chemical hygiene plan mt. sinai school of medicine institutional biosafety program philip g. hauck,...
TRANSCRIPT

CHEMICAL HYGIENE PLAN
Mt. Sinai School of Medicine
Institutional Biosafety Program
Philip G. Hauck, M.S., MSHS, CIH,CPEA
3 / 2005

Introduction
• This presentation gives an over view of the main points found in OSHA and US EPA regulations covering health and safety in laboratories
• It is not all- inclusive or comprehensive• Resources, additional materials are available at:
www.mssm.edu/health_safety– http://www.mssm.edu/health_safety/pdf/chemical_hygiene_pa
rti.pdf– http://www.mssm.edu/health_safety/pdf/chemical_hygiene_pa
rtii.pdf

Material Safety Data Sheets
• Collect and keep available in your laboratory at all times-it is required by OSHA and the US EPA!!
• Refer to sheets often, especially for hazardous and toxic materials you handle in the laboratory.
• Copy and attach to Standard Operating Procedures.

Material Safety Data Sheets
• Must be provided by Vendor/Distributor as required by OSHA Standards 29 CFR 1910.1200 and .1450
http://www.osha.gov/SLTC/hazardcommunications/index.html
Must contain,CHEMICAL IDENTITY, HAZARD, CHEMICAL IDENTITY, HAZARD, HEALTH EFFECTS, TOXICITYHEALTH EFFECTS, TOXICITY information.
• Labels on containers must be printed with manufacturer/ vendor/ distributor address and lot numbers. No photocopies or hand-written labels.
Sources Of Information• MSDS’s supplied by Chemical Distributor
• Labels (NFPA and DOT hazard symbols)
• Toxicology Texts in MSSM Library
• RTEC’s Registry of Toxic Effects of Chemical Substances - NIOSH “Phonebook” of toxics
• Internet WEB sites
• Computer soft-ware
• Chemical Vendor catalogs
Sources of Information
• Merck Index
• Chemical vendor/distributor hot-lines
• IARC Monographs
• NIOSH Publications on specific carcinogens
• Toxicology Journals and Publications

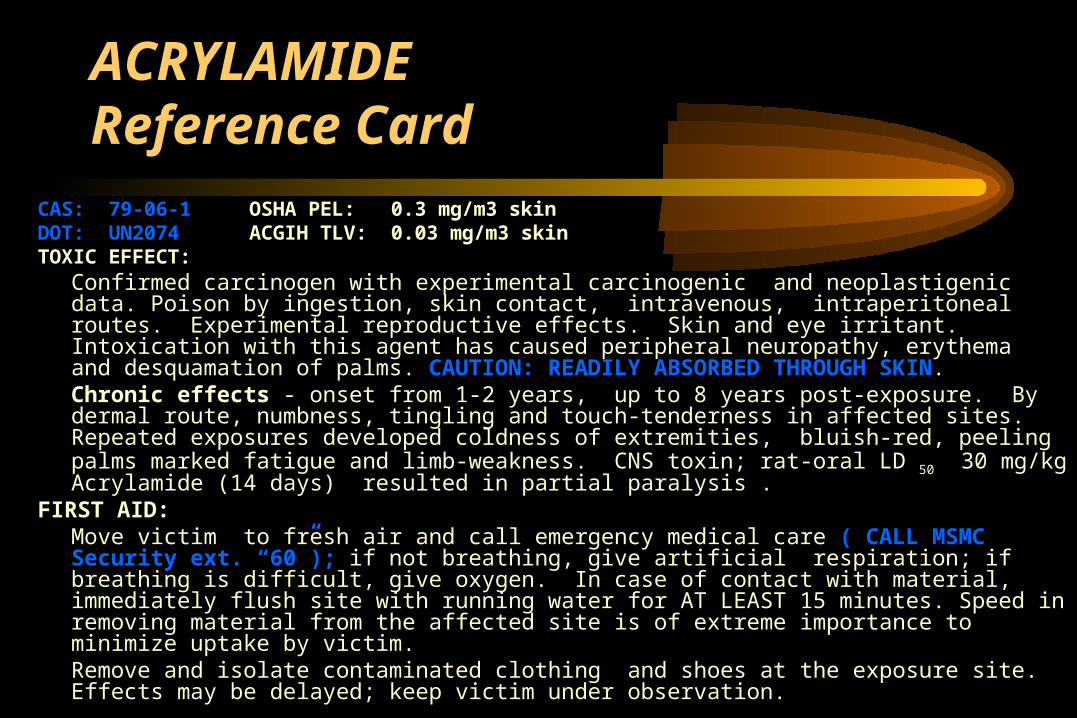
Sample Hazard Reference CardACRYLAMIDECAS: 79-06-1 OSHA PEL: 0.3 mg/m3 skinDOT: UN2074 ACGIH TLV: 0.03 mg/m3
skin TOXIC EFFECT:Confirmed carcinogen with experimental carcinogenic and neoplastigenic data. Poison by
ingestion, skin contact, intravenous, intraperitoneal routes. Experimental reproductive effects. Skin and eye irritant. Intoxication with this agent has caused peripheral neuropathy, erythema and desquamation of palms. CAUTION: READILY ABSORBED THROUGH SKIN.
Chronic effects - onset from 1-2 years, up to 8 years post-exposure. By dermal route, numbness, tingling and touch-tenderness in affected sites. Repeated exposures developed coldness of extremities, bluish-red, peeling palms marked fatigue and limb-weakness. CNS toxin; rat-oral LD 50 30 mg/kg Acrylamide (14 days) resulted in partial paralysis .
FIRST AID:Move victim to fresh air and call emergency medical care ( CALL MSMC Security ext. “60”);
if not breathing, give artificial respiration; if breathing is difficult, give oxygen. In case of contact with material, immediately flush site with running water for AT LEAST 15 minutes. Speed in removing material from the affected site is of extreme importance to minimize uptake by victim.
Remove and isolate contaminated clothing and shoes at the exposure site. Effects may be delayed; keep victim under observation.

Toxicology (PDQ)
• LD50 -- Median Dose toxic to 50% of Test population (usually mg/kg, ug/kg etc.)
• LC50 -- Same as LD50, but usually an inhalation dose i.e. (quantity) /m3 or ppm
• Dose x Response Curve -- Plot of an effect or mortality verses a given dose of chemical
• Portal of Entry -- Many chemicals exhibit different toxicities or effects depending upon point of entry.

Two Points To Remember
• How toxic is the compound?– In Humans?– In Mammals?– Ames Test / Mutagenicity Data?
• How does it enter the body?– Inhalation?– Percutaneous / injection?– Ingestion?

Inhalation:
• Uptake and distribution by bloodstream to other target organs
• Local toxicity to airways and lung • Simple asphixiant (just displaces oxygen) or anesthetic like Carbon Dioxide• Local irritation ( NH4OH )or deep in alveolar
region (COCl2)• Systemic effect on deep organs & tissues

Percutaneous ~ Injection (Dermal)
• Dilipidation of skin (local) i.e. Chloroform
• Penetration through stratum corneum - i.e. dimethyl sulfoxide (acts as a “vehicle”)
• Accidental needlestick, cuts, other skin breaks; entry into deep tissues, bloodstream
• Local Toxicity / effect (dermatitis, cracking of skin)
• Systemic Toxicity / effect (organ inflammation and /or necrosis)

Ingestion
• Deliberate / inadvertent ingestion
• Splash / spray into mouth, nasal passages
• Deposition on hands -- face
• Deposition on surfaces that are handled ~ “fomites” in biohazard control
• Hand-to-Mouth ingestion (object-to-mouth)

Standard Operating Procedures
1910.1450(e)(3)(i) “Standard operating procedures relevant to safety and health considerations to be followed when laboratory work involves the use of hazardous chemicals; “

Standard Operating Procedures
• For chemicals with toxicity < 500mg/kg (oral or inhalation) and carcinogens, ca-suspect agents, embryotoxic and allergenic chemicals
• WRITTEN PROTOCOL (not an outline) identifying all toxic chemicals and all steps to be used by personnel handling the agent(s) re: receiving, manipulation, storage, and disposal

Standard Operating Procedures
• SPECIFY ALL MANIPULATIONS/SAFETY PRECAUTIONS FOR EACH STEP
• SPECIFY ALL STORAGE / DISOSAL PRACTICES

Exposure Prevention ~ Reduction
• Perform risk assessment for all chemicals in use in your protocols
• Substitute less toxic / less hazardous chemicals if at all possible
Exposure Prevention ~ Reduction
• Design-out exposures using closed systems, screw caps, covered reservoirs, fume hoods
• Scale-down procedures (smaller quantities)
• Select appropriate personal protective equipment (PPE) that will protect you
Medical Surveillance• Employee Health Service monitoring of exposures
• Suspected poisonings / exposures / accidents go to Employee Health or MSMC Emergency Department!!
• Give: Identity of Chemical -- Exposure Conditions -- Signs and symptoms of exposure
• Written Report – MSMC Employee Medical File
ACRYLAMIDEReference Card
CAS: 79-06-1 OSHA PEL: 0.3 mg/m3 skinDOT: UN2074 ACGIH TLV: 0.03 mg/m3 skin TOXIC EFFECT:
Confirmed carcinogen with experimental carcinogenic and neoplastigenic data. Poison by ingestion, skin contact, intravenous, intraperitoneal routes. Experimental reproductive effects. Skin and eye irritant. Intoxication with this agent has caused peripheral neuropathy, erythema and desquamation of palms. CAUTION: READILY ABSORBED THROUGH SKIN.Chronic effects - onset from 1-2 years, up to 8 years post-exposure. By dermal route, numbness, tingling and touch-tenderness in affected sites. Repeated exposures developed coldness of extremities, bluish-red, peeling palms marked fatigue and limb-weakness. CNS toxin; rat-oral LD 50 30 mg/kg Acrylamide (14 days) resulted in partial paralysis .
FIRST AID:Move victim to fresh air and call emergency medical care ( CALL MSMC Security ext. “60”); if not breathing, give artificial respiration; if breathing is difficult, give oxygen. In case of contact with material, immediately flush site with running water for AT LEAST 15 minutes. Speed in removing material from the affected site is of extreme importance to minimize uptake by victim.Remove and isolate contaminated clothing and shoes at the exposure site. Effects may be delayed; keep victim under observation.

Control Of Hazards • INHALATION
– Use of Tight Fitting caps
– Closed Reservoirs (covers on buffer tanks)
– Eliminate evaporation / aerosol generation in the open space
– Use of Chemical Fume Hood / Glove Box to control release of vapors to general work space
– Reduction of Bench work exposures
Control Of Hazards
• DERMAL– Barrier garment use (Gloves, Aprons, PPE)
– Limited use of needles, glass pipettes
– Substitution of solvents (where possible) to less hazardous

Control Of Hazards
• INGESTION– Face Shields (splash to face-skin deposition)
– Hand Protection – gloves
– No Food in Laboratories / refrigerators/ walk-ins
– Routine Housekeeping i.e. cleaning benches, Hood surfaces, phones etc.

Exposure Prevention ~ Reduction
• Perform risk assessments for all chemicals in use in your protocols
• Substitute less toxic~ less hazardous chemicals if at all possible
• Design-out exposures using closed systems, screw caps, covered reservoirs, chem fume hoods or glove boxes
Exposure Prevention ~ Reduction
• Scale-down procedures (smaller quantities)
• Select appropriate personal protective equipment that will protect you specifically for the chemicals you use (no latex exam gloves for acutely toxic chemicals!!)

In Memorium**The New York Times
HANOVER, N.H., June 10 [1997] - A Dartmouth College chemistry professor has died from exposure to a rare form of mercury, first synthesized more than 130 years ago.
Karen E. Wetterhahn, 48, who also had served as an associate dean and a dean at the college, died on Sunday, about 10 months after accidentally spilling a few drops of dimethylmercury on her disposable latex gloves while performing a laboratory experiment. The substance, which has no practical application, is used in research on heavy metals.
Prof. John S. Winn, chairmen of the college's chemistry department, said Professor Wetterhahn was a leader in the study of how heavy metals can initiate cancer at the molecular level. Dimethylmercury is so rare that it is only in use in perhaps 100 laboratories worldwide at any given time, he said.
In Memorium**Through a search of medical literature, the college determined that exposure to the substance killed two laboratory assistants in 1865, shortly after it was first synthesized, and a 28-year-old chemist in 1971.
After years of study[ing] chromium metal toxicity, Professor Wetterhahn had turned to the study of mercury in a sabbatical at Harvard University in September 1995, Professor Winn said. In the experiment at Dartmouth last August, she had used dimethylmercury to set up a standard against which to measure other mercury involved in her research.
The drops apparently spilled onto her gloves, passed quickly through the latex and were absorbed through her skin. After her illness was diagnosed in late January, the college had the latex gloves independently tested, and it was determined that the mercury could pass through in 15 seconds or much less.

**It was Dr. Wetterhahn’s wish that all Occupational H&S Professionals get
the word out to her colleagues about the dangers of using the wrong Personal Protective Equipment with hazardous chemicals


Good Chemical Handling and Storage
• Refer to:
www.mssm.edu/health_safety
http://www.mssm.edu/health_safety/pdf/chemical_storage_practices.pdf
http://www.mssm.edu/health_safety/pdf/HazardousChemicalsStorage.pdf
http://www.mssm.edu/health_safety/pdf/HazWasteManagement.pdf

And now……Let’s play…..
http://www.epa.gov/region02/capp/cip/cases.htmhttp://www.epa.gov/region02/capp/cip/agreeex.htm

“TOXIC” Jeopardy!!


What is….”Improper Chemical Storage!!”


What is: “food storage in a refrigerator with toxic chemicals”


What is: “Improperly labeled container”-for $10,000 (fine-EPA!!)

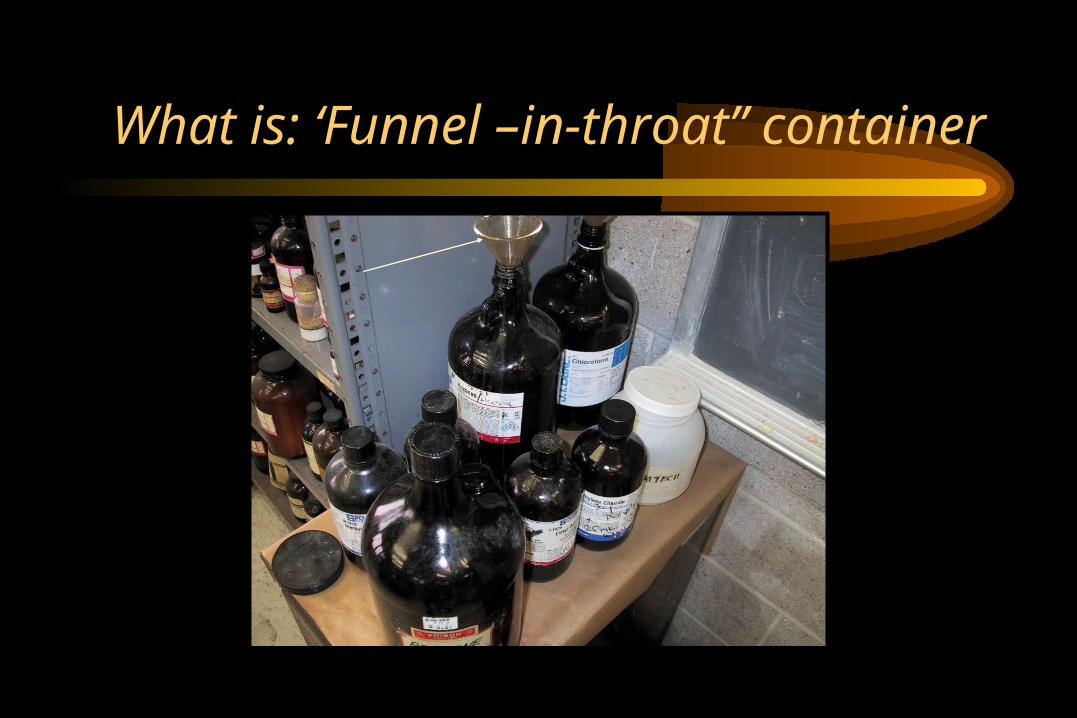
What is: ‘Funnel –in-throat” container


What is: “old chemicals, some open, bad housekeeping”


What is: “improperly labeled waste container on a
sink”…$10,000


What is: “‘Funnel –in-throat” container”


What is: “‘Funnel –in-throat” container”


What is: “Funnel –in-throat” containerand improperly labeled” (Waste Organics??)


What is: “ improperly labeled container”


What is: “ unlabeled inherently waste-like (Hg!!) and improperly labeled containers”


What is: “ an unknown, waste-like container”


What is: “ inherently waste-like container”


What is: “ improperly labeled containers-two labels / label over original ”


What is: “Improper disposal of a hazardous waste”—guaranteed $10,000 EPA fine!!


What is: “Poutpourri” You name it!! All of the above???


What is: “The right way”

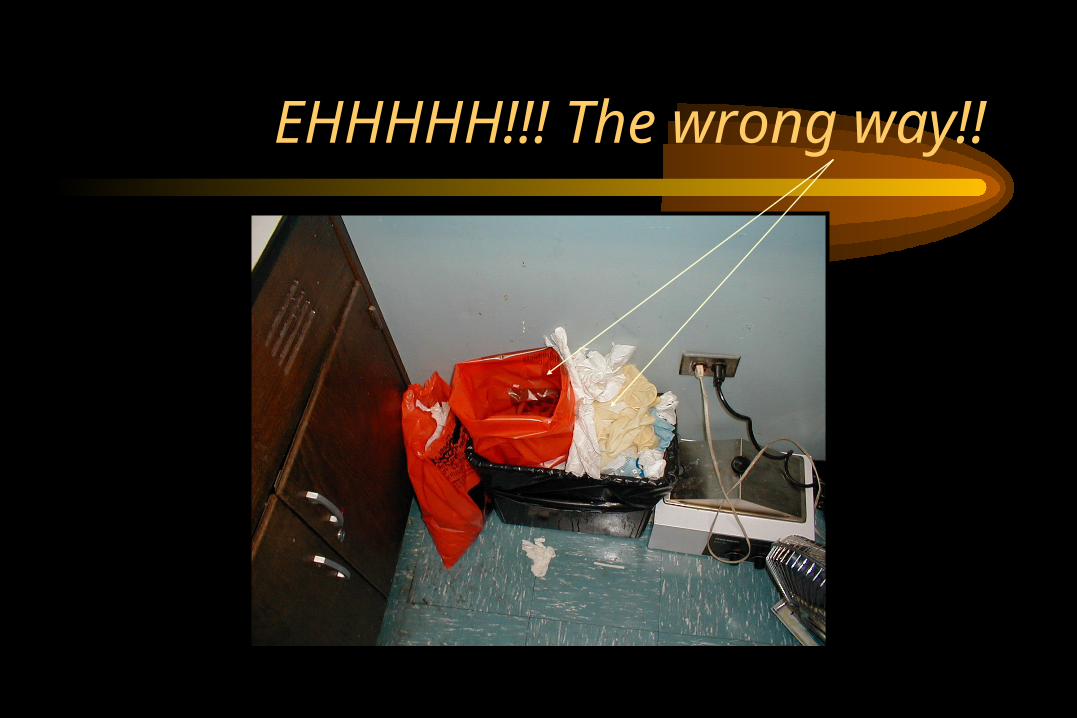
EHHHHH!!! The wrong way!!

Previous slides “stolen” from:
“Health and Safety Lessons Learned from College Environmental Assessments”
•Edward Wilson, MS, CIH, CSP
•Stuart Spiegel, MS

Summation• Even though it was done in a humorous
manner, none of the above slides are funny from a health and safety point of view
• There are some serious and potentially hazardous conditions demonstrated above
• One chemical among some shown above, if mishandled can result in…well…look at the following……..

Peroxide Crystals formed from Isopropyl Ether

Another bottle from the same college’s laboratory that has peroxidized, with a light-impact detonation cap.
(RHR-Inc)
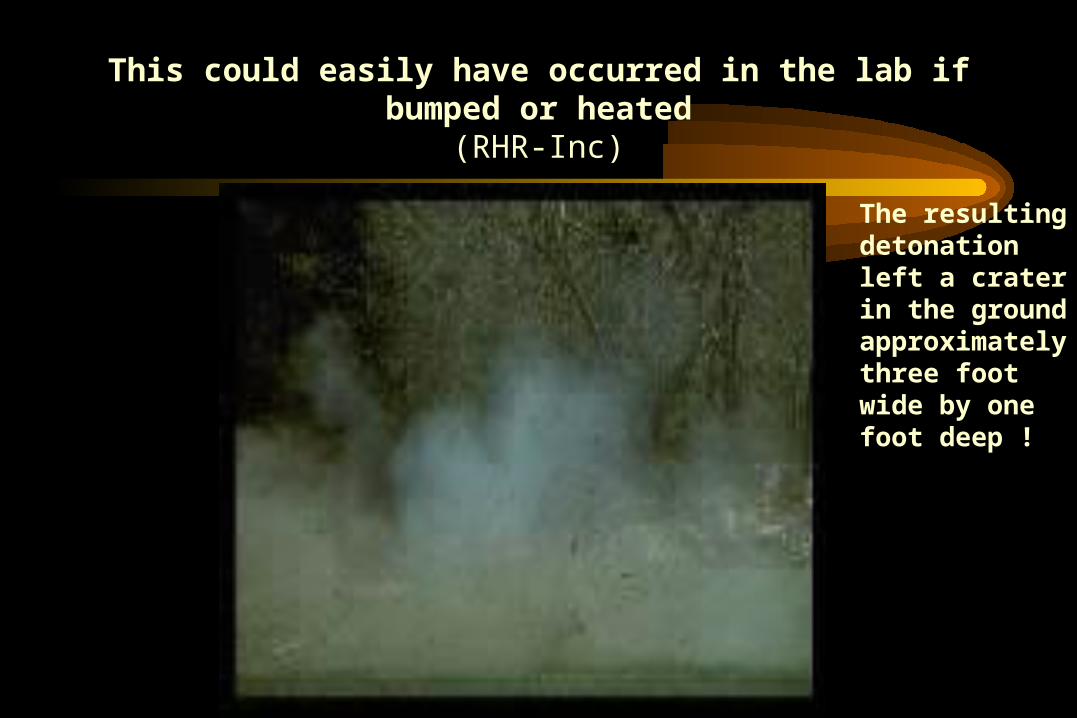
This could easily have occurred in the lab if bumped or heated
(RHR-Inc)
The resulting detonation left a crater in the ground approximately three foot wide by one foot deep !
A laboratory chemical that has been stored / handled improperly can be hazardous to your health!

Three 5 gal. containers of peroxidized Tetrahydrofuran at
@ 120 o F!!Courtesy RHR-Inc

Do any of these look like chemicals in your lab areas? Courtesy RHR-Inc.

Good Chemical Handling / Storage
• Check your inventories……• Get rid of what you do not need• Manage those containers with bad labels• Manage waste collection containers with correct
labeling of contents, and keep caps closed when not adding to them
• Make sure all chemicals have proper labels and are within expiration dates / known shelf lives

CONCLUSIONResources:www.osha.gov
http://www.osha.gov/SLTC/hazardoustoxicsubstances/index.htmlhttp://www.osha.gov/SLTC/laboratories/index.html
www.epa.govhttp://www.ert.org/http://www.epa.gov/sbo/labguide.htmhttp://www.epa.gov/region02/p2/college/ca-sites.htm
www.mssm.edu/health_safety

Questions???
Chemical Disposal:
Kevin McQuillan; 4-SAFE
Chemical Information:
www.mssm.edu/health_safety
Assistance / additional training:
Philip Hauck; 241 5169

Thank you for attending…see you next year!!