chf what the big picture
TRANSCRIPT

Case conference “Heart Failure” From clinical to Basic Research
96/4/6 R 林軒名 / VS 陳業鵬

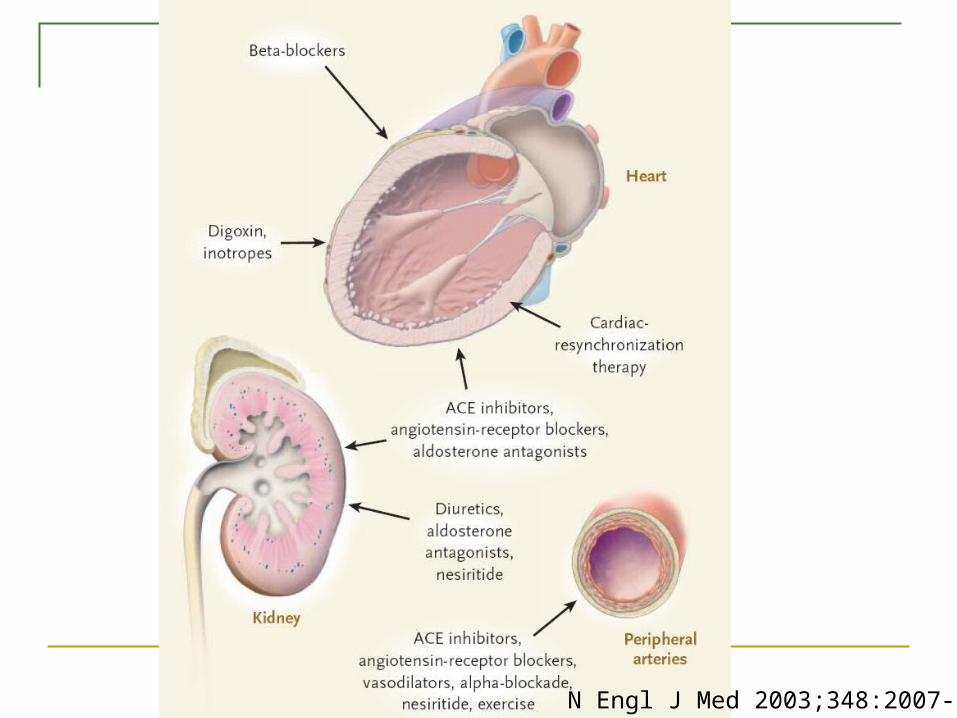
Pathophysiological Mechanisms Important in the Syndrome of Heart Failure
N Engl J Med 2003;348:2007-18
N Engl J Med 2003;348:2007-18

N Engl J Med 2003;348:2007-18

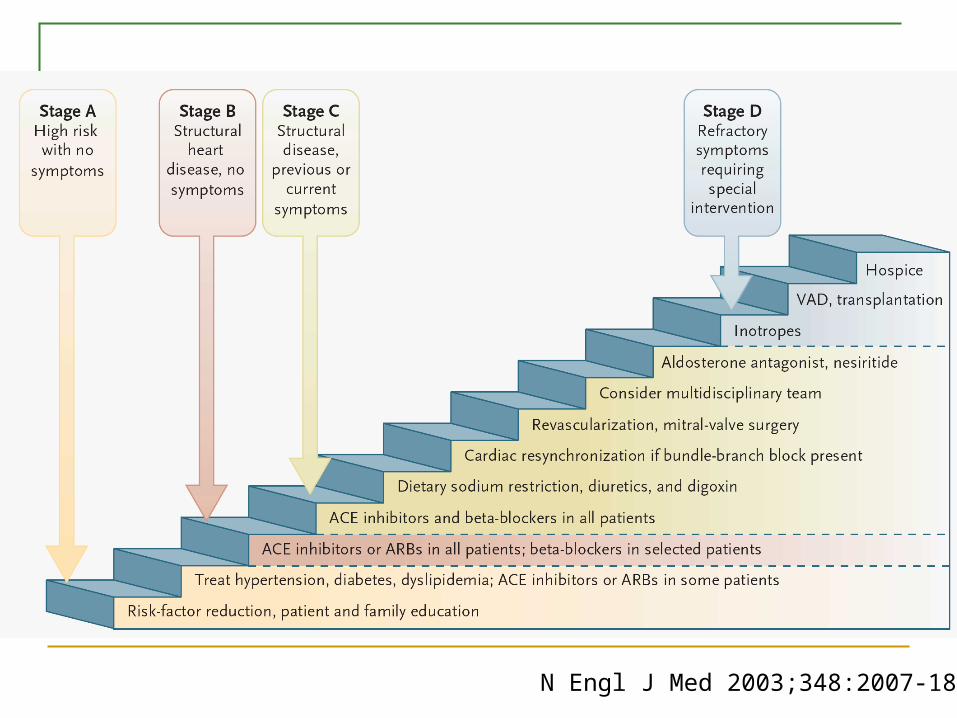
ACC/AHA 2005 Guideline

N Engl J Med 2003;348:2007-18

Heart failure imbalance of energy and load

Energy
Loading Ischemia
Infarction
Myopathy
Hypertension
Vulvular disease
Myopathy
Failing Heart
Neurohormonal activation:Renin-Angioensin system,
Adrenergic system, cytokine, etc.Peripheral alteration
kidney, lung, muscel…
Peripheral vascular resistence
Journal of physiology 2003:055 Energy matabolism in heart failure

Medical ProgressThe Failing heart : An engine out of fuel
N Engl J Med 2003;348:2007-18

30 to 40% of patients die from heart failure within 1 year after receiving the diagnos
Treatment of chronic heart failure with angiotensin-converting–enzyme (ACE) inhibitors, aldosterone antagonists, beta-receptor blockers, and resynchronization therapy.
The modulation of cardiac metabolism has promise as a new approach to the treatment of heart failure.
Cardiac energy metabolism
Fuel form food: substrate utilization Glucose or free fatty acid breakdown Beta-oxidation and glycolysis, Kerb’s cycle. Mainly energy is from
Energy production: Oxidative phosphorylation. Mitochondria respiratory chain
Transport of energy and consumption by the engine: ATP transfer and utilization.


Assesment of cardiac energy system Phosphorus-31 magnetic resonace In vivo turnover rate of glucose and free fatty
acid Rate of oxidative phosphorylation and ATP tr
ansfer.
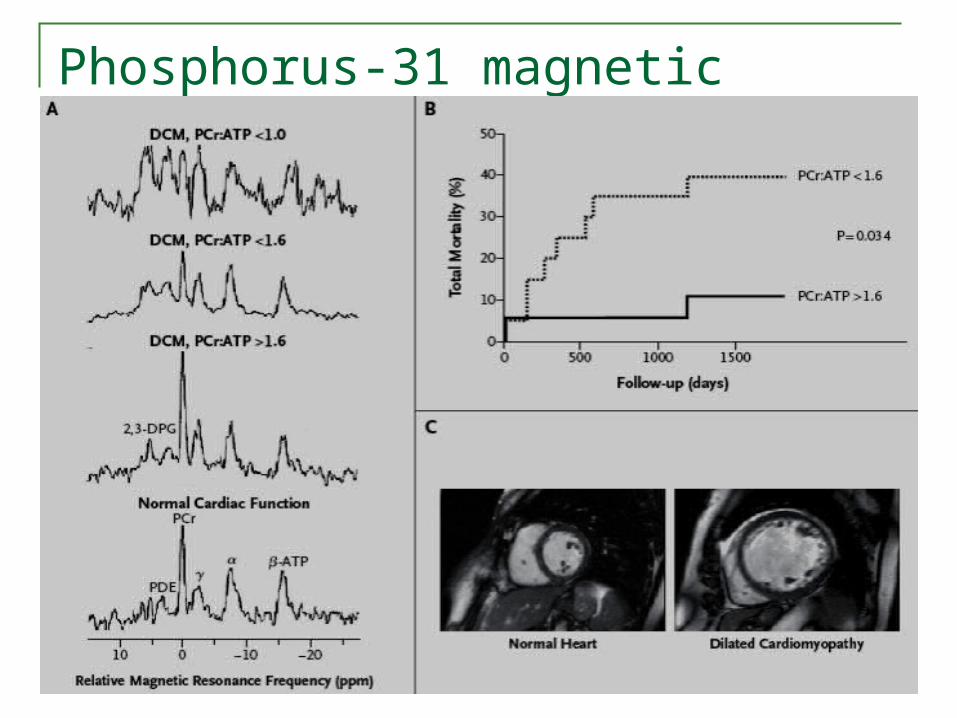
Phosphorus-31 magnetic resonace

Derangement of “Substrate Utilization” Free fatty acid:
unchange or sligh ▲ uptake in early HF, ▼ uptake in advanced HF.
Glucose ▲ uptake in early HF ▼ uptake in advanced HF: insulin resistance deve
lops in the myocardium In late HF, substantial increases in the conce
ntrations of plasma free fatty acids, glucose, and insulin that are common.
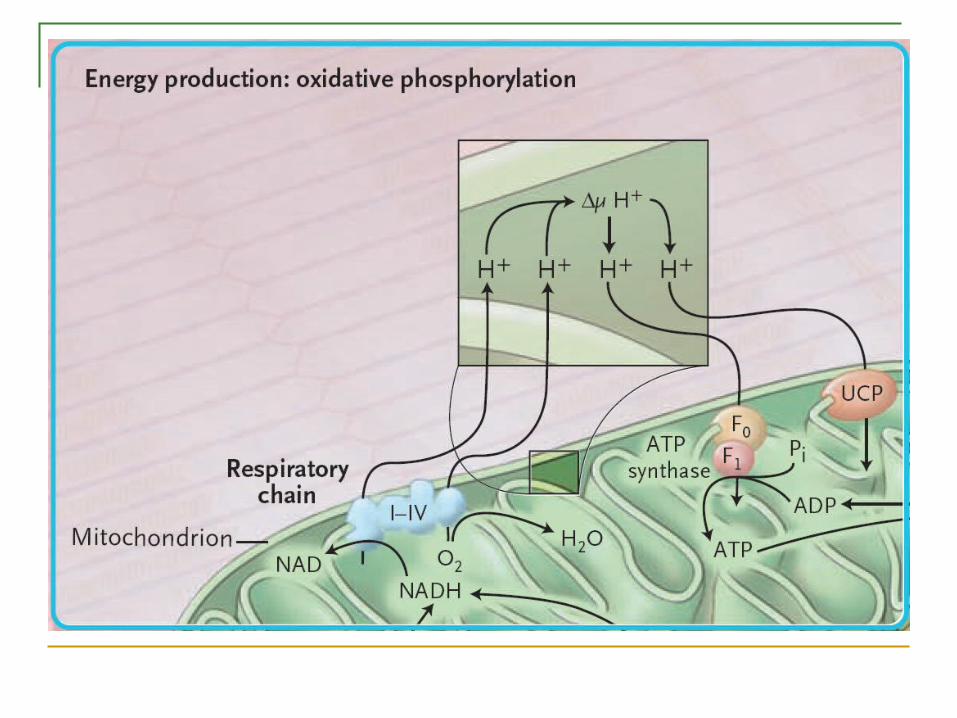

Derangement of “Oxidative phosphorylation” Cardiac mitochondria have structural abnormalitie a
nd are probably increased in number. The activity of electron transport–chain complexes a
nd ATP synthase capacity are reduced The regulation of oxidative phosphorylation by the p
hosphate acceptors ADP, AMP, and creatine is impaired
The levels of uncoupling proteins may be increased. Result in a substantial reduction of oxygen consump
tion and energy production in the failing myocardium.

Change in ATP transfer and utilization ATP transfer ▽ Cr pCr ▽ ADP ATP ▽ Free ADP △
Contractile work is not affected due to remaining ATP in early HF.
Derangement of “high-energy phosphate metabolism” phosphocreatine and total creatine levels decrease Down-regulation of the creatine transporter function
contributes to the reduced total creatine, and thus phosphocreatine levels.
The losses of high-energy phosphates and creatine kinase activity cause a severe decline in ATP transfer.
Reduction in energy delivery to the myofibrils by up to 71%.
Loss of inotropic reserve. dyspnea on exertion.

Derangement of “high-energy phosphate metabolism” The ratio of phosphocreatine to ATP: powerfu
l index of the energetic state of the heart The total creatine level falls, and this reductio
n further decreases the phosphocreatine:ATP ratio.
pCr:ATP ratio correlate with NYHA fc and with indexes of systolic and diastolic function.
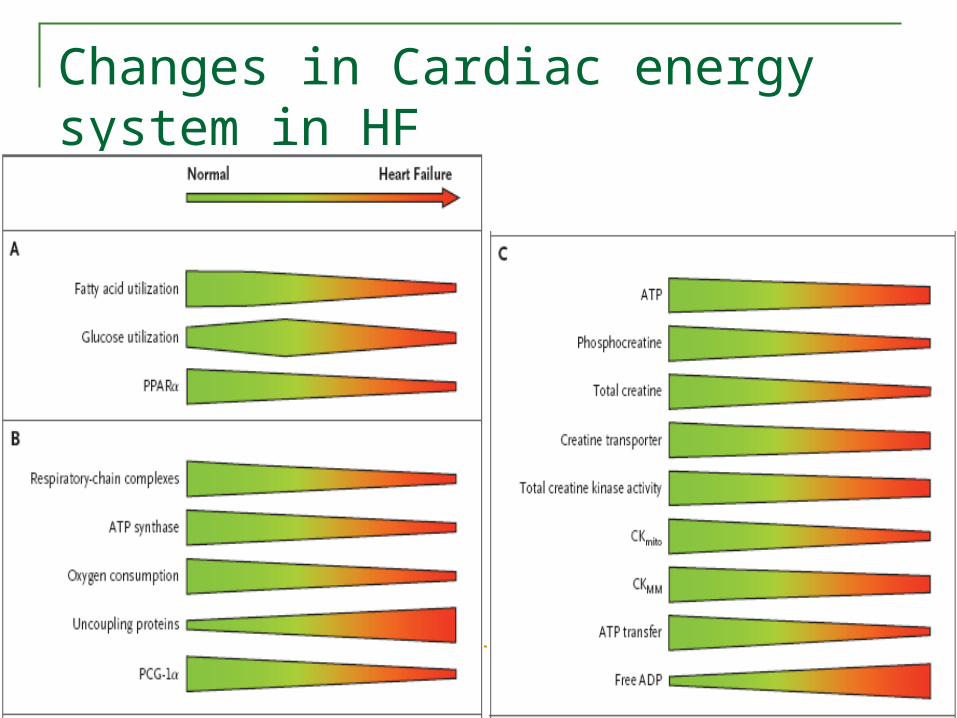
Changes in Cardiac energy system in HF

Energy production
↓ O2 and nutrient
↓ Mitochondria
↓ Mi-CK
Energy transfer
↓ Cytosolic CK
↓ AK
↓ Creatine
Energy utilization
↓ ATPase
↓ Bound CK
↓ Organella interaction
↓ ATPase synthesis↓ PCr synthesis
↓ Phosphate: potential
↓ pCr/ATP ratio↓slowing of pCr shuffle
↓ calcium uptake↓contractile kinetics
↓ Ion pump
Journal of physiology 2003:055 Energy matabolism in heart failure
Molecular Regulators of Energy Metabolism Proliferator–activated receptor (PPAR) :
PARα PPARβ PPARγ(PGC-1 )
Also see Insulin-Resistant Heart Exhibits a Mitochondrial Biogenic Response Driven by the Peroxisome Proliferator-Activated Receptor-/PGC-1 Gene Regulatory PathwayCirculation. 2007;115:909-917.

PPARα
PPARα controls the expression of enzymes directly involved in fatty acid oxidation
In cardiac Hypertrophy, the expression of PPARα is decreased in proportion to the depression of fatty acid utilization.
The down-regulation of PPARα is thought to be the main mechanism underlying the switch in substrate utilization from fatty acids to glucose. This switch is typical of the hypertrophied heart.

PPARγ
PPARγ coactivator-1 (also known as PCG-1α), is a master regulator of metabolic function in mitochondria.
Activates multiple genes : PPARα and PPARβ and nuclear respiratory factors 1,2 For fatty acid uptake and oxidation and for oxidative phosp
horylation. Inhibition of PCG-1α probably as a direct consequen
ce of high plasma catecholamine levels, leads to down-regulation of mitochondrial gene expression.

Mouse Gene-Knockout Models and Human Inborn Errors of Metabolism and Their Cardiac Phenotypes.
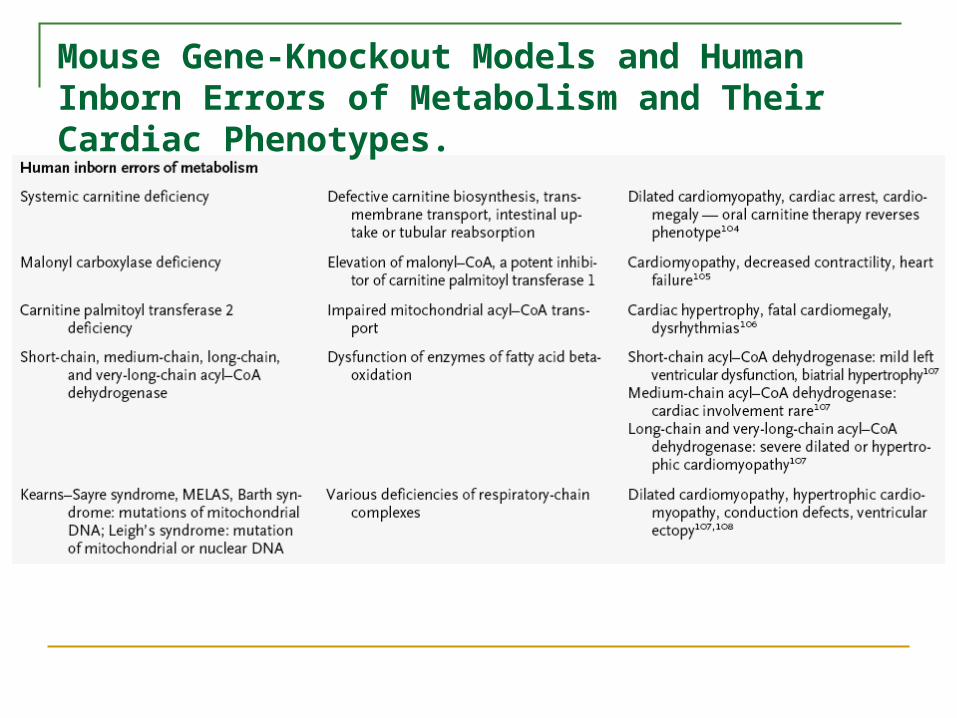
Mouse Gene-Knockout Models and Human Inborn Errors of Metabolism and Their Cardiac Phenotypes.

Modulation of Substrate Utilization Hint:
intracoronary infusion of pyruvate glucagon-like peptide 1 transgenic overexpression of glucose transporter 1
Partial inhibition of fatty acid oxidation: trimetazidine, perhexiline
Carnitine palmitoyl transferase 1 inhibitor: etoxomir

Modulation of Oxidative Phosphorylation Direct stimulation of oxidative phosphorylatio
n is not available Possible way : increasing PCG-1α activity as
a means of up-regulating oxidative phosphorylation enzymes

Manipulation of High-Energy Phosphate Metabolites Creatine and phosphocreatine levels can be
augmented by increasing the creatine transporter function ( not effective)
Improve the myofibrillar efficiency of ATP utilization with new calcium-sensitizing or myosin activator compounds.
What is the big picture ?
Truth of cardiac energy metabolism? Metabolic therapy of heart failure? Energy metabolism of other organ?
N Engl J Med 2003;348:2007-18

ACC/AHA 2005 Guideline