chapter 6msleejichs.wikispaces.com/file/view/06_lecture_ppt+bone+histo+and...•bones are organs...
TRANSCRIPT
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.
Chapter 6 Histology and
Physiology of
Bones
Osteon

Skeletal System
• 4 components
– Bones
– Cartilage
– Tendons
– Ligaments
• Bones are organs composed of
– Nerve tissue
– Vascular tissue

Functions of Bones
• Support: framework that supports body and cradles soft organs
• Protection: protective case for brain, spinal cord, vital organs
• Movement: provide levers for muscles
• Storage: reservoir for minerals, especially Ca & P
• Blood cell production: hematopoiesis within marrow cavities of bones

Cartilage
• Chondroblasts produce cartilage and become chondrocytes
• Chondrocytes located in lacunae surrounded by matrix
• matrix contains collagen fibers (for strength) and proteoglycans (trap water)
• perichondrium surrounds cartilage – outer layer contains fibroblasts
– inner layer contains chondroblasts

Fig. 6.1
Cartilage grows by appositional and interstitial growth
Bone Histology
• Bone Matrix
~35% organic and 65% inorganic material
• Organic
– Collagen provides flexible strength
– Proteoglycan proteins
• Inorganic
– Hydroxyapatite (mineral-calcium phosphate crystals)
provides weight-bearing strength

Effects of Changing the Bone Matrix!!!
Fig. 6.2

Bone Histology
• Bone Cells – Osteoblasts produce bone matrix, become osteocytes
• Osteoblasts connect to 1 another through cell processes
– surround themselves with bone matrix to become osteocytes
• Osteocytes located in lacunae, connected to 1 another through canaliculi
• Osteoblasts originate from osteochondral progenitor cells
– Osteoclasts break down bone • originate from stem cells in red bone marrow

Bone Histology
• Ossification
(Osteogenesis)
1. Osteoblasts on a
preexisting surface, such
as cartilage or bone. Cell
processes of different
osteoblasts join together
2. Osteoblasts produce bone
matrix. Osteoblasts then
become osteocytes.
Fig. 6.3

Bone Histology
• woven or lamellar bone, according to organization of collagen fibers
– Woven bone • collagen fibers in many diff directions
• remodeled to form lamellar bone
– Lamellar bone • Mature bone
• collagen fibers parallel to 1 another
• Arranged in thin layers called lamellae
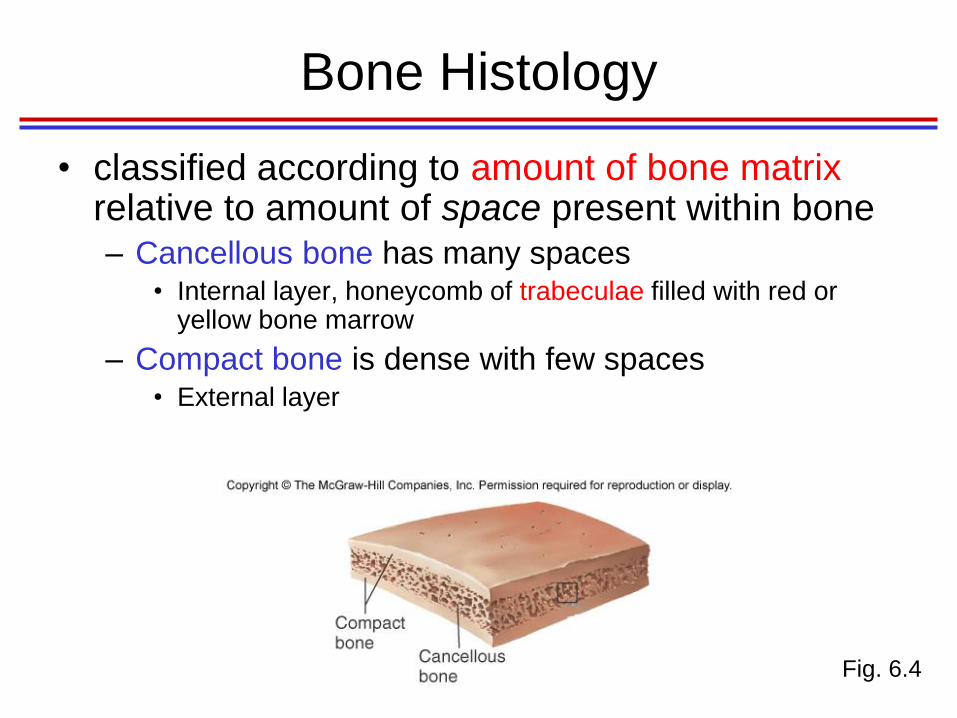
Bone Histology
• classified according to amount of bone matrix relative to amount of space present within bone – Cancellous bone has many spaces
• Internal layer, honeycomb of trabeculae filled with red or yellow bone marrow
– Compact bone is dense with few spaces • External layer
Fig. 6.4

Bone Histology
• Cancellous
– Lamellae combine to form trabeculae
• Beams of bone that interconnect to form a lattice-like structure with spaces
• filled w/bone marrow and blood vessels
– Trabeculae oriented along lines of stress: provide structural strength
Fig. 6.4

Compact Bone Histology
– organized lamellae
• Circumferential lamellae form outer surface of compact
bones
• Concentric lamellae surround central canals, forming osteons
• Interstitial lamellae are remnants of lamellae left after bone
remodeling
– Canals within compact bone provide a means for
exchange of gases, nutrients, and waste products
• From periosteum (endosteum), perforating canals carry blood
vessels to central canals
• Canaliculi connect central canals to osteocytes

Fig. 6.5

Bone Anatomy
• Individual bones classified according to shape – Long
• Longer than wide
• Most bones of appendages
– Short • About as wide as long
• carpals and tarsals
– Flat • Relatively thin, flattened shape, usually curved
• Certain bones of skull, all ribs, breastbone (sternum), shoulder blades (scapulae)
– Irregular • Do not fit into other 3 categories
• Vertebrae, pelvic girdle, facial bones

Bone Anatomy
• Structure of Long Bone
• diaphysis and epiphysis
– Diaphysis • Tubular shaft, forms axis of long bones
• compact bone, surrounds medullary cavity – Yellow bone marrow (fat) in medullary cavity of adults
• Not to same extent, but certain bones also contain red marrow

Bone Anatomy
• Structure of Long Bone
– Epiphyses
• Expanded ends of long bones
• Exterior is compact bone, interior is spongy bone
• Joint surface is covered with articular (hyaline)
cartilage
• Epiphyseal line separates diaphysis from epiphyses
• Epiphyseal plate is site of bone growth in length
– Epiphyseal plate becomes epiphyseal line when all its
cartilage is replaced with bone

Bone Anatomy
• Bone Membranes
– Periosteum: double layer of protective
membrane covering outer surface of bone
• Outer fibrous layer is dense regular conn tissue,
contains blood vessels and nerves
• Inner osteogenic layer contains osteoblasts,
osteoclasts, and osteochondral progenitor cells
– Endosteum: delicate membrane covering
internal surfaces of bone
• Contains osteoblasts, osteoclasts, and osteochondral
progenitor cells

Fig. 6.6
Bone Anatomy
• Structure of Flat, Short, and Irregular
Bones
– Flat bones contain interior framework of
cancellous bone sandwiched between 2
layers of compact bone
– Short and Irregular bones have a
composition similar to ends of long bones

Bone Development
• Begins at week 8 of embryonic development
• Intramembranous ossification: bone develops from a fibrous membrane
– Some skull bones, part of mandible, diaphyses of clavicles
• Endochondral ossification: bone forms by replacing hyaline cartilage
– Bones of base of skull, part of mandible, epiphyses of clavicles, most of remaining skeletal system
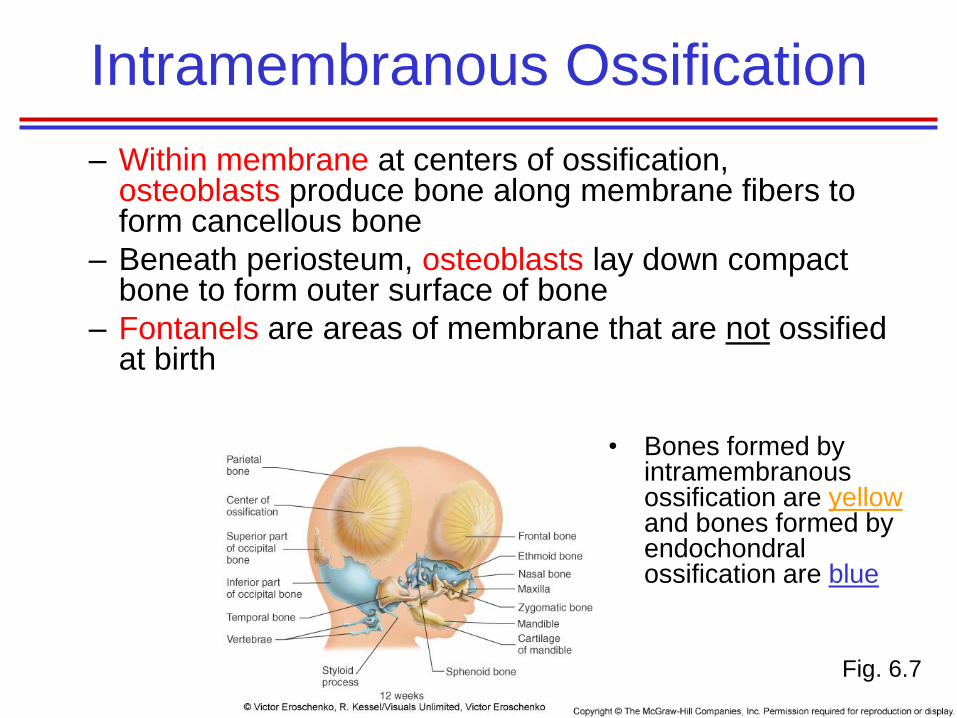
Intramembranous Ossification
– Within membrane at centers of ossification, osteoblasts produce bone along membrane fibers to form cancellous bone
– Beneath periosteum, osteoblasts lay down compact bone to form outer surface of bone
– Fontanels are areas of membrane that are not ossified at birth
Fig. 6.7
• Bones formed by intramembranous ossification are yellow and bones formed by endochondral ossification are blue

Fig. 6.7

Fig. 6.8

Endochondral Ossification
– Uses hyaline cartilage “bones” as models for bone construction
– Requires breakdown of hyaline cartilage prior to ossification
– perichondrium covering hyaline cartilage “bone” infiltrated with blood vessels, converting it to vascularized periosteum
– change in nutrition transforms underlying osteochondral progenitor cells into osteoblasts
– Formation of bone collar around diaphysis of hyaline cartilage model

Endochondral Ossification cont.
– Blood vessels grow into calcified cartilage, bringing
osteoblasts and osteoclasts from periosteum
– primary ossification center forms as osteoblasts lay
down bone matrix
– Medullary cavity forms
– Appearance of secondary ossification centers in
epiphyses
– Ossification of epiphyses, with hyaline cartilage
remaining only in epiphyseal plates

Fig. 6.9a
Endochondral Ossification

Fig. 6.9b
Endochondral
Ossification
Continued

http://www.flashcardmac
hine.com/anatomy.html
Study by app
Anatomy & physiology
Anatomy & Physiology
Revealed

Bone Growth
• Bones increase in thickness/width by
appositional growth
– Adding of new bone on surface of older bone
or cartilage
• Bones increase in length by interstitial
growth
• Trabeculae grow by appositional growth

Bone Growth
• Growth in Bone Length
– Bone length increases because of growth at
epiphyseal plate
– Epiphyseal plate growth involves
• Interstitial growth of cartilage
• Followed by appositional bone growth on cartilage
– Epiphyseal plate growth results in an increase in
length of diaphysis and bony processes
– Bone growth in length ceases when epiphyseal
plate becomes ossified and forms epiphyseal line

Postnatal Bone Growth
• Growth in Long Bones – epiphyseal plate
1. Zone of resting cartilage • Cartilage attaches to epiphysis
2. Zone of proliferation • New cartilage produced on epiphyseal side of plate as
chondrocytes divide and form stacks of cells
3. Zone of hypertrophy • Chondrocytes mature and enlarge
4. Zone of calcification • Matrix is calcified, and chondrocytes die
• Ossified bone – calcified cartilage on diaphyseal side of plate is
replaced by bone
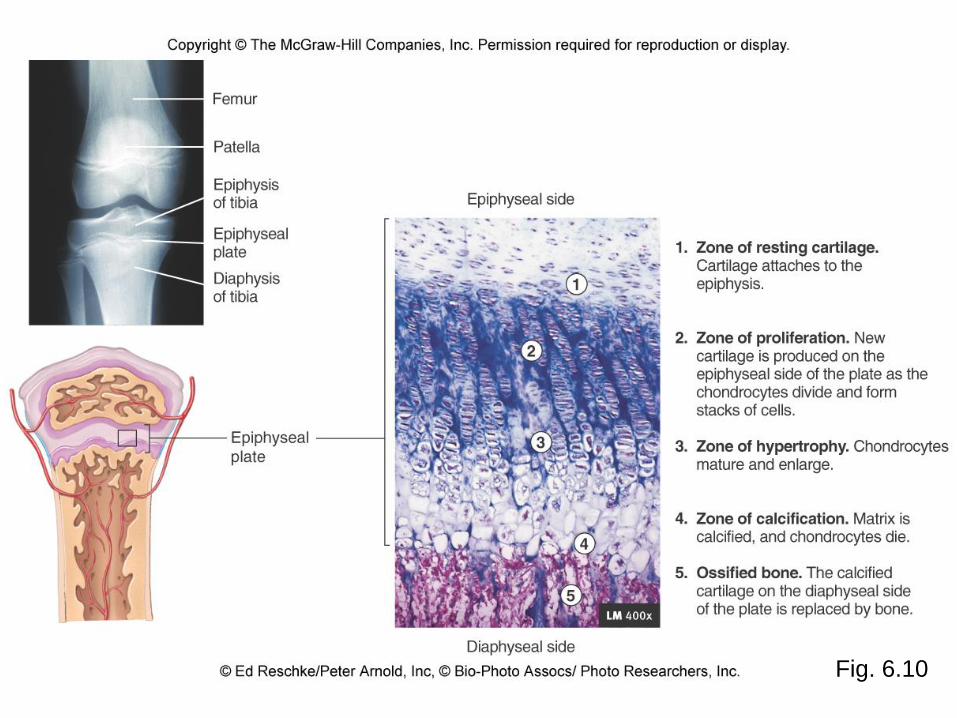
Fig. 6.10

Fig. 6.11

Bone Growth
• Growth at Articular Cartilage
– interstitial growth of cartilage followed by
appositional bone growth on cartilage
– Results in larger epiphyses and increase in
size of bones that do not have epiphyseal
plates

Bone Growth
• Growth in Bone Width – Appositional bone growth beneath
periosteum increases diameter of long bones and size of other bones
– Osteoblasts from periosteum form ridges with grooves between them
– ridges grow together, converting grooves into tunnels filled with concentric lamellae to form osteons
– Osteoblasts from periosteum lay down circumferential lamellae, which can be remodeled
Fig. 6.12

http://highered.mcgraw-
hill.com/sites/0042561336/student_view0/chapter7/bone_g
rowth_in_width.html

Bone Growth
• Factors Affecting Bone Growth
– Genetic factors determine bone shape and size
• expression of genetic factors can be modified
– Factors that alter mineralization process or production of organic matrix
• Deficiencies in vitamin D
– Hormones • Growth hormone, estrogen, testosterone stimulate
bone growth
• Estrogen and testosterone cause closure of epiphyseal plate

Bone Remodeling
• Remodeling converts woven bone to lamellar bone and allows bone to – Change shape
– Adjust to stress
– Repair itself
– Regulate body calcium levels
• Basic multicellular units (BMUs) make tunnels in bone, which are filled with concentric lamellae to form osteons – BMUs are temporary assemblies of osteoclasts and osteoblasts
– BMU activity renews the entire skeleton every 10 years
• Interstitial lamellae are remnants of bone not removed by BMUs
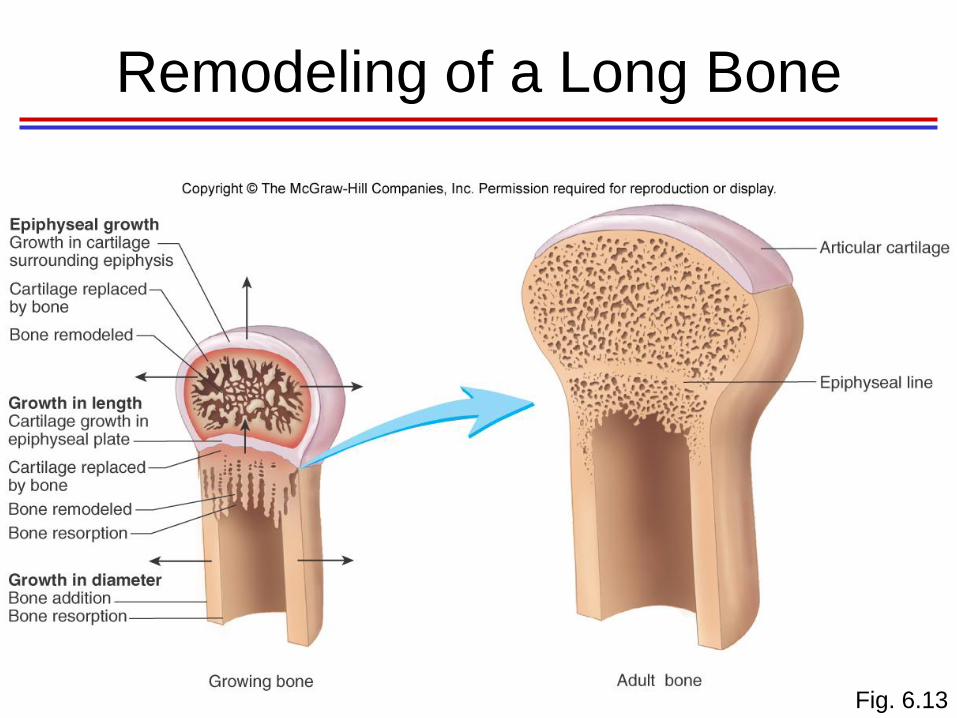
Remodeling of a Long Bone
Fig. 6.13

Bone Fractures (Breaks)
• Bone fractures classified by:
– position of bone ends after fracture
– completeness of break
– orientation of bone to long axis
– Whether or not bone ends penetrate skin

Page
137

Bone Repair
Fig. 6.14

Bone Repair
1. Hematoma formation
–Torn blood vessels
hemorrhage
–mass of clotted blood
(hematoma) forms at
fracture site
–Site becomes swollen,
painful, and inflamed
Fig. 6.14

Bone Repair
2. Callus formation
– Granulation tissue
(soft callus) forms a
few days after
fracture
– Capillaries grow into
tissue and
phagocytic cells
begin cleaning
debris
Fig. 6.14

Bone Repair
2. Callus formation cont.
– external callus forms when:
• Osteoblasts and fibroblasts migrate to fracture
and begin reconstructing the bone
• Fibroblasts secrete collagen fibers that connect
broken bone ends
• Osteoblasts begin forming woven bone
• Osteoblasts furthest from capillaries secrete an
externally bulging cartilaginous matrix that later
calcifies

Bone Repair
3. Callus ossification
– fibers and cartilage of
internal and external
calluses are ossified to
produce woven,
cancellous bone
– Cancellous bone
formation in callus
usually complete 4-6
weeks after injury
Fig. 6.14
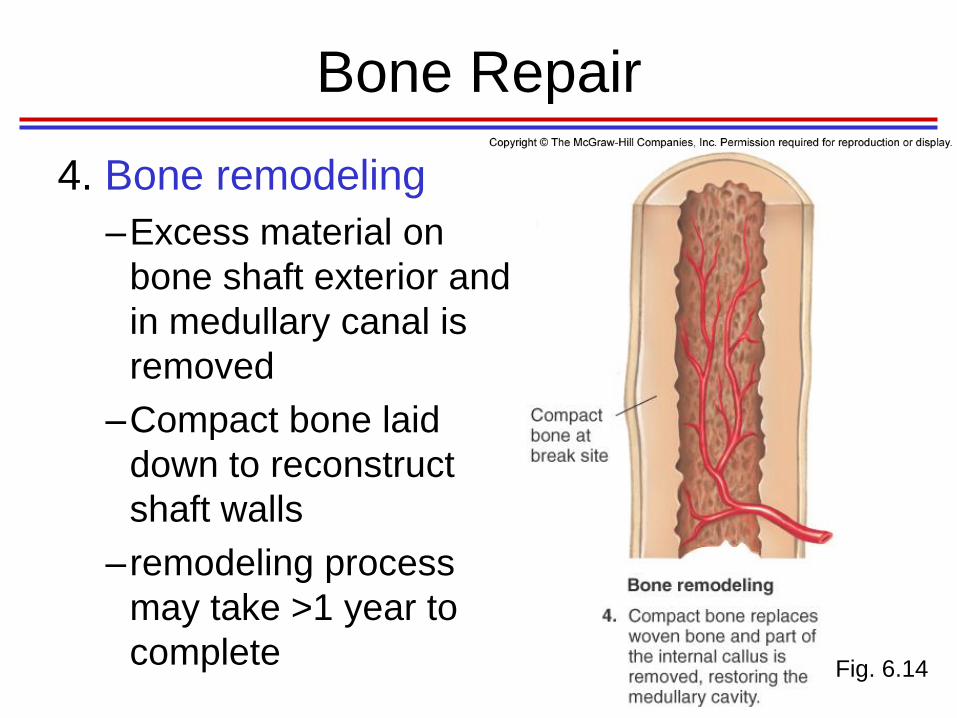
Bone Repair
4. Bone remodeling
–Excess material on
bone shaft exterior and
in medullary canal is
removed
–Compact bone laid
down to reconstruct
shaft walls
–remodeling process
may take >1 year to
complete Fig. 6.14

Bone Repair
Fig. 6.14

Calcium Homeostasis
• Bone is major storage site for calcium (Ca2+)
• 2 hormones regulate Ca2+ levels in blood: parathyroid hormone (PTH) and calcitonin – PTH is major regulator of blood Ca2+
• Falling blood Ca2+ levels signal parathyroid glands to release PTH
• PTH signals
– Osteoclasts to degrade bone matrix and release Ca2+ into blood
– Ca2+ absorption from small intestines
– Reabsorption of Ca2+ from urine
– Calcitonin • Rising blood Ca2+ levels trigger thyroid to release calcitonin
• Calcitonin stimulates calcium salt deposition in bone by decreasing osteoclast activity

Fig. 6.15

Effects of Aging
on the Skeletal System
• With aging, bone matrix is lost and matrix becomes more brittle
• Cancellous bone loss results from a thinning and loss of trabeculae
• Compact bone loss mainly occurs from inner surface of bones and involves less osteon formation
• Loss of bone – Increases risk for fractures
– Causes deformity
– Loss of height
– Pain
– Stiffness
– Loss of teeth

Osteoporosis
Page 138

http://highered.mcgraw-
hill.com/sites/0072495855/student_view0/chapter6/animation__os
teoporosis.html

Page
142