cheryl mccullagh - sydney children's hospitals network - emm - patient safety in an imperfect...
TRANSCRIPT

Patient Safety in an imperfect world
Cheryl McCullagh
Director Clinical IntegrationMarch 2016



Safety First
Lifetime Care

E ref
Registered with pt portal
My team
Triage/Pre assessment
Education commences
referrer informed of
plan and dates
SMS reminders
Allied/nursing check in
E-clinic with GP
Self check in kiosk
Specialty clinic face to face
billing
Specialty care
Team update
eRFA Pre planning
education
billing
admit
Self check inPt portal
update for DC
IP notes
IP education
DC communication
Follow up

The MEMORY strategy describes the plan for implementation of a fully integrated
health record across SCHN; it involves more than 30 projects. Aims include:
safer care
better access, for multiple users
current complete records
reduced risk around missing or incomplete information
reduced errors
accessible to all from anywhere
improved reporting
In supporting these strategic aims, there are implications for the way we do business. The overarching guiding principles and business implications need
to be dealt with as much as possible before implementation

Westmead
Randwick
2013 2014 2015 2016 2017
EMM
Clin-docs EMR2
SurgiNet
PathNetc/compass
Move off iPMto SCHN stack
Voice Recin ED
eRFA
PAS feedTo CHW
EMM
FirstNet
SCHN Roadmap
7
EIR SCH scanning
HealthenetNEHR
Voice Rec. Doc
EMR SCHN
BackscanningLanier
Endoscopy
Endoscopy
VR Lanier
VR Lanier
Reports Lync MRD Scanning Coding Email tap-on log-on WIFI IT support BYOD
NAP forms
CCIS
CCIS
NAP forms
EMR SCHN
Mental Health doc.
Mental Health Doc.
Rehab
Referrals
EMR2
FirstNet
Oncology
Billing App.
HealthenetNEHR

EMM Progress so far…..
8
• Project formally commenced in March 2014
• Completed IT2
• Technical go-live in 4 weeks
• Design reviews
• Pharmacy processes: 48 representatives from eHealth, SESI and Pharmacy
• Oncology processes: Almost 70 staff from Oncology (CHW and SCH)
• Medication Processes: 250 staff from Medical, Nursing, Pharmacy, Allied Health, Blood Bank, Nuclear Medicine, Radiology, eHealth and members from other EMM pilot sites
• Focus groups formed for specific issues
• Future state workflows in partnership with NSW
• Training has commenced
• Research plan underway with support of Macquarie University and NHMRC partnership grant

SCHN
Board
Exec
ISEC
SCHN
HCRC
AlliedMedicalNursing
State EMR2
TechnicalAdmin
Forms POW
Governance
SCHN
HCQC
State EMM
MEMORY
SCH
(forms)
EMM/EMRPCHW
(forms)
EFG
ICT SES
EMR SES
POW EMMDoc.
Imaging

Principles for safe EMM
Don’t make things worse
Decisions are clinically lead
New risks have to balance current state
Safety nets for risks
Mandatory training JIT
E-process becomes the standard
Research and evaluation
Consider the question safe vs Safer?

Current drivers
Networked patients
Shared care
Patient Safety
SCHN reported in 2015
1523 Medication/IV Fluid Events were reported
931 (61%) related to administration
404 (27%) related to prescribing
56 (4%) related to dispensing
Top 10 Medications Implicated in Medication/IV Fluid Incidents CHW SCH Grand Total
IV Fluids 86 49 135
Morphine 39 30 69
Paracetamol 27 34 61
Parenteral nutrition 34 9 43
Vancomycin 26 16 42
Piperacillin + tazobactam 17 19 36
Oxycodone 19 10 29
Flucloxacillin 19 10 29
Fentanyl 14 14 28
Gentamicin 14 10 24
Over 200 different medicines were reported during 2015.

Cerner eMM
MedChart eMM
ICCIS
HPPL
HNE LHD
MDC
12
SCHN, SESI,
SWS
St Vincents
NSW Health
(metavision)
NSW Health
(iPharmacy)
JHH and others
Working with ehealth and
other sites
To standardise content and
encourage intra-operability
between systems.

Improved Patient Safety
Benefits of eMM translated into research
DecisionSupport
and Alerts
AllergyChecking
Automated Rules
ImprovedLegibility of
Prescriptions
Dosage Calculation Support
Improved communicatio
n between HCP and care
settingsImproved worflow
Reduction in serious
errors
Increased staff and patient /carer
satisfaction
Standard-isation

Supporting safer medication workflows, working with the software
Drug-Drug interactions
Dose capping
Reference text links
Height, Weight, Allergy rule
Phone order process
Banner bar weight
Order sentence filtering
Referenced order sentences
Paracetamol alert
Minimal interval checking
Powerplans
IV fluid m-page
Hot Keys

• This is standard Cerner functionality.
• We have aligned with the other lead sites and set the
sensitivity to Major-Contraindicated for prescribers and Major
+ Major Contraindicated for pharmacists
Drug-Drug Interactions

• SCHN is a testing partner for new functionality
• Targeted to high risk drugs and utilising the “normalised” or
mg/kg weight-based calculations to ensure that maximum
doses are not exceeded for overweight patients
Dose Capping

• Hyperlinks to specific drug related policies on the SCHN
intranet
• Reference text can be set to pop-up or open after clicking an
icon
• E.g. direct link per drug to the AMS approval form for restricted
antimicrobials
Reference text links

• Alerts prescriber if patient parameters are missing
• Once the medication order is selected, alert is fired when
patient parameters have not been recorded.
Height, Weight & Allergy Rule

Proposed phone order process –
Nurse 1 takes
phone order and
searches for drug
and order sentence
Selects name of
prescriber from list
and chooses
‘phone order’
communication type
Completes order
details, change
frequency to ONCE
Nurse 2 reads back
order details to
prescriber
Nurse 2 enters
name in order
comments as
“Phone Order”
Nurse 1 administers
medication
Nurse 2 witnesses
and password entry
for dose
administration
Prescriber gets
message to
approve order in
message centre

Proposed Banner Bar weight
20
Current
Proposed

• To minimise the risk of inappropriate selection from long lists
• Paediatric lists are long due to various age and weight options
Order Sentence Filtering

Filtering by age and weight
22
• SCHN is a test partner for this new functionality.
• Improves the prescriber’s experience by displaying relevant orders
• Improves patient safety by minimising risk of inappropriate doses being
selected (e.g. neonatal doses won’t display for adolescents and vice versa)

• All order sentences have been referenced where possible via
the Drug Dosage Guidelines field to indicate source of
information (e.g. CHW or AMH references)
Referenced Order Sentences

• Warns nurses if the patient is about to receive more than the
maximum recommended daily dose.
• The rule is being configured to check for doses that would
exceed 60mg/kg/day and 4000mg/day, whichever is the lower
value.
• Common overdosing error, and can be fatal in paediatrics
Paracetamol Alert

• Warns nurses if they are attempting to give a dose too soon
after a previous dose. Particularly useful for PRN orders.
• E.g. Oxycodone ordered as a PRN medication
• Alert is fired when attempting to administer the medication
before the scheduled time.
Minimum Interval Checking
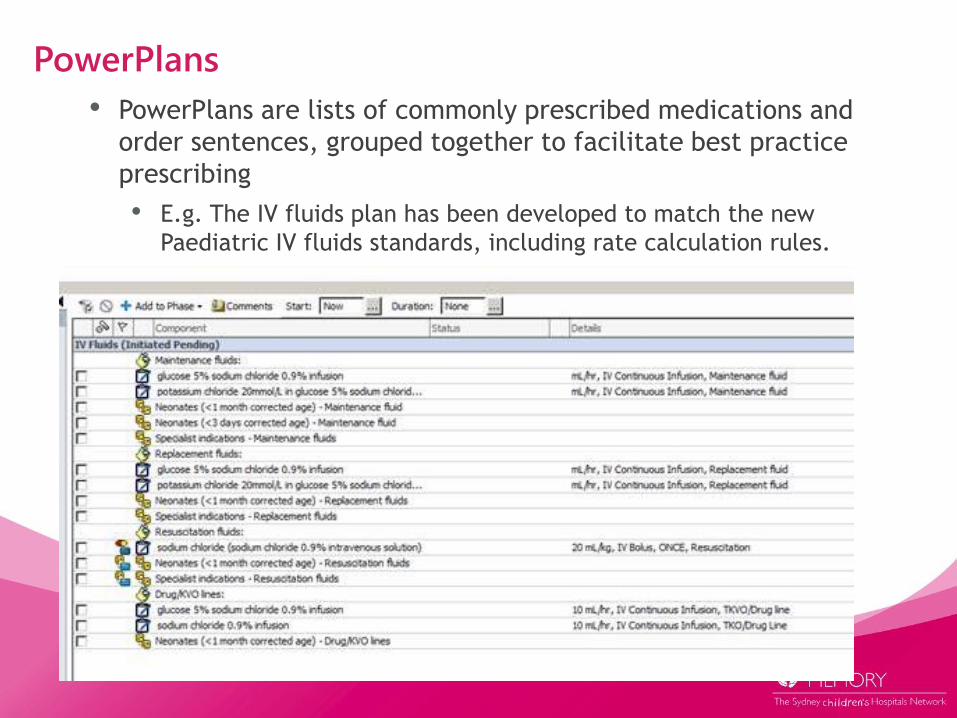
• PowerPlans are lists of commonly prescribed medications and
order sentences, grouped together to facilitate best practice
prescribing
• E.g. The IV fluids plan has been developed to match the new
Paediatric IV fluids standards, including rate calculation rules.
PowerPlans

IV fluids m-page app.

What if the software doesn’t do what you need?

Hotkeys –unintentional errorY = 1st January
R = 31st December
M = 1st day of the current month
H = last day of the current month
W = 1st day of the current week (last Monday)
K = last day of the current week (next Sunday)
T = today
If the medication has a mandatory witness field, and you don’t move the cursor
into the field before typing, and the witness has a surname beginning with one of
the letters listed above, they may inadvertently adjust the time the medication is
documented to one of the above dates.
Default settings -No restriction on backdating, 60 minute restriction for forward
dating.

Delay issue 1. Additional doses
Issue: 1072 Status
Inappropriate additional dose
administration tasks generated on
MAR by system due to various end-
user activities.
These include nurse documenting an
administration task prior to the
scheduled time and a modify action
occurring between the early
administration time and the scheduled
administration time:• Clinician or Pharmacy modify on Core
attributes to the order• Modify on user defined fields
Modify on order comments
Mitigation strategies have been
proposed for Australian paediatric
setting.
Fix requires code (no release date and
code upgrade required)
Overall, this defect in the Millennium code results in non-physician prescribing
– the system is generating additional dose administration.

Modifications Leading to Additional Task
Pharmacist ‘verify’ or ‘modify’ an order in PharmNet, including adding a
comment (annotation), specifying a dose form (product assignment required for
dispensing).
Prescriber modifying an order, including adding an Antimicrobial Approval
Number.
2. MO changes
dose of
morphine or
Pharmacist
verifies order
and adds order
comment.
3. Patient returns to room after dressing
change – shift change, new nurse
reviews chart and sees outstanding task,
task is now overdue and shows up red
1. Nurse gives dose
of morphine one
hour early as
dressing change
rescheduled.
4. Patient is on
multiple
medications so
MAR is visually
complex. The last
morphine dose is
not shown on the
screen5. The minimum
interval checking
doesn’t fire, the
extra dose is given
and the patient
develops respiratory
depression.

Possible Mitigation Strategies (1 of 2)
Mitigation Factor Work Effort Next Step
Minimise core modifications by
seeking to increase Auto Product
Assignment.
Revisit APA and evaluate
whether risk of inappropriate
APA is outweighed by task
generation
Build review
(order
catalogue,
order
sentences)
Review all order sentences and
include dose form where possible
Will require more dose form
specific order sentences
Build review
Rule to advise Prescribers and
Pharmacists that they may be
creating an additional task and to
review and act on it.
Not possible functionally for
prescribers but is for
pharmacists in PharmNet on
verification.
Workflow
changes
Rule to warn nursing staff of
duplicate task on opening chart.
Possible functionally. Will
require acceptance by
nursing.
Workflow
changes
Rule when fired can also produce
following actions: page, message
centre, task list, email.
Under investigation (including
who would receive and act on
the information)
Cerner
Investigating

Possible Mitigation Strategies (2 of 2)
Mitigation Factor Work Effort Next Step
Minimal interval alert Will require education/training
for exceptions.
Update training
point
Last dose administered tile along all
orders
Will require
education/training.
Update training
point
Single chart open at any one time Alert fires on chart opening if
additional task present.
Requires
configuration
Close chart after each medication
administration session
Education/Training point Update training
point
Audit report at each Go Live (of
alert)
Which medications and
actions created the task
Create report
No order modification by
Prescribers (Oncology excepted)
Oncology prescribers Workflow
changes and
Training
24/7 pharmacist support From Go Live onwards for
prompt verification of all
orders
Executive
Decision

Impact in Tertiary Paediatrics vs Other Sites
Task Other sites Risk at CHW
Pharmacy
verification
Workflow differs to American workflow, where 24/7
Pharmacy services and unit dose dispensing allow
for verification prior to all doses being
administered.
Many more doses given
before verification.
Autoverification Some adult sites in Australia utilise autoverification
– CHW has this preference turned off as few
orders would qualify due to the high usage of
weight based dosing and other paediatric
complexities.
As above – more orders
affected by the defect.
Auto product
Assign
Utilised by adult sites in Australia but turned off for
CHW as dose form assigned often inappropriate
(50% cases for dispensed products)
Dose form could be included
by adding many more order
sentences – could introduce
menu selection error risk.
Dose form in order
sentence
Utilised in other sites to maximise APA and AV See above
Administration prior
to scheduled time
Schedule built according to NIMC and to minimise
menu selection error with all potential schedules
included.
Each ward at CHW has a different variance on
administration times due to medications
prescribed, meals and snacks, sleep patterns,
gate leave, shift patterns, patient acuity,
procedures and interventions. Challenge to
standardise administration times.
Rescheduling of doses
common. Dose are more
likely to be administered
before the scheduled time.

Adverse Events Reported At Other Sites in Australia
Site Adverse Events
A Incident has occurred but was picked up
B 2 incidents occurred.
C Investigating – an issue early on, less of a problem now
Alternative workflows/mitigations not accepted
• Ops job created to run continuously to remove additional tasks so
it is not visible to the administrator
• Reports created to check additional dose events
Consequence, 4 +4 week delay $500K

Issue 2 Between the flags
• Issues with the current build were identified
36

Issues CHW CERS Committee comments Status/Cerner’s comments
Alterations to calling Criteria (ACC) 48hrs is
the maximum time an ACC should be
prescribed for (as per State policy), however
the current build allows clinicians to enter an
indefinite review date/time (for example; the
next review may be set for 24 months’ time).
Once an ACC is prescribed it disables the
pop-up alert that notifies clinicians that the
patient is in the yellow or red zone. This is
a significant patient safety issue as staff
may not realise a patient is in the red
zone and/or deteriorating, and requires a
mandatory Rapid Response.
This item is not currently included
within the enhancements project.

Issues CHW CERS Committee comments Status/Cerner’s comments
Alterations to calling Criteria (ACC) 48hrs is
the maximum time an ACC should be
prescribed for (as per State policy), however
the current build allows clinicians to enter an
indefinite review date/time (for example; the
next review may be set for 24 months’ time).
Once an ACC is prescribed it disables the
pop-up alert that notifies clinicians that the
patient is in the yellow or red zone. This is
a significant patient safety issue as staff
may not realise a patient is in the red
zone and/or deteriorating, and requires a
mandatory Rapid Response.
This item is not currently included
within the enhancements project.
CHW CERS Committee comments Status/Cerner’s comments
2. Prescribing an Alteration to Calling Criteria (ACC)
does not require the user to sign off/enter their
password. There is box labelled ‘sign’ that must be
selected to complete the transaction but selecting it
just results in the user activating the prescription
and exiting the screen.
This prescription can currently be completed
by any clinician with access to it. State policy
identifies that only a Medical Officer has the
authority to do this.
Logged as an enhancement (ref 7.5
Acc Form Design CR 1-8777290216 -
7.5.2 Requirements #13) and
available for install to all domains by
this time next year.

Issues CHW CERS Committee comments Status/Cerner’s comments
3. Observations that are charted outside the
range of the chart are not able to be viewed.
Single observations and trending of
observations will be impacted. This is a
particular concern for those patients (such
as febrile/neutropenic oncology patients)
that can sit outside the graph for extended
periods of time.
Logged as an enhancement (ref
7.3 Extreme Values Displayed CR
1-8777290173 - 7.3.2
Requirements #6 & #10) and
available for install to all domains
by this time next year.

Issues CHW CERS Committee comments Status/Cerner’s comments
The most recently entered heart rate measure
is cut off affecting the readability of the
observation.
This issue is also transferred to the
printed version of the chart (in the
instance the patient is transferred to
another facility or is the subject of a case
review and the chart needs to be printed).
This will be addressed in the
enhancements under 10.7 Time
Modification and available for
install to all domains by this time
next year.
An additional 15 minutes of blank
graph space beyond the current
time will be visible to the right of
the graph so that observations are
displayed clearly.

Issue examples: Cannot see the trend where measurements are off the chart
41

Issue examples: alerts have to be suspended before review
42

Implications of BTF
• eHealth/Cerner have agreed to changes/corrections for delivery in 2016
• CHW CERS Committee recommended that the issues be addressed prior to implementing within SCHN
• SCHN decision to delay introduction of electronic charts
• Interruption of emm/emr workflow
• Delay device integration with vitals monitors
• Paper charts to continue to be used
• Delay to importing observations from fixed and mobile monitors
• BTF will go live after the EMM/EMR rollout, split workflow with aspects of meds, iview, carecompass, and devices
43

Delay Issue 3 Prescription outputOption Risk / Challenges
Implement ‘V1 - white’ prescription for go-live.
• Computer generated prescriptions for hospital
dispensing
• Schedule 2, 3 and 4 meds
• Schedule 8 meds
• May need to exclude S4B and Clause 37
meds
• Handwritten prescriptions for S100 HSD meds
(current state)
• Handwritten prescriptions from outpatient clinics
(current state)
• Require legislative exemptions (eHealth to
facilitate)
• Split workflow for different medication types and
prescription types
• Credibility / adoption
• Risk of error
• V1-white requires further testing and potentially
defect resolution
Do not go-live with prescription output in April and
continue with handwritten prescriptions.
Implement ‘V2 – white, blue and green’ when
available
Split electronic/paper transcribing workflow
• Credibility / adoption
• Risk of error
Lack of resources to test and implement final V2
code when available
V2 White, Blue and Green would be developed by
another site. CHW lose control of development.
Concern that estimate to complete V2 White, Blue,
Green is too low. This is being validated.

Implications
• 2 month delay to project
• Cost of $500K
• Modified workflow for some medications for an
indeterminate period
• Future implications of aiming for a paper workflow
within and electronic workflow

Doing it safer
• Be aware not all solutions suitable to US sites work in Australia
• Involve the state or authority where it is important
• Have the support of your executive to keep safety as the first principle
• All risks need to be accepted by clinical leadership
• All risks have to be weighed against current state risks
• Work closely with vendors to resolve issues
• Don’t wait for perfect, but manage risk with strong mitigations
• Training is important but cant solve variance
• Beware the emotional whistle blower


Please
share
error data!