chronic kidney disease for the pcm you can make a difference!
TRANSCRIPT
Chronic Kidney DiseaseFor the PCM
YOU Can Make a Difference!
Goals and Objectives
• Review the K/DOQI definition and classification of chronic kidney disease (CKD)
• Review the prevalence and causes of CKD in the locally and in the USA.
• Understand the primary evaluation and management of patients with CKD.
Defining “CKD”
Kidney damage for ≥ 3 months, defined by structural or functional abnormalities of the kidney, with or without decreased GFR, manifest by either Pathologic abnormalities, or Markers of kidney damage, such as abnormalities
of the blood or urine, or in imaging tests (but NOT HTN).
GFR < 60 mL/min/1.73 m2 for ≥ 3 months with or without kidney damage.
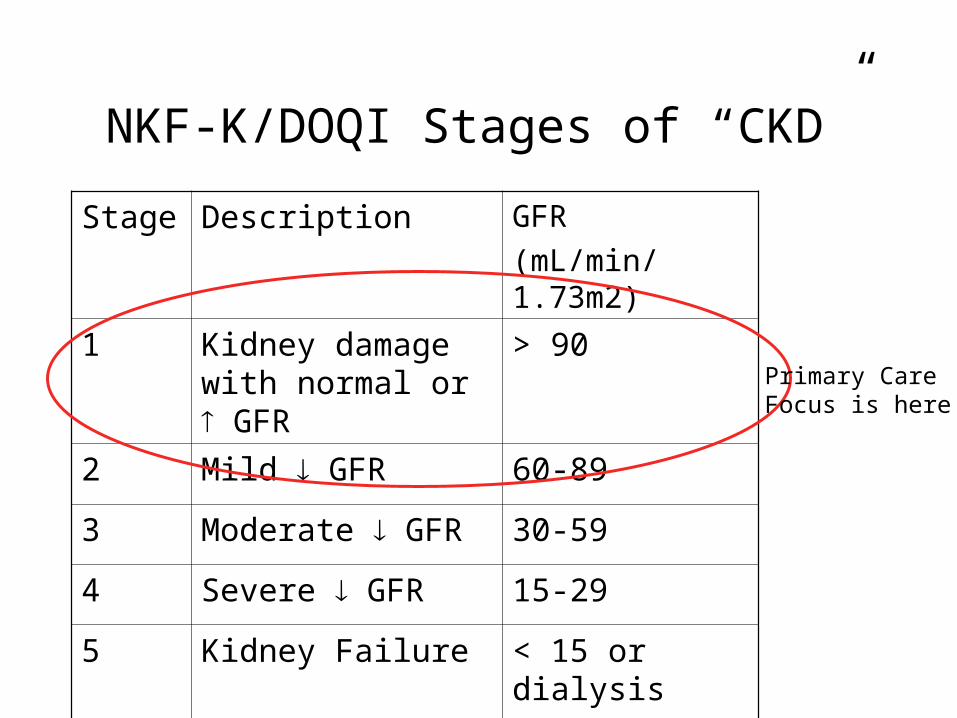
NKF-K/DOQI Stages of “CKD”
Stage Description GFR
(mL/min/1.73m2)
1 Kidney damage with normal or GFR
> 90
2 Mild GFR 60-89
3 Moderate GFR 30-59
4 Severe GFR 15-29
5 Kidney Failure < 15 or dialysis
Primary CareFocus is here!
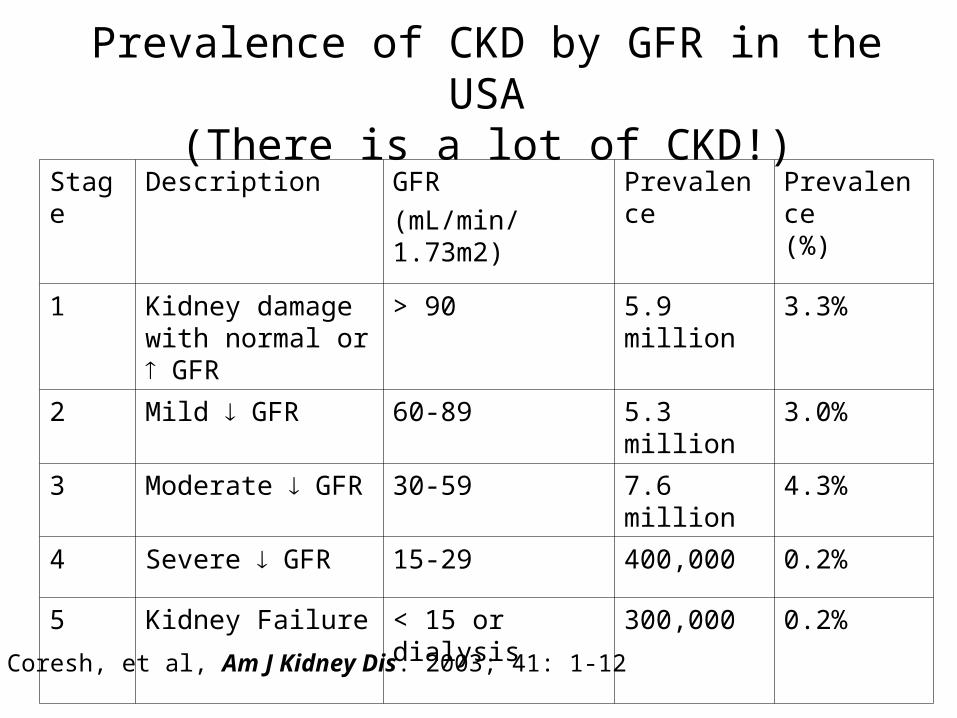
Prevalence of CKD by GFR in the USA(There is a lot of CKD!)
Stage Description GFR
(mL/min/1.73m2)
Prevalence Prevalence (%)
1 Kidney damage with normal or GFR
> 90 5.9 million 3.3%
2 Mild GFR 60-89 5.3 million 3.0%
3 Moderate GFR 30-59 7.6 million 4.3%
4 Severe GFR 15-29 400,000 0.2%
5 Kidney Failure < 15 or dialysis
300,000 0.2%
Coresh, et al, Am J Kidney Dis. 2003; 41: 1-12
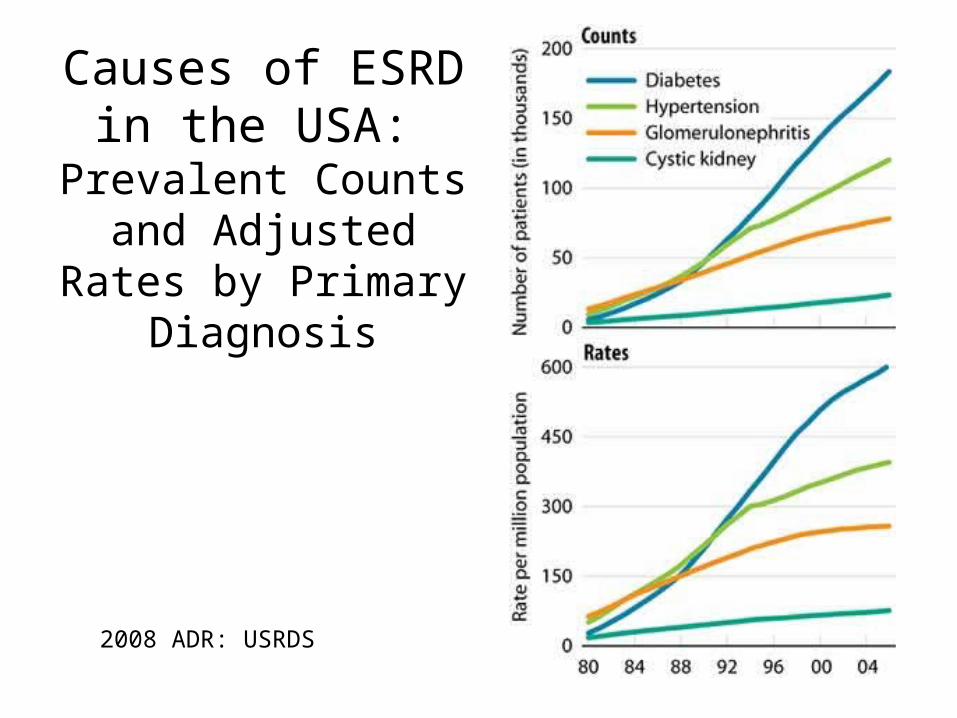
Causes of ESRD in the USA:
Prevalent Counts and Adjusted
Rates by Primary Diagnosis
2008 ADR: USRDS
Incidence of ESRD in the DC Metropolitan Area
• For the Washington DC Metropolitan area:– Incidence of ESRD
• White: 214 cases per million population• African American: 907 cases per million population• Hispanic: 330 cases per million population
– For comparison: Incidence in Pittsburgh, PA is 1265/million for African Americans, and 325 for caucasians.
(USRDS 2008 Annual Report, Table 2a, Vol 2.)
15 Dec 2008 “Zip Code” Report for DC Metropolitan Area
• 1787 prevalent ESRD (dialysis) patients. Top 4 Zip Codes (54% of patients):– 293 at 20019– 235 at 20020– 232 at 20011– 208 at 20002
• Basically, this is Southeast Washington.– 20019 is bounded in west by Kenilworth Ave; east by Rte 704;
south by Ft. Deposit Park; north by Eastern Ave.– 20020 is directly south of 20019.– 20011 bounded in west by 16th St; east by New Hampshire Ave;
south by USSAH, and north by WRAMC.– 20002 bounded in west by Bladensburg Rd; east by I395; south by
Constitution Ave, and north by NY Ave/Rte 50.
http://www.esrdnet5.org/zipcode.asp
Epidemiology of ESRD in Network 5 (MD, VA, WV, and DC)
• For DC– 390 incident ESRD (dialysis) patients– 1809 prevalent ESRD (dialysis) patients– 6 (1.5%) were under age 25– 25 (6%) were ≥ 85– 110 (28%) were 50-59--younger than in MD and VA (about
20% each)
• 51% Male• 87% African American• 35% DM; 38% HTN
MARC (Mid-Atlantic Renal Coalition) 2007 Annual Reporthttp://www.esrdnet5.org/2007ARDataTables.asp
Mortality Among Prevalent Dialysis Patients in the DC Metropolitan Area
(From the MARC 2007 Annual Report and 2005 Clinical Performance Measures Project)
• For DC– 286 deaths among prevalent ESRD (dialysis) patients– 64 (22%) were in patients 50-59 years old– 263 (92%) were African American– 94 (35%) had DM as the cause of ESRD– 124 (43%) had HTN as the cause of ESRD
• Primary cause of death was cardiac in 33% and infection in 17%.
• Clinical performance (reported in 2005):– Lowest rate of AV fistula placement in incident and prevalent HD
patients in the US.– 3rd highest use of dialysis catheters in the US.
http://www.esrdnet5.org/2007ARDataTables.asphttp://www.esrdnet5.org/cpm2005.asp

CKD Patients Are More Likely to Die than to Progress to ESRD
0% 20%
40%
60%
80%
100%
GFR 60-89, NoProteinuria
GFR 60-89; + Proteinuria
GFR 30-59
GFR 15-29
DiedRRTEvent FreeDisenrolled
Keith, et al, Arch Int Med; 2004; 164:659-663
5 year follow-up
N=27998
The Patient with early stage CKD is 5 to 10 times more
likely to die from a cardiovascular event than
progress to ESRD.
Foley RN, Murray AM, Li S, Herzog CA, McBean AM, Eggers PW, Collins AJ. Chronic kidney disease and the risk for cardiovascular disease, renal replacement, and death in the United States Medicare population, 1998 to 1999. J Am Soc Nephrol 2005; 16:489-95.
So what do we do about this?
• Screening for CKD
• Differential Diagnosis and Staging
• Clinical Action Plan– Delaying Progression of CKD– Managing Complications of CKD– Preparation and Referral for Renal
Replacement Therapy and Transplantation
See the KDOQI guidelines at:http://www.kidney.org/professionals/KDOQI/index.cfm
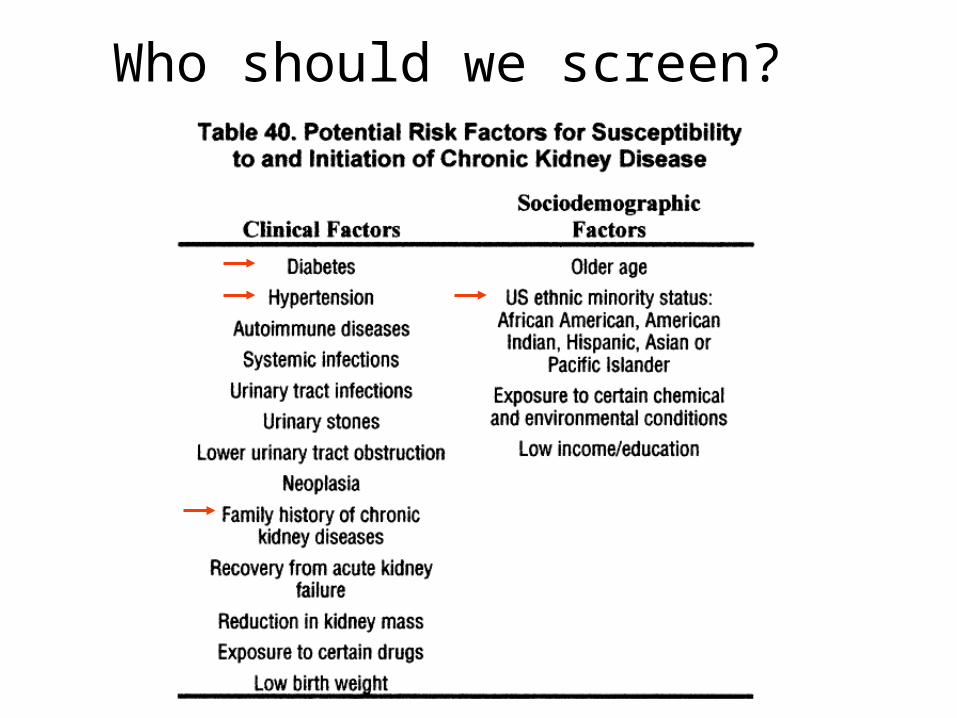
Who should we screen?

How should we screen?
Serum Creatinine, CrCl, and eGFR--Serum Creatinine, CrCl, and eGFR--Nothing is Perfect!Nothing is Perfect!
Serum Creatinine alone CAN NOT be used to accurately assess level of kidney function.
S. creatinine is a function of production (muscle mass) and excretion (both GFR and tubular secretion).
S. creatinine may be increased by some drugs, due to inhibition of creatinine secretion. These include: trimethoprim, cimetidine, flucytosine, and some cephalosporins.
Age, sex, and lean body mass have to be taken into account.
Estimations of eGFR (MDRD equation) and CrCl (Cockcroft-Gault equation) were NOT developed in subjects with normal renal function or normal health.
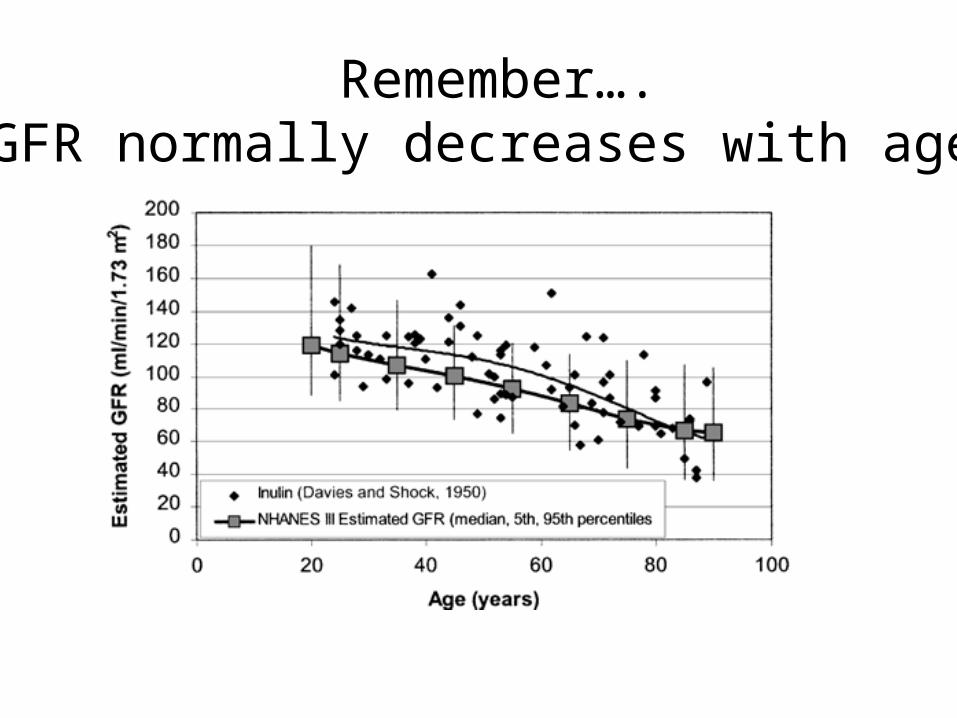
Remember….GFR normally decreases with age!
Cockcroft-Gault Equation to Predict GFR
• Developed to predict creatinine clearance (CrCl), thus an overestimate of GFR
• Prediction based on age, gender, creatinine and ideal body weight
• ClCr (cc/min) = [140-age] x IBW/72 x SCr x [0.85 if female]
• Used almost universally as the basis for drug dosing!
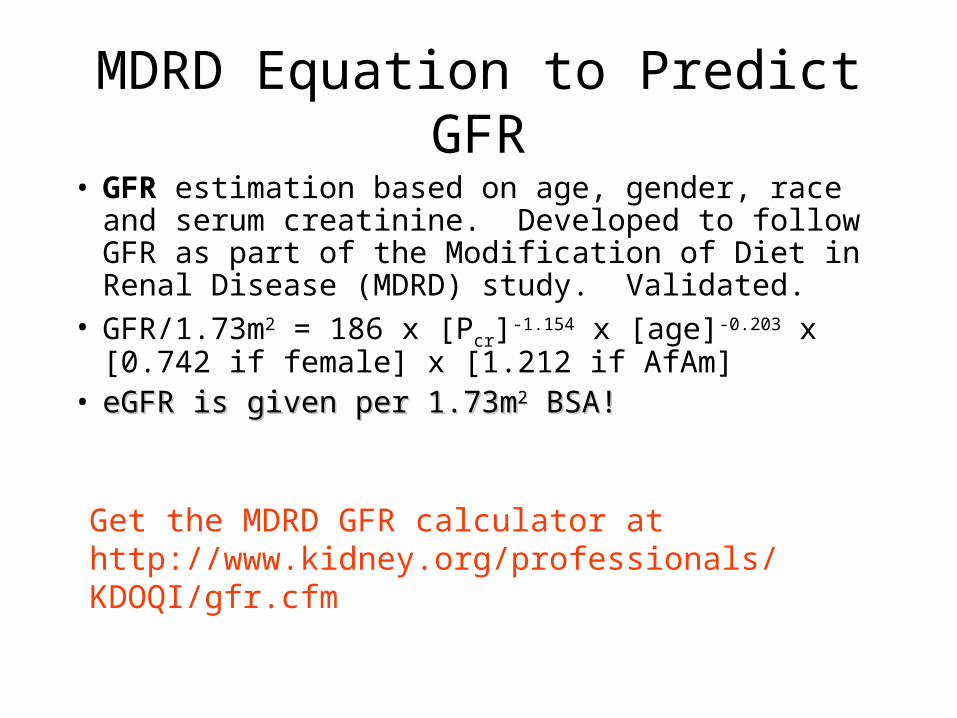
Get the MDRD GFR calculator athttp://www.kidney.org/professionals/KDOQI/gfr.cfm
MDRD Equation to Predict GFR
• GFR estimation based on age, gender, race and serum creatinine. Developed to follow GFR as part of the Modification of Diet in Renal Disease (MDRD) study. Validated.
• GFR/1.73m2 = 186 x [Pcr]-1.154 x [age]-0.203 x [0.742 if female] x [1.212 if AfAm]
• eGFR is given per 1.73meGFR is given per 1.73m22 BSA! BSA!
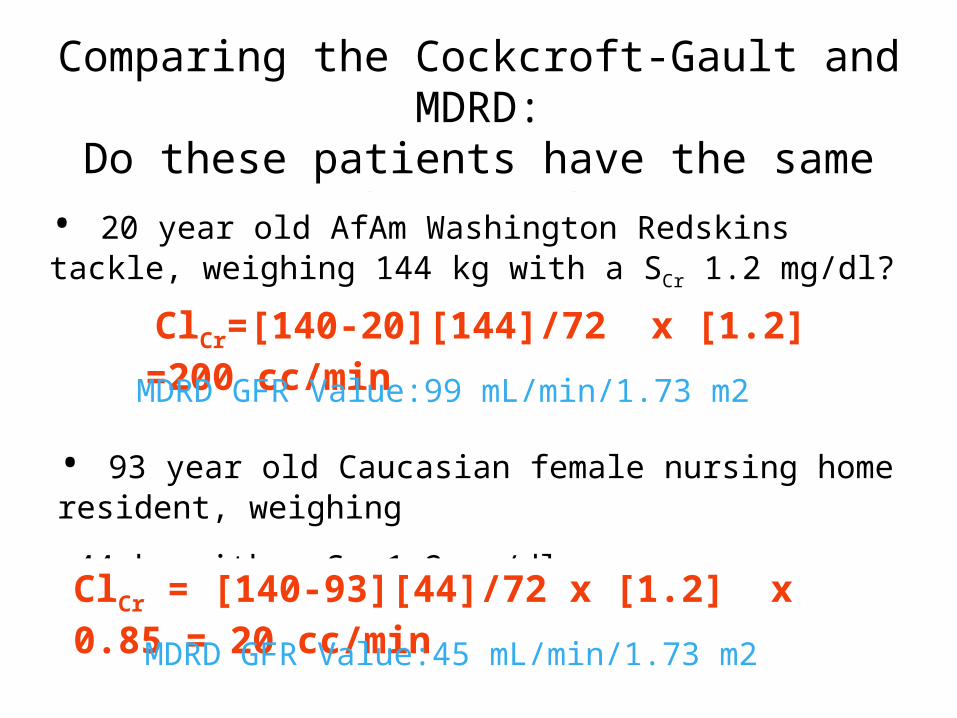
Comparing the Cockcroft-Gault and MDRD:Do these patients have the same level of renal
function?
• 20 year old AfAm Washington Redskins tackle, weighing 144 kg with a SCr 1.2 mg/dl?
ClCr=[140-20][144]/72 x [1.2] =200 cc/min
• 93 year old Caucasian female nursing home resident, weighing
44 kg with a SCr 1.2 mg/dl.
ClCr = [140-93][44]/72 x [1.2] x 0.85 = 20 cc/min
MDRD GFR Value:99 mL/min/1.73 m2
MDRD GFR Value:45 mL/min/1.73 m2

YES NO
Risk Factor ReductionDetermine Stage of CKD Determine underlying cause Identify risk factors for progression Identify comorbidites
Patient meets definition of Chronic Kidney Disease?
Tools for Determining the Cause of Chronic Kidney Disease
• CKD is often silent. Assessment relies on laboratory testing and imaging.
• A Good History! ROS, existence of chronic diseases (DM, HTN, CHF, cirrhosis), medication review, accurate PMH and FH of kidney disease.
• Helpful Physical Examination! BP, evidence of co-morbid conditions and complications of CKD.
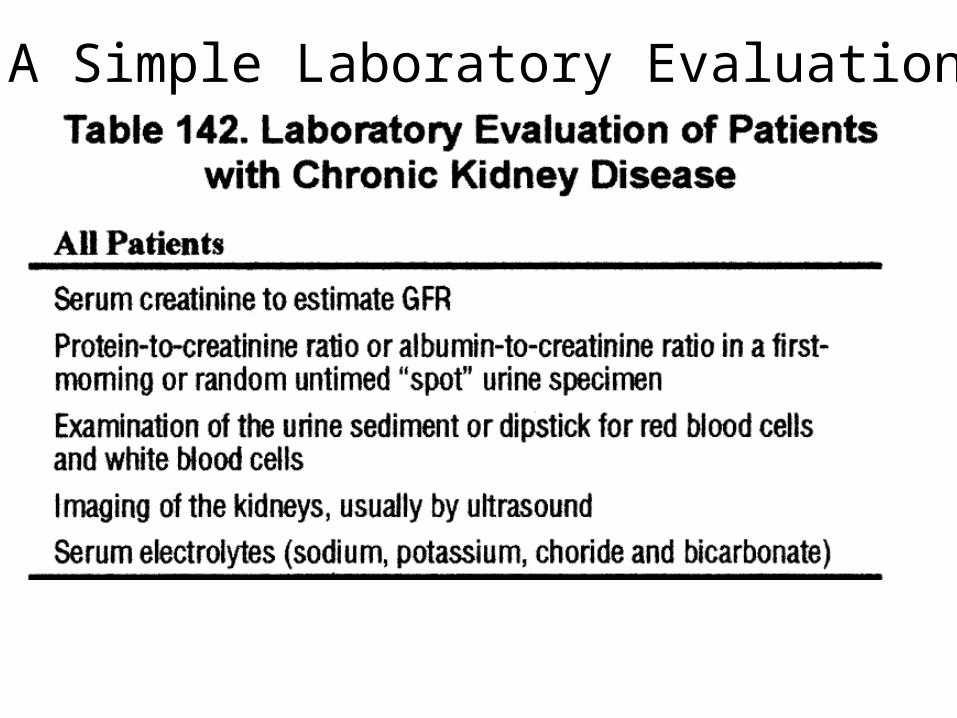
A Simple Laboratory Evaluation!
Simplified Classification of CKD by Diagnosis
• Diabetic Kidney Disease
• Nondiabetic Kidney Disease • Glomerular disease
– autoimmune, sytemic infections, drugs, neoplasia, idiopathic
• Vascular disease – ischemic renal disease, hypertensive
nephrosclerosis, microangiopathy
• Tubulointerstitial disease – UTO, stones, UTI, drug toxicity
• Cystic disease• Post-Transplant (get a T designator for their
CKD)
Differential Diagnosis of Chronic Kidney Disease
• Everyone deserves a diagnosis! • This is especially true for Stage 1 or 2 CKD!• When in doubt, consult a nephrologist!• Initial evaluation will guide further diagnostics,
decisions about renal biopsy and often decisions about treatment and prognosis.
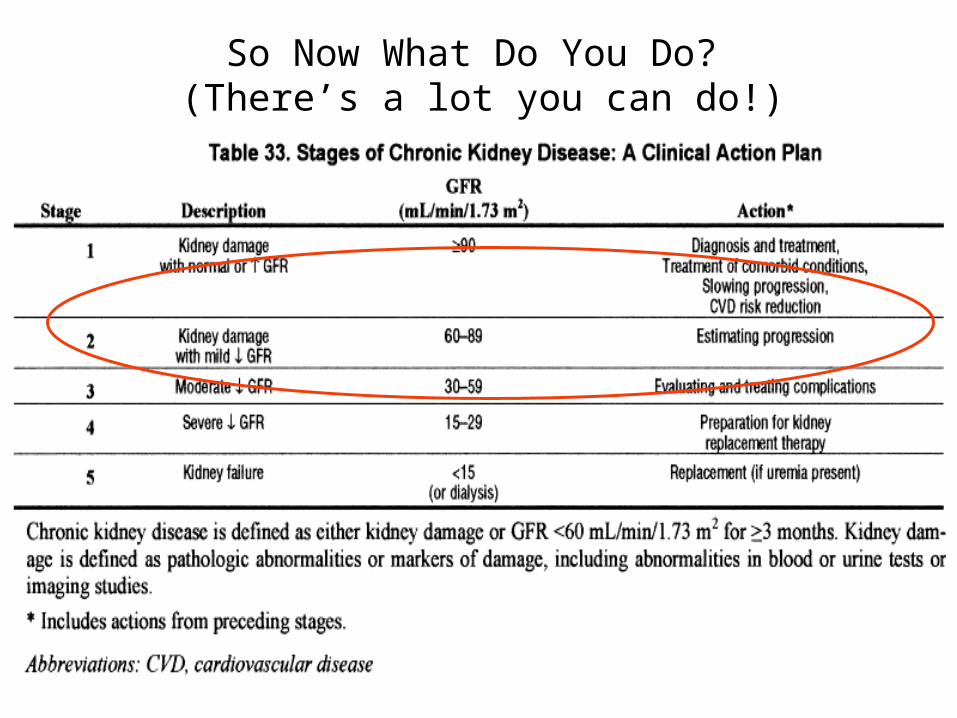
So Now What Do You Do? (There’s a lot you can do!)
Primary Goals of CKD Care
• To prevent cardiovascular events and death• Heart Attacks• Congestive Heart Failure• Sudden Cardiac Death• Stroke
• To prevent the progression of CKD • To prevent complications of CKD• To prepare for dialysis/transplantation in a
timely manner
Online CKD Clinical Action Plan available at:http://www.kidney.org/professionals/kdoqi/cap/index.html

Management of Patients with Chronic Kidney Disease
B lood g lu cose con tro l
B P C on tro l
A R B s
A C E In h ib ito rs
In te rven tion s th a t d e lay p rog ress ion
R ed u ced F u n c tion in g an d W e ll-b e in g
M a ln u trit ion
O s teod ys trop h y
A n em ia
P reven tion o f U rem ic C om p lica tion s(G F R < 6 0 cc /m in /1 .7 3 m 2 )
C ard iovascu la r D isease
M od ifca tion o f C om orb id ity
P re -em p tive Tran sp lan ta tion
K id n ey Tran sp lan t E va lu a tion
T im e ly D ia lys is In it ia tion
T im e ly D ia lys is A ccess P lacem en t
C h o ice o f D ia lys is M od a lity
E d u ca tionA n "E S R D C lin ic "
P rep ara tion fo r R en a l R ep lacem en t Th erap y(G R F < 3 0 cc /m in /1 .7 3 m 2 )
E arly D e tec tion o f C K D
Nonmodifiable Modifiable
Patient characteristics associated with increased rate of GFR decline
• African American race
• Male gender • Older age• Lower baseline level
of kidney function
• Higher level of proteinuria
• Higher BP • Poor glycemic
control • Smoking
Interventions that delay progression of CKD: ACEI and ARBs
• Mechanisms – Lower systemic blood pressure – Lower glomerular capillary blood pressure and
protein filtration (and thus, proteinuria)– Reduce AT II mediated cell proliferation and
fibrosis
Should be used in all proteinuric kidney diseases!
Interventions that delay progression of CKD: ACEI and ARBs
• Diabetic Kidney Disease – ACEI or ARB in ALL diabetic patients with microalbuminuria– ACEI (alt ARB) for Type 1 Diabetics with macroalbuminuria– ARB (alt. ACEI) in Type 2 Diabetics with macroalbuminuria
• Nondiabetic Kidney Disease – ACEI/ARB recommended in all proteinuric (>200 mg/g Cr on
spot urine) patients with CKD– ACEI and ARB may be used in combination, with caution
-KDOQI Guideline 8, Table 110
http://www.kidney.org/professionals/KDOQI/guideline_diabetes/pdf/Diabetes_AJKD_linked.pdf-JNC 7, 2003 http://www.nhlbi.nih.gov/guidelines/hypertension/express.pdf
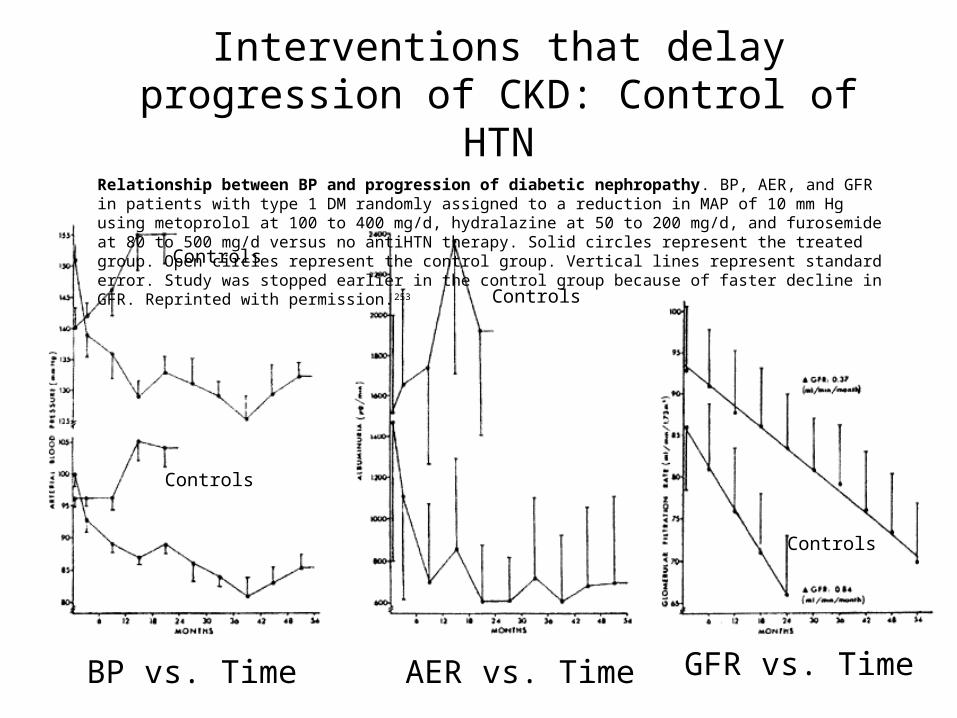
Interventions that delay progression of CKD: Control of HTN
Relationship between BP and progression of diabetic nephropathy. BP, AER, and GFR in patients with type 1 DM randomly assigned to a reduction in MAP of 10 mm Hg using metoprolol at 100 to 400 mg/d, hydralazine at 50 to 200 mg/d, and furosemide at 80 to 500 mg/d versus no antiHTN therapy. Solid circles represent the treated group. Open circles represent the control group. Vertical lines represent standard error. Study was stopped earlier in the control group because of faster decline in GFR. Reprinted with permission.253
BP vs. Time
Controls
AER vs. Time GFR vs. Time
Controls
Controls
Controls
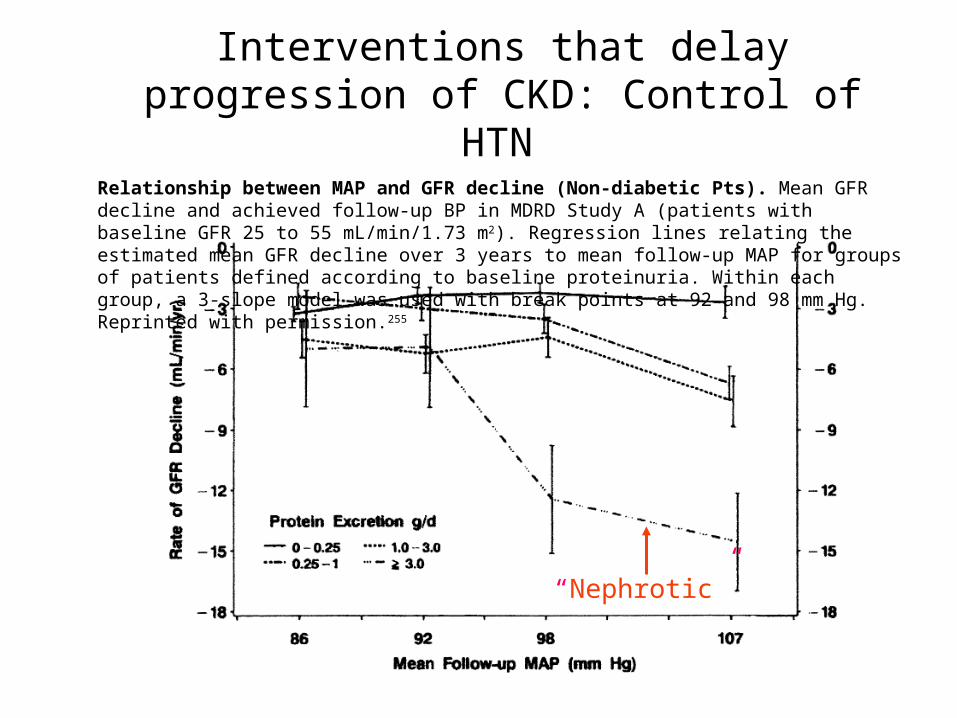
Interventions that delay progression of CKD: Control of HTN
Relationship between MAP and GFR decline (Non-diabetic Pts). Mean GFR decline and achieved follow-up BP in MDRD Study A (patients with baseline GFR 25 to 55 mL/min/1.73 m2). Regression lines relating the estimated mean GFR decline over 3 years to mean follow-up MAP for groups of patients defined according to baseline proteinuria. Within each group, a 3-slope model was used with break points at 92 and 98 mm Hg. Reprinted with permission.255
“Nephrotic”
• JNC-7 recommends goal BP <130/80 mm Hg for both diabetics and non-diabetics with HTN and CKD.
• All patients should begin a low sodium diet, optimize BMI, exercise, moderate ETOH use, and stop smoking!
• Diabetics should receive an ACEI/ARB first-line. Second agent should be a thiazide diuretic.
• Non-diabetics with > 200mg Protein/g urCr should receive an ACEI/ARB first-line. Second agent should be a thiazide diuretic.
• Non-diabetics with no proteinuria should receive a thiazide first-line. Second line therapy could probably be an ACEI/ARB or a BB.
• 3 or more drugs may be required! One will probably be a diuretic (thiazide first, then loop as GFR declines). Beta blockers and non-dihydropyridine CCBs are good third-line agents. Other agents may be used for specific indications.
• ACEI/ARB use is often associated with a “functional” rise in creatinine. Up to a 35% rise may be tolerated.
Interventions that delay progression of CKD: Recommendations for control of HTN
KDOQI Table 118, Guideline 9
http://www.nhlbi.nih.gov/guidelines/hypertension/express.pdf
Interventions that delay progression of CKD: Strict Glycemic Control
• Studies in both Type I and Type 2 DM with microalbuminuria show benefit in reducing progression to overt proteinuria and diabetic nephropathy. (DCCT, UKPDS 33, Steno Type 2)
• Recommended Therapy: – HgbA1c < 7% – Additional information in 2001 ADA Clinical Practice
Guidelines www.diabetes.org/clinicalrecommendations/Supplement101/
S3.htm
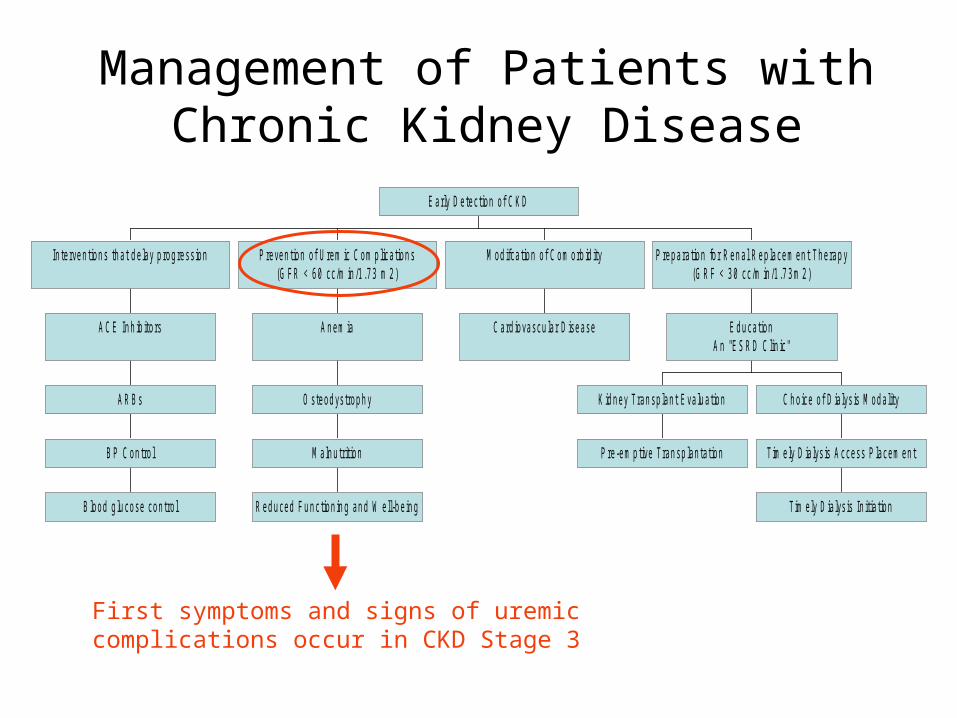
Management of Patients with Chronic Kidney Disease
B lood g lu cose con tro l
B P C on tro l
A R B s
A C E In h ib ito rs
In te rven tion s th a t d e lay p rog ress ion
R ed u ced F u n c tion in g an d W e ll-b e in g
M a ln u trit ion
O s teod ys trop h y
A n em ia
P reven tion o f U rem ic C om p lica tion s(G F R < 6 0 cc /m in /1 .7 3 m 2 )
C ard iovascu la r D isease
M od ifca tion o f C om orb id ity
P re -em p tive Tran sp lan ta tion
K id n ey Tran sp lan t E va lu a tion
T im e ly D ia lys is In it ia tion
T im e ly D ia lys is A ccess P lacem en t
C h o ice o f D ia lys is M od a lity
E d u ca tionA n "E S R D C lin ic "
P rep ara tion fo r R en a l R ep lacem en t Th erap y(G R F < 3 0 cc /m in /1 .7 3 m 2 )
E arly D e tec tion o f C K D
First symptoms and signs of uremiccomplications occur in CKD Stage 3
Prevention of Uremic Complications: Prevention of Uremic Complications: Evaluation and Management of AnemiaEvaluation and Management of Anemia
Anemia usually develops during the course of CKD and is primarily due to erythropoietin deficiency.
Adults with ≥ Stage 3 CKD: Assess Hemoglobin level If anemia (HgB ≤ 12)
RBC indices/CBC Reticulocyte count Iron studies Test for occult GI bleeding as indicated Medical evaluation of comorbid conditions
Erythropoetin levels are usually NOT indicated.
Prevention of Uremic Complications:Anemia Therapy
• Subcutaneous administration of erythropoietin once to thrice weekly (sometimes less).
• Supplemental oral or IV iron to keep ferritin > 100 and iron saturation >20%.
• Monthly monitoring of Hgb, iron stores.• Monthly adjustments in EPO dose and
frequency to meet target Hgb 11-12 g/dl (HCT 33-36%).
Prevention of Uremic Complications:Osteodystrophy
• Osteitis fibrosis cystica, due to 2o HPT, is major form of bone disease.
• Check indices of bone and mineral metabolism (Ca, PO4, iPTH, Alk Phos) at Stage 3 CKD (GFR < 60 cc/min/1.73m2) :– iPTH the earliest marker– Hypocalcemia, hyperphosphatemia – Phosphorus control is cornerstone of treatment
http://www.kidney.org/professionals/KDOQI/guidelines_bone/index.htm
Prevention of Uremic Complications:Osteodystrophy Therapy
• Restrict dietary phosphorus to 800-1,000 mg/d. • Start with calcium-based phosphate binders to
combat hypocalcemia and bind phosphorus. • Assure repletion of Vitamin D 25. • Avoid acidosis. Maintain HCO3> 23 mEq/l.• For patients at ≥ Stage CKD 3 with known
osteoporosis, treat as for the general population.• Bisphosphonates must be dose reduced if used in
patients with CKD and osteoporosis, and are NOT recommended in patients with CrCl < 30-35 cc/min.
Prevention of Uremic Complications:Malnutrition and Nutrition Guidelines• Malnutrition in CKD due to:
– low protein and calorie intake – metabolic acidosis – resistance to insulin, GH, IGF-1 – proinflammatory cytokines
• Assessment of nutritional status required.
• Protein intake – 0.75g/kg/d (RDA)
– GFR < 25 cc/min(Stages 4-5) consider 0.6g/kg/d
• Energy intake – RDA depends on energy expenditure
– GFR < 25 cc/min(Stages 4-5) 30-35kcal/kg/d • Patients with less than recommended intake need frequent follow-
up of nutritional status.
Prevention of Uremic Complications:Just a Word About Immunizations
• Don’t forget to continue routine immunizations, e.g.– Tetanus– Pneumococcus– Influenza
• Hepatitis B – Check for immunity first--ie, hepatitis B sAb, sAg, cAb – Those who are immune or have chronic infection do not
need the vaccine.– All others should receive the vaccine. Don’t wait for dialysis!
Patients with advanced chronic kidney disease are less likely to gain immunity from the vaccine. Consider for all Stage 3 or greater CKD patients!
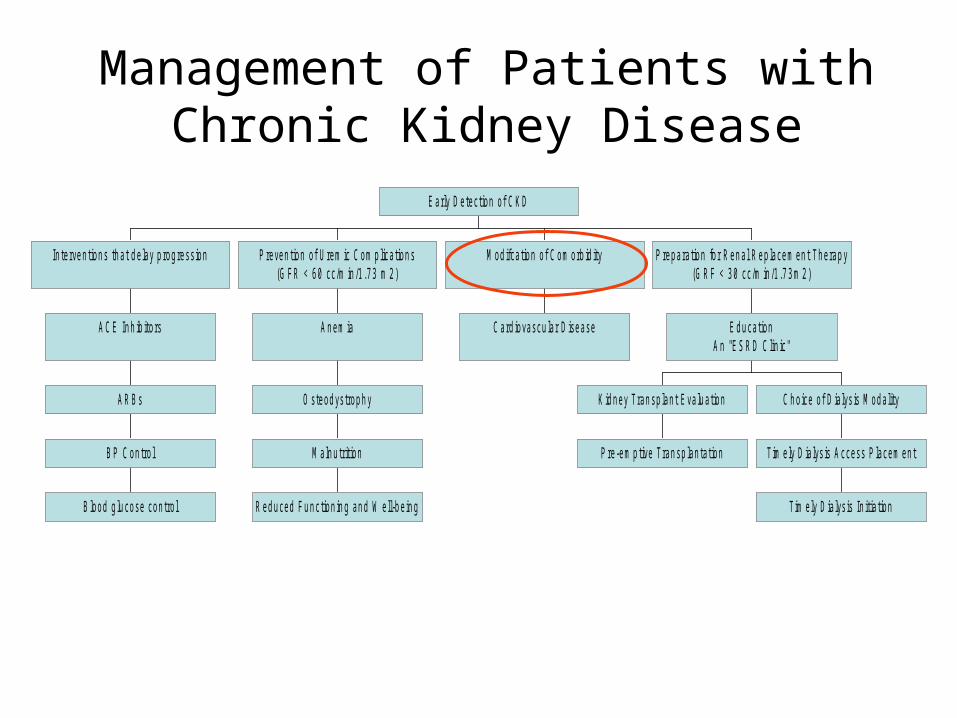
Management of Patients with Chronic Kidney Disease
B lood g lu cose con tro l
B P C on tro l
A R B s
A C E In h ib ito rs
In te rven tion s th a t d e lay p rog ress ion
R ed u ced F u n c tion in g an d W e ll-b e in g
M a ln u trit ion
O s teod ys trop h y
A n em ia
P reven tion o f U rem ic C om p lica tion s(G F R < 6 0 cc /m in /1 .7 3 m 2 )
C ard iovascu la r D isease
M od ifca tion o f C om orb id ity
P re -em p tive Tran sp lan ta tion
K id n ey Tran sp lan t E va lu a tion
T im e ly D ia lys is In it ia tion
T im e ly D ia lys is A ccess P lacem en t
C h o ice o f D ia lys is M od a lity
E d u ca tionA n "E S R D C lin ic "
P rep ara tion fo r R en a l R ep lacem en t Th erap y(G R F < 3 0 cc /m in /1 .7 3 m 2 )
E arly D e tec tion o f C K D
Modification of Comorbidity:Cardiovascular Disease
• CVD is the most common cause of death in ESRD patients--mortality rates 15x higher than general population.
• CVD is leading cause of death in patients with CKD, regardless of stage.
• Patients with CKD should be considered highest risk for CVD.
• Aggressive intervention and management of traditional CV risk factors is indicated.– All adults with Stage1-5 CKD should be evaluated for dyslipidemia.– Fasting lipid profile with total cholesterol, LDL, HDL and
triglycerides, at baseline, and at least annually.
Management of Dyslipidemia in CKD
Expert Panel on Detection Evaluation and Treatment of High Blood Cholesterol in Adults. Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA, 2001, 285;2486-2497.
http://www.kidney.org/professionals/KDOQI/guidelines_lipids/index.htm
• Diet, exercise, “lifestyle” changes are base of therapy. All dyslipidemic patients should receive dietary counseling.
• Goal LDL < 100. Statins are safe and effective, but may require dose reduction..
• Goal TG <500. Fibrates can be problematic in patients with CKD, but may be better tolerated than niacin.
• Await ongoing trials evaluating mortality and prevention of CV events specifically in patients with CKD not yet on dialysis.
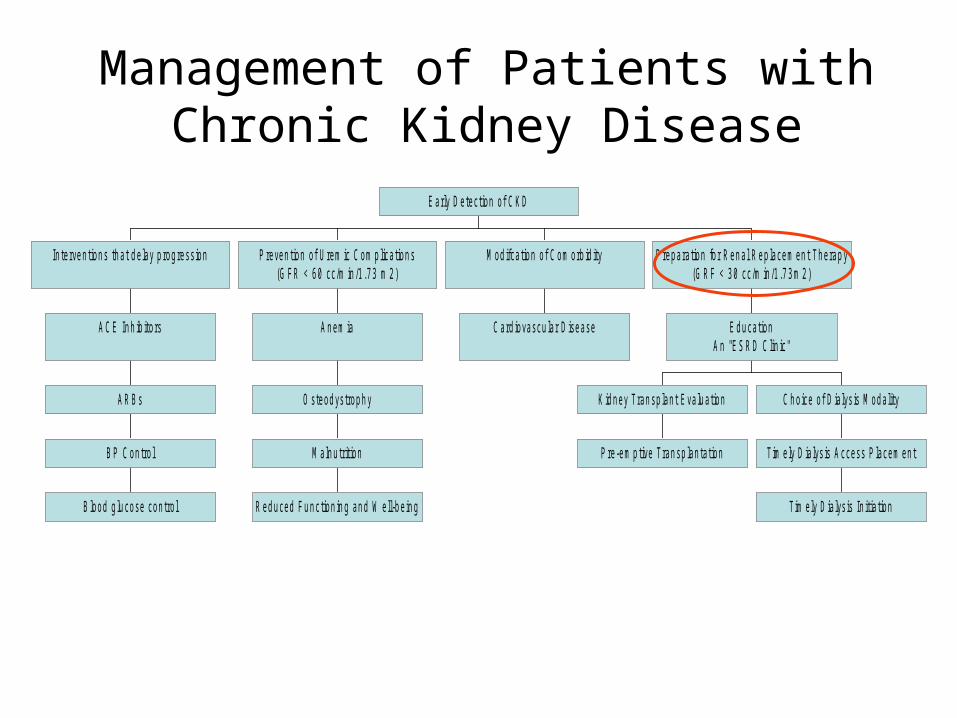
Management of Patients with Chronic Kidney Disease
B lood g lu cose con tro l
B P C on tro l
A R B s
A C E In h ib ito rs
In te rven tion s th a t d e lay p rog ress ion
R ed u ced F u n c tion in g an d W e ll-b e in g
M a ln u trit ion
O s teod ys trop h y
A n em ia
P reven tion o f U rem ic C om p lica tion s(G F R < 6 0 cc /m in /1 .7 3 m 2 )
C ard iovascu la r D isease
M od ifca tion o f C om orb id ity
P re -em p tive Tran sp lan ta tion
K id n ey Tran sp lan t E va lu a tion
T im e ly D ia lys is In it ia tion
T im e ly D ia lys is A ccess P lacem en t
C h o ice o f D ia lys is M od a lity
E d u ca tionA n "E S R D C lin ic "
P rep ara tion fo r R en a l R ep lacem en t Th erap y(G R F < 3 0 cc /m in /1 .7 3 m 2 )
E arly D e tec tion o f C K D
When to Refer!
• Consider co-management with a nephrologist if the clinical action plan cannot be carried out.
• Consider subspecialty referral when*: – Unexplained proteinuria (>1gm/day) or microalbumin/Cr ratio
>250mg albumin/gCr– Unexplained macroscopic or microscopic hematuria– Diabetes and macroalbuminuria– Multiple and recurring kidney stones– Rapidly deteriorating kidney function– Difficult to control hypertension
• Refer to a nephrologist when GFR <30 mL/min/1.73 m2 (CKD Stages 4-5)!
Mandatory Referral to Nephrologist guideline, Niagara Health Quality Coalition, NY
Preparation for Renal Replacement Therapy
(GFR < 30cc/min/1.73m2)
• Referral to a Nephrologist allows: – Early identification of RRT modality, with timely
dialysis access placement and initiation. – Evaluation for kidney transplantation with goal of
pre-emptive transplantation. – REMEMBER, in eligible patients transplantation
confers a survival advantage over dialysis!– Identification of social, functional or nutritional
needs.
Conclusions
• CKD is a public health problem with poor outcomes and high cost. CKD is under-diagnosed and under-treated in the U.S.
• Early CKD detection and intervention may increase opportunities for the prevention of ESRD and of complications of CKD, including death.
YOU, the PCM, CAN MAKE A Difference!