chronic limb ulcer
TRANSCRIPT

Chronic Limb Ulcer
BYPROF GOUDA ELLABBANSCU HOSPITAL/ EGYPT
Definition
• Ulcer is break of continuity of an epithelium.

Types of chronic limb ulcer
• Ischemic ulcer. Also called arterial ulcer
• Neuropathic ulcer.• Venous ulcer. Also called stasis ulcer
They are distinct with regard to their location, appearance, bleeding, and associated pain.

ISCHEMIC ULCER

Ischemic Ulcer
• Pathophysiology
Obliteration of arterial lumen decrease blood supply to distal tissues ischemia of the skin ulceration.

Ischemic Ulcer
• Common in the elderly, who also have symptoms of coronary or cerebral vascular disease.
• Very painful even at rest “rest pain”.• Decreased or absent pulse.• Pallor of the foot on elevation. • May be Associated with gangrene.
Clinical picture

Ischemic Ulcer
Obliteration of
Large artery Small artery
• Atherosclerosis.
• Embolism.
• Buerger’s disease.
• Diabetes.
• Embolism.
• Scleroderma.
Causes

Ischemic Ulcer
• Site: tip of the toe, dorsum of the foot & pressure area.
• Size: vary from small deep lesion to large flat ulcer.
• Shape: most often elliptical.
• Edge: either punched – out or sloping.
• Base: usually contain grayish granulation tissue.
• Depth: very deep, may penet. to underlying structures.
• Discharge: may be clear fluid, serum or pus.
• Tenderness: very tender
• Temperature: ischemic cold surrounding tissue.
Character



VENOUS ULCER

Venous Ulcer
• Anatomy • Deep system
• Returns blood to heart.
• Superficial system• Drain into deep system
• Perforator system• Connects superficial and deep allows one way flow• Superficial deep heart
Venous Ulcer
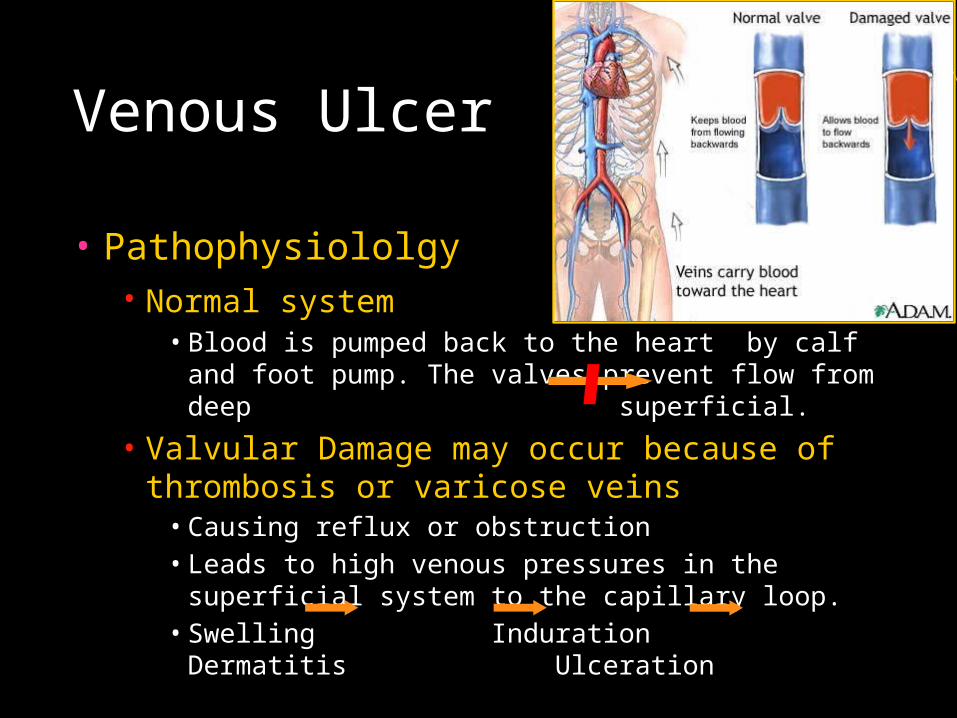
• Pathophysiololgy• Normal system
• Blood is pumped back to the heart by calf and foot pump. The valves prevent flow from deep superficial.
• Valvular Damage may occur because of thrombosis or varicose veins
• Causing reflux or obstruction• Leads to high venous pressures in the superficial system to the
capillary loop. • Swelling Induration Dermatitis Ulceration

Venous ulcer
• Majority of the patient are above the age of 40.• More in women than in men.• Discomfort and tenderness of the skin for a long time before
ulcer appear.• Usually not painful.
Clinical picture

Venous Ulcer
• Site: commonly found around the gaiter area of lower leg.
• Size: can be of any size.
• Shape: can be of any shape.
• Edge: sloping.
• Base: covered with yellow slough.
• Depth: usually shallow and flat.
• Discharge: usually seropurulent but can be blood stained.
• Tenderness: not severe. • Surrounding tissue: pigmented d\t hemosidren deposition.
Character



NEUROPATHIC ULCER

Neuropathic Ulcer
• Pathophysiology• Pain is the mechanism by which the body appreciates that
any part of the skin is becoming deprived of blood.• So, when pain sensation is lost any compressed tissue
may become permanently damaged. • Therefore, neuropathic ulcer is indirectly caused by local
ischemia.

Neuropathic Ulcer
Lesion of
Peripheral nerves Spinal cord
• Diabetes.
• Nerve injury.
• Leprosy.
• Spina bifida.
• Tabes dorsalis.
• Syringomyelia.
Causes

Neuropathic Ulcer
Site: occur over pressure area
Size: variable.
Shape: usually oval.
Edge: punched – out.
Depth: deep, penetrating.
Tenderness: non – tender.
Surrounding tissue: chronic inflammatory tissue.
Character


plantar aspect of the first & fifth metatarsophalangeal joint

Neuropathic Ulcer
• Diagnostic features• The ulcer is painless.• The surrounding tissues are unable to appreciate pain.• The surrounding tissues may have normal blood supply.

INVESTIGATIONS

Investigations
• Angiography when visualization of the vessels of the lower extremities is desired.
• Magnetic resonance angiography (MRA) can also be useful when evaluating lower extremity disease.
• Doppler duplex scanning can detect venous reflux with a high sensitivity
• Ascending venography also may be considered to obtain detailed anatomic information. This study can reveal perforator incompetence, obstruction, and the presence of deep venous thrombosis.

Investigations
• Assess the vascular supply to the site of ulceration so that the likelihood of satisfactory wound healing may be estimated. Several methods of determining the adequacy of the pedal circulation are available.
• Ankle-brachial indices (ABIs) and toe digital pressures with pulse volume recordings can provide good clues to the perfusion of the foot.
• Xenon-133 clearance to measure blood flow can help estimate the chance of wound healing.
• Transcutaneous oxygen tension may be measured

MANAGEMENT

Conservative management
• Apply appropriate dressing to the ulcer.• Correct the underlying cause.• Relief of pain; analgesics.• Antibiotics• Elevation of the leg in venous ulcer.
Ischemic ulcer

Conservative management
• Basic requirements of the ideal ulcer dressing• Maintain high humidity between wound and dressing.• Absorbent, remove excess exudate.• Non – adherent, allowing easy removal w/o trauma at
dressing change.• Safe and acceptable to patient ( non – allergic).• Permit gaseous exchange but impermeable to micro –
organism.• Cost – effective.

Surgical management
Skin grafting: Once a clean granulating wound
bed has been established through debridement, placement
of a skin graft is usually all that is required to attain closure.
Skin grafting can be effective for coverage of venous ulcers,
Ischemic wounds located in areas that are difficult to treat.
Microvascular flap: has met with much success in the
treatment of arterial ulcers.
free tissue transfer: recently used for the treatment of venous ulcer and has mixed results.

THANK YOU