choice and access to palliative care
TRANSCRIPT

Choice and Access to Palliative CareDr Jane Collins, 19 April 2016
2
About Marie Curie
Marie Curie is a provider of care and support to people affected by terminal illness. Our core business is: • Nursing care (primarily overnight, but some variations)• Hospice care through our 9 hospices• Research program• Information and Support service (telephone line, peer to peer online)• Marie Curie Helper – a volunteer befriending service• Campaigning – right to access palliative care
We have been providing services for as long as the NHS!
3
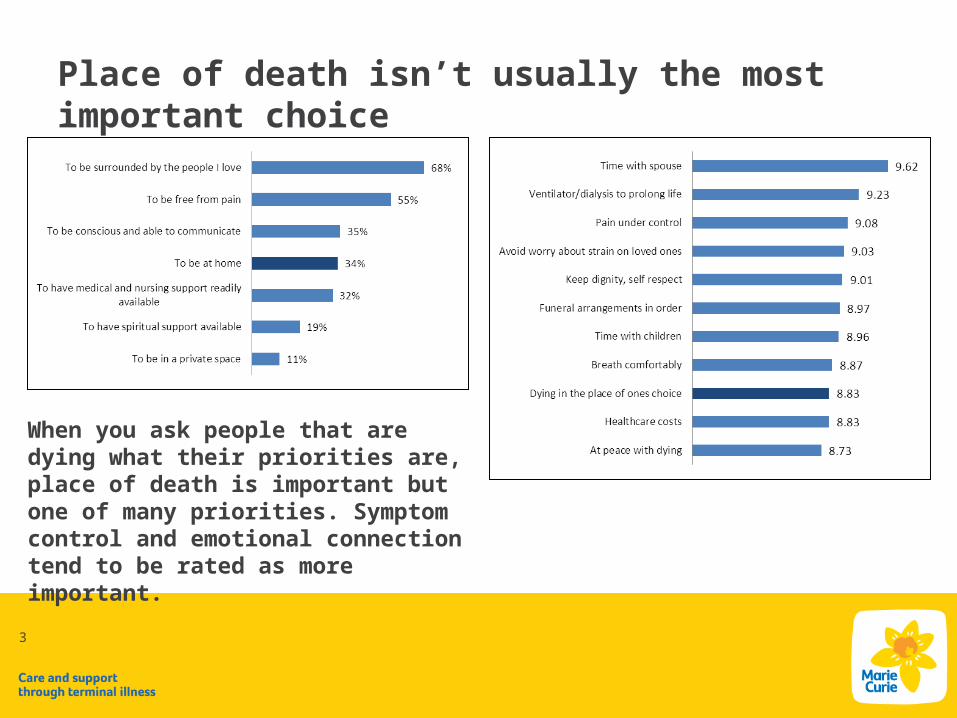
Place of death isn’t usually the most important choice
When you ask people that are dying what their priorities are, place of death is important but one of many priorities. Symptom control and emotional connection tend to be rated as more important.
4
But is a ‘good death’ possible in hospital?
• Place of death might not be people’s most pressing priority, but:
• Around half of the UK population dies in hospital• And we should ask whether hospital is the place
where people’s other priorities – like emotional connection and symptom control – can realistically be met.

5
More face-to-face access to specialist palliative care needed…
But latest hospital audit shows this is where they struggle:
• Most measures improving over last two years, but access to specialist palliative care still low
• Face-to-face, 24/7 specialist palliative care available in 11% of Trusts (up from 2%)
• Face-to-face, 9-5, Mon-Sun specialist palliative care in 37% of Trusts (up from 21%)
• Still too low, but a workforce issue with a £ implication
6
But what about emotional support?
• Currently access to friends and family when in hospital isn’t monitored, even though this is one of people’s top priorities!
• Closest we get is ‘emotional support’ – hospital is a poor performer here:o 59.4% of people strongly agreed or agreed that their loved one
had sufficient emotional support in the last two days of life in hospital. By comparison:
o Home – 74.9%o Hospice – 87.6%o Care home – 77.6%
- ONS, Voices 2015
7
What do we need to do to improve quality of care in hospitals?
1. More access to specialist palliative care around the clock, face-to-face. This has a money implication and is a challenge for the Government. Extending junior doctor hours won’t make the NHS anymore 24/7 for people who are dying!
2. More training for non-palliative care specialists in hospitals – it is available, but not mandatory or necessarily accessible
3. Improve emotional support and gain a better understanding of emotional needs. This is an ideal place to use volunteers - Marie Curie have piloted volunteer companion programme at Musgrove Park.
8
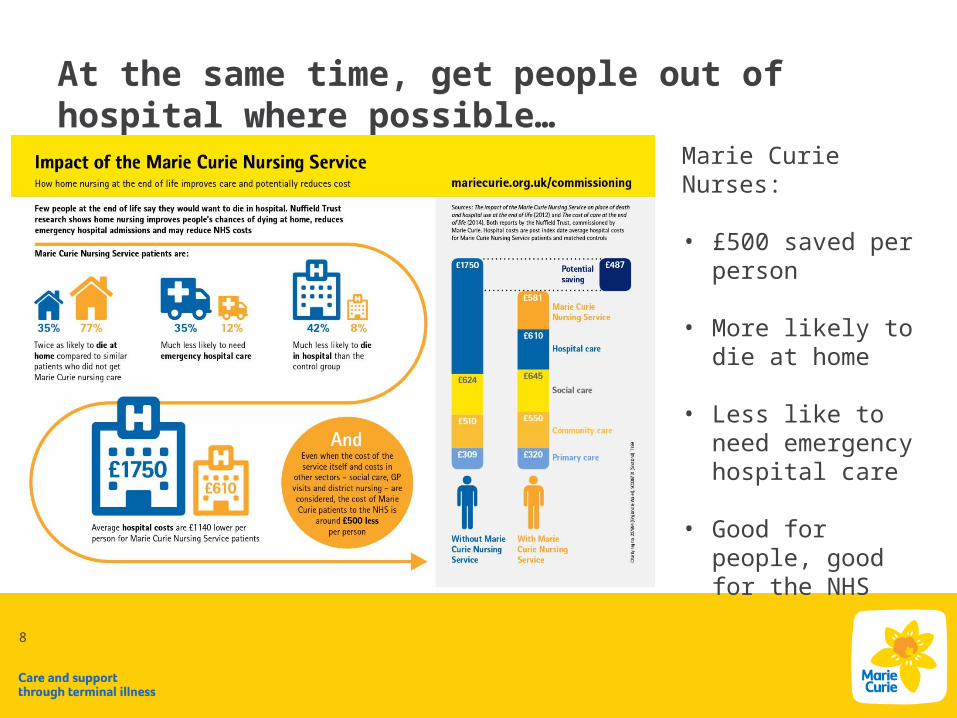
At the same time, get people out of hospital where possible…
Marie Curie Nurses:
• £500 saved per person
• More likely to die at home
• Less like to need emergency hospital care
• Good for people, good for the NHS

9
• Nuffield Trust evaluation of Marie Curie Nursing service. Place of death versus matched controls.
Community palliative care is hugely effective…

But only where we can work with other services…
Meals-on-wheels or other home delivered mealsSomething else1
Any other nurse at homeSocial worker/ support worker
Religious leaderOccupational therapist (OT)
Rapid response teamHospice at home
Home care worker, home care aide or home helpMacmillan nurse, hospice nurse or specialist
District or community nurse
0% 20% 40% 60% 80% 100%
Services received at home by MCNS patients vs. non-MCNS patients
source: VOICES survey / ONS
MCNS pa-tient

Source: details here (or delete)
11
Getting people out of hospital can be close to impossible…
Notes: further details here (or delete)
• In our own work we are seeing more and more delayed transfers of care
• Fast track Continuing Healthcare (CHC) was designed to address this issue, with 48 hour transfers of care. But in one Trust in which we work we are seeing an average delay of 9.1 days with one patient waiting 14. Many patients die while waiting to leave hospital.
• Availability of social care is the barrier. Either: a provider cannot be found; or, providers are unwilling to take on someone so close to death!

12
There seems to be no strategic approach to resolving delayed transfers of care…
Research conducted in 2015 by Marie Curie, based on research by Hospice UK and NCPC
Health and Wellbeing Boards are the ideal place to discuss how health and social care services can be commissioned strategically to facilitate faster transfers of care from hospital, but…
55%
10%
35%
All UK Health and Well-being Strategies
55% of Health and Wellbeing Boards have no dedicated, multi-condition strategy for end of life care
Source: details here (or delete)
13
Making choice a reality…
Notes: further details here (or delete)
1. Improved access to specialist palliative care in hospitals2. Improved emotional support and understanding of emotional and spiritual
needs in hospital3. Greater focus on speedy transfers of care4. Improved availability of social care5. Strategic approach to getting people out of hospital that involves social and
health care providers working together6. A response to the Choice Review from the Government (it’s been over a year)
with some additional funds to make this a reality!
14
For more information contact:Dr Jane CollinsMarie Curie89 Albert EmbankmentLondon SE1 7TP Phone: 020 7599 7130Email: [email protected] us on Twitter @mariecurieuk @mariecuriePA