cigna 3-month plan review (july-sept. 2015)
TRANSCRIPT

UTILIZATION/CLAIM REPORTING
..... , ::.f{-: Cigna.
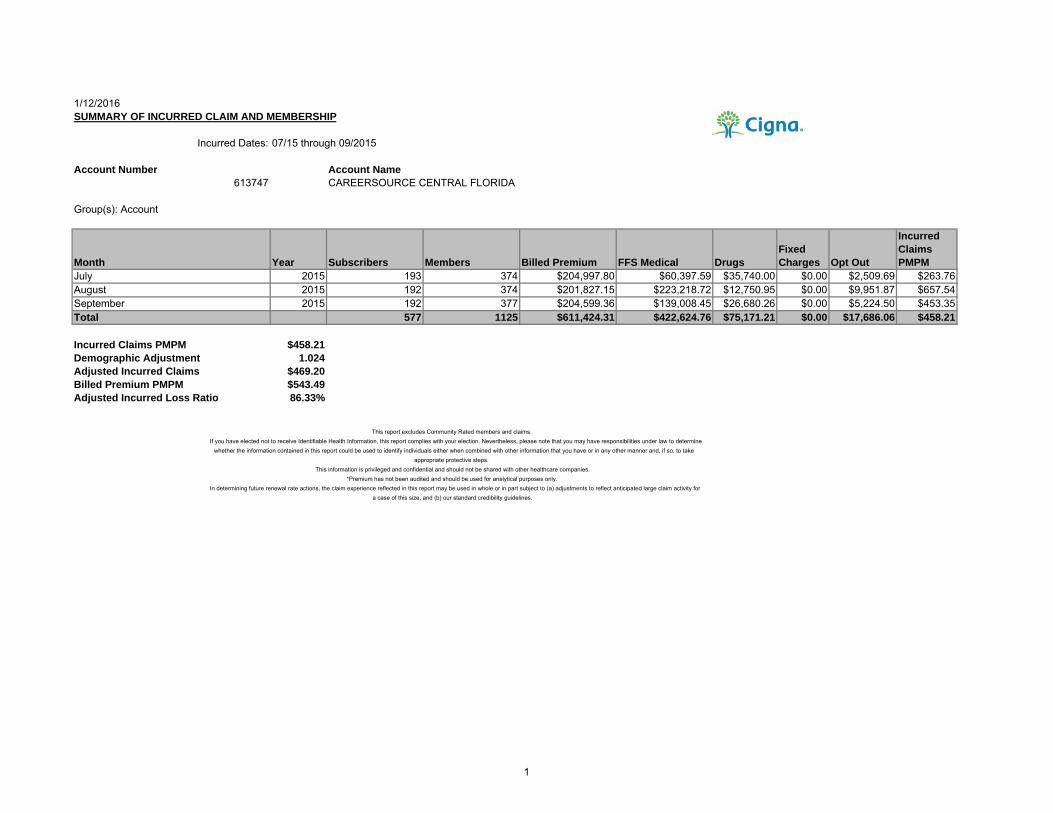
1/12/2016SUMMARY OF INCURRED CLAIM AND MEMBERSHIP
Incurred Dates: 07/15 through 09/2015
Account Number Account Name613747 CAREERSOURCE CENTRAL FLORIDA
Group(s): Account
Month Year Subscribers Members Billed Premium FFS Medical DrugsFixed Charges Opt Out
Incurred Claims PMPM
July 2015 193 374 $204,997.80 $60,397.59 $35,740.00 $0.00 $2,509.69 $263.76August 2015 192 374 $201,827.15 $223,218.72 $12,750.95 $0.00 $9,951.87 $657.54September 2015 192 377 $204,599.36 $139,008.45 $26,680.26 $0.00 $5,224.50 $453.35Total 577 1125 $611,424.31 $422,624.76 $75,171.21 $0.00 $17,686.06 $458.21
Incurred Claims PMPM $458.21Demographic Adjustment 1.024Adjusted Incurred Claims $469.20Billed Premium PMPM $543.49Adjusted Incurred Loss Ratio 86.33%
This report excludes Community Rated members and claims.If you have elected not to receive Identifiable Health Information, this report complies with your election. Nevertheless, please note that you may have responsibilities under law to determine
whether the information contained in this report could be used to identify individuals either when combined with other information that you have or in any other manner and, if so, to takeappropriate protective steps.
This information is privileged and confidential and should not be shared with other healthcare companies.*Premium has not been audited and should be used for analytical purposes only.
In determining future renewal rate actions, the claim experience reflected in this report may be used in whole or in part subject to (a) adjustments to reflect anticipated large claim activity fora case of this size, and (b) our standard credibility guidelines.
1
, ...... _
~-:(.:_ Cigna.
I I I
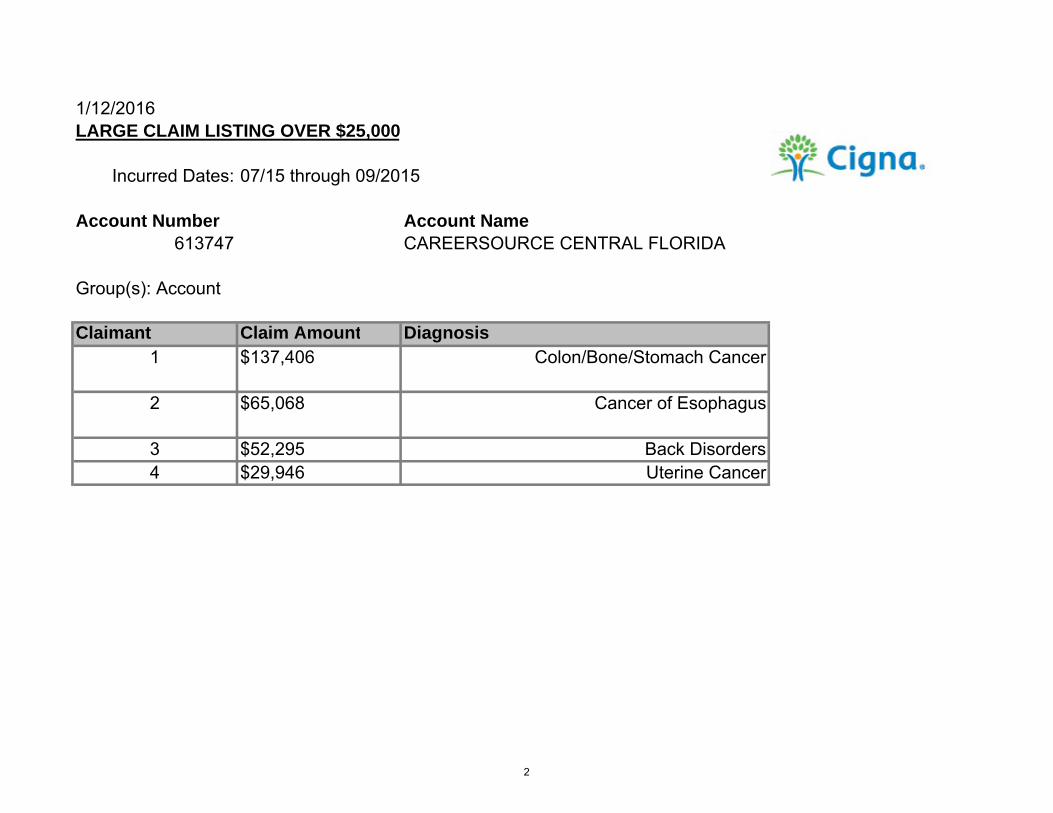
1/12/2016LARGE CLAIM LISTING OVER $25,000
Incurred Dates: 07/15 through 09/2015
Account Number Account Name613747 CAREERSOURCE CENTRAL FLORIDA
Group(s): Account
Claimant Claim Amount Diagnosis1 $137,406 Colon/Bone/Stomach Cancer
2 $65,068 Cancer of Esophagus
3 $52,295 Back Disorders4 $29,946 Uterine Cancer
2
···~ ~r_Cigna.
Consultative Analytics CareerSource Central Florida
Copyright 2016 Cigna - Confidential & Privileged - Not for Distribution
SM
3
Table of Contents
• Executive Summary
• Population Profile & Health Status
• Financial & Utilization Review
• Pharmacy
Global Parameters
Overall Dates Current
Incurred 10/2014 to 09/2015
Incurred Runout 10/2014 to 11/2015
Catastrophic Threshold $25,000
Exclude Pharmacy No
4
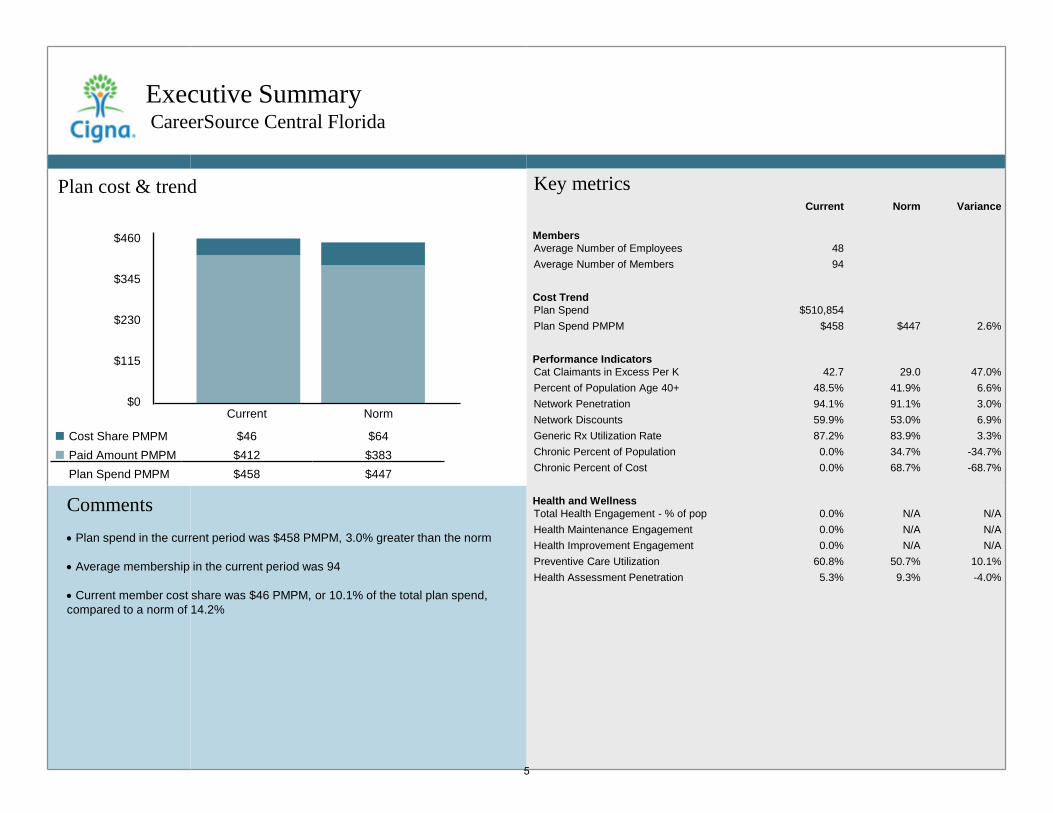
Plan cost & trend
Executive Summary CareerSource Central Florida
Comments • Plan spend in the current period was $458 PMPM, 3.0% greater than the norm • Average membership in the current period was 94 • Current member cost share was $46 PMPM, or 10.1% of the total plan spend, compared to a norm of 14.2%
$460
$345
$230
$115
$0
Key metrics Current Norm Variance
Members Average Number of Employees 48 Average Number of Members 94
Cost Trend Plan Spend $510,854 Plan Spend PMPM $458 $447 2.6%
Performance Indicators Cat Claimants in Excess Per K 42.7 29.0 47.0% Percent of Population Age 40+ 48.5% 41.9% 6.6% Network Penetration 94.1% 91.1% 3.0% Network Discounts 59.9% 53.0% 6.9% Generic Rx Utilization Rate 87.2% 83.9% 3.3% Chronic Percent of Population 0.0% 34.7% -34.7% Chronic Percent of Cost 0.0% 68.7% -68.7%
Health and Wellness Total Health Engagement - % of pop 0.0% N/A N/A Health Maintenance Engagement 0.0% N/A N/A Health Improvement Engagement 0.0% N/A N/A Preventive Care Utilization 60.8% 50.7% 10.1% Health Assessment Penetration 5.3% 9.3% -4.0%
Current Norm
$46 $64 $412 $383 $458 $447
Cost Share PMPM Paid Amount PMPM
Plan Spend PMPM
5
• •
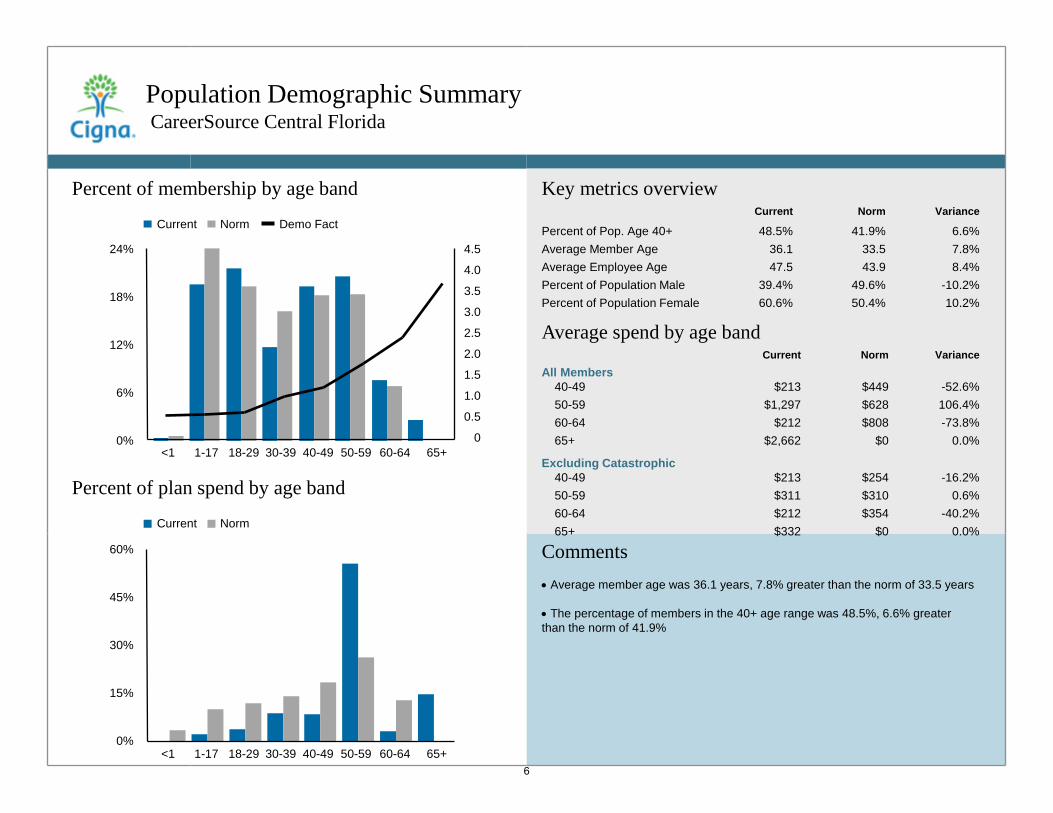
Population Demographic Summary CareerSource Central Florida
Percent of membership by age band
Comments • Average member age was 36.1 years, 7.8% greater than the norm of 33.5 years • The percentage of members in the 40+ age range was 48.5%, 6.6% greater than the norm of 41.9%
Key metrics overview Current Norm Variance
Percent of Pop. Age 40+ 48.5% 41.9% 6.6% Average Member Age 36.1 33.5 7.8% Average Employee Age 47.5 43.9 8.4% Percent of Population Male 39.4% 49.6% -10.2% Percent of Population Female 60.6% 50.4% 10.2%
Percent of plan spend by age band
Average spend by age band Current Norm Variance
All Members 40-49 $213 $449 -52.6% 50-59 $1,297 $628 106.4% 60-64 $212 $808 -73.8% 65+ $2,662 $0 0.0%
Excluding Catastrophic 40-49 $213 $254 -16.2% 50-59 $311 $310 0.6% 60-64 $212 $354 -40.2% 65+ $332 $0 0.0%
24%
18%
12%
6%
0% <1 1-17 18-29 30-39 40-49 50-59 60-64 65+
4.5
4.0
3.5
3.0
2.5
2.0
1.5
1.0
0.5
0
Current Norm Demo Fact
60%
45%
30%
15%
0% <1 1-17 18-29 30-39 40-49 50-59 60-64 65+
Current Norm
6
• • -
• •
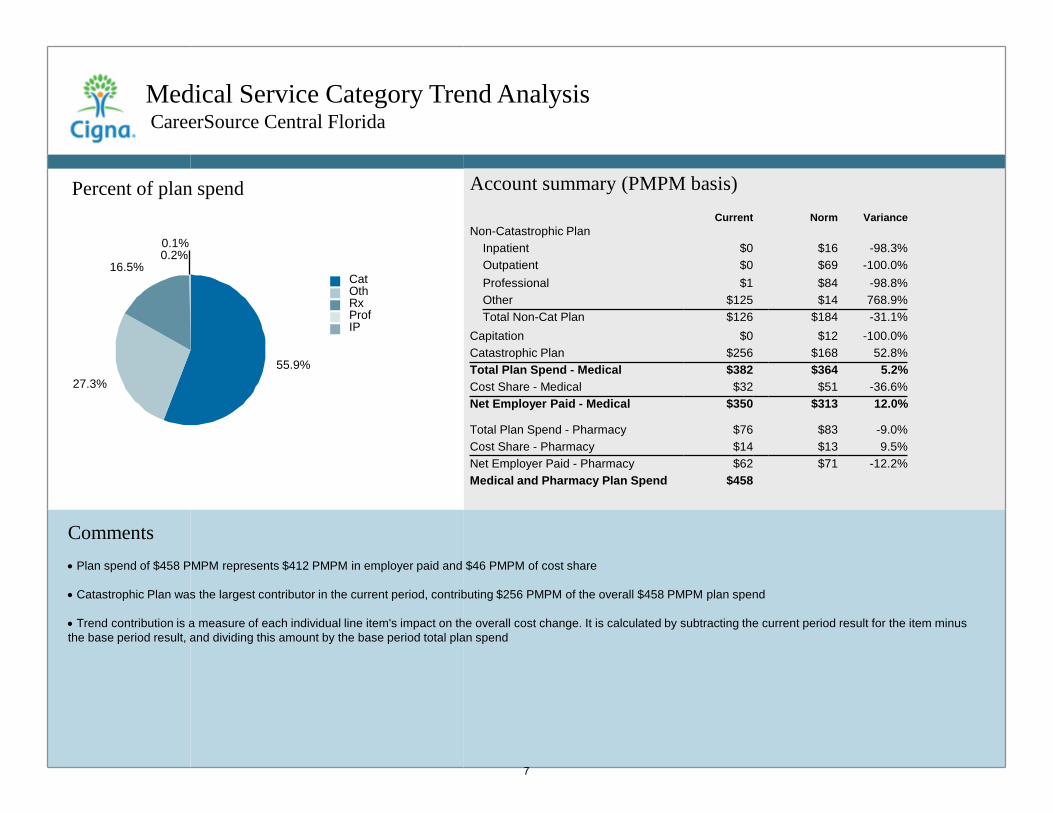
Medical Service Category Trend Analysis CareerSource Central Florida
Comments • Plan spend of $458 PMPM represents $412 PMPM in employer paid and $46 PMPM of cost share • Catastrophic Plan was the largest contributor in the current period, contributing $256 PMPM of the overall $458 PMPM plan spend • Trend contribution is a measure of each individual line item's impact on the overall cost change. It is calculated by subtracting the current period result for the item minus the base period result, and dividing this amount by the base period total plan spend
Account summary (PMPM basis) Current Norm Variance
Non-Catastrophic Plan Inpatient $0 $16 -98.3% Outpatient $0 $69 -100.0% Professional $1 $84 -98.8% Other $125 $14 768.9% Total Non-Cat Plan $126 $184 -31.1%
Capitation $0 $12 -100.0% Catastrophic Plan $256 $168 52.8% Total Plan Spend - Medical $382 $364 5.2% Cost Share - Medical $32 $51 -36.6% Net Employer Paid - Medical $350 $313 12.0%
Total Plan Spend - Pharmacy $76 $83 -9.0% Cost Share - Pharmacy $14 $13 9.5% Net Employer Paid - Pharmacy $62 $71 -12.2% Medical and Pharmacy Plan Spend $458
Cat Oth Rx Prof IP
55.9% 27.3%
16.5% 0.2% 0.1%
Percent of plan spend
7
• • • •
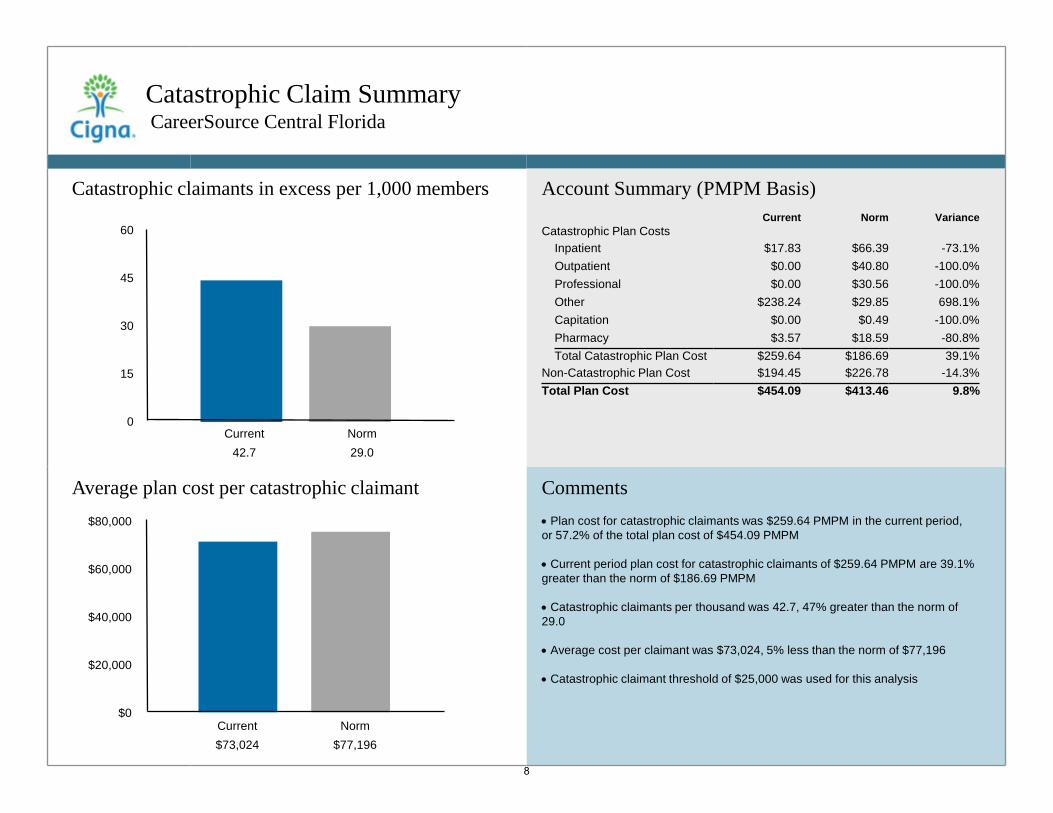
Catastrophic Claim Summary CareerSource Central Florida
Comments • Plan cost for catastrophic claimants was $259.64 PMPM in the current period, or 57.2% of the total plan cost of $454.09 PMPM • Current period plan cost for catastrophic claimants of $259.64 PMPM are 39.1% greater than the norm of $186.69 PMPM • Catastrophic claimants per thousand was 42.7, 47% greater than the norm of 29.0 • Average cost per claimant was $73,024, 5% less than the norm of $77,196 • Catastrophic claimant threshold of $25,000 was used for this analysis
60
45
30
15
0
Account Summary (PMPM Basis) Current Norm Variance
Catastrophic Plan Costs Inpatient $17.83 $66.39 -73.1% Outpatient $0.00 $40.80 -100.0% Professional $0.00 $30.56 -100.0% Other $238.24 $29.85 698.1% Capitation $0.00 $0.49 -100.0% Pharmacy $3.57 $18.59 -80.8% Total Catastrophic Plan Cost $259.64 $186.69 39.1%
Non-Catastrophic Plan Cost $194.45 $226.78 -14.3% Total Plan Cost $454.09 $413.46 9.8%
Catastrophic claimants in excess per 1,000 members
Average plan cost per catastrophic claimant
Current Norm 42.7 29.0
$80,000
$60,000
$40,000
$20,000
$0 Current Norm $73,024 $77,196
8
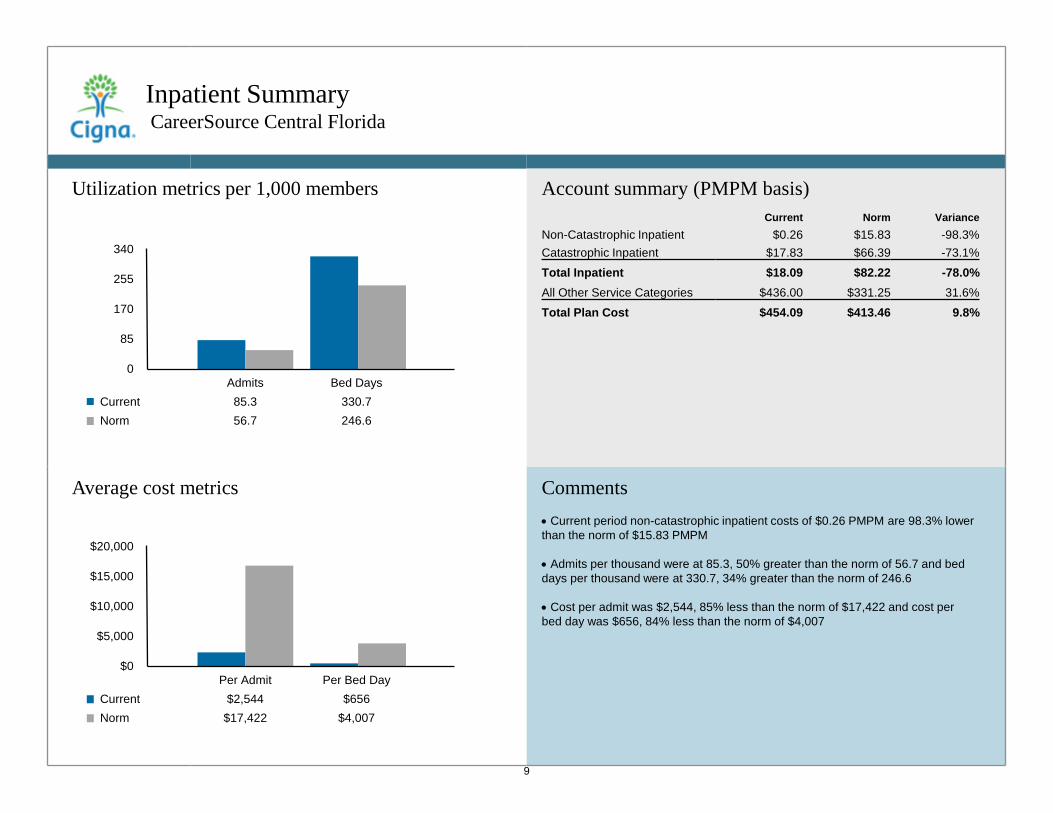
Inpatient Summary CareerSource Central Florida
Comments • Current period non-catastrophic inpatient costs of $0.26 PMPM are 98.3% lower than the norm of $15.83 PMPM • Admits per thousand were at 85.3, 50% greater than the norm of 56.7 and bed days per thousand were at 330.7, 34% greater than the norm of 246.6 • Cost per admit was $2,544, 85% less than the norm of $17,422 and cost per bed day was $656, 84% less than the norm of $4,007
Account summary (PMPM basis) Current Norm Variance
Non-Catastrophic Inpatient $0.26 $15.83 -98.3% Catastrophic Inpatient $17.83 $66.39 -73.1%
Total Inpatient $18.09 $82.22 -78.0% All Other Service Categories $436.00 $331.25 31.6%
Total Plan Cost $454.09 $413.46 9.8%
Utilization metrics per 1,000 members
Average cost metrics
340
255
170
85
0
Current Norm
Admits Bed Days 85.3 330.7 56.7 246.6
$20,000
$15,000
$10,000
$5,000
$0
Current Norm
Per Admit Per Bed Day $2,544 $656
$17,422 $4,007
9
• •
• •
I l
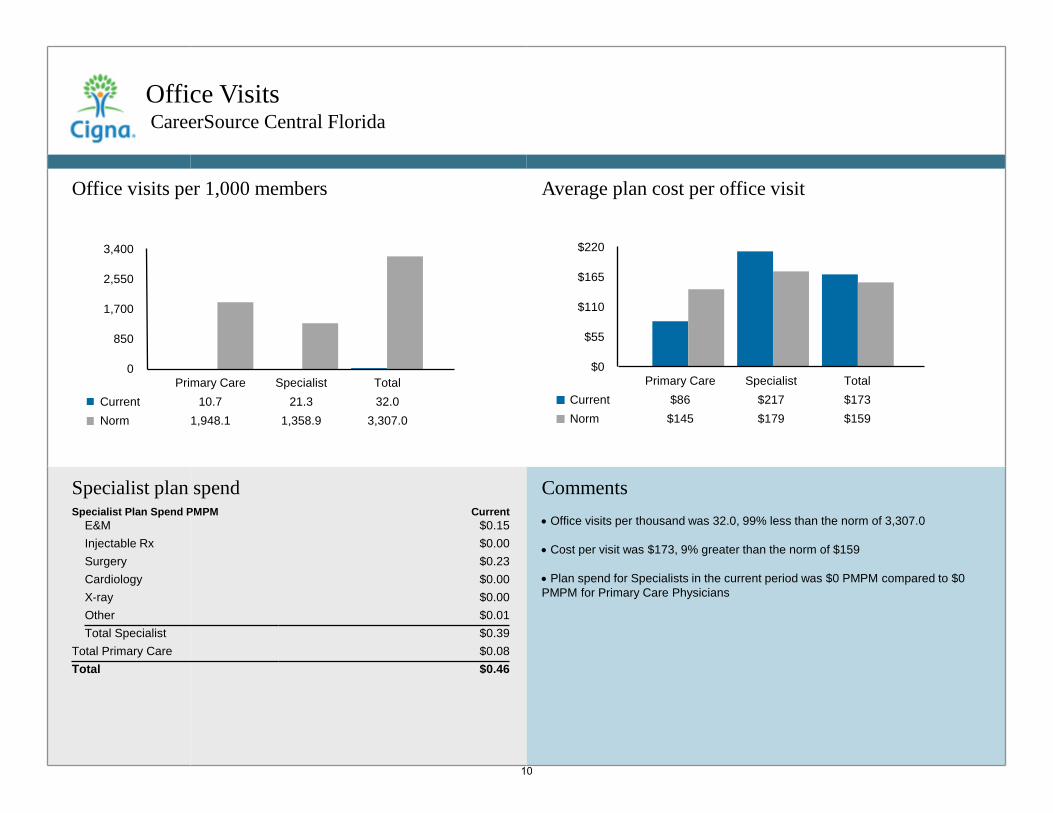
Office Visits CareerSource Central Florida
Comments • Office visits per thousand was 32.0, 99% less than the norm of 3,307.0 • Cost per visit was $173, 9% greater than the norm of $159 • Plan spend for Specialists in the current period was $0 PMPM compared to $0 PMPM for Primary Care Physicians
3,400
2,550
1,700
850
0
Current Norm
Primary Care Specialist Total 10.7 21.3 32.0
1,948.1 1,358.9 3,307.0
$220
$165
$110
$55
$0
Current Norm
Primary Care Specialist Total $86 $217 $173
$145 $179 $159
Specialist plan spend Specialist Plan Spend PMPM Current
E&M $0.15 Injectable Rx $0.00 Surgery $0.23 Cardiology $0.00 X-ray $0.00 Other $0.01 Total Specialist $0.39
Total Primary Care $0.08 Total $0.46
Office visits per 1,000 members Average plan cost per office visit
10
• •
• •
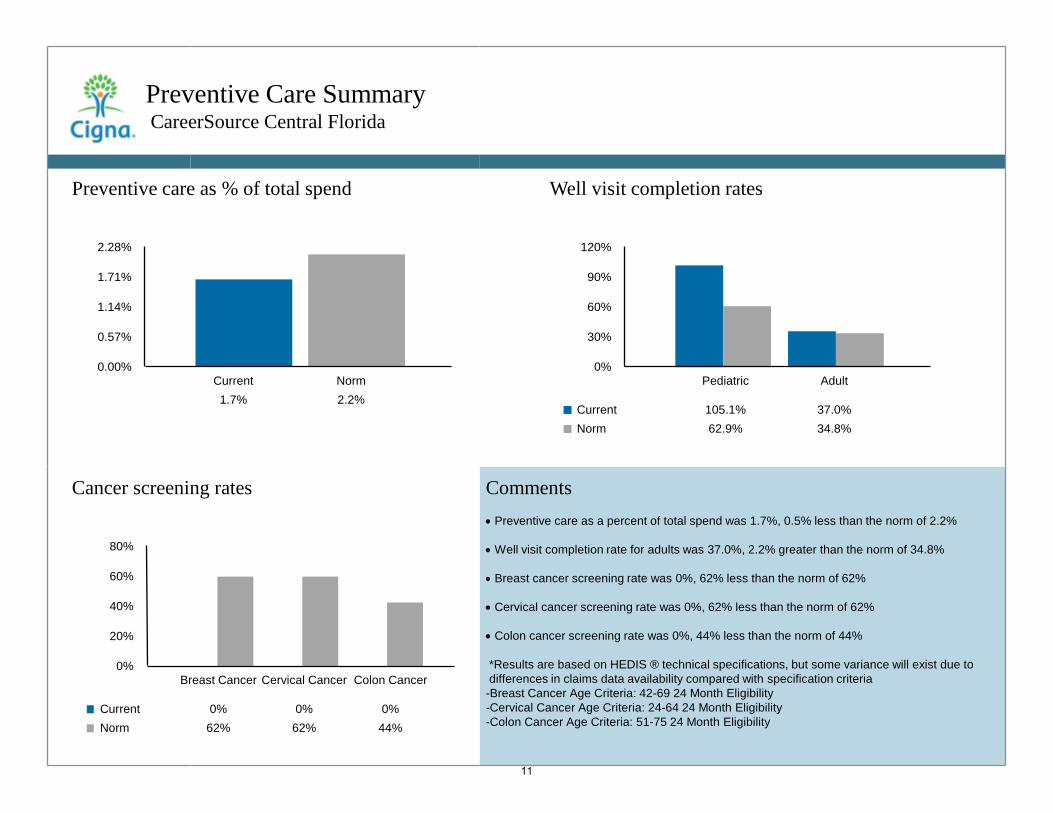
Preventive Care Summary CareerSource Central Florida
Preventive care as % of total spend
2.28%
1.71%
1.14%
0.57%
0.00%
Cancer screening rates
80%
60%
40%
20%
0%
Current Norm
Breast Cancer Cervical Cancer Colon Cancer
0% 0% 0% 62% 62% 44%
Current Norm 1.7% 2.2%
Well visit completion rates
120%
90%
60%
30%
0%
Current Norm
Pediatric Adult
105.1% 37.0% 62.9% 34.8%
Comments • Preventive care as a percent of total spend was 1.7%, 0.5% less than the norm of 2.2% • Well visit completion rate for adults was 37.0%, 2.2% greater than the norm of 34.8% • Breast cancer screening rate was 0%, 62% less than the norm of 62% • Cervical cancer screening rate was 0%, 62% less than the norm of 62% • Colon cancer screening rate was 0%, 44% less than the norm of 44% *Results are based on HEDIS ® technical specifications, but some variance will exist due to differences in claims data availability compared with specification criteria -Breast Cancer Age Criteria: 42-69 24 Month Eligibility -Cervical Cancer Age Criteria: 24-64 24 Month Eligibility -Colon Cancer Age Criteria: 51-75 24 Month Eligibility
11
• •
- -
• •
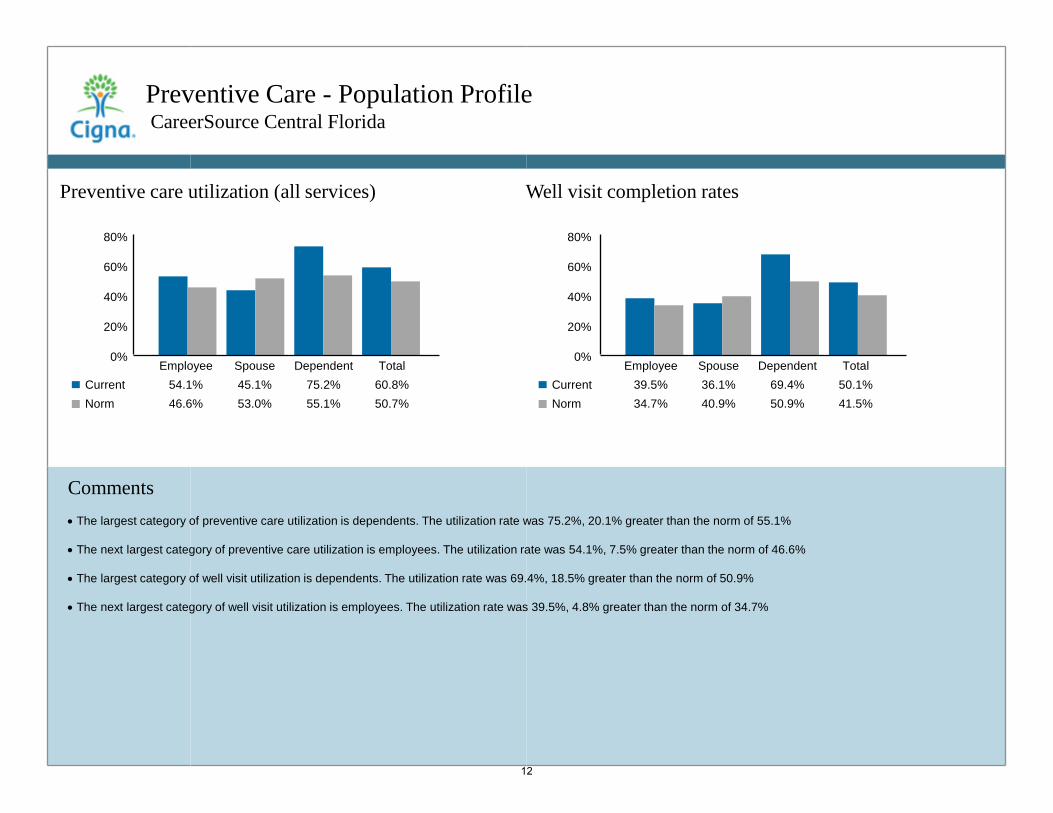
Preventive Care - Population Profile CareerSource Central Florida
Comments • The largest category of preventive care utilization is dependents. The utilization rate was 75.2%, 20.1% greater than the norm of 55.1% • The next largest category of preventive care utilization is employees. The utilization rate was 54.1%, 7.5% greater than the norm of 46.6% • The largest category of well visit utilization is dependents. The utilization rate was 69.4%, 18.5% greater than the norm of 50.9% • The next largest category of well visit utilization is employees. The utilization rate was 39.5%, 4.8% greater than the norm of 34.7%
Current Norm
80%
60%
40%
20%
0%
Well visit completion rates Preventive care utilization (all services)
80%
60%
40%
20%
0%
Current Norm
Employee Spouse Dependent Total 54.1% 45.1% 75.2% 60.8% 46.6% 53.0% 55.1% 50.7%
Employee Spouse Dependent Total 39.5% 36.1% 69.4% 50.1% 34.7% 40.9% 50.9% 41.5%
12
• •
• •
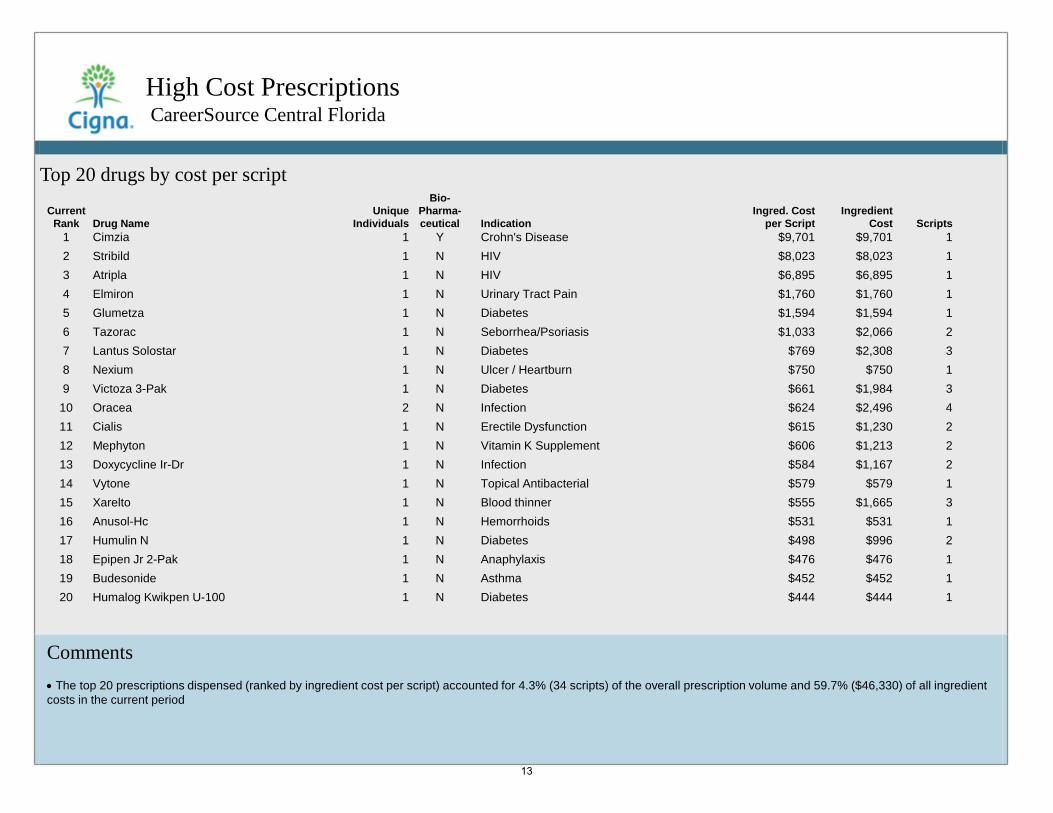
High Cost Prescriptions CareerSource Central Florida
Comments • The top 20 prescriptions dispensed (ranked by ingredient cost per script) accounted for 4.3% (34 scripts) of the overall prescription volume and 59.7% ($46,330) of all ingredient costs in the current period
Top 20 drugs by cost per script
Current Rank Drug Name
Unique Individuals
Bio-Pharma-ceutical Indication
Ingred. Cost per Script
Ingredient Cost Scripts
1 Cimzia 1 Y Crohn's Disease $9,701 $9,701 1 2 Stribild 1 N HIV $8,023 $8,023 1 3 Atripla 1 N HIV $6,895 $6,895 1 4 Elmiron 1 N Urinary Tract Pain $1,760 $1,760 1 5 Glumetza 1 N Diabetes $1,594 $1,594 1 6 Tazorac 1 N Seborrhea/Psoriasis $1,033 $2,066 2 7 Lantus Solostar 1 N Diabetes $769 $2,308 3 8 Nexium 1 N Ulcer / Heartburn $750 $750 1 9 Victoza 3-Pak 1 N Diabetes $661 $1,984 3
10 Oracea 2 N Infection $624 $2,496 4 11 Cialis 1 N Erectile Dysfunction $615 $1,230 2 12 Mephyton 1 N Vitamin K Supplement $606 $1,213 2 13 Doxycycline Ir-Dr 1 N Infection $584 $1,167 2 14 Vytone 1 N Topical Antibacterial $579 $579 1 15 Xarelto 1 N Blood thinner $555 $1,665 3 16 Anusol-Hc 1 N Hemorrhoids $531 $531 1 17 Humulin N 1 N Diabetes $498 $996 2 18 Epipen Jr 2-Pak 1 N Anaphylaxis $476 $476 1 19 Budesonide 1 N Asthma $452 $452 1 20 Humalog Kwikpen U-100 1 N Diabetes $444 $444 1
13
_.....,,
!i~ Cigna.
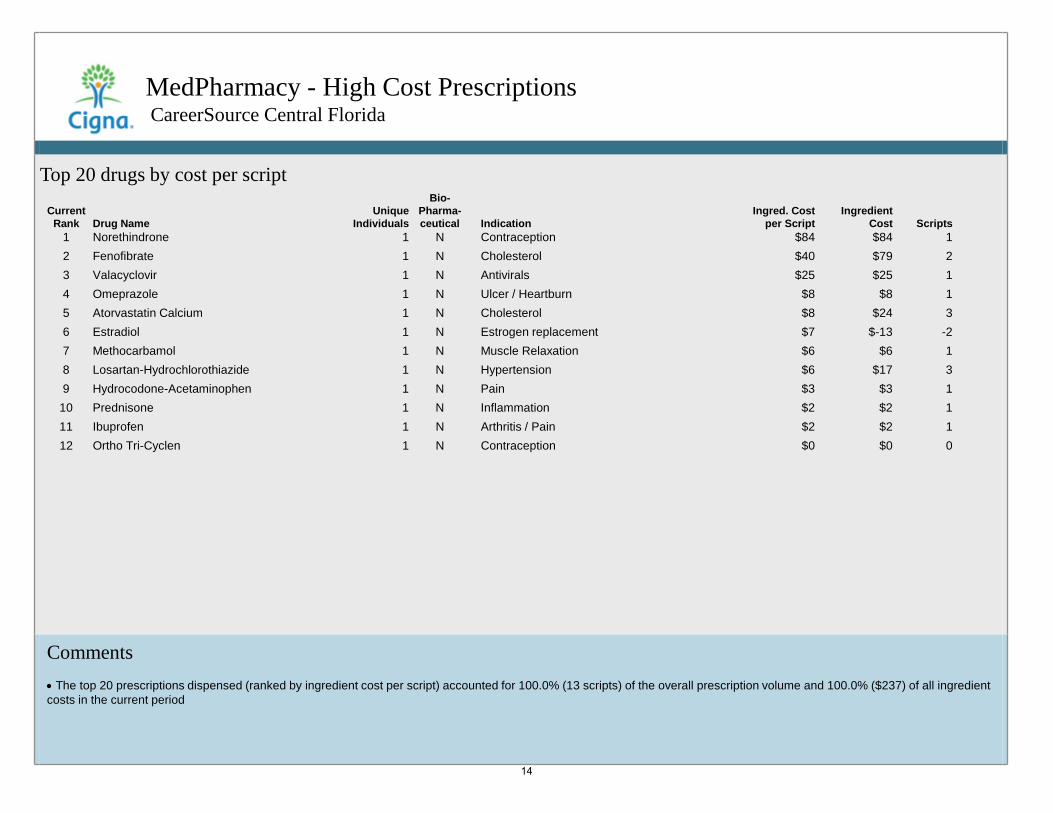
MedPharmacy - High Cost Prescriptions CareerSource Central Florida
Comments • The top 20 prescriptions dispensed (ranked by ingredient cost per script) accounted for 100.0% (13 scripts) of the overall prescription volume and 100.0% ($237) of all ingredient costs in the current period
Top 20 drugs by cost per script
Current Rank Drug Name
Unique Individuals
Bio-Pharma-ceutical Indication
Ingred. Cost per Script
Ingredient Cost Scripts
1 Norethindrone 1 N Contraception $84 $84 1 2 Fenofibrate 1 N Cholesterol $40 $79 2 3 Valacyclovir 1 N Antivirals $25 $25 1 4 Omeprazole 1 N Ulcer / Heartburn $8 $8 1 5 Atorvastatin Calcium 1 N Cholesterol $8 $24 3 6 Estradiol 1 N Estrogen replacement $7 $-13 -2 7 Methocarbamol 1 N Muscle Relaxation $6 $6 1 8 Losartan-Hydrochlorothiazide 1 N Hypertension $6 $17 3 9 Hydrocodone-Acetaminophen 1 N Pain $3 $3 1
10 Prednisone 1 N Inflammation $2 $2 1 11 Ibuprofen 1 N Arthritis / Pain $2 $2 1 12 Ortho Tri-Cyclen 1 N Contraception $0 $0 0
14
_.....,,
!i~ Cigna.
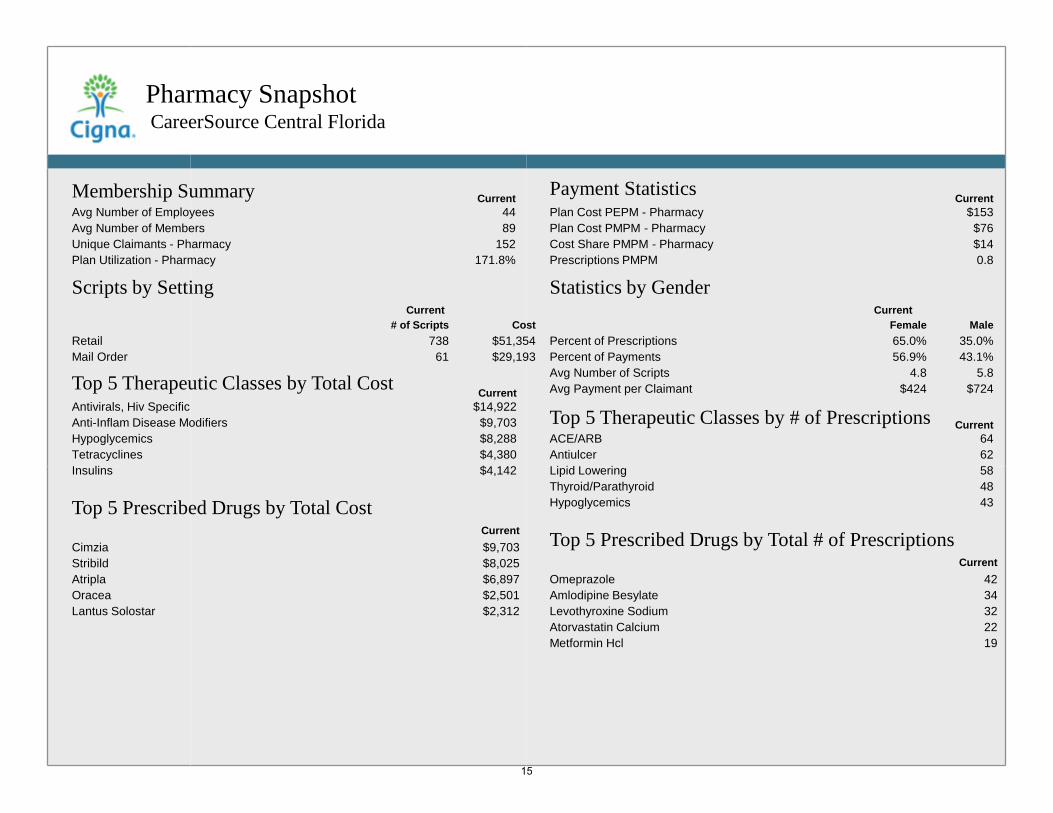
Pharmacy Snapshot CareerSource Central Florida
Top 5 Therapeutic Classes by Total Cost Current Antivirals, Hiv Specific $14,922 Anti-Inflam Disease Modifiers $9,703 Hypoglycemics $8,288 Tetracyclines $4,380 Insulins $4,142
Top 5 Therapeutic Classes by # of Prescriptions Current ACE/ARB 64 Antiulcer 62 Lipid Lowering 58 Thyroid/Parathyroid 48 Hypoglycemics 43 Top 5 Prescribed Drugs by Total Cost
Current Cimzia $9,703 Stribild $8,025 Atripla $6,897 Oracea $2,501 Lantus Solostar $2,312
Statistics by Gender Current
Female Male Percent of Prescriptions 65.0% 35.0% Percent of Payments 56.9% 43.1% Avg Number of Scripts 4.8 5.8 Avg Payment per Claimant $424 $724
Payment Statistics Current Plan Cost PEPM - Pharmacy $153 Plan Cost PMPM - Pharmacy $76 Cost Share PMPM - Pharmacy $14 Prescriptions PMPM 0.8
Top 5 Prescribed Drugs by Total # of Prescriptions Current
Omeprazole 42 Amlodipine Besylate 34 Levothyroxine Sodium 32 Atorvastatin Calcium 22 Metformin Hcl 19
Scripts by Setting Current
# of Scripts Cost Retail 738 $51,354 Mail Order 61 $29,193
Membership Summary Current Avg Number of Employees 44 Avg Number of Members 89 Unique Claimants - Pharmacy 152 Plan Utilization - Pharmacy 171.8%
15
Glossary
Acute An illness of short duration (as opposed to chronic illness). Admission An overnight confinement to a facility. Brand Name The proprietary or trade name of the medication. Breast Cancer Screening Measures the percent of qualified women 40-69 years of age that are compliant with mammogram screening. Capitation Arrangement where network providers receive a set dollar amount of money per covered member assigned to their practice, even if no services rendered. Cardiac catheterization A medical procedure used to diagnose and treat certain heart conditions. Catastrophic Term used to describe when a member has accumulated payments in excess of $50,000 for a specified time period. Centers of Excellence Cigna's defined network of facilities deemed superior in status due to their clinical and financial performance in providing patient care. Cervical Cancer Screening Measures the percent of qualified members greater than 29 years of age who received at least one pap smear. Chronic Defined as an illness or sickness that is not curable but may be controlled with treatment.
Chronic Obstructive Pulmonary Disease (COPD) Defines a group of diseases characterized by airflow obstruction and includes chronic bronchitis and emphysema. Churn Those members who either enrolled or disenrolled or did both during the analysis period (includes newborns). Coinsurance The percentage of covered expenses paid by the member when costs are being shared by both the plan and the individual member. Colon Cancer Screening Colorectal Cancer Screening (CRC) can detect pre-malignant polyps and guide their removal, which in theory can prevent the development of colon cancer. Convenience Care Treatment for common family ailments such as strep throat, pinkeye and athlete's foot Coordination of Benefits (COB) The amount saved when Cigna is the secondary insurer. It represents the difference between what Cigna pays and (COB) what it would have paid if it were primary. Copay Predetermined fees for medical services covered by a benefit plan, which are paid by the member at the time of service. Coronary angioplasty A medical procedure in which a balloon is used to open a blockage in a coronary (heart) artery narrowed by atherosclerosis, improving blood flow. Coronary Artery Bypass Graft (CABG) Surgery where blood flow is rerouted through a new artery or vein that is grafted around diseased sections of coronary arteries.
16
....... .. ,,,;:. • · ·~· . . ,- ......._
Cigna.
Glossary
Cost Share Benefit plan arrangement requiring that the participant pay a portion of the costs. This includes copayments, coinsurance and deductibles. Covered Charges Net charges minus the items not covered by the benefit plan. Items not covered include charges for ineligible services, network discounts, etc. CT A diagnostic imaging scan also called a Cat Scan (computed tomography). Deductible An amount specified in plan design that must be paid by member for covered expenses in a benefit period before the plan will pay benefits. Denied Charges Amounts not covered due to lack of information about the claim. Diagnostic Testing Refers to other significant testing procedures not named - examples include: doppler electrocardiograph, cardiac ultrasound and sleep studies. Discounts Amounts reduced by a contractual fee arrangement with network participating providers, prompt pay arrangements, or Hospital Savings Program (HSP). Emergency Room - Diagnostic Groupings Musc - Musculoskeletal ENT - Ear/Nose/Throat Skin - Skin Resp - Respiratory Circ - Circulatory Dig - Digestive Inj - Injury
Episode Treatment Group (ETG) An illness classification methodology derived by analyzing actual claim experience and clinical review. Esophagitis (digestive) Inflammation of the lining of the esophagus, the tube that carries food from the throat to the stomach. Evaluation and Management (E&M) E&M services refer to visits and consultations furnished by physicians. Facility A site where health care services are delivered including hospitals, convalescent units, skilled nursing facilities, and birthing centers. Facility Outpatient Refers to services and costs that are incurred at a facility but did not result in an admission. Fee for Service Compensating providers for rendering patient care which is based on an as services are rendered basis. Gastroenteritis (digestive) A condition that causes irritation and inflammation of the stomach and intestines (the gastrointestinal tract). Generic Drug A prescription drug that has the same active-ingredient formula as a brand-name drug. Generic Efficiency This metric illustrates the rate of generic utilization for drugs in which a generic option is available.
17
....... .. ,,,;:. • · ·~· . . ,- ......._
Cigna.
Glossary
Health Advocacy Health Advocacy is the term Cigna uses to describe the process we use to improve health and lower costs for our customers and members. Inpatient Refers to services and costs that are incurred during a facility admission. Lipotropics Drugs which are designed to lower cholesterol and triglyceride levels which help reduce amount of overall fatty substances in the blood. Mail Order Drugs A feature of a pharmacy program that enables a participant to send their prescription (and any applicable copay) directly to a mail-order vendor. Maintenance Drugs Medications that are prescribed for long-term treatment of chronic conditions, such as diabetes, high blood pressure or asthma. Major Diagnostic Categories (MDC) Industry standard groupings of ICD diagnostic codes which relate to various body systems for inpatient and outpatient claims. Major Joint (musculoskeletal) Examples of what comprises this category are: major joint and limb reattachments, hip or knee replacement. MRI Magnetic Resonance Imaging - a type of diagnostic test Network Dollar Penetration All charges submitted by in-network providers as a percentage of overall charges. Non-Preferred Brand Drug Drugs in the third tier of a pharmacy program, brand-name drugs that either have generic equivalents or may have one or more preferred brand options.
Norm Norm refers to the comparison group based on book of business or industry experience for the defined parameters. Norms are annualized unless otherwise stated. Office visit Services delivered by a physician, clinician, or practitioner within the confines of a professional office setting. Orthopedic A branch of medicine concerned with the correction or prevention of deformities, disorders, or injuries of the skeleton (tendons and ligaments) Other Medical (cardiac) Some examples of what comprises this category: hypertension, vascular procedures and angina. Other Surgical (cardiac) Some examples of what comprises this category: major cardiovascular procedures, circulatory disorders and pacemaker. Outpatient Refers to services and costs that are incurred outside of a facility admission. Pathology The study and diagnosis of disease through examination of organs, tissues, bodily fluids and whole bodies PET scan Positron Emission Tomography scan (specialized imaging) Pharmacy Payments Includes prescription drug expenses paid under a pharmacy program. These expenses would not include drugs covered under the medical benefit plan.
18
....... .. ,,,;:. • · ·~· . . ,- ......._
Cigna.
Glossary
Preferred Brand Drug Drugs in the second tier of a Cigna HealthCare two or three tier pharmacy program which have no generic equivalent. Preventive Care Measures taken to prevent illness or injury and may include examinations/screening tests tailored to an individual's age, health, and family history. Primary Care Practitioner Include physicians and nonphysician primary care practitioners whom members are able to select as primary care practitioners. Professional This category includes primary care physicians, specialists (oncologists, cardiologists, neurologists, obstetricians, etc.), surgeons, etc.. Radiology Radiology is the medical specialty directing medical imaging technologies to diagnose and treat diseases. Retail Relates to services rendered by participating retail pharmacies. Script A dispensed prescription. Spinal fusion A surgical procedure used to correct problems with the bones (vertebrae) of the back (spine). Therapeutic Class Major therapeutic classes include Central Nervous System, Cardiovascular, Hormonal, Anti-infectives, Pain, Allergy/Respiratory and other drugs.
Unique Claimants A count of members who had one or more claims processed for a benefit plan during a specified time period. Valve Replacement Example of what comprises this category: cardiac valve and other major cardiothoracic procedures. Well Visits Designed to discuss general health and any problems, then focus on general disease prevention and health maintenance on a regular basis
19
....... .. ,,,;:. • · ·~· . . ,- ......._
Cigna.

ADDITIONAL REPORTING
..... , ::.f{-: Cigna.
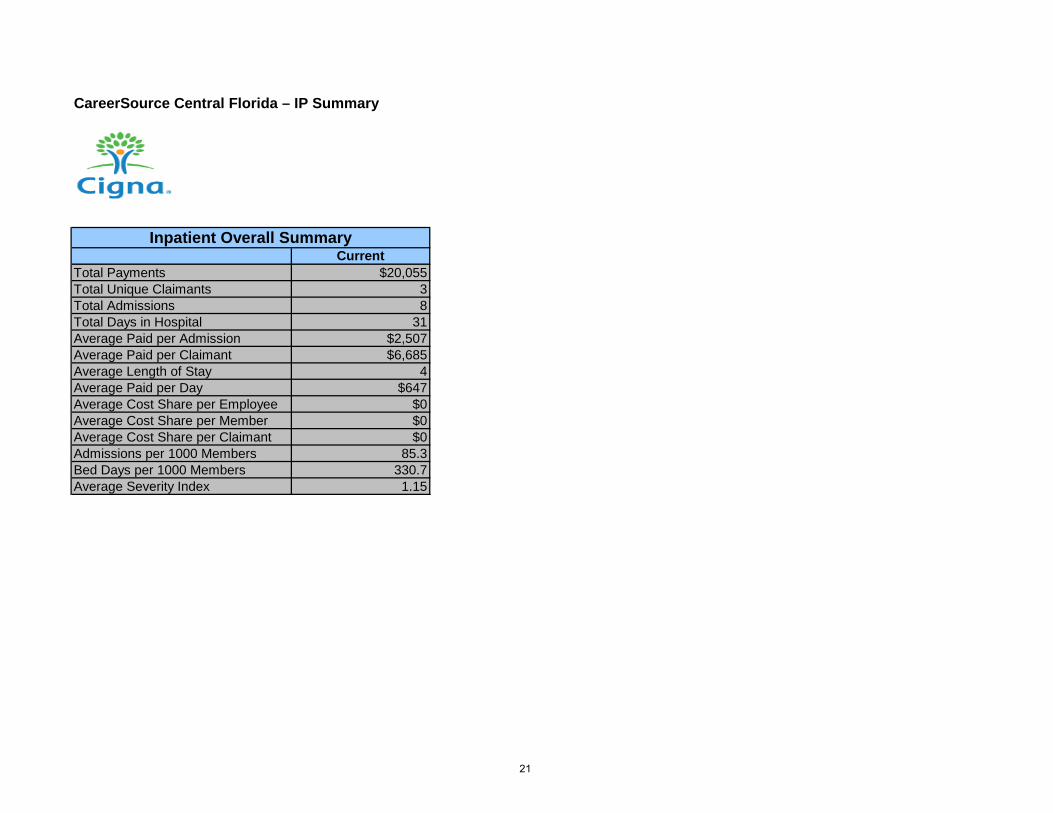
CareerSource Central Florida – IP Summary
CurrentTotal Payments $20,055Total Unique Claimants 3Total Admissions 8Total Days in Hospital 31Average Paid per Admission $2,507Average Paid per Claimant $6,685Average Length of Stay 4Average Paid per Day $647Average Cost Share per Employee $0Average Cost Share per Member $0Average Cost Share per Claimant $0Admissions per 1000 Members 85.3Bed Days per 1000 Members 330.7Average Severity Index 1.15
Inpatient Overall Summary
21
.. --..•~--~-~
Cigna.

CURRENT BENEFITS
..... , ::.f{-: Cigna.
7/1/2015 FL / EHB State: FLHealth Savings Account Open Access Plus - CareerSource Central Florida HSA OAP - 4630917. Version# 5KitTrak: CSW09464
©Cigna 2015
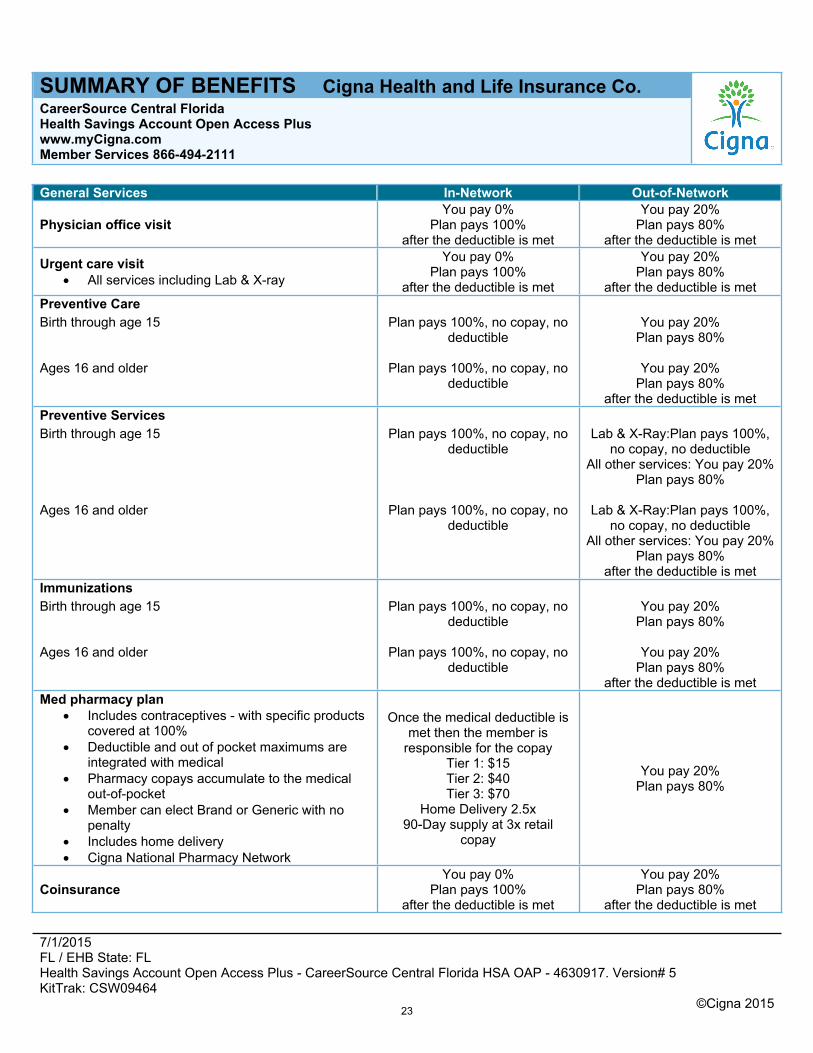
SUMMARY OF BENEFITS Cigna Health and Life Insurance Co.CareerSource Central FloridaHealth Savings Account Open Access Pluswww.myCigna.comMember Services 866-494-2111
General Services In-Network Out-of-Network
Physician office visitYou pay 0%
Plan pays 100%after the deductible is met
You pay 20%Plan pays 80%
after the deductible is met
Urgent care visit All services including Lab & X-ray
You pay 0%Plan pays 100%
after the deductible is met
You pay 20%Plan pays 80%
after the deductible is metPreventive CareBirth through age 15 Plan pays 100%, no copay, no
deductibleYou pay 20%
Plan pays 80%
Ages 16 and older Plan pays 100%, no copay, no deductible
You pay 20%Plan pays 80%
after the deductible is metPreventive ServicesBirth through age 15 Plan pays 100%, no copay, no
deductibleLab & X-Ray:Plan pays 100%,
no copay, no deductibleAll other services: You pay 20%
Plan pays 80%
Ages 16 and older Plan pays 100%, no copay, no deductible
Lab & X-Ray:Plan pays 100%, no copay, no deductible
All other services: You pay 20%Plan pays 80%
after the deductible is metImmunizationsBirth through age 15 Plan pays 100%, no copay, no
deductibleYou pay 20%
Plan pays 80%
Ages 16 and older Plan pays 100%, no copay, no deductible
You pay 20%Plan pays 80%
after the deductible is metMed pharmacy plan
Includes contraceptives - with specific products covered at 100%
Deductible and out of pocket maximums are integrated with medical
Pharmacy copays accumulate to the medical out-of-pocket
Member can elect Brand or Generic with no penalty
Includes home delivery Cigna National Pharmacy Network
Once the medical deductible is met then the member is
responsible for the copayTier 1: $15Tier 2: $40Tier 3: $70
Home Delivery 2.5x90-Day supply at 3x retail
copay
You pay 20%Plan pays 80%
CoinsuranceYou pay 0%
Plan pays 100%after the deductible is met
You pay 20%Plan pays 80%
after the deductible is met
23
7/1/2015 FL / EHB State: FLHealth Savings Account Open Access Plus - CareerSource Central Florida HSA OAP - 4630917. Version# 5KitTrak: CSW09464
©Cigna 2015
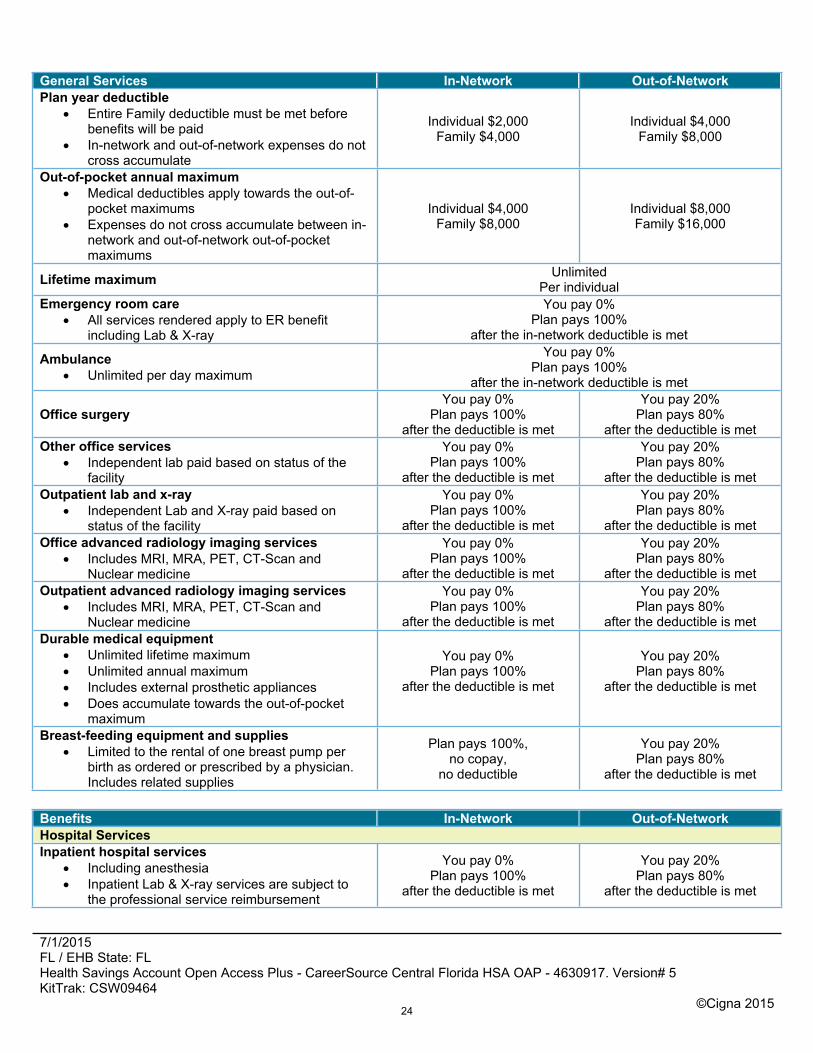
General Services In-Network Out-of-NetworkPlan year deductible
Entire Family deductible must be met before benefits will be paid
In-network and out-of-network expenses do not cross accumulate
Individual $2,000Family $4,000
Individual $4,000Family $8,000
Out-of-pocket annual maximum Medical deductibles apply towards the out-of-
pocket maximums Expenses do not cross accumulate between in-
network and out-of-network out-of-pocket maximums
Individual $4,000Family $8,000
Individual $8,000Family $16,000
Lifetime maximum UnlimitedPer individual
Emergency room care All services rendered apply to ER benefit
including Lab & X-ray
You pay 0%Plan pays 100%
after the in-network deductible is met
Ambulance Unlimited per day maximum
You pay 0%Plan pays 100%
after the in-network deductible is met
Office surgeryYou pay 0%
Plan pays 100%after the deductible is met
You pay 20%Plan pays 80%
after the deductible is metOther office services
Independent lab paid based on status of the facility
You pay 0%Plan pays 100%
after the deductible is met
You pay 20%Plan pays 80%
after the deductible is metOutpatient lab and x-ray
Independent Lab and X-ray paid based on status of the facility
You pay 0%Plan pays 100%
after the deductible is met
You pay 20%Plan pays 80%
after the deductible is metOffice advanced radiology imaging services
Includes MRI, MRA, PET, CT-Scan and Nuclear medicine
You pay 0%Plan pays 100%
after the deductible is met
You pay 20%Plan pays 80%
after the deductible is metOutpatient advanced radiology imaging services
Includes MRI, MRA, PET, CT-Scan and Nuclear medicine
You pay 0%Plan pays 100%
after the deductible is met
You pay 20%Plan pays 80%
after the deductible is metDurable medical equipment
Unlimited lifetime maximum Unlimited annual maximum Includes external prosthetic appliances Does accumulate towards the out-of-pocket
maximum
You pay 0%Plan pays 100%
after the deductible is met
You pay 20%Plan pays 80%
after the deductible is met
Breast-feeding equipment and supplies Limited to the rental of one breast pump per
birth as ordered or prescribed by a physician. Includes related supplies
Plan pays 100%,no copay,
no deductible
You pay 20%Plan pays 80%
after the deductible is met
Benefits In-Network Out-of-NetworkHospital ServicesInpatient hospital services
Including anesthesia Inpatient Lab & X-ray services are subject to
the professional service reimbursement
You pay 0%Plan pays 100%
after the deductible is met
You pay 20%Plan pays 80%
after the deductible is met
24
7/1/2015 FL / EHB State: FLHealth Savings Account Open Access Plus - CareerSource Central Florida HSA OAP - 4630917. Version# 5KitTrak: CSW09464
©Cigna 2015
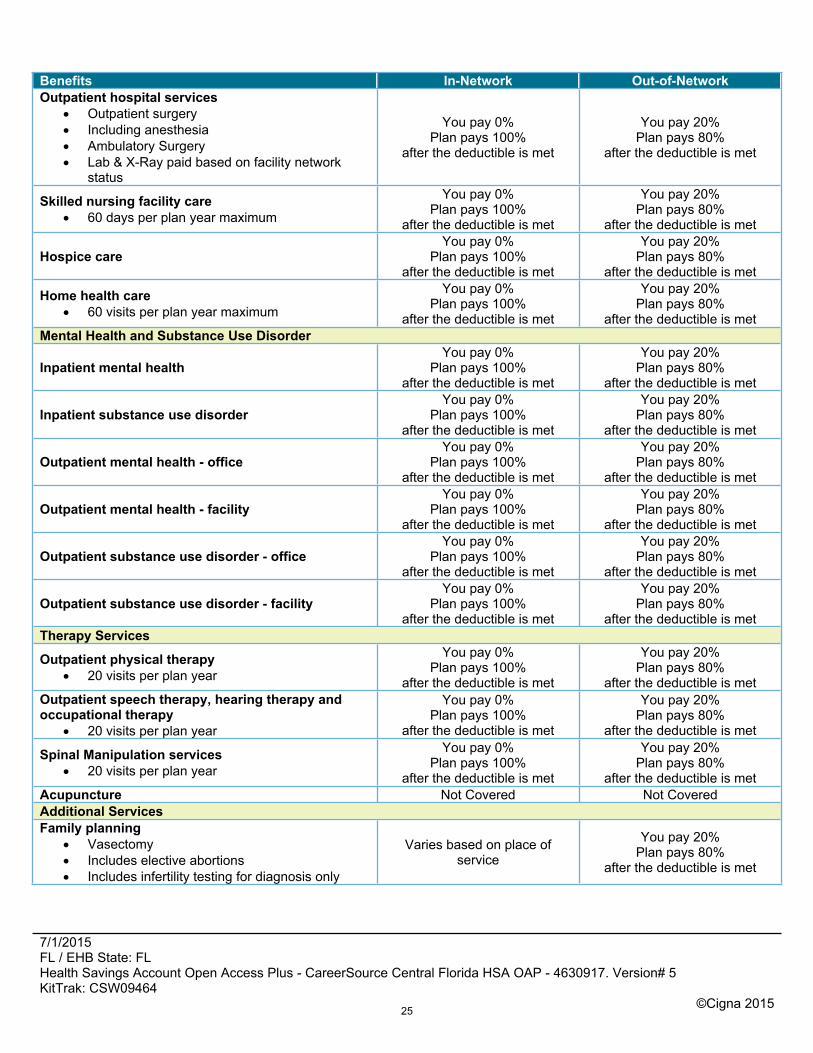
Benefits In-Network Out-of-NetworkOutpatient hospital services
Outpatient surgery Including anesthesia Ambulatory Surgery Lab & X-Ray paid based on facility network
status
You pay 0%Plan pays 100%
after the deductible is met
You pay 20%Plan pays 80%
after the deductible is met
Skilled nursing facility care 60 days per plan year maximum
You pay 0%Plan pays 100%
after the deductible is met
You pay 20%Plan pays 80%
after the deductible is met
Hospice careYou pay 0%
Plan pays 100%after the deductible is met
You pay 20%Plan pays 80%
after the deductible is met
Home health care 60 visits per plan year maximum
You pay 0%Plan pays 100%
after the deductible is met
You pay 20%Plan pays 80%
after the deductible is metMental Health and Substance Use Disorder
Inpatient mental healthYou pay 0%
Plan pays 100%after the deductible is met
You pay 20%Plan pays 80%
after the deductible is met
Inpatient substance use disorderYou pay 0%
Plan pays 100%after the deductible is met
You pay 20%Plan pays 80%
after the deductible is met
Outpatient mental health - officeYou pay 0%
Plan pays 100%after the deductible is met
You pay 20%Plan pays 80%
after the deductible is met
Outpatient mental health - facilityYou pay 0%
Plan pays 100%after the deductible is met
You pay 20%Plan pays 80%
after the deductible is met
Outpatient substance use disorder - officeYou pay 0%
Plan pays 100%after the deductible is met
You pay 20%Plan pays 80%
after the deductible is met
Outpatient substance use disorder - facilityYou pay 0%
Plan pays 100%after the deductible is met
You pay 20%Plan pays 80%
after the deductible is metTherapy Services
Outpatient physical therapy 20 visits per plan year
You pay 0%Plan pays 100%
after the deductible is met
You pay 20%Plan pays 80%
after the deductible is metOutpatient speech therapy, hearing therapy and occupational therapy
20 visits per plan year
You pay 0%Plan pays 100%
after the deductible is met
You pay 20%Plan pays 80%
after the deductible is met
Spinal Manipulation services 20 visits per plan year
You pay 0%Plan pays 100%
after the deductible is met
You pay 20%Plan pays 80%
after the deductible is metAcupuncture Not Covered Not CoveredAdditional ServicesFamily planning
Vasectomy Includes elective abortions Includes infertility testing for diagnosis only
Varies based on place of service
You pay 20%Plan pays 80%
after the deductible is met
25

7/1/2015 FL / EHB State: FLHealth Savings Account Open Access Plus - CareerSource Central Florida HSA OAP - 4630917. Version# 5KitTrak: CSW09464
©Cigna 2015
Benefits In-Network Out-of-NetworkContraceptives
Includes contraceptive devices as ordered or prescribed by a physician
Surgical services such as tubal ligation are covered (excluding reversals)
Physician services
Plan pays 100%, no copay, no deductible
You pay 20%Plan pays 80%
after the deductible is met
TMJ Unlimited plan year maximum for surgical and
non-surgical treatment
You pay 0%Plan pays 100%
after the deductible is met
You pay 20%Plan pays 80%
after the deductible is met
Organ transplant Services paid at network level if performed at
Cigna LifeSOURCE Transplant Network® Facilities
Travel maximum $10,000 per lifetime (only available if using Cigna LifeSOURCE Transplant Network® facility)
You pay 0%Plan pays 100%
after the deductible is met
You pay 20%Plan pays 80%
after the deductible is metwith transplant maximums
Heart - $150,000Liver - $230,000
Bone Marrow - $130,000Kidney - $80,000
Pancreas - $50,000Kidney/Pancreas - $80,000
Heart/Lung - $185,000Lung - $185,000
26
7/1/2015 FL / EHB State: FLHealth Savings Account Open Access Plus - CareerSource Central Florida HSA OAP - 4630917. Version# 5KitTrak: CSW09464
©Cigna 2015
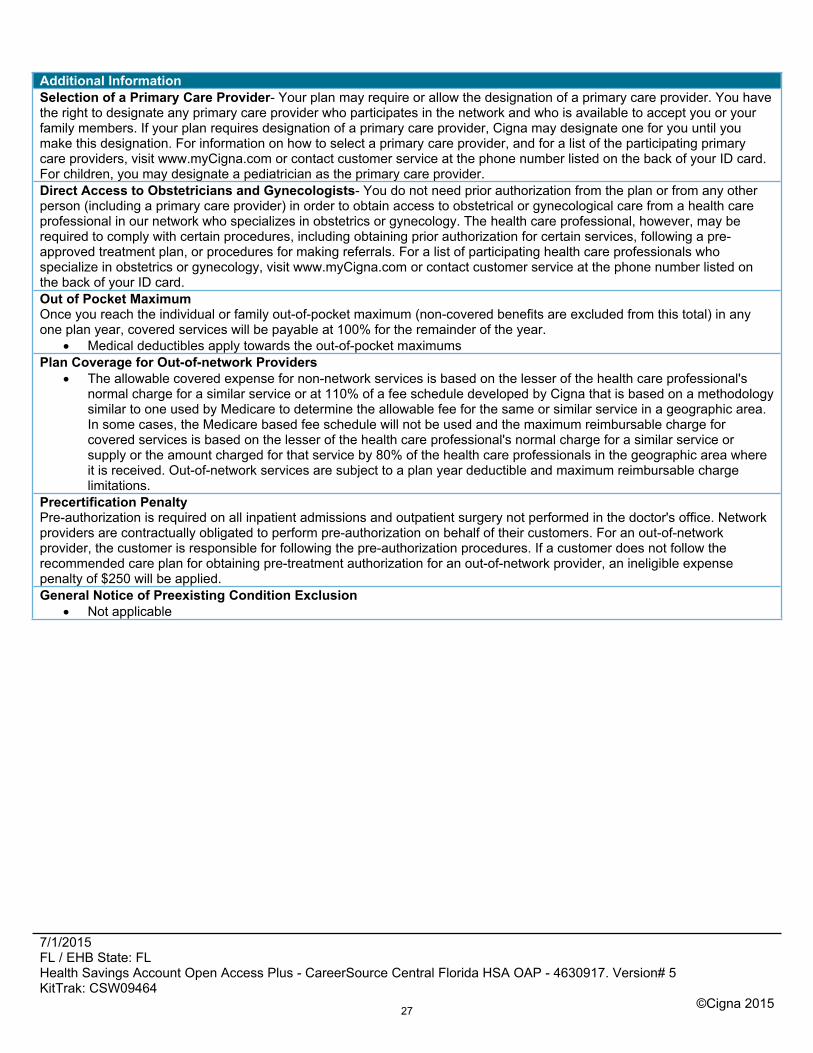
Additional InformationSelection of a Primary Care Provider- Your plan may require or allow the designation of a primary care provider. You have the right to designate any primary care provider who participates in the network and who is available to accept you or your family members. If your plan requires designation of a primary care provider, Cigna may designate one for you until you make this designation. For information on how to select a primary care provider, and for a list of the participating primary care providers, visit www.myCigna.com or contact customer service at the phone number listed on the back of your ID card.For children, you may designate a pediatrician as the primary care provider.Direct Access to Obstetricians and Gynecologists- You do not need prior authorization from the plan or from any other person (including a primary care provider) in order to obtain access to obstetrical or gynecological care from a health care professional in our network who specializes in obstetrics or gynecology. The health care professional, however, may be required to comply with certain procedures, including obtaining prior authorization for certain services, following a pre-approved treatment plan, or procedures for making referrals. For a list of participating health care professionals who specialize in obstetrics or gynecology, visit www.myCigna.com or contact customer service at the phone number listed on the back of your ID card.Out of Pocket MaximumOnce you reach the individual or family out-of-pocket maximum (non-covered benefits are excluded from this total) in any one plan year, covered services will be payable at 100% for the remainder of the year.
Medical deductibles apply towards the out-of-pocket maximumsPlan Coverage for Out-of-network Providers
The allowable covered expense for non-network services is based on the lesser of the health care professional's normal charge for a similar service or at 110% of a fee schedule developed by Cigna that is based on a methodology similar to one used by Medicare to determine the allowable fee for the same or similar service in a geographic area. In some cases, the Medicare based fee schedule will not be used and the maximum reimbursable charge for covered services is based on the lesser of the health care professional's normal charge for a similar service or supply or the amount charged for that service by 80% of the health care professionals in the geographic area where it is received. Out-of-network services are subject to a plan year deductible and maximum reimbursable charge limitations.
Precertification PenaltyPre-authorization is required on all inpatient admissions and outpatient surgery not performed in the doctor's office. Network providers are contractually obligated to perform pre-authorization on behalf of their customers. For an out-of-network provider, the customer is responsible for following the pre-authorization procedures. If a customer does not follow the recommended care plan for obtaining pre-treatment authorization for an out-of-network provider, an ineligible expense penalty of $250 will be applied.General Notice of Preexisting Condition Exclusion
Not applicable
27
7/1/2015 FL / EHB State: FLHealth Savings Account Open Access Plus - CareerSource Central Florida HSA OAP - 4630917. Version# 5KitTrak: CSW09464
©Cigna 2015
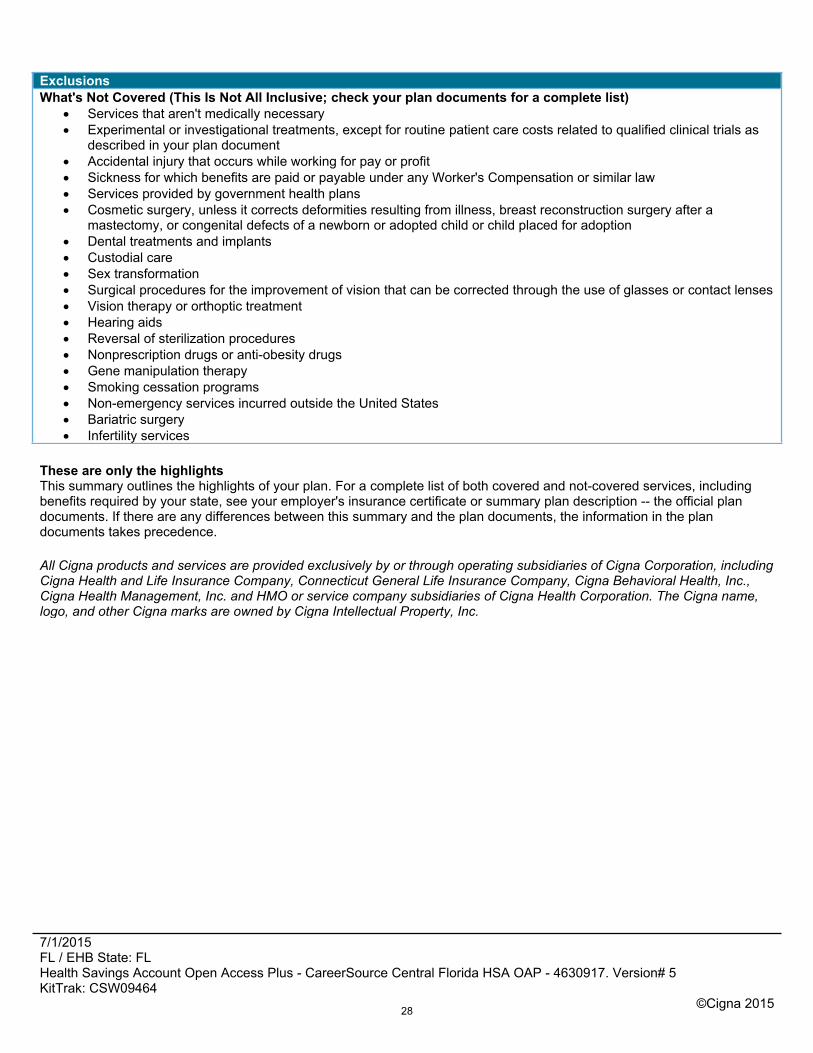
ExclusionsWhat's Not Covered (This Is Not All Inclusive; check your plan documents for a complete list)
Services that aren't medically necessary Experimental or investigational treatments, except for routine patient care costs related to qualified clinical trials as
described in your plan document Accidental injury that occurs while working for pay or profit Sickness for which benefits are paid or payable under any Worker's Compensation or similar law Services provided by government health plans Cosmetic surgery, unless it corrects deformities resulting from illness, breast reconstruction surgery after a
mastectomy, or congenital defects of a newborn or adopted child or child placed for adoption Dental treatments and implants Custodial care Sex transformation Surgical procedures for the improvement of vision that can be corrected through the use of glasses or contact lenses Vision therapy or orthoptic treatment Hearing aids Reversal of sterilization procedures Nonprescription drugs or anti-obesity drugs Gene manipulation therapy Smoking cessation programs Non-emergency services incurred outside the United States Bariatric surgery Infertility services
These are only the highlightsThis summary outlines the highlights of your plan. For a complete list of both covered and not-covered services, including benefits required by your state, see your employer's insurance certificate or summary plan description -- the official plan documents. If there are any differences between this summary and the plan documents, the information in the plan documents takes precedence.
All Cigna products and services are provided exclusively by or through operating subsidiaries of Cigna Corporation, including Cigna Health and Life Insurance Company, Connecticut General Life Insurance Company, Cigna Behavioral Health, Inc., Cigna Health Management, Inc. and HMO or service company subsidiaries of Cigna Health Corporation. The Cigna name, logo, and other Cigna marks are owned by Cigna Intellectual Property, Inc.
28
7/1/2015 FL / EHB State: FLOpen Access Plus - CareerSource Central Florida OAP Base - 4630912. Version# 5KitTrak: CSW09465
©Cigna 2015
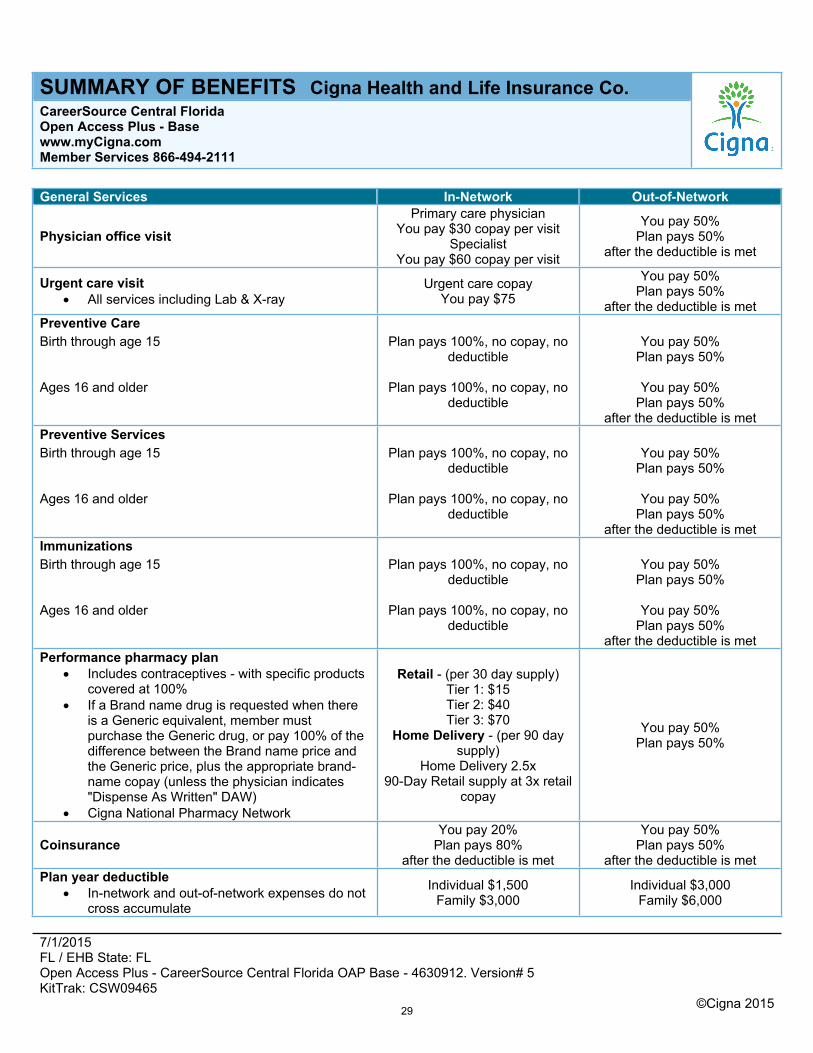
SUMMARY OF BENEFITS Cigna Health and Life Insurance Co.CareerSource Central Florida Open Access Plus - Basewww.myCigna.comMember Services 866-494-2111
General Services In-Network Out-of-Network
Physician office visitPrimary care physician
You pay $30 copay per visitSpecialist
You pay $60 copay per visit
You pay 50%Plan pays 50%
after the deductible is met
Urgent care visit All services including Lab & X-ray
Urgent care copayYou pay $75
You pay 50%Plan pays 50%
after the deductible is metPreventive CareBirth through age 15 Plan pays 100%, no copay, no
deductibleYou pay 50%
Plan pays 50%
Ages 16 and older Plan pays 100%, no copay, no deductible
You pay 50%Plan pays 50%
after the deductible is metPreventive ServicesBirth through age 15 Plan pays 100%, no copay, no
deductibleYou pay 50%
Plan pays 50%
Ages 16 and older Plan pays 100%, no copay, no deductible
You pay 50%Plan pays 50%
after the deductible is metImmunizationsBirth through age 15 Plan pays 100%, no copay, no
deductibleYou pay 50%
Plan pays 50%
Ages 16 and older Plan pays 100%, no copay, no deductible
You pay 50%Plan pays 50%
after the deductible is metPerformance pharmacy plan
Includes contraceptives - with specific products covered at 100%
If a Brand name drug is requested when there is a Generic equivalent, member must purchase the Generic drug, or pay 100% of the difference between the Brand name price and the Generic price, plus the appropriate brand-name copay (unless the physician indicates "Dispense As Written" DAW)
Cigna National Pharmacy Network
Retail - (per 30 day supply)Tier 1: $15Tier 2: $40Tier 3: $70
Home Delivery - (per 90 day supply)
Home Delivery 2.5x90-Day Retail supply at 3x retail
copay
You pay 50%Plan pays 50%
CoinsuranceYou pay 20%
Plan pays 80%after the deductible is met
You pay 50%Plan pays 50%
after the deductible is metPlan year deductible
In-network and out-of-network expenses do not cross accumulate
Individual $1,500Family $3,000
Individual $3,000Family $6,000
29
7/1/2015 FL / EHB State: FLOpen Access Plus - CareerSource Central Florida OAP Base - 4630912. Version# 5KitTrak: CSW09465
©Cigna 2015
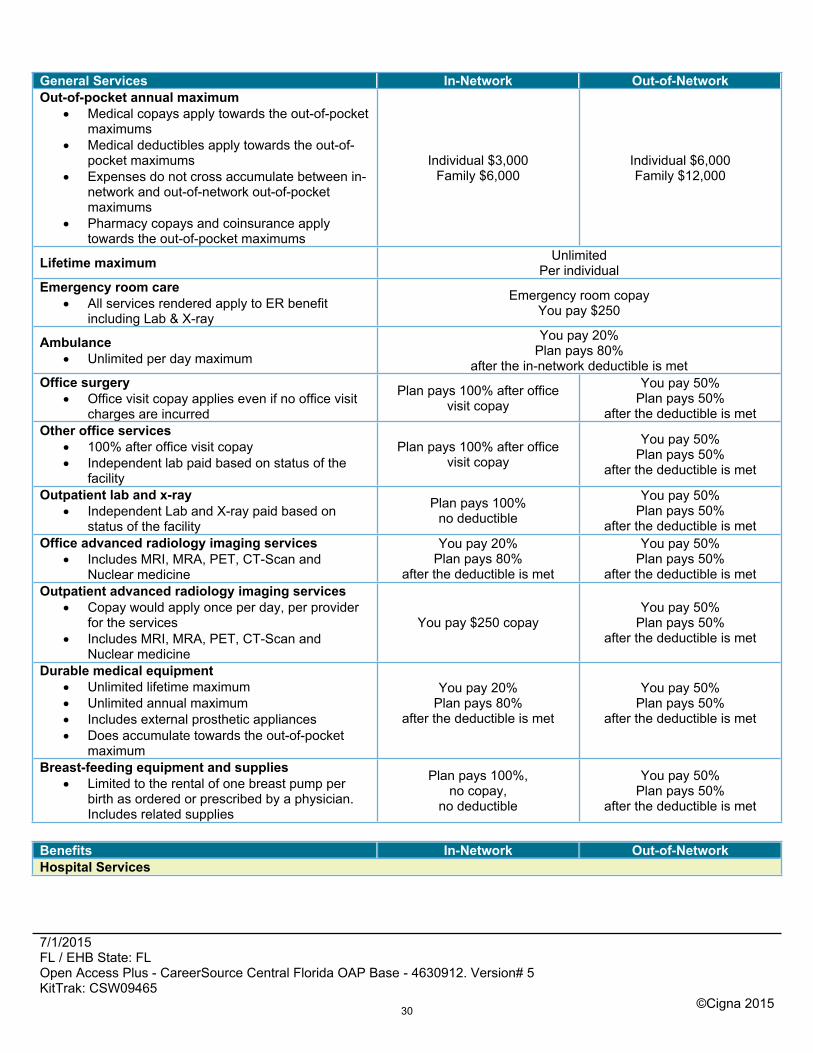
General Services In-Network Out-of-NetworkOut-of-pocket annual maximum
Medical copays apply towards the out-of-pocket maximums
Medical deductibles apply towards the out-of-pocket maximums
Expenses do not cross accumulate between in-network and out-of-network out-of-pocket maximums
Pharmacy copays and coinsurance apply towards the out-of-pocket maximums
Individual $3,000Family $6,000
Individual $6,000Family $12,000
Lifetime maximum UnlimitedPer individual
Emergency room care All services rendered apply to ER benefit
including Lab & X-ray
Emergency room copayYou pay $250
Ambulance Unlimited per day maximum
You pay 20%Plan pays 80%
after the in-network deductible is metOffice surgery
Office visit copay applies even if no office visit charges are incurred
Plan pays 100% after office visit copay
You pay 50%Plan pays 50%
after the deductible is metOther office services
100% after office visit copay Independent lab paid based on status of the
facility
Plan pays 100% after office visit copay
You pay 50%Plan pays 50%
after the deductible is met
Outpatient lab and x-ray Independent Lab and X-ray paid based on
status of the facility
Plan pays 100%no deductible
You pay 50%Plan pays 50%
after the deductible is metOffice advanced radiology imaging services
Includes MRI, MRA, PET, CT-Scan and Nuclear medicine
You pay 20%Plan pays 80%
after the deductible is met
You pay 50%Plan pays 50%
after the deductible is metOutpatient advanced radiology imaging services
Copay would apply once per day, per provider for the services
Includes MRI, MRA, PET, CT-Scan and Nuclear medicine
You pay $250 copayYou pay 50%
Plan pays 50%after the deductible is met
Durable medical equipment Unlimited lifetime maximum Unlimited annual maximum Includes external prosthetic appliances Does accumulate towards the out-of-pocket
maximum
You pay 20%Plan pays 80%
after the deductible is met
You pay 50%Plan pays 50%
after the deductible is met
Breast-feeding equipment and supplies Limited to the rental of one breast pump per
birth as ordered or prescribed by a physician. Includes related supplies
Plan pays 100%,no copay,
no deductible
You pay 50%Plan pays 50%
after the deductible is met
Benefits In-Network Out-of-NetworkHospital Services
30
7/1/2015 FL / EHB State: FLOpen Access Plus - CareerSource Central Florida OAP Base - 4630912. Version# 5KitTrak: CSW09465
©Cigna 2015
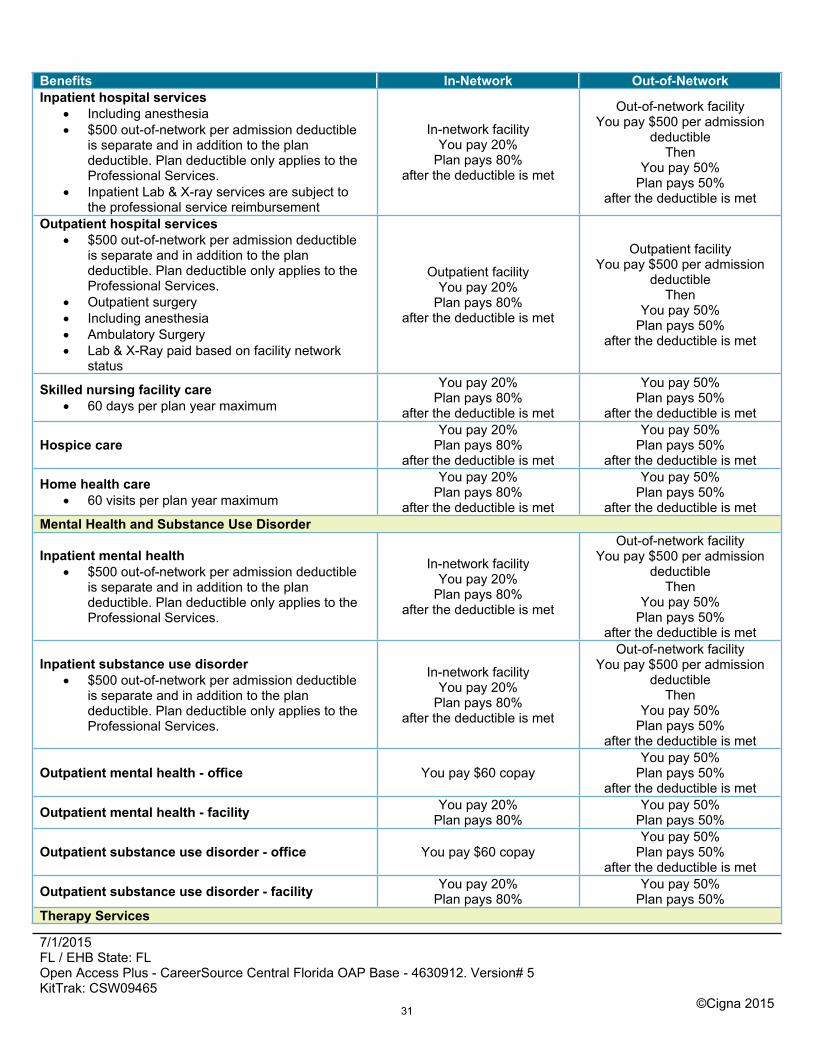
Benefits In-Network Out-of-NetworkInpatient hospital services
Including anesthesia $500 out-of-network per admission deductible
is separate and in addition to the plan deductible. Plan deductible only applies to the Professional Services.
Inpatient Lab & X-ray services are subject to the professional service reimbursement
In-network facilityYou pay 20%
Plan pays 80%after the deductible is met
Out-of-network facilityYou pay $500 per admission
deductibleThen
You pay 50%Plan pays 50%
after the deductible is met
Outpatient hospital services $500 out-of-network per admission deductible
is separate and in addition to the plan deductible. Plan deductible only applies to the Professional Services.
Outpatient surgery Including anesthesia Ambulatory Surgery Lab & X-Ray paid based on facility network
status
Outpatient facilityYou pay 20%
Plan pays 80%after the deductible is met
Outpatient facilityYou pay $500 per admission
deductibleThen
You pay 50%Plan pays 50%
after the deductible is met
Skilled nursing facility care 60 days per plan year maximum
You pay 20%Plan pays 80%
after the deductible is met
You pay 50%Plan pays 50%
after the deductible is met
Hospice careYou pay 20%
Plan pays 80%after the deductible is met
You pay 50%Plan pays 50%
after the deductible is met
Home health care 60 visits per plan year maximum
You pay 20%Plan pays 80%
after the deductible is met
You pay 50%Plan pays 50%
after the deductible is metMental Health and Substance Use Disorder
Inpatient mental health $500 out-of-network per admission deductible
is separate and in addition to the plan deductible. Plan deductible only applies to the Professional Services.
In-network facilityYou pay 20%
Plan pays 80%after the deductible is met
Out-of-network facilityYou pay $500 per admission
deductibleThen
You pay 50%Plan pays 50%
after the deductible is met
Inpatient substance use disorder $500 out-of-network per admission deductible
is separate and in addition to the plan deductible. Plan deductible only applies to the Professional Services.
In-network facilityYou pay 20%
Plan pays 80%after the deductible is met
Out-of-network facilityYou pay $500 per admission
deductibleThen
You pay 50%Plan pays 50%
after the deductible is met
Outpatient mental health - office You pay $60 copayYou pay 50%
Plan pays 50%after the deductible is met
Outpatient mental health - facility You pay 20%Plan pays 80%
You pay 50%Plan pays 50%
Outpatient substance use disorder - office You pay $60 copayYou pay 50%
Plan pays 50%after the deductible is met
Outpatient substance use disorder - facility You pay 20%Plan pays 80%
You pay 50%Plan pays 50%
Therapy Services
31
7/1/2015 FL / EHB State: FLOpen Access Plus - CareerSource Central Florida OAP Base - 4630912. Version# 5KitTrak: CSW09465
©Cigna 2015
Benefits In-Network Out-of-Network
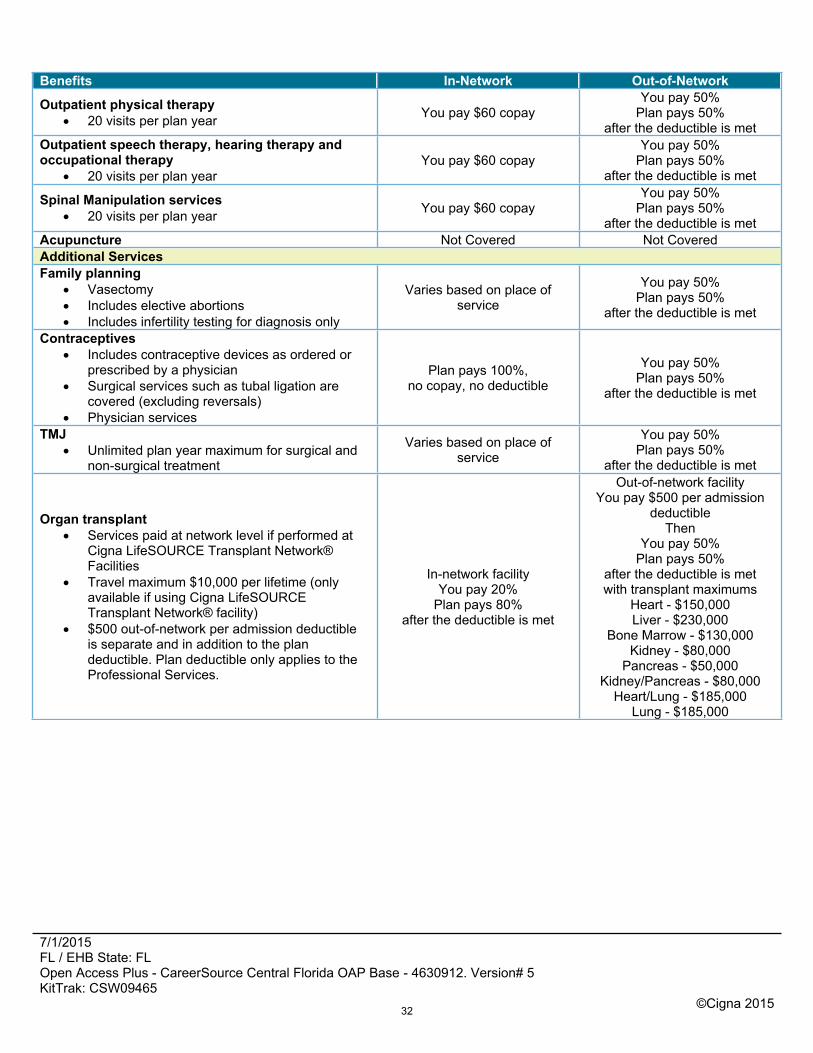
Outpatient physical therapy 20 visits per plan year You pay $60 copay
You pay 50%Plan pays 50%
after the deductible is metOutpatient speech therapy, hearing therapy and occupational therapy
20 visits per plan yearYou pay $60 copay
You pay 50%Plan pays 50%
after the deductible is met
Spinal Manipulation services 20 visits per plan year You pay $60 copay
You pay 50%Plan pays 50%
after the deductible is metAcupuncture Not Covered Not CoveredAdditional ServicesFamily planning
Vasectomy Includes elective abortions Includes infertility testing for diagnosis only
Varies based on place of service
You pay 50%Plan pays 50%
after the deductible is met
Contraceptives Includes contraceptive devices as ordered or
prescribed by a physician Surgical services such as tubal ligation are
covered (excluding reversals) Physician services
Plan pays 100%,no copay, no deductible
You pay 50%Plan pays 50%
after the deductible is met
TMJ Unlimited plan year maximum for surgical and
non-surgical treatment
Varies based on place of service
You pay 50%Plan pays 50%
after the deductible is met
Organ transplant Services paid at network level if performed at
Cigna LifeSOURCE Transplant Network® Facilities
Travel maximum $10,000 per lifetime (only available if using Cigna LifeSOURCE Transplant Network® facility)
$500 out-of-network per admission deductible is separate and in addition to the plan deductible. Plan deductible only applies to the Professional Services.
In-network facilityYou pay 20%
Plan pays 80%after the deductible is met
Out-of-network facilityYou pay $500 per admission
deductibleThen
You pay 50%Plan pays 50%
after the deductible is metwith transplant maximums
Heart - $150,000Liver - $230,000
Bone Marrow - $130,000Kidney - $80,000
Pancreas - $50,000Kidney/Pancreas - $80,000
Heart/Lung - $185,000Lung - $185,000
32
7/1/2015 FL / EHB State: FLOpen Access Plus - CareerSource Central Florida OAP Base - 4630912. Version# 5KitTrak: CSW09465
©Cigna 2015
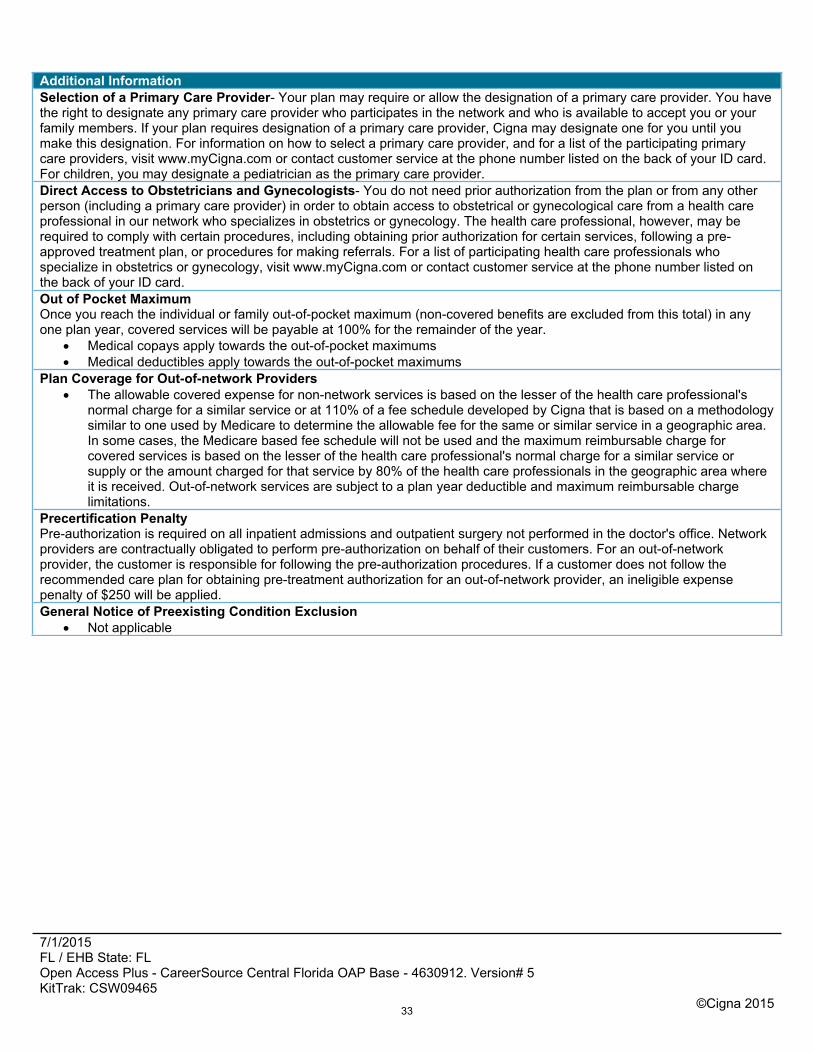
Additional InformationSelection of a Primary Care Provider- Your plan may require or allow the designation of a primary care provider. You have the right to designate any primary care provider who participates in the network and who is available to accept you or your family members. If your plan requires designation of a primary care provider, Cigna may designate one for you until you make this designation. For information on how to select a primary care provider, and for a list of the participating primary care providers, visit www.myCigna.com or contact customer service at the phone number listed on the back of your ID card.For children, you may designate a pediatrician as the primary care provider.Direct Access to Obstetricians and Gynecologists- You do not need prior authorization from the plan or from any other person (including a primary care provider) in order to obtain access to obstetrical or gynecological care from a health care professional in our network who specializes in obstetrics or gynecology. The health care professional, however, may be required to comply with certain procedures, including obtaining prior authorization for certain services, following a pre-approved treatment plan, or procedures for making referrals. For a list of participating health care professionals who specialize in obstetrics or gynecology, visit www.myCigna.com or contact customer service at the phone number listed on the back of your ID card.Out of Pocket MaximumOnce you reach the individual or family out-of-pocket maximum (non-covered benefits are excluded from this total) in any one plan year, covered services will be payable at 100% for the remainder of the year.
Medical copays apply towards the out-of-pocket maximums Medical deductibles apply towards the out-of-pocket maximums
Plan Coverage for Out-of-network Providers The allowable covered expense for non-network services is based on the lesser of the health care professional's
normal charge for a similar service or at 110% of a fee schedule developed by Cigna that is based on a methodology similar to one used by Medicare to determine the allowable fee for the same or similar service in a geographic area. In some cases, the Medicare based fee schedule will not be used and the maximum reimbursable charge for covered services is based on the lesser of the health care professional's normal charge for a similar service or supply or the amount charged for that service by 80% of the health care professionals in the geographic area where it is received. Out-of-network services are subject to a plan year deductible and maximum reimbursable charge limitations.
Precertification PenaltyPre-authorization is required on all inpatient admissions and outpatient surgery not performed in the doctor's office. Network providers are contractually obligated to perform pre-authorization on behalf of their customers. For an out-of-network provider, the customer is responsible for following the pre-authorization procedures. If a customer does not follow the recommended care plan for obtaining pre-treatment authorization for an out-of-network provider, an ineligible expense penalty of $250 will be applied.General Notice of Preexisting Condition Exclusion
Not applicable
33
7/1/2015 FL / EHB State: FLOpen Access Plus - CareerSource Central Florida OAP Base - 4630912. Version# 5KitTrak: CSW09465
©Cigna 2015
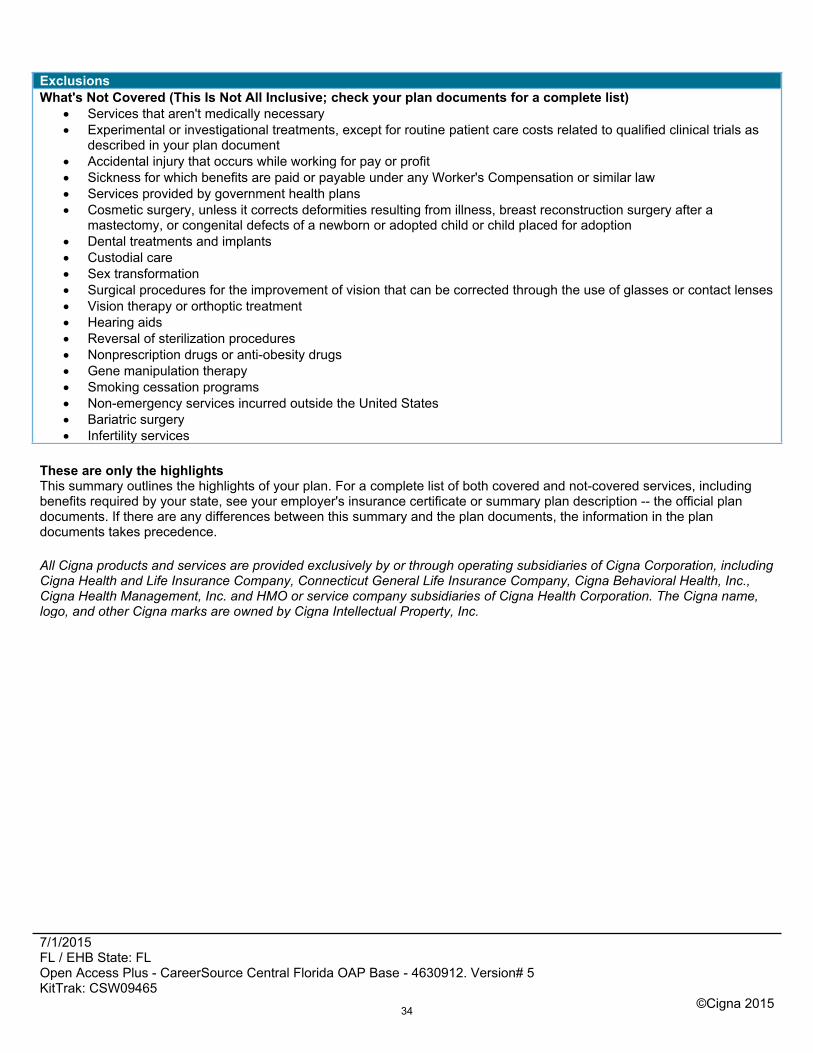
ExclusionsWhat's Not Covered (This Is Not All Inclusive; check your plan documents for a complete list)
Services that aren't medically necessary Experimental or investigational treatments, except for routine patient care costs related to qualified clinical trials as
described in your plan document Accidental injury that occurs while working for pay or profit Sickness for which benefits are paid or payable under any Worker's Compensation or similar law Services provided by government health plans Cosmetic surgery, unless it corrects deformities resulting from illness, breast reconstruction surgery after a
mastectomy, or congenital defects of a newborn or adopted child or child placed for adoption Dental treatments and implants Custodial care Sex transformation Surgical procedures for the improvement of vision that can be corrected through the use of glasses or contact lenses Vision therapy or orthoptic treatment Hearing aids Reversal of sterilization procedures Nonprescription drugs or anti-obesity drugs Gene manipulation therapy Smoking cessation programs Non-emergency services incurred outside the United States Bariatric surgery Infertility services
These are only the highlightsThis summary outlines the highlights of your plan. For a complete list of both covered and not-covered services, including benefits required by your state, see your employer's insurance certificate or summary plan description -- the official plan documents. If there are any differences between this summary and the plan documents, the information in the plan documents takes precedence.
All Cigna products and services are provided exclusively by or through operating subsidiaries of Cigna Corporation, including Cigna Health and Life Insurance Company, Connecticut General Life Insurance Company, Cigna Behavioral Health, Inc., Cigna Health Management, Inc. and HMO or service company subsidiaries of Cigna Health Corporation. The Cigna name, logo, and other Cigna marks are owned by Cigna Intellectual Property, Inc.
34
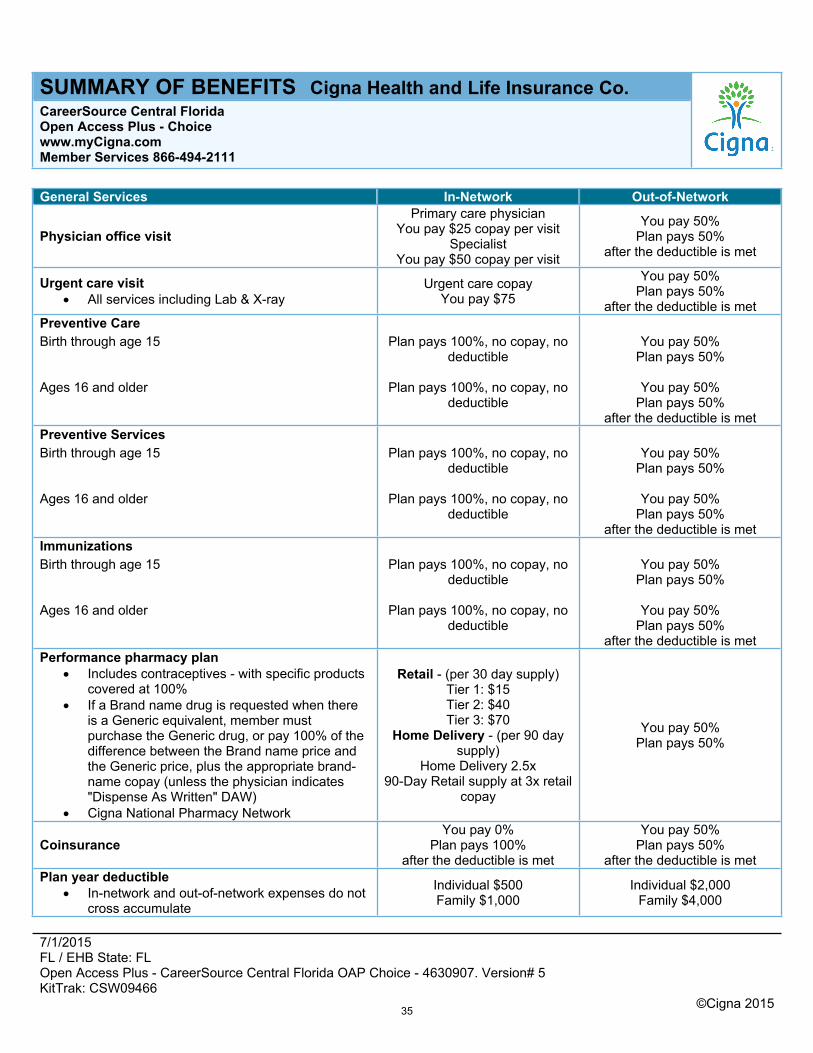
7/1/2015 FL / EHB State: FLOpen Access Plus - CareerSource Central Florida OAP Choice - 4630907. Version# 5KitTrak: CSW09466
©Cigna 2015
SUMMARY OF BENEFITS Cigna Health and Life Insurance Co.CareerSource Central Florida Open Access Plus - Choicewww.myCigna.comMember Services 866-494-2111
General Services In-Network Out-of-Network
Physician office visitPrimary care physician
You pay $25 copay per visitSpecialist
You pay $50 copay per visit
You pay 50%Plan pays 50%
after the deductible is met
Urgent care visit All services including Lab & X-ray
Urgent care copayYou pay $75
You pay 50%Plan pays 50%
after the deductible is metPreventive CareBirth through age 15 Plan pays 100%, no copay, no
deductibleYou pay 50%
Plan pays 50%
Ages 16 and older Plan pays 100%, no copay, no deductible
You pay 50%Plan pays 50%
after the deductible is metPreventive ServicesBirth through age 15 Plan pays 100%, no copay, no
deductibleYou pay 50%
Plan pays 50%
Ages 16 and older Plan pays 100%, no copay, no deductible
You pay 50%Plan pays 50%
after the deductible is metImmunizationsBirth through age 15 Plan pays 100%, no copay, no
deductibleYou pay 50%
Plan pays 50%
Ages 16 and older Plan pays 100%, no copay, no deductible
You pay 50%Plan pays 50%
after the deductible is metPerformance pharmacy plan
Includes contraceptives - with specific products covered at 100%
If a Brand name drug is requested when there is a Generic equivalent, member must purchase the Generic drug, or pay 100% of the difference between the Brand name price and the Generic price, plus the appropriate brand-name copay (unless the physician indicates "Dispense As Written" DAW)
Cigna National Pharmacy Network
Retail - (per 30 day supply)Tier 1: $15Tier 2: $40Tier 3: $70
Home Delivery - (per 90 day supply)
Home Delivery 2.5x90-Day Retail supply at 3x retail
copay
You pay 50%Plan pays 50%
CoinsuranceYou pay 0%
Plan pays 100%after the deductible is met
You pay 50%Plan pays 50%
after the deductible is metPlan year deductible
In-network and out-of-network expenses do not cross accumulate
Individual $500Family $1,000
Individual $2,000Family $4,000
35
7/1/2015 FL / EHB State: FLOpen Access Plus - CareerSource Central Florida OAP Choice - 4630907. Version# 5KitTrak: CSW09466
©Cigna 2015
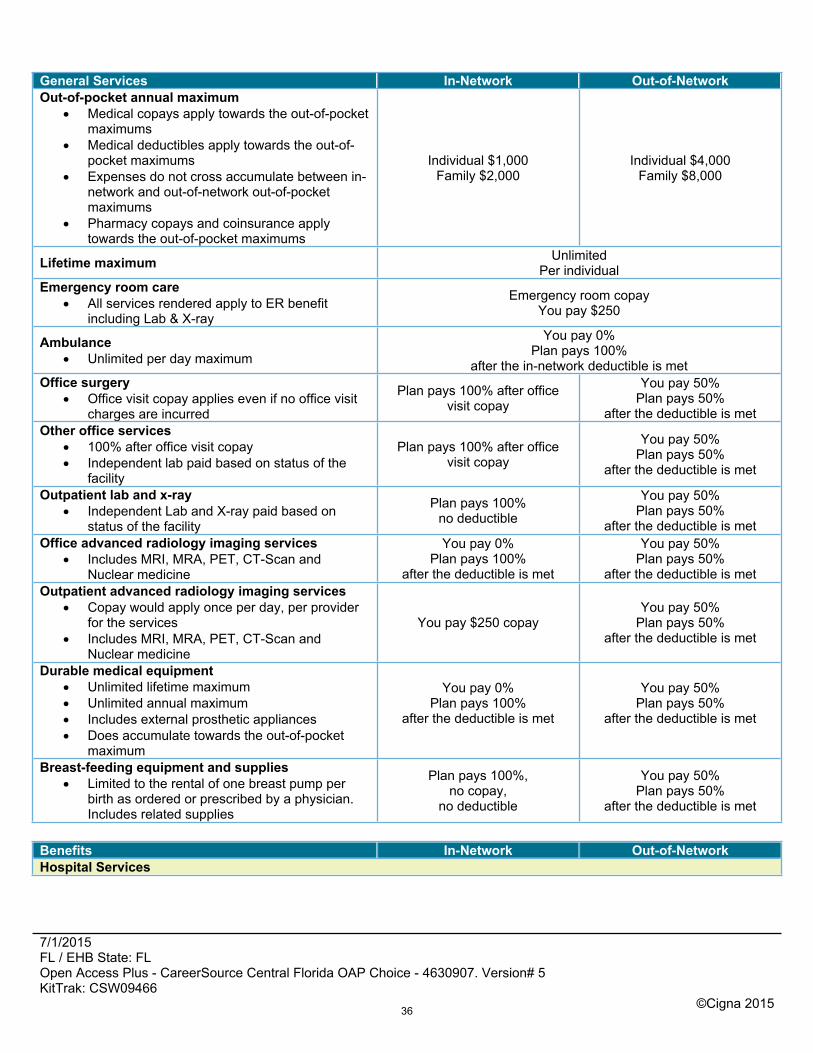
General Services In-Network Out-of-NetworkOut-of-pocket annual maximum
Medical copays apply towards the out-of-pocket maximums
Medical deductibles apply towards the out-of-pocket maximums
Expenses do not cross accumulate between in-network and out-of-network out-of-pocket maximums
Pharmacy copays and coinsurance apply towards the out-of-pocket maximums
Individual $1,000Family $2,000
Individual $4,000Family $8,000
Lifetime maximum UnlimitedPer individual
Emergency room care All services rendered apply to ER benefit
including Lab & X-ray
Emergency room copayYou pay $250
Ambulance Unlimited per day maximum
You pay 0%Plan pays 100%
after the in-network deductible is metOffice surgery
Office visit copay applies even if no office visit charges are incurred
Plan pays 100% after office visit copay
You pay 50%Plan pays 50%
after the deductible is metOther office services
100% after office visit copay Independent lab paid based on status of the
facility
Plan pays 100% after office visit copay
You pay 50%Plan pays 50%
after the deductible is met
Outpatient lab and x-ray Independent Lab and X-ray paid based on
status of the facility
Plan pays 100%no deductible
You pay 50%Plan pays 50%
after the deductible is metOffice advanced radiology imaging services
Includes MRI, MRA, PET, CT-Scan and Nuclear medicine
You pay 0%Plan pays 100%
after the deductible is met
You pay 50%Plan pays 50%
after the deductible is metOutpatient advanced radiology imaging services
Copay would apply once per day, per provider for the services
Includes MRI, MRA, PET, CT-Scan and Nuclear medicine
You pay $250 copayYou pay 50%
Plan pays 50%after the deductible is met
Durable medical equipment Unlimited lifetime maximum Unlimited annual maximum Includes external prosthetic appliances Does accumulate towards the out-of-pocket
maximum
You pay 0%Plan pays 100%
after the deductible is met
You pay 50%Plan pays 50%
after the deductible is met
Breast-feeding equipment and supplies Limited to the rental of one breast pump per
birth as ordered or prescribed by a physician. Includes related supplies
Plan pays 100%,no copay,
no deductible
You pay 50%Plan pays 50%
after the deductible is met
Benefits In-Network Out-of-NetworkHospital Services
36
7/1/2015 FL / EHB State: FLOpen Access Plus - CareerSource Central Florida OAP Choice - 4630907. Version# 5KitTrak: CSW09466
©Cigna 2015
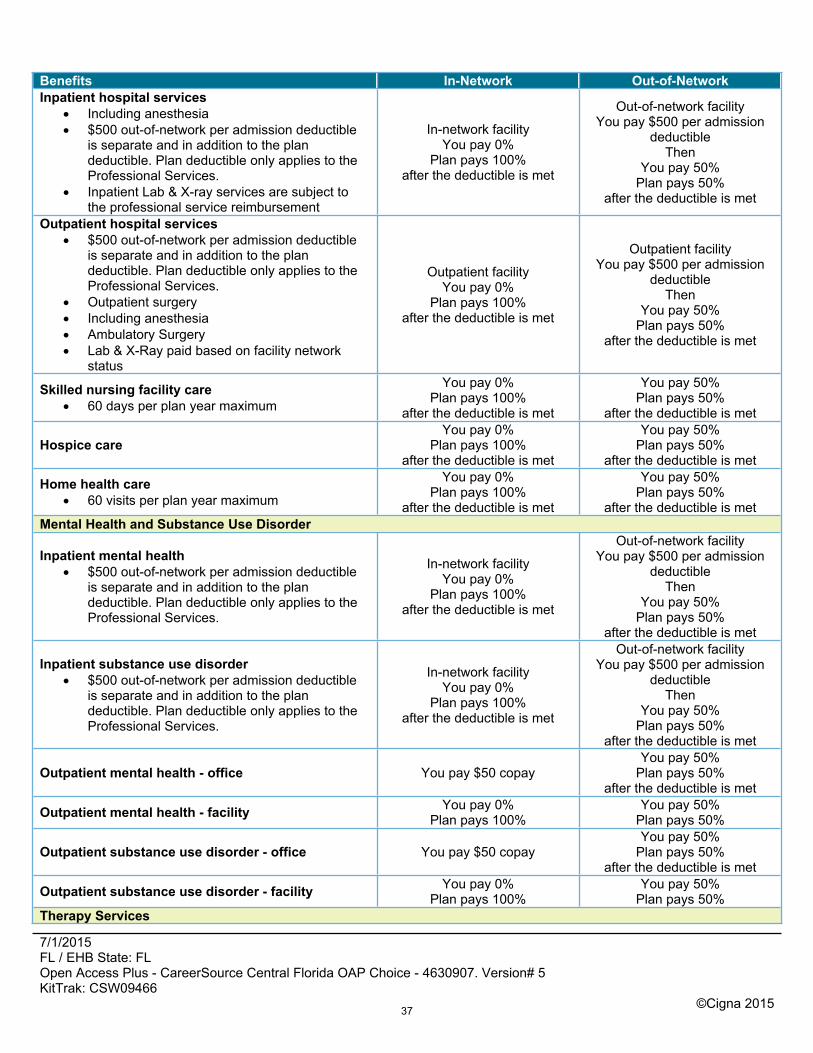
Benefits In-Network Out-of-NetworkInpatient hospital services
Including anesthesia $500 out-of-network per admission deductible
is separate and in addition to the plan deductible. Plan deductible only applies to the Professional Services.
Inpatient Lab & X-ray services are subject to the professional service reimbursement
In-network facilityYou pay 0%
Plan pays 100%after the deductible is met
Out-of-network facilityYou pay $500 per admission
deductibleThen
You pay 50%Plan pays 50%
after the deductible is met
Outpatient hospital services $500 out-of-network per admission deductible
is separate and in addition to the plan deductible. Plan deductible only applies to the Professional Services.
Outpatient surgery Including anesthesia Ambulatory Surgery Lab & X-Ray paid based on facility network
status
Outpatient facilityYou pay 0%
Plan pays 100%after the deductible is met
Outpatient facilityYou pay $500 per admission
deductibleThen
You pay 50%Plan pays 50%
after the deductible is met
Skilled nursing facility care 60 days per plan year maximum
You pay 0%Plan pays 100%
after the deductible is met
You pay 50%Plan pays 50%
after the deductible is met
Hospice careYou pay 0%
Plan pays 100%after the deductible is met
You pay 50%Plan pays 50%
after the deductible is met
Home health care 60 visits per plan year maximum
You pay 0%Plan pays 100%
after the deductible is met
You pay 50%Plan pays 50%
after the deductible is metMental Health and Substance Use Disorder
Inpatient mental health $500 out-of-network per admission deductible
is separate and in addition to the plan deductible. Plan deductible only applies to the Professional Services.
In-network facilityYou pay 0%
Plan pays 100%after the deductible is met
Out-of-network facilityYou pay $500 per admission
deductibleThen
You pay 50%Plan pays 50%
after the deductible is met
Inpatient substance use disorder $500 out-of-network per admission deductible
is separate and in addition to the plan deductible. Plan deductible only applies to the Professional Services.
In-network facilityYou pay 0%
Plan pays 100%after the deductible is met
Out-of-network facilityYou pay $500 per admission
deductibleThen
You pay 50%Plan pays 50%
after the deductible is met
Outpatient mental health - office You pay $50 copayYou pay 50%
Plan pays 50%after the deductible is met
Outpatient mental health - facility You pay 0%Plan pays 100%
You pay 50%Plan pays 50%
Outpatient substance use disorder - office You pay $50 copayYou pay 50%
Plan pays 50%after the deductible is met
Outpatient substance use disorder - facility You pay 0%Plan pays 100%
You pay 50%Plan pays 50%
Therapy Services
37
7/1/2015 FL / EHB State: FLOpen Access Plus - CareerSource Central Florida OAP Choice - 4630907. Version# 5KitTrak: CSW09466
©Cigna 2015
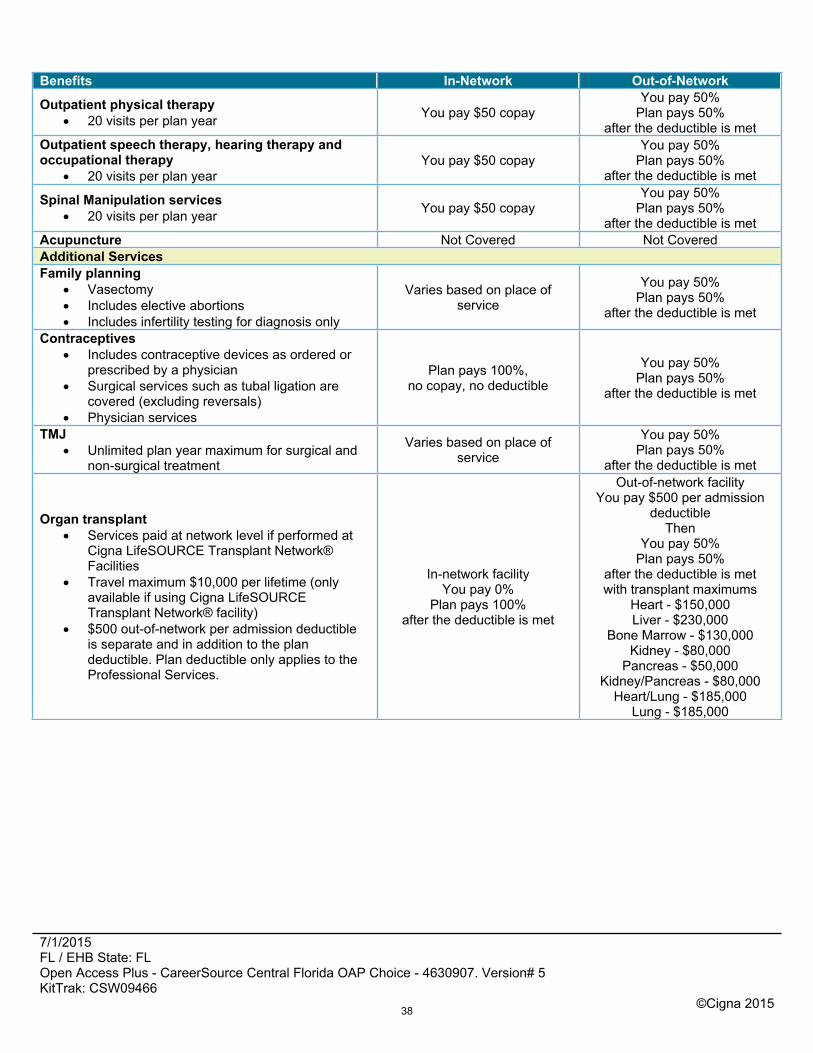
Benefits In-Network Out-of-Network
Outpatient physical therapy 20 visits per plan year You pay $50 copay
You pay 50%Plan pays 50%
after the deductible is metOutpatient speech therapy, hearing therapy and occupational therapy
20 visits per plan yearYou pay $50 copay
You pay 50%Plan pays 50%
after the deductible is met
Spinal Manipulation services 20 visits per plan year You pay $50 copay
You pay 50%Plan pays 50%
after the deductible is metAcupuncture Not Covered Not CoveredAdditional ServicesFamily planning
Vasectomy Includes elective abortions Includes infertility testing for diagnosis only
Varies based on place of service
You pay 50%Plan pays 50%
after the deductible is met
Contraceptives Includes contraceptive devices as ordered or
prescribed by a physician Surgical services such as tubal ligation are
covered (excluding reversals) Physician services
Plan pays 100%,no copay, no deductible
You pay 50%Plan pays 50%
after the deductible is met
TMJ Unlimited plan year maximum for surgical and
non-surgical treatment
Varies based on place of service
You pay 50%Plan pays 50%
after the deductible is met
Organ transplant Services paid at network level if performed at
Cigna LifeSOURCE Transplant Network® Facilities
Travel maximum $10,000 per lifetime (only available if using Cigna LifeSOURCE Transplant Network® facility)
$500 out-of-network per admission deductible is separate and in addition to the plan deductible. Plan deductible only applies to the Professional Services.
In-network facilityYou pay 0%
Plan pays 100%after the deductible is met
Out-of-network facilityYou pay $500 per admission
deductibleThen
You pay 50%Plan pays 50%
after the deductible is metwith transplant maximums
Heart - $150,000Liver - $230,000
Bone Marrow - $130,000Kidney - $80,000
Pancreas - $50,000Kidney/Pancreas - $80,000
Heart/Lung - $185,000Lung - $185,000
38
7/1/2015 FL / EHB State: FLOpen Access Plus - CareerSource Central Florida OAP Choice - 4630907. Version# 5KitTrak: CSW09466
©Cigna 2015
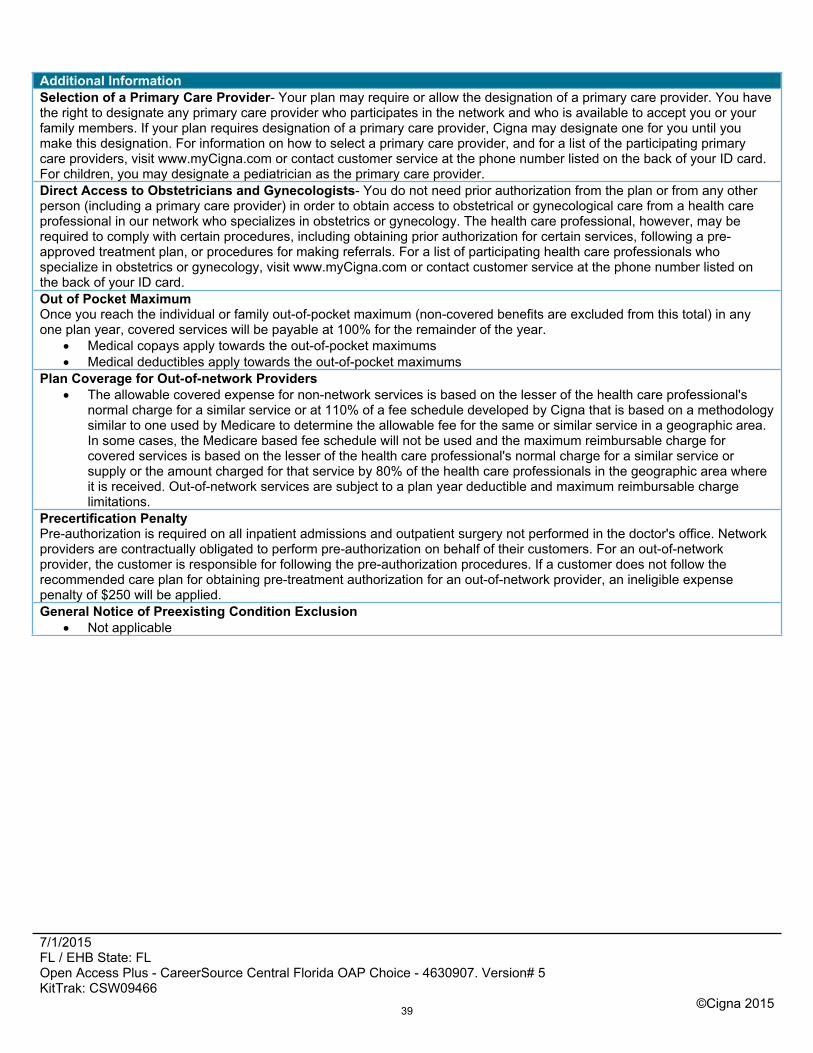
Additional InformationSelection of a Primary Care Provider- Your plan may require or allow the designation of a primary care provider. You have the right to designate any primary care provider who participates in the network and who is available to accept you or your family members. If your plan requires designation of a primary care provider, Cigna may designate one for you until you make this designation. For information on how to select a primary care provider, and for a list of the participating primary care providers, visit www.myCigna.com or contact customer service at the phone number listed on the back of your ID card.For children, you may designate a pediatrician as the primary care provider.Direct Access to Obstetricians and Gynecologists- You do not need prior authorization from the plan or from any other person (including a primary care provider) in order to obtain access to obstetrical or gynecological care from a health care professional in our network who specializes in obstetrics or gynecology. The health care professional, however, may be required to comply with certain procedures, including obtaining prior authorization for certain services, following a pre-approved treatment plan, or procedures for making referrals. For a list of participating health care professionals who specialize in obstetrics or gynecology, visit www.myCigna.com or contact customer service at the phone number listed on the back of your ID card.Out of Pocket MaximumOnce you reach the individual or family out-of-pocket maximum (non-covered benefits are excluded from this total) in any one plan year, covered services will be payable at 100% for the remainder of the year.
Medical copays apply towards the out-of-pocket maximums Medical deductibles apply towards the out-of-pocket maximums
Plan Coverage for Out-of-network Providers The allowable covered expense for non-network services is based on the lesser of the health care professional's
normal charge for a similar service or at 110% of a fee schedule developed by Cigna that is based on a methodology similar to one used by Medicare to determine the allowable fee for the same or similar service in a geographic area. In some cases, the Medicare based fee schedule will not be used and the maximum reimbursable charge for covered services is based on the lesser of the health care professional's normal charge for a similar service or supply or the amount charged for that service by 80% of the health care professionals in the geographic area where it is received. Out-of-network services are subject to a plan year deductible and maximum reimbursable charge limitations.
Precertification PenaltyPre-authorization is required on all inpatient admissions and outpatient surgery not performed in the doctor's office. Network providers are contractually obligated to perform pre-authorization on behalf of their customers. For an out-of-network provider, the customer is responsible for following the pre-authorization procedures. If a customer does not follow the recommended care plan for obtaining pre-treatment authorization for an out-of-network provider, an ineligible expense penalty of $250 will be applied.General Notice of Preexisting Condition Exclusion
Not applicable
39
7/1/2015 FL / EHB State: FLOpen Access Plus - CareerSource Central Florida OAP Choice - 4630907. Version# 5KitTrak: CSW09466
©Cigna 2015
ExclusionsWhat's Not Covered (This Is Not All Inclusive; check your plan documents for a complete list)
Services that aren't medically necessary Experimental or investigational treatments, except for routine patient care costs related to qualified clinical trials as
described in your plan document Accidental injury that occurs while working for pay or profit Sickness for which benefits are paid or payable under any Worker's Compensation or similar law Services provided by government health plans Cosmetic surgery, unless it corrects deformities resulting from illness, breast reconstruction surgery after a
mastectomy, or congenital defects of a newborn or adopted child or child placed for adoption Dental treatments and implants Custodial care Sex transformation Surgical procedures for the improvement of vision that can be corrected through the use of glasses or contact lenses Vision therapy or orthoptic treatment Hearing aids Reversal of sterilization procedures Nonprescription drugs or anti-obesity drugs Gene manipulation therapy Smoking cessation programs Non-emergency services incurred outside the United States Bariatric surgery Infertility services
These are only the highlightsThis summary outlines the highlights of your plan. For a complete list of both covered and not-covered services, including benefits required by your state, see your employer's insurance certificate or summary plan description -- the official plan documents. If there are any differences between this summary and the plan documents, the information in the plan documents takes precedence.
All Cigna products and services are provided exclusively by or through operating subsidiaries of Cigna Corporation, including Cigna Health and Life Insurance Company, Connecticut General Life Insurance Company, Cigna Behavioral Health, Inc., Cigna Health Management, Inc. and HMO or service company subsidiaries of Cigna Health Corporation. The Cigna name, logo, and other Cigna marks are owned by Cigna Intellectual Property, Inc.
40
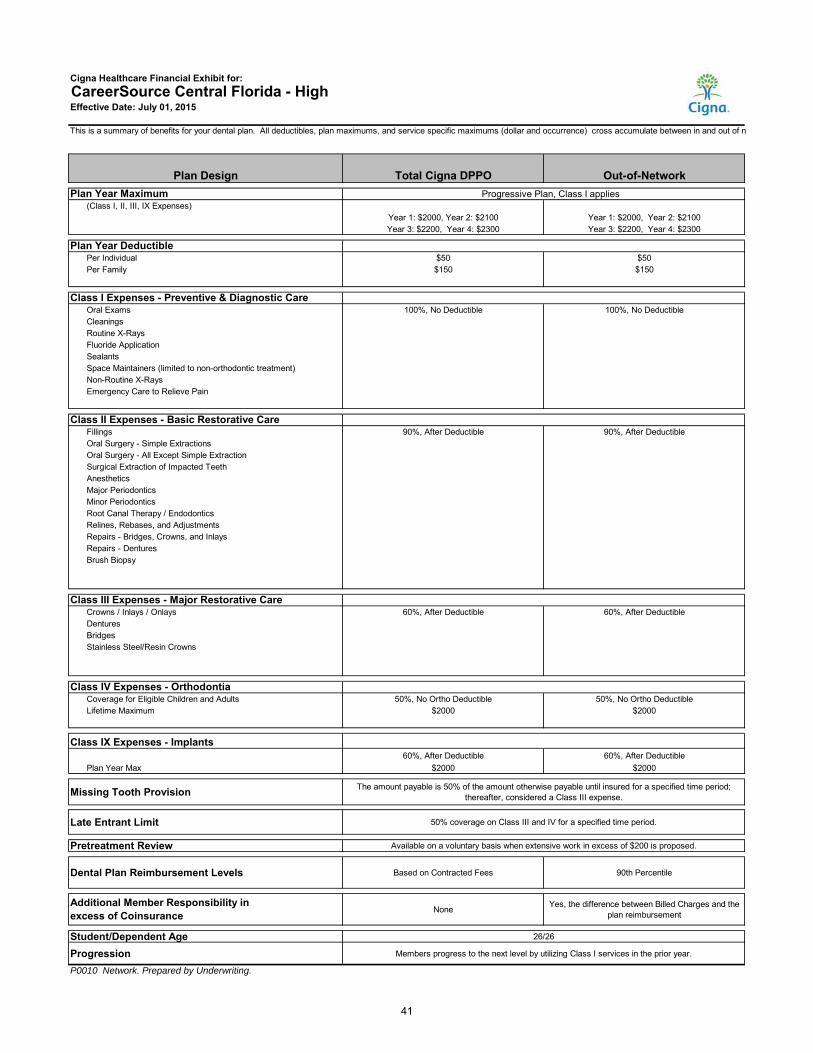
Cigna Healthcare Financial Exhibit for: CareerSource Central Florida - HighEffective Date: July 01, 2015
This is a summary of benefits for your dental plan. All deductibles, plan maximums, and service specific maximums (dollar and occurrence) cross accumulate between in and out of n
Plan Design Total Cigna DPPO Out-of-NetworkPlan Year Maximum Progressive Plan, Class I applies
(Class I, II, III, IX Expenses) Year 1: $2000, Year 2: $2100 Year 1: $2000, Year 2: $2100Year 3: $2200, Year 4: $2300 Year 3: $2200, Year 4: $2300
Plan Year DeductiblePer Individual $50 $50Per Family $150 $150
Class I Expenses - Preventive & Diagnostic CareOral Exams 100%, No Deductible 100%, No DeductibleCleaningsRoutine X-RaysFluoride ApplicationSealantsSpace Maintainers (limited to non-orthodontic treatment)Non-Routine X-RaysEmergency Care to Relieve Pain
Class II Expenses - Basic Restorative CareFillings 90%, After Deductible 90%, After DeductibleOral Surgery - Simple ExtractionsOral Surgery - All Except Simple ExtractionSurgical Extraction of Impacted TeethAnestheticsMajor PeriodonticsMinor PeriodonticsRoot Canal Therapy / EndodonticsRelines, Rebases, and AdjustmentsRepairs - Bridges, Crowns, and InlaysRepairs - DenturesBrush Biopsy
Class III Expenses - Major Restorative CareCrowns / Inlays / Onlays 60%, After Deductible 60%, After DeductibleDenturesBridgesStainless Steel/Resin Crowns
Class IV Expenses - Orthodontia Coverage for Eligible Children and Adults 50%, No Ortho Deductible 50%, No Ortho DeductibleLifetime Maximum $2000 $2000
Class IX Expenses - Implants60%, After Deductible
Plan Year Max $2000
Missing Tooth Provision The amount payable is 50% of the amount otherwise payable until insured for a specified time period; thereafter, considered a Class III expense.
Late Entrant Limit Standard 50% coverage on Class III and IV for a specified time period.
Pretreatment Review Available on a voluntary basis when extensive work in excess of $200 is proposed.
Dental Plan Reimbursement Levels Based on Contracted Fees 90th Percentile
None Yes, the difference between Billed Charges and the plan reimbursement
Student/Dependent Age 26/26
Progression Members progress to the next level by utilizing Class I services in the prior year.
P0010 Network. Prepared by Underwriting.
60%, After Deductible$2000
Additional Member Responsibility in excess of Coinsurance
41
.,. ~~~
Cigna.
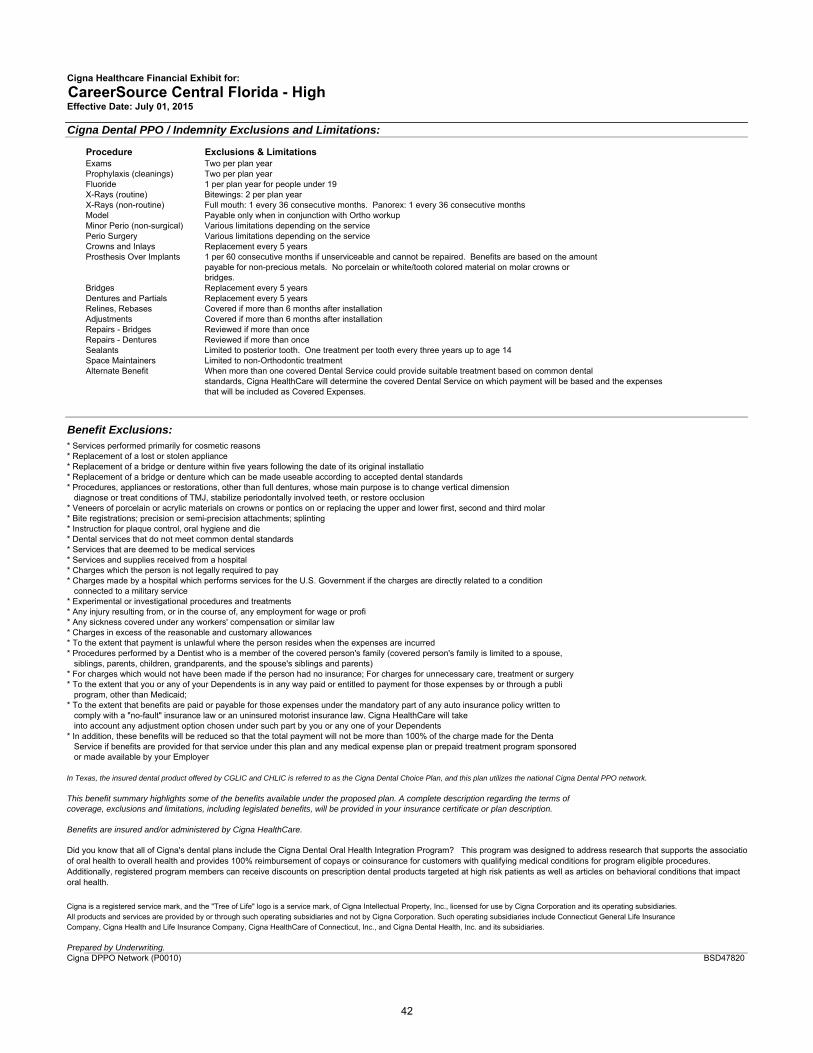
Cigna Healthcare Financial Exhibit for: CareerSource Central Florida - HighEffective Date: July 01, 2015
Cigna Dental PPO / Indemnity Exclusions and Limitations:
Procedure Exclusions & LimitationsExams Two per plan yearProphylaxis (cleanings) Two per plan yearFluoride 1 per plan year for people under 19X-Rays (routine) Bitewings: 2 per plan yearX-Rays (non-routine) Full mouth: 1 every 36 consecutive months. Panorex: 1 every 36 consecutive monthsModel Payable only when in conjunction with Ortho workupMinor Perio (non-surgical) Various limitations depending on the servicePerio Surgery Various limitations depending on the serviceCrowns and Inlays Replacement every 5 yearsProsthesis Over Implants 1 per 60 consecutive months if unserviceable and cannot be repaired. Benefits are based on the amount
payable for non-precious metals. No porcelain or white/tooth colored material on molar crowns or bridges.
Bridges Replacement every 5 yearsDentures and Partials Replacement every 5 yearsRelines, Rebases Covered if more than 6 months after installationAdjustments Covered if more than 6 months after installationRepairs - Bridges Reviewed if more than onceRepairs - Dentures Reviewed if more than onceSealants Limited to posterior tooth. One treatment per tooth every three years up to age 14Space Maintainers Limited to non-Orthodontic treatmentAlternate Benefit When more than one covered Dental Service could provide suitable treatment based on common dental
standards, Cigna HealthCare will determine the covered Dental Service on which payment will be based and the expenses that will be included as Covered Expenses.
Benefit Exclusions:* Services performed primarily for cosmetic reasons* Replacement of a lost or stolen appliance* Replacement of a bridge or denture within five years following the date of its original installatio* Replacement of a bridge or denture which can be made useable according to accepted dental standards* Procedures, appliances or restorations, other than full dentures, whose main purpose is to change vertical dimension diagnose or treat conditions of TMJ, stabilize periodontally involved teeth, or restore occlusion* Veneers of porcelain or acrylic materials on crowns or pontics on or replacing the upper and lower first, second and third molar* Bite registrations; precision or semi-precision attachments; splinting* Instruction for plaque control, oral hygiene and die* Dental services that do not meet common dental standards* Services that are deemed to be medical services* Services and supplies received from a hospital* Charges which the person is not legally required to pay* Charges made by a hospital which performs services for the U.S. Government if the charges are directly related to a condition connected to a military service * Experimental or investigational procedures and treatments* Any injury resulting from, or in the course of, any employment for wage or profi* Any sickness covered under any workers' compensation or similar law* Charges in excess of the reasonable and customary allowances* To the extent that payment is unlawful where the person resides when the expenses are incurred* Procedures performed by a Dentist who is a member of the covered person's family (covered person's family is limited to a spouse, siblings, parents, children, grandparents, and the spouse's siblings and parents)* For charges which would not have been made if the person had no insurance; For charges for unnecessary care, treatment or surgery* To the extent that you or any of your Dependents is in any way paid or entitled to payment for those expenses by or through a publi program, other than Medicaid; * To the extent that benefits are paid or payable for those expenses under the mandatory part of any auto insurance policy written to comply with a "no-fault" insurance law or an uninsured motorist insurance law. Cigna HealthCare will take into account any adjustment option chosen under such part by you or any one of your Dependents* In addition, these benefits will be reduced so that the total payment will not be more than 100% of the charge made for the Denta Service if benefits are provided for that service under this plan and any medical expense plan or prepaid treatment program sponsored or made available by your Employer
In Texas, the insured dental product offered by CGLIC and CHLIC is referred to as the Cigna Dental Choice Plan, and this plan utilizes the national Cigna Dental PPO network.
This benefit summary highlights some of the benefits available under the proposed plan. A complete description regarding the terms ofcoverage, exclusions and limitations, including legislated benefits, will be provided in your insurance certificate or plan description.
Benefits are insured and/or administered by Cigna HealthCare.
Cigna is a registered service mark, and the "Tree of Life" logo is a service mark, of Cigna Intellectual Property, Inc., licensed for use by Cigna Corporation and its operating subsidiaries. All products and services are provided by or through such operating subsidiaries and not by Cigna Corporation. Such operating subsidiaries include Connecticut General Life InsuranceCompany, Cigna Health and Life Insurance Company, Cigna HealthCare of Connecticut, Inc., and Cigna Dental Health, Inc. and its subsidiaries.
Prepared by Underwriting.Cigna DPPO Network (P0010)
Did you know that all of Cigna's dental plans include the Cigna Dental Oral Health Integration Program? This program was designed to address research that supports the associatioof oral health to overall health and provides 100% reimbursement of copays or coinsurance for customers with qualifying medical conditions for program eligible procedures. Additionally, registered program members can receive discounts on prescription dental products targeted at high risk patients as well as articles on behavioral conditions that impact oral health.
BSD47820
42
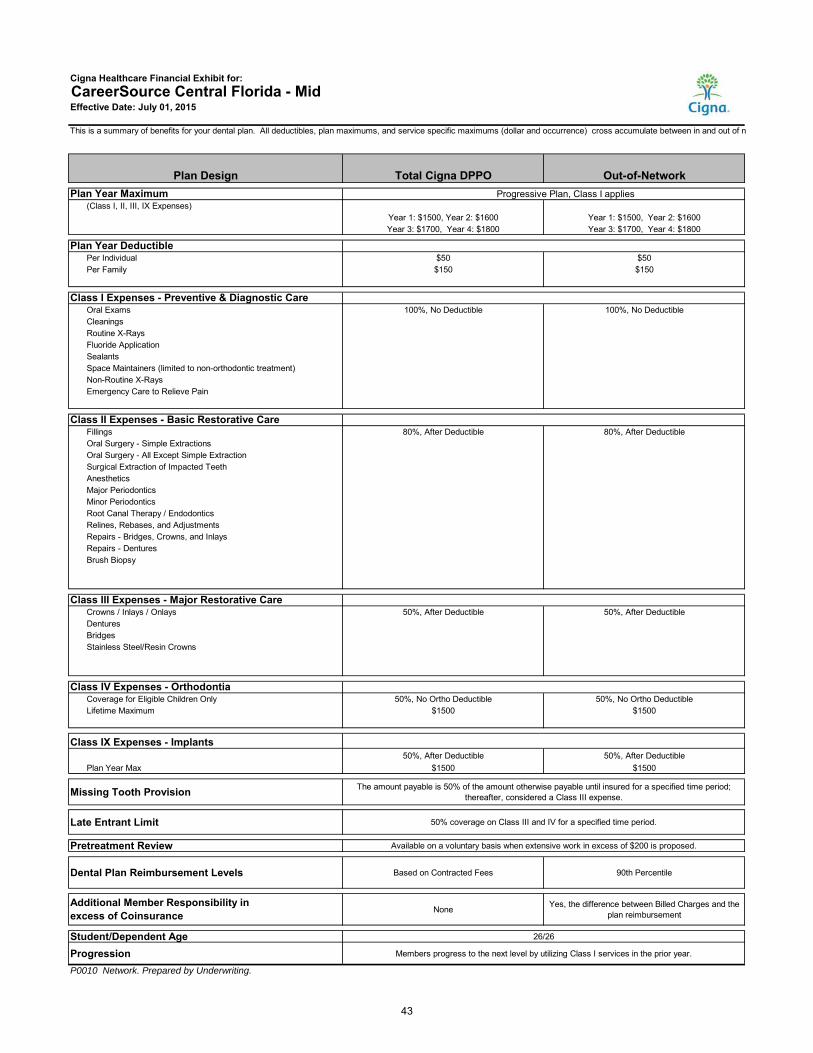
Cigna Healthcare Financial Exhibit for: CareerSource Central Florida - MidEffective Date: July 01, 2015
This is a summary of benefits for your dental plan. All deductibles, plan maximums, and service specific maximums (dollar and occurrence) cross accumulate between in and out of n
Plan Design Total Cigna DPPO Out-of-NetworkPlan Year Maximum Progressive Plan, Class I applies
(Class I, II, III, IX Expenses) Year 1: $1500, Year 2: $1600 Year 1: $1500, Year 2: $1600Year 3: $1700, Year 4: $1800 Year 3: $1700, Year 4: $1800
Plan Year DeductiblePer Individual $50 $50Per Family $150 $150
Class I Expenses - Preventive & Diagnostic CareOral Exams 100%, No Deductible 100%, No DeductibleCleaningsRoutine X-RaysFluoride ApplicationSealantsSpace Maintainers (limited to non-orthodontic treatment)Non-Routine X-RaysEmergency Care to Relieve Pain
Class II Expenses - Basic Restorative CareFillings 80%, After Deductible 80%, After DeductibleOral Surgery - Simple ExtractionsOral Surgery - All Except Simple ExtractionSurgical Extraction of Impacted TeethAnestheticsMajor PeriodonticsMinor PeriodonticsRoot Canal Therapy / EndodonticsRelines, Rebases, and AdjustmentsRepairs - Bridges, Crowns, and InlaysRepairs - DenturesBrush Biopsy
Class III Expenses - Major Restorative CareCrowns / Inlays / Onlays 50%, After Deductible 50%, After DeductibleDenturesBridgesStainless Steel/Resin Crowns
Class IV Expenses - Orthodontia Coverage for Eligible Children Only 50%, No Ortho Deductible 50%, No Ortho DeductibleLifetime Maximum $1500 $1500
Class IX Expenses - Implants50%, After Deductible
Plan Year Max $1500
Missing Tooth Provision The amount payable is 50% of the amount otherwise payable until insured for a specified time period; thereafter, considered a Class III expense.
Late Entrant Limit Standard 50% coverage on Class III and IV for a specified time period.
Pretreatment Review Available on a voluntary basis when extensive work in excess of $200 is proposed.
Dental Plan Reimbursement Levels Based on Contracted Fees 90th Percentile
None Yes, the difference between Billed Charges and the plan reimbursement
Student/Dependent Age 26/26
Progression Members progress to the next level by utilizing Class I services in the prior year.
P0010 Network. Prepared by Underwriting.
50%, After Deductible$1500
Additional Member Responsibility in excess of Coinsurance
43
.,. ~~~
Cigna.
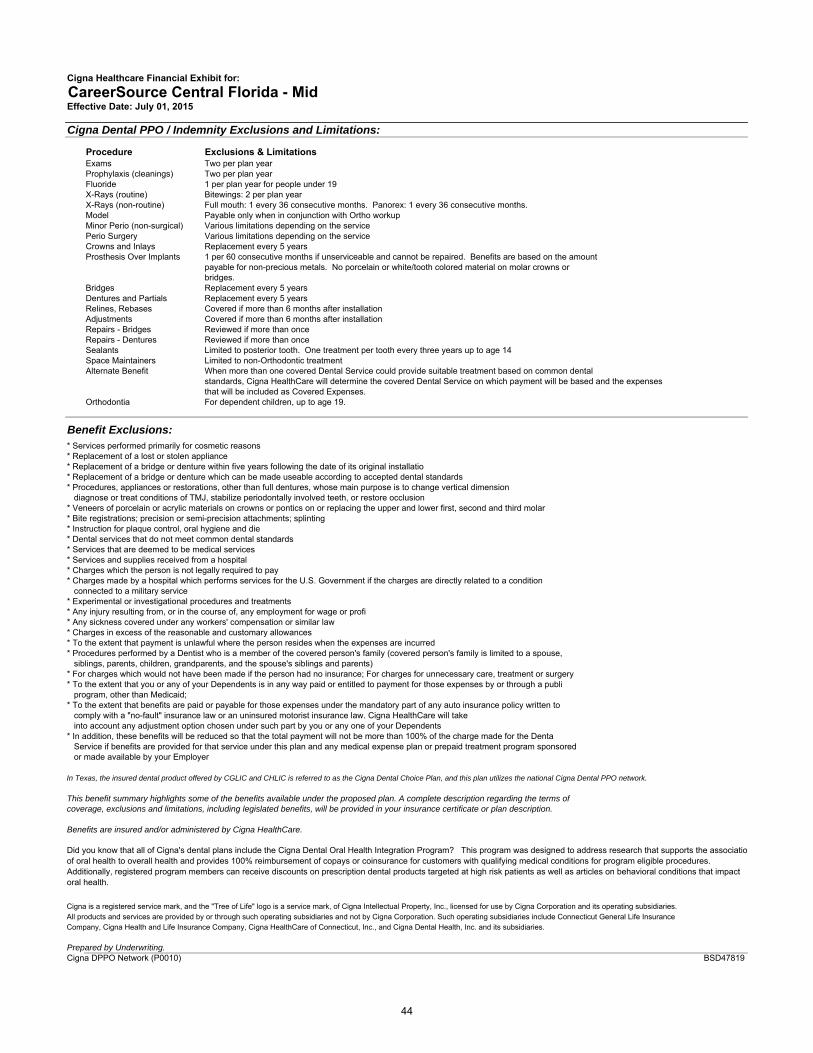
Cigna Healthcare Financial Exhibit for: CareerSource Central Florida - MidEffective Date: July 01, 2015
Cigna Dental PPO / Indemnity Exclusions and Limitations:
Procedure Exclusions & LimitationsExams Two per plan yearProphylaxis (cleanings) Two per plan yearFluoride 1 per plan year for people under 19X-Rays (routine) Bitewings: 2 per plan yearX-Rays (non-routine) Full mouth: 1 every 36 consecutive months. Panorex: 1 every 36 consecutive months.Model Payable only when in conjunction with Ortho workupMinor Perio (non-surgical) Various limitations depending on the servicePerio Surgery Various limitations depending on the serviceCrowns and Inlays Replacement every 5 yearsProsthesis Over Implants 1 per 60 consecutive months if unserviceable and cannot be repaired. Benefits are based on the amount
payable for non-precious metals. No porcelain or white/tooth colored material on molar crowns or bridges.
Bridges Replacement every 5 yearsDentures and Partials Replacement every 5 yearsRelines, Rebases Covered if more than 6 months after installationAdjustments Covered if more than 6 months after installationRepairs - Bridges Reviewed if more than onceRepairs - Dentures Reviewed if more than onceSealants Limited to posterior tooth. One treatment per tooth every three years up to age 14Space Maintainers Limited to non-Orthodontic treatmentAlternate Benefit When more than one covered Dental Service could provide suitable treatment based on common dental
standards, Cigna HealthCare will determine the covered Dental Service on which payment will be based and the expenses that will be included as Covered Expenses.
Orthodontia For dependent children, up to age 19.
Benefit Exclusions:* Services performed primarily for cosmetic reasons* Replacement of a lost or stolen appliance* Replacement of a bridge or denture within five years following the date of its original installatio* Replacement of a bridge or denture which can be made useable according to accepted dental standards* Procedures, appliances or restorations, other than full dentures, whose main purpose is to change vertical dimension diagnose or treat conditions of TMJ, stabilize periodontally involved teeth, or restore occlusion* Veneers of porcelain or acrylic materials on crowns or pontics on or replacing the upper and lower first, second and third molar* Bite registrations; precision or semi-precision attachments; splinting* Instruction for plaque control, oral hygiene and die* Dental services that do not meet common dental standards* Services that are deemed to be medical services* Services and supplies received from a hospital* Charges which the person is not legally required to pay* Charges made by a hospital which performs services for the U.S. Government if the charges are directly related to a condition connected to a military service * Experimental or investigational procedures and treatments* Any injury resulting from, or in the course of, any employment for wage or profi* Any sickness covered under any workers' compensation or similar law* Charges in excess of the reasonable and customary allowances* To the extent that payment is unlawful where the person resides when the expenses are incurred* Procedures performed by a Dentist who is a member of the covered person's family (covered person's family is limited to a spouse, siblings, parents, children, grandparents, and the spouse's siblings and parents)* For charges which would not have been made if the person had no insurance; For charges for unnecessary care, treatment or surgery* To the extent that you or any of your Dependents is in any way paid or entitled to payment for those expenses by or through a publi program, other than Medicaid; * To the extent that benefits are paid or payable for those expenses under the mandatory part of any auto insurance policy written to comply with a "no-fault" insurance law or an uninsured motorist insurance law. Cigna HealthCare will take into account any adjustment option chosen under such part by you or any one of your Dependents* In addition, these benefits will be reduced so that the total payment will not be more than 100% of the charge made for the Denta Service if benefits are provided for that service under this plan and any medical expense plan or prepaid treatment program sponsored or made available by your Employer
In Texas, the insured dental product offered by CGLIC and CHLIC is referred to as the Cigna Dental Choice Plan, and this plan utilizes the national Cigna Dental PPO network.
This benefit summary highlights some of the benefits available under the proposed plan. A complete description regarding the terms ofcoverage, exclusions and limitations, including legislated benefits, will be provided in your insurance certificate or plan description.
Benefits are insured and/or administered by Cigna HealthCare.
Cigna is a registered service mark, and the "Tree of Life" logo is a service mark, of Cigna Intellectual Property, Inc., licensed for use by Cigna Corporation and its operating subsidiaries. All products and services are provided by or through such operating subsidiaries and not by Cigna Corporation. Such operating subsidiaries include Connecticut General Life InsuranceCompany, Cigna Health and Life Insurance Company, Cigna HealthCare of Connecticut, Inc., and Cigna Dental Health, Inc. and its subsidiaries.
Prepared by Underwriting.Cigna DPPO Network (P0010)
Did you know that all of Cigna's dental plans include the Cigna Dental Oral Health Integration Program? This program was designed to address research that supports the associatioof oral health to overall health and provides 100% reimbursement of copays or coinsurance for customers with qualifying medical conditions for program eligible procedures. Additionally, registered program members can receive discounts on prescription dental products targeted at high risk patients as well as articles on behavioral conditions that impact oral health.
BSD47819
44
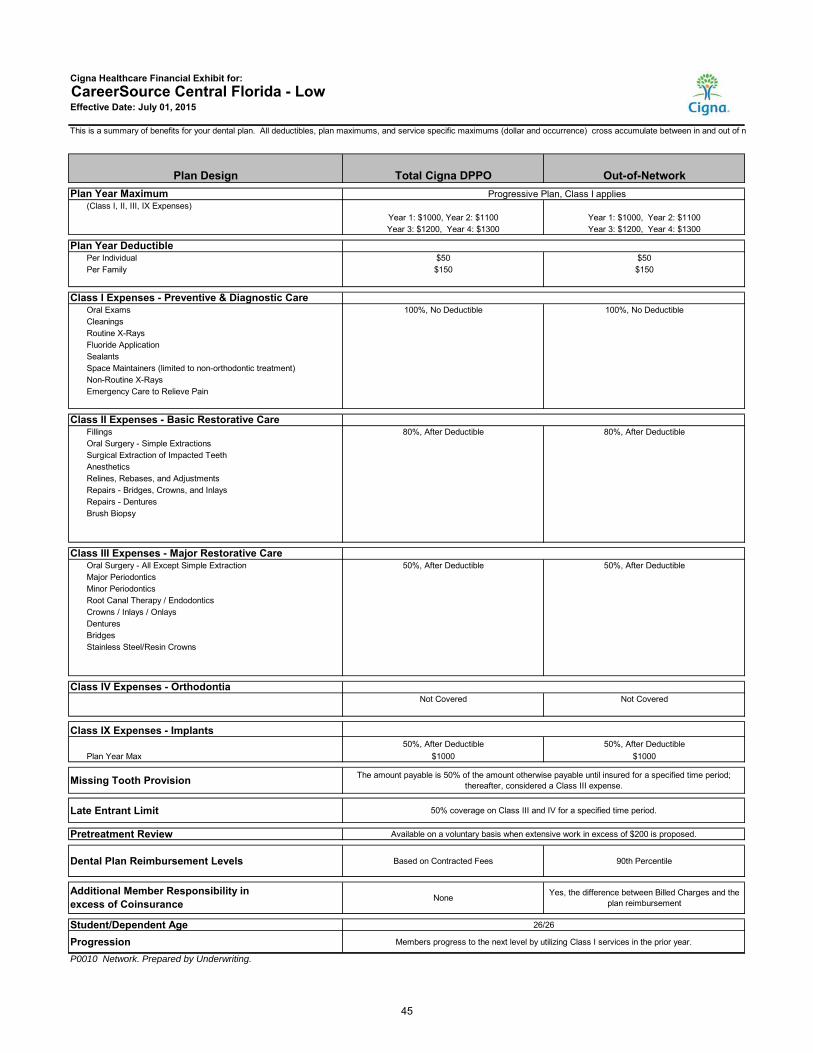
Cigna Healthcare Financial Exhibit for: CareerSource Central Florida - LowEffective Date: July 01, 2015
This is a summary of benefits for your dental plan. All deductibles, plan maximums, and service specific maximums (dollar and occurrence) cross accumulate between in and out of n
Plan Design Total Cigna DPPO Out-of-NetworkPlan Year Maximum Progressive Plan, Class I applies
(Class I, II, III, IX Expenses) Year 1: $1000, Year 2: $1100 Year 1: $1000, Year 2: $1100Year 3: $1200, Year 4: $1300 Year 3: $1200, Year 4: $1300
Plan Year DeductiblePer Individual $50 $50Per Family $150 $150
Class I Expenses - Preventive & Diagnostic CareOral Exams 100%, No Deductible 100%, No DeductibleCleaningsRoutine X-RaysFluoride ApplicationSealantsSpace Maintainers (limited to non-orthodontic treatment)Non-Routine X-RaysEmergency Care to Relieve Pain
Class II Expenses - Basic Restorative CareFillings 80%, After Deductible 80%, After DeductibleOral Surgery - Simple ExtractionsSurgical Extraction of Impacted TeethAnestheticsRelines, Rebases, and AdjustmentsRepairs - Bridges, Crowns, and InlaysRepairs - DenturesBrush Biopsy
Class III Expenses - Major Restorative CareOral Surgery - All Except Simple Extraction 50%, After Deductible 50%, After DeductibleMajor PeriodonticsMinor PeriodonticsRoot Canal Therapy / EndodonticsCrowns / Inlays / OnlaysDenturesBridgesStainless Steel/Resin Crowns
Class IV Expenses - Orthodontia Not Covered Not Covered
Class IX Expenses - Implants50%, After Deductible
Plan Year Max $1000
Missing Tooth Provision The amount payable is 50% of the amount otherwise payable until insured for a specified time period; thereafter, considered a Class III expense.
Late Entrant Limit Standard 50% coverage on Class III and IV for a specified time period.
Pretreatment Review Available on a voluntary basis when extensive work in excess of $200 is proposed.
Dental Plan Reimbursement Levels Based on Contracted Fees 90th Percentile
None Yes, the difference between Billed Charges and the plan reimbursement
Student/Dependent Age 26/26
Progression Members progress to the next level by utilizing Class I services in the prior year.
P0010 Network. Prepared by Underwriting.
50%, After Deductible$1000
Additional Member Responsibility in excess of Coinsurance
45
.,. ~~~
Cigna.
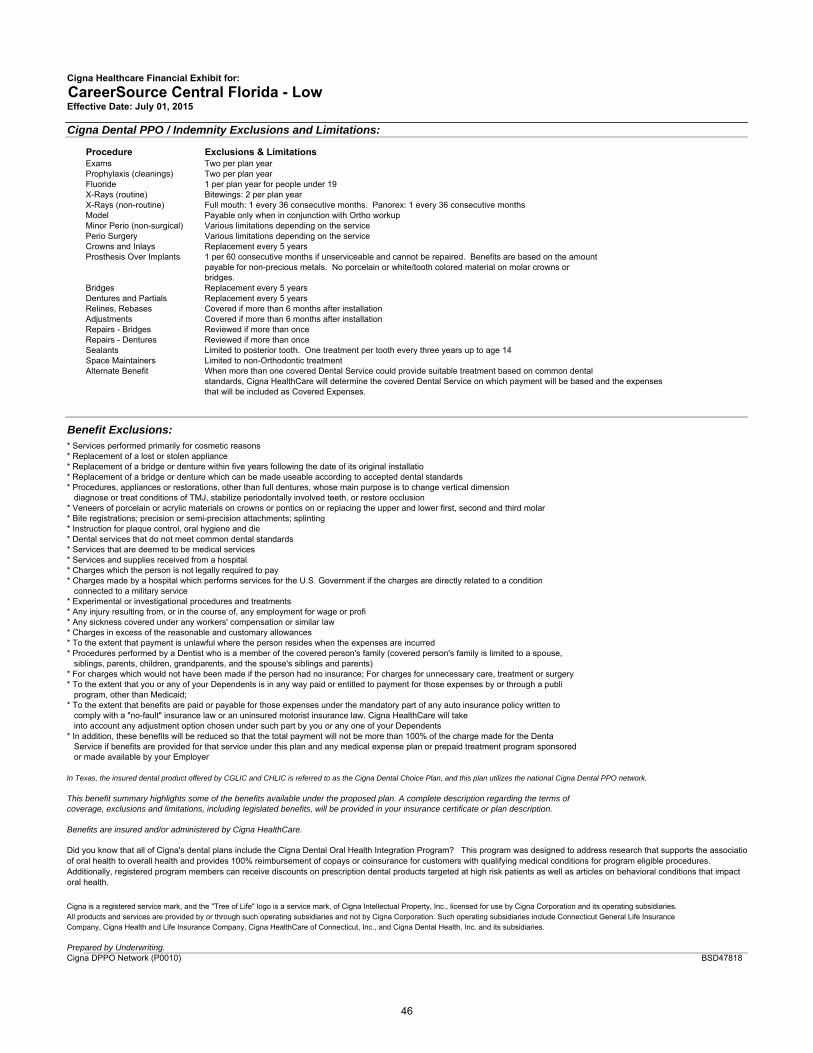
Cigna Healthcare Financial Exhibit for: CareerSource Central Florida - LowEffective Date: July 01, 2015
Cigna Dental PPO / Indemnity Exclusions and Limitations:
Procedure Exclusions & LimitationsExams Two per plan yearProphylaxis (cleanings) Two per plan yearFluoride 1 per plan year for people under 19X-Rays (routine) Bitewings: 2 per plan yearX-Rays (non-routine) Full mouth: 1 every 36 consecutive months. Panorex: 1 every 36 consecutive monthsModel Payable only when in conjunction with Ortho workupMinor Perio (non-surgical) Various limitations depending on the servicePerio Surgery Various limitations depending on the serviceCrowns and Inlays Replacement every 5 yearsProsthesis Over Implants 1 per 60 consecutive months if unserviceable and cannot be repaired. Benefits are based on the amount
payable for non-precious metals. No porcelain or white/tooth colored material on molar crowns or bridges.
Bridges Replacement every 5 yearsDentures and Partials Replacement every 5 yearsRelines, Rebases Covered if more than 6 months after installationAdjustments Covered if more than 6 months after installationRepairs - Bridges Reviewed if more than onceRepairs - Dentures Reviewed if more than onceSealants Limited to posterior tooth. One treatment per tooth every three years up to age 14Space Maintainers Limited to non-Orthodontic treatmentAlternate Benefit When more than one covered Dental Service could provide suitable treatment based on common dental
standards, Cigna HealthCare will determine the covered Dental Service on which payment will be based and the expenses that will be included as Covered Expenses.
Benefit Exclusions:* Services performed primarily for cosmetic reasons* Replacement of a lost or stolen appliance* Replacement of a bridge or denture within five years following the date of its original installatio* Replacement of a bridge or denture which can be made useable according to accepted dental standards* Procedures, appliances or restorations, other than full dentures, whose main purpose is to change vertical dimension diagnose or treat conditions of TMJ, stabilize periodontally involved teeth, or restore occlusion* Veneers of porcelain or acrylic materials on crowns or pontics on or replacing the upper and lower first, second and third molar* Bite registrations; precision or semi-precision attachments; splinting* Instruction for plaque control, oral hygiene and die* Dental services that do not meet common dental standards* Services that are deemed to be medical services* Services and supplies received from a hospital* Charges which the person is not legally required to pay* Charges made by a hospital which performs services for the U.S. Government if the charges are directly related to a condition connected to a military service * Experimental or investigational procedures and treatments* Any injury resulting from, or in the course of, any employment for wage or profi* Any sickness covered under any workers' compensation or similar law* Charges in excess of the reasonable and customary allowances* To the extent that payment is unlawful where the person resides when the expenses are incurred* Procedures performed by a Dentist who is a member of the covered person's family (covered person's family is limited to a spouse, siblings, parents, children, grandparents, and the spouse's siblings and parents)* For charges which would not have been made if the person had no insurance; For charges for unnecessary care, treatment or surgery* To the extent that you or any of your Dependents is in any way paid or entitled to payment for those expenses by or through a publi program, other than Medicaid; * To the extent that benefits are paid or payable for those expenses under the mandatory part of any auto insurance policy written to comply with a "no-fault" insurance law or an uninsured motorist insurance law. Cigna HealthCare will take into account any adjustment option chosen under such part by you or any one of your Dependents* In addition, these benefits will be reduced so that the total payment will not be more than 100% of the charge made for the Denta Service if benefits are provided for that service under this plan and any medical expense plan or prepaid treatment program sponsored or made available by your Employer
In Texas, the insured dental product offered by CGLIC and CHLIC is referred to as the Cigna Dental Choice Plan, and this plan utilizes the national Cigna Dental PPO network.
This benefit summary highlights some of the benefits available under the proposed plan. A complete description regarding the terms ofcoverage, exclusions and limitations, including legislated benefits, will be provided in your insurance certificate or plan description.
Benefits are insured and/or administered by Cigna HealthCare.
Cigna is a registered service mark, and the "Tree of Life" logo is a service mark, of Cigna Intellectual Property, Inc., licensed for use by Cigna Corporation and its operating subsidiaries. All products and services are provided by or through such operating subsidiaries and not by Cigna Corporation. Such operating subsidiaries include Connecticut General Life InsuranceCompany, Cigna Health and Life Insurance Company, Cigna HealthCare of Connecticut, Inc., and Cigna Dental Health, Inc. and its subsidiaries.
Prepared by Underwriting.Cigna DPPO Network (P0010)
Did you know that all of Cigna's dental plans include the Cigna Dental Oral Health Integration Program? This program was designed to address research that supports the associatioof oral health to overall health and provides 100% reimbursement of copays or coinsurance for customers with qualifying medical conditions for program eligible procedures. Additionally, registered program members can receive discounts on prescription dental products targeted at high risk patients as well as articles on behavioral conditions that impact oral health.
BSD47818
46
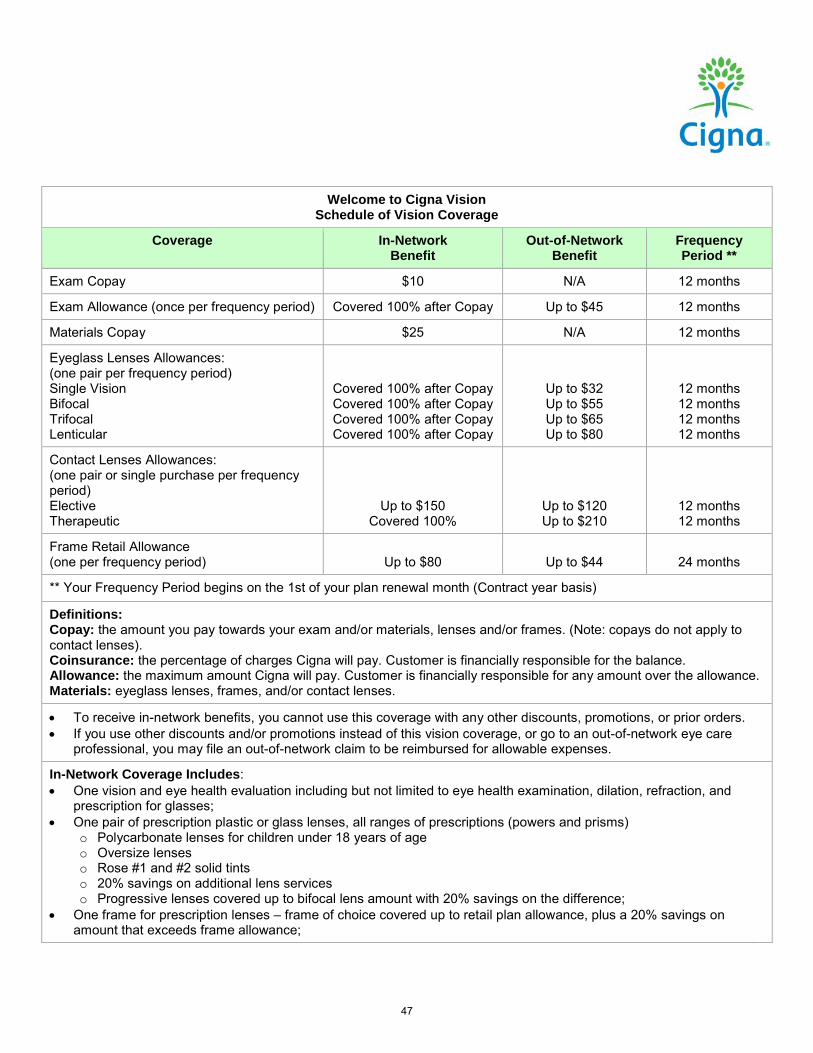
Welcome to Cigna Vision Schedule of Vision Coverage
Coverage In-Network Benefit
Out-of-Network Benefit
Frequency Period **
Exam Copay $10 N/A 12 months
Exam Allowance (once per frequency period) Covered 100% after Copay Up to $45 12 months
Materials Copay $25 N/A 12 months
Eyeglass Lenses Allowances: (one pair per frequency period) Single Vision Bifocal Trifocal Lenticular
Covered 100% after Copay Covered 100% after Copay Covered 100% after Copay Covered 100% after Copay
Up to $32 Up to $55 Up to $65 Up to $80
12 months 12 months 12 months 12 months
Contact Lenses Allowances: (one pair or single purchase per frequency period) Elective Therapeutic
Up to $150 Covered 100%
Up to $120 Up to $210
12 months 12 months
Frame Retail Allowance (one per frequency period)
Up to $80
Up to $44
24 months
** Your Frequency Period begins on the 1st of your plan renewal month (Contract year basis)
Definitions: Copay: the amount you pay towards your exam and/or materials, lenses and/or frames. (Note: copays do not apply to contact lenses). Coinsurance: the percentage of charges Cigna will pay. Customer is financially responsible for the balance. Allowance: the maximum amount Cigna will pay. Customer is financially responsible for any amount over the allowance. Materials: eyeglass lenses, frames, and/or contact lenses.
• To receive in-network benefits, you cannot use this coverage with any other discounts, promotions, or prior orders. • If you use other discounts and/or promotions instead of this vision coverage, or go to an out-of-network eye care
professional, you may file an out-of-network claim to be reimbursed for allowable expenses.
In-Network Coverage Includes: • One vision and eye health evaluation including but not limited to eye health examination, dilation, refraction, and
prescription for glasses; • One pair of prescription plastic or glass lenses, all ranges of prescriptions (powers and prisms)
o Polycarbonate lenses for children under 18 years of age o Oversize lenses o Rose #1 and #2 solid tints o 20% savings on additional lens services o Progressive lenses covered up to bifocal lens amount with 20% savings on the difference;
• One frame for prescription lenses – frame of choice covered up to retail plan allowance, plus a 20% savings on amount that exceeds frame allowance;
47
••• ..... ,,._, _:rr Cigna~
• One pair of contact lenses or a single purchase of a supply of contact lenses – in lieu of lenses and frame benefit, (may not receive contact lenses and frames in same benefit year). Allowance applied towards cost of supplemental contact lens professional services (including the fitting and evaluation) and contact lens materials
•
Coverage for Therapeutic contact lenses will be provided when visual acuity cannot be corrected to 20/70 in the better eye with eyeglasses and the fitting of the contact lenses would obtain this level of visual acuity; and in certain cases of anisometropia, keratoconus, or aphakis; as determined and documented by your Vision eye care professional. Contact lenses fitted for other therapeutic purposes or the narrowing of visual fields due to high minus or plus correction will be covered in accordance with the Elective contact lens coverage shown on the Schedule of Benefits.
Vision Network Savings Program: • When you see a Cigna Vision Network Eye Care Professional*, you can save 20% (or more) on additional frames
and/or lenses, including lens options, with a valid prescription. This savings does not apply to contact lens materials. See your Cigna Vision Network Eye Care Professional for details.
* Provider participation is 100% voluntary; please check with your Eye Care Professional for any offered discounts.
What’s Not Covered: • Orthoptic or vision training and any associated supplemental testing • Medical or surgical treatment of the eyes • Any eye examination, or any corrective eyewear, required by an employer as a condition of employment • Any injury or illness when paid or payable by Workers’ Compensation or similar law, or which is work-related • Charges in excess of the usual and customary charge for the Service or Materials • Charges incurred after the policy ends or the insured’s coverage under the policy ends, except as stated in the policy • Experimental or non-conventional treatment or device • Magnification or low vision aids not shown as covered in the Schedule of Vision Coverage • Any non-prescription eyeglasses, lenses, or contact lenses • Spectacle lens treatments, “add-ons”, or lens coatings not shown as covered in the Schedule of Vision Coverage • Prescription sunglasses • Two pair of glasses, in lieu of bifocals or trifocals • Safety glasses or lenses required for employment not shown as covered in the Schedule of Vision Coverage • VDT (video display terminal)/computer eyeglass benefit • Claims submitted and received in excess of twelve (12) months from the original Date of Service •
48
How to use your Cigna Vision Benefits (Please be aware that the Cigna Vision network is different from the networks supporting our health/medical plans).
1. Finding a doctor There are three ways to find a quality eye doctor in your area:
1. Log in to myCigna.com, go to your Cigna Vision coverage page and select “View Details.” Then select “Find a Cigna Vision Network Eye Care Professional” to search the Cigna Vision Directory.
2. Don’t have access to myCigna.com? Go to Cigna.com and click on the orange Find a Doctor tab at the top. Then select “Vision Directory”, for routine eye exams and eyewear services, from the Other Directories listed below.
3. Prefer the phone? Call the toll-free number found on your Cigna insurance card and talk with a Cigna Vision customer service representative.
2. Schedule an appointment Identify yourself as a Cigna Vision customer when scheduling an appointment. Present your Cigna or Cigna Vision ID card at the time of your appointment, which will quickly assist the doctor’s office with accessing your plan details and verifying your eligibility. 3. Out-of-network plan reimbursement
How to use your Cigna Vision Benefits
Send a completed Cigna Vision claim form and itemized receipt to: Cigna Vision, Claims Department: PO Box 997561, Sacramento, CA 95899-7561. To get a Cigna Vision claim form: • Go to Cigna.com and go to Forms, Vision Forms • Go to myCigna.com and go to your vision coverage page Cigna Vision will pay for covered expenses within ten business days of receiving the completed claim form and itemized receipt.
Benefits are underwritten or administered by Connecticut General Life Insurance Company or Cigna Health and Life Insurance Company. Any benefit information displayed is intended as a summary of benefits only. It does not describe all the terms, provisions and limitations of your plan. Participating providers are independent contractors solely responsible for your routine vision examinations and products. “Cigna” is a registered service mark, and the “Tree of Life” logo, “Cigna Vision” and “CG Vision” are service marks, of Cigna Intellectual Property, Inc., licensed for use by Cigna Corporation and its operating subsidiaries. All products and services are provided by or through such operating subsidiaries, including Connecticut General Life Insurance Company and Cigna Health and Life Insurance Company, and not by Cigna Corporation. In Arizona and Louisiana, the Cigna Vision product is referred to as CG Vision. Vision Network Savings Program powered by Cigna Vision is a discount program, not an insured benefit.
49
.. ,·~•:,. ~-r Cigna