chapter four cad - med-ed-online.org · cad-mdm chapter four cad 1- a 70 year-old man develops...
TRANSCRIPT

CAD-mdm
Chapter Four CAD
1- A 70 year-old man develops chest pain since three days ago and the peak lasted for 3 hours. In his ECG, Q wave can be seen in leads V1-V4. What lab test is good for a diagnosis? A- SGOT B-CPK-MB C-LDH D-ESR 2- A 35 year-old man comes to ED with the chief complaint of fever and chest pain referring to his left arm. BP=130/80 mmHg T=38.5 c PR=110 bpm No murmur can be heard. His ECG shows ST elevation in all leads. His CXR shows no sign of cardiomegaly. His echocardiography shows slight effusion. What course of action is appropriate for this case? A- Heparin B-Aspirin C-Lidocaine D-SK 3-A 50 year- old man comes with the chief complaint of chest pain. His BP is130/80 mmHg. ECG reveals acute anterior ischemia. How many TGN can be prescribed for him? A-two with a 5 minute interval B-three with a five minute interval C-three with a 10 minute interval D-two with a 10 minute interval 4-A 68 year-old man is hospitalized in CCU with an inf MI diagnosis. His heart rhythm is NSR. What drug has an adverse effect on the prognosis of this case? A- IV TNG B-IV betablocker C-Aspirin D-Lidocaine 5-Which one is not considered as acute coronary syndrome? A-Non-Q wave MI B- Stable Angina Pectoris C- Q wave MI D-Unstable Angina

CAD-mdm
6-A 72 year-old man comes with the chief complaint of chest pain. His ECG recording is as follows. Which artery is affected? A- Right Circumflex Artery B-Left Circumflex Artery C-LAD D-Diagonal
7- A 69 year-old man complains of chest pain. The pain is accentuated in supine position. BP=120/70 PR=110 bpm T= 39.5c
Heart sounds=muffled Gallops can be heard. No rales
His ECG is shown. What course of action do you suggest? A- Heparin B-SK C-Aspirin D-Prednisolone

CAD-mdm
8-A 50 year-old diabetic man has a sudden dyspnea and weakness. He is referred to you 6 hours later. PR=50 bpm BP=75/50 mmHg JVP=raised No rales or murmur ECG reading= sinus bradicardia and ST elevation. What is the best management? A-Pace-maker B-IV NS C- IV Dopamine 5 mcg/kg/min D-IV TNG 9- Who is not a good candidate for sublingual TNG? A- An 80 year old female with BP=100/80 mmHg and ST depression in inf leads B- A 50 year old male with BP=95/70 mmHg and raised JVP with inf MI C- A 40 year old female with BP=105/70 mmHg with ST elevation in inf leads that disappears D- A 65 year old with a BP=120/80 with antrolateral ischemic traits in ECG 10-A 45 year-old man has the chief complaint of chest pain which lasts for 20 minutes. His ECG reading shows ST depression in anterolateral leads. CPK and Troponin are normal. Which is not advised for this case? A-ASA 300 mg PO B- SK C-IV Heparin D-Nitrates 11-Which does not imply a poor prognosis for angina pectoris? A- S3 B-S4 C-MR murmurs D-lower lung rales 12-Which is not among the absolute contraindications for thrombolytic agents in acute MI? A- SBP> 180 mmHg with chest pain B- Cerebral Hemorrhage 3 years ago C- Diabetic retinopathy D-Aortic dissection 13- Tall R in lead V1 points to the diagnosis of: A- Posterior MI B- Inf MI C- Anterior Mi D- Right Ventricular MI

CAD-mdm
14-Which is not used as a secondary prevention in MI? A- Beta blockers B- CCB C- ACE inhibitors D- Anti platelet drugs 15-A 45 year old man has the chief complaint of epigastric pain which radiates to the lower jaw. The pain is accompanied by sweating and nausea. He doesn’t respond to sublingual TNG. Anti acid relieves the pain after 10 minutes. His ECG is presented here. What is the best approach? A- CCU admit B- Endoscopy C- TNG and Aspirin and discharge D- ED admit
16- A 45 year old man has chest pain. His ECG reading shows ST elevation in inferior leads. His BP is70/50 mmHg and a raised JVP is detected. Lung auscultation is normal. A systolic murmur can be heard. Which drug is the best choice? A- IV TNG B- Beta blocker C- Dobutamine D- NS 17- A 55 year old man has undergone a cholecystectomy. Twenty-four hours later, he develops retrosternal pain which lasts one hour. ECG reading shows LBBB. Which cardiac marker can be more diagnostic? A- CK B- CKMB C- Myoglobin D- Troponin

CAD-mdm
18-What is the diagnosis for the following ECG? A- Inferior MI B- Anteroseptal MI C- Lateral MI D- Anterolateral MI
19- A 20 year old woman has the chief complaint of palpitations. Each episode lasts for some hours with a chest pain. What is the most probable diagnosis? A- WPW syndrome B- HCMP C- Prolonged QT syndrome D- Psychogenic 20- A 52 year old man is hospitalized in CCU with an inf MI diagnosis. His ECG reading is as follows. His BP is100/70 mmHg and he has no chest pain. What course of action is recommended? A- Lidocaine IV drip B- Procainemide Po C- Propanolol Po D- No action is necessary
21- What is not among the reasons to administer TNG in acute MI? A- To lower the oxygen demand B- To help right ventricular function in right ventricular MI C- To increase oxygen supply D- Three to four TNG pearls SL can be given before morphine administration

CAD-mdm
Patients status is emergent
There is ST-segment elevation or new or presumably new LBBB.
1- Non coated aspirin 2-Betablocker 3-IV Heparin 4-Nitroglycerin 5- Oral ACE-inhibitors 6-Analgesics 7-If percutaneous revascularization can not be accomplished within 90 minutes, assess for thrombolysis 8-Transfer to CCU
Unstable angina/non ST-segment elevation MI
1- Aspirin if not already done, clopidogrel if unable to take aspirin. 2-IV Heparin 3- Betablocker 4-IV Nitroglycerine for persistent or recurrent symptoms 5-IV Morphine as needed 6- Admit to monitored bed 7-Assess serial ECG, cardiac specific markers and lipid profile 8-ACE-inh for patients with diabetes or LV dysfunction. 9- Treat exacerbating non-cardiac causes of unstable angina 10- Assess LV dysfunction. If it is less than 0.40 treat for CHF/LV
Stable Angina 1- Ensure patient is taking antiplatelet therapy (ASA 81-325 mg/qd) 2- Assess LV function 3-Consider Stress Tests
Table4-1: IHD management

CAD-mdm
Indication for further diagnostic tests beside EKG:
1-Resting ST-segment depression >1 mm (in the absence of digoxin, or valvular,
hypertensive, or myopathic heart disease or female gender) is a marker for a higher
prevalence of severe CAD and is associated with a poor prognosis.
2-In the presence of baseline ECG abnormalities, the diagnostic accuracy of standard
exercise testing is reduced. These patients should be considered for cardiology
consultation, myocardial nuclear perfusion scan, or exercise stress echocardiography.
Patients with marked resting ST-segment depression should be considered high risk, until
proven otherwise.
3-Patients with >1 mm ST dynamic segment depression on holter monitor, for more than
120 seconds, should be referred for an appropriate ischemic work-up.
4-There is little evidence to support screening asymptomatic individuals for IHD.
Although LBBB is frequently associated with CAD, there are no retrospective or
prospective trials that support evaluating patients with LBBB who are asymptomatic and
who have a normal echocardiogram.
5- Likewise, asymptomatic individuals with Q-waves on ECG, but a normal
echocardiogram, do not require further evaluation.
Indications for echocardiography :
1- Holosystolic or late systolic murmur
2- Grade 3 or midsystolic murmurs
3- Murmurs associated with an abnormal ECG or chest x-ray
4- Physical signs of LV dysfunction or CHF
5- Enlarged cardiac silhouette and/or signs of pulmonary venous congestion on

CAD-mdm
chest x-ray
6- New Q-waves in 2 or more contiguous leads or new LBBB
Indication for stress test: Asymptomatic ST depression during exercise is relatively
common and should raise the suspicion for occult CAD. However, the accuracy of exercise
testing in asymptomatic patients has never been defined. Therefore, an abnormal exercise
test result in an asymptomatic patient is most appropriately viewed within the context of
the pre-test probability of CAD based on age, gender, and the presence of coronary risk
factors.
Usual ECG evolution of a Q-wave MI Not all of the following patterns may be seen; the time from onset of MI to the final pattern is quite variable and related to the size of MI, the rapidity of reperfusion (if any), and the location of the MI.
A. Normal ECG prior to MI
B. Hyperacute T wave changes - increased T wave amplitude and width; may also see ST elevation
C. Marked ST elevation with hyperacute T wave changes (transmural injury)
D. Pathologic Q waves, less ST elevation, terminal T wave inversion (necrosis) (Pathologic Q waves are usually defined as duration >0.04 s or >25% of R-wave
amplitude)
E. Pathologic Q waves, T wave inversion (necrosis and fibrosis)
F. Pathologic Q waves, upright T waves (fibrosis)
Diagram4-1: ECG change after MI

CAD-mdm
Diagram4-2: Enzyme change after MI
Inferior MI Family of Q-wave MI's (Includes inferior, true posterior, and right ventricular MI's due to Right Circumflex Artery occlusion)
Inferior MI Pathologic Q waves and evolving ST-T changes in leads II, III, aVF
Q waves usually largest in lead III, next largest in lead aVF, and smallest in lead II
Example #1: frontal plane leads with fully evolved inferior MI (note Q-waves, residual
ST elevation, and T inversion in II, III, aVF)

CAD-mdm
Example #2: Old inferior MI (note largest Q in lead III, next largest in aVF, and smallest in lead II)
True posterior MI ECG changes are seen in anterior precordial leads V1-3, but are the mirror image of an
anteroseptal MI: Increased R wave amplitude and duration (i.e., a "pathologic R wave" is a mirror image
of a pathologic Q)
R/S ratio in V1 or V2 >1 (i.e., prominent anterior forces)
Hyperacute ST-T wave changes: i.e., ST depression and large, inverted T waves in V1-3
Late normalization of ST-T with symmetrical upright T waves in V1-3

CAD-mdm
Often seen with inferior MI (i.e., "inferoposterior MI")
Example #3: Acute inferoposterior MI (note tall R waves V1-3, marked ST depression
V1-3, ST elevation in II, III, aVF)
Example #4: Old posterolateral MI (precordial leads): note tall R waves and upright T's in V1-3, and loss of R in V6
Right Ventricular MI (only seen with proximal right coronary occlusion; i.e., with inferior family MI's)
ECG findings usually require additional leads on right chest (V1R to V6R, analogous to the left chest leads)
ST elevation, >1mm, in right chest leads, especially V4R (see below)

CAD-mdm
Anterior Family of Q-wave MI's (LAD is the occluded artery)
Anteroseptal MI Q, QS, or qrS complexes in leads V1-V3 (V4) Evolving ST-T changes Example #5: Fully evolved anteroseptal MI (note QS waves in V1-2, qrS complex in
V3, plus ST-T wave changes)

CAD-mdm
Anterior MI (similar changes, but usually V1 is spared; if V4-6 involved call it "anterolateral")
Example #6: Acute anterior or anterolateral MI (note Q's V2-6 plus hyperacute ST-T changes)
High Lateral MI (typical MI features seen in leads I and/or aVL) Example: note Q-wave, slight ST elevation, and T inversion in lead aVL
(Note also the slight U-wave inversion in leads II, III, aVF, V4-6, a strong marker for coronary disease)
CAD-mdm
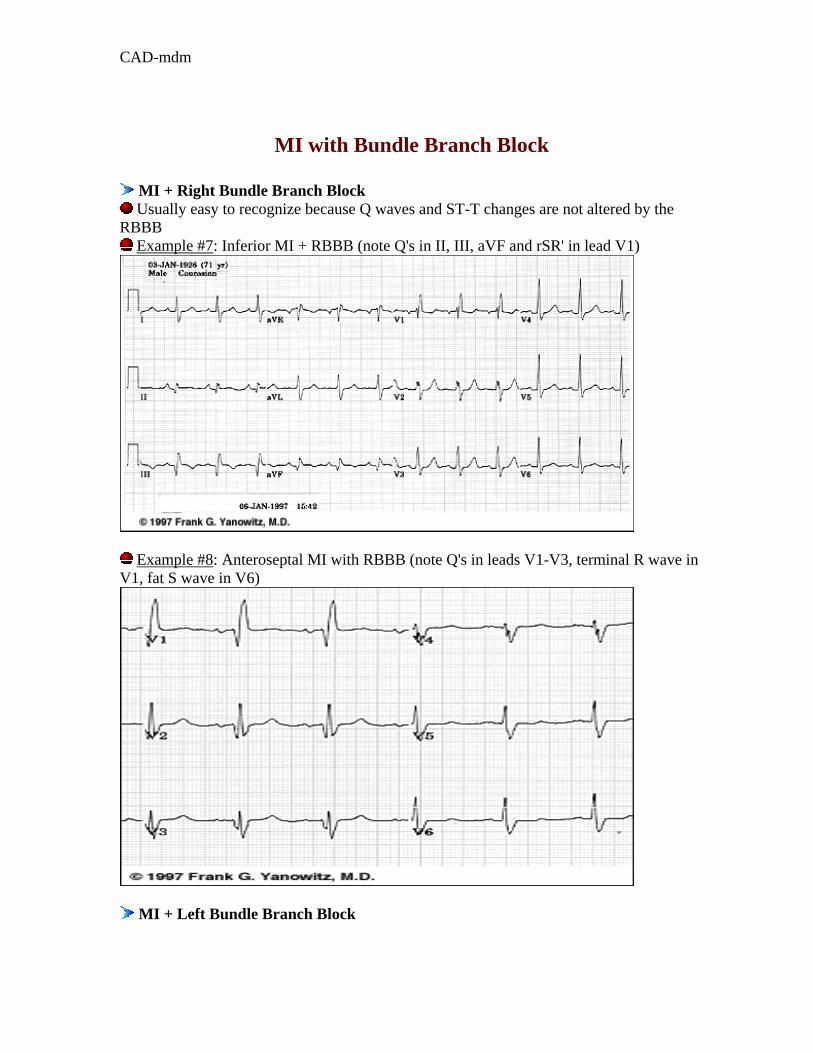
MI with Bundle Branch Block
MI + Right Bundle Branch Block Usually easy to recognize because Q waves and ST-T changes are not altered by the
RBBB Example #7: Inferior MI + RBBB (note Q's in II, III, aVF and rSR' in lead V1)
Example #8: Anteroseptal MI with RBBB (note Q's in leads V1-V3, terminal R wave in V1, fat S wave in V6)
MI + Left Bundle Branch Block

CAD-mdm
Often a difficult ECG diagnosis because in LBBB the right ventricle is activated first and left ventricular infarct Q waves may not appear at the beginning of the QRS complex (unless the septum is involved).
The Pseudoinfarcts These are ECG conditions that mimic myocardial infarction either by simulating
pathologic Q or QS waves or mimicking the typical ST-T changes of acute MI. WPW preexcitation (negative delta wave may mimic pathologic Q waves)
IHSS (septal hypertrophy may make normal septal Q waves "fatter" thereby mimicking
pathologic Q waves)
LVH (may have QS pattern or poor R wave progression in leads V1-3)
RVH (tall R waves in V1 or V2 may mimic true posterior MI)
Complete or incomplete LBBB (QS waves or poor R wave progression in leads V1-3)
Pneumothorax (loss of right precordial R waves)
Pulmonary emphysema and cor pulmonale (loss of R waves V1-3 and/or inferior Q waves with right axis deviation)
Left anterior fascicular block (may see small q-waves in anterior chest leads)
Acute pericarditis (the ST segment elevation may mimic acute transmural injury)
Central nervous system disease (may mimic non-Q wave MI by causing diffuse ST-T wave changes)
CAD-mdm
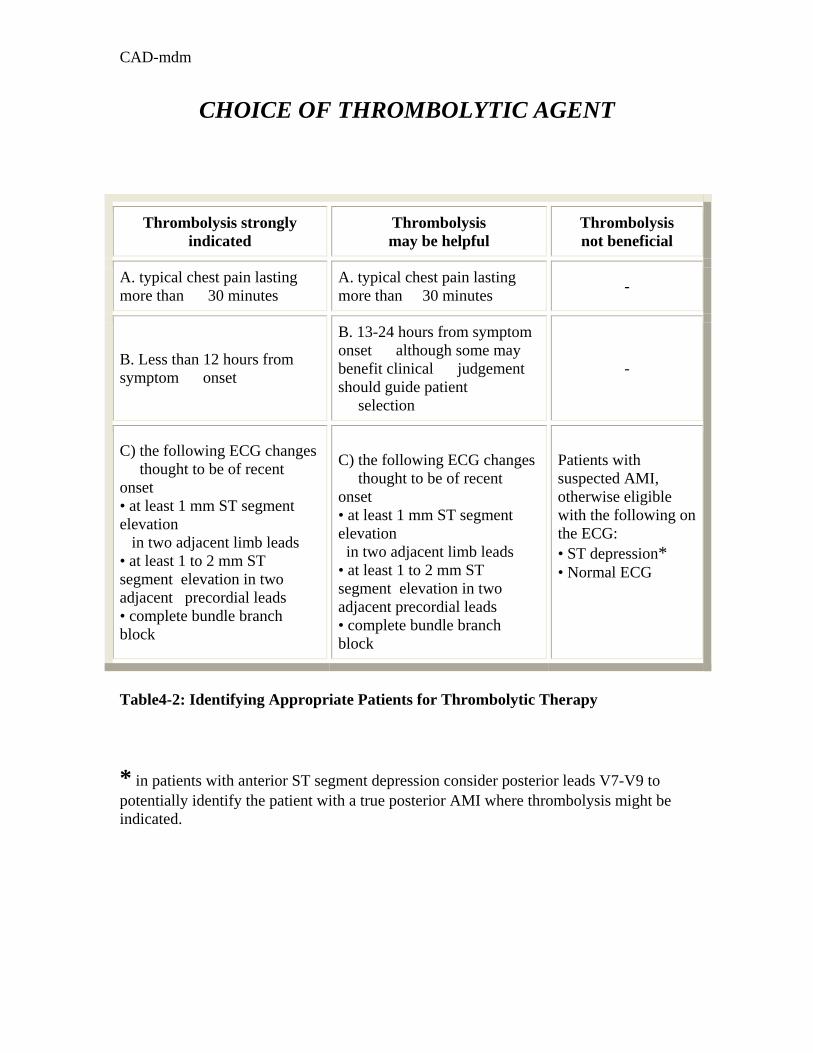
CHOICE OF THROMBOLYTIC AGENT
Thrombolysis strongly indicated
Thrombolysis may be helpful
Thrombolysis not beneficial
A. typical chest pain lasting more than 30 minutes
A. typical chest pain lasting more than 30 minutes -
B. Less than 12 hours from symptom onset
B. 13-24 hours from symptom onset although some may benefit clinical judgement should guide patient selection
-
C) the following ECG changes thought to be of recent onset • at least 1 mm ST segment elevation in two adjacent limb leads • at least 1 to 2 mm ST segment elevation in two adjacent precordial leads • complete bundle branch block
C) the following ECG changes thought to be of recent onset • at least 1 mm ST segment elevation in two adjacent limb leads • at least 1 to 2 mm ST segment elevation in two adjacent precordial leads • complete bundle branch block
Patients with suspected AMI, otherwise eligible with the following on the ECG: • ST depression* • Normal ECG
Table4-2: Identifying Appropriate Patients for Thrombolytic Therapy
* in patients with anterior ST segment depression consider posterior leads V7-V9 to potentially identify the patient with a true posterior AMI where thrombolysis might be indicated.

CAD-mdm
Absolute contraindication Relative
• aortic dissection • acute pericarditis • active bleeding • cerebral haemorrhage , known intracerebral vascular disease (malignancy , AV malformation) at any time*
• GI or GU bleed < 6 months • stroke < 6 months • history of bleeding diathesis, hepatic dysfunction or cancer • diabetic proliferative retinopathy • surgery or major organ biopsy < 2-4 weeks • puncture of a non-compressible vessel < 2-4 weeks • major trauma < 4 weeks • prolonged CPR with chest compressions in a patient who now has evidence of chest trauma or who remains unconcious • persistent severe uncontrolled hypertension with DBP>120 mm Hg and/or SBP>200 mm Hg • endocarditis • pregnancy
Table4-3: Contraindications for thrombolytic drugs.
* although cerebral hemorrhage is usually considered a ‘relative’ contraindication, the possibility of harm were a thrombolytic agent administered in this situation is sufficiently high that we have classified it as an absolute contraindication. We recommend that rt-PA is the agent of choice for all eligible AMI unless:
SK Preferred
• age >/= 85 years, or • time from symptom onset > 6 hours, or • systolic BP < 100 mm Hg, or cardiogenic shock*
and the patient has not previously received SK or APSAC at any time. * in the setting of cardiogenic shock strong consideration should be given to urgent angiography with a view to possible intra-aortic balloon pump insertion and/or PTCA, following discussion with the Cardiologist-on-call. Failing that, SK is the preferred agent.

CAD-mdm
DRUG ADMINISTRATION Prior to Initiation of Thromobolysis 1- Draw all necessary bloodwork and send to the laboratory. Do not wait for the results of the coagulation screen unless there is a suspicion of a haemostatic defect. A chest X-ray is not mandatory prior to initiation of thrombolysis. 2- Establish at least 2 IV access sites. Use both arms if necessary. An 18 g needle is preferred. If venous access for blood testing is a problem insert an arterial cannula prior to the onset of therapy. More IV access sites may be required depending upon the number of infusions and drug compatibility. 3- For ease of blood sampling one IV site may have IVAC tubing and arterial extension site. DO NOT use a hand vein - use a larger median vein in the forearm. 4- Record vital signs every 10 minutes. BP may be measured with a standard inflatable BP cuff, an automatic BP cuff or if necessary an intra-arterial cannula. 5- Have the following available for use if necessary: a) emergency cardiac medications: atropine, adrenaline, vasopressors and lidocaine. b) normal saline or ringers lactate for volume expansion to treat hypotension. c) defibrillator. d) sterile gauze for a pressure dressing. e) external transthoracic pacemaker. 6- Start thrombolysis in the ED unless patient can be in CCU and receiving the drug within the same time it would take to commence the infusion in the ED. Do not wait for the CCU bed to become available. 7- Central venous cannulation should be avoided, if possible, but if access to the central circulation is required, consideration should be given to either a brachial cut-down or a percutaneous approach to a readily compressible vessel. Tissue plasminogen activator: accelerated dosage regimen over 90 minutes • reconstitute by aseptically adding to the vial of Activase (100 mg) 100 ml of sterile water for injection without preservatives. • using an 18 G needle direct the stream of the sterile water into the lyophilized cake. Avoid excess shaking. • observe for particulate matter and discolouration (should be colourless to pale yellow and transparent). If observed, do not use.

CAD-mdm
• insert the spike end of an infusion set through the puncture site created by the transfer device in the stopper of the vial of reconstituted Activase. Hang the vial of Activase from the plastic moulded capping attached to the bottom of the vial. • do not add other medication to the solution. • administer via infusion pump. - 15 mg. bolus (alternatively, may be administered as a bolus injection) - then, 0.75 mg/kg (not to exceed 50 mg) over 30 min. - then, 0.50 mg/kg (not to exceed 35 mg) over 60 min. The total dose should not exceed 100 mg. The total administration time is 90 min.
Streptokinase: 1,500,000 units over 1 hour ( vial 750000 IU, 250000 Rials) • add 5 ml NaCL Injection or 5% Dextrose Injection slowly to the vacuum packed container. • direct the NaCL or Dextrose Injection at the side of the container, not the powder. • roll and tilt the vial gently, do not shake. • observe for particulate matter and discolouration. If observed, do not use. (Note: the human albumin may impart a slight yellow colour to the solution). • withdraw 5 ml from 100 ml minibag of 0.9% NaCL or D5W. Add reconstituted contents of vial and add to minibag. Avoid agitation. • do not add other medications to the SK infusion. • infuse via infusion pump over 60 minutes. The total dose is 1.5 million units. The total administration time is 60 min. Heparin(amp 10000 u/ml , 4400 Rials) In the absence of thrombolytic therapy, the risk/benefit ratio of routine heparin use in AMI remains unclear. Intravenous heparin is recommended for at least 48 hours in patients who receive rt-PA. Certain sub-groups are likely to benefit more than others from a more prolonged infusion

CAD-mdm
(see below). Heparin should be considered for patients who receive SK, but the indications are related more to the presence of determinants of high risk for systemic or venous thromboembolism (anterior AMI, congestive heart failure, previous embolus, atrial fibrillation) than simply to the administration of SK. Following SK the optimal dose and route of administration of heparin are uncertain. It is strongly recommended that all anterior AMI receive options b or c, irrespective of whether they received SK or rt-PA. Unless specifically contraindicated, one of the following approaches should be considered: a) Subcutaneous low dose: 5,000 units s.c. q.12.h. until ambulatory or at the discretion of the attending physician. b) Subcutaneous calcium heparin - fixed high dose: 12,500 units s.c. - 17,500 units s.c. q.12.h starting 4 hours from the onset of the SK infusion, continue for 7 days or at the discretion of the attending physician. c) Intravenous heparin. i) Tissue plasminogen activator: Administer an intravenous bolus of either 75 units/kg or 5000 units of heparin at the time of initiating the rt-PA infusion, with an initial maintenance infusion of 1000 units/hour. For the first 12 hours the goal is to achieve a therapeutic aPTT > 60 seconds, then within the desired range (60-85 sec) thereafter. Consequently, only the first two lines of the nomogram should be used for the 6 and 12 hour aPTTs and heparin should be adjusted upward if the aPTT< 60 seconds. High aPTTs likely reflect the effect of the thrombolytic agents. For later aPTTs the entire nomogram should be used. ii) Streptokinase: Measure INR/aPTT at 4 hours from the start of the SK infusion and start heparin infusion at 1,000 units/hr if the aPTT is within or below the therapeutic range. Thereafter, adjust as per nomogram (see table). In general, draw aPTT at 6,12,24, hours. If the 4 hour aPTT is above the therapeutic range, do not start the heparin infusion; repeat the aPTT in 2-6 hours as appropriate. Repeat until aPTT is within the therapeutic range.
CAD-mdm
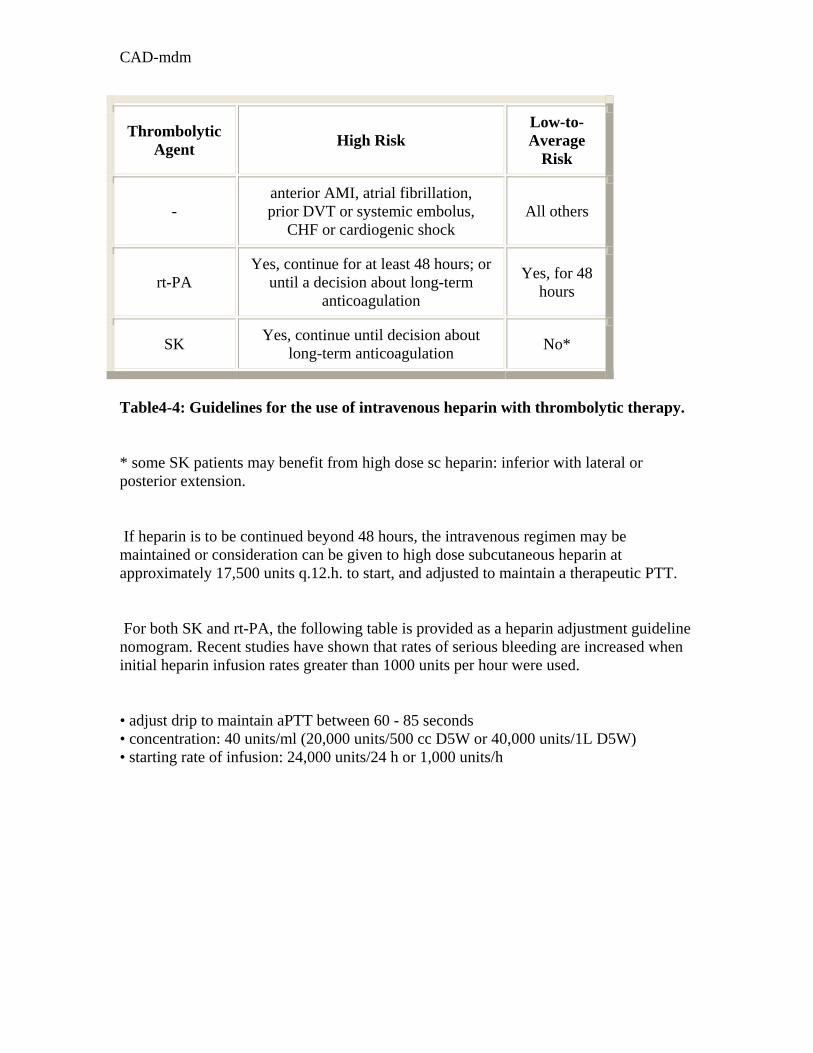
Thrombolytic Agent High Risk
Low-to-Average
Risk
- anterior AMI, atrial fibrillation, prior DVT or systemic embolus,
CHF or cardiogenic shock All others
rt-PA Yes, continue for at least 48 hours; or
until a decision about long-term anticoagulation
Yes, for 48 hours
SK Yes, continue until decision about long-term anticoagulation No*
Table4-4: Guidelines for the use of intravenous heparin with thrombolytic therapy.
* some SK patients may benefit from high dose sc heparin: inferior with lateral or posterior extension.
If heparin is to be continued beyond 48 hours, the intravenous regimen may be maintained or consideration can be given to high dose subcutaneous heparin at approximately 17,500 units q.12.h. to start, and adjusted to maintain a therapeutic PTT.
For both SK and rt-PA, the following table is provided as a heparin adjustment guideline nomogram. Recent studies have shown that rates of serious bleeding are increased when initial heparin infusion rates greater than 1000 units per hour were used.
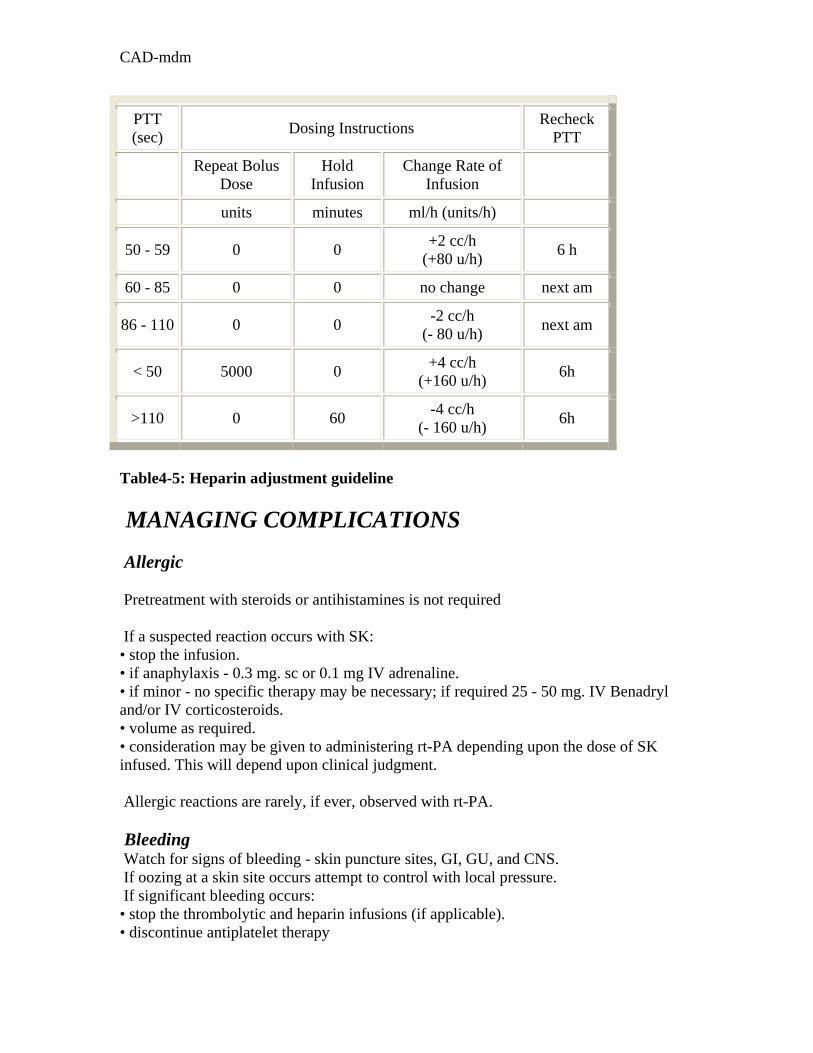
• adjust drip to maintain aPTT between 60 - 85 seconds • concentration: 40 units/ml (20,000 units/500 cc D5W or 40,000 units/1L D5W) • starting rate of infusion: 24,000 units/24 h or 1,000 units/h
CAD-mdm
PTT (sec) Dosing Instructions Recheck
PTT
Repeat Bolus Dose
Hold Infusion
Change Rate of Infusion
units minutes ml/h (units/h)
50 - 59 0 0 +2 cc/h (+80 u/h) 6 h
60 - 85 0 0 no change next am
86 - 110 0 0 -2 cc/h (- 80 u/h) next am
< 50 5000 0 +4 cc/h (+160 u/h) 6h
>110 0 60 -4 cc/h (- 160 u/h) 6h
Table4-5: Heparin adjustment guideline MANAGING COMPLICATIONS Allergic Pretreatment with steroids or antihistamines is not required If a suspected reaction occurs with SK: • stop the infusion. • if anaphylaxis - 0.3 mg. sc or 0.1 mg IV adrenaline. • if minor - no specific therapy may be necessary; if required 25 - 50 mg. IV Benadryl and/or IV corticosteroids. • volume as required. • consideration may be given to administering rt-PA depending upon the dose of SK infused. This will depend upon clinical judgment. Allergic reactions are rarely, if ever, observed with rt-PA. Bleeding Watch for signs of bleeding - skin puncture sites, GI, GU, and CNS. If oozing at a skin site occurs attempt to control with local pressure. If significant bleeding occurs: • stop the thrombolytic and heparin infusions (if applicable). • discontinue antiplatelet therapy

CAD-mdm
• apply pressure to the area, if possible. • STAT: INR/aPTT, Thrombin time, and Fibrinogen level • Group & reserve or crossmatch • volume replacement as required; transfuse if appropriate • If fibrinogen </= 1.0 G/L replace fibrinogen with 10-20 units of cryoprecipitate. Aim for a fibrinogen level > 1.0 G/L. If ongoing bleeding or life-threatening bleeding: • give 4-6 units FFP. • consider Amicar: dilute 5 grams in 250 cc D5W and infuse over 1 hour, then about 0.5-1.0 gram per hour as a continuous infusion depending upon coagulation profile (adjust dose for renal impairment). • consider Trasylol: 500,000 KIU IV over 15 minutes. • consider Tranexamic Acid: 10 mg/kg IV q6h (adjust dose for renal impairment). Bleeding from mouth • take a 500 mg tablet of tranexamic acid (Cyklokapron) and dissolve it in 10 cc of sterile normal saline • have the patient hold it in their mouth and swish it around for as long as possible (30 seconds), and then spit it out. Repeat as necessary. • tranexamic acid is an orally active agent - swallowing of the solution should be avoided. Suspected CNS haemorrhage • stop thrombolytic agent, aspirin and heparin • arrange urgent CT scan • if CNS hemorrhage confirmed, urgent Neurosurgical consultation • frequent neurological vitals; maintain airway and oxygenation • raise head of bed 45 degrees • consider IV mannitol or intubation, mechanical ventilation and hyperventilation Other considerations: • Heparin can be reversed using protamine sulphate. If heparin was administered within the previous 4 hours, give protamine sulphate 25-50 mg over 10 minutes. • The anti-platelet effect of ASA and plasmin can be reversed with ddAVP (Desmopressin) 20 micrograms intravenously over 20 minutes. Hypotension
CAD-mdm
• stop the SK infusion. • it is not necessary to stop an infusion of rt-PA. • lay the patient flat or in Trendelenburg position if tolerated. • volume expand with 0.9% NaCl or Ringers lactate. • use vasopressors if the above steps are not successful. • use Atropine if bradycardic. • search for other causes if not responding to the above. • once the hypotension resolves resume the SK infusion. Arrhythmias "Reperfusion arrhythmias" such as accelerated idioventricular rhythm or "slow VT" (AIVR) are usually benign and do not require therapy. More serious arrhythmias (VT, VF and all cardiac arrests) may occur slightly less frequently with thrombolytic therapy than with conventionally treated AMI. Treat all arrhythmias in the same manner as in conventionally-treated AMI.

CAD-mdm
Some words on hyperlipidemia How do you manage these cases of hyperlipidemia: 22- 45 year old man with no adverse history, TG=300 ,HDL=40, Total Cholesterol=200? 23- 45 year old woman with chronic hepatitis, TG=148,HDL=45,Total Chol=292? 24- 45 year old man with a CAD history, TG=450,HDL=40,Total chol=450? 25-45 year old woman with DM and obesity, TG=280,HDL=36,total chol=220?
Diagram4-3: approach to Hyperlypidemia(* Total Cholesterol=LDL+(HDL+TG/5)
Estimate LDL level according to risk
factors*
Low LDL High LDL
High TG (>150 mg/dl)
(hypertriglyceridemia)
VLDL/TG<3/10 (Dysbetalipoproteinemia)
High TG (Hyperlipidemia)
Normal TG (hypercholesterolemia)
Niacin gemfibrozil
Niacin Gemfibrozil
statins
Niacin Gemfibrozil
statins
Niacin Statin
cholestyramine

CAD-mdm
TABLE4-6 Determining Patient-Specific LDL Goals Through Risk Factors
Risk-factor score* LDL goal, by risk-factor score†
Age: men > 45 years; women >55 years or postmenopausal without ERT Current smoker Hypertension Diabetes CHD in first-degree relative (male relative <55 years; female relative <65 years) HDL <35 mg per dL (0.9 mmol per L); subtract 1 risk factor if HDL >60 mg per dL
0 to 1 point: <160 mg per dL (<4.15 mmol per L).If more than 190 needs drug therapy. 2 or more points: <130 mg per dL (<3.35 mmol per L)If more than 160 needs drug therapy. Patients with history of CHD: <100 mg per dL (<2.60 mmol per L).If more than 130 needs drug therapy
LDL = low-density lipoprotein; ERT = estrogen replacement therapy; CHD = coronary heart disease; HDL = high-density lipoprotein. *--Score 1 point for each positive factor. †--LDL goals established by National Cholesterol Education Program.

CAD-mdm
TABLE4-7:HMG-CoA Reductase Inhibitors (Statins)
Drug
Dosage
Adverse effects
Patient information Monitoring
Lovastatin (Mevacor)* (tab 20 mg, 400 Rials)
Initially, 20 mg with evening meal. If serum cholesterol is >300 mg per dL, start with 40 mg daily. Increase dosage if response is inadequate at 4 weeks. Maximum dosage: 80 mg daily. If CrCl is < 30 mL per minute (<0.5 mL per second), daily dose should not exceed 20 mg.
GI, myalgias, arthralgias, headaches, dizziness, elevated liver enzymes
Report malaise, fever or any muscle tenderness or weakness. Avoid consumption of alcohol and grapefruit juice while taking this medicine.
Obtain lipid profiles for response at 4 weeks. Perform LFTs before initiating therapy, at 6 and 12 weeks and every 6 months thereafter. Repeat LFTs after dosage escalation. Discontinue drug if serum transaminase levels exceed 3 times normal level or if myopathy or myositis occurs.
Simvastatin (Zocor)* (tab 20 mg, 1200 Rials)
Initially, 20 mg daily at bedtime. Increase dosage if response is inadequate at 4 weeks. Maximum dosage: 40 mg twice daily 5 mg daily at bedtime if patient is elderly or has severe renal insufficiency.
GI, headaches, elevated liver enzymes
Report malaise, fever or any muscle tenderness or weakness. Avoid consumption of alcohol and grapefruit juice while taking this medicine.
Obtain lipid profiles for response at 4 weeks. Perform LFTs before initiating therapy and every 6 months for the first year of therapy. Repeat LFTs every 6 months after dosage escalation for an additional year. Patients taking 80 mg daily should have LFTs every 3 months. Discontinue drug if serum transaminase levels exceed 3 times normal level or if myopathy or myositis occurs. Closely monitor patients with severe renal insufficiency. Do not exceed 10 mg daily if given in combination with fibrates or niacin.

CAD-mdm
TABLE 4-8:Niacin (Nicotinic Acid)
Drug
Dosage Adverse effects
Patient information Monitoring
Nonprescription niacin (tab 100 mg, 45 Rials, tab 500 mg 1450 Rials)
50 to 100 mg twice daily for the first week. Double the dosage every week to 1,000 to 1,500 mg daily, in 2 or 3 divided doses. If response is inadequate after 4 to 8 weeks, increase dosage slowly to maximum of 3,000 mg daily. If patient switches brands, restart from low dosage and titrate up to minimize risk of hepatic necrosis.
Flushing, pruritus, abdominal pain, nausea, vomiting, elevated liver enzyme levels, glucose intolerance, rare reversible acanthosis nigricans
To decrease flushing, take in p.m.; take aspirin 30 minutes before, avoid concomitant ingestion of alcohol or hot beverage. To decrease gastrointestinal distress, take daily in 2 or 3 divided doses; take after a low-fat snack.
Check lipid levels before and 4 weeks after reaching desired dosage, and 4 weeks after every dosage increase. Perform LFTs, uric acid determination and fasting glucose test before initiating therapy and 6 weeks after target dose is reached. Repeat LFTs every 12 weeks thereafter for first year, then every 6 to 12 months. Discontinue drug if serum transaminase levels exceed 3 times normal level.

CAD-mdm
TABLE 4-9:Fibric Acid Derivatives (Fibrates)
Drug Dosage
Adverse effects
Patient information Monitoring
Gemfibrozil (Lopid)* (cap 300 mg, 470 Rials)
600 mg twice daily, 30 minutes before morning and evening meals. Maximum dosage: 600 mg twice daily
Dyspepsia, diarrhea, fatigue, nausea, vomiting, abdominal pain, eczema, rash, vertigo
Take with meals. Report any muscle pain, tenderness or weakness.
Perform LFTs before initiating therapy and repeat periodically during first year of therapy.

CAD-mdm
TABLE 4-10:Bile Acid Sequestrants
Drug
Dosage Adverse effects Patient information Monitoring
Cholestyramine (LoCholest) powder (4 gr sachet, 1700 Rials)
Initially, 4 g daily in 2 or 3 divided dosesIncrease dosage at 4-week intervals as tolerated. Maximum dosage: 24 g daily
Constipation Take 1 hour before or 4 hours after other medications. Take with meals. Mix with 3 to 6 oz of water, fruit juice or pulpy fruit (applesauce or crushed pineapple). Mixing a dose the night before and refrigerating it will improve palatability. Stir well. Increase fluid intake to avoid constipation.
Check lipid profile at 2 to 4 weeks and monitor for constipation. If constipation occurs, increase fluid and fiber intake, consider stool softener. Some patients require a laxative to prevent constipation.
Colestipol (Colestid) granules
Initially, 5 g daily in 2 or 3 divided doses (granules) or 2 g daily (tablets) Increase dosage at 4-week intervals as tolerated. Maximum dosage: 30 g daily
Constipation Flavored products contain aspartame. Avoid in phenyketonuric patients.
Same as above Same as above

CAD-mdm
Answers: 1-c 2-b 3-b 4-a 5-b 6-a 7-b
8-b 9-b 10-b 11-b 12-c 13-a 14-b
15-a 16-d 17-d 18-a 19-d 20-d 21-b
22-DX=hypertriglyceridemia/TX=Niacin&Gemfibrozil 23-DX=hypercholesterolemia/TX=cholestyramine 24-DX=dysbetalipoproteinemia/TX=Niacin&Gemfibrozil&Statins 25-DX=hypertriglyceridemia/TX=Niacin&Gemfibrozil References: 1- Braunwald et al . IHD clinical practice guidelines. 2002 2- Braunwald Eugene, et al. Harrison's Principles of Internal Medicine. 16h edition. McGrawHill; 2005 3- Iranian Council for Graduate Medical Education. Exam questions. 4-Katzung Bertram G. Pharmacology: Examination & Board Review.7th edition Mcgrawhill. 2005 5- Laboratory Findings in Heart Disease. Cardiac Enzymes .www.hoslink.com.2006 6-Massel ,David And Klein.,George J. Guidelines & Policies At The London Health Sciences Centre. 2002. www.lhsc.on.ca/uwodoc/pages/policy.htm 7- Drug prices. Ministry of health. Iran.2006 8- Safeer ,Richard S., Lacivita ,Cynthia L. Choosing Drug Therapy for Patients with Hyperlipidemia American Family Physician. Vol. 61/No. 11 (June 1, 2000) 9- Yanowitz, Frank..ECG learning center.2006

CAD-mdm