childhood and adolescent obesity are we in crisis?
TRANSCRIPT
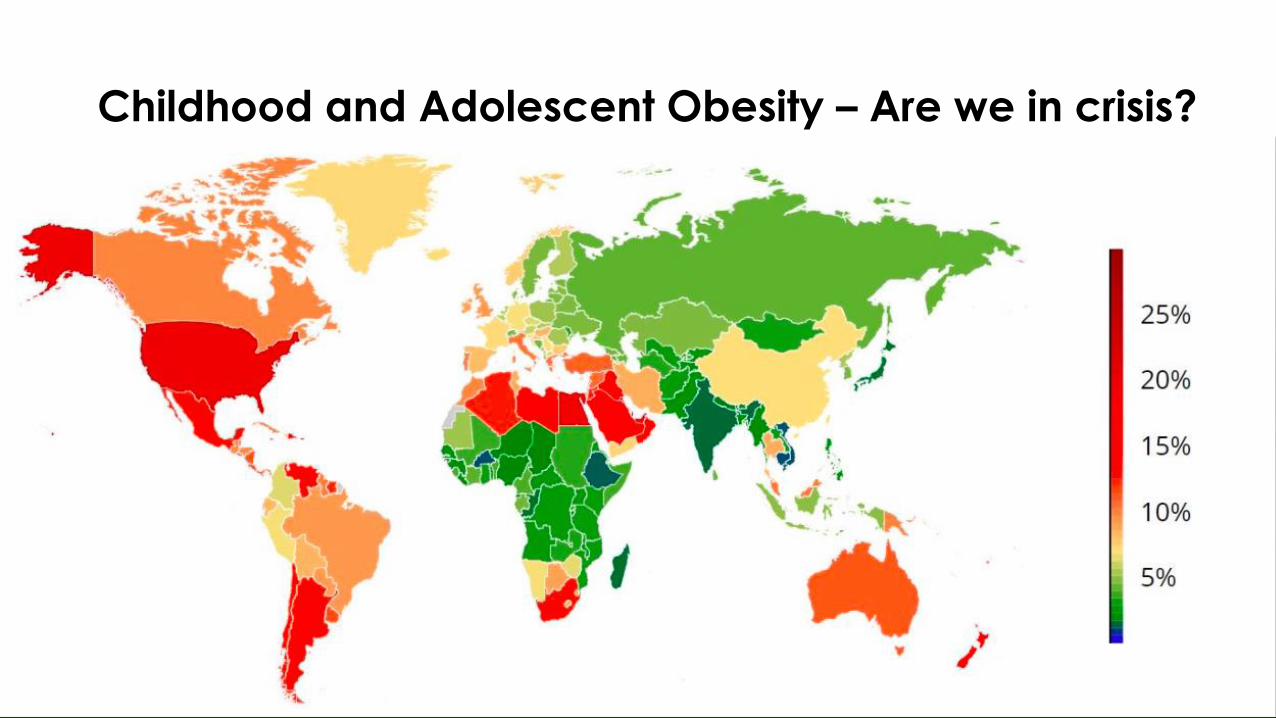
Childhood and Adolescent Obesity – Are we in crisis?


Lancet study: what are the trends 1975 – 2016?
• Mean BMI and obesity in children and adolescents aged 5–19 years have increased in most regions and countries• Prevalence rates from < 1% (5 million girls, 6 million boys) in 1975 to 6% in
girls (50 million) and 8% in boys (74 million) in 2016
• More children and adolescents are moderately or severely underweight than obese ( esp south Asia and central, east and west Africa)
• The rise in children’s and adolescents’ BMI has plateaued around 2000, in many high-income countries but has accelerated in parts of Asia.

How do we interpret these trends?
• Can we take lessons from slowing trend in high income countries?• Evidence of the effectiveness of interventions for overweight and
obesity in children and adolescents in several systematic reviews
• However, implementation and their post- implementation effects at the population level are rarely investigated
• No systematic information on the determinants of the divergent trends in BMI in children and adolescents and in adults • specifc initiatives by governments, community groups, schools?
• public awareness leading to changes in nutrition and activity?


Tracking into adulthood – local data
• HPB study (June 2017) showed that 70% of 7 year olds who were overweight were likely to remain overweight as adults
• In 1990 – 68.7% flagged as overweight remained so 5 years later
• In 2010 – 81.3% overweight 7 year olds remained so 5 years later
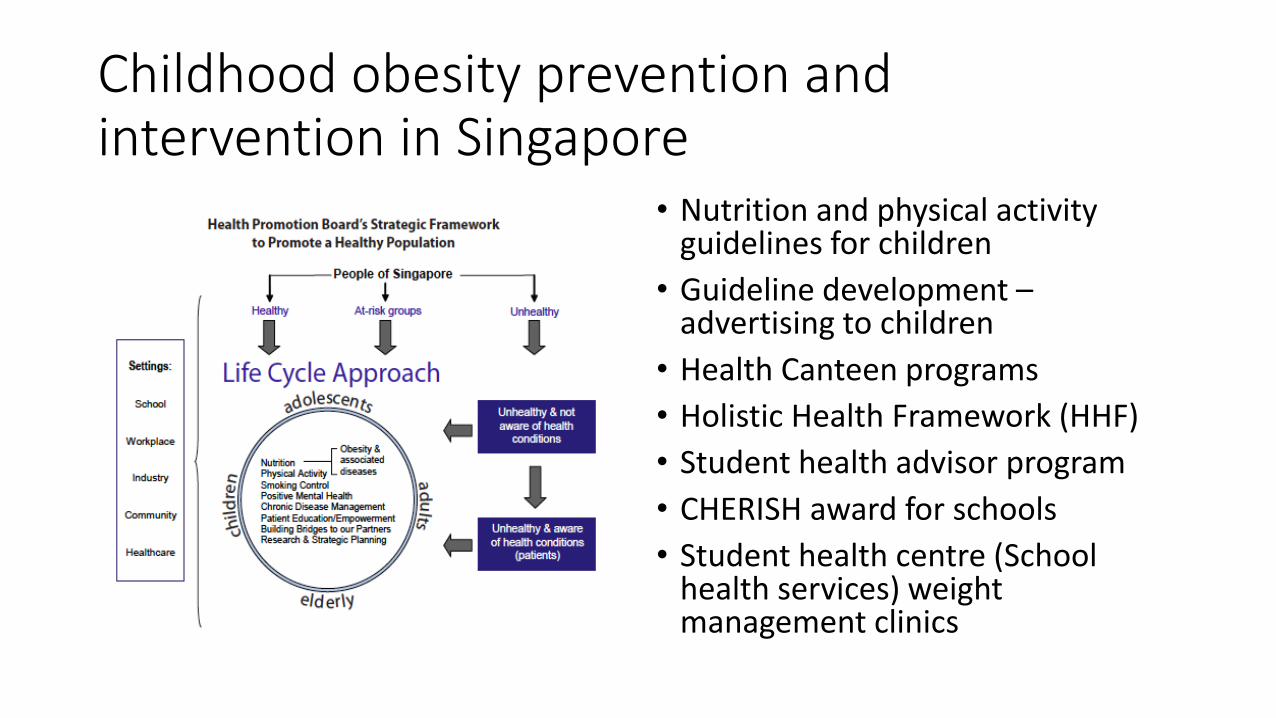
Childhood obesity prevention and intervention in Singapore
• Nutrition and physical activity guidelines for children
• Guideline development –advertising to children
• Health Canteen programs
• Holistic Health Framework (HHF)
• Student health advisor program
• CHERISH award for schools
• Student health centre (School health services) weight management clinics

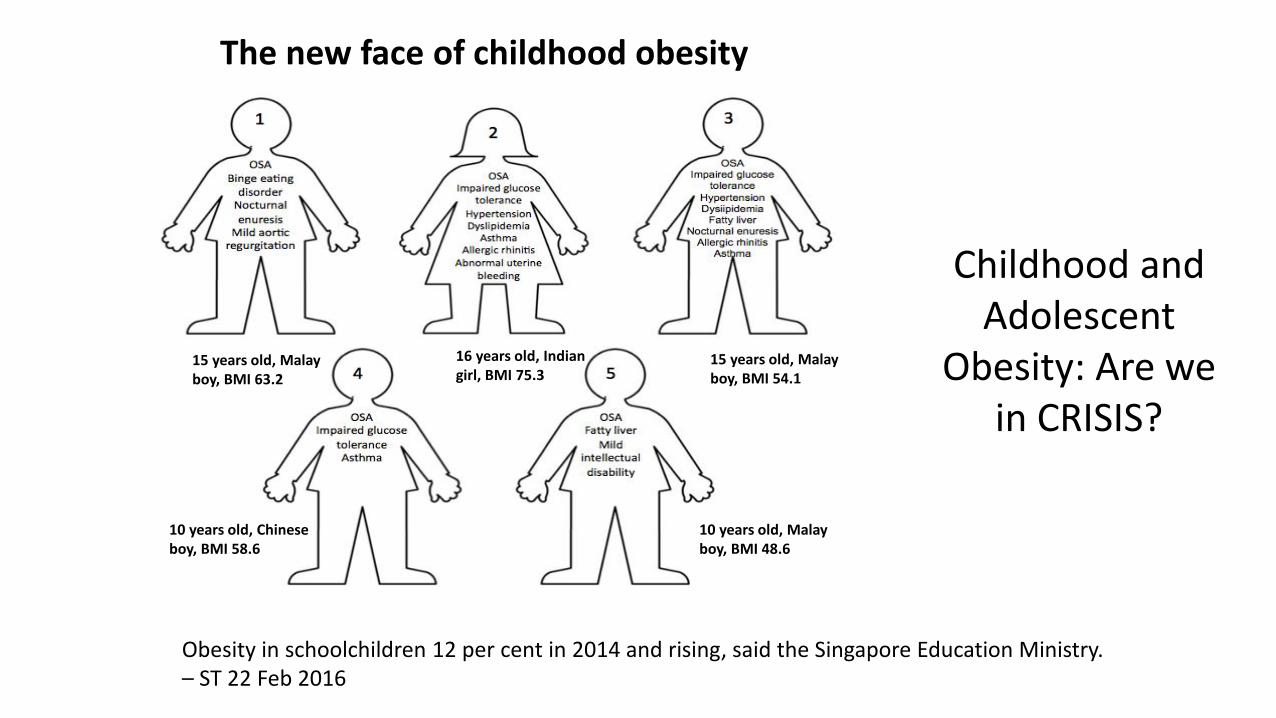
15 years old, Malay boy, BMI 63.2
10 years old, Malay boy, BMI 48.6
10 years old, Chinese boy, BMI 58.6
15 years old, Malay boy, BMI 54.1
16 years old, Indian girl, BMI 75.3
Obesity in schoolchildren 12 per cent in 2014 and rising, said the Singapore Education Ministry. – ST 22 Feb 2016
The new face of childhood obesity
Childhood and Adolescent
Obesity: Are we in CRISIS?
Case 4: at presentation
▪ Referral from Sleep Clinic for severe OSAHS needing Tonsillectomy & Adenoidectomy and nocturnal CPAP
▪ Presenting with weight 125 kg (>97%tile) height 1.46 m (75-90%tile) ➔BMI 58.6 (> 95%tile)
▪ The extent of obesity?▪ Birth weight 3.8kg
▪ Weight gain started as a toddler
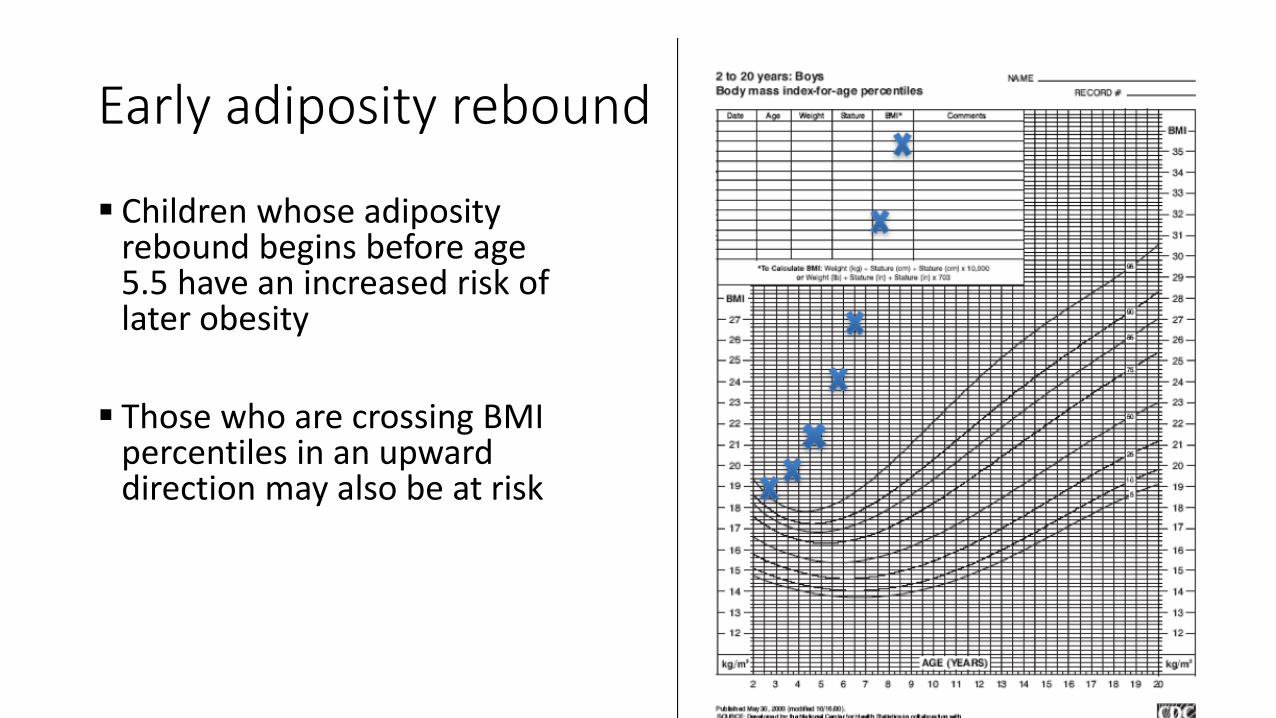
Early adiposity rebound
▪ Children whose adiposity rebound begins before age 5.5 have an increased risk of later obesity
▪ Those who are crossing BMI percentiles in an upward direction may also be at risk
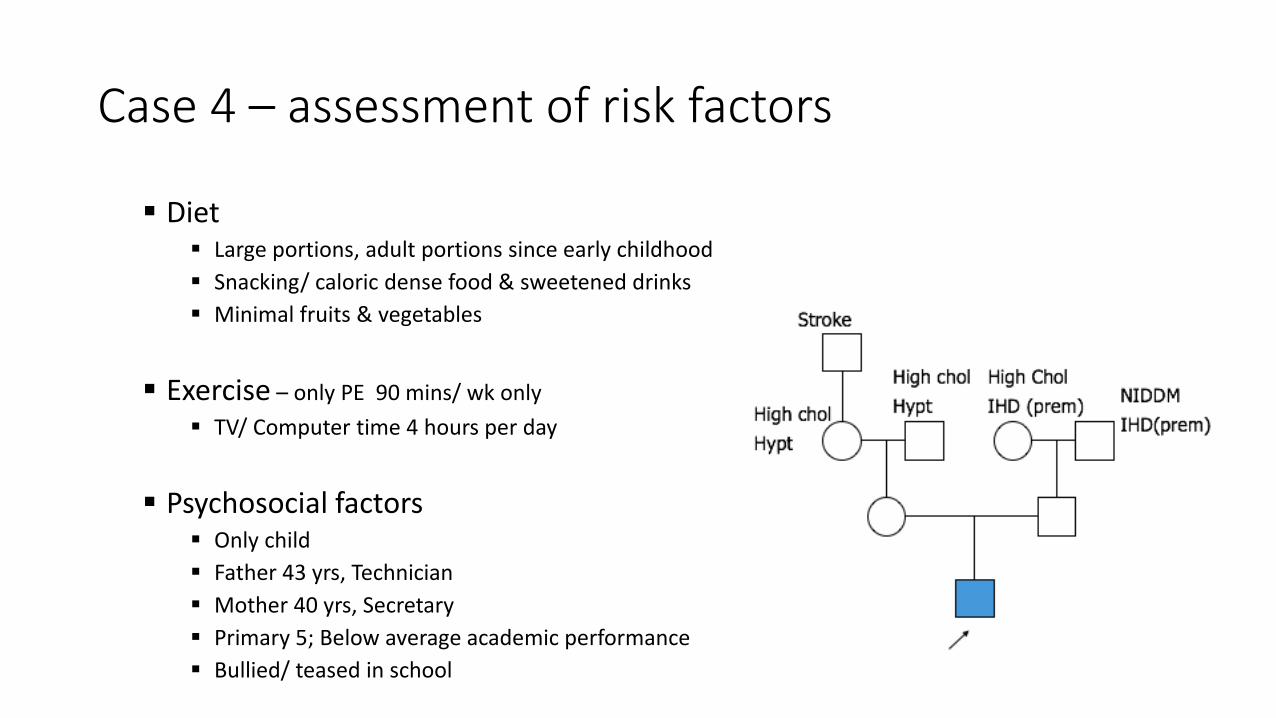
Case 4 – assessment of risk factors
▪ Diet ▪ Large portions, adult portions since early childhood
▪ Snacking/ caloric dense food & sweetened drinks
▪ Minimal fruits & vegetables
▪ Exercise – only PE 90 mins/ wk only
▪ TV/ Computer time 4 hours per day
▪ Psychosocial factors▪ Only child
▪ Father 43 yrs, Technician
▪ Mother 40 yrs, Secretary
▪ Primary 5; Below average academic performance
▪ Bullied/ teased in school

Morbidity in childhood obesity

Case 4 - management
▪ Medical management▪ Impaired glucose tolerance – weight control measures; use of Metformin still controversial
▪ Severe OSAHS – T&A done, nocturnal CPAP+8
▪ Setting realistic targets ▪ Target weight loss at 6 mths: 6-10 kg (not more than 1-2 kg per month)
▪ Calculating energy requirements (for impending pubertal boy wrt standard weight for height)▪ RDA = 3410 kcal/day
▪ REE x 1.3 = 2286 kcal/day

Case 4 - management
▪ Dietary intervention▪ Meal plan providing 2500→2000 kcal/day▪ Increase fruit & vegetable intake, calcium
supplements▪ Strategies for healthier food choices when
eating out, cut down on snacks/sweetended/ soft drinks
▪ Exercise prescription ▪ Exercise programme: 1-2 weekly for 12
months, monthly for 6 months▪ Recommended activities prescribed by
Sports trainer
▪ Family focus – Multi-disciplinary team
▪ SMART goals
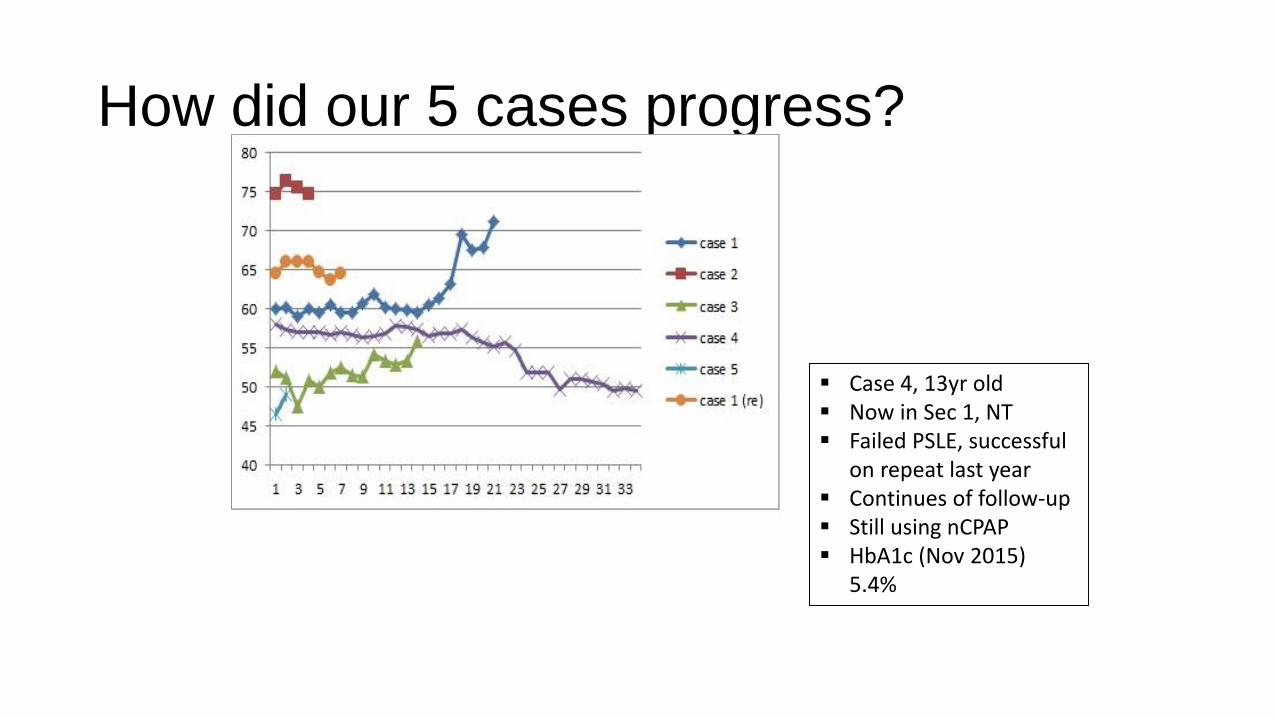
How did our 5 cases progress?
▪ Case 4, 13yr old▪ Now in Sec 1, NT▪ Failed PSLE, successful
on repeat last year▪ Continues of follow-up▪ Still using nCPAP▪ HbA1c (Nov 2015)
5.4%

Childhood obesity management programs
▪ Lifestyle intervention (Dietary, Physical activity, Behavioural)
▪ Combined (Behavioural + Pharmacologic) intervention
▪ Bariatric surgery programs

The evidence for components of obesity programs
▪ Multi-component approach with strategies that target motivation for change and emotional obstacles more useful
▪ Knowledge of nutrition and exercise alone is not sufficient
▪ Time frame to completion
▪ Structured behavioural programme
▪ Self-monitoring of food and physical activity, goal setting, stimulus control, contingency planning

Effectiveness of Lifestyle interventions in Childhood obesity
▪ Efficacy depends on duration, dose and content of treatment programmes
▪ Optimal treatment for maintaining long term weight loss has not been identified
▪ Studies reviewed in meta-analysis – heterogenous (age group, severity of BMI, duration, intensity)
▪ Improvement to cardiometabolic outcomes
▪ Can be independent of weight loss or body composition change
Family based and novel approaches
Family based:
▪ Parents taught nutrition and physical activity components with behaviourchange strategies
▪ Empower parents to provide an environment that is conducive to healthy behaviour instead of weight loss
▪ Sustain healthy behaviours that will lead to BMI changes
▪ Outcomes for < 12yrs is better
▪ Some parent only interventions
Novel approaches
• App based interventions – child/ youth friendly
• Tracking and monitoring with coaching features

Severe obesity in children
▪ Few studies of lifestyle modification therapy in youth with severe obesity
▪ High attrition rate
▪ Family based behavioural interventions associated with better outcomes, especially in early childhood
▪ Medication + behavioural therapy: Orlistat only approved by FDA for > 12 yr old (modest weight loss – BMI reduction 2.4%)
▪ Bariatric Surgery Programs
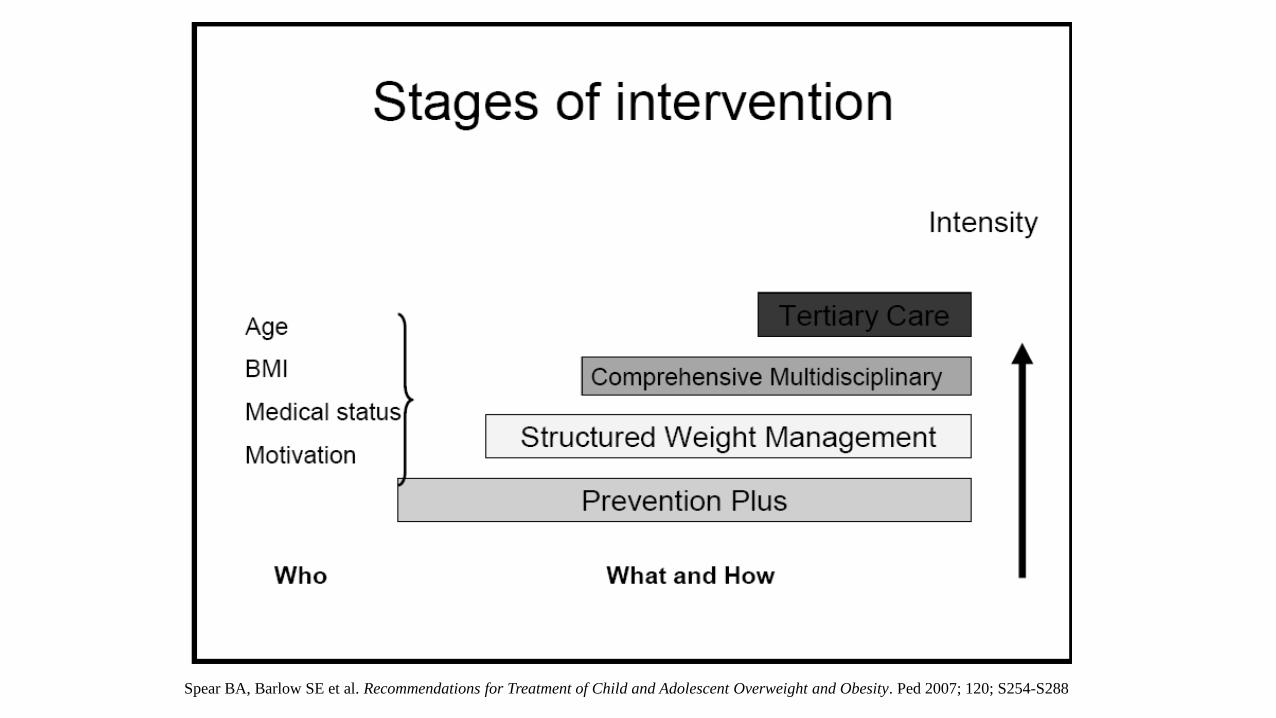
Spear BA, Barlow SE et al. Recommendations for Treatment of Child and Adolescent Overweight and Obesity. Ped 2007; 120; S254-S288

Focus on a fitter futurePlanning, Building and Sustaining a Pediatric Obesity Program: A Survival Guide
Section 1: Starting with a vision

Final points: Are we in crisis?
▪ The components of interventions for childhood and adolescent obesity needs approaches that are:-▪ Evidenced based, Risk stratified, Accessible, Sustainable, Cost-effective
▪ “Knowledge alone is insufficient”
▪More resources – Obesity as a chronic disease
▪ Implementation of policy changes needed (ideally studied)
▪ A call to action!

References1. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to
2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. NCD Risk Factor Collaboration (NCD-RisC)
2. “Chubby kids are more likely to be fat as adults” Straits Times (20 June 2017)
3. Obesity prevention and management: Singapore's experience. Foo LL, Vijaya K, Sloan RA, Ling A. Obes Rev 2013 Nov;14 Suppl 2:106-13. doi: 10.1111/obr.12092
4. NutureSG: Action Plan Report 2017. Building Strong Minds, Strong Bodies, Strong Hearts.
5. Early adiposity rebound: review of papers linking this to subsequent obesity in children and adults. Taylor RW, Grant AM, Goulding A, Williams SM. Curr Opin Clin Nutr Metab Care 2005 Nov; 8(6):607-12
6. Kelly, Barlow et al. Severe Obesity in Children and Adolescents: Identification, Associated Health Risks and Treatment Approaches: A Scientific Statement from the American Heart Association. Circulation 2013; 128
7. Spear BA, Barlow SE et al. Recommendations for Treatment of Child and Adolescent Overweight and Obesity. Ped 2007; 120; S254-S288
8. Whitlock et al. Effectiveness of Weight Management Interventions in Children: A Targeted Systematic Review for the USPSTF. Ped 2010; 125; e396
9. Shrewsbury, Vanessa A., et al. "A randomised controlled trial of a community-based healthy lifestyle program for overweight and obese adolescents: the Loozit® study protocol." BMC Public Health 9.1 (2009): 119.
10.Oude Luttikhuis, H., Baur, L., Jansen, H., Shrewsbury, V. A., O’Malley, C., Stolk, R. P.,et al. (2009). Interventions for treating obesity in children. Cochrane Database of Systematic Reviews. doi:10.1002/14651858.CD001872.pub2.
11.Ho, M., Garnett, S.P., Baur, L., Burrows, T., Stewart, L., Neve, M., Collins, C. (2012). Effectiveness of Lifestyle Interventions in Child Obesity: Systematic Review with metanalysis. Pediatrics, 130, e1647