chapter 6 - the muscular systemfaculty.madisoncollege.edu/cshuster/general/aa-lecture-notes/... ·...
TRANSCRIPT
Chapter 6 - The Muscular System
- Muscle = “Little mouse”. Only tissue that can cause movement.
I. OVERVIEW OF MUSCLE TISSUES
- cells = “fibers”
- use special organelles called myofilaments to contract (“shorten”). Myofilaments are made of the contractile proteins actin and myosin.
- prefixes “myo-” and “sarco-” are used for the naming of organelles.
- they are excitable!! (that is...increase Na+ leads to an AP on their PM,which will be propagated). Therefore, their PM also has a special name:Sarcolemma.
A. Muscle Functions
1. Producing Movement
2. Maintaining Posture
3. Stabilizing Joints
4. Generating Heat : thermoregulation. We are homeothermic, whichmeans we control our body temperature (recall Chemistry Chapter for whytemperature is important for your body).
Hypothermia: low body temperature.
Therefore, your skeletal muscles are never turned off. Instead, we loweror increase activity. If for some reason they lose stimulation (say,because the neurons that control them are destroyed), your body gets ridof this tissue very quickly (= atrophy).

*consequences of this: the amount of aerobic cellular respiration is huge!
Oxygen + glucose -------> ATP + CO2 + HOH
**These tissues need an almost constant oxygen input, and theirmetabolism makes a lot of CO2 and lactic acid (both are acids), soyou must get rid of this or body pH changes rapidly.
**also, because of their huge energy needs, muscle is the onlytissue that can directly use your fatty acids. Must use them to burnfat!
B. Muscle Types
- NOTE: (not in book) For all these tissue types, there will be a generaltrend:
An AP causes an increase in Ca++, which will cause contraction”. ATPwill be used to contract, and heat will be generated
* If we increase Na+ permeability of the sarcolemma, we’ll have anAP run down the sarcolemma.
*This will inevitably increase [Ca++] within the cell’s cytoplasm(called the sarcoplasm).
*Ca++ will attach to the myofilaments, which will cause them toshorten.

*This will shorten the cell (fiber), causing contraction.
*Difference between muscle tissue types:
i. how generate the AP (some = neurotransmitter, somehave spontaneous generation), and which nervous system iscontrolling them.
ii. where does the Ca++ come from (some store it inside thecell, some get it from the extracellular fluid).
iii. how are the myofilaments arranged.*2 have sarcomeres*1 does not
iv. Shape of the cells, and how are they arranged withrespect to each other.
*long & parallel*shorter and in sheets*very short and branching and forming a bag
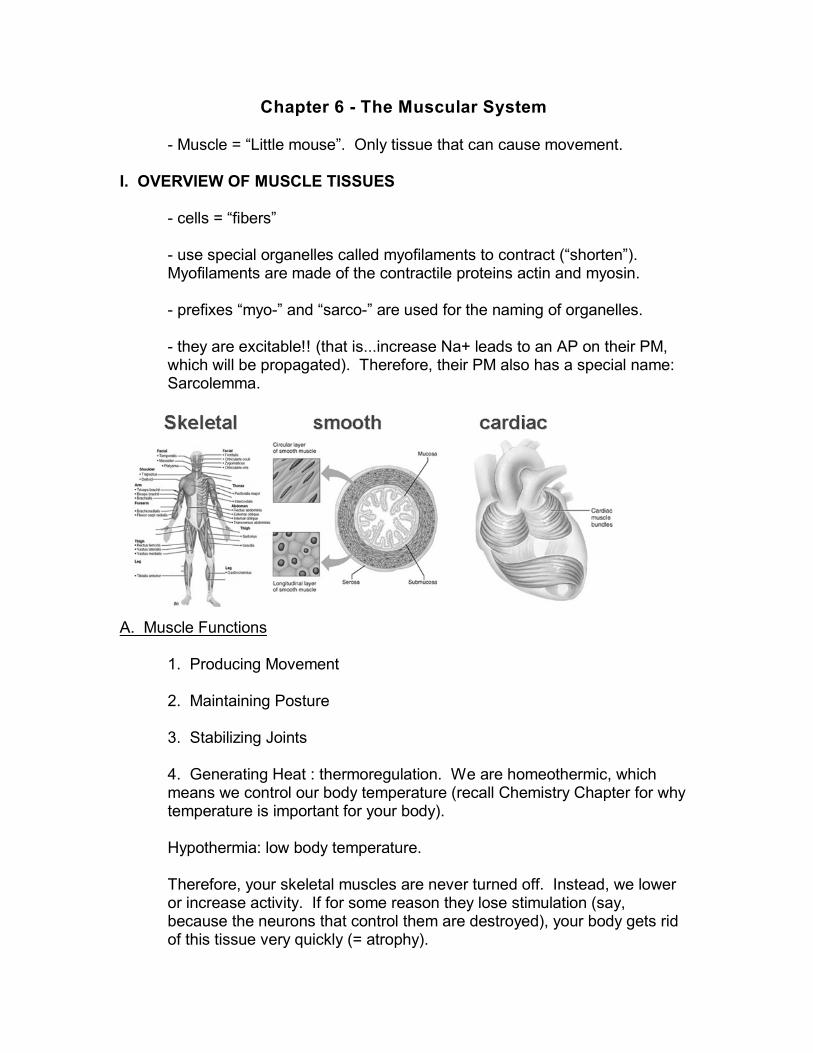
1. Skeletal Muscle : contraction causes movement of a bone around anarticulation = locomotion (movement through pace).
*spindle (cigar) shaped, multinucleate, long. Up to a foot long. Fibers of hip can be seen with naked eye.
*”striated” muscle, because myofilaments are arranged instructures called sarcomeres, which actually do the contracting(therefore, sarcomeres are organelles in striated tissue thatcontract, made out of myofilaments).
*”voluntary” = controlled byy the somatic nervous system...but it issomething of a misnomer, as most contractions are not controlledby the conscious cerebral cortex.
*exert a lot of force when they contract. Therefore, use a lot of ATP(very red tissue due to presence of lots of mitochondria). Also,generate a lot of heat, which is used for thermoregulation (goosebumps are contractions of the erector pillae muscles of the hairs inorder to generate heat. Also, shivering).

2. Smooth Muscle : squeeze a tube in waves called peristalsis.
*shorter cells, uninucleate.
*not striated, but still use myofilaments (but they are not arrangedinto sarcomeres). Not a lot of ATP, not a lot of force. However,contractions are sustained.
*synonyms: visceral, non-striated, involuntary (controlled by theautonomic system...no conscious awareness).
*found in sheets around all visceral organs. Recall our discussionof how visceral organs are set up in the “Cells & Tissues” chapter.
*these cells can spontaneously generate APs. APs spread throughentire sheet.
3. Cardiac Muscle : contract the heart.
*even shorter cells, usually uninucleate.
*short, branching cells forming a bag. Contraction causes bag tosqueeze.
*striations present (although not called “striated muscle tissue”). Lots of ATP, lots of force.
*spontaneously generate APs.
*cells attached to each other with intercalated disks. These diskspass APs from one cell to the next...so if one contracts, they all do(myocardium acts as a unit ... that is, they all squeeze together!).

II. MICROSCOPIC ANATOMY OF SKELETAL MUSCLE
- Skeletal muscle: A muscle is a large bundle of fibers, blood vessels,adipose and nerves that, when the individual cells contract, contracts andpulls one bone towards another around a joint. Muscle is surrounded bythe epimysium.
*origin, insertion, belly, tendons
- muscle fibers are arranged in fascicles (“bundles) of fibers, surroundedby the perimysium.
*fibers within a fasiculus are connected to each other by motorneurons. Motor unit = motor neuron + fibers it innervates.
- individual fibers are bundles of myofibrils. Fiber is surrounded byendomysium.
- myofibrils are composed of myofilaments, thick (made of myosin)and thin(made of actin), arranged in sarcomeres, that are lined up end-to-end likeboxcars on a train.
*thin myofilaments have a binding site for heads of myosinmolecules.

At rest (not contracting), these sites are covered. Ca++ ions cause them tobecome “uncovered”, and the heads attach forming cross bridges. Then,contraction will occur (see later) if ATP is present.
III. SKELETAL MUSCLE ACTIVITY
A. Stimulation and Contraction of Single Skeletal Muscle Cells
1. Mechanism of Muscle Contraction: The Sliding Filament Theory(different order from book)
- we will just look at skeletal muscle tissue as an example. Cardiac worksin much the same way. Smooth works differently, but still hasmyofilaments.
- fibers are packed with myofilaments, made of Actin (thin filaments) andMyosin (thick filament). They are arranged in a sarcomere:
i. Thin & thick filaments are interdigitated. They are connected to aplate at each end called the Z-line or Z-plate. At rest, thesarcomere is “opened”...that is, the z-lines are far apart from eachother.

ii. If Ca++ is present, binding sites on thin are revealed, and thecross bridges are formed between the thin & thickmyofilaments
iii. These cross bridges do the “Power Stroke”:*1. Cross bridges bond to a thin filament*2. “cocking” the head back, sliding the thin past the thick*3. letting go of the thin filament, grabbing it again,etc.....sliding the thin past the thick and moving the z-linestowards the middle and shortening the sarcomere.
iv. Each “stroke” of the cross bridges needs an ATP molecule sothey can let go and get ready for the next stroke.
*rigor mortis: after death, cells run out of ATP becausecellular respiration stops. Cross bridges can’t letgo....muscles are “stuck”. Last until the proteins begin todegrade, which are at a fairly constant rate giventemperature & humidity, which is why we can place the timeof death for a couple of days.
v. This continues as long as Ca++ is present, which continues aslong as there is stimulation by an AP on the sarcolemma.

2. The Nerve Stimulus the Action Potential, and Ca++ release.
- Ok. .... .we’ve seen what happens IF Ca++ is released...but how do weget it there (in the sarcoplasm)?
*Sarcoplasmic Reticulum (SR): special organelle that stores Ca++in the cell.
- Uses a lot of ATP to pump Ca++ into itself.
- If it is electrically stimulated, it will release Ca++ into thesarcoplasm, which will diffuse throughout and bind to thesarcomeres, and contraction begins.
- Ok ..... but how do we electrically stimulate the SR?

The synapse (here, referred to as the Neuromuscular Junction) & thesarcolemma! The CNS sends an AP down a motor neuron, and:
*1. Neurotransmitter is released from the end bulb of neuron,diffuses across the cleft.
*2. NT binds to Na++ channels on a special region of thesarcolemma called the motor end plate.
*3. Na++ channels open, sarcolemma depolarizes, and an APrushes down the sarcolemma (recall that muscle tissue isexcitable!).
*4. In order to get the AP close to the SR, there are tubes in thesarcolemma called T-tubules. AP goes down T-tubules, comingclose enough to the SR to excite it, causing it to release Ca++,etc......
**NOTE: a lot of things can go wrong here. Myosenia gravis= loss of the channels, leading to muscle weakness. Someneurotoxins (like snake & spider venoms) affect the systemhere.

B. Contraction of a Skeletal Muscle as a Whole
1. Graded Responses, Muscle Response to Increasingly RapidStimulation and Muscle Response to Stronger Stimuli
- How do we increase contraction of a single fiber?
*if we increase the # of APs on the motor neuron, we increase theamount of Ca++ in the sarcoplasm, which increase the # of crossbridges formed, which increase contraction.. Once all thesarcomeres are contracted all the way, the muscle cells can’tincrease contraction anymore.
- Muscle Twitch: contraction of a single cell.
- contraction of a single fiber is “all or none”. But we canincrese frequency of APs to “summate the contractions”.
- there is a limit when all the sarcomeres are fully contracted Tetanus is this limit.
-another limitation: based on Ca++ and ATP availability. Fatigue will eventually happen.

-So, can the system increase contraction power?
*The CNS can stimulate more fibers in the same muscle. If all thefibers are contracted all the way, we can’t get any more contractionout of the muscle.
- Motor Unit: a motor neuron & all the fibers it innervates. Bychanging this, we change strength. This is the differencebetween a “tap” and a “slap”.
- Grade Responses: we can change the speed of musclestimulation, or the # of motor units involved.
- So how do we stop contraction?
*Contraction is never “off” completely....there is always somestimulation to the sarcolemma, and some contraction, forthermoregulation and posture.
*We can lessen contraction by lessening the frequency of APs onthe motor neuron, which lessens the amount of Ca+ being released(and lets the SR pump it back into itself), which lessens thecontraction of the sarcomeres.

C. Providing Energy for Muscle Contraction

The “machine”is really 3 energy routes. However, they are attached to eachotehr. The limiting factor is time:
1. Energy Routes : 3 ways to do it, 2 inefficient & 1 efficient (usingoxygen). Depends on how much time you give the muscles:
i. Direct Phosphorylization of ADP (Phosphorylization =”put on aphosphorus”):
ADP + Pi --------creatine kinase---------> ATP
*the phosphate comes from an enzyme called creatinephosphatase
*energy to put the Pi onto the ADP comes from fatty acids.
*good points: easy to make the enzyme creatine kinase.
*bad points: NEEDS ENERGY! Inefficient to use energy to makeenergy, so your body will do ANYTHING not to have to do this!
*this is why it’s hard to burn off your fat!

ii. Aerobic Respiration : (“oxygen breathing”) - needs O2!
*takes place in the Mitochondria. Needs O2 and Glucose (energysources).
*several chemical steps involved in the process called OXIDATIVEPHOSPHORYLIZATION (“putting on a phosphorus by usingoxygen”)
* the chemical bonds of the fuel molecules (O2 and glucose) arebroken, which releases energy that is then used to put a Pi on ADPto form ATP.
Glucose + O2 -----------> CO2 + H2O + ATP
*the CO2 must be gotten rid of thru the respiratory system, as it isan acid.
*Good points: LOTS of ATP are formed (36 ATP/glucose molecule)= very efficient!
*Bad points: SLOW!!! Takes a long time to kick in.
iii. Anaerobic Respiration : (“breathing w/out oxygen”).
*also known as GLYCOLYSIS (“sugar splitting”).
*In the cytoplasm:
Glucose -------(enzymes)-------> 2 pyruvic acids + energy released
*then, the energy that is released is used for directphosphorylization:
2 ADP + Pi + energy -------------> ATP
*glucose is split into 2 smaller molecules:
*good points: FAST, no O2 required.

*Bad points: inefficient, not many ATPs / glucose. Also, pyruvicacid is converted into LACTIC ACID, which builds up in bloodstream, which can change the pH of the blood. (see later section on“Fatigue and Oxygen Debt”).
-so, when do we use one system or another?
*low exertion: Aerobic Respiration; have time for the more efficienttype.
*high exertion: Anaerobic Respiration (GLYCOLYSIS)--IF OVER70% OF MAXIMUM ACTIVITY.
**muscles bulge, which restrict blood flow (= availability ofO2). This cues fibers to switch to glycolysis.
**but, have a lactic acid build-up, which will increase the pHand damage muscle proteins; how get rid of it? In the liver:
lactic acid + O2------------->CO2 + H2O

2. Muscle Fatigue and Oxygen Debt
- eventually, muscle lowers contraction even though stimulation by motorneuron continues. Of course, we can run out of ATP, fatty acids, etc. Buta major reason is the Oxygen Debt
*Recall:During anaerobic respiration, pyruvic acid is converted into LACTICACID, which builds up in blood stream, which can change the pH ofthe blood.
In the liver:lactic acid + O2------------->CO2 + H2O
So: you still need oxygen, even during anaerobic respiration. Thissi why you breath hard after you are done exercising hard(anaerobically)
3. Types of Skeletal Muscles
i. Based on Tissue types:
- Red Fibers (not in book): lots of mitochondria, do not fatigue easily (slowtwitch). Sustained contractions
- White fibers (not in book): fewer mitochondria, go anaerobic easily,strong & forceful (fast-twitch) but fatigue easily.
- Pink fibers: in-between.

ii. Based on Functions:
- Prime Movers
- Antagonist
- Synergists
- Fixators
iii. Based on Shapes: we won’t go into it here.
4. Types of Muscle Contractions - Isotonic and Isometric : Outdated tosome degree, but still a useful lesson:
i. Isotonic: “same tone” = “same shape”. On the prime mover, themuscle shortens, bone moves, tone is maintained (the antagonists are notcontracted at the same time. The fixators maintain coordination)
ii. Isometric = “same metric” = “same length”. No contraction, no movingof bone. Antagonists are contracted equally.
5. Muscle Tone : as mentioned, skeletal muscle tissue is alwayscontracting slightly. This is tone....always have some shape. If fibers arecut = “Flaccid Paralysis” = will lead to atrophy.
6. Effect of Exercise on Muscles : Aerobic (greater resistence to fatique)versus Resistance (increase size via isometric exercise) exercise. Increase in size is due to wider cells (more myofilaments), not more cells.

III. MUSCLE MOVEMENTS, TYPES, AND NAMES
A. Types of Body Movements
- with relation to how the body part is moved. Some muscles can doseveral of these movements. Always take about which bone is beingmoved, and around which joint (EX: flex the arm at the elbow, etc.).
Flexion Extension Abduction Adduction Rotation Circumduction Pronation Supination Inversion Eversion Dorsiflexion Plantar Flexion
B. Naming Skeletal Muscles
- based on size (maximus versus minimus), location (pectoralis, etc.),number of origins (biceps, etc.), location of attachments(sternocleidomastoid, etc.), shape (deltoid, etc.) and action (extensor,adductor, etc.)
IV. GROSS ANATOMY OF SKELETAL MUSCLES
A. Head Muscles
Facial Muscles : expressions & chewingFrontalis Orbicularis Oculi Orbicularis Oris Buccinator Zygomaticus Chewing Muscles:
Masseter Temporalis

B. Trunk and Neck Muscles
Anterior Muscles : flexion, raising of upper torso, moving entire arm atshoulder and respiration
Platysma Sternocleidomastoid Pectoralis Major Intercostal Muscles
Muscles of the Abdominal Girdle : flexion of lower torso and hold inabdominal organs
Rectus Abdominus External Oblique Internal Oblique Transversus Abdominus
Posterior Muscles : extension of torso (posture) and moving entire arm atshoulder
Trapezius Latissimus Dorsi Erector Spinae Deltoid
C. Muscles of the Upper Limb
Muscles of the Humerus That Act on the Forearm
Biceps Brachii : anterior = flexTriceps Brachii : posterior = extend
D. Muscles of the Lower Limb
Muscles Causing Movement at the Hip Joint
Iliopsoas Adductor Muscles Gluteus Maximus Gluteus Medius

Muscles Causing Movement at the Hip Joint and Knee Joint together:
Sartorius
Quadriceps Group Rectus Femoris Vastus Muscles
Hamstring Group
Biceps Femoris Semimembranosus Semitendinosus
Muscles Causing Movement at the Ankle and Foot
Tibialis Anterior Peroneus Muscles Gastrocnemius