblasts(62). Histamine is al so a competitive inhibitorof lysyl oxidase, \'lhich could explain the dimin-ished concentration of lysyl oxidase al-rd correrobserved in keloid (80). Depressed enzyme (lysyloxidase) activity mar result in abnormal collagencross linkages (81) and contribute to the in-creased amount of soluble collagen in keloids(20, 36).
Autoimmunity. Experimental data algo point toan autoimmune cause. The natural history ofkeloids is to grow progressively larger "lith time;keloids that had been transplanted to the nudemouse, diminished in size despite retention of

188 SURGERY, C.ynecology & Obsti?tncs' August
theoriginal histowe (82, 83). These results sug-gest th4t the acc~lerated growth of autogenous(versusti"anspl~ted) keloids mar require immu-nologicstimulation. Another team of researchersstated that they ~ere capable of producing keloid$after immunization with autologous skin (84).An autoimmune ~esponse to trapped sebum hasbeen assumed (85) : Based on this hypothesis,the investigators have claimed to have prepareda vaccine and to have successfully desensitizedten of 1) patientsto keloid recurrence (86).
AutoiIIimune(noncomplement fixing) antifi-broblastantibodies (AFA) have been extracted..from thel~phocyte lsolates of every kelolda;¡patient exarnined in a recent study; these anti-bodies were specifically dil-ected against the fi-broblasts of fue individua.ls andwere not detectedin the lympho~e eluates of subjects with norm~or hypertI-ophic scars (87). The authors hypoth-esized that fue AFA have a fibroblast stimulatingraJe in fue pathogenesis of keloid, One of thesame investigatorsdescribed the presence of sim-ilar antibodies in patients with psoriasis; theseantibodies are directed against psoriasis specificnonhistone proteins. This discovery suggests apossible mechanism by which antibodies mayexert control ayer the expression of fue generesponsible for psoriasis (88, 89), Noncómple-ment binding AFA have also been reported tooccur in an instance of hematoporphyrin-inducedkeloid (90). Other investigators did not detectthe presence oí AFA in five patients with keloids(91),
Immunologic mediators. The influence of immu-nologic mediators (cytokines and peptide growthfactors) must also be considered. Excellent re-views detaling the role of these substances inwound healing are available (92, 93), These sub-stances (l~phokines, monokines, growth factors)affect fibroblast proliferation, chemotaxis and col-lagen, col..lagenase and hyaluronic acid produc-tion (94). Recent reports have focused on thecalterations ofcytokine production in patients withkeloids. Peripheral blood monoclear cell fractionsfrom black patients with keloids demonstrate de-pressed production of interferon-alpha, inter-feron-garnma and interleukin-2 and enhancedproduction of tumor necrosis factor alpha andinterferon-beta when compared with normal pa-tients (95).
Some of these agents promote collagen accu-mulation. Interleukin-l, a monokine, stimulatescollagen production (94)., Antigen stimulated T-cells produce l~phokines that are capable of
1992.
110lulne 175
stimulating fibroblast proliferation and collagensynthesis (96). Accumulations of T-cells in claseassociation with fibroblasts have be en describedin the keloid-like lesions of patients with progeria.It is believed that these activated T -cells interactwith fibroblasts through a lJInphokine interme-diary, resulting in accelerated fibroblast growthand production of unusual amounts of type IVcollagen (74, 97). Enhanced collagen depositionby cu.ltured fibroblasts has been reported whenly¡nphokine-rich supernatants, derived from phy-tohemagglutinin (PHA) stimulated cells, wel-eadded to the fibroblast medium (98). Thesely¡nphokines have been identified and charac-tel-ized as a 100,000 to 170,000 molecular ,veightly¡nphokine (99) and transforming gro,vth factorteta (100, 101). Transforming gro,vth factor tetahas also enhanced the activity of epidermalgrowth factor on keloid derived fibroblast cultures(102). Adult rat wounds treated with neutralizingantibody to transforming gro,vth factor-teta havereportedly healed ,vithout formation of scar tissue(103).
Substances derived from leukocytes can alsolimit the deposition of collagen. Lymphocytes can
produce collagenase (104). Monokines can de-crease collagen deposition-interleukin-1 and tu-mor necrosis factor alpha stimulates fibroblast
collagenase production (93, 105), while teta in-terferon inhibits collagen production (106). Ahuman monocyte-macrophage factor, labeledmononuclear cell factor (MCF), which is capableof stimulating collagenase synthesis by culturedfibroblasts, has be en described (107, 108). T-celllymphocytes or immunoglobulin interact withmonocytes-macrophages to modulate the produc-tion of MCF. Human MCF is similar to murineinterleukin-1. Stimulated T-cellly¡nphocytes pro-duce lymphokines such as alpha and gamma in-terferon that can inhibir fibroblast collagen pro-duction (99, 106, 109).
Results of preliminary studies have sho,vn thatimmunotherapy mar have a role in the treatmentof keloids. Investigators have injected gamma in-terferon into keloidal and hypertrophic lesions;they claim that the treatments produced at leasta 50 percent reduction in the size of five often scars studied, with no serious toxic side effects(110, 111). Another group of investigators haveconfirmed these results, using intralesional re-combinant interferon-gamma in the treatment ofkeloidal scarring (112). Intralesional injectionsof interferon-alpha-2b have produced reductionin the size of a progressively enlarging keloid
Placik and Lewis: IMMUNOLOGIC ASSOCIAnONS OF KELOIDS 189
(113). Topical cyclosporin resulted in uniformreductions in T -cell numbers in keloidal scars(114) The use of neutralizing antibody to trans-forming growth factor-beta was previously men-tioned (103).
FIBROBLAST HETEROGENEITY
interact with nuclear proteins, as described pre-viously.
Fibroblast heterogeneity mar account for theabnol-mal fibl-oblasts that have been recoveredfrom scar tissues. If the cell lines are atypical,the question arises as to why fue lesions are lim-ited to fue skin, when fibroblasts are presentiliroughout the body? Keloids are focal pathologicscars witllout systemic manifestations. A theol-Yfor the propensity for lesions to develop in spe-cific anatomic locations has been proposed inthe results of another study (81). The authorof tllis study believes tllat secondary adaptationsby fibroblasts to alterations in the regional en-vironment mar render them particularly sensitiveto circulating substances. Fibroblasts from the re-ticular dermis synthesize more collagen in re-sponse to a circulating factor than tll0se fromthe papillary dermis in patients with scleroderma(120, 121). Estrogen will cause different responsesin collagen production by lung derived fibroblastsin comparison ",ith dermis derived fibroblasts(122). Hypertrophic scar-derived fibroblasts dem-onstrated a decreased responsiveness to epider-mal growth factor and tumor necrosis factor alphaand significantly elevated collagen synthesis inresponse to transforming growtll factor beta whencompared with normal cells (123).
Keloid fibroblasts, in vitro, exhibit a reduceddependence on serum growth factol-s similar tofetal cells reflecting an inappropriate expressionof growth related genes (102). These data marindicate that fue underlying mechanism respon-sible for fibroplasia mar be identical in keloidand fetal wounds. Clinically, it is evident thatkeloid scars differ tremendously when comparedwith healing of fetal \'lounds, which is gene rallyconsidered to be scarless. Clearly, the abnormalbehavior of keloid fibroblasts is initiated and pro-moled by the environment of fue wound. It isnot known why the keloid wounds do not displaythe same degree of regulation of collagen de-position that fetal \'lounds exhibit. The "second-ary adaptations" of keloid fibroblasts mar alsorender them resistant to the typical negative feed-back signals that normal cells obey. In anotherstudy, it was proposed that keloid fibroblasts marbe unresponsive to normal feedback signals thatregulate physiologic wound healing (52). The au-thors of the cun-ent article conducted a studythat suggested that lymphocyte derived factorsdepress normal skin fibroblast collagen synthesis,\'lhereas scar and keloid cells are progressivelymore resistant to the depressant effects. Thus,
lntrinsic fibroblast abnormalities interactingwith tl1e immunologic res pon se mar result inkeloids. Results of experimental studies llaveshown that keloid fibroblast stI'ains demonstratean autonomous capacity to synthesize large quan-tities of collagen (52). These fibroblast celllineswere subcultured more than three passages and,therefore, were performed in fue absence of anyin vivo humoral factors.
Heterogeneous fibroblast populations are likelyto be present within wounds at the same time(synchronous). Studies on cloning llave revealedheterogeneity with respect to fue growth potentialof human fibroblasts (115). ~fetabolic differencesamong human fibroblasts have been identified;these cells, when cultured and replated, will main-tain their differentiation through late passage(116). Cultured fibroblasts harvested from thedermis of patients ,vith progressive systemic scle-rosis produce more collagen than normal cells(117). Subpopulations of fibroblasts mar algo varywith the age of the wound (metachronous). Forexample, myofibroblasts are abundant in the earlystages of wound healing (third week), but rapidlydiminish in number by fue 20th week (118).Myofibroblasts are not abundant in mature ke-loids (118).
The different subpopulations are likely to ex-press different antigenic surface markers. Thisphenomenon mar explain fue presence of anti-fibroblast antibodies early in wound healing andthe absence of immunologic activity in olderwounds in which fue keloid fibroblasts mar reflecta more mature, nonantigenic and homogeneous,fibroblast population. Myofibroblasts are presentin normal quantities in mature keloids (118, 119).Is the primary pathologic lesion in keloids at-tributable to AFA directed against and stimulatinga susceptible fibroblast cell line to produce ex-cessive amounts of collagen, or to an abnormalfibroblast population with an increased rate ofcollagen synthesis that present an antigenic chal-lenge triggering the secondary appearance ofAFA? Humoral immunity results classically in thesynthesis of complement binding antibodies. TheAFA are noncomplement fIXing and mar instead

190 SURGERY; Gynecology & Obstetncs. August 1992. Volu~ 175
...potentlal expl.anat1o~$for the pat.hologlC b~!tav-lar and locallZed natW"e of kelolds are attac-quired susceptibilio/ and resistance of regiQnalfibroblasts to circillating substances, thatls; in-
hibitoryagents, immunologic mediators, growthfactors or supstances, limited to the woul1dsit~,which induce fibroblast transformation or a diE:;ferentiatedand localized fibroblast subpopulationthat inherently produces excessive quantitiesof
collagen.
SUMMARY
~:
1'11 : "
1..,j" 1'
i!:1J"j
The mechanismsunderlying fue pathogenesisofkelóids havenot been fully characterized de-spite extensive past and present research. Resultsofpast and present studies have ShO'Vll that fueimmune system is actively involved in the deye.1-opment oftheselesions. Future investigationsintofue biochemistry and immunologic factors ofke-loids are anticipated and expected to produceadditional insight. The inability to identify cel-lular (fibroblast) abnormalities has led most in-vestigators to focus ón fue humoral regulatorsofwound healing., that is, biochemical substances,immunologic mediatórs and growth factors. Fu-ture studies are needed to confirm or refutefue p!esence of AFA. AFA, if they exist, marprove to be useful as immunologic markers ofkeloids and mar help distinguish keloids fromhypertrophic scar in the early stages of woundhealing. The influence of immunologic mediatorsmar be more impressive early in the developmentof scars. "Young" or "early" is defined as lessthan two years of age, whereas "old" or "late"keloids are more than two years of age. We sug-gest thatfuture studies stratify keloids into earlyversus lateand also measure the rates of collagensynthesis of fibroblasts derived from fue normaland abnormal specimens from the same patient.Analysis of fue leukocyte factors will clarify therole the immune system has in the regulationof collagen synthesis. Preliminary investigationshave shown that immunotherapy mar be of valuein fue treatment of keloids. The role of fibroblastheterogeneity needs to be investigated. It is notknown which aspects of fibroblast heterogeneityare responsible for the localized and acceleratedrates of collagen synthesis of keloid fibroblasts.
[:f\il'¡ '" .t, '!
tf': l li\¡ ..1~..c. 11,.,""', 'ti
jJ':.~i
111
REFERENCES'
l. Peacock, E. E., lr., Madden, l. W., and Trier, W. C.Biologic basis fór the treatment of keloids and hy-pertrophic scars. South. Med. l., 1970, 63: 755-760.
2. Ketchum, L. D. Hypertrophic scars and keloids. CIin.PIast. Surg., 1977, 4: 301-310.
3. Ketchum, L. D., Cohen, l. K, and Masters, F. W.
Hypertrophic scars and keloids. A collecrive re\iew.Plast. Reconstr. Surg., 1974, 53: 140-154.
4. Davies, D. M. Scars, h}pertrophic scars, and keloids.Br. Med. T., 1985, 290: 1056-1059.
5. Cosman, B., Crik~~ir, G. F.,. Ju, D. M., and others.The surgical treatrnent of keloids. Plast. Reconstr.Surg., 1961, 27: 335-358.
6. Cohen, l. K, and McCoy, B.J. The biolog}' and controlof surface overhealing. World J. Surg., 1980, 4: 289-295.
7. Edington, G. M., andGilles, H. M. Pathology in theTropics. P. 589. London: Edward AInold Ltd., 1969.
8. Bohrod,M. G. Keloids and sexual selection; study inracial distributi9n of disease. Arch. Denn. S}'Ph. Chic.,1937, 36: 19.
9. Tempest, M. N. Hypertrophic scarring and keloids.In: Tropical Surgery. Edited by S. l., and others. P.80. New York: McGra\v-Hill Book Co., 1971.
10. Cohen, l. K, and P$cock, E. E., Jr. Keloids andh}pertropic scars.Jn:P~astic Surgery. Edited by J. G.McCarthy. Vol. l, Chap, 21, Pp. 732-747. Philadelphia:W. B. Saunders Co., 1990.
11. MurraY,J. C., PolIack, S.V., and Pinnell, S. R Keloids:A Revie\v. J. AIn. Acad.Dennatol., 1981, 4: 461-470.
12. Bloom, D. Heredity of keloids: A re\ie\v of the lit-erature and report~f a family \.,ith multiple keloidsin five generations. N. Y. State J. Med., 1956, 56:511-519.
13. Gominne, L. A new probably x-linked inhe¡ited S}'ll-drome: congenital muscular torticollis, multiple ke-loids, cryptorchidismand renal dysplasia. Acta Genet.Med. (Roma), 1968, 17: 439.
14. Crockett, D. J. Regional keloid suscepribility. Br. J.Plast. Surg., 1964, 17: 245-253.
15. Parsons, R. W. A case of keloid of the penis. Plast.Reconstr. Surg., 1966, 37: 431.
16. Rudolph R. Wide spread scars, h}'Pertrophic scars,and keloids. Clin. Plast. Surg., 1987, 14: 253-260.
17. Koonin, A.]. The aetiology of keloids: a revie\v ofthe literature and a ne\v hypothesis. S. Mr. Med. J.,1964, 38: 913-916.
18. SmolIer, B. R., McNutt, N. S., and Hsu, A. HMB-45recognizes stimulated melanocytes. J. Cutan Pathol.,1989, 16: 49-53.
19. Mancini, RE., and Quaife, J. V. Histogenesis of ex-perimentalIy produ(;ed keloids. J. lnvest. Dermatol.,1962, 38: 143-181;
20. Cohen, l. K., Diegelmann, R. F., and Keiser, H. RColIagen metabolism in J<eloid and h}pertrophic scar.In: The Ultrastructure of ColIagen: lts Relarion tothe Healing of Wounds and to the Management ofHypertrophic Scar. Edited by J. J. Longacre. Chap.15, Pp. 119-212. Springfield, IlI.: Charles C ThomasPublisher, 1973.
21. Lever, W. F. Tumors of fibrous rissue. In: Histopa-thcilogy of the Skin. Edited by W. F. Lever and G.Schaumberg-Lever. 6th ed., Chap. 29, Pp. 604-605.Philadelphia: J. B. Lippincott Co., 1983.
22. Kischer, C. W., and Shetlar, M. R. Collagen and mu-copolysaccharides in the hypertrophic scar. Connect.Tissue Res., 1974, 2: 205-213.
23. Knapp, T. R., Daniels, J. R., and Kaplan, E. N. Patho-logic scar fonnation. Am J. Pathol., 1977, 86: 47-70.
24. RockwelI, W. B., Cohen, l. K, and Ehrlich, H. P.Keloids and hypertrophic scars: a comprehensive re-view. Plast. Reconstr. Surg., 1989, 84: 827-837.
25. Jacobsson, F. The treatment of keloids at Radium-hemmet: 1921-1941. Acta Radiol. (Stockh.), 1948, 29:251-267.
26. Van den Brenk, H. A. S., and Minty, C. C.J. Radiationin the management of keloids and h}pertrophic scars.Br. J. Surg., 1960, 47: 595-605.

:"e\'lTis:
IMMUNOLOGIC ASSOCIA.nON~ OF KELOIDS 191Placik and
27. Allan, J. C., and Keen, P. S. Tl1e management ofkeloid in the South Mrican Bantu. So Mr. Med. J.,.1954, 28: 103+1037.
28. Asboe-Hansen, G. H}'Pertrophic scars andkeloid. Der-matologica, 1960, 120: 178-184.
29. Garb, J., and Stone, M.. J. Keloids: Review of theliterature and a report of eighty cases. Am. J. Surg.,1942, 58: 315-335.
30. Asboe-Hansen, G~ Endocrine control of connective tis-sue. Am. J. Med., 1959, 26: 470-484.
31. Pautrier, L. M., and Zorn, R. Calcémie: Teneur encalcium de la peau dans les chéloides et les acnéschéloidiennes. Bull. SOCo Fr. Derm. Syph., 1931, 38:953-961.
32. Oluwasanmi, J. O. Keloids in the Mrican. Clin. Plast.Surg., 1974, 1: 179-195.
33. Ramak1;shnan, K. M., Thomas, K. P., and Sundara-rajan, C. R. Study of 1,000 patients with keloids "1South India. Plast. Reconstr. Surg., 1974, 53: 276-280.
34. Crikelair, G. F., Ju,D. M. C., Cosman, B., and others.Scars and Keloids. In: Reconstructive Plastic Surgery.Edited by J. M. Converse. Vol. 1, Pp. 413-441. Phil.:adelphia: W. B. Saunders Co., 1977.
35. Ford, L. C., King, D. F., Lagasse, L. D., and Newcomer,V. Increased androgen binding in keloids: A prelim-inary communication.J. Dermatol. Surg. Oncol., 1983,9: 545-547.
36. Harris, E. D., Jr., and Sjoerdsma, A. Collagen profi1ein various clinical conditions. Lancet, 1966,2: 707-711.
37. Abergel, R. P., Pizzurro, D., Meeker, B. S., and others.Biochemical composition of the connective tissue inkeloids and analysis of collagen metabolism in keloidfibroblast cultures. J. lnvest. Dermato1., 1985, 84: 38+390.
38. Psillakis, J. M., Jurge, F. B. de, Sucena, R. C., andothers. Water and electrolyte content of normal skin,scars, and keloid. Plast. Reconstr. Surg., 1971, 42:272-274.
39. Caben, l. K., Beaven, M. A., Horáková, Z., and Keiser,H. R. Histamine and collagen synthesis in keloid andhypertrophic scar. Surg. Forum, 1972, 23: 509-510.
40. Hakanson, R., Owman, C., and Sjoberg, N. O. Directhistochemical demonstration of histamine in cutane-ous mast cells: urticaria pigmentosa and keloids. Ex-perientia, 1969, 25: 854.
41. 1m, M. J. C., and Hoopes, J. E. Alpha-naphthyl acidphosphatase activity in normal human skin and ke-loids. J. lnvest. Dermatol., 1971, 57: 18+189.
42. Hoopes, J. E., Su, C.-T., and 1m, M. J. C. EnZ}'meactivities in hypertrophic scars and keloids. Plast. Re-constr. Surg., 1971, 47: 132-137.
43. Kemble, J. V. H., and Brown, R F. R. Enzy¡ne activitiesin human scars, hypertrophic scars, and keloids. Br.J. Dermatol., 1976, 94: 301-305.
44. Cohen, l. K., Diegelmann, R. F., and Bryant, C. P.Alpha globulin collagenase inhibitors in keloid andhypertrophic scar. Surg. Forum, 1975, 26: 61-62.
45. Babu, M., Diegelmann, R., and Oliver, N. Fibronectinis overproduced by keloid fibroblasts during abnormalwound healing. Mol. CeII. Biol., 1989, 9: 1642-1650.
46. Bazin, S., Nicoletis, C., and Delaunay, A. lntercellularmatrix of hypertrophic scars and keloids. In: Biologyof the Fibroblast. Edited by E. Kulonen and J. Pikka-rainen. Pp. 571-578. London: Academic Press lnc.,1972.
47. Cohen, l. K, Keiser, H. R., and Sjoerdsma, A. Collagensymhesis in human keloid and hypertrophic scar. Surg.Forum, 1971, 22: 488-489.
48. Cohen, J. K., and Keiser, H. R Collagen synthesisin keloid and hY1)ertrophic scar following intralesionaluse of triamcinolone. Surg. Forum, 1973, 24: 521-523.
49. Craig, R. D. P., Schofield, J. O., and Jackson, D. S.
Collagen bios}11thesis in non:nal human skin, nonnaland hypertI'ophic scar and keloid. Eur. J. Clin. lnvest.,1975,5: 69-74.
50. Ala-Kokko, L., Rintala, A., and Savolainen, E-R Col-lagen gene expression in keloids: Analysis of collagenmetabolism and type 1, m, IV, V procollagen mRNAsin keloid tissue and keloid fibroblast clutures. J. lnvest.Dermatol., 1987, 89: 238-244.
51. Cohen, l. K, Diegelmann, R. F., and McCoy, B. El-e\'ated collagen synthesis in cultured keloid fibroblasts.Surg. Forum, 1977,28: 526-527.
52. Diegelmam1, R. F., Cohen, l. K, and McCoy, B. J.Gro\\'th kinetics and collagen synthesis of nonnal skin,nonnal scar, and keloid fibroblasts in viEra. J. CellPhysiol., 1979, 98: 341-346.
53. Cohen, l. K, and McCoy, B. J. Keloids and hyper-trophic scars. In: Problems in Aesthetic Surgery. Ed-ited by R. Rudolph. Pp. 141-157. Sto Louis: C. V.Mosby Co., 1986.
54. Weber, L., Meigel, W. N., ;lnd Spier, W. Collagenpol\'ll1orphism in pathologic human scars. Arch. Der-matoJo Res., 1978, 261: 63-71.
55. Harper, E., and Gross, J. Collagen degradation innormal and abnormal tissues. In: The Ultrastructureof Collagen: lts Relation to the Hea1ing of Woundsand to the Management of Hypertrophic Scar. EditedbyJ.J. Longacre. Chap. 11, pp. 175-176. Springfield,111.: Charles C Thomas Publisher, 1973.
56. Milsom,J. P., and Craig, R. D. P. Collagen degradationin cultured kc1oid and h)rpertrophic scar tissue. Br.J. Dermatol., 1977, 89: 635-644.
57. Vino, J. Perejda, A. J., Abergel, R. P, and others.,-\ltered steady-state ration of type l/m procollagenmR.i'\TAs corre late s with selectively increased rype 1procollagen biosynthesis in cultured keloid fibroblasts.Proc. Natl. Acad. Sci. U. S. A., 1985, 82: 5935-5939.
58. Clore, J. N., Cohen, l. K., and Diegelmann, R. F.Quantitative assays of types 1 and m collagen syn-thesized by keloid biopsies and fibroblasts. Acta Bio-chim. Biophys. Acad., 1979, 586: 384-390.
59. Russell, J. D., and Witt, W. S. Cell size and gro\vthcharacteristics of cultured fibroblasts isolated fromnonnal and keloid tissue. Plast. Reconstr. Surg., 1976,57: 207-212.
60. Craig, R. D. P., Schofield, J. O., and Jackson, D. S.ColIagen biosynthesis in normal and hypertrophicscars as a function of the duration of the scar. Br.J. Surg., 1975, 62: 741-744.
61. Rubenstein, R., Roenigk H. H., Jr., Stegman, S. J.,and Hanke, C. W. Atypical keloids after dermabrasionof patients taking isotretinoin. J. AIn. Acad. Dermatol.,1986, 15: 280-285.
62. Abergel, R. P., Meeker, C. A., Oikarincn, H., andVino, J. Retinoid modulation of connective tissue me-tabolism in kcloid fibroblast cultures. Arch. Dcrmatol.,1985, 121: 632-635.
63. Sandberg, N. Accelerated collagen formation and his-lamine. Nature, 1962, 194: 183.
64. Kahlson, B., Nilsson, K., Rosengren, E., and Zederfeldt,B. Wound healing as dependent on rate of histaminefonnation. Lancet, 1960, 2: 230-234.
65. Benveniste, K., and Bitar, M. Effects of phenytoin oncultured human gingival fibroblasts. In: Phenytoin-lnduced Teratology and Gingival Pathology. Editedby T. M. Hassell, and others. Pp. 199-213. New York:Raven Press, 1980.
66. Hassell, T. M., Page, R. C., and Narayanan, A. S.Diphenylhydantoin (dilantin) gingival hyperplasia:drug-induced abnormality of connective tissue. Proc.;"ratl. Acad. Sci. U. S. A., 1976, 73: 2909-2912.
67. Oluwasanmi, J. O., Lucas, D. O., and Chvapil, M.Effect of a concurrent immune response on the col-
,192 SURGERY, Gynecológ'}!& Obstetncs' AugusH992' Volume 175
~~
of psoriasis patieritSrea~tive\\TÍth basal nuclei. ActaDerm. Venereol. (StóCkh.) , Suppl., 1.984, 113: 50-54.
89. Cormane, R. H. P¿;rtortal communication.90. Nunzi, E., Parodi, A., Rebora,A.lmmunofluorescence
findings in haematoporph)nn-induced keloid. Br. J.Dermatol., 1983, 108: 263-266.
91. Placik, O., Le\\TÍs, V. L., Jr., Dixit, S. The etfects ofIymphocyte eluates, bea¡;ng antifibroblast antibodies,on collagen synthesis by keloid fibroblast strains. Sub-mitted for publication. Presented at thePlastic SurgeryResearch Council, April 1989, Atlanta, Georgia.
92. McGrath, M. H. Peptide growth factors and woundhealing. Clin. Plast. Surg., 1990, 17(3): 421-432.
93. Barbul, A. Immune aspects of wound repair. Clin.Plast. Surg., 1990, 17(3): 433-442.
94. Fibroblasts. In: Infla,n:lmation: Basic PrincipIes andCli:nical Correlates. ~~~byJ. 1. Gallin, l. M. Gold-steln, and R. Snyderlrian;Ch~. 30, Pp. 591-592. NewYork: Raven Press, 1988.
95. McCauley, R L., Chorra, V., Li, Y-Y., and others.Altered cytokine production in black patients. Pre-sented at the 37th Annual Meeting of Plastic SurgeryResearch Council. April 1992, Toronto, Ontario.
96. Wahl, S. M., Wahl, L. ~., and McCarthy, J. B. Lym-phocyte-mediated activadon of fibroblast proliferationand collagen production. J. Immunol., 1978, 121: 942-946.
97. Wahl, S. M., ~nd Gately, C. Lo Modulation of fibroblastgrowth by a lymphokine of human T cell and con-tinuous T cell line ori~.. J. Immunol., 1982, 130:1226-1230.
98. Johnson, R. L., and Zitf, M.J. Lymphokine stimulationof collagen accumulation. J. Clin. Invest., 1976, 58:240-250.
99. Postlethwaite, A E., Smifu, G\N., Mainardi, C. L.,and others. L}rmphocytemod\Jlation of fibroblast func-tions in viera: stimulatidh andinhibition of collagenproduction by ditferent etfector molecules. J. Im-munol., 1984, 132: 2470-2477.
100. Ignotz, R A., and Massaque, J. Transforming growthfactor ~ stimulates the express ion of fibronectin andcollagen and their incorporation into the extracellularmatrix. J. Biol. Chem., 1986, 261: 4337-4345.
101. Kehrl, J. H., Wakefield, L. M., Roberts, A. B., andothers. Production of transforming growth factor ~by human T lymphocytes and its potential role infue growth regulation of T cell growth. J. Exp.. Med.,1986, 163: 1037-1050,
102. Russell, S. B., Trupin.K P., 'Rodriguez-Eaton, S., andothers. Reduced gro~-factor requirement of keloid-derived fibroblasts m;a:y account for tumor growth.Proc. Natl. Acad. Sci. U. S. A., 1988, 85: 587-591.
103. Shah, M., Foreman, D. M., and Ferguson, M. W. J.Control of scarring in adult wounds to neutralizingantibody to transforming growth factor-beta. Lancet,1992, 339: 87.
194. Simpson,.:r. W., Mackler, B. F., O'Neill, P., and Mail-man, M. L. ldentification of collagenase in culturedblood mononuclear cells.]. Dent. Res., 1980,59: 2-10.
lQ5. Postleth\vaite, A. E., Lacfiman, L., Mainardi, C. L.,and Kang, A. H. lnterleukin 1 stimulation of colla-genase production byculmred fibroblasts. J. Exp.Med., 1983, 157: 801..a06.
106. Duncan, M. R, and Berman, B. Gamma-interferon isthe Iymphokine and beta interferon the monokineresponsible for inhibition of fibroblast collagen pro-duction and late but not early fibroblast proliferation.J. Exp. Med., 1985, 162: 516-527.
107. Krane, S. M., Heberden oration 1980: Aspects of cellbiology of the rheumatoid synovial lesiono Ann.RheuIfi. Dis., 1981, ~: 433-448.
108. Dayer, J. M., Stephenson, M. L., Schmidt, E., and
la g en Syn thesisar.ound~m p lanted Ivalon Sp on g es.in,
rats. P.last.Reconstr..Su~~ 197.~;58: 601-607,.
68. Kazeem, &.A: The Im~unQI~~aspects of~~lold
tumQr fQrmauQn. J...Surg!O~cQI., 1988, 38: ~&l.8.
69. La:ur.entaci, G., andD~gu~;~: H:4 antig:eQs~n
keloldsand hypertrophlc scars. &ch. Dermatof., 1.977,
1.13: 1726.
70. Cohen, 1. K;, McCoy,. B. l., MQhanakumar, T., and
Diegelmann,. R. F. Immunoglob\1Íin.éomplem~t,~d
histocompatibilityantigen studies in keloid patients.
Plast. Reconstr. Surg..,1979, 63: 689-695.
11. Kischer, C. W., Shetlar¡; M. R., Shetlar, C. L., ~d
Chva p il, M. .JmmuniW.lobulins in h yp ertro p hic ~s.-"'.
and kelolds. Plast. Reconstr. Surg., 1983, 71: 821~...
72. Bloch, E, F., Hall,M. G., lr., Denson, M. l., and
Sla>:,-Solomon,V. Gene~i~mune reacti~ty in kel()i~
pauents. PlasL Reconstr, ~urg., 1984, 73. 448451,
73.. Oluwasanmi, J., O.. Keloi~ in Ibadan. Trop. G~.
Med., 1974, 26. 231-241-
74. limbow,. K, Koba~hi,H., .Jshii, M.o and otherscSCat
and keloidlike lesionsin progeria. An electrprj;.f11i-
croscopicand immunohistochemical study. Arch. Der-
matol., 1988, 124: 1261-1.266.
75. Hazrau, E., and Hoomand, A The keloida\.di~tbesis,
a resistantstateto maligpancies? Plast. Reconstr.~..,
1977,59: 555-559.
76. Mukheljee, A" Mukherjee, A, ~d Saha, K C. Delayed
type hypersensitiVity reactionto cutaneous anugen
in .keloid. Indi~nJ. Dermatol:, 1982, 27: 12r;:::1~.
77. Smlth, C. J., Smltb, J. C.. and Fmn, M. C. Thep<?~ple
Tole of mast cells (allergy) in the production ofkelqid
and hypertrophic scarring. J. Buro Care Reha:bil.,
1987,8: 126-131.78. Craig, S. S., Deblois, G., and Sch~rtz, L. B. Mast
cells in human keloid, small intesti~e, -,;¡ndJung by
an immunoperoxidase technique using a wüPne
monoclonal antibody against u-yptase. An1,J.'Pathol.,-1986, 124: 427-435. '
79. Sch,..artz, L.B., Riedel, C., Caulfield, l. P., andotherS.
Cell association of co~plexes of chymas~, hepann
proteoglycan, and protem after degranulatlon by rat
mast cells. J. lmmunol., 1981, 126: 2071-2078.
80. Buffoni, F., and RaimQndi, L. A lysyl oxidase ,..ith
histaminase actiVity in the pig aorta. Agents Actions,
1981,1.1: 38-41.
81. Nimni, M. E. Collagen: structure, function, and me-
tabolism in normal and fibrotic tissues. gemiD. &-
thritis Rheum., 1.983, 13: 1-86.
82. Shetlar, M. R, Shetlar, C. L.., Hedricks, L., and Kischer,
C. W. The use of atbymic nude mice for thestudy
of human keloids. Proc. Soco Exp. Biol. Med., 1.985,
179: 549-552. ...83. Kischer, C. W., Pindur, J., Shetlar, M. R., ~dShetlar,
C, L. Implants oí hypertrophic scars andi,ke.l9idsin
to fue nude (athymic) mouse: viability and mórphol-
ogy. T. Trauma, 1989, 29: 672-677.
84. ChytiTova,H. Kulhanek, V., and Horn, V. Experimental
production oí keloids after immunization with auto1-
ogous skin. Acta Chir. Plast., 1959, 1: 72-78.
85. Osman, A. A. A, Gunma, K A" and~tir, A. A.
Highlights on the etiplogy of keloids. Int. Sqrg. 1978,
63: 33-37.86. Yagi, K l., Dafalla, A. A., and Osman, A A. Does
an immune reaction to sebum in wounds cause keloid
scars? Beneficia\. effect of desensitization. Br. l. Plast.
Surg.; 1979, 32: 223-225.
87. De Limpens, J., and Cormane, R. H. Kel.oids and
hypertrophic scars: immunol.ogical aspects.Aesthetic
Plast. Surg., 1982, 6: 149-152.
88. Asghar, S.S., Ali-Bri.ggs, E. F., ~ei!ller, G., andyorm-
ane, R. H. lnteractlon of psonasls scale nort~lstone
proteins ,\'ith fue antibodies eluted from 1)'II1phocytes

Placik aI1d LeWis: IMMUNOLOGIC ASSOCIA110NSOF:KEWIDS 193
1'16. Pinsky, L., Finkelberg, R., Straisfeld, C., and others.Testosterone metabolism by serially subcultured fi-broblasts from genital and nongenital skin of indi-Vidual human donors. Biochem.Biophys. Res. Com-mM.., 1972, 46: 364-369. '
117. day,. R. E., Buckingham, R. B., Prince, R. K, and, others. Collagen types s~thesized in dermal fibroblastcultures from patients with early progressive systemicsclerosis. Arthritis Rheum., 1980, 23: 190-196.
118.~rl-abee, W. F., Jr., Bolen, l. W., and Sutton, D.Myofibroblasts in head and neck surgery. An exper-ime1}tal and clinical study. Arch. Otolaryngol. HeadNeck Surg., 1986, 114: 982-986.
119. Matsuoka, L. Y., Uitto, J., Wortsman, l., and others.Ultrastructure characteristics of keloid fibroblasts. Am.
J. Dermatopathol., 1988, 10: 505-508.120. Keyser, A. J., Cooper, S. M., Ruoslahti, E., and others.
Scleroderma: enhancement of connective tissue bia-SYJ1thesis by a circulating factor.. Fed. Proc., 1979,38: 1339.
1.21.. ~ser, A. J., Cooper, S. M., and Nimni, M. E. TheTole of circulating factor in the pathogenesis of scle-rodenna. Fed. Proc., 1980, 39: 874.
122. Hosokawa, M., Ishii, M., Inque, K, and others. Es-trogen induces different responses in dermal and lungfibroblasts: special reference to collagen. Connect. Tis-sue Res., 1981, 9: 115-120.
123. Gamer, W. L. Soveim, K, Smith, D., and others. Al-tered cytokine response of hypertrophic scar fibro-blasts. Presented at the 37th Annual Meeting of thePlastic Surgery Research Council. Apri11992, Toronto,Ontario.
otbers. Purification of a lactar from human blood~onocyte-macrophageswhichsum~lates the produc-tlonofcollagenasean? pros~~lan~m E2 by cells cul-tured from rheumatold synoVlal ussues. F. E. B. S.Lett., 1981, 124: 25~256.
109. J!m~n~~, S.A.,Freundlic.h,~.,Rosenblo~~,J.Selec~,!emhlbluon of humandlplold fibroblast.coll~en ~tbesis byinterferons.J. Clin. lnvest., 1984;74:1112-
11)6.110. Thompson, J., and Crumley, R. Facwl plastic ne~.s:research advances. Arch. Otol~gol. Head NeckSurg., 1990, 116: 768-769.
.111. Larrabee, W. F., Jr., East, C. A., Jaffee, H. S., andotbe!s. lntralesional int~rfér9n~amma treatmen~:Qfkelolds and hypertrophic Scar$. Arch. Otola~gol.Head Neck Surg.., 1990,116(10): )159-1162,
112. Granstein, R. D., Rook, A" Flotte.,T. J..,~<JÓ~érs.A controlled tríal of inttalesionalrecombittant intér..feron~ma in tbe treatment of keloidál s<~k.Clinical and Histologic Findings. Arch. Dermatm.,1990,126(10): 1295-1302.
113, Berman, B., and Duncan, M. R. Short-term keloidtreatment in ,oivo witb human interferon~a-2b: Re-sults. in a selective and persistent ~~iz4~on ofkeloldal fibroblast c.olla~en, .glyco~mog'Yca!), andcollagenase producuon In VltrO.. J. ~¡A~d. Der-matol., 1989, 21(4): 694-702.
114. Duncan, J. l., Thomason, A.W., ~nd M~, l. F. KTopical Cj'closporin and T l~ph~si9 keloid scars.Br.J. permatol., 1991, 124. 109-114.
115. Martin, G. M., Sprague, C. A.,~orW90d, T. ¡.{.~andPendergass, W. R. Clonal selecuol..1,attenuatiOn~nddifferentiation in an in vitro model of hyperplasia.Am. J. Pathol., 1974, 74: 137-150.