circulatorysystems ananimal’spersonal“ocean…circulatorysystems ananimal’spersonal“ocean...
TRANSCRIPT

Circulatory systems an animal’s personal “ocean”
•Water flows over single-‐celled creatures…
hydra sponge Mul6cellular algae
•Delivers dissolved gases (O2,CO2) and nutrients, washes away waste.
A system of vessels and pump is needed to push fluid around, and bathe all cells: this is the circulatory system, which func6ons to deliver gases and nutrients to all 6ssues
Ever hear the ocean in a seashell?
Bacterium protozoan
single-‐cell algae
•Insufficient for organisms of considerable size or complexity.
and through small, simple organisms…

Increasingly Complex Circulatory Systems with increasingly complex animals
“Open” circulatory system: blood and 8ssue fluid is con8nuous – Arthropods
• insects • arachnids (spiders, scorpions) • myriapods (millipedes, cen5pedes) • crustaceans (crabs, lobsters, crayfish, shrimp)
– molluscs (clams, snails, octopus, squid)
“Closed” circulatory system: blood and 8ssue fluid are separate – Fish, sharks, rays – Amphibians, rep6les, birds, mammals

“Open” circulatory system of insects Anterior
Posterior
Heart Aorta
Valve-‐like openings
4 3
2 1
Fluid (“haemolymph”) flows out through the open end at the anterior and bathes the body.
It re-‐enters through openings of the elongated heart in the distal porNon of the body.
SequenNal peristalic contracNons close each “valve” and force fluid towards the anterior.
This corresponds to their open respiraNon system. Their “blood” pulls nutrients through the body. This is inefficient and imposes a
size limita8on.
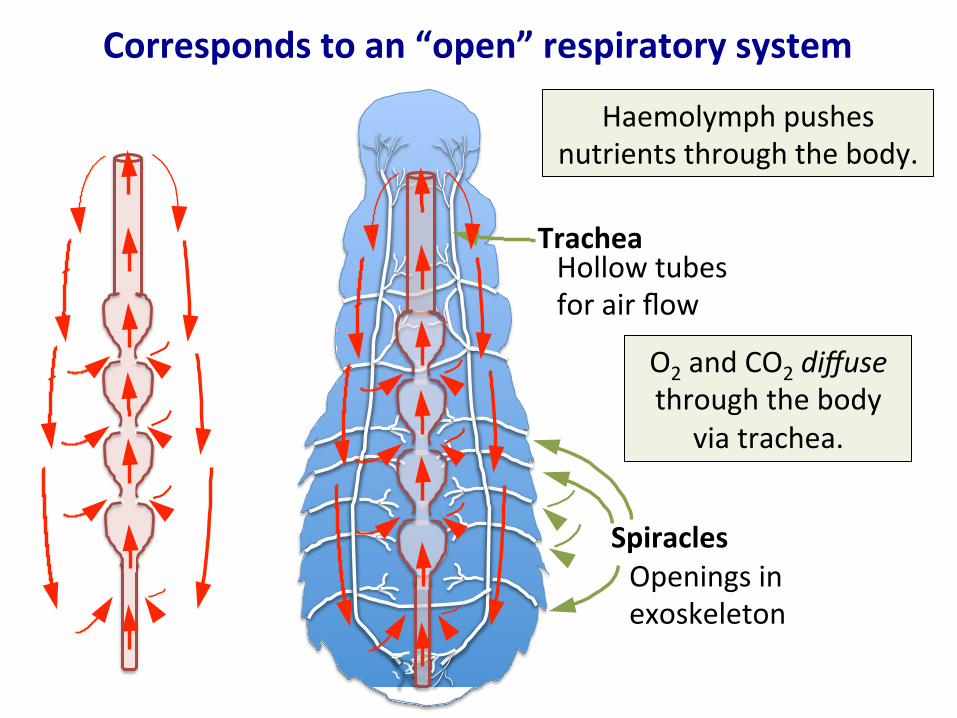
Corresponds to an “open” respiratory system
Spiracles
Trachea Hollow tubes for air flow
Openings in exoskeleton
Haemolymph pushes nutrients through the body.
O2 and CO2 diffuse through the body
via trachea.
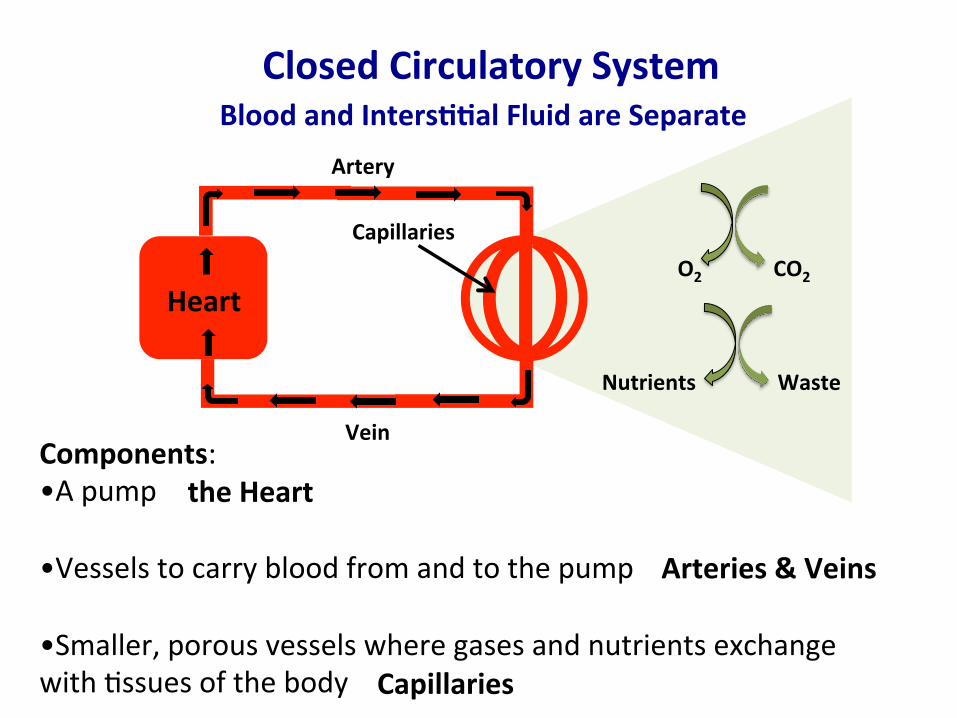
Closed Circulatory System Blood and Inters66al Fluid are Separate
Components: •A pump •Vessels to carry blood from and to the pump •Smaller, porous vessels where gases and nutrients exchange with Nssues of the body
Pump O2 CO2
Nutrients Waste
the Heart
Arteries & Veins
Capillaries
Vein
Artery
Heart
Capillaries
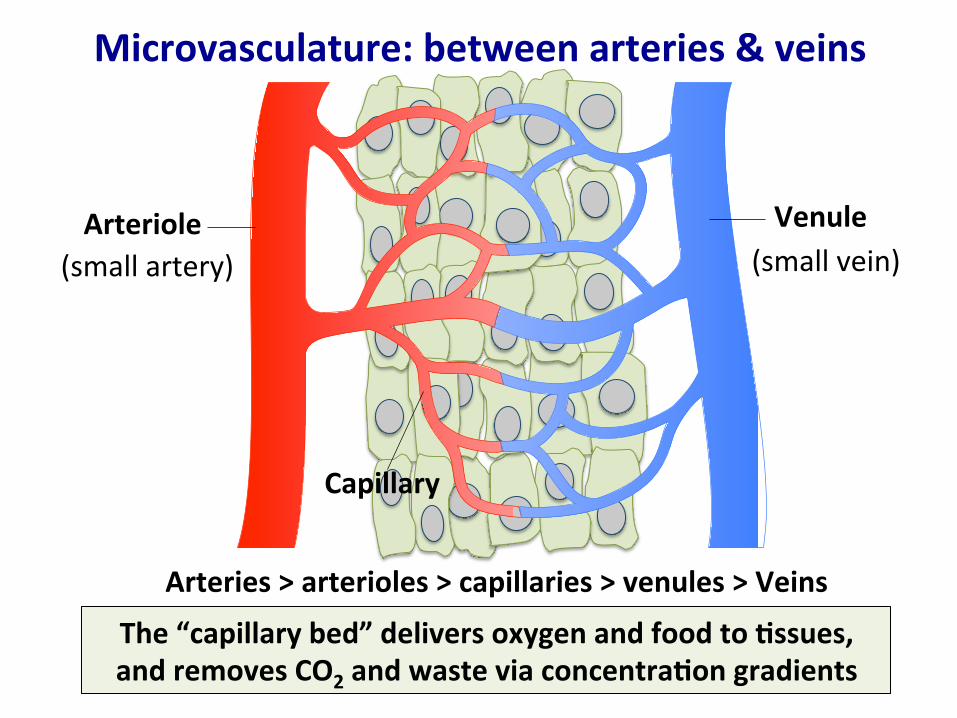
Microvasculature: between arteries & veins
Arteriole Venule
Capillary
Arteries > arterioles > capillaries > venules > Veins
The “capillary bed” delivers oxygen and food to 6ssues, and removes CO2 and waste via concentra6on gradients
(small artery) (small vein)
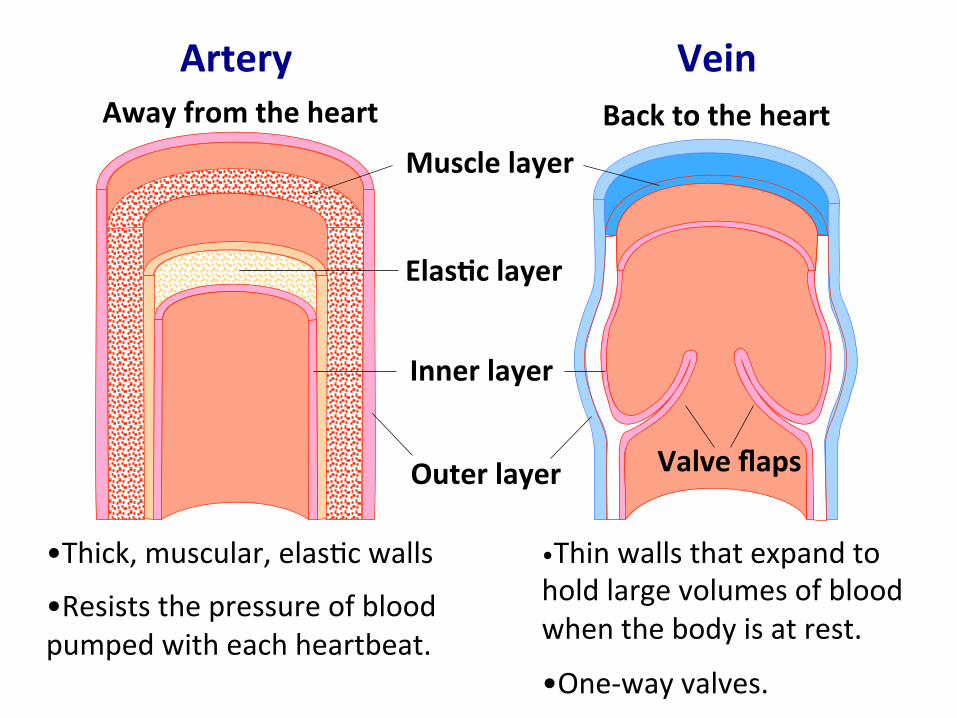
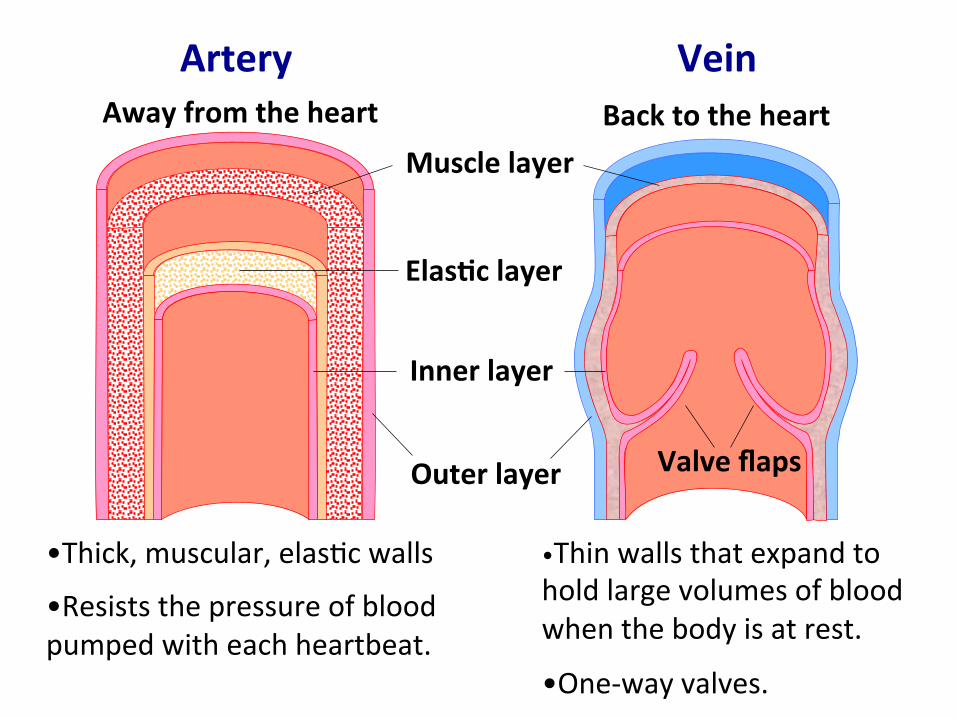
Artery Vein
•Thin walls that expand to hold large volumes of blood when the body is at rest.
•One-‐way valves.
Valve flaps
Muscle layer
Elas6c layer
Inner layer
•Thick, muscular, elasNc walls
•Resists the pressure of blood pumped with each heartbeat.
Outer layer
Away from the heart Back to the heart

Gaps between cells allow substances to pass through Fenestrated
Capillaries
Their walls are only one cell thick
Side view Front view
Con6nuous Cells are Nghtly connected, restricNng flow in and out

A problem with closed circulatory systems •Blood pressure (“pump force”) dissipates as blood flows through capillaries, which creates a problem…
Heart Gills Body
Capillaries
•When blood goes through the capillaries of gills/lungs first, there is only sluggish delivery of O2-‐rich blood to body.
•If blood instead goes to body Nssues first, there is only sluggish delivery of O2-‐poor blood back to gills/lungs.
•Both gills/lungs AND body Nssues must have capillary beds, which results in a further loss of pressure.
Strong pressure
Sluggish
Even more sluggish
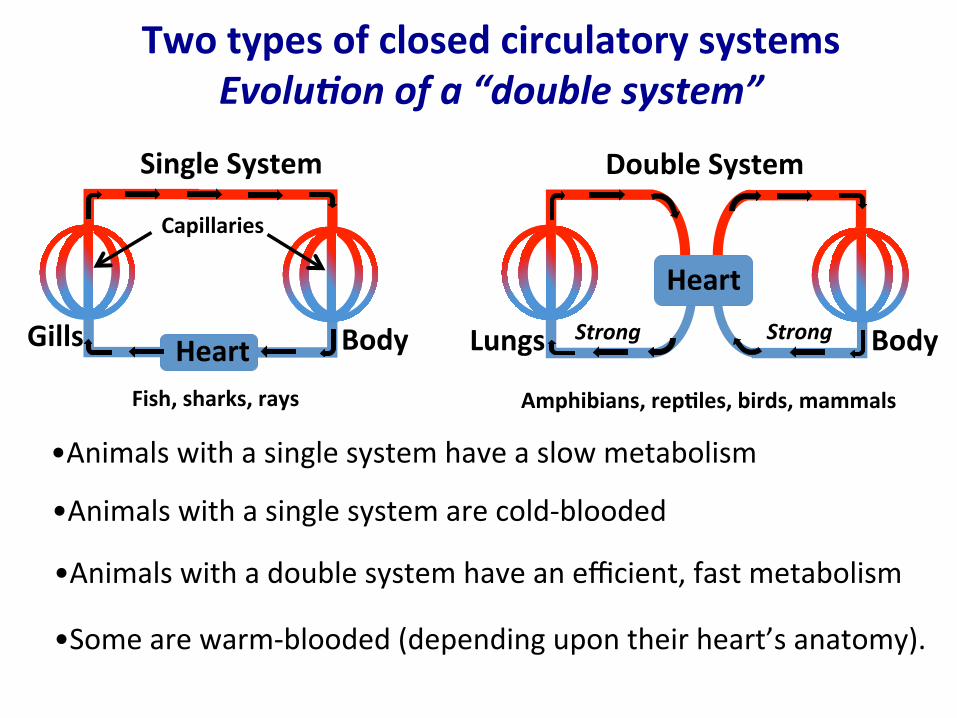
Two types of closed circulatory systems Evolu8on of a “double system”
Single System
Heart Gills Body
Capillaries
Double System
Lungs Body
Heart
Fish, sharks, rays Amphibians, rep6les, birds, mammals
•Animals with a single system have a slow metabolism
•Animals with a double system have an efficient, fast metabolism
•Some are warm-‐blooded (depending upon their heart’s anatomy).
•Animals with a single system are cold-‐blooded
Strong Strong

Hearts are not all created equal Fish have a 2-‐chambered heart
Liver
Kidney Gills
Heart
Atrium
Ventricle
• Blood enters the atrium. • As the heart relaxes, the blood passes through a valve into the
thick-‐walled, muscular ventricle. • Ventricle contracts, pumps blood to gill capillaries (gas exchange). • O2-‐rich blood flows to the capillary networks of the body. • Blood returns to the atrium. • Not efficient, poor pressure a^er gill capillaries.
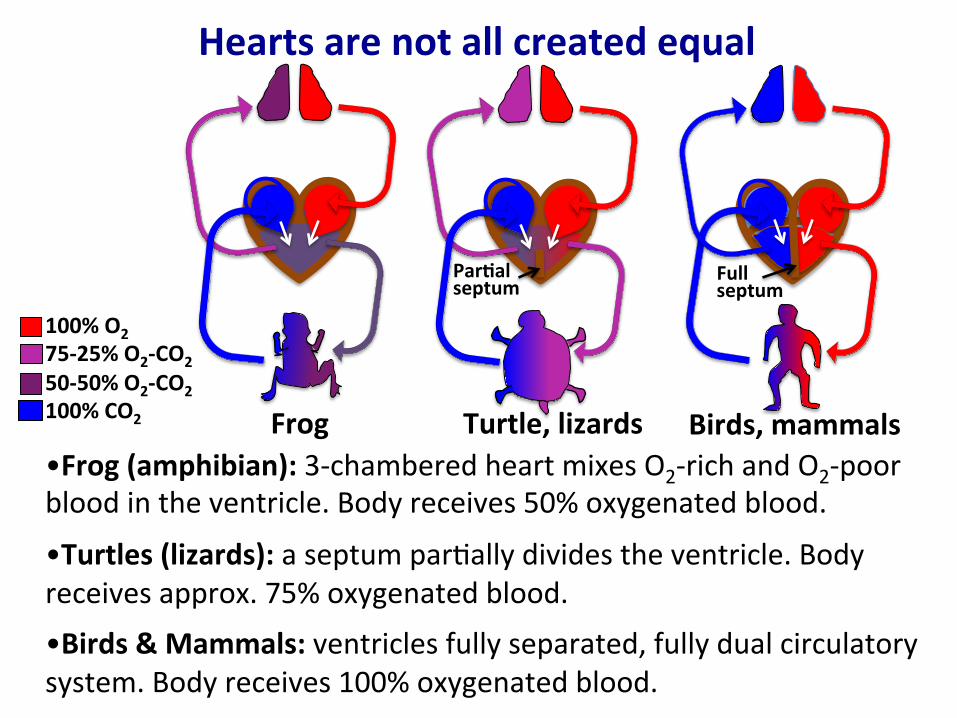
Hearts are not all created equal
•Frog (amphibian): 3-‐chambered heart mixes O2-‐rich and O2-‐poor blood in the ventricle. Body receives 50% oxygenated blood.
•Turtles (lizards): a septum parNally divides the ventricle. Body receives approx. 75% oxygenated blood.
•Birds & Mammals: ventricles fully separated, fully dual circulatory system. Body receives 100% oxygenated blood.
100% O2 75-‐25% O2-‐CO2 50-‐50% O2-‐CO2 100% CO2
Par6al septum
Turtle, lizards Frog Birds, mammals
Full septum
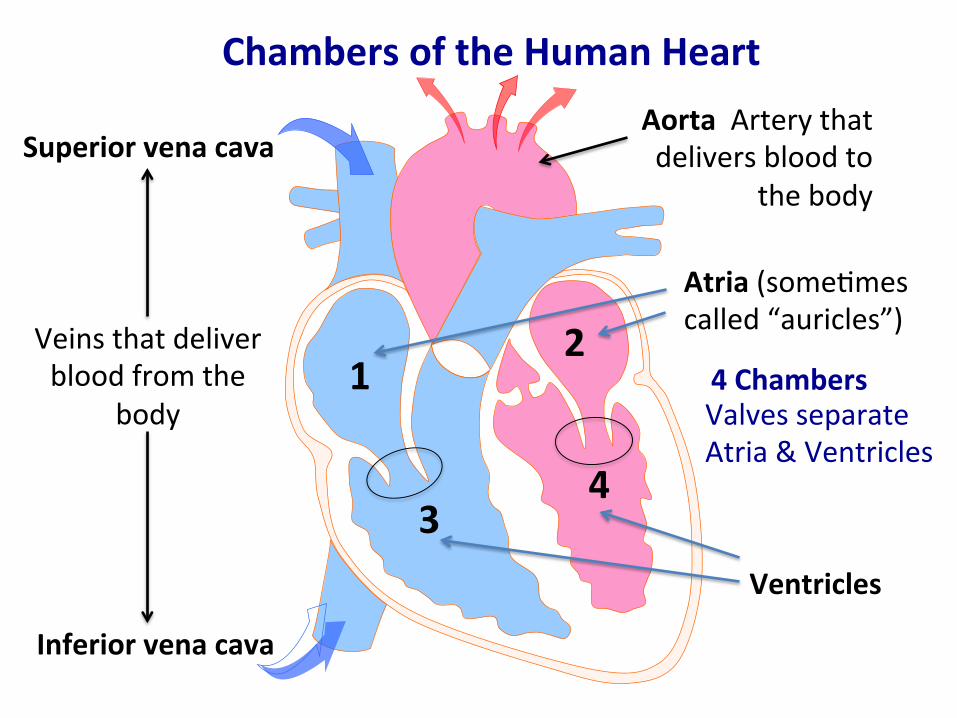
Chambers of the Human Heart
Atria (someNmes called “auricles”)
Ventricles
Superior vena cava
Veins that deliver blood from the
body
Inferior vena cava
Aorta Artery that delivers blood to
the body
Valves separate Atria & Ventricles
1 2
3 4
4 Chambers

Blood flow through the human heart Deoxygenated blood
(from the upper body)
Superior vena cava
Inferior vena cava
Oxygenated blood (to the upper body)
Aorta
Pulmonary veins (from the lungs)
Pulmonary artery (to the lungs)
Aorta
Pulmonary veins (from the lungs)
Pulmonary artery (to the lungs)
Oxygenated blood (to the lower body)
Deoxygenated blood (from the lower body)

Heart valves maintain a one-‐way flow
Low pressure
Valve leaflet (flap)
High pressure
High pressure
Valve leaflet
Low pressure
Open heart valve •Heart chamber contracts. •Blood pressure pushes open the valve leaflets •Blood flows through to the other side of the valve.
Closed heart valve •Blood pressure on the other side of the valve rises •Forces the valve leaflets back. •Closed valve prevents backflow.

The heart cycle - Diastole
Movement of blood Blood enters the atria
Electrical activity
Deoxygenated blood from upper body
Oxygenated blood from
right lung
Oxygenated blood from left lung
Superior vena cava
Full left atrium
Full right atrium
Deoxygenated blood from lower body
Electrical pulse
Sinoatrial node
•Heart muscle cells signal each other to coordinate contraction: the sinoatrial node is the pacemaker.
•The RATE (not strength) can be changed by nervous system input

The heart cycle – Atrial systole
Movement of blood
Electrical activity
Electrical pulse
Atrioventricular node
Full right ventricle
Open valve
Contracted right atrium
Open valve
Full left ventricle
Contracted left atrium
Contraction of atria pushes blood to ventricles

The heart cycle – Ventricular systole
Movement of blood
Electrical activity
Electrical pulse
Aorta Oxygenated blood flows to upper and lower body
Closed valve
Closed valve
Contracted ventricles
Open valve
Pulmonary artery
Open valve
Deoxygenated blood flows to
the lungs
Contraction of ventricles pushes blood out of heart
Simultaneous delivery of blood to
body and lungs
Artery Vein
•Thin walls that expand to hold large volumes of blood when the body is at rest.
•One-‐way valves.
Valve flaps
Muscle layer
Elas6c layer
Inner layer
•Thick, muscular, elasNc walls
•Resists the pressure of blood pumped with each heartbeat.
Outer layer
Away from the heart Back to the heart
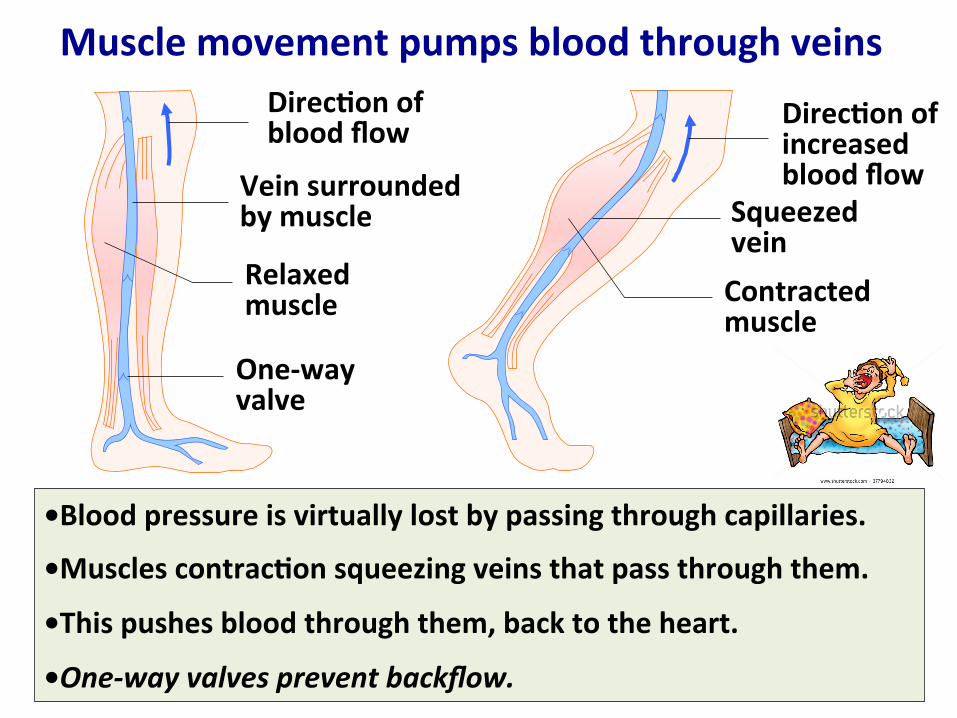
Muscle movement pumps blood through veins
•Blood pressure is virtually lost by passing through capillaries.
•Muscles contrac6on squeezing veins that pass through them.
•This pushes blood through them, back to the heart.
•One-‐way valves prevent backflow.
Direc6on of blood flow
Vein surrounded by muscle
Relaxed muscle
One-‐way valve
Direc6on of increased blood flow
Squeezed vein Contracted muscle

Inhala6on also moves blood through veins
Air inhaled Chest cavity pressure is lowered
Blood drawn toward heart
Diaphragm
•Chest cavity expands during inhala6on. •Pressure in chest is lowered. •Higher pressure in the rest of the body pushes blood in the veins toward the heart.

Circulatory System Gas exchange
To and from other 6ssues
Exhaled air 120 u O2 27 u CO2
Inhaled air 160 u O2 0.3 u CO2
Blood from Lungs 104 u O2 40 u CO2
Lung Alveoli 104 u O2 40 u CO2
Blood entering 6ssues
104 u O2 40 u CO2
Blood leaving 6ssues 40 u O2 45 u CO2
Tissues <40 u O2 >45 u CO2
Blood entering lung
40 u O2 45 u CO2
•Incomplete exchange in lungs •Total lung volume is 6 liters •Only 0.5 liters exchanges with a normal breath (heavy breath more) •1.5 liters “residual volume”

Erythrocytes: Red Blood Cells •Generated throughout life from stem cells
Stem Cell Commieed Differen6a6on Nuclear Ejec6on Erythrocyte
Ribosome synthesis Hemoglobin accumula8on
•Essen6ally a bag of hemoglobin (250 million molecules/cell) •Jejson their nucleus
•3-‐5 days to differen6ate
•Last about 120 days
Immune system cells and thrombocytes (for forma6on of clots)
•insect hemolymph does not contain hemoglobin or red blood cells •Snails and slugs creatures have haemocyanin (Cu++-‐containing protein that binds O2) •Some snails have hemoglobin

Hemoglobin: a metaloprotein
Heme (iron-‐containing
group)
Pep6de A complex of four pep6des
4O2 binding sites
High affinity for O2 increases amount of O2 in blood by 7-‐fold more than the amount that can dissolve in blood
O2 from lungs
O2 to 6ssues
Blood cell with
“loaded” hemoglobin in circula6on

•Hemoglobin also binds CO2. •Occurs at Nssues and lungs depending upon relaNve levels. •CO2 binds to the protein, not heme; RBC can carry both O2 and CO2 •Needn’t rely on diffusion of CO2 through plasma, which is weak.
Removal of CO2 from 6ssues
Low O2, high CO2 environment
• CO2 dissolved in water forms Bicarbonate and hydrogen ions: CO2 + H2O -‐> HCO3
-‐ + H+ •Most CO2 in plasma of blood undergoes this reacNon. •H+ would lower blood pH, but binds to hemoglobin. •HCO3
-‐ is a buffer for blood: maintains blood pH at approx 7.4. •HCO3
-‐ will bind H+ generated during metabolism to yield H2CO3

More on control of blood pH •CO2 dissolved in plasma forms CO2 + H2O -‐> HCO3
-‐ + H+
•Hemoglobin binds and sequesters H+. The “free” HCO3-‐ can
then bind H+ generated during metabolism to yield H2CO3
•Hemoglobin, H2O and CO2 are essenNally in unlimited supply
•Allows the above reacNon to provide excellent pH control. Under stress: •Increased breathing will eliminates more CO2, which will push the above reacNon to the le^, and elevate blood pH.
•Increased acNvity of the kidneys will eliminate HCO3-‐, which will
push the reacNon to the right, and lower blood pH.

O2 and CO2 exchange: lungs, blood, tissues
Tissue
O2-rich blood lungs > heart > tissues
O2-poor blood tissues > heart >lungs
Capillary
Carbon dioxide diffuses from tissues into plasma,
binds to hemoglobin. Oxygen diffuses from red
blood cells into tissues
Bronchiole Alveolar air space Alveolar wall
Carbon dioxide ( ) diffuses from red blood cells > plasma > alveoli.
Red blood cell
Oxygen ( ) diffuses across the alveolar wall > plasma (fluid of blood) > red blood cells, binds to hemoglobin
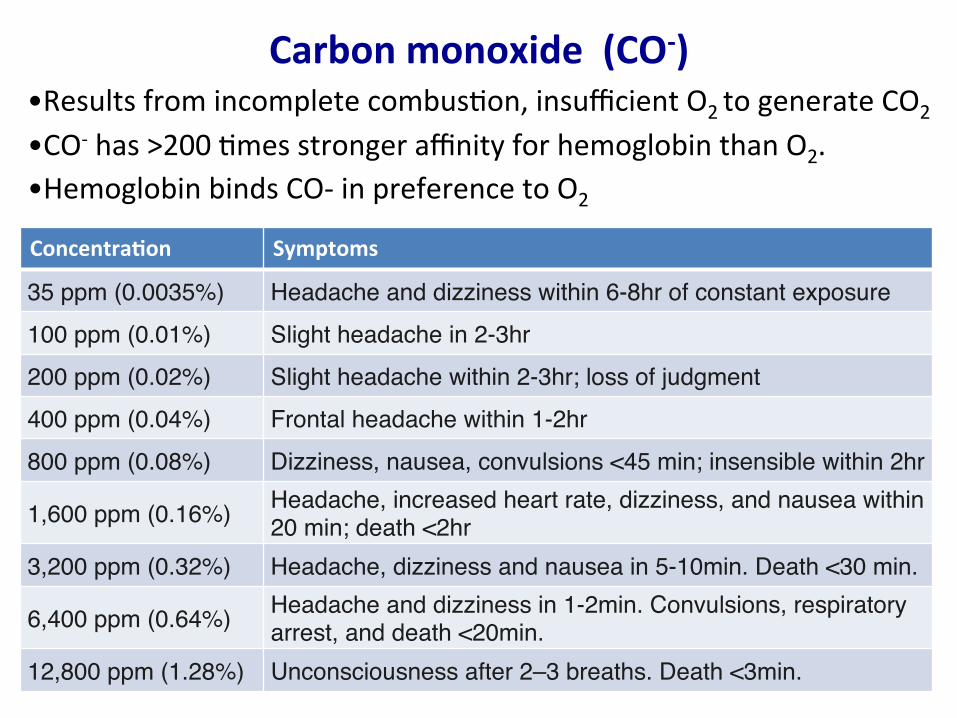
Carbon monoxide (CO-‐)
•Hemoglobin binds CO-‐ in preference to O2
•Results from incomplete combusNon, insufficient O2 to generate CO2
•CO-‐ has >200 Nmes stronger affinity for hemoglobin than O2.
Concentra6on Symptoms
35 ppm (0.0035%) Headache and dizziness within 6-8hr of constant exposure100 ppm (0.01%) Slight headache in 2-3hr200 ppm (0.02%) Slight headache within 2-3hr; loss of judgment400 ppm (0.04%) Frontal headache within 1-2hr800 ppm (0.08%) Dizziness, nausea, convulsions <45 min; insensible within 2hr
1,600 ppm (0.16%) Headache, increased heart rate, dizziness, and nausea within 20 min; death <2hr
3,200 ppm (0.32%) Headache, dizziness and nausea in 5-10min. Death <30 min.
6,400 ppm (0.64%) Headache and dizziness in 1-2min. Convulsions, respiratory arrest, and death <20min.
12,800 ppm (1.28%) Unconsciousness after 2–3 breaths. Death <3min.
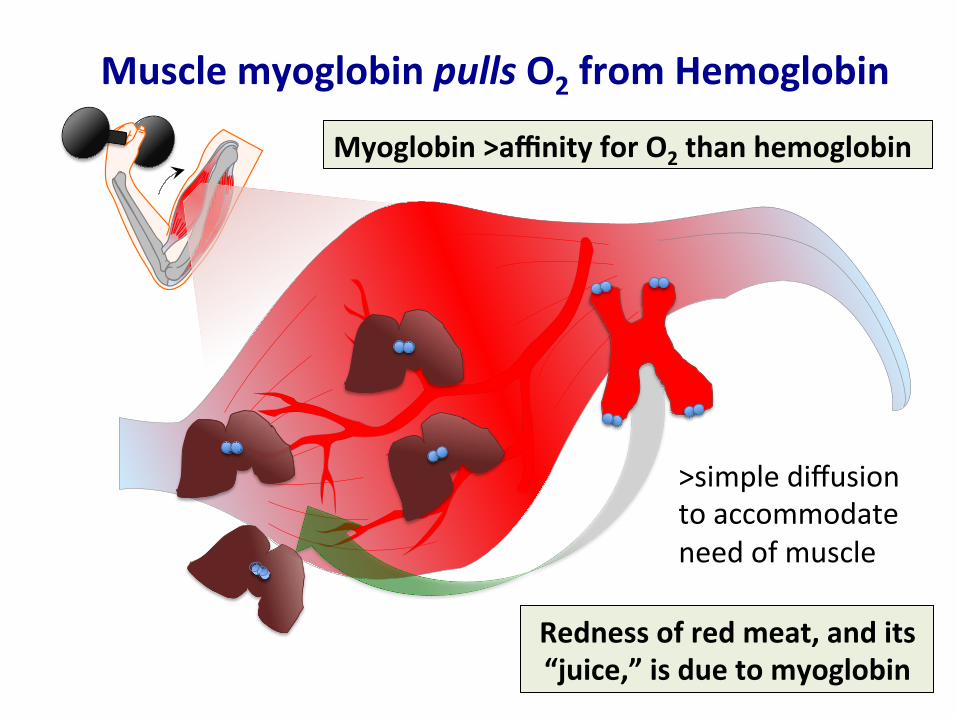
Muscle myoglobin pulls O2 from Hemoglobin
Myoglobin >affinity for O2 than hemoglobin
Redness of red meat, and its “juice,” is due to myoglobin
>simple diffusion to accommodate need of muscle
Composi6on of Blood
• Plasma (water and dissolved salts, proteins)
• RBCs (3-‐6 million for average human)
• Platelets (“thrombocytes,”which help with clolng; 400,000-‐500,000 for average human)
• “White” blood cells (“leukocytes,” 4,000-‐11,000 for average human) – anNbody-‐producing cells (and their secreted anNbodies) – Macrophages (“big eaters”) that engulf foreign parNcles – Natural-‐killer cells
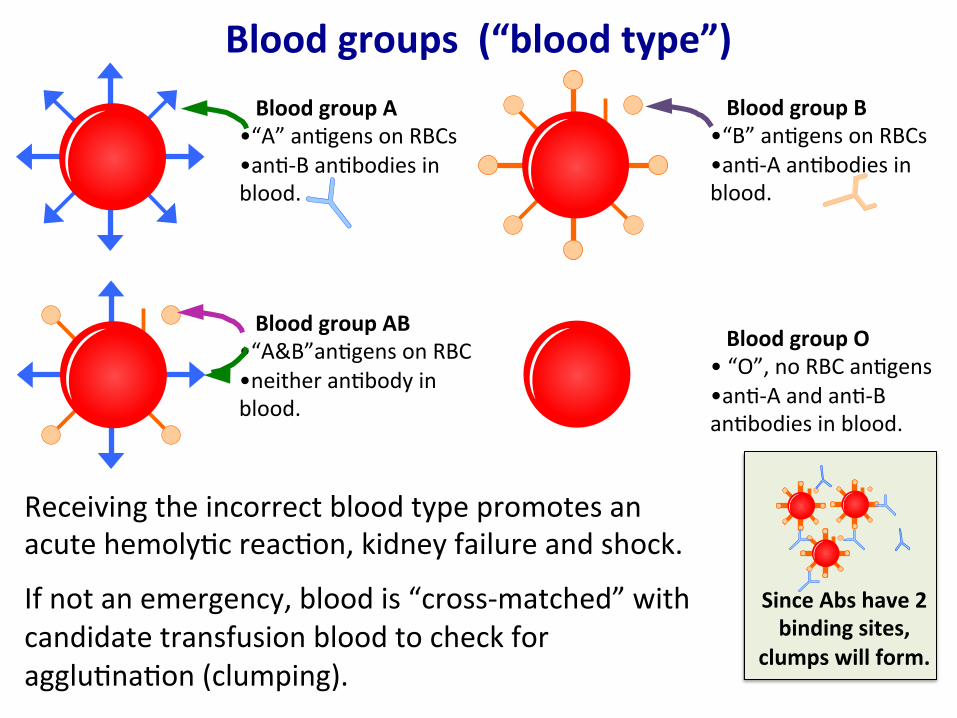
Blood groups (“blood type”) Blood group A •“A” anNgens on RBCs •anN-‐B anNbodies in blood.
Blood group AB •“A&B”anNgens on RBC •neither anNbody in blood.
Blood group B •“B” anNgens on RBCs •anN-‐A anNbodies in blood.
Blood group O • “O”, no RBC anNgens •anN-‐A and anN-‐B anNbodies in blood.
Receiving the incorrect blood type promotes an acute hemolyNc reacNon, kidney failure and shock.
If not an emergency, blood is “cross-‐matched” with candidate transfusion blood to check for aggluNnaNon (clumping).
Since Abs have 2 binding sites,
clumps will form.

Blood type: Rh+ or Rh-‐ •Rh+ means “D anNgen” present on RBCs, Rh-‐ means absent.
•Fetus can have different blood type than the mother.
•Not a problem, BUT mother Rh-‐ and fetus Rh+, mother may form anNbodies against Rh+ during delivery.
•Maternal anNbodies cross placenta, protects fetus from infecNons.
•Once mother encounters fetal blood, forms anNbodies against the Rh+ “D anNgen.”
•Maternal anN-‐RH+ anNbodies can anack and destroy fetal RBCs. Can cause mild-‐severe fetal low blood count, can be lethal.
•TesNng and immunosuppression if appropriate.
•An Rh-‐ individual cannot receive a transfusion of RH+ blood, although, an Rh+ individual can receive RH-‐ blood. (similar to type O being acceptable for individuals who are type A, B or AB)
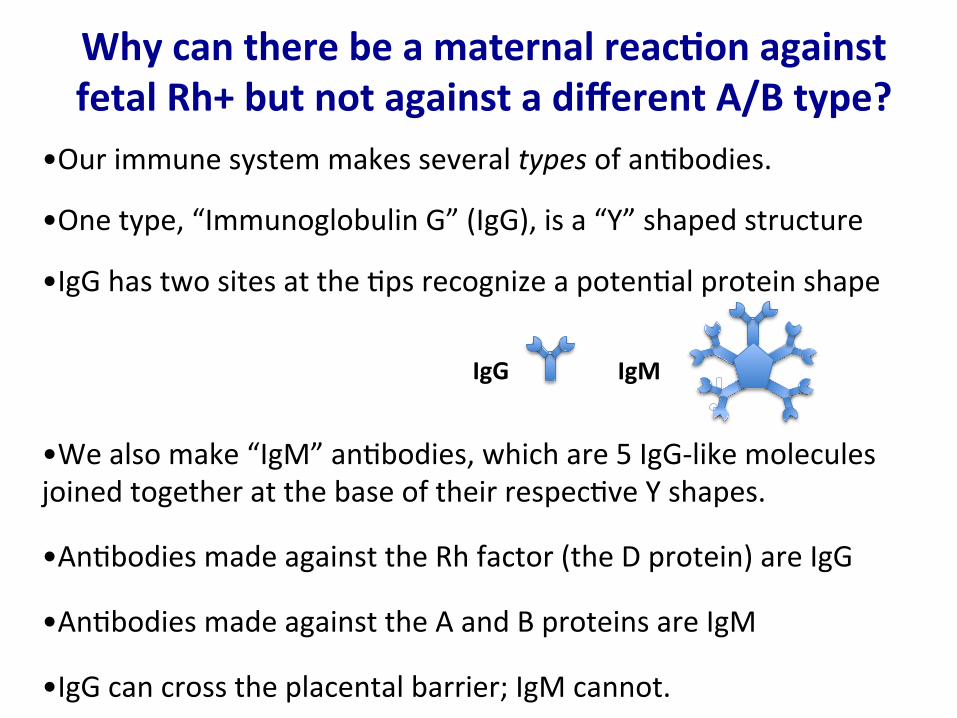
Why can there be a maternal reac6on against fetal Rh+ but not against a different A/B type?
•Our immune system makes several types of anNbodies.
•One type, “Immunoglobulin G” (IgG), is a “Y” shaped structure
•IgG has two sites at the Nps recognize a potenNal protein shape
•We also make “IgM” anNbodies, which are 5 IgG-‐like molecules joined together at the base of their respecNve Y shapes.
•AnNbodies made against the Rh factor (the D protein) are IgG
•AnNbodies made against the A and B proteins are IgM
•IgG can cross the placental barrier; IgM cannot.
IgG
IgG IgM

Lympha6c system
Lympha6c vessels
Lymph nodes
Thymus
Spleen •Fluid within the lymphaNc system is called lymph.
•Fluid in the circulatory system is plasma.
•inters88al fluid is among Nssues
•Recall open circulatory system of arthropods: “haemolymph” is a combinaNon of blood and lymph
Inters66al fluid drains into the lympha6c system, where it is filtered and eventually drains into veins
Lymph nodes
“Close-‐up” image

•Important for proper funcNoning of the immune system
•Major locaNon of immune system cells
•Filters foreign parNcles and cancer cells.
•Become inflamed or enlarged in various infecNons and diseases ranging from minor throat infecNons to cancer.
Outgoing Lymph vessel
Incoming Lymph vessel
Cortex
Paracortex (mostly T cells)
Medulla (macrophages and plasma cells)
Follicle
Germinal center (mostly B cells)
B cells synthesize an6bodies T cells regulate the immune system
Lymph node
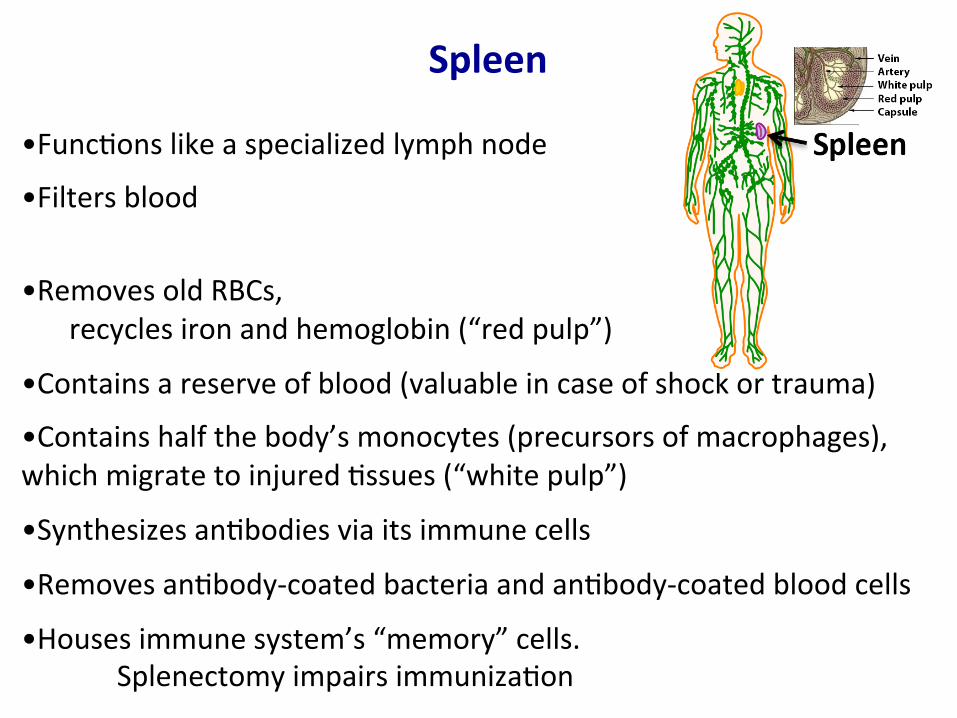
Spleen
•FuncNons like a specialized lymph node
•Filters blood
•Removes old RBCs, recycles iron and hemoglobin (“red pulp”)
•Contains a reserve of blood (valuable in case of shock or trauma)
•Contains half the body’s monocytes (precursors of macrophages), which migrate to injured Nssues (“white pulp”)
•Synthesizes anNbodies via its immune cells
•Removes anNbody-‐coated bacteria and anNbody-‐coated blood cells
•Houses immune system’s “memory” cells. Splenectomy impairs immunizaNon
Some Problems, Natural Responses and Interven6ons
• Blood clojng
• Impaired circula6on due to clogging of arteries – Heart anack – Stroke
• Pacemaker
• Valve disorders and surgical replacement
• Arterial rupture (aneurism)
• Control of blood pressure

Thrombocytes: “platelets” essen8al for blood cloPng
Stem Cell
the same stem cell populaNon
Megakaryoblast Megakaryocyte Platelets
Cytoplasmic extensions are platelet precursors
Cytoplasmic fragments
•Platelets are “ac6vated” following damage to blood vessels •SNck to vessel walls at the injury and clump together •Release chemicals that start the “coagula6on cascade.” •Fibrinogen (dissolved in blood), forms sNcky fibrin strands. •ResulNng tangled mesh traps blood cells, forming a clot.
Erythrocyte
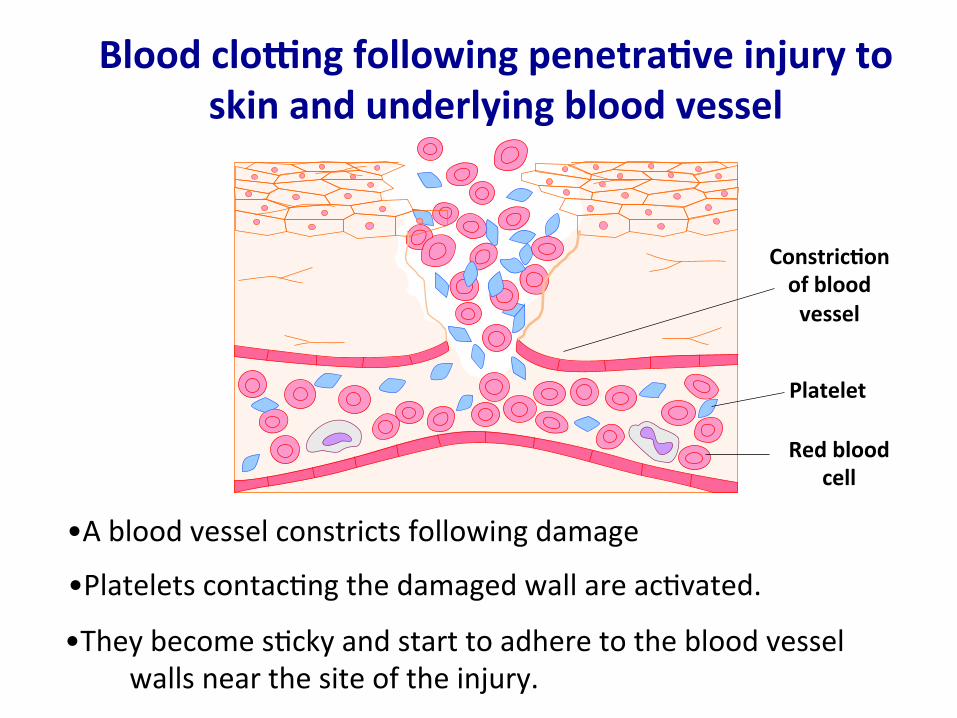
Blood clojng following penetra6ve injury to skin and underlying blood vessel
•A blood vessel constricts following damage
Red blood cell
Platelet
Constric6on of blood vessel
•Platelets contacNng the damaged wall are acNvated.
•They become sNcky and start to adhere to the blood vessel walls near the site of the injury.

Blood clojng following penetra6ve injury to skin and underlying blood vessel
•AcNvated platelets clump together.
Platelets clumped together Released
chemicals
•Damaged Nssue and acNvated platelets release chemicals that start a “coagulaNon cascade”
•A series of clolng factors are acNvated. •Inability to make factor(s) prevents clolng (hemophilia)

Blood clojng following penetra6ve injury to skin and underlying blood vessel
•Fibrinogen, (a protein dissolved in blood), forms fibrin strands.
Endothelial cells will heal vessel wall
Epithelial cells will cover over from edges
•A bruise occurs when a blood vessel is broken but the overlying skin is not. (“hematoma” means “body of blood”)
•SNcky fibrin threads traps blood cells and platelets, forming a clot.

Blood supply to the heart
Le^ main coronary artery
Le^ circumflex artery
Coronary vein
Le^ anterior descending artery
Right main coronary artery
Coronary arteries bring food and oxygen to heart muscle
Coronary vein
The blood pumped through the heart does not “feed” it!

Atherosclerosis
Early atherosclerosis
Muscle layer Fat globule
Faey deposit (“plaque”)
Advanced atherosclerosis Faey deposit
New muscle cell Thickened muscle layer
•Faey substances gradually accumulate in the artery lining. Minor irregulari6es/breakage may be how adherence begins. •The muscle layer thickens as new muscle cells form in the faey deposit. ?Body is trying to bury/repair the wall’s irregularity •The artery becomes progressively narrowed.
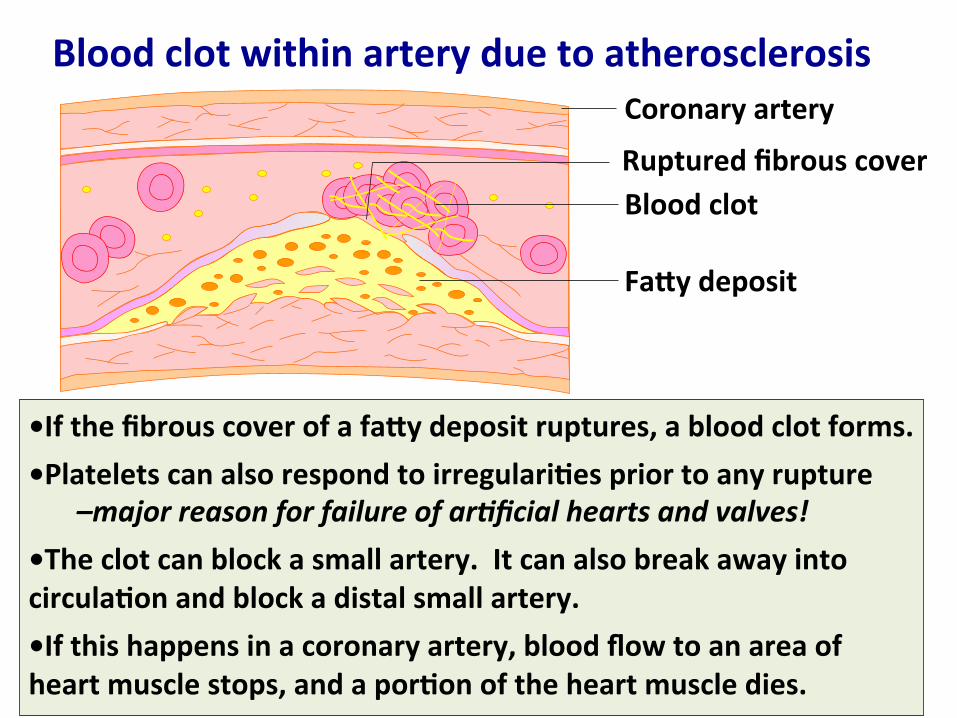
Blood clot within artery due to atherosclerosis
•If the fibrous cover of a faey deposit ruptures, a blood clot forms.
•Platelets can also respond to irregulari6es prior to any rupture –major reason for failure of ar8ficial hearts and valves!
•The clot can block a small artery. It can also break away into circula6on and block a distal small artery.
•If this happens in a coronary artery, blood flow to an area of heart muscle stops, and a por6on of the heart muscle dies.
Coronary artery
Faey deposit
Blood clot Ruptured fibrous cover

When the heart does not receive enough O2…
Symptoms range from shortness of breath, faNgue and dizziness to the following: •Angina: chest pain or discomfort when the heart muscle doesn’t get enough O2-‐rich blood. Can feel like indigesNon.
•Arrhythmia: heart beats too fast, slow, or irregular rhythm. Most harmless, some can be serious or even life-‐threatening.
•Atrial Fibrilla6on: rapid, disorganized electrical signals in the atria, fast, irregular contracNon, blood pools in atria
•Heart Aeack: blood flow to a secNon of heart muscle is blocked. If not restored quickly, that secNon dies.
Stroke or Clauda6on: alterna8ve results of infarc8on depending
upon loca8on of infarct
• Blockage of blood flow in brain can lead to stroke
• ClaudaNon (weakening and/or numbness) can result from infarcNon in legs
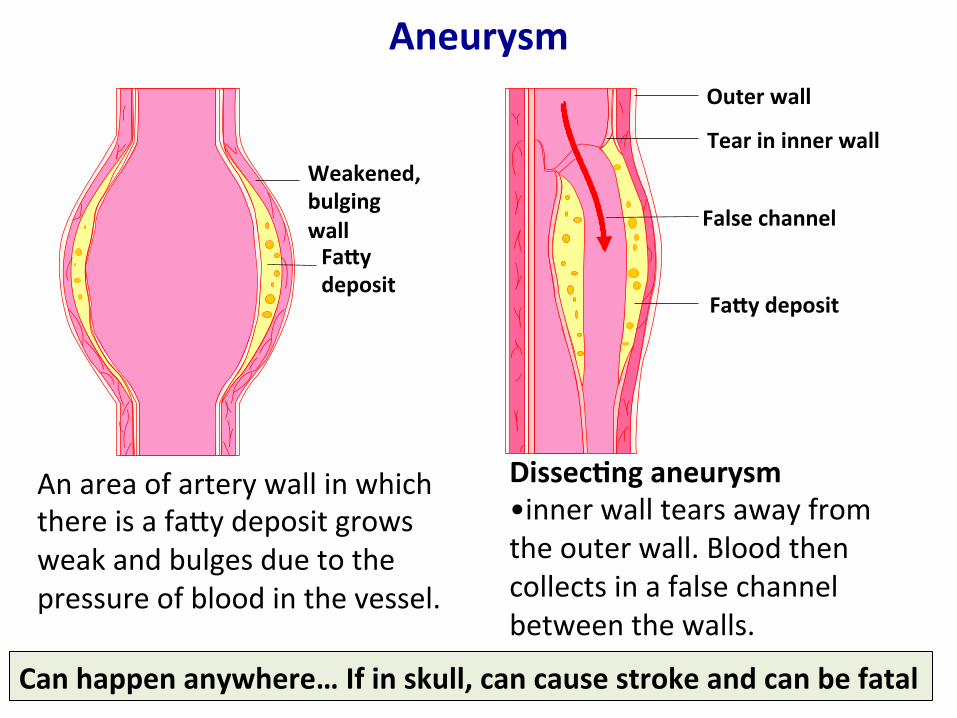
Aneurysm
Weakened, bulging wall Faey deposit
An area of artery wall in which there is a fany deposit grows weak and bulges due to the pressure of blood in the vessel.
Outer wall
Tear in inner wall
False channel
Faey deposit
Dissec6ng aneurysm •inner wall tears away from the outer wall. Blood then collects in a false channel between the walls.
Can happen anywhere… If in skull, can cause stroke and can be fatal

Coronary angiography To monitory coronary artery flow
•The catheter is inserted in the femoral artery, and passed through the aorta to a coronary artery, where a contrast dye is injected.
•The artery and vessels leading from it are visualized by X-‐rays.
•The catheter is reposiNoned to check all the coronary arteries.
Coronary artery
Aorta
Catheter
Aorta Unobstructed flow Obstructed flow

Coronary angioplasty
Catheter
Balloon before infla6on
Faey deposit
A catheter is used to place a balloon within the narrowed area of the coronary artery.
The balloon is inflated and deflated several Nmes to compress the fany deposit.
Narrowed area of artery
Inflated balloon
Compressed faey deposit
Artery is par6ally cleared The catheter is withdrawn.
A small tube (“stent”) may be inserted to keep the artery open.

“Coronary bypass” graXing a vein
Cujng site
Cujng site
Saphenous vein Sec6ons of graqed vein
Aorta
Blockages in the coronary arteries
The saphenous vein is removed and divided into
sec6ons to make several graqs
Each graq is aeached to the aorta and to the coronary artery beyond a blockage, which is now “bypassed.”
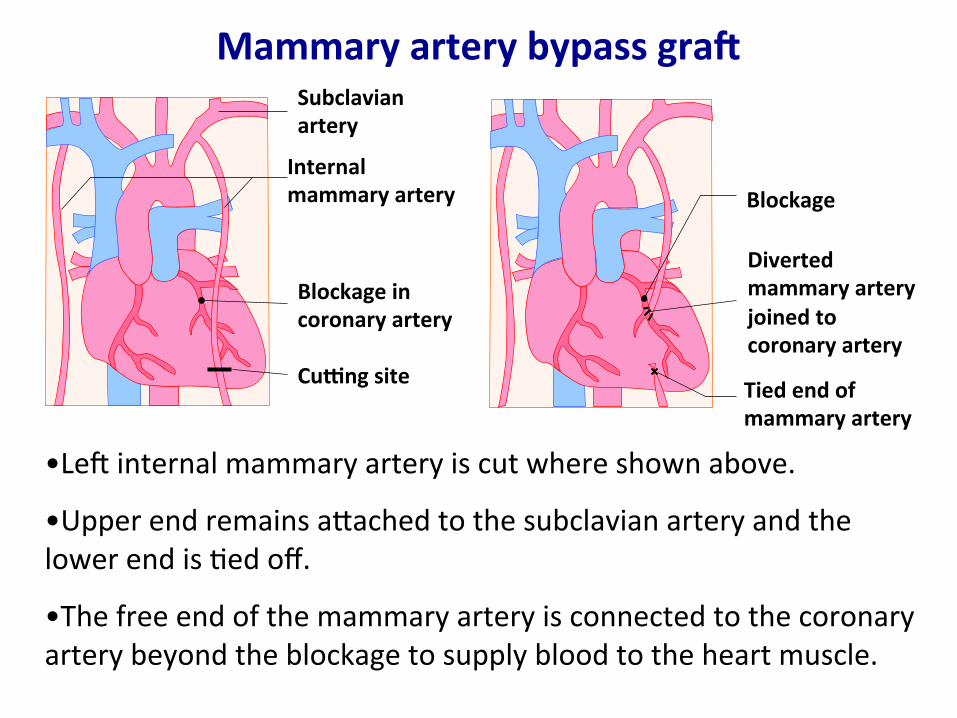
Mammary artery bypass graq Subclavian artery
Internal mammary artery
Blockage in coronary artery
Cujng site
Blockage
Diverted mammary artery joined to coronary artery
Tied end of mammary artery
•Le^ internal mammary artery is cut where shown above.
•Upper end remains anached to the subclavian artery and the lower end is Ned off.
•The free end of the mammary artery is connected to the coronary artery beyond the blockage to supply blood to the heart muscle.
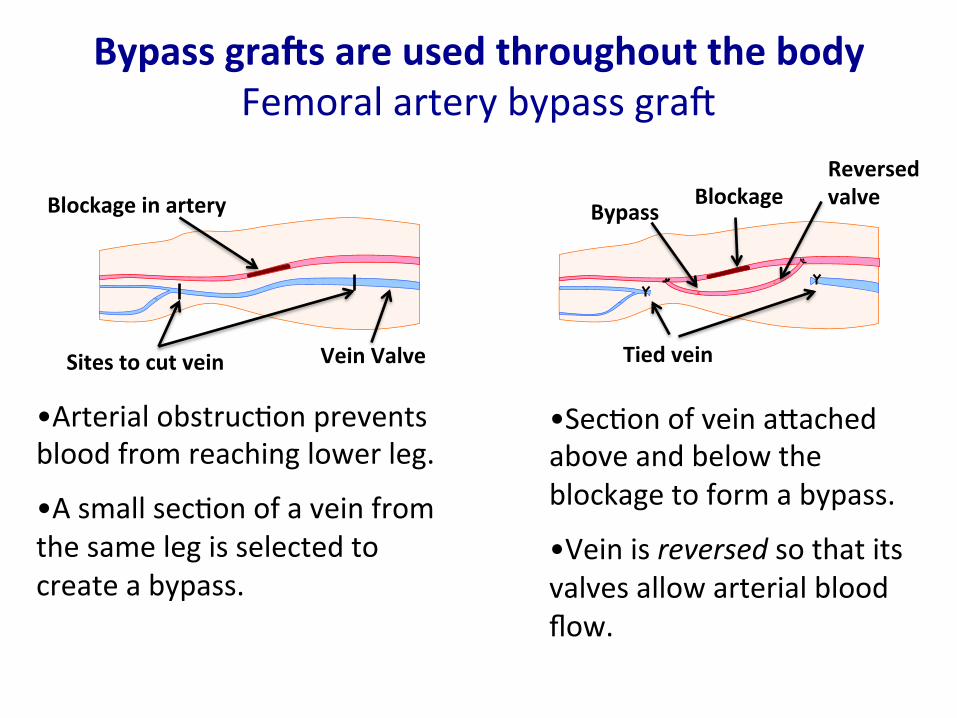
Bypass graqs are used throughout the body Femoral artery bypass gra^
•Arterial obstrucNon prevents blood from reaching lower leg.
•A small secNon of a vein from the same leg is selected to create a bypass.
•SecNon of vein anached above and below the blockage to form a bypass.
•Vein is reversed so that its valves allow arterial blood flow.
Reversed valve Blockage
Bypass
Tied vein Sites to cut vein
Blockage in artery
Vein Valve
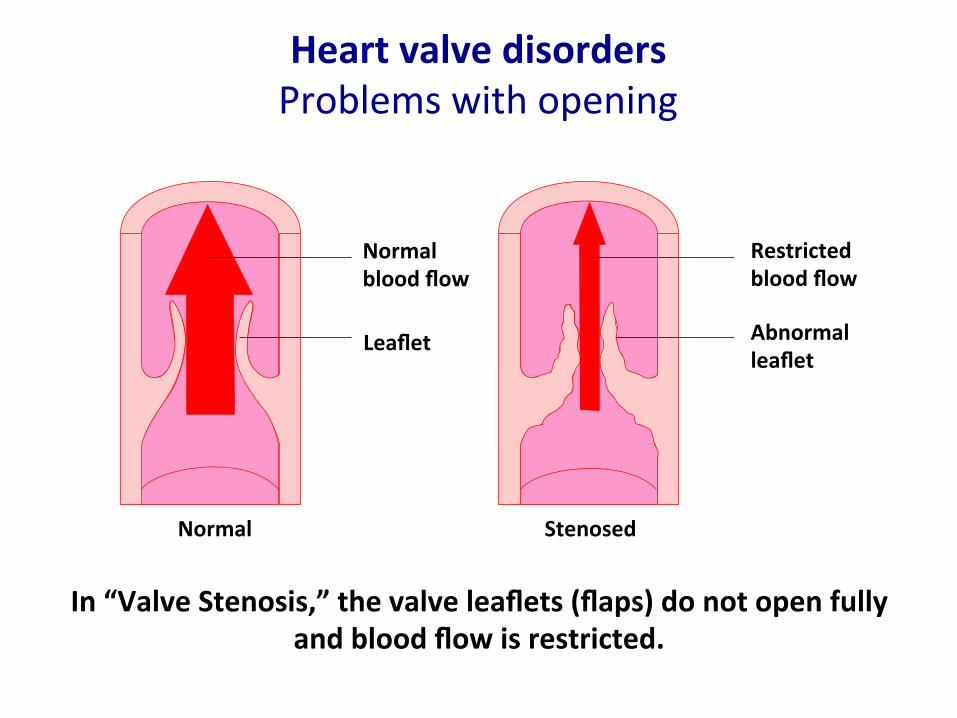
Heart valve disorders Problems with opening
Normal blood flow
Restricted blood flow
Leaflet Abnormal leaflet
In “Valve Stenosis,” the valve leaflets (flaps) do not open fully and blood flow is restricted.
Normal Stenosed
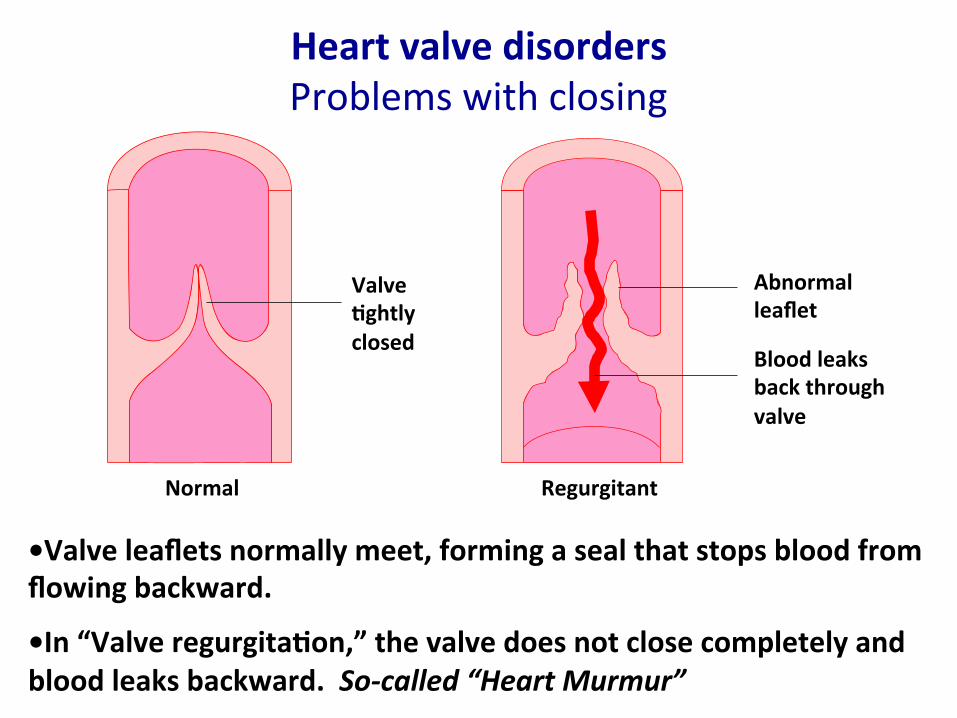
Heart valve disorders Problems with closing
•Valve leaflets normally meet, forming a seal that stops blood from flowing backward.
•In “Valve regurgita6on,” the valve does not close completely and blood leaks backward. So-‐called “Heart Murmur”
Blood leaks back through valve
Abnormal leaflet
Normal Regurgitant
Valve 6ghtly closed
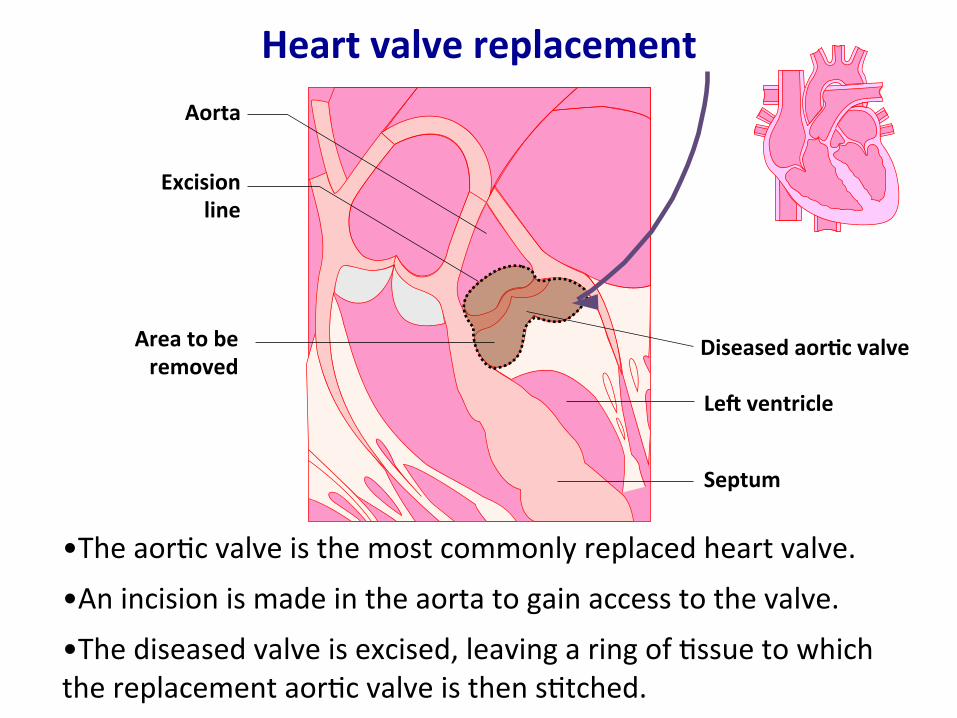
Heart valve replacement
•The aorNc valve is the most commonly replaced heart valve.
•An incision is made in the aorta to gain access to the valve.
•The diseased valve is excised, leaving a ring of Nssue to which the replacement aorNc valve is then sNtched.
Aorta
Excision line
Area to be removed
Diseased aor6c valve
Leq ventricle
Septum

Hypertrophic cardiomyopathy
•Septum and the le^ ventriclular wall become abnormally thick.
•Prevents the le^ ventricle from filling properly and obstructs the ouslow to the aorNc valve.
•leading cause of “sudden cardiac death” in athletes •Sudden Cardiac Arrest (SCA): heart suddenly and unexpectedly stops beaNng, causes death if not treated in minutes.
•can be asymptomaNc unNl death
Normal muscle
Thickened muscle
Thickened Septum
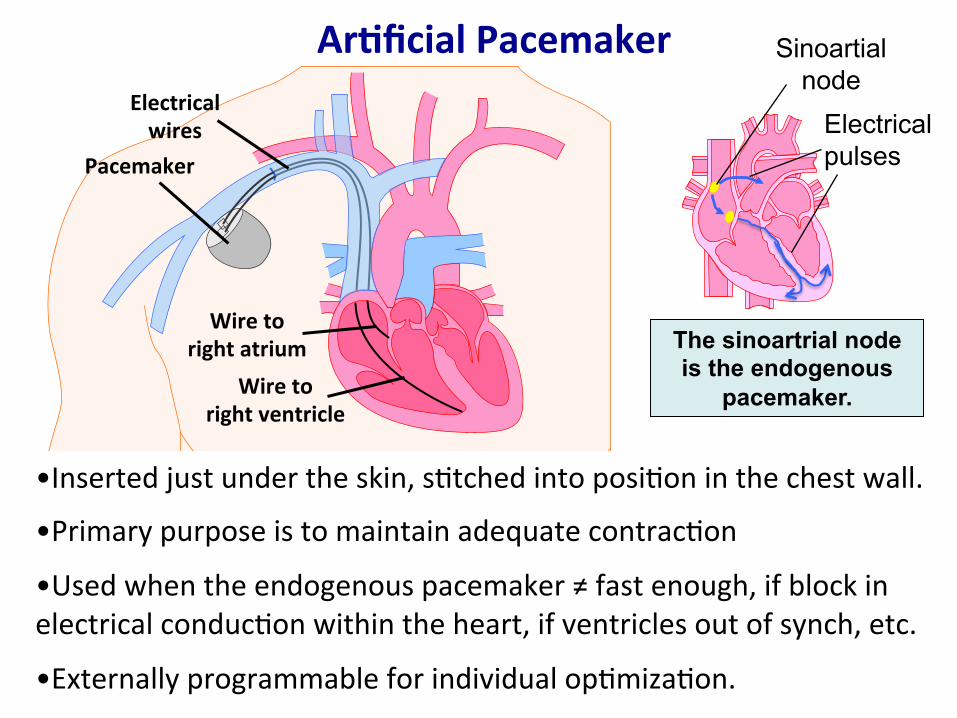
Ar6ficial Pacemaker Electrical wires
Pacemaker
Wire to right atrium
Wire to right ventricle
•Inserted just under the skin, sNtched into posiNon in the chest wall.
•Primary purpose is to maintain adequate contracNon
•Used when the endogenous pacemaker ≠ fast enough, if block in electrical conducNon within the heart, if ventricles out of synch, etc.
•Externally programmable for individual opNmizaNon.
Electrical pulses
Sinoartial node
The sinoartrial node is the endogenous
pacemaker.

Blood Pressure (BP) •Usually = arterial pressure in systemic circulaNon
•Expressed as systolic (maximum) / diastolic (minimum) in units of “mm Hg.”
Systolic: when the heart contracts Diastolic: between contracNons
•Normal resNng BP for adult: Between 90/60 and 120/80
•low = hypotension, high = hypertension
•Long-‐term hypertension is a risk factor for kidney failure, heart disease, stroke: places mechanical stress on artery walls
• If severely high (≥50% >average), only survive a few years without treatment
Hg manometer MV Hayes Wikipedia
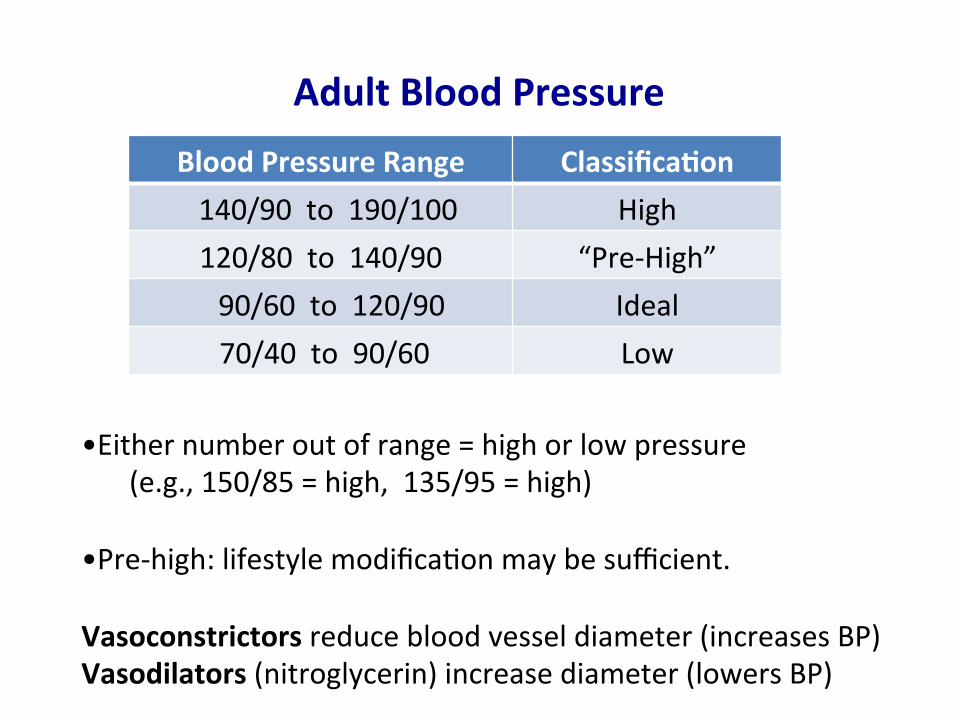
Adult Blood Pressure Blood Pressure Range Classifica6on 140/90 to 190/100 High 120/80 to 140/90 “Pre-‐High” 90/60 to 120/90 Ideal 70/40 to 90/60 Low
•Either number out of range = high or low pressure (e.g., 150/85 = high, 135/95 = high)
•Pre-‐high: lifestyle modificaNon may be sufficient. Vasoconstrictors reduce blood vessel diameter (increases BP) Vasodilators (nitroglycerin) increase diameter (lowers BP)
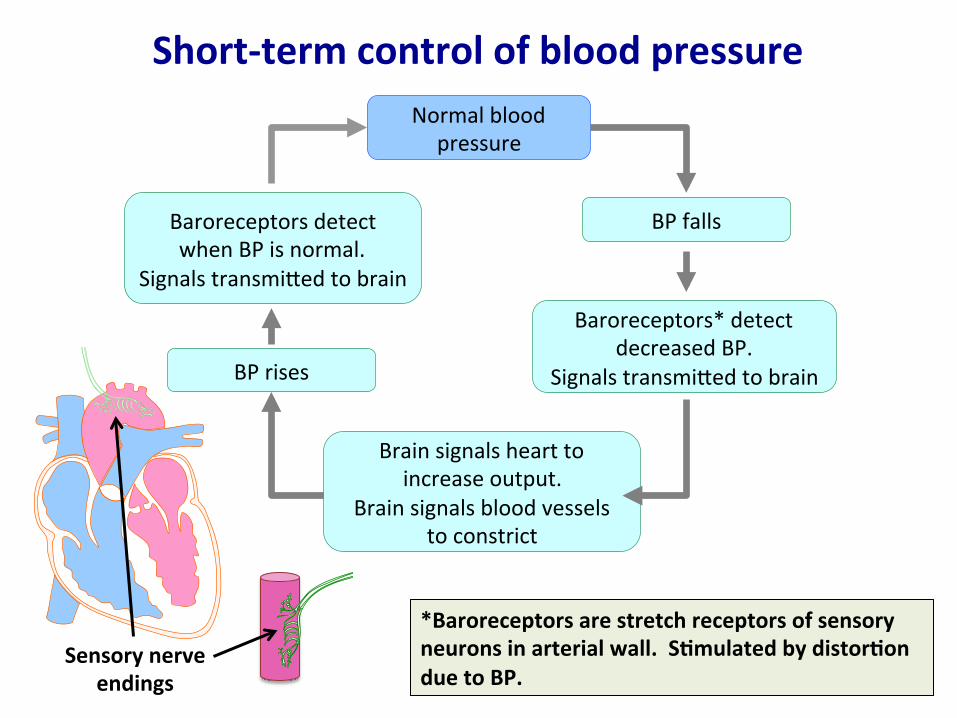
Short-‐term control of blood pressure Normal blood
pressure
Brain signals heart to increase output.
Brain signals blood vessels to constrict
Baroreceptors detect when BP is normal.
Signals transmined to brain
BP rises
Baroreceptors* detect decreased BP.
Signals transmined to brain
BP falls
*Baroreceptors are stretch receptors of sensory neurons in arterial wall. S6mulated by distor6on due to BP.
Sensory nerve endings
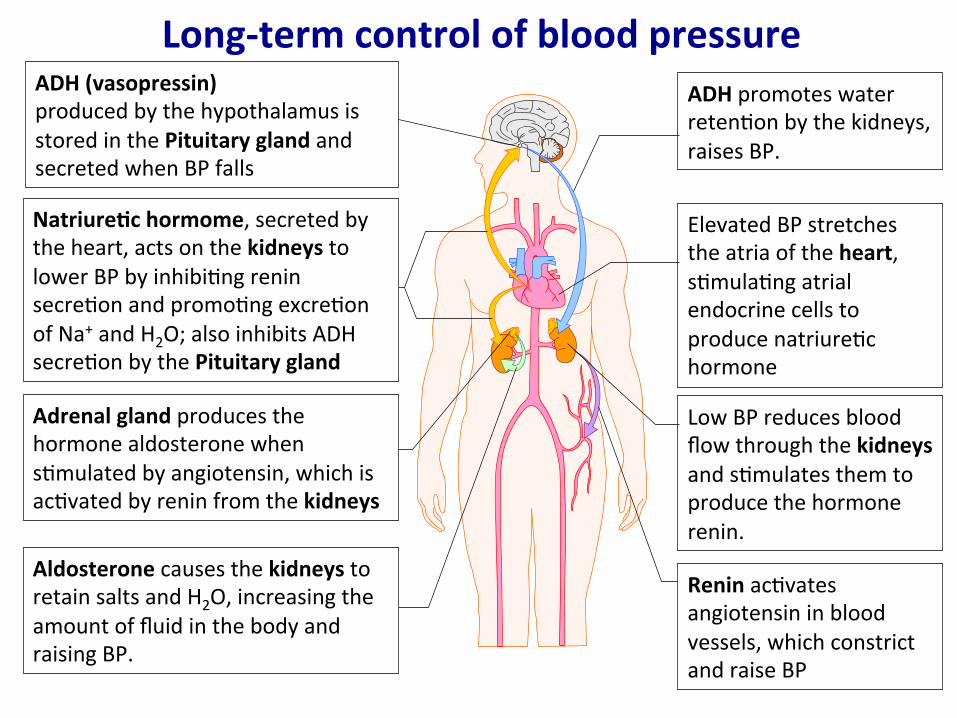
Long-‐term control of blood pressure ADH promotes water retenNon by the kidneys, raises BP.
Elevated BP stretches the atria of the heart, sNmulaNng atrial endocrine cells to produce natriureNc hormone
Low BP reduces blood flow through the kidneys and sNmulates them to produce the hormone renin.
Renin acNvates angiotensin in blood vessels, which constrict and raise BP
Aldosterone causes the kidneys to retain salts and H2O, increasing the amount of fluid in the body and raising BP.
Adrenal gland produces the hormone aldosterone when sNmulated by angiotensin, which is acNvated by renin from the kidneys
Natriure6c hormome, secreted by the heart, acts on the kidneys to lower BP by inhibiNng renin secreNon and promoNng excreNon of Na+ and H2O; also inhibits ADH secreNon by the Pituitary gland
ADH (vasopressin) produced by the hypothalamus is stored in the Pituitary gland and secreted when BP falls
What raises blood pressure? •Dietary Salt
OsmoNc problem, system trying to balance, therefore kidneys remove less H2O. Increased total fluid, increases BP.
DiureNcs (to deplete salt and H2O) can help
•Dietary Fat Creates resistance within the circulatory system, which
increases upstream BP. Resistance is related to vessel radius (the larger the radius,
the lower the resistance), as well as the smoothness of the blood vessel walls.
Smoothness is reduced by the buildup of fany deposits on the arterial walls.

What raises blood pressure?
• Chronic stress – “Fight or flight” reacNon causes a transient increase in BP. – Chronically under stress MAY contribute to long-‐term trouble
• Smoking – Temporary increase in blood pressure
• Excessive alcohol – Temporary increase blood pressure
• Overweight – Places extra strain on heart – Body mass index (weight vs. height) – Current lifestyle (sedentary) contributes… need to move!
Anemia • Abnormally low levels of RBCs or hemoglobin
• Individual with anemia feels constantly Nred, weak, due to insufficient O2. (more extreme: increased thirst, feeling faint)
• Results from – blood loss (trauma) – decreased RBC producNon (iron or B12 deficiency) – increased RBC breakdown (sickle cell anemia; infecNon, malaria, autoimmune disorder)
• ErythropoiNn, produced by kidneys, sNmulates bone marrow to generate more RBCs.
• “Blood doping” = syntheNc erythropoiNn. Gives an advantage in sports. (difficult to detect – erythropoiNn normally present and the syntheNc version is rapidly eliminated from blood)