choroidal detachment associated with malignant choroidal tumors
TRANSCRIPT

Choroidal Detachment Associated with Malignant Choroidal Tumors SCOTT R. SNEED, MD; SANDRA F. BYRNE,2 WILLIAM F. MIELER, MD,3 DON H. NICHOLSON, MD,2 KARL OLSEN, MD,2 J. RANDALL HUGHES, BS2
Abstract: The association of choroidal detachment with malignant choroidal tumors is not well recognized. The authors' experience with six cases suggests that choroidal detachment may be associated with both metastatic tumors and choroidal melanoma. In two of these cases, the choroidal or retinal detachment was so massive that echography was necessary to detect the underlying tumor. Three patients presented with painful visual loss, and three patients presented with painless visual loss or a visual field defect. In one patient, the correct diagnosis and appropriate treatment of the choroidal metastasis with external radiation relieved the patient's pain and improved visual acuity from 1/200 to 20/35. Metastatic and primary uveal malignant tumors should be added to the list of causes of choroidal detachment and can be excluded only after thorough clinical, and often echographic, examination. Ophthalmology 1991; 98:963-970
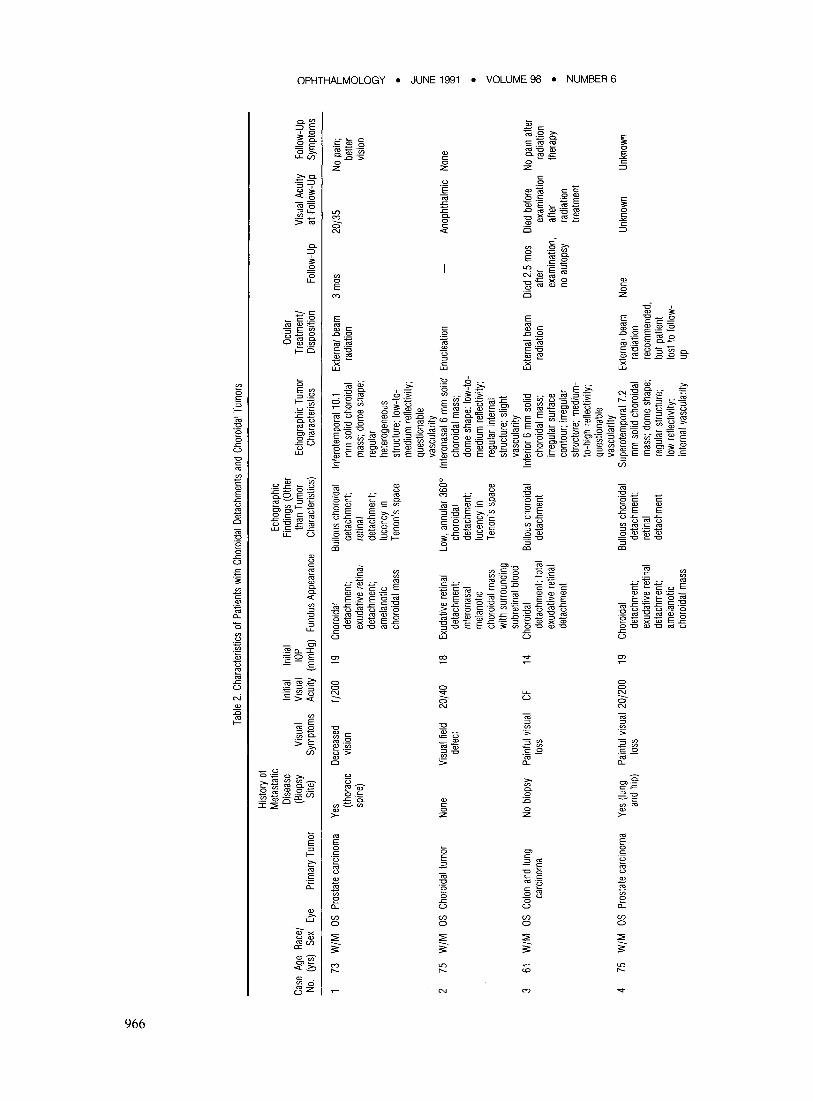
Choroidal detachments are associated with a number of processes (Table 1).1-19 However, the association of choroidal detachment with malignant choroidal tumors is not well recognized. We have treated six cases (Table 2) of malignant choroidal tumors associated with choroidal detachment. All patients were phakic men between the ages of 60 and 75 years. A choroidal detachment was recognized clinically in four cases and was documented echographically in all six cases. The following four case reports illustrate the features of this entity.
CASE REPORTS
Case 1. A 73-year-old white man developed a fairly well-differentiated adenocarcinoma of the prostate in 1979, which was
Originally received: July 3, 1990. Revision accepted: February 4, 1991 .
1 W.K. Kellogg Eye Center. Department of Ophthalmology, University of Michigan, Ann Arbor.
2 Bascom Palmer Eye Institute, University of Miami, Miami. 3 Medical College of Wisconsin, Department of Ophthalmology, Milwaukee.
Supported in part by an unrestricted grant from Research to Prevent Blind· ness, Inc, New York, New York, and the Florida Lions Eye Bank, Miami, Florida.
Reprint requests to Scott R. Sneed, MD, W. K. Kellogg Eye Center, 1000 Wall St, Ann Arbor, M148105.
treated with irradiation. In late 1983, severe pain developed in his thoracic spine, and biopsy of adjacent tissue showed a highly undifferentiated carcinoma. Results of endoperoxidase and melanin stains were negative. He noted a decrease in vision in his left eye in December 1983. In January 1984, visual acuity was 1/200 in the left eye. A relative afferent pupillary defect was present and applanation tension was 19 mmHg. Results of slitlamp examination showed minimal anterior segment inflammation with mild vitreous cells. Results of dilated ophthalmoscopic examination showed massive choroidal elevation, especially nasally, with an underlying amelanotic choroidal mass (Fig I). The choroidal elevation extended anteriorly in a 360 0
annular fashion and transilluminated brightly. The right eye was normal.
Results of echographic examination showed extensive choroidal detachments, a localized exudative retinal detachment, and a dome-shaped, solid mass inferotemporally extending from the posterior pole to the ciliary body, with maximal elevation of 10.1 mm. The mass exhibited slightly irregular internal structure with mainly low-to-medium reflectivity and questionable vascularity. A localized area of echolucency was noted in Tenon's space, immediately behind the mass (Fig 2).
Clinically, it was believed that this lesion represented a metastatic carcinoma to the choroid. The echographic findings were more suggestive of a melanoma than metastatic carcinoma; however, an anaplastic or small-cell carcinoma can so closely mimic the echographic pattern of melanoma that they are virtually indistinguishable. Because the biopsy of tissue adjacent to the spine, performed in late 1983, showed this tumor to be anaplastic, and because the clinical presentation and picture most
963

OPHTHALMOLOGY • JUNE 1991 • VOLUME 98 • NUMBER 6
Table 1. Differential Diagnosis of Choroidal Detachments
Entity Associated with Choroidal Detachment
After cataract extraction After glaucoma filtering procedures After retinal detachment surgery Trauma Harada's disease Sympathetic ophthalmia Posterior scleritis Pars planitis Toxoplasmosis Multiple myeloma Occlusive vasculitis Syphilis After panretinal photocoagulation Uveal effusion syndrome Malignant hypertension Carotid cavernous fistulas Rhegmatogenous retinal detachments Nanophthalmos Myxedema Sporadic
suggested a metastatic lesion, external radiation therapy was recommended.
Three thousand rad of external beam radiation therapy were administered to the left eye in 10 treatment fractions over 13 days. The patient was seen 3 months after radiation treatment. Examination of the left eye documented a visual recovery to 20/35 with normal intraocular pressure and anterior segment findings. There was a minimal left relative afferent pupillary defect. Results of dilated ophthalmoscopic examination showed marked retinal pigment epithelial dispersion with curvilinear hi~-water marks, indicating the pattern of regressed choroidal elevation (Fig 3). There was no choroidal thickening and the retina was attached.
Case 2. A 75-year-old white man, who was previously healthy, noticed a visual field defect in the left eye 1 day before examination.
Evaluation of the right eye was normal. Visual acuity in the left eye was 20/25, intraocular pressure was 18 mmHg, and there was a left relative afferent pupillary defect. The anterior chamber was deep and quiet. Results of dilated ophthalmoscopic examination showed an inferonasal pigmented choroidal mass approximately 10 mm in diameter with an extensive inferior retinal detachment. A clinical diagnosis of malignant melanoma with secondary retinal detachment was made and potential therapeutic options were discussed with the patient.
When the patient returned the next day for echographic examination, the eye had become red and painful. Visual acuity was 20/40, and intraocular pressure was 28 mmHg. The anterior chamber was flat with occlusion of the trabecular meshwork. Gonioscopy showed a grade four open angle in the right eye and a closed angle in the left eye. The ciliary body in the left eye was believed to be rotated anteriorly. Results offundus examination showed a 3600 choroidal detachment that transilluminated brightly. The tumor and retinal detachment were clinically unchanged.
Results of echographic examination showed a 6-mm domeshaped tumor inferonasally, which had fairly regular internal structure, low-to-medium reflectivity, and was slightly vascular. Reflectivity of the sclera behind the tumor was reduced, suggesting infiltration by inflammatory or tumor cells. Furthermore,
964
Reference
Swyers, 19721
Berke et ai, 19872
Packer et ai, 19833
Zentmayer, 19244
Hertz, 19545
de Veer, 19526
Sears, 19647
Brockhurst et ai, 19608, 1961 9
Green, 198510
Green, 198510
Green, 198510
Deluise et ai, 198211
Huamonte et ai, 197612
Schepens and Brockhurst, 196313
Friedman et ai, 196414
Guerry et ai, 197515
Gottlieb, 197216
Brockhurst, 197517
Richardson and Walsh, 196918
Velzeboer, 196019
there was diffuse echolucency in the adjacent Tenon's space, a finding that is commonly associated with scleritis. However, a component of extrascleral extension could not be ruled out. There was extensive retinal detachment inferiorly, and there were low, annular ciliochoroidal detachments 3600 (Fig 4).
The clinical and echographic examinations were most consistent with a malignant melanoma. Because of the pain and irritation from the secondary glaucoma, an enucleation was performed. Results of histopathologic examination of the left eye showed a pigmented mass with extensive hemorrhagic necrosis arising from the inferior choroid. The plump cells in the periphery displayed large nuclei with prominent nucleoli (Fig 5), findings consistent with a malignant melanoma. A hemorrhagic retinal detachment was present and the adjacent choroid was detached and filled with erythrocytes as well as acute and chronic inflammatory cells (Fig 6). There was no tumor infiltration in the sclera. The episclera was infiltrated with inflammatory cells.
Case 3. A 61-year-old white man underwent a colostomy for colon cancer in 1982, and in August 1986 he underwent radiotherapy for lung cancer. He presented on April 16, 1987, with a I-month history of mild visual field distortion in the left eye. One week before evaluation, he developed severe pain in the left eye, which kept him awake at night.
Evaluation of the right eye was normal. Visual acuity in the left eye was finger counting and there was a left relative afferent pupillary defect. Intraocular pressure in the left eye was 14 mmHg. Results of slit-lamp examination of the left eye showed a shallow temporal anterior chamber with a clear lens. Results of dilated fundus examination of the left eye showed extensive choroidal detachments nasally, temporally, and superiorly with a total exudative retinal detachment (Fig 7). No definite metastasis could be seen by indirect ophthalmoscopy.
Results of echographic examination of the left eye showed an extensive bullous choroidal detachment with a total retinal detachment (Fig 8). There was a solid choroidal lesion inferiorly with greatest elevation near the ora serrata at the 6-0'clock position. The lesion had irregular internal structure and questionable vascularity (Fig 9). The lesion was maximally elevated at 6mm.
The history and echographic examination were most consis-

SNEED et al • CHOROIDAL DETACHMENT
Fig 1. Case 1. Fundus photograph of the choroidal mass (arrow) with the choroidal detachment extending nasally and partly obscuring the disc.
Fig 2. Case 1. Top. transverse B-scan at high sensitivity (gain) setting. Bullous, exudative choroidal detachment (C) inserts into tumor (white arrow). Diffuse echoes beneath choroidal indicate exudate rather than serous fluid. Center. tumor is better delineated at medium sensitivity setting and lucent area (black arrow) is displayed in Tenon's space. Bottom. standardized A-scan at tissue sensitivity setting. High tumor surface spike is followed by a chain of medium to low internal tumor spikes (small arrow). Large arrow indicates lesion in Tenon's space.
Fig 3. Case 1. Fundus photograph, 3 months after radiation therapy. Notice the curvilinear high-water marks that indicate the pattern of tumor regression.
Fig 4. Case 2. Top left. B-scan shows dome-shaped mass with diffuse echolucency in Tenon's space (arrow), corresponding to inflammation. Bottom left. standardized A-scan at tissue sensitivity setting shows tumor is medium reflective. Scleral spike (S) is decreased in height. Small arrow = inflammation in Tenon's space. Curved arrow = Tenon's capsule. Top right. longitudinal B-scan of tumor (T) and peripheral, ciliochoroidal detachment (C). Bottom right. vertical transverse section through far nasal periphery shows retinal detachment (R) and choroidal detachment (C).
tent with a metastatic choroidal tumor associated with choroidal and retinal detachments.
Four thousand rad of palliative radiation therapy were administered to the left eye in a split course with 20 applications over 35 days.
The patient died 6 weeks after completion of the radiation treatment. No fundus examination was obtained after the radiation treatment, however, by history, the patient had marked resolution of the pain in his left eye after radiation therapy. An autopsy was not performed.
Case 4. A 75-year-old white man was diagnosed with prostatic carcinoma in 1979 with initial hormonal therapy and transurethral resection ofthe prostate. Metastases to the lung were identified in July 1984 and to the hip in January 1985, for which he received radiation therapy. He was initially seen on January 30,
965
'D
0\
0\
Case
Ag
e Ra
ce/
No.
(yrs
) Se
x Ey
e Pr
imar
y Tu
mor
73
W/M
as
Pro
stat
e ca
rcin
oma
2 75
W
/M
as C
horo
idal
tum
or
3 61
W
/M
as C
olon
and
lung
ca
rcin
oma
4 75
W
/M
as P
rost
ate
carc
inom
a
Hist
ory
of
Met
asta
tic
Dise
ase
(Bio
psy
Site
)
Yes (th
orac
ic sp
ine)
None
No b
iops
y
Yes
(lung
an
d hi
p)
Tabl
e 2.
Cha
ract
erist
ics o
f Pat
ient
s w
ith C
horo
idal
Det
achm
ents
and
Cho
roid
al T
umor
s
Echo
grap
hic
Initia
l In
itial
Find
ings
(O
ther
O
cula
r Vi
sual
Vi
sual
lO
P th
an T
umor
Ec
hogr
aphi
c Tu
mor
Tr
eatm
ent/
Sym
ptom
s Ac
uity
(m
mH
g)
Fund
us A
ppea
ranc
e C
hara
cter
istics
) C
hara
cter
istics
D
ispos
ition
Decr
ease
d 1/
200
19
Cho
roid
al
Bullo
us c
horo
idal
In
fero
tem
pora
l 10.
1 Ex
tern
al b
eam
vis
ion
deta
chm
ent;
deta
chm
ent;
mm
sol
id c
horo
idal
ra
diat
ion
exud
ative
ret
inal
re
tinal
m
ass;
dom
e sh
ape;
de
tach
men
t; de
tach
men
t; re
gula
r am
elan
otic
luce
ncy
in he
tero
gene
ous
chor
oida
l mas
s Te
non'
s sp
ace
stru
ctur
e; lo
w-to
-m
ediu
m r
efte
ctivi
ty;
ques
tiona
ble
vasc
ular
ity
Visu
al f
ield
20
/40
18
Exud
ative
ret
inal
Lo
w, a
nnul
ar 3
600
Infe
rona
sal 6
mm
sol
id
Enuc
leat
ion
defe
ct
deta
chm
ent;
chor
oida
l ch
oroi
dal m
ass;
in
fero
nasa
l de
tach
men
t; do
me
shap
e; lo
w-to
-m
elan
otic
luce
ncy
in m
ediu
m r
efle
ctivi
ty;
chor
oida
l mas
s Te
non's
spa
ce
regu
lar
inte
rnal
w
ith s
urro
undi
ng
stru
ctur
e; s
light
su
bret
inal
blo
od
vasc
ular
ity
Pain
ful v
isual
CF
14
C
horo
idal
Bu
llous
cho
roid
al
Infe
rior
6 m
m s
olid
Ex
tern
al b
eam
lo
ss
deta
chm
ent;
tota
l de
tach
men
t ch
oroi
dal m
ass;
ra
diat
ion
exud
ative
ret
inal
irr
egul
ar s
urfa
ce
deta
chm
ent
cont
our;
irreg
ular
st
ruct
ure;
med
ium
-to
-hig
h re
flect
ivity
; qu
estio
nabl
e va
scul
arity
Pa
infu
l visu
al 2
0/20
0 19
C
horo
idal
Bu
llous
cho
roid
al
Supe
rote
mpo
ral 7
.2
Exte
rnal
bea
m
loss
de
tach
men
t; de
tach
men
t; m
m s
olid
cho
roid
al
radi
atio
n ex
udat
ive r
etin
al
retin
al
mas
s; d
ome
shap
e;
reco
mm
ende
d,
deta
chm
ent;
deta
chm
ent
regu
lar
stru
ctur
e;
but
patie
nt
amel
anot
ic lo
w re
flect
ivity
; lo
st to
follo
w-
chor
oida
l mas
s in
tern
al v
ascu
larit
y up
Visu
al A
cuity
Fo
llow
-Up
0 Fo
llow
-Up
at F
ollo
w-U
p Sy
mpt
oms
"1J
I --I
I 3
mas
20
/35
No p
ain;
l>
r
bette
r s: 0
visio
n 5 (j
) -< • c..
.. c z m
Anop
htha
lmic
None
~ • <
0 r c s:
Died
2.5
mas
Di
ed b
efor
e No
pai
n af
ter
m
<0
af
ter
exam
inat
ion
radi
atio
n co
ex
amin
atio
n,
afte
r th
erap
y •
no a
utop
sy
radi
atio
n z
treat
men
t c s: ro
m
::0
(j
)
None
Un
know
n Un
know
n

~
'" =J:_ xc.'" ~E-g (/.)~C:
'" >-
'" E o c .~
'" g c
'" "'C
'" 0> C ::> -' Cl o
o o N
M
i;;' c. o :c o z
'" E o c '0 (;j '-' 0> C ::> -' U) o
SNEED et aI • CHOROIDAL DETACHMENT
1985, at which time he was receiving hormonal therapy and prednisone. He presented with a 3-week history of left-sided head pain and decreased vision in the left eye.
Evaluation of the right eye was normal. Visual acuity in the left eye was 20/200 and there was a left relative afferent pupillary defect. Intraocular pressure in the left eye was 19 mmHg. Results of slit-lamp examination of the left eye showed a mild narrowed anterior chamber with a clear lens. Results of dilated fundus examination of the left eye showed a normal disc with a large hypopigmented choroidal tumor in the superotemporal periphery (Fig 10). Inferior to this and extending inferiorly and nasally to the II-o'clock position, there was a choroidal detachment with some minimal secondary exudative retinal detachment inferiorly. There also was a shallow choroidal detachment superiorly, extending from the tumor mass and engaging the nasal choroidal detachment (Fig 11).
Results of echographic examination (Figs 12 and 13) of the left eye showed a solid, dome-shaped, low reflective vascularized lesion superotemporally with maximal elevation of7.2 mm. Extensive bullous choroidal detachments were present.
Although the ultrasound was most consistent with a malignant melanoma, with the patient's history and the clinical appearance, a diagnosis of metastatic carcinoma of the choroid with associated choroidal detachments was made. Radiation therapy was recommended, however, the patient was lost to follow-up.
DISCUSSION
Choroidal detachment associated with a malignant choroidal tumor is not well recognized and has been documented in one case of malignant melanoma associated with trauma20 and in four cases of malignant tumors metastatic to the choroidy-24
In 1977, Kline et afo reported a case of posttraumatic hemorrhagic choroidal and retinal detachments. Initial B-scan echography showed a homogeneous "shadow" under the choroid, almost filling the vitreous cavity. There was an area of increased density, which was believed to be a subchoroidal hemorrhage. An underlying tumor could not be ruled out. One month later, the B-scan findings were unchanged. The eye was removed 2 months later, after the development of panophthalmitis. Results of microscopic examination showed a choroidal melanoma in the area, which was believed to have been a choroidal hemorrhage on B-scan. There was a localized ciliary body detachment with a proteinaceous exudate in the suprachoroidal spaGe.
Four cases of carcinoma metastatic to the choroid have been reported in association with choroidal detachment. In 1969, Kreiger et aJ22 reported a case presenting with extensive choroidal detachments and suspected metastatic disease. Echography was not performed. Five months later, the patient died and results of histologic examination showed the choroid to be densely infiltrated with nodules of undifferentiated carcinoma cells, probably of pulmonary origin. The choroid was almost completely infiltrated with tumor cells, however, no choroidal detachment was present. In 1953, Taake et at21 reported a histopathologic examination of an eye with choroidal metastases from a
967

OPHTHALMOLOGY • JUNE 1991 • VOLUME 98 • NUMBER 6
Fig 5. Case 2. Histopathologic specimen of area of viable tumor demonstrating cells with large nuclei and prominent nucleoli (hematoxylineosin; original magnification, x250).
Fig 6. Case 2. Choroidal effusion (star) separates lamella of choroidal stroma at the anterior border of partially necrotic, hemorrhagic tumor (black arrow) (hematoxylin-eosin; original magnification, X44).
Fig 7. Case 3. Fundus photograph shows the retinal detachment (left) and the smooth, dome-shaped choroidal detachment (right).
968
Fig 8. Case 3. Choroidal and retinal detachments. Top, longitudinal Bscan at medium-high gain setting shows peripheral dome-shaped choroidal detachments (C) and retinal detachment (arrow) inserting into the optic disc. Bottom, corresponding standardized A-scan at tissue sensitivity shows thick, highly reflective spikes from choroidal detachment (C). Retinal detachment (arrow) produces lower reflective spike due to oblique sound beam incidence.
hepatoma and an associated choroidal detachment, although clinical details were not reported. Stephens and Shields,24 in their 1979 review of 70 cases of metastatic cancer to the uvea, described a single case of a choroidal metastasis with an associated choroidal detachment. Their patient had metastatic melanoma from the skin to the choroid and presented with glaucoma secondary to a hemorrhagic detachment of the choroid and ciliary body. In 1976, Eichholtz23 reported a patient who presented with a 3-week history of painful visual loss in the right eye. A large choroidal detachment was noted nasally and an exudative retinal detachment temporally. No tumor was detected by transillumination or echography. The left eye was normal. The right eye was enucleated for relief of pain. Results of pathologic examination showed tumor cells in the ciliary body, peripheral choroid, and invading the blood vessels. The peripheral choroid and ciliary body were detached. Nuchal lymph nodes and a change on the chest x-ray were noted, but a complete medical evaluation was not completed before the patient died 14 days later. An autopsy was not performed.
All six cases in the current series were noted in phakic elderly men. Painful visual loss was present in three of

SNEED et al • CHOROIDAL DEl ACHMENT
Fig 9. Case 3. Tumor, choroidal, and retinal detachments. Top, B-scan, taken at medium-high gain setting, shows mass (arrows) with irregular appearance. Notice overlying retinal detachment (R) and elevated choroidal detachment (C) extending from tumor margins. BOl/om, standardized A-scan at tissue sensitivity shows highly elevated choroidal detachment beneath probe (C) and tumor in opposite fundus (arrow). Slightly detached retina (R), tumor surface (T), sclera (S). Notice high internal reflectivity and irregular internal structure of tumor.
the six patients, and decreased vision or a visual field defect was present in the remaining cases. Results of echographic examination of all six cases showed a solid choroidal mass associated with a serous choroidal detachment (the choroidal detachment was bullous in five of the six cases). Five of the six cases presented with exudative retinal detachment, and in one case (case 5) the retinal detachment was so extensive that the underlying tumor and choroidal detachment were not seen clinically and were identified only after echographic examination. The choroidal tumor was noted ophthalmoscopically in four cases (three were amelanotic and one was melanotic). In the other two cases (case 3 and case 5) the tumor was identified with echography.
A dramatic improvement was noted in case 1 after external beam radiation therapy (visual acuity improved,
Fig 10. Case 4. Fundus photograph shows the amelanotic choroidal tumor superotemporally and the nasal, inferior, and inferotemporal choroidal detachment, which is somewhat out of focus due to its elevation.
Fig 11. Case 4. Fundus photograph of the left eye shows the amelanotic choroidal tumor superotemporally (right) with the associated choroidal detachment superiorly and superonasally (left).
Fig 12. Case 4. Peripheral choroidal detachment. Transverse B-scan through peripheral globe shows bullous choroidal detachment with typical scalloped appearance.
969

OPHTHALMOLOGY • JUNE 1991 • VOLUME 98 • NUMBER 6
Fig 13. Case 4. Tumor with associated choroidal detachment. Top, transverse B-scan shows dome-shaped tumor (arrow). Elevated choroidal detachment (C) extends from tumor margin. Bottom, standardized Ascan at tissue sensitivity shows low to medium reflective tumor (arrow) with slightly irregular internal structure. Tumor surface (T), sclera (S).
pain subsided, and the tumor and choroidal detachment disappeared). Clinical improvement was also noted in case 6 after external beam radiation (visual acuity improved and the tumor size decreased). A third patient (case 3) improved clinically with pain relief after radiation treatment, however, this patient was not seen by an ophthalmologist before his death.
We de~ribe the clinical and echographic characteristics in eyes harboring malignant choroidal tumors that are associated with choroidal detachments. Although the association of malignant choroidal tumors and choroidal detachment has been described previously,20-24 malignant choroidal tumors are not included in most tables listing causes of choroidal detachment. Because of our experience with these six cases, we believe that metastatic and primary malignant choroidal tumors should be added to the list of causes of choroidal detachment and can be excluded only after thorough clinical and often echographic ex-
970
amination. Eyes harboring a metastatic tumor with a choroidal detachment may respond well to external beam radiation.
REFERENCES
1. Swyers EM. Choroidal detachment immediately following cataract ex· traction. Arch Ophthalmol1972; 88:632-4.
2. Berke SJ, Bellows AR, Shingleton BJ, et al. Chronic and recurrent choroidal detachment after glaucoma filtering surgery. Ophthalmology 1987; 94:154-62.
3. Packer AJ, Maggiano JM, Aaberg TM, et al. Serous choroidal detachment after retinal detachment surgery. Arch Ophthalmol 1983; 101 :1221-4.
4. Zentmayer W. Traumatic detachment of the choroid. Trans College Physicians Philadelphia 1924 (3rd ser.); 46:338-9.
5. Hertz V. Choroidal detachment with notes on scleral depression and pigmented streaks in the retina. Acta Ophthalmol [Suppl] 1954; 41: 159.
6. de Veer JA Sympathizing eye in sympathetic ophthalmia: a pathologic study. Arch Ophthalmol1952; 48:723-37.
7. Sears ML. Choroidal and retinal detachments associated with scleritis. Am J Ophthalmol1964; 58:764-6.
8. Brockhurst RJ, Schepens Cl, Okamura 10. Uveitis. II. Peripheral uveitis: clinical description, complications and differential diagnosis. Am J Ophthalmol1960; 49:1257-66.
9. Brockhurst RJ, Schepens Cl, Okamura 10. Uveitis. III. Peripheral uveitis: pathogenesis, etiology and treatment. Am J Ophthalmol 1961; 51: 19-26.
10. Green WR. Retina. In: Spencer WH, ed. Ophthalmic Pathology: An Atlas and Textbook, 3rd ed. Vol 2. Philadelphia: W.B. Saunders, 1985;1178-91.
11. Deluise VP, Clark SW III, Smith Jl, Collart P. Syphilitic retinal detachment and uveal effusion. Am J Ophthalmol1982; 94:757-61.
12. Huamonte FU, Peyman GA, Goldberg MF, locketz A Immediate fundus complications after retinal scatter photocoagulation. I. Clinical picture and pathogenesis. Ophthalmic Surg 1976; 7(1):88-99.
13. Schepens Cl, Brockhurst RJ. Uveal effusions. 1. Clinical picture. Arch Ophthalmol1963; 70:189-201.
14. Friedman E, Smith TR, Kuwabara T, et al. Choroidal vascular pattems in hypertension. Arch OphthalmoI1964; 71:842-50.
15. Guerry DP III, Harbison JW, Wiesinger H. Bilateral choroidal detachment and fluctuating proptosis secondary to bilateral dural arteriovenous fistulas treated with transcranial orbital decompression with resolution: report of a case. Trans Am Ophthalmol Soc 1975; 73:64-73.
16. Gottlieb F. Combined choroidal and retinal detachment. Arch Ophthalmol 1972; 88:481-6.
17. Brockhurst RJ. Nanophthalmos with uveal effusion: a new clinical entity. Arch Ophthalmol1975; 93:1289-99.
18. Richardson J, Walsh M. Uveal effusion as a sign of myxoedema. Br J OphthalmoI1969; 53:557-60.
19. Velzeboer CMJ. Spontaneous choroidal detachment: report of two cases. Am J Ophthalmol1960; 49:898-903.
20. Kline lB, Bright M, Brownstein S. Uveal melanoma presenting as post-traumatic choroidal hemorrhage and panophthalmitis. Can J Ophthalmol1977; 12:226-9.
21. Taake WH, Allen RA, Straatsma BR. Metastasis of a hepatoma to the choroid. Am J Ophthalmol1953; 56:208-13.
22. Kreiger AE, Meyer 0, Smith TR, Riemer K. Metastatic carcinoma to the choroid with choroidal detachment. A case presenting as uveal effusion. Arch Ophthalmol 1969; 82:209-13.
23. Eichholtz W. Mikrometastasen der Uvea: ungewohnliche Ursache einer Aderhautabhebung. Klin Monatsbl Augenheilkd 1976; 169:104-7.
24. Stephens RF, Shields JA Diagnosis and management of cancer metastatic to the uvea: a study of 70 cases. Ophthalmology 1979; 86: 1336-49.