chapter i: previous measurements of tissue pressure
Post on 29-Sep-2016
212 views
TRANSCRIPT
CHAPTER I
PREVIOUS MEASUREMENTS OF TISSUE PRESSURE
In principle, a distinction must be made between the direct methods and the more indirect attempts a t elucidating the pressure in the tissues.
The filtration rate of fluid from the capillaries into the tissues a t a given venous pressure affords some information about the tissue pressure, Thus, ceferis paribus, a higher filtra- tion rate implies less resistanceon the part of the tissue. Plethys- mographic investigations may be used to obtain supplementary information about the tissue pressure, and the results express a certain function of the pressure. These two methods are best suited for measurements on the limbs.
In all essentials, the principle of the direct methods has been the same in the numerous investigations into this subject con- ducted by American workers during the past two decades. This applies to the studies of Landis d Gibbon (1933), Kerr d Scott (1936), Gunther d Heitstell (1942), and Moses ( 1947).
The procedures used by the various authors will be briefly outlined below.
The simplest method is that of Bzirrh d Sodemanit (1937). A needle full of fluid is inserted into the tissue. The pressure required to make the fluid flow into the tissue is taken to be the tissue pressure. The amount of fluid necessary to perform
11
the test is about 0.1 cu. mm. during the five minutes required for the measurement.
This method has been elaborated by Wells , Youmarziz d Miller (1938), who observed the flow of the fluid into the tissue with a microscope through a small glass tube connec- ted with the needle. Another modification of this method is due to Moiztgomery, Mickle, S w a n n d Coleman (1910). By this method, the system behind the needle is charged with several different pressures, and interpolation is made between the pressure giving a flow into the tissue and retrograde move- ment of the column of fluid in the needle. The changes in volume occurring within 5 minutes amount to about 1 cu. mm of fluid. This method also is inapplicable for measuring rapid changes in tissue pressure.
Bush, C o f f m a n , Mon tgomery d S w a n n (1949) introdu- ced the term force-fluid-pressure, meaning the pressure re- quired to make 1 cu. mm of fluid flow into the tissue in the course of 1 seconds.
The different methods give quite similar results. For in- stance, the subcutaneous pressure has been found to be about 20-30 mm of water. The measurements of intramuscular pressure show values of about 60-70 mm of water. The in- trarenal pressure is considerably higher, viz. about 25 mm of mercury or about 340 mm of water. The force-fluid-pressure method shows even higher intrarenal pressure. In this con- nection, the tense renal capsule is no doubt a decisive factor. The advantage of the force-fluid-pressure method is that to a certain extent it permits calculation of fluctuations in tissue pressure, if they are not too rapid. So, even if it does give higher results than the other methods in intrarenal measure- ments, the values are comparable.
From 1950, S w a m , Montgomery , Davis jr. d Mickle have
12
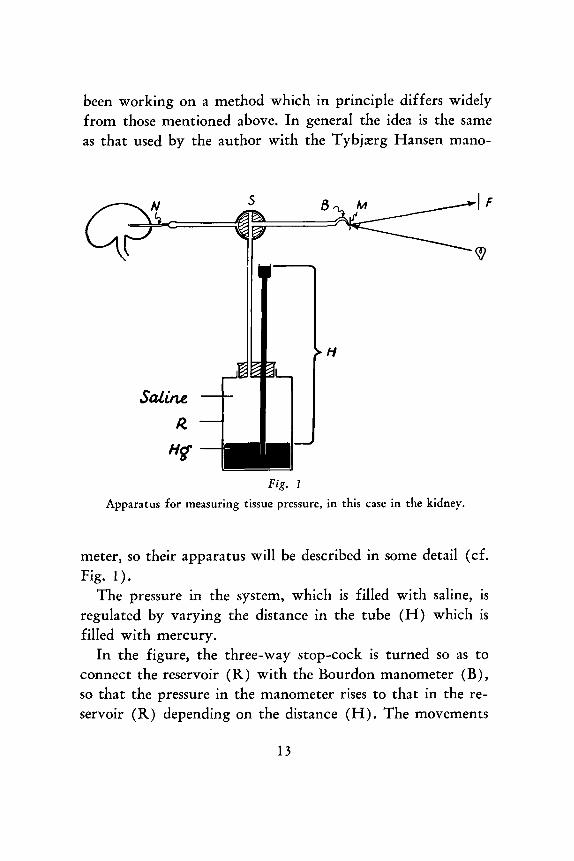
been working on a method which in principle differs widely from those mentioned above. In general the idea is the same as that used by the author with the Tybjzrg Hansen mano-
Fig. 1
Apparatus for measuring tissue pressure, in this case in the kidney.
meter, so their apparatus will be described in some detail (cf. Fig. 1 ) .
The pressure in the system, which is filled with saline, is regulated by varying the distance in the tube (H) which is filled with mercury.
In the figure, the three-way stop-cock is turned so as to connect the reservoir (R) with the Bourdon manometer (B), so that the pressure in the manometer rises to that in the re- servoir (R) depending on the distance (H). The movements
1 3
in the manometer and consequently the pressure in the latter are recorded by throwing light from a light source on the mirror (M) fastened on the Bourdon tube whence it is re- flected on a moving film (F).
Then, the stop-cock ( S ) is turned so as to connect the manometer with the syringe needle (N) placed in the kidney. Thereby, about 1 cu. mm of saline is infused through the system into the kidney. Before the fluid is infused into the kidney, the pressure in the system is usually 250 mm of mer- cury. After the manometer has been connected with the needle, there will be a rather abrupt fall, and not until about 1 minute later is equilibrium established between the pressure in the manometer and that resting on the tip of the needle. This equilibrium is taken to represent the intrarenal pressure.
Experiments have been conducted with needles of varying bore. The amount of fluid and the pressure at which it is in- fused have been varied as well. These factors do not alter the final pressure which is about 26 mm of mercury.
The novelty of this method is that the measurement is not performed until equilibrium has been obtained between the pressure in the manometer and the pressure from the tissue on the tip of the needle. It is this same idea that was used by the author in tissue pressure measurements with the Tybjzrg Han- sen condenser manometer. This is the decisive difference from previous methods which more or less record a sort of force- fluid-pressure.
If the equilbrium is awaited, the quantity of fluid infused plays only a minor r81e - within certain limits. The results of measurements in the subcutaneous tissue and muscles are close to those found by previous workers. The intrarenal pres- sure, on the other hand, is lower by this method than by the original force-fluid pressure method. The main drawback of
14
the force-fluid-pressure and other methods mentioned is that they do not give any possibility of recording rapid fluctua- tions in pressure. In addition, they are time-consuming.
The results obtained by the tissue pressure measurements described above are of the same order of magnitude, although the various methods are not particularly accurate. Thus, the results, e. g . of measurements of the intrarenal pressure may vary by up to 10 mm of mercury, when done in quick suc- cession on the same person. By the Burch 6 Sodemaizrz method the values may vary by nearly 100 %.
On the whole, their method is the most inaccurate of those mentioned. Naturally, there must be a marked diffe- rence in the resistance met by the small drop of fluid in the tissue when the needle is lying loose in the subcutaneous tissue and when the drop is pressed through the needle against fir- mer connective-tissue structures.
The method advocated by Swann, Montgomery, Davis d MicRZe appears to be the most accurate one, although it also has its drawbacks, primarily of not being able to record rapid fluctuations.