children with special healthcare needs 1 st trimester march 2013 continuing education
TRANSCRIPT

Children With Special Healthcare Needs
1st Trimester March 2013 Continuing Education
Our agenda today
• System announcements• Children with special healthcare needs• Children with special psychiatric needs• (ALS) Strip o’ the month: Bradycardia• (ALS) Drug o’ the month: Atropine
Special thanks to:
The Alameda County (CA) Public Health Department
I. Introduction to Children With Special Health Care Needs (CSHCN)

CSHCN: Definition
CSHCN (Children with Special Health Care Needs) –Children who have or are at increased risk for a chronic
condition – physical – developmental– behavioral– emotional and who also require health and related services of a type or
amount beyond that are required by children generally.
From: Commentary in Pediatrics, Vol. 102, No.1, July 1998.

CSHCN: Epidemiology
• 12 million US children are considered “special needs,” which is 18% of all U.S. children
From: 1994 National Health Interview Survey on Disability
• Estimated that 25% of children treated in pediatric EDs have special needs
From: Pediatric Emergency Care, Vol 12, No. 3 June 1996

CSHCN: Health Care Realities
• Managed Care– Complicated home care financially
driven– Parents forced to provide
advanced care• Societal Changes
– “Family-centered care”– Disabled have right to be home
• Medical Advances– Portable technology– Improved techniques and
medications
CSHCN: Equipment
Technology-Assisted Children • Feeding catheters• Colostomies• Pacemakers• Glucometers• Nebulizers• Apnea monitors
• Tracheostomies• Ventilators/BiPAP• Central venous
catheters• CSF shunts• Vagal nerve stimulators
CSHCN: Important Points
• Assess and manage ABCs as with any other child
• Listen to parents/caregivers– They know problems and treatments very
well
II. Common Chronic Pediatric Illnesses: Pulmonary Disorders and
Airway Defects
Pulmonary Disorders and Airway Defects
Apnea• Definition
– Respirations cease for > 20 seconds or
– Respirations cease for < 20 seconds with cyanosis or bradycardia
• Causes– Obstructive, central, or mixed– Affects both premature and full-
term infants
Pulmonary Disorders and Airway
Defects Cystic Fibrosis• Overview
– Affects 30,000 Americans– Autosomal recessive disorder– Mucus builds up in lungs
• Signs and symptoms– Increased respiratory rate– Increased oxygen requirement– Paleness or cyanosis
• Management– Give active form of the abnormal protein product– Chest therapy with bronchial or postural draining– Antibiotics– Bronchodilators
III. Cardiovascular Defects
Cardiovascular Defects
Congenital Heart Defects (CHDs)• 1 in 1,000 live births• Two types
1. Acyanotic
2. Cyanotic

Cardiovascular Defects
Acyanotic Heart Defects• Account for the majority of CHD in children• Mixing of desaturated blood in the systemic
arterial circulation• Oxygen saturation is in the normal range• Generally septal defects, obstructions to the flow
of blood, and incomplete heart development.

Cardiovascular Defects
Signs/Symptoms of Acyanotic Heart Disease• Increased respiratory rate• Increased heart rate• Heart murmur• Signs of heart failure
– Rales on lung exam– Palpable liver edge– Swollen extremities

Cardiovascular DefectsTypes of Acyanotic Heart Defects• VSD (most common)
• Ventral Septal Defect– Defect in wall that separates
ventricles
• ASD• Atrial Septal Defect
• Patent ductus arteriosus• Fetal blood passage doesn’t close after
birth
• Obstructive lesions• Narrows the aorta or valves
Cardiovascular Defects
Cyanotic Heart Defects• Blood from arteries and veins mix in the heart • Typical oxygen saturation—70% to 90% on room
air• Palliative procedures often performed at birth• Caregivers/medical control may advise that you
avoid administration of O2 unless O2 saturation is below usual – Otherwise, never withhold oxygen!
Cardiovascular Defects
Signs/Symptoms of Cyanotic Heart Disease• Cyanosis• Increased respiratory rate, retractions• Increased heart rate• Poor perfusion• Diminished peripheral pulses• Poor feeding, sweats with feeds
Cardiovascular Defects
Types of Cyanotic Heart Defects• Hypoplastic Left Heart Syndrome• Transposition of the great arteries• Tetrology of Fallot• Tricuspid Atresia• Pulmonary Atresia• Truncus Arteriosus• Cardiac Arrhythmias

IV. Down Syndrome

Down Syndrome
Down Syndrome (Trisomy 21)• Chromosomal abnormality• Affects 1 in 800 births• Highest risk: women > 35 years• At risk for medical complications of multiple
systems

Down Syndrome
Signs/Symptoms of DS• Large tongue• Short neck• Obesity• Short stature• Loose ligaments• Epicanthal folds

Down Syndrome
Conditions Associated with DS• Congenital heart disease
– VSD, ASD, AV canal• Orthopedic conditions
– Atlantoaxial subluxation• Neurologic Conditions
– Epilepsy• Airway and Respiratory problems
– Dental and speech abnormalities

V. Traumatically Disabled Children
Traumatically Disabled Children
• Unintentional injuries are the leading cause of morbidity and mortality
• Traumatic brain injuries– Risk of seizures – May need CSF shunt/feeding tube/wheelchair
• Spinal cord injuries– Difficulty regulating body temperature– Pressure sores are serious concerns– Disabled child may be unaware he or she is injured– High risk of abuse
VI. Neurologic Diseases

Neurologic Diseases
Causes of Seizures• Epilepsy• Traumatic brain injury• Genetic/metabolic defect• Congenital brain abnormality
– Including mental retardation
• Tumor
Neurologic Diseases
Generalized Seizures • Tonic clonic or grand mal
– Duration seconds to minutes– Most common type of seizure
• Absence– Vacant, blank stare– May occur many times a day
• Myoclonic– Infantile spasms– Difficult to control

Neurologic Diseases
Partial Seizures• Simple partial
– One part of brain involved– Child awake and aware– Involves one limb or one side of body– Can progress to generalized seizure
• Complex partial – Child unconscious– Affects one side of the body
• Psychomotor partial– Repetitive fine-motor activity– Most common; one part of the brain
Neurologic Diseases
Management of Seizures• Antiepileptic medications
– Most common treatment
• Home Valium per rectum– For frequent and/or prolonged seizures
– Can NOT give unless you are trained to do so and with approval of medical control
• Vagal nerve stimulators• Ketogenic diet
– For intractable seizures
Neurologic Diseases
Hydrocephalus• Excessive build-up of CSF
within the cavities of the brain• Causes
– Congenital hydrocephalus (occurs before birth)
– Acquired hydrocephalus (occurs after birth)
Neurologic Diseases
Management of Hydrocephalus• CSF shunts
– Ventriculoparietal shunt most common type
• Shunt complications– Shunt malfunction, obstruction – Infection
• Signs and symptoms of shunt malfunction– Headache– Nausea/Vomiting– Diminished mental status– Bradycardia, hypertension, irregular
respirations– “Sundown eyes”
Neurologic Diseases
Mental Retardation• IQ < 70• Non-progressive disorder• Cause is prenatal problem, brain injury, or genetic
syndrome• Requires special education
Developmental Delay• Results from prolonged illness or prematurity• Potential to “catch up”• Requires special education
Neurologic Diseases
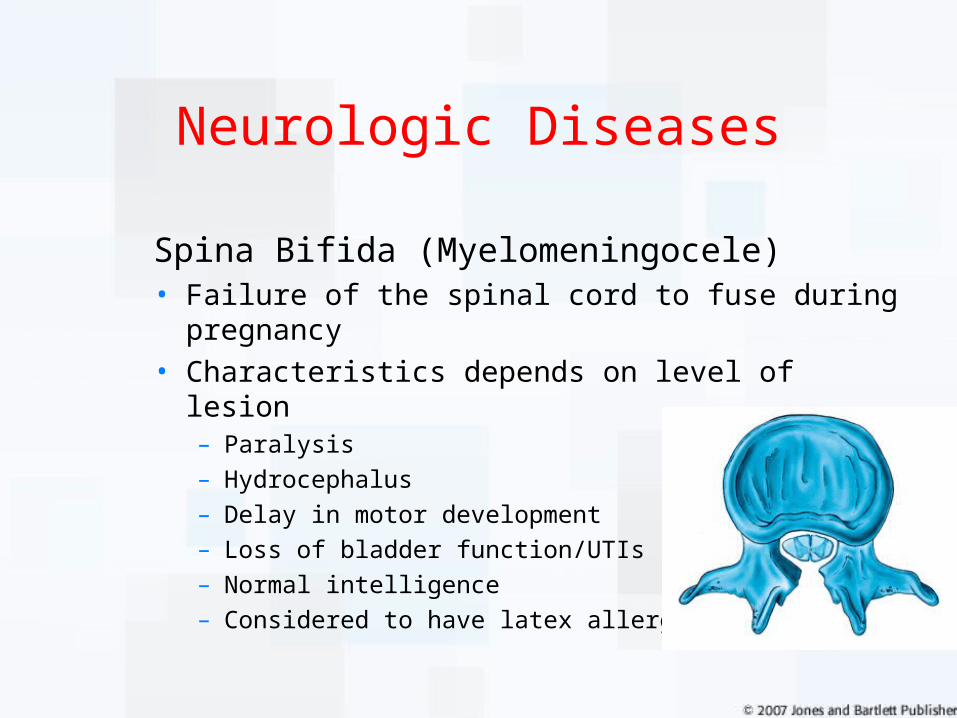
Spina Bifida (Myelomeningocele)• Failure of the spinal cord to fuse during pregnancy• Characteristics depends on level of lesion
– Paralysis– Hydrocephalus– Delay in motor development– Loss of bladder function/UTIs– Normal intelligence– Considered to have latex allergy

Neurologic Diseases
Cerebral Palsy (CP)• Characteristics
– Damage to brain center controlling muscle control– Multiple types– Congenital or acquired
• Often occurs in very-low-birth-weight babies
– Hypertonic, contracted limbs– 50% have seizure disorder– Two-thirds have mental retardation
Neurologic Diseases
Cerebral Palsy• Management• Braces• Wheelchairs• Oral medications• Baclofen intrathecal pumps
VII. Hematology and Oncology Diseases

Hematology and Oncology Diseases
Sickle Cell Anemia (SCA)• An inherited hemoglobinopathy that
causes sickling of RBCs• Characteristics
– Pain,“vaso-occlusive crisis”– Splenic sequestration– Aplastic crisis– Sepsis

Hematology and Oncology Diseases
Hemophilia• An inherited disorder in which a factor needed for
clotting blood is either too low or missing• Incidence
– 15,000 in U.S. (mostly males)– 60% severe form– 15% moderate form– 25% mild form
• Characteristics– Prolonged bleeding– Factor routinely administered at home– Seemingly minor injury can be serious

X. Musculoskeletal Disorders
Musculoskeletal Disorders
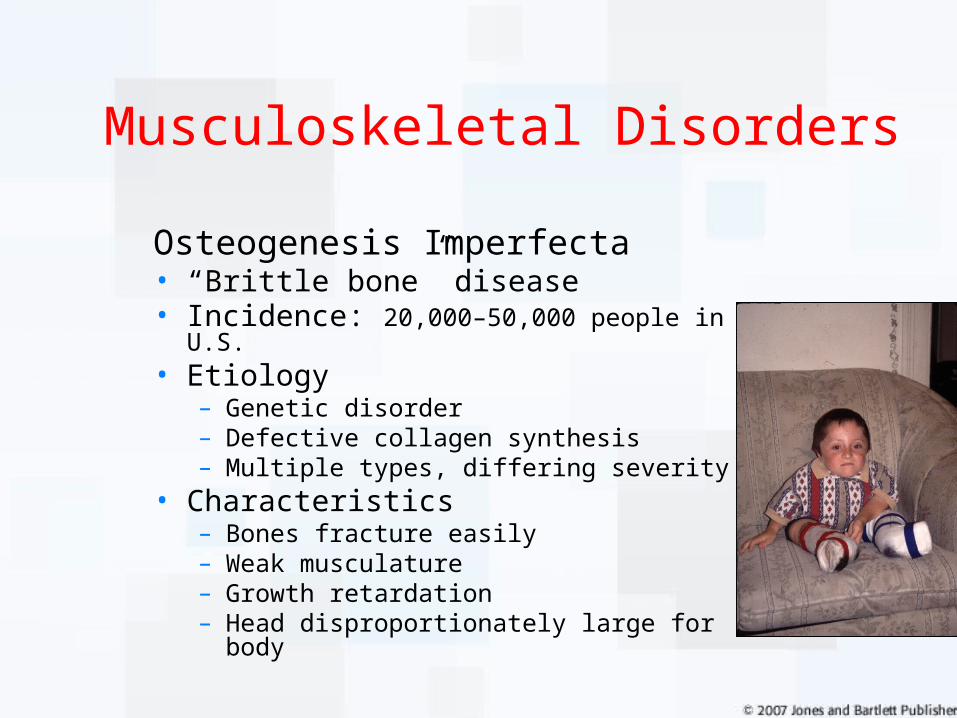
Osteogenesis Imperfecta • “Brittle bone” disease• Incidence: 20,000–50,000 people in U.S.• Etiology
– Genetic disorder – Defective collagen synthesis– Multiple types, differing severity
• Characteristics– Bones fracture easily– Weak musculature– Growth retardation– Head disproportionately large for body

Musculoskeletal Disorders
Muscular Dystrophy• Cause
– Most common type is Duchenne’s
– Flaw in muscle protein – Muscle-wasting disease– Most are inherited
• Characteristics– Motor skills deteriorate– Cardiomyopathy– Shortened lifespan

XI. Tips for Chronic Conditions

Tips for Chronic Conditions
• Medical Identification Jewelry
• Parents trained in child’s care
• Often part-time home health care assistance
• DNR forms—Follow local protocols
• EMS Outreach Program• EMS Notification
Courtesy of the MedicAlert Foundation®. © 2006, All Rights Reserved. MedicAlert® is a federally registered trademark and service mark.
Tips for Chronic Conditions
• Assess and manage ABCs as with any other child
• Listen to parents/caregivers• They know problems and treatments very well
A Different Look
Why CSHCN Caregivers Call 9-1-1• 97 of 100 CSHCN families surveyed have sought
emergency care • 75 sought emergency care three or more times• CSHCN require EMS services because:
– Home health care equipment fails– Caregivers panic– No improvement with therapy– Child in respiratory or cardiac distress/arrest
A Different Look
Differences to Consider• Medical issues vs. equipment issues• Atypical baseline vital signs• May be smaller than same age peers• May be developmentally delayed

A Different Look
General Approach• Ask “What is normal for your child?”• Respect caregiver’s opinion on child’s condition.
– Many know as much as the doctors do about their child’s illness.
• Treat the child, not the technology.• Simple illnesses can be life-threatening .• Caregivers are experienced with the medical
system.
II. The ABCDEs:Interventions Using Special
Technology
AIRWAY: Tracheostomies
Airway
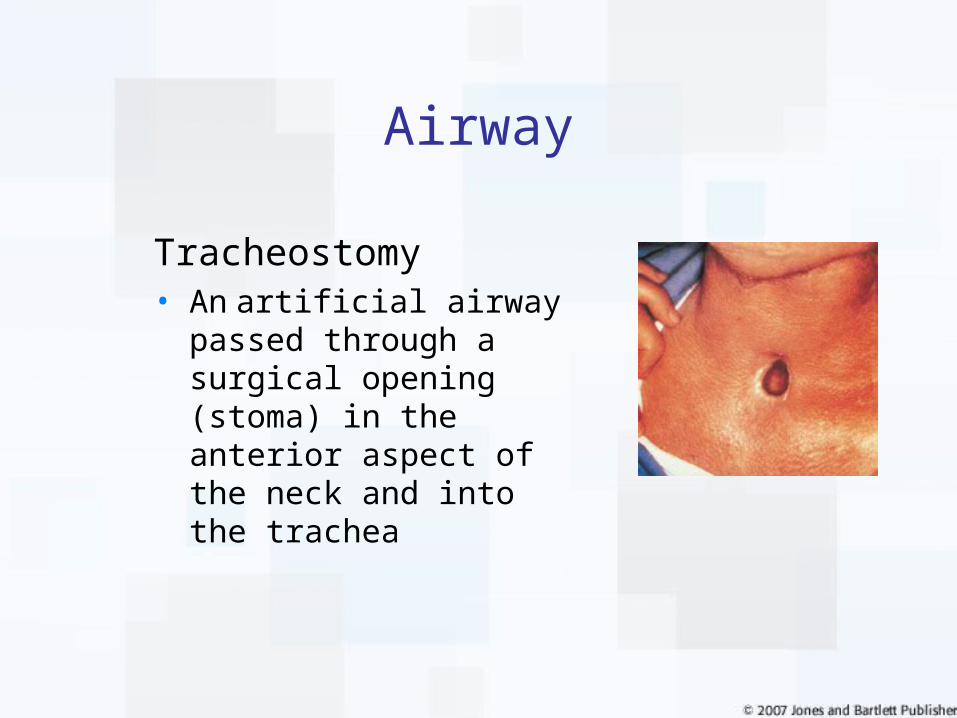
Tracheostomy• An artificial airway passed
through a surgical opening (stoma) in the anterior aspect of the neck and into the trachea
Airway
Tracheostomy Indications:• To bypass an upper-airway obstruction• To provide long-term mechanical ventilation• To facilitate clearance of excess secretions

Airway
Tracheostomy Types and Features
Single Lumen
Double Lumen
Fenestrated

Airway
Interventions:• Position of comfort
• Humidified air or O2
• Nebulized 1:1000 epinephrine, if protocols allow• If child is in extremis, consider endotracheal
intubation
Airway
Alleviating Respiratory Distress• Position• Suction• Oxygen• Repeat• An emergency tracheostomy tube change
may be necessary.

Airway
When to ventilate manually • Upon removal from ventilator• Consider before/after
suctioning or trach change• Signs of respiratory distress or
failure

Airway
Causes of Tube Obstruction• Improper airway positioning• Improper insertion of the trach tube
– Creation of a “false track”• Mucous plug• Failure to remove obturator after tube insertion

Breathing
Interventions• Disconnect patient from the ventilator• Began manual ventilation• Assess for chest rise, breath sounds• If no improvement, check for tracheostomy-
tube obstruction• If improved, consider ventilator issue• Prepare for transport
CIRCULATION: Central Venous Catheters
Circulation
Purpose of Central Venous Catheters• Administration of Medications• Delivery of chemotherapy• Nutritional support• Infusion of blood products• Blood draws

Circulation
Types of Catheters• Broviac, Hickman, Groshong
-Tunneled central venous catheters
- Proximal tip in the subclavian vein
- External access
• Port-a-Cath/Med-a-Port/PAS Port- Catheter system is completely beneath skin
• Percutaneous Intravenous Catheter (PICC)- Proximal tip in central vein
- Looks like a PIV

DISABILITY
Disability
Interventions • Position• Oxygen• Maintain body temperature• ALS: IV, fluids, IO• ALS: Consider inotropes for shock if
unresponsive to fluid resuscitation
Assessment of neurological status• Ask caregiver to compare child’s present
status to baseline

Disability
Cause of symptoms:• Shunt infection
– If child presents with a fever or redness along the shunt tubing, suspect a shunt infection
• Meningitis• Encephalitis
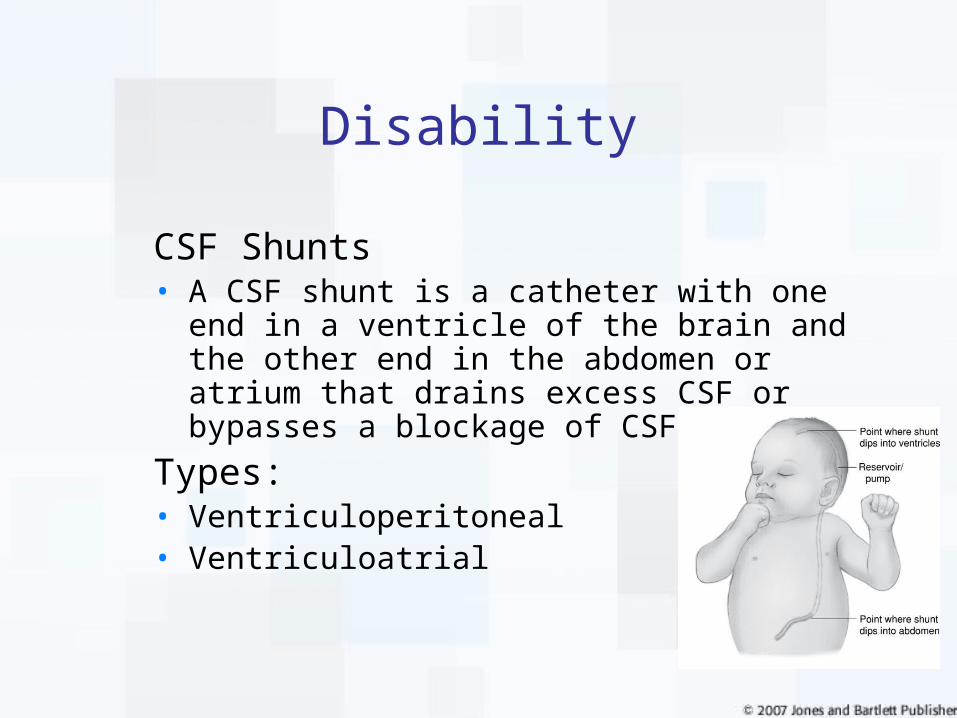
Disability
CSF Shunts• A CSF shunt is a catheter with one end in a
ventricle of the brain and the other end in the abdomen or atrium that drains excess CSF or bypasses a blockage of CSF.
Types:• Ventriculoperitoneal• Ventriculoatrial

Disability
Concern• The shunt could be damaged or
disconnected. This can result in increased intracranial pressure.
Disability
Causes of Complications:• Brain infection• Shunt obstruction (resulting in a
dangerous build-up of fluid in the skull)• Shunt malfunction• Peritonitis

Children with Special Healthcare Needs
• Cerebrospinal fluid shunts– Emergency care• Vomit, aspiration• Suction• O2• Assist breathing, intubate• Blood sugar• Treat seizures

Children with Special Healthcare Needs
Shunt Drainage Routes
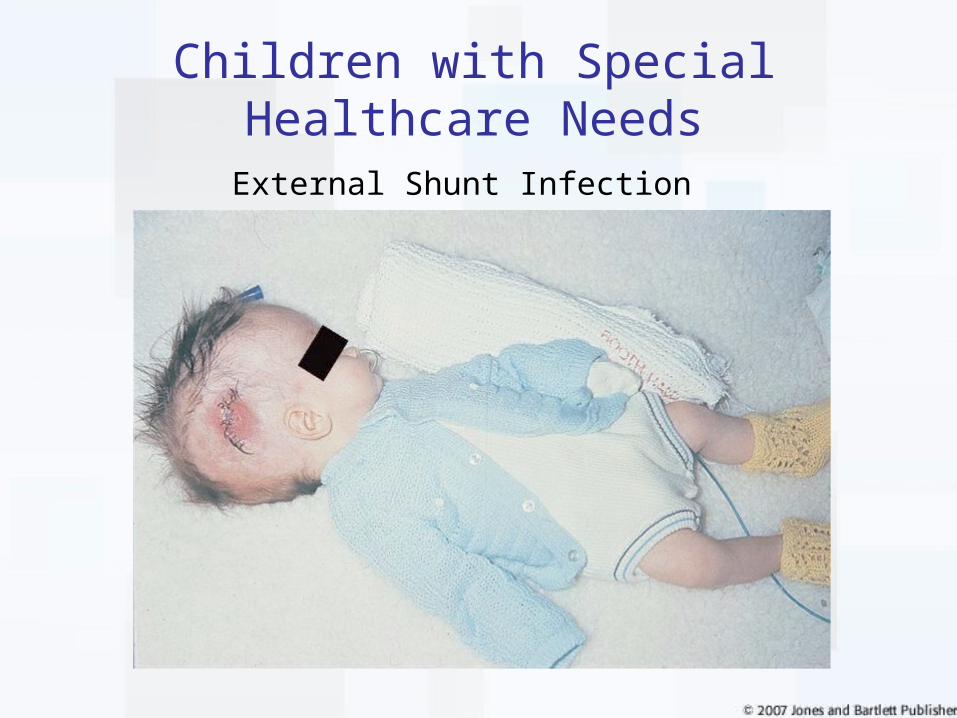
Children with Special Healthcare Needs
External Shunt Infection

EXPOSURE

Exposure
Interventions• Assess neurovascular status distal to the
injury.• Gently place on a long-board splint. • Avoid taking the blood pressure of a child with
osteogenesis imperfecta. • Do not use a hare traction splint or MAST
trousers.

IMPORTANT POINTS
• Cover the child to maintain normal body temperature
• Respect the child’s privacy

• Carefully examine for injuries– Assessment may be difficult due to
developmental level– CSHCN are at high risk for abuse
• Report any suspicious injuries to the proper agency.
IMPORTANT POINTS
II. SAMPLE History:Feeding Catheters
Feeding Catheters
• Nasogastric Tube (NGT):– Catheter placed through the nose into
stomach– For supplementation in children who
cannot take enough by mouth– Short-term use– Can use to decompress stomach
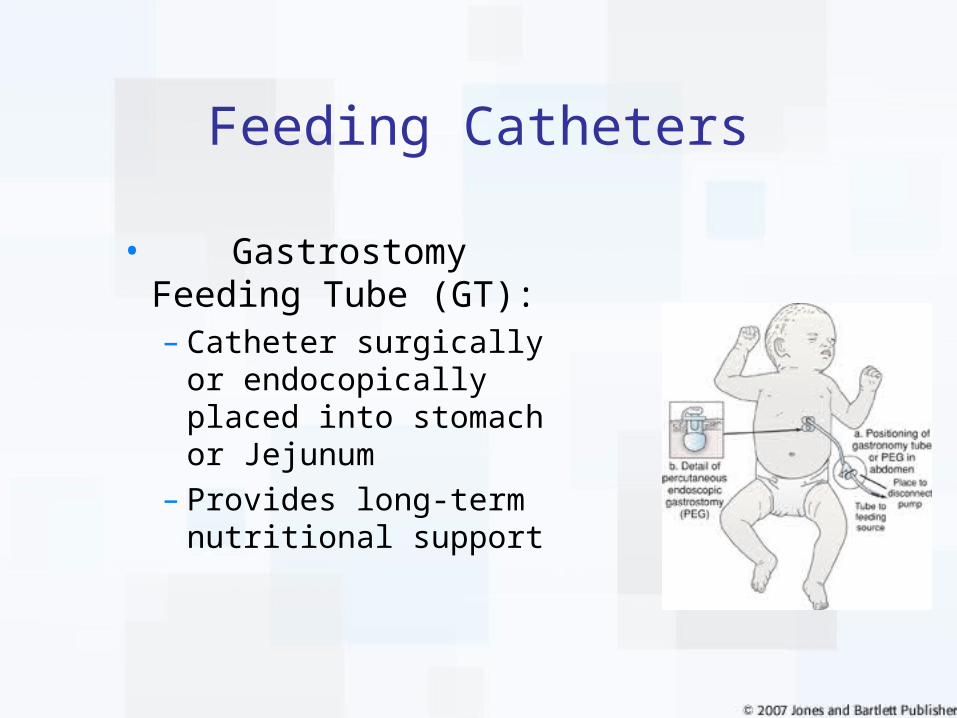
Feeding Catheters
• Gastrostomy Feeding Tube (GT):– Catheter surgically or
endocopically placed into stomach or Jejunum
– Provides long-term nutritional support
Feeding Catheters
• Feeding Catheter Complications:– Gastric contents can leak, causing
irritation– Tube obstructed– Tube dislodged– Abdominal distention
I. Moving Children with Special Needs
Communication
• Challenges:– Language barriers– Is the person with the
child the primary caregiver?
– Assess child’s ability to understand.• Developmental delay• Visual/auditory deficits

Communication
•Management:– Use a soothing voice to provide comfort.– Explain each movement.– Ask the caregiver for a medical summary
card. Oftentimes, the caregiver may be too stressed to remember vital information.
Environment
•Challenges:– The scene and the child’s
response to that environment can be a great source of tension and anxiety.
– Multiple providers can create fear.
– Multiple voices can cause confusion.

Environment
• Management:– Limit the number of providers.– Ask one person to speak and interact
with the child.– Decrease chaos.– Keep the noise down.

TRANSPORT AND TRANSFER

Transport
•Challenges:
– Anxiety in child.– Child may resist being restrained.– Brittle bones and muscle contractures
can easily lead to injuries during transport.
– Do not pull on extremities!
Transfer
• Management– Make secure, firm contact– Suggest that family member move child.– Allow the child to lay in a comfortable
position.– Use padding around buckles and
contractures.– Do not pull on extremities!
Stabilization
• Secure and transport child in own special restraint device if:– No suspicion of cervical injury.– Child is not critically ill.– Device doesn’t impede assessment and
treatment.– Device can be properly secured in
ambulance.
Destination Decisions
• Challenges:– Parents’ confidence in EMS system*• 82% very confident in EMS care and home hospital• 77% uneasy/not confident in community hospital
care• 98% very confident in “home” hospital care
• Parents trust 9-1-1 but not 9-1-1 transport decisions!
*100 CSHCN families surveyed in 2000
Children with Special Behavioral and Emotional Needs
• Behavioral emergencies involving children present special challenges to EMS.
• Aggressive behavior may really be symptom of an underlying disorder or disability.
• Parents of mentally ill children often overwhelmed and isolated from community and social support network.
• Family may hesitate to call 911 because of fear of stigma or misinterpretation by EMS personnel.
EMS Response
• Volatile situations require shift from common EMS response to integrated community collaboration and adaptive “out-of-the-box” decision making.
• 911 call may be from a mother or school staff member desperate for help with “out-of-control” child.
• Immediate link to pediatric or mental health professionals may de-escalate the child’s psychiatric emergency and ensure continuity of care.
• Unfortunately many EMS system policies, procedures, guidelines, and training do not include these options.

Common Behavioral Emergencies in Children
• Major psychiatric disorders that may predispose to behavioral emergencies in children include – mood disorders (e.g., depression, bipolar disorder); – thought disorders (e.g., schizophrenia);– developmental disorders (e.g., autism); – anxiety disorders (e.g., posttraumatic stress
disorder); – other disorders such as attention deficit hyperactivity
disorder.

EMS considerations
• EMS can assist and advocate for child and the family during a behavioral emergency.
• Family of a child with behavioral problems lives in fear of restraints, hospitalizations, false accusations.
• Understanding emotional fatigue, physical exhaustion, and chronic life disruptions of families is is integral to addressing their needs.
EMS Considerations
• Families of children with psychiatric disorders often have competing fears: – Love for their child– Fear of a violent outburst by the child toward the
family– Fear of the violence that may occur if the child needs
to be restrained by the police or EMS providers.
For more information on pediatric psych issues and EMS response:
• http://www.acphd.org/media/109325/meeting_challenges_pediatric_behavioral_emergencies.pdf

Rhythm O’ the Month• Bradycardia
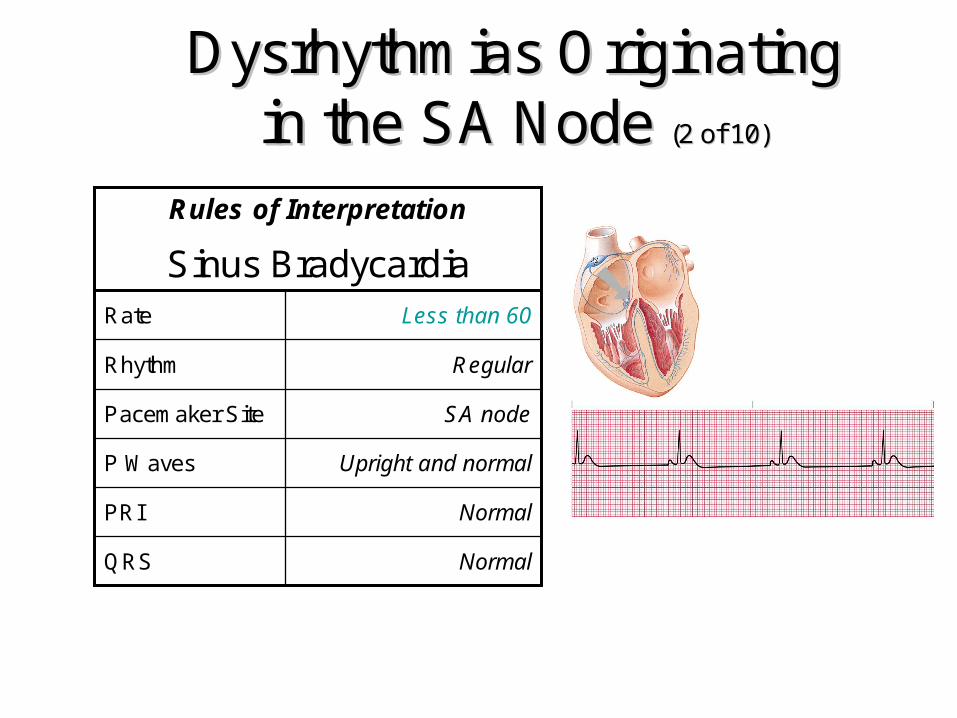
Dysrhythmias Originating Dysrhythmias Originating in the SA Node in the SA Node (2 of 10)(2 of 10)
NormalQRS
NormalPRI
Upright and normalP Waves
SA nodePacemaker Site
RegularRhythm
Less than 60Rate
Sinus Bradycardia
Rules of Interpretation
Sinus Bradycardia - Causes
• Decrease in sympathetic tone on the AV node (increase in parasympathetic tone)
• Pressure on fontanels in infants• Intracranial swelling• Glottic irritation from ET tubs, gagging,
emesis• Disease of the SA node• Hypothermia, Hypoxia

Sinus Bradycardia
• Administration of digitalis, propranolol (Inderal), verapamil, and quinidine
• Common in acute inferior AMI - Involves the right coronary artery which supplies the SA node with blood
Sinus Bradycardia in Children
• Life threatening, especially in newborns and infants.
• Often a respiratory issue– Newborn• Dry, stimulate, suction first• Then oxygen, ventilation• CPR if heart rate remains under 60
– Babies/children• Treat respiratory issues unless child has known cardiac
issue

Sinus Bradycardia
Treat the patient, not the monitor!
Bradycardia is also common during sleep, rest and in trained athletes!

Sinus Bradycardia
• Ultimate clinical significance…..– Decreased heart rate/BP which leads
to decreased CARDIAC OUTPUT
Sinus Bradycardia
• Treatment Modalities– Asymptomatic – pulse and adequate
BP (>100 systolic)
Routine Medical Care
IV, O2, monitor
Position of Comfort

Sinus Bradycardia
• Symptomatic– Hemodynamic Instablity (BP <100
systolic)• Syncope, hypotension, altered mentation• Chest pain, palpitations, diaphoresis• Difficulty in breathing• Poor skin vitals and perfusion
Symptomatic Bradycardia - ALS
• Do not delay pacing while getting ready for Atropine
• Pace at 70. – Increase MA until pulse matches.
• While pacing, consider Versed, 2.5 mg slow IVP.
• If necessary, Dopamine to maintain SBP 90-105 and pulse >60.
Sinus Bradycardia
• Hypotension– Leads to decreased cardiac output
– Palpitations• Because of SA node’s increased relative
refractory period permits refractory firing

Sinus Bradycardia
– Chest Pain• Heart disease already exists• Coronary blood flow is decreased
Sinus Bradycardia
• Bottom Line: TREAT THE UNDERLYING CAUSE TO ABOLISH THE DYSRHYTHMIA AND INCREASE THE RATE
Drug O’ the Month• Atropine!
Atropine Indications
• Symptomatic bradycardia. • NO LONGER USED: asytole or
PEA• Nerve agent exposure• Organophosphate poisoning
Adverse Reactions
• Dry mouth, hot skin, intense facial flushing• Blurred vision or dilation of the pupils with
subsequent photophobia• Tachycardia• Restlessness• May cause paradoxical bradycardia if the
dose administered is too low or pushed to slowly

Contraindications
• Acute MI• Myasthenia Gravis• GI Obstruction• Closed angle glaucoma • Known sensitivity to atropine,
belladonna alkaloids or sulfates (NOT sulfa)
How Atropine Works
• Increases firing of the SA node.• Increases conduction through the
AV node.• Opposes the action of the vagus
nerve.• Blocks acetylcholine receptor sites• Decreases bronchial secretions.
Atropine Dosage
Symptomatic Bradycardia• Adult: 0.5 mg IV/IO every 3 to 5 minutes to a
max dose of 0.04 mg/kg. Don’t delay pacing for Atropine.
• Peds: Oxygen/ventilation first. Then Epi! If that doesn’t work then 0.02 mg/kg (min of 0.1 mg/dose; max of 0.5 mg/dose). – Repeat once in 5 minutes
Dosage
Nerve Agent or Organophosphate Poisoning
• Adult: 2 mg IVP repeated if needed every 5 minutes until symptoms dissipate
• Peds: 0.02 mg/kg IV/IM every 5 minutes as needed until symptoms dissipate

Special Children, Special
Care
Questions? If you are watching live, feel free to type in the text box to your right.
If you are watching the recording, or the Powerpoint, feel free to email [email protected] or call 815-300-7130.