chapter 35 cardiac disorders
TRANSCRIPT

CHAPTER 35 Cardiac DisordersJUDY L. MALTASObjectives
After reading and studying this chapter, you should be able to:
1. Label the major parts of the heart. 2. Describe the flow of blood through the heart and coronary vessels. 3. Name the elements of the heart's conduction system. 4. State the order in which normal impulses are conducted through the heart. 5. Explain the nursing considerations for patients having procedures to detect or evaluate
cardiac disorders. 6. Identify nursing implications for common therapeutic measures, including drug, diet,
or oxygen therapy; pacemakers and cardioverters; cardiac surgery; and cardiopulmonary resuscitation.
7. Explain the pathophysiology, risk factors, signs and symptoms, complications, and treatment for selected cardiac disorders.
8. List the data to be obtained in assessing the patient with a cardiac disorder. 9. Assist in developing nursing care plans for patients with cardiac disorders.
Key Termsafterload
(p. 631)
arteriosclerosis
( , p. 652)
atherosclerosis
( , p. 653)
bradycardia
( , p. 633)
contractility
(p. 631)
diastole
(p. 631)
dysrhythmia
( , p. 655)
hemodynamics
( , p. 661)
murmur
( , p. 633)
myocardial infarction
( , p. 654)
palpitation
( , p. 632)
perfusion
( , p. 648)
preload
(p. 631)
regurgitation
( , p. 670)
syncope
( , p. 632)
systole
(p. 627)
tachycardia
( , p. 633)
thromboembolism
( , p. 655)
The cardiovascular system carries oxygenated blood and nutrients to the cells and transports carbon dioxide and wastes from the cells. It requires a reservoir for blood coming from the tissues, pumping action to send blood to the lungs and the body, and an intact vascular system to transport the blood. A malfunction in any of these components may affect other body systems and may threaten the life and health of the person.
The heart is a hollow muscular pump located in the mediastinum (Fig. 35-1). The right and left sides of the heart receive blood from and send blood to different parts of the body. The heart is covered and protected by the sternum and the ribs anteriorly and flanked by the lungs laterally. The esophagus, the descending aorta, and the fifth through the eighth thoracic vertebrae are directly behind the heart. The heart rests on the diaphragm, with two thirds of it to the left of the sternum. The right side of the heart is located under the sternum. The heart is approximately the size of the person's fist, weighs 10 to 14 ounces in the adult, and is covered by membranes called the visceral and parietal pericardium. The space between the pericardial membranes contains fluid that lubricates the membranes and decreases friction.
ANATOMY AND PHYSIOLOGY OF THE HEARTCHAMBERS
The heart is divided into four chambers: two upper atria (right and left) and two lower ventricles (right and left). The four chambers are separated by septa (walls) with two chambers on the right (right atrium and ventricle) and two chambers on the left (left atrium and ventricle). Valves separate the atria from the ventricles.
The right atrium (RA) is a thin-walled reservoir and conduit for systemic blood. It receives blood from the inferior and the superior venae cavae and from the coronary sinuses. The right ventricle (RV) has thicker walls than the RA and receives blood from the RA through the tricuspid valve. Blood moves rather passively from the RA to the RV. When the RV contracts (systole), blood is ejected through the pulmonic valve into the pulmonary artery. The pulmonary artery carries the blood to the lungs, where it releases carbon dioxide as waste and picks up oxygen to be taken to the tissues. Pulmonary veins carry the blood from the lungs to the left atrium (LA).
FIGURE 35-1 Anatomic location of the heart.
The blood passes from the LA through the mitral valve into the left ventricle (LV), the chamber with the thickest, strongest muscle. The LV is cone-shaped and contains the apex of the heart located at the midclavicular line at the fourth or fifth intercostal space. An apical pulse is taken by auscultating the heartbeat at this location.
When the LV contracts (systole), blood is ejected through the aortic valve into the aorta and the systemic circulation. The systemic circulation carries oxygen and nutrients to all active cells and transports wastes to the kidneys, liver, and skin for excretion (Fig. 35-2).
The pressures in the RA and RV are very low compared with the pressures in the LA and LV. This is because the LV pumps blood out into the systemic circulation. The pressure in the LV is the highest of all the chambers.
MUSCLE LAYERS
There are three layers of cardiac muscle tissue: the endocardium, the myocardium, and the epicardium. The endocardium is the inner layer that lines the heart chambers. The middle layer, the myocardium, is made of muscle fibers. It is responsible for the pumping action of the heart. The thickness of the myocardium varies with each chamber. The outer layer, the epicardium, is also the visceral pericardium. The coronary arteries are embedded in the epicardium.
VALVES
There are four valves in the heart: the mitral, the tricuspid, the aortic, and the pulmonic. Their purpose is to retain blood in one chamber until the next chamber is ready to receive it. The valves keep blood flowing in one direction. The valves open and close passively in response to changes in pressure and volume. A valve opens when the pressure behind it is greater than the pressure ahead of it. A valve closes when the pressure ahead of it is greater than the pressure behind it.
Atrioventricular Valves
The mitral and tricuspid valves are called atrioventricular (AV) valves because they separate the atria from the ventricles. The mitral valve is between the LA and the LV. The tricuspid valve separates the RA from the RV. The cusps, or leaflets, are attached by chordae tendineae to the papillary muscles that line the floor of the ventricles. These valves are closed during systole and open in diastole.
Semilunar Valves
The semilunar valves, called aortic and pulmonic, separate the ventricles from the aorta and the pulmonary artery, respectively. These valves are open during systole and are closed during diastole. The semilunar valves have three cusps (cup-shaped structures) each.
FIGURE 35-2 Normal circulation through the heart.

Heart Sounds
Closure of the valves produces the heart sounds auscultated over the heart. The first heart sound (S1), referred to as “lub,” occurs when the ventricles contract during systole and when the mitral and tricuspid valves close. The second heart sound (S2), called “dub,” occurs during ventricular relaxation or diastole and is caused by the closing of the aortic and pulmonic valves.
CORONARY BLOOD FLOW
The coronary arteries are the first branches of the systemic circulation. These arteries supply blood to the myocardium and the conductive tissue of the heart. The two major coronary arteries, the left coronary artery and the right coronary artery, arise from the aorta just beyond the aortic valve. Blood flow through the coronary arteries occurs during diastole. The left coronary artery, which branches into the left anterior descending and circumflex arteries, supplies blood to the LA, most of the LV, and most of the septum between the two ventricles (interventricular septum). The right coronary artery branches to supply the sinoatrial (SA) and the atrioventricular (AV) nodes, the RA and RV, and the inferior part of the LV. Variations in the pattern of arterial branching are common.
Collateral arteries are connections between two branches of arteries. They are more common in certain areas of the heart. It is thought that collateral circulation protects the heart and that coronary collaterals develop over time as a result of gradual coronary occlusion.
In general, the venous system parallels the arterial system: the great cardiac vein follows the left anterior descending artery; and the small cardiac vein follows the right coronary artery. The veins meet to form the coronary sinus (the largest coronary vein), which returns deoxygenated blood from the myocardium to the right atrium (Fig. 35-3).
CONDUCTION SYSTEM
For the heart to pump blood through the chambers, nerves must stimulate muscle contractions in an orderly fashion. The conduction pattern follows a particular route. The SA node, also called the pacemaker, initiates the impulse. The impulse is carried throughout the atria to the AV node, located on the floor of the RA. The impulse is delayed in the AV node and then transmitted to the ventricles through the bundle of His. The bundle is made up of Purkinje cells and is located where the atrial and ventricular septa meet. The bundle of His divides into the left and right bundle branches. The left bundle branch divides into anterior and posterior branches called fascicles. The terminal ends of the right and left branches are called the Purkinje fibers. When the impulse reaches the Purkinje fibers, the ventricles contract (Fig. 35-4).
FIGURE 35-3 Coronary arteries and veins.
FIGURE 35-4 The conduction system of the heart.

The impulse produces a change in the movement of electrically charged ions across the membrane of cardiac cells. Cardiac cells at rest are electrically polarized, with the inside of the cell negatively charged and the outside of the cell positively charged. When stimulated, cardiac cells lose their internal negativity by a process called depolarization. Depolarization moves from cell to cell, producing a wave of electrical activity that is transmitted throughout the heart. Once depolarization is complete, the resting state (i.e., inside of the cell more negative than the outside) is restored through a process called repolarization.
The SA node normally generates these impulses at a rate between 60 and 100 beats per minute (bpm). The SA node is called the pacemaker of the heart. The AV node is also capable of generating an impulse if the SA node should fail. The AV node rate is 40 to 60 bpm. The Purkinje network also can generate an impulse, but at less than 40 bpm, which could prevent cessation of heart function for a short time (Table 35-1).
Cardiac Innervation
The heart is innervated by sympathetic and parasympathetic fibers of the autonomic nervous system. Sympathetic fibers are distributed throughout the heart. Sympathetic stimulation results in increased heart rate, increased speed of conduction through the AV node, and more forceful contractions. Parasympathetic fibers, which are part of the vagus nerve, are found primarily in the SA and AV nodes and the atrial tissue. Parasympathetic stimulation results in slowing of the heart rate, slowing of conduction through the AV node, and decreased strength of contraction.
CARDIAC FUNCTION
The primary function of the heart is to pump blood through the pulmonary and systemic circulations. This is accomplished by a continually repeating pattern of contraction and relaxation.
Cardiac Cycle
Contraction and relaxation of the heart make up one heartbeat and are called the cardiac cycle. When the ventricles are at rest (relaxation phase), they are filling up with blood coming from the atria. This is called diastole. At the end of diastole, the atria contract to eject more blood into the ventricles (called the atrial kick). Once the ventricles have filled with blood and the electrical impulse has reached the terminal fibers of the conduction system, the ventricles contract and eject blood into the pulmonary artery from the RV and into the aorta from the LV. This is called systole. In a person with a heart rate of 60 bpm, there would be 60 cardiac cycles per minute.
Cardiac Output
The volume of blood ejected by the heart each minute is determined by the stroke volume and the heart rate. Stroke volume is the amount of blood ejected with each ventricular contraction. The normal stroke volume is 60 to 100 mL. Cardiac output is the amount of blood (in liters) ejected by the heart per minute. It is calculated by multiplying the heart rate by the stroke volume (CO 5 HR 3 SV). The normal cardiac output is 4 to 8 L/min. In the normal heart, cardiac output

responds to the increased demands for oxygen and nutrients that occur with exercise, infection, or stress.
Table 35-1 Intrinsic Heart RatesINITIATION OF IMPULSE RATESinoatrial node 60-100 bpmAtrioventricular node 40-60 bpmVentricle 15-40 bpm
Three factors affect stroke volume: preload, contractility, and afterload.
Preload.
Preload is the amount of blood remaining in a ventricle at the end of diastole or the pressure generated at the end of diastole. Increased preload results in increased stroke volume and, therefore, increased cardiac output. Factors that increase preload include increased venous return to the heart and overhydration. Factors that decrease preload include dehydration, hemorrhage, and venous vasodilation.
Contractility.
Contractility is the ability of cardiac muscle fibers to shorten and produce a muscle contraction. Inotropy is a term used to refer to the contractile state of the cell. Factors that increase contractility are said to have a positive inotropic effect, and factors that decrease contractility create a negative inotropic effect.
Afterload.
Afterload is the amount of pressure the ventricles must overcome to eject the blood volume. It is determined primarily by the pressure in the arterial system. Afterload is decreased by vasodilation and increased by vasoconstriction.
Myocardial Oxygen Consumption
Myocardial tissue routinely needs 70% to 75% of the oxygen delivered to it by the coronary arteries. Skeletal muscles, by contrast, need 35% at rest and up to 75% during exercise. The only ways to increase oxygen supply to the myocardium are to (1) increase the coronary blood flow by coronary artery vasodilation or to (2) increase the oxygen in the blood by administering supplemental oxygen.
AGE-RELATED CHANGES
It is difficult to separate the normal age-related changes in the heart and blood vessels from the changes caused by disease. In general, age-related changes progress slowly, whereas pathogenic changes are more likely to be sudden.

HEART
Changes in the heart muscle include increased density of connective tissue and decreased elasticity. Cardiac contractility may decline, making the heart less able to adapt to changes in circulating blood volume. The valves may thicken and stiffen. If they do not close properly, the patient may have a murmur. The valves may also partially block the path of blood flow, causing incomplete emptying of the chambers.
The number of pacemaker cells in the SA node decreases, as does the number of nerve fibers in the ventricles. The aging heart takes longer to respond to stress and then responds less dramatically. It also takes longer to return to normal after exercise or stress. Cardiac dysrhythmias are more common in older people but should still be evaluated because they can be dangerous.
Health Promotion ConsiderationsLong-Term Conditioning
Long-term conditioning with an exercise program may help decrease arterial stiffening and improve the function of the left ventricle in older individuals. Physical exercise does not have to be strenuous to be helpful. Activity should become a part of an individual's regular routine.
BLOOD VESSELS
Changes in connective tissue and elastic fibers in arteries cause them to become stiffer. Physical activity can help reverse or delay this process (see the Health Promotion Considerations box above). Pulse pressure (the difference between the systolic and diastolic pressures) and systolic blood pressure generally increase. Experts disagree about what exactly constitutes hypertension in older adults. The veins stretch and dilate, leading to venous stasis and sometimes impaired venous return. Thrombophlebitis and varicosities are more common in older people.
The cardiovascular system adapts more slowly to changes in position; therefore postural hypotension may occur.
NURSING ASSESSMENT OF CARDIAC FUNCTIONHEALTH HISTORY
A complete assessment is important for the cardiac patient. If the patient is having acute symptoms, however, a detailed assessment must be deferred until the patient is stable.
Chief Complaint and History of Present Illness
Determine the patient's reason for seeking medical care. Common symptoms that may be related to cardiac disorders include fatigue, edema, palpitations, dyspnea, and pain. Note when symptoms occur, what aggravates them, and what relieves them.
Medical History

Ask whether the patient has had specific conditions that may be related to cardiac disease. These include hypertension, kidney disease, pulmonary disease, stroke, rheumatic fever, streptococcal sore throat, and scarlet fever. Document previous cardiac disorders and hospitalizations. List recent and current medications and note allergies in appropriate records. It is also important to ask whether the patient is taking any vitamins, herbs, or homeopathic remedies. It may be easier to ask something such as “What are you doing to stay healthy or to help you feel better?”
Family History
Because cardiovascular problems are often familial or hereditary, ask whether immediate relatives have had hypertension, coronary artery disease (CAD), other cardiac disorders, or diabetes mellitus.
Review of Systems
Inquire whether the patient has experienced the following specific symptoms: weight gain, fatigue, dyspnea (shortness of breath), cough, orthopnea (difficulty breathing in a supine position), paroxysmal nocturnal dyspnea (sudden dyspnea during sleep), palpitations, chest pain, syncope (fainting), concentrated urine, or leg edema.
If the patient has had dyspnea or orthopnea, determine when it occurred and whether the onset was gradual or sudden. Pain also requires detailed descriptions. The pain of heart problems may radiate or be referred to other areas. The pain may radiate down either arm, to the jaw, or to just below the sternum. The severity may range from mild, intermittent discomfort to severe, crushing chest pain. Ask the patient to rate the severity of the pain on a scale of 1 (mildest) to 10 (worst possible). Chest pain may be different in women and may be described as indigestion, as a feeling of anxiety, as nausea, or as a feeling of fatigue. Document the exact description, location, and severity, whether there is radiation, events causing the pain, and what relieves the pain.
Functional Assessment
Determine how this illness has affected the patient's ability to carry out usual activities. Describe activity and rest patterns and usual diet. It is especially important to record salt and fat intake. Ask the patient about sources of stress and coping strategies.
PHYSICAL EXAMINATION
Begin the physical examination with measurement of height and weight and recording of vital signs.
Vital SignsBlood Pressure.
The correct-size blood pressure cuff must be used. Position the arm at the heart level, and check the blood pressure in both arms. Note the pulse pressure (difference between the systolic and diastolic pressures) because it is a noninvasive measure of cardiac output. Next, measure blood
pressures and pulse rates in the lying, sitting, and standing positions. A blood pressure decrease of 20 mm Hg or more with a position change indicates decreased blood volume or an autonomic response. As blood pressure decreases, the pulse should increase as a compensatory mechanism.
Pulses.
Palpate the radial pulses for rate, rhythm, quality, and equality. Auscultate the apical pulse for rate and rhythm. Apical and radial pulses may be taken simultaneously to detect a pulse deficit. The normal heart rate is 60 to 100 bpm. A rate of less than 60 bpm is considered to be bradycardia; tachycardia is characterized by a heart rate in excess of 100 bpm. The rhythm is described as regular, irregular, or regularly irregular. The quality of the pulse is graded on a four-point scale: 0, absent pulse (not palpable); 1, weak or thready pulse (pulse easily obliterated by slight finger pressure, returning as pressure is released); 2, normal pulse (easily palpable); and 3, bounding pulse (forceful, not easily obliterated by finger pressure). With a stethoscope, listen at the fifth intercostal space at the midclavicular line to assess the apical pulse. In addition to the radial pulse, assess the carotid, brachial, femoral, popliteal, posterior tibial, and dorsalis pedis pulses at appropriate times in the physical examination.
Respirations.
Observe the patient's respiratory effort and skin color. Count the respiratory rate, and auscultate the breath sounds for crackles and wheezes. If the patient produces sputum, describe the color, amount, and appearance.
Skin
Inspect the skin for color, hair distribution, and capillary refill, and palpate the temperature. Skin color and temperature should be relatively the same over the entire body.
Heart Sounds
The heart sounds are systole (lub) and diastole (dub). To auscultate heart sounds, place the diaphragm of the stethoscope firmly on the anterior chest. Avoid auscultating heart sounds through clothing. Figure 35-5 shows where the heart sounds, made by closing of the valves, may be heard best. With practice, you can learn to distinguish these. The following pattern of auscultation is recommended:
1.Listen to the aortic area first and then the pulmonic. As the aortic and the pulmonic valves close, the dub should be louder than the lub in the aortic and pulmonic areas.
2.Listen to the tricuspid and mitral valves in the areas indicated. In these areas, the lub should be louder than the dub.
3.After listening to each area with the diaphragm, repeat the pattern with the bell of the stethoscope. Note additional sounds of S3 and S4. The S3 and S4 sounds are heard best with the bell of the stethoscope placed at the apex when the patient is positioned on the left side. S3, also called a ventricular gallop, occurs early in diastole. S3 is normal in

children and young adults and may be pathologic after age 30. S4, also called an atrial gallop, occurs late in diastole. S4 is an abnormal heart sound.
FIGURE 35-5 Auscultation of the heart. A, Aortic valve at the second intercostal space to the right of the sternum. B, Pulmonic valve at the second intercostal space to the left of the sternum. C, Tricuspid valve at the fifth intercostal space to the left of the sternum. D, Mitral valve at the fifth intercostal space in the midclavicular line.
Table 35-2 Grading of Heart Murmurs
GRADE DESCRIPTIONI Very faintII Faint, but recognizableIII Loud, but moderate in intensityIV Loud and accompanied by a palpable thrill
V Very loud, accompanied by a palpable thrill, and audible with the stethoscope partially off the client's chest
VI Extremely loud, may be heard with the stethoscope slightly above the client's chestFrom Ignatavicius, D.D., Workman, M.L., & Mishler, M.A. (1999).Medical-surgical nursing across the health care continuum (3rd ed., p. 735). Philadelphia: Saunders.
Heart Murmurs. A heart murmur is the sound produced by turbulent blood flow across the valves.
Murmurs are recorded as having high, low, or medium pitch, and they are located using the anatomic landmarks where they are heard best. The timing of a murmur relates to when it is heard in the cardiac cycle: systole or diastole. Murmurs are graded according to intensity or loudness (Table 35-2).
A rub is heard when the pericardium is inflamed. A scratchy or muffled sound may be heard best by having the patient sit upright and lean forward. This position brings the pericardium closer to the chest wall. A pericardial friction rub is best heard along the left sternal border throughout the cardiac cycle. It may help to ask patients to hold their breath briefly. If a rub is heard during this brief time, it is a pericardial rub rather than pleural.
Box 35-1 ASSESSMENT of Patients with Cardiac Disorders Health History Present Illness: Fatigue, edema, palpitations, pain; aggravating and relieving factors Past Medical History: Hypertension, kidney disease, pulmonary disease, diabetes mellitus, stroke, rheumatic
fever, streptococcal sore throat, scarlet fever, previous cardiac diseases or conditions, previous hospitalizations, recent and current medications, allergies
Family History: Hypertension, coronary artery disease or other cardiac conditions, diabetes mellitus Review of Systems: Weight gain, fatigue, dyspnea, cough, orthopnea, palpitations, chest pain, fainting,
concentrated urine, leg edema
Functional Assessment: Effects of illness on usual activities, activity and rest pattern, lifestyle, diet, sodium and
fat intake, sources of stress, coping strategies Physical Examination General Survey: Apparent distress Height and Weight Vital Signs: Blood pressure in both arms and while supine, sitting, standing; apical heart rate and
rhythm; peripheral pulses: rate, rhythm, quality, equality; respiratory effort and rate Skin: Color, hair distribution, capillary refill, temperature Thorax: Heart sounds, heart murmurs, rubs; breath sounds, crackles, wheezes; presence and
appearance of sputum Extremities: Pulses, color, warmth, edema, hair distribution Extremities Inspect and palpate the extremities for color, edema, warmth, temperature, pulse quality,
and hair distribution. Assessment of the cardiac patient is summarized in Box 35-1. DIAGNOSTIC TESTS AND PROCEDURES A number of tests or procedures may be employed to assess cardiac structure and
function. More common tests are described here. Patient preparation and postprocedure care are detailed in the Diagnostic Tests and Procedures table on pp. 635 and 636.
ELECTROCARDIOGRAM The electrocardiogram (ECG) allows study of the electrical activity (conduction system)
through the heart muscle. An electrical impulse causes contractions as it passes through the heart muscle. Electrodes placed on the surface of the skin pick up the electrical impulses of the heart. Moving electrodes to various positions permits detection of conduction disturbances in specific areas of the heart.
The ECG is graphed on standardized paper or viewed on an oscilloscope. Each cardiac cycle is represented by a series of P, Q, R, S, and T waves. The activity represented by each wave is explained in the Interpretation of Electrocardiograms section on pp. 673 to 675. The ECG is interpreted to detect abnormalities in rate, rhythm, or impulse conduction. The normal finding is called a normal sinus rhythm, which is characterized by the following:
1.A rate of 60 to 100 bpm 2.A regular rhythm 3.A P wave preceding each QRS complex 4.A PR interval that is within 0.12 to 0.20 second 5.A QRS complex that is 0.10 second or less
AMBULATORY ECG (HOLTER MONITOR)
An ambulatory ECG uses a portable ECG machine with a memory to provide continuous cardiac monitoring for 24 to 48 hours. A complete record of the heart rhythm is stored and analyzed later. This type of monitoring is used to detect dysrhythmias that occur infrequently, to determine if symptoms correlate with any underlying cardiac disease, to assess the effects of medications, and for research purposes. The patient records in a diary all activity that occurs during the monitoring, such as walking, stair climbing, sleeping, and engaging in sexual activity. The monitor strip is computer scanned and then interpreted by a physician.
Even more sophisticated monitoring is accomplished by transtelephonic means. An audio signal is sent over telephone lines to a station operated by personnel trained to recognize potentially dangerous dysrhythmias.
DIAGNOSTIC TESTS and PROCEDURES The Heart
TEST PURPOSE/PROCEDURE PATIENT PREPARATION
POSTPROCEDURE NURSING CARE
Electrocardiogram (ECG)
Electrodes are placed on the skin to detect electrical activity of the heart.
Detects abnormalities in conduction of impulses, including changes caused by heart damage.
Tell the patient what to expect and that the procedure is painless.
No special preparation is needed.
Remove gel from skin.
No special care needed.
Holter monitor
Provides continuous ECG monitoring for a 24-to-48–hour period.
Detects occasional dysrhythmias that may be correlated with specific activities noted in patient's diary.
Tell patient to wear loose clothing, take only sponge bath, avoid magnets and metal detectors, and monitor placement of electrodes.
Emphasize keeping accurate diary of activities and to push “event button” if symptoms occur.
Return at scheduled time. ECG recording will be retrieved for inspection.
Implantable loop recorder (ILR)
Provides ECG monitoring for longer time periods and saves on a memory loop for analysis.
Detects dysrhythmias causing syncopal episodes.
Tell patient/family member/significant other to activate recorder when symptoms occur and to keep a written record of events.
Return at scheduled time. ECG recording will be retrieved for inspection.
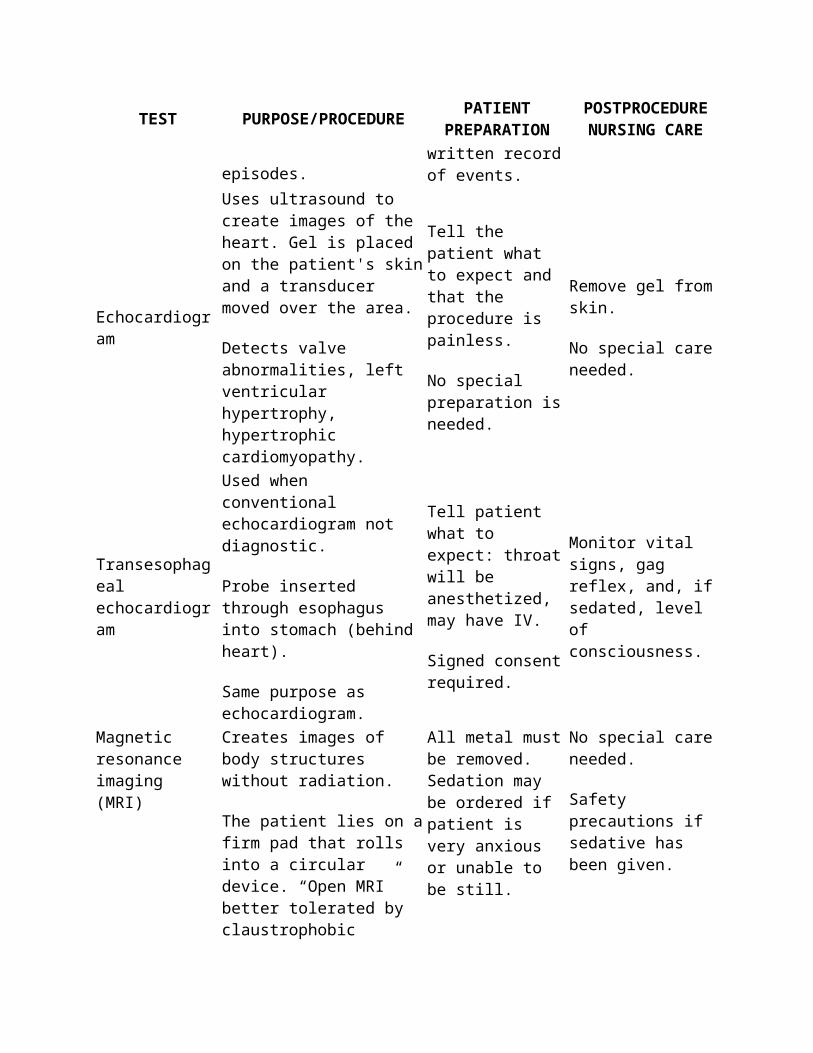
Echocardiogram Uses ultrasound to create images of the heart. Gel is placed on the patient's skin and
Tell the patient what to expect and that the
Remove gel from skin.
No special care needed.

TEST PURPOSE/PROCEDURE PATIENT PREPARATION
POSTPROCEDURE NURSING CARE
a transducer moved over the area.
Detects valve abnormalities, left ventricular hypertrophy, hypertrophic cardiomyopathy.
procedure is painless.
No special preparation is needed.
Transesophageal echocardiogram
Used when conventional echocardiogram not diagnostic.
Probe inserted through esophagus into stomach (behind heart).
Same purpose as echocardiogram.
Tell patient what to expect: throat will be anesthetized, may have IV.
Signed consent required.
Monitor vital signs, gag reflex, and, if sedated, level of consciousness.
Magnetic resonance imaging (MRI)
Creates images of body structures without radiation.
The patient lies on a firm pad that rolls into a circular device. “Open MRI” better tolerated by claustrophobic patients because machine does not surround patient.
Clanging sounds are heard as the machine works.
All metal must be removed. Sedation may be ordered if patient is very anxious or unable to be still.
No special care needed.
Safety precautions if sedative has been given.
Multiple-gated acquisition scanning
Radioactive material is injected intravenously and the heart scanned to evaluate function. May be done at rest or during exercise.
Tell patient what to expect.
Nothing by mouth (NPO) for 2 hr before procedure.
Start intravenous infusion as ordered. Signed consent required.
No special care needed.
Stress test (exercise tolerance test)
Assess presence and severity of coronary artery disease by having the patient exercise during ECG monitoring.
Blood pressure is monitored.
Tell the patient what to expect. NPO for 2 hr before test.
Give beta-blocker if
No special care needed.

TEST PURPOSE/PROCEDURE PATIENT PREPARATION
POSTPROCEDURE NURSING CARE
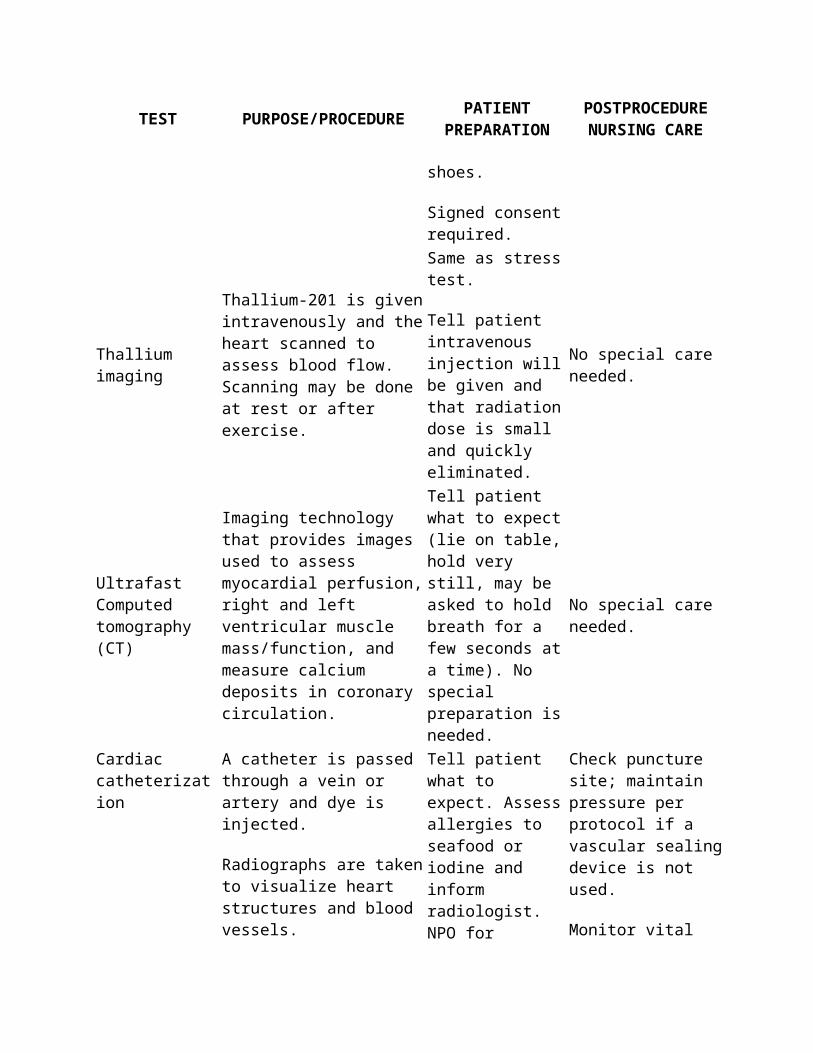
The test is stopped if symptoms of coronary artery disease occur.
prescribed.
Have patient wear loose clothing and comfortable shoes.
Signed consent required.
Thallium imaging
Thallium-201 is given intravenously and the heart scanned to assess blood flow. Scanning may be done at rest or after exercise.
Same as stress test.
Tell patient intravenous injection will be given and that radiation dose is small and quickly eliminated.
No special care needed.
Ultrafast Computed tomography (CT)
Imaging technology that provides images used to assess myocardial perfusion, right and left ventricular muscle mass/function, and measure calcium deposits in coronary circulation.
Tell patient what to expect (lie on table, hold very still, may be asked to hold breath for a few seconds at a time). No special preparation is needed.
No special care needed.
Cardiac catheterization
A catheter is passed through a vein or artery and dye is injected.
Radiographs are taken to visualize heart structures and blood vessels.
The procedure is done in a special room.
Blood pressure, pulse, and ECG are monitored throughout test.
Tell patient what to expect. Assess allergies to seafood or iodine and inform radiologist. NPO for specified time before procedure.
Tell patient to expect flushing sensation when dye is injected. Give sedative if ordered.
Signed consent required.
Check puncture site; maintain pressure per protocol if a vascular sealing device is not used.
Monitor vital signs and peripheral pulses on affected extremity.
Enforce bed rest as ordered.
Electrophysiology study (EPS)
A catheter with multiple electrodes is passed into the
Tell the patient what to expect. NPO for 6
Similar to cardiac catheterization

TEST PURPOSE/PROCEDURE PATIENT PREPARATION
POSTPROCEDURE NURSING CARE
right side of the heart through the femoral vein. The electrodes record electrical activity of the conduction system and may be used to stimulate the patient's dysrhythmia.
hr before procedure. Premedicate with prescribed sedatives.
Signed consent required.
(described above).
Arterial blood gases
Assesses acid-base balance by measuring pH, PCO2, PO2, HCO3
− and base excess.
Tell patient about arterial puncture.
Prepare heparinized syringe and obtain blood sample.
Remove air bubbles from sample. Place tube on ice and send for immediate analysis.
Apply pressure to puncture site for 5 min.
Report results.
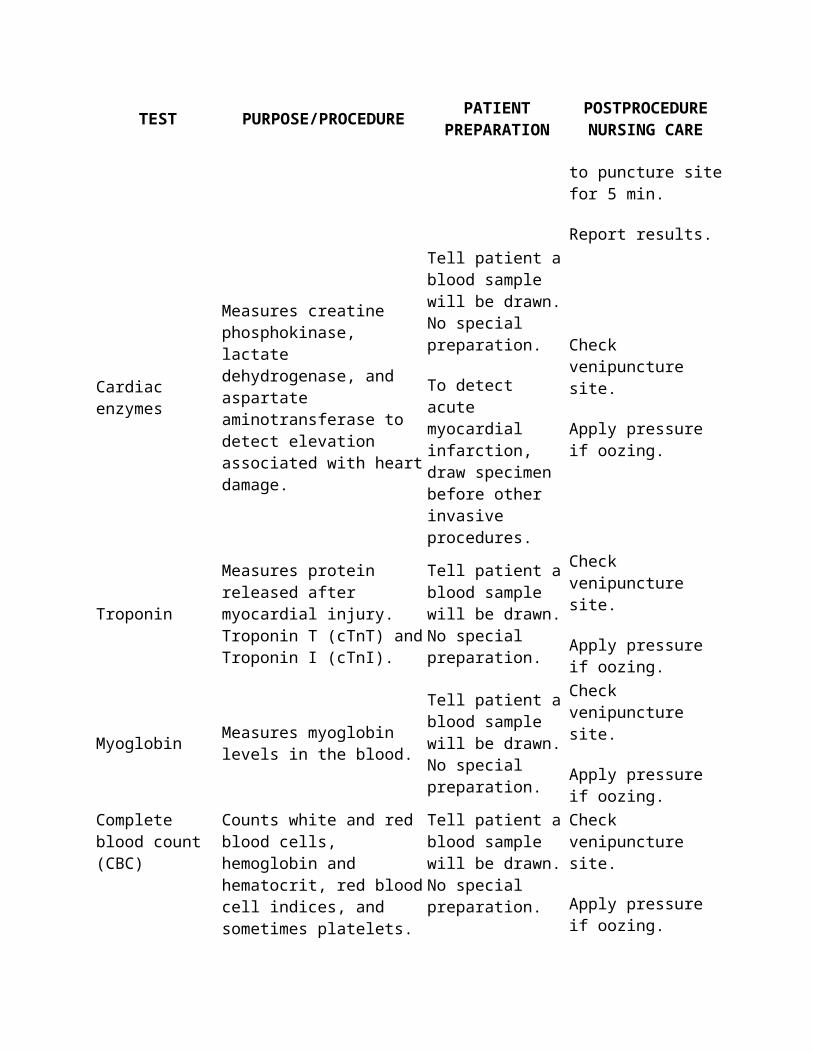
Cardiac enzymes
Measures creatine phosphokinase, lactate dehydrogenase, and aspartate aminotransferase to detect elevation associated with heart damage.
Tell patient a blood sample will be drawn. No special preparation.
To detect acute myocardial infarction, draw specimen before other invasive procedures.
Check venipuncture site.
Apply pressure if oozing.
TroponinMeasures protein released after myocardial injury. Troponin T (cTnT) and Troponin I (cTnI).
Tell patient a blood sample will be drawn. No special preparation.
Check venipuncture site.
Apply pressure if oozing.
Myoglobin Measures myoglobin levels in the blood.
Tell patient a blood sample will be drawn. No special preparation.
Check venipuncture site.
Apply pressure if oozing.
Complete blood count (CBC)
Counts white and red blood cells, hemoglobin and hematocrit, red blood cell indices, and sometimes platelets. (See Normal Values in Table 35-5.)
Tell patient a blood sample will be drawn. No special preparation.
Check venipuncture site.
Apply pressure if oozing.
Lipid profile Measures common serum Tell patient to expect Check venipuncture

TEST PURPOSE/PROCEDURE PATIENT PREPARATION
POSTPROCEDURE NURSING CARE
lipids (cholesterol, triglycerides, lipoproteins). Used to evaluate risk of coronary artery disease.
venipuncture. NPO for 12 hr before sample drawn. Usual diet for 2 weeks before test.
site.
Apply pressure if oozing.
B-type natriuretic peptide (BNP)
Measures naturally occurring BNP levels. Elevated in HF, CMP. Helps differentiate dyspnea related to cardiac problems from non–cardiac related dyspnea.
Tell patient a blood sample will be drawn.
No special preparation.
Check venipuncture site.
Apply pressure if oozing.
C-reactive protein (CRP)
Acute phase protein that is elevated in system inflammation. Elevated levels seen with ACS.
Tell patient a blood sample will be drawn. No special preparation.
Check venipuncture site.
Apply pressure if oozing.
ACS, Acute coronary syndrome; CMP, cardiomyopathy; HF, heart failure.IMPLANTABLE LOOP MONITOR/RECORDER
For longer monitoring time periods, to record a patient's ECG during syncopal episodes, an implantable loop monitor/recorder (ILR) may be used. This device, implanted just under the patient's skin in the chest area, continually monitors the ECG activity of the patient in a memory loop. The patient and/or family member/significant other is taught to activate the recorder when symptoms are felt. The ECG can then be analyzed and appropriate treatment implemented. The device can be used for up to 14 months, as needed (Morton, Tucker, & Van Roeden, 2005).
ECHOCARDIOGRAM (HEART SONOGRAM)
The echocardiogram visualizes and records the size, shape, position, and behavior of the heart's internal structures, especially the valves. Ultrasonic waves are beamed into the heart, and their echoes are recorded. This painless test may be performed at the bedside or in a laboratory. Gel is applied to the skin, and a special device called a transducer is moved over the precordium. The transducer picks up sound waves and converts them to electrical impulses that are recorded as waveforms on an oscilloscope, a videotape, or a strip chart. Common echocardiogram types include motion mode (M-mode) and two-dimensional mode (2-D mode). Echocardiograms can also be enhanced using Doppler technology (Doppler echocardiogram) and color-flow imaging.
TRANSESOPHAGEAL ECHOCARDIOGRAM
At times, the echocardiogram is not diagnostic and a transesophageal echocardiogram (TEE) is used. A flexible endoscopic probe with an ultrasound transducer is passed down the back of the throat into the esophagus. A local anesthetic to the throat decreases the gag reflex. Occasionally, an intravenous sedative is needed to reduce patient anxiety. Images are obtained from behind the heart as the probe moves down into the stomach. The probe is down for approximately 15 to 20

minutes. The TEE provides information useful in the evaluation of ventricular wall motion and function and possible heart valve disorders.
MAGNETIC RESONANCE IMAGING
A magnetic resonance imaging (MRI) scan provides high-resolution, three-dimensional images of body structures. Cardiac tissue is imaged without lung or bone interference. The patient is enclosed in a chamber for approximately 5 minutes for an MRI scan of the heart. No loose metallic objects are permitted in the chamber during the procedure. Patients with intracranial aneurysm clips, intraocular metal foreign bodies, heart valves manufactured before 1964, and some middle-ear prostheses should not have MRI scans because the devices may be affected by the magnetic field or may interfere with the MRI. Other implanted devices that contraindicate MRI include pacemakers, automatic implantable cardioverter-defibrillators (AICDs), and implanted infusion pumps. For patients who are claustrophobic, an open MRI may be available.
MULTIPLE-GATED ACQUISITION SCAN
In a multiple-gated acquisition scan (MUGA), the patient is injected with technetium 99m, which concentrates in acutely necrotic myocardial tissue. The heart is then scanned to assess left ventricular structure and function, to evaluate myocardial wall motion, to detect intracardiac shunting, to assess valvular disease, and to identify location and size of an acute myocardial infarction (AMI). Assessment of ventricular function can be done while the patient is resting or exercising. Sublingual nitroglycerin may be administered to assess its effect on ventricular function.
STRESS TEST (EXERCISE TOLERANCE TEST)
The stress test is a noninvasive method of assessing the presence and severity of CAD by recording a person's cardiovascular response to exercise. It is also used to measure functional capacity for work, sport, or participation in a rehabilitation program. The stress test is not flawless—false-positive and false-negative results are common. A negative test result does not absolutely exclude CAD. It is, however, the best noninvasive screening procedure available. The alternative is the much more invasive cardiac catheterization.
For the stress test, a continuous ECG is monitored while the patient uses a treadmill or a stationary bicycle. Every 2 to 3 minutes the speed and incline angle of the treadmill are increased (or pedal resistance is increased with a bicycle) until (1) the patient cannot continue for whatever reason, (2) the patient's maximum heart rate is achieved (220 2 patient's age 5 maximum heart rate), (3) symptoms intervene, or (4) significant changes are detected on the ECG. The target heart rate is 85% of the predicted maximum heart rate for the patient's age and gender.
Significant CAD limits blood flow to the myocardium. The increased demands of exercise may cause the patient to have symptoms of CAD, which are angina, dizziness, dyspnea, dysrhythmias, a falling blood pressure, and certain ECG findings. If these symptoms occur, the test must be stopped immediately.

Contraindications for the test include acute systemic illness, severe aortic stenosis, uncontrolled congestive heart failure (CHF), severe hypertension, angina at rest, and significant dysrhythmia. Although the mortality rate for test participants is very low, cardiopulmonary resuscitation equipment must be available.
PERFUSION IMAGING
Perfusion studies, performed most commonly in conjunction with exercise tolerance testing, provide information about the presence of coronary artery disease and the location and extent of ischemic and infarcted myocardium. There are several radioactive tracers approved for perfusion scanning. Thallium-201 is the most widely used over the years and will be addressed here.
Thallium Imaging
Thallium-201 may be administered to assess myocardial blood flow during stress testing. Thallium, which is taken up by normal myocardial cells, is used to detect old or new myocardial ischemia and to evaluate patency of coronary artery bypass grafts. After thallium-201 is injected intravenously, the heart is scanned to assess the areas of concentration. The scan takes approximately 1 hour to complete and is repeated in 2 to 4 hours to assess for redistribution.
Thallium does not enter infarcted or scarred areas and, therefore, shows “cold spots” in areas without blood flow. Exercise-induced ischemia resolves with rest. Scar-induced ischemia, such as that caused by AMI, does not resolve with rest.
For patients who are physically not able to exercise, the heart can be stressed with medications such as dipyridamole (Persantine). These medications mimic the effects of exercise by causing vasodilation of the coronary arteries, which increases blood flow to well-perfused areas, thereby stealing blood from ischemic areas. These differences in flow will show up on the scan.
ULTRAFAST COMPUTED TOMOGRAPHY
Ultrafast CT (also known as electron-beam CT or EBCT) is a fast form of imaging technology that allows for high-quality images not affected by the movement of the heart as it contracts and relaxes. The images obtained are used to assess myocardial perfusion, along with right and left ventricular muscle mass and function. In addition, Ultrafast CT can measure calcium deposits in the coronary arteries, and a coronary calcium score can be derived. The greater the amount of coronary calcium, the higher the score and the higher the risk of coronary occlusive disease. This procedure is not a substitute for cardiac catheterization (Morton, Tucker, & Van Roeden, 2005).
CARDIAC CATHETERIZATION (CARDIAC ANGIOGRAPHY, CORONARY ARTERIOGRAPHY)
Cardiac catheterization is a procedure in which a catheter is inserted into a vein or artery and is threaded into the heart chambers, coronary arteries, or both, under fluoroscopy (Fig. 35-6). A contrast dye is injected through the catheter, and films are made of the visualized heart structures. Vital signs and ECG are monitored during the procedure.
In a catheterization of the right side of the heart, the catheter is inserted into a vein and threaded into the vena cava, RA, RV, and pulmonary artery. Pressures in the RA, RV, and pulmonary artery may be determined. The function of the pulmonic and tricuspid valves may be assessed.
In a catheterization of the left side of the heart, the catheter is inserted into an artery and threaded against the flow of blood into the coronary arteries or the LV. The femoral vein and artery are the preferred insertion sites. The function of the coronary arteries and the aortic and mitral valves may be assessed. Blood samples may be drawn, and pressures in the various structures are measured.
Complications of cardiac catheterization include bleeding, hematoma formation, infection, and embolus or thrombus formation. Nursing care before and after the procedure is very important.
ELECTROPHYSIOLOGY STUDY
The electrophysiology study (EPS) is used to record the heart's electrical activity from within the heart using catheters with multiple electrodes inserted through the femoral vein into the right side of the heart. The electrodes record the electrical activity of the heart's conduction system. In addition, the electrodes can be used to stimulate dysrhythmias that will help locate the source of the patient's dysrhythmia.
LABORATORY TESTSArterial Blood Gases
Arterial blood gases are analyzed to determine the body's ability to maintain the acid-base balance. Acidity or alkalinity is determined by pH. If the serum pH is less than 7.35, the blood is acidic; greater than 7.45 indicates alkalinity. Carbonic acid dissociates into carbon dioxide and water. The lungs regulate carbon dioxide. The partial pressure of carbon dioxide in the blood is abbreviated Pco2. A Pco2 greater than 45 with an acidic pH is a respiratory acidosis and indicates that the body is unable to excrete the excess carbon dioxide through the lungs. With a pH in excess of 7.45 and a Pco2 of less than 35, a respiratory alkalosis is present.
The kidneys regulate bicarbonate (HCO32) through excretion and retention. The HCO3
2 (or base excess—a combination of all serum bases) is assessed to determine metabolic causes of imbalance. If the pH is less than 7.35 and the HCO3
2 is less than 22, the body is in metabolic acidosis. With a pH greater than 7.45 and an HCO3
2 greater than 26, the interpretation is metabolic alkalosis (Table 35-3).
Pulse Oximetry
Pulse oximetry, though not a laboratory test, noninvasively measures arterial oxygen saturation. Light is passed through a pulsating artery and interpreted mechanically to determine the oxygen saturation. The transdermal clip or patch may be applied to a digit (finger or toe), the ear, or the nose (Fig. 35-7).
FIGURE 35-6 Right-sided (A) and left-sided (B) heart catheterization.

Table 35-3 Interpreting Arterial Blood GasesCONDITION pH Pco2 HCO3
−
Normal range 7.35–7.45 35–45 22–26Respiratory acidosis ↓ ↑ NormalRespiratory alkalosis ↑ ↓ NormalMetabolic acidosis ↓ Normal ↓Metabolic alkalosis ↑ Normal ↑↑, Elevated; ↓, decreased. If the arrows are in the same direction, a metabolic problem exists. If arrows are in opposite directions, a respiratory problem exists.Cardiac Enzymes
Cardiac enzymes are released when heart cells die as a result of damage. These enzymes are measured in the serum, and their values rise as indicators of damage to the heart cells. Table 35-4 lists normal cardiac enzyme levels.
Creatine Phosphokinase.
The creatine phosphokinase enzyme is found in high concentration in three tissues: the brain, the heart, and the skeletal muscle. The type of creatine phosphokinase (CPK) specific to heart tissue is CPK-MB. Elevation of the CPK-MB level indicates damage to the myocardial cells. The CPK-MB can be expected to rise 4 to 6 hours after an AMI, peak in 12 to 24 hours at more than 6 times the normal value, and return to normal within 2 to 3 days if no new damage occurs. Serial trends should be observed. The nurse can plot these trends. Musculo-skeletal injuries (especially fractures and surgery) and recent excessive athletic activity can also elevate the total CPK level.
FIGURE 35-7 Pulse oximeter. A, Ear probe. B, Clip on finger.Table 35-4 Cardiac Enzymes and Markers
TEST* NORMAL VALUES
Creatine Phosphokinase (CPK)Male: 55–170 U/LFemale: 96–140 U/L
CPK IsoenzymesMM: 100%MB: 0%BB: 0%
Troponin T (cTnT) <0.1 ng/mLTroponin I (cTnI) <0.3 ng/mLMyoglobin Male: <92 ng/mL
Female: <76 ng/mL
Cardiac Protein MarkersTroponin.
Troponin is a protein involved in the contraction of muscles. Two subtypes, troponin T (cTnT) and troponin I (cTnI) are specific to cardiac muscle and are released into the circulation after an acute myocardial infarction. Troponin levels, generally not detectable in healthy individuals, will elevate significantly after an acute myocardial infarction. Levels may elevate slightly as a result of lesser insults, such as an episode of angina. Troponin levels rise in 3 to 6 hours from onset of symptoms, peak in 24 hours, and remain in the circulation for up to 2 weeks. This test is done in the emergency department because the results are available more quickly than the cardiac enzymes.
Myoglobin.
Myoglobin is another protein found in cardiac and skeletal muscle that is released into the circulation very quickly after myocardial infarction. Myoglobin levels increase in 1 to 4 hours after symptoms. Because it is found also in skeletal muscle, myoglobin levels may be elevated by such things as strenuous exercise, renal failure, and neuromuscular diseases. This makes interpreting myoglobin levels difficult in some circumstances.
Complete Blood Count
The complete blood count is a basic screening test. Included in this test are the white blood cell (WBC) count, the red blood cell (RBC) count, the hemoglobin (Hgb) and hematocrit (Hct) measurements, the RBC indices, and, in some laboratories, the platelet count. Components of the complete blood count are presented in Table 35-5.
White Blood Cell Count.
The WBC count indicates the body's ability to defend itself against infection and inflammation. The WBC level usually is elevated with inflammatory processes such as AMI and bacterial infections, but it may be below normal with viral infections and bone marrow depression.
Red Blood Cell Count.
The RBC count is assessed to determine the ability of the blood to carry oxygen from the lungs to the tissues and carbon dioxide from the tissues to the lungs. The RBC level may be below normal with anemias and malignancies and may be elevated in dehydration.
Table 35-5 Complete Blood CountTEST* NORMAL VALUES
White Blood Cells: 5,000–10,000/mm3
Differential:Neutrophils 60%–70%Eosinophils 1%–4%Basophils 0.5%–1.0%Lymphocytes 20%–40%Monocytes 2%–6%

TEST* NORMAL VALUESRed Blood Cells:Male 4,200,000–5,400,000/mm3
Female 3,600,000–5,000,000/mm3
Hematocrit:Male 40%–54%Female 37%–47%
Hemoglobin:Male 13.5–17.5 g/dLFemale 12–16 g/dL
Platelets 150,000–350,000/mm3
Hematocrit.
The hematocrit is the percentage of packed RBCs in the total sample of whole blood. With severe dehydration, the plasma portion of the blood decreases and the Hct is elevated. In anemias and hemorrhage, the Hct is below normal. In general, the Hct is three times the Hgb measurement.
Hemoglobin.
Hemoglobin is the main component of the RBCs. Its function is to transport oxygen to the cells. The Hgb measurement may be below normal in anemias and hemorrhage. It is elevated in dehydration, chronic obstructive pulmonary disease (COPD), and CHF. An Hgb of less than 5 g/dL leads to heart failure and death if not corrected.
Platelet (Thrombocyte) Count.
The platelets (thrombocytes) are the smallest of the formed elements in the blood. They are necessary for coagulation. The platelet count is below normal with anemias, bone marrow depression, and bleeding. The count may be increased in acute infections and some heart diseases. A count of less than 20,000 may result in spontaneous bleeding.
Lipid Profile
A lipid profile is a battery of tests that measure the most common serum lipids: cholesterol, triglycerides, and lipoproteins.
Cholesterol is a blood lipid produced by the liver. It is used to form bile salts for the digestion of fat and for the production of adrenal, ovarian, and testicular hormones. The normal adult serum cholesterol level is less than 200 mg/dL. Elevated cholesterol levels (hypercholesterolemia) are associated with increased risk of CAD, hypertension, and AMI. The cholesterol accumulates in the arterial lumen and in time results in decreased blood flow and occlusion.
Several forms of cholesterol are identified; however, the high-density lipoproteins (HDLs) and the low-density lipoproteins (LDLs) are the two that most closely correlate with coronary artery disease. The HDLs are desirable because they promote the excretion of cholesterol; therefore higher levels of HDLs are encouraged. On the other hand, elevated LDL levels are associated with a higher risk of CAD; therefore lower LDL levels are encouraged. A good way to remember the difference is that HDLs are healthy and LDLs are lethal. Currently, the recommendations are for HDL levels greater than 40 mg/dL and for LDL levels less than 100 mg/dL (American Heart Association, 2007). See the Health Promotion Considerations box above for advice about increasing HDL levels.
Triglycerides are a major contributor to CAD. They are produced in the liver. Triglyceride levels increase when LDL levels increase. The normal triglyceride level is less than 150 mg/dL.
Health Promotion ConsiderationsLow HDL Levels
Low HDL levels can be raised by being physically active at least 30 minutes every day, by not smoking, and by losing weight (or maintaining a healthy weight).
B-type Natriuretic Peptide
B-type natriuretic peptide (BNP) is a cardiac hormone released when there is ventricular dilation and stretch (such as occurs in heart failure). Less than 100 pg/mL is considered a normal BNP level, and elevated levels relate closely to the severity of heart failure (e.g., the higher the levels, the more severe the failure). In addition, BNP levels can be monitored to assess the effectiveness of treatment.
C-reactive Protein
C-reactive protein (CRP) is an acute-phase protein and a marker for systemic inflammation. Elevated levels of CRP are present in patients with acute coronary syndromes. CRP is being studied to determine its usefulness in predicting recurrent and new cardiovascular events.
COMMON THERAPEUTIC MEASURESDRUG THERAPY
Commonly used cardiac drugs are cardiac glycosides, antianginals, antidysrhythmics, and miscellaneous and emergency drugs. Examples of these drugs, their actions and adverse effects, and associated nursing considerations are provided in the Drug Therapy table on pp. 642 to 646.
Cardiac Glycosides
The cardiac glycosides are also called cardiotonics or digitalis glycosides. Examples are digoxin (Lanoxin) and digitoxin. These drugs have several important pharmacologic actions on the heart. They slow the heart rate (negative chronotropic effect) and increase the force of myocardial contraction (positive inotropic effect), causing increased stroke volume and cardiac output.

Cardiac glycosides are widely used in the treatment of heart failure (HF). They are also used to treat some cardiac dysrhythmias.
When rapid effects are needed, a patient can be given a loading dose (called a digitalizing dose) of cardiac glycosides. Once therapeutic blood levels are obtained, a maintenance dose is prescribed to maintain the therapeutic effects. These drugs have high potential for toxicity and require close monitoring. Common practice is to count the apical pulse before giving each dose. If the rate is below 60 bpm in adults, withhold the dose and contact the physician. Because patients are often on cardiac glycosides for long-term therapy, they must be taught to monitor their own pulse and to report symptoms of toxicity (anorexia, nausea, visual disturbances). Other specific nursing considerations are presented in the Drug Therapy table on p. 642.
Antianginals
Drugs used to treat angina (chest pain related to myocardial ischemia) include nitrates, beta-adrenergic blockers, and calcium channel blockers. Nitrates are used to treat actual anginal episodes and to prevent angina. Beta-adrenergic blockers and calcium channel blockers are used in the long-term management of angina. Examples of each classification and nursing considerations are presented in the Drug Therapy table on pp. 642 and 643.
Antidysrhythmics
Drugs used to treat abnormal cardiac rhythms are called antidysrhythmics or antiarrhythmics. There are four main classes of antidysrhythmics, each with various actions. In general, they work by slowing the rate of impulse conduction, depressing automaticity, or increasing resistance to premature stimulation. All antidysrhythmics have the potential to cause additional dysrhythmias. Specific drugs and nursing considerations are presented in the Drug Therapy table on pp. 644 and 645.
Angiotensin-Converting Enzyme Inhibitors
Angiotensin-converting enzyme (ACE) inhibitors (ACEI) work against the renin-angiotensin-aldosterone system to dilate arteries and decrease the resistance to blood flow in the arteries (reduced afterload). In addition, less fluid is retained because aldosterone release is blocked. ACE inhibitors are prescribed for patients with heart failure, some cases of hypertension, and in some cases after myocardial infarction Examples of these medications are captopril (Capoten), enalapril (Vasotec), and quinapril (Accupril). Information about these medications is presented in the Drug Therapy table on p. 721.
DRUG THERAPY Cardiovascular DrugsDRUG USE/ACTION NURSING INTERVENTIONS
CARDIAC GLYCOSIDES Digoxin (Lanoxin) Delays impulse conduction through
AV node to slow heart rate (negative chronotropic effect). Increases strength or force of myocardial
Obtain baseline vital signs, ECG, and electrolytes before administering first dose. Assess apical pulse for 1 min; hold and notify physician if <60.

DRUG USE/ACTION NURSING INTERVENTIONS
contraction (positive inotropic effect). Increases stroke volume and CO. Used for HF, atrial fibrillation and flutter, and paroxysmal atrial tachycardia.
Cannot be administered intramuscularly. Monitor K+ levels; administer K+ supplements as ordered. Decreased renal function may delay excretion and lead to toxicity. Toxic effects may be indicated by dysrhythmias, pulse <60, anorexia, nausea, syncope, visual disturbances, and abdominal pain.
Therapeutic level: 0.8–2.0 ng/mL.
Toxic level: >2.0 ng/mL.
Teach the patient:
• Take radial pulse for 1 min at the same time each day.
ANTIANGINALS Nitroglycerin
Available as sublingual tablets, ointment, transdermal patch, buccal tablets, mist, and sustained-release oral tablets
Vasodilator (arteries and veins). Relaxes all smooth muscles, especially vascular smooth muscle. Decreases preload, afterload, BP, CO, and systemic vascular resistance. Used to prevent and treat angina.
Assess BP and pulse before administration. Apply ointment in uniform layer on paper provided; apply to nonhairy skin (chest, back, upper arm); do not touch (causes headache); rotate sites.
IV drug is delivered in glass containers with special tubing; use an infusion pump; monitor closely.
Teach the patient:
• Sit or lie down at onset of chest pain.
• Place tablet under tongue; tablet causes tingling sensation if effective (older adults may not detect this).
• Repeat q 5 min for total of three doses; if chest pains not relieved, have someone else drive to emergency department.
• Keep tablets in containers in which
DRUG USE/ACTION NURSING INTERVENTIONS
supplied; drug decomposes on exposure to light and air.
• Headache decreases with tolerance.
• Drug may be taken before activities likely to cause angina (exercise, sex).
Isosorbide dinitrate (Isordil)
Vasodilator that works by relaxing smooth muscles. Decreases preload, afterload, left ventricular end-diastolic pressure, and myocardial oxygen consumption. Used for acute angina and maintenance of chronic angina.
Assess vital signs before administration. Teach the patient:
• Take 1-2 hr before meals and at bedtime.
• Sit when taking the sublingual or chewable medications.
• Change positions slowly to avoid orthostatic hypotension.
• Avoid hot showers, tubs, saunas.
• Headache decreases over time.
• Alcohol potentiates hypotension.
• If three sublingual or chewable doses do not relieve angina, go to the emergency department.
Nadolol (Corgard) Beta-adrenergic blocker. Decreases HR and CO at rest and with exercise.
Assess BP and apical pulse before administration.
Dosage increased gradually until optimal response is achieved
Decreases conduction velocity through the AV node. Used in hypertension and prophylactically for chronic stable angina.
Monitor weight (fluid retention with HF). Teach the patient:
• Take radial pulse for 1 min.
• Hold medication and notify physician if HR
• Weigh daily; report a gain of 3-4 lb.
• Do not discontinue this drug abruptly; taper off over 1-2 weeks.
Propranolol (Inderal) Nonselective beta-adrenergic Monitor vital signs. May be

DRUG USE/ACTION NURSING INTERVENTIONS
blocker. Decreases HR, myocardial irritability, and contractibility. Decreases BP in hypertension. Decreases CO. Used in dysrhythmia, myocardial infarction, hypertension, migraines, and chronic stable angina.
administered with diuretic to decrease Na+ and water retention. May cause bronchial constriction. Use with caution in all patients with obstructive lung disease. Auscultate lungs for crackles and heart for S3 and S4. Monitor weight daily; check for peripheral edema. Monitor blood glucose with diabetes.
Teach the patient:
• Do not discontinue this drug abruptly; taper over 2 weeks.
• Take at the same time(s) each day.
• While on this drug, use alcohol only in moderation; no smoking; decrease sodium intake.
• There is not the normal increase in heart rate with exercise and stress; increase activity slowly.
• Weigh daily; check for edema.
Atenolol (Tenormin) and metoprolol tartrate (Lopressor)
Cardioselective beta-adrenergic blockers used to treat angina and hypertension.
Reduce heart rate, BP, cardiac output, and myocardial oxygen consumption.
Monitor vital signs. Continuous ECG monitoring with IV administration. Take apical pulse before each dose.
Teach the patient:
• Take with or after meals.
• Do not discontinue abruptly.
• Take pulse and report to physician if below 60
• Avoid alcohol and smoking.
• Avoid over-the-counter cold remedies.
Diltiazem hydrochloride
Calcium channel blocker. Dilates coronary arteries; increases
Dosage may need to be reduced in
DRUG USE/ACTION NURSING INTERVENTIONS
(Cardizem)
availability of oxygen to the myocardium. Decreases total PVR, afterload, and systolic blood pressure. Slightly decreases myocardial contractility. Prolongs AV node refractory period. Used in chronic stable angina, coronary artery spasm, and hypertension.
older adult patients.
Teach the patient:
• Take radial pulse for 1 min.
• Limit caffeine intake.
• Change positions with caution to prevent postural hypotension.
• Take before meals and at bedtime.
Nifedipine (Procardia)
Calcium channel blocker. Decreases myocardial oxygen consumption. Dilates coronary arteries. Decreases PVR. Increases CO. Used for angina, mild to moderate hypertension, vascular headaches, coronary artery spasms.
Monitor BP during titration (during dosage adjustment).
Teach the patient:
• Smoking is contraindicated (nicotine constricts coronary arteries).
• Do not discontinue this drug abruptly.
• Limit caffeine intake.
Verapamil hydrochloride (Calan, Isoptin)
Calcium channel blocker. Slows AV conduction. Dilates peripheral and coronary arteries. Increases oxygen supply to myocardium. Used to treat supraventricular tachycardias, atrial fibrillation and flutter, angina, hypertension, and vascular headaches.
Assess baseline vital signs, hepatic and renal function. Assess for signs of CHF (pulmonary or peripheral edema). Monitor pulse and BP before each dose. Administer IV bolus more slowly to older adults.
Teach the patient:
• Take radial pulse for 1 min; report irregular or slow pulse.
• No caffeine (opposes calcium channel–blocking effect).
• Change position slowly until tolerance develops.
• Exercise with caution; drug's effects may give false impression of tolerance.

DRUG USE/ACTION NURSING INTERVENTIONSANTIDYSRHYTHMICS
Amiodarone hydrochloride (Cordarone)
Antidysrhythmic. Increases action potential duration and effective refractory period. Increases CO. Decreases PVR, coronary artery resistance, and HR. Used for severe tachycardia and supraventricular tachycardias.
Continuously monitor ECG for a decrease in dysrhythmia. Observe for thyroid dysfunction (each 200-mg tablet contains 75 mg of iodine) and neurologic effects (tremors, ataxia, headache, insomnia).
Teach the patient:
• Take radial pulse daily.
• Photosensitivity and photophobia may occur.
• Pharmacologic action may have a delayed onset of 5 days to 3 mo.
• Skin discolorations fade with time.
Bretylium tosylate (Bretylol)
Adrenergic blocker. Suppresses ventricular fibrillation and ventricular tachycardia. Used for short-time treatment of life-threatening ventricular tachycardias in patients who do not respond to conventional therapy, ventricular fibrillation, and cardioversion.
Monitor vital signs, ECG.
Have resuscitation equipment available.
If nausea and vomiting occur, decrease the rate of infusion.
Disopyramide phosphate (Norpace)
Reduces the rate of spontaneous diastolic depolarization in pacemaker cells.
Increases SVR. Decreases myocardial conductivity. Suppresses ectopic focal activity. Used to suppress and prevent recurrent PVCs and ventricular tachycardia.
Assess apical pulse before administration; hold if <60 or >120 and notify physician. Monitor BP. Monitor intake and output. Urinary retention and constipation may occur.
Teach the patient:
• Take radial pulse daily.
• Weigh daily; observe for edema.
• Change position slowly.
• No alcohol (severely decreases BP).
• Relieve dry mouth with sugarless

DRUG USE/ACTION NURSING INTERVENTIONS
gum or dry candy.
• Avoid sunlight (photosensitivity).
Flecainide acetate (Tambocor)
Antidysrhythmic. Decreases conduction velocity. Increases ventricular refractory period. Used to treat PVCs, atrial tachycardia, and other dysrhythmias not responsive to other antidysrhythmics.
Monitor ECG.
Lidocaine (Xylocaine)
Increases the electrical stimulation threshold of the ventricular conduction system. Used for rapid control of ventricular dysrhythmias during myocardial infarction, cardiac surgery, cardiac catheterization, and digitalis intoxication.
Administer with an infusion pump.
Monitor BP and ECG. May precipitate malignant hyperthermia (tachycardia, tachypnea, elevated temperature). Assess breath sounds for crackles.
Mexiletine hydrochloride (Mexitil)
Antidysrhythmic structurally similar to lidocaine. Used to suppress symptomatic ventricular dysrhythmias.
Administer with food or antacids.
Monitor ECG.
Mix IV solution immediately before administration.
Phenytoin sodium (Dilantin)
Used to treat paroxysmal atrial tachycardia and ventricular dysrhythmias.
May need lower dosage in older adults.
Administer only in normal saline (drug crystallizes in dextrose). Do not exceed 50 mg/min IV.
Teach the patient:
• Alcohol potentiates the action and therefore may precipitate toxicity.
Propranolol (Inderal) See description under Antianginals.
Quinidine
Antidysrhythmic. Depresses myocardial excitability, contractility, automaticity, and conduction velocity. Anticholinergic effects increase the ventricular rate.
Relaxes muscles. Used for atrial and ventricular dysrhythmias.
If administered with digoxin, may produce toxicity or unpredictable dysrhythmias. Administer with meals to decrease gastric distress. Severe hypotension may occur with large doses. Monitor electrolytes; continuing diarrhea may indicate electrolyte imbalance.
Tocainide Antidysrhythmic. Primary analogue Monitor ECG. Administer with food

DRUG USE/ACTION NURSING INTERVENTIONS
hydrochloride (Tonocard)
of lidocaine. Used for life-threatening ventricular dysrhythmias associated with prolonged QT interval.
or antacids to decrease gastro-intestinal side effects. Monitor CBC for blood dyscrasias (agranulocytosis, leukocytosis, neutropenia).
Verapamil (Calan, Isoptin) See description under Antianginals.
ANTIPLATELET AGENTS
Clopidogrel (Plavix)
Decreases platelet aggregation. Prolongs bleeding time. Used to prevent thromboembolic disorders such as stroke and MI.
Monitor bleeding time, CBC with differential, platelet count. Avoid OTC medications with aspirin or NSAIDs unless prescribed by physician.
Teach the patient:
• Report bleeding.
• Keep appointments for blood work.
Ticlopidine (Ticlid) Same as Plavix.
Monitor liver function studies, CBC, prothrombin time.
Teach the patient:
• Report bleeding.
• Take with food.
• Keep appointments for blood work.
Abciximab (ReoPro)
Inhibits platelet aggregation.
Given IV to reduce ischemic complications with angioplasty or arthrectomy.
Used only in the hospital. Monitor vital signs, ECG, and level of consciousness. Assess hemoglobin, hematocrit, platelet count, and clotting factors frequently.
Watch for bleeding. Protect from trauma.
LIPID-LOWERING AGENTS Cholestyramine (Questran)
Prescribed when diet, exercise, and weight loss fail to bring cholesterol levels under control. Lowers LDL cholesterol. Increases HDL cholesterol.
Interferes with absorption of some other drugs, so check drug-drug interactions before giving.
To get the best effect, teach patients:

DRUG USE/ACTION NURSING INTERVENTIONS
• Continue diet and exercise.
• Increase fluid intake to counter constipating effects.
Gemfibrozil (Lopid)Decreases synthesis and secretion of VLDL by liver. Decreases triglyceride levels.
For best effect, teach patient:
• Continue diet and exercise.
• Take with meals.
Nicotinic acid (niacin)
Decreases synthesis/secretion of VLDL and LDL by liver. Increases HDL.
For best effect, teach patient:
• Continue diet and exercise.
• Take with meals to decrease GI side effects.
Pravastatin (Pravachol)
Simvastatin (Zocor)
Lovastatin (Mevacor)
Atorvastatin (Lipitor)
Increases rate of removal of LDL from plasma. Decreases synthesis of LDL.
Monitor liver function tests.
For best effect, teach patient:
• Continue diet and exercise.
• Report muscle tenderness.
• Take as single dose in the evening.
• Have routine eye examinations.MISCELLANEOUS AND EMERGENCY DRUGS
Amrinone lactate (Inocor)
Inotropic agent. Vasodilator. Increases myocardial contractions without increasing HR. Increases blood flow through collateral coronary vessels. Increases stroke volume and CO. Decreases preload and afterload. Used to treat HF refractory to other medications.
Administer with an infusion pump. Titrate to target BP. Monitor intake and output. Avoid extravasation. Discard solution 24 hr after preparation.
Atropine sulfate
Vagal blocker. Increases HR and CO in heart blocks and severe bradycardia. Used in symptomatic bradycardia and bradydysrhythmias.
Assess HR and rhythm and BP.
Calcium chloride Necessary for cardiac rhythm, tone, and contraction. Increases muscle tone and force of contraction. Used in cardiac resuscitation and in
Monitor ECG, BP, and arterial blood gases. Avoid extravasation; causes necrosis. Alkalosis decreases the absorption of calcium. Acidosis

DRUG USE/ACTION NURSING INTERVENTIONScardiac irregularities associated with hyperkalemia. increases the absorption of calcium.
Dobutamine (Dobutrex)
Synthetic catecholamine. Beta-adrenergic agonist. Increases CO with less increase in HR and BP than other catecholamines. Used in CHF and after cardiac surgery to increase myocardial contractility, stroke volume, and CO.
Continuous monitoring of ECG, cardiac parameters, and urinary output; titrate to HR and BP. Urinary output should increase with improved CO and renal function. Often used with nitroprusside or dopamine for additive effects. Causes less increase in HR, PVR, and dysrhythmias than dopamine. At a rate <7 mcg/kg/min, expect increased myocardial contraction, CO, and renal blood flow. At a rate of >7 mcg/kg/min, expect peripheral vasoconstriction and increased MAP.
Dopamine hydrochloride (Intropin)
Neurotransmitter, precursor to norepinephrine. Increases CO and BP. Improves renal blood flow and therefore urine output with lower doses. Used for hemodynamic support in shock.
Avoid extravasation; causes necrosis. Monitor vital signs, ECG, urine output, and extremity color. Titrate to target BP; use an infusion pump. Peripheral vasoconstriction is noted with cold upper and lower extremities.
Epinephrine hydrochloride (Adrenalin chloride)
Catecholamine. Strengthens myocardial contraction; increases BP, HR, and CO. Dilates bronchial tree. Used in anaphylactic shock and to restore cardiac rhythm in cardiac arrest.
Monitor vital signs and ECG continuously. Avoid extravasation; causes sloughing. Titrate to cardiac response. Caution: available in several concentrations (1:100, 1:1000, 1:10,000); be sure to check for prescribed solution. May be administered by endotracheal tube because drug is rapidly absorbed from the lungs.
Isoproterenol hydrochloride (Isuprel)
Cardiac stimulant (positive inotropic and chronotropic effects). Bronchodilator. Peripheral vasodilator. Increases HR and contractility. Decreases PVR and diastolic BP, resulting in increased CO and systolic BP, decreased MAP, and increased myocardial oxygen consumption. Used as a cardiac stimulant in cardiac arrest, cardiogenic shock, ventricular
Continuously monitor ECG. Monitor vital signs, urine output, and peripheral blood flow. Titrate to desired HR, BP, and urine output. Avoid extravasation.
DRUG USE/ACTION NURSING INTERVENTIONSdysrhythmias, and heart block.
Sodium nitroprusside (Nipride)
Vasodilator. Decreases preload and afterload. Used in hypertensive crises.
Light-sensitive preparation; wrap in aluminum foil. Administer with an infusion pump. Titrate to maintain CO. Continuously monitor BP. Discard solution 4 hr after preparation. Assess thiocyanate levels daily for patients on long-term therapy.
Norepinephrine (Levophed)
Catecholamine. Vasoconstrictor. Cardiac stimulant: increased BP, myocardial oxygen, and coronary artery blood flow. Used in acute hypertensive states, myocardial infarction, and cardiac arrest.
Mix only with dextrose in water or dextrose in saline. Administer with an infusion pump. Report decreased urine output immediately. Continuously monitor and titrate to desired BP. Monitor peripheral blood flow. Avoid extravasation.
Sodium bicarbonate Systemic alkalinizer. Used to correct metabolic acidosis in cardiac arrest.
Do not infuse with calcium. Monitor arterial blood gases. Avoid extra-vasation; causes severe tissue damage.
Milrinone (Primacor)
Inotropic agent. Increases myocardial contractility and cardiac output.
Vasodilation decreases preload and afterload. Used to treat CHF that does not respond to usual therapy.
Monitor vital signs, intake and output, and daily weight during therapy.
Monitor ECG continuously. Give potassium as ordered for hypokalemia.
AV, Atrioventricular; BP, blood pressure; CBC, complete blood count; CHF, congestive heart failure; CO, cardiac output; ECG, electrocardiogram; HDL, high-density lipoprotein; HF, heart failure; HR, heart rate; IV, intravenous; LDL, low-density lipoprotein; MAP, mean arterial pressure; NSAID, nonsteroidal anti-inflammatory drug; OTC, over-the-counter; PVC, premature ventricular contraction, PVR, peripheral vascular resistance; SVR, systemic vascular resistance; VLDL, very-low-density lipoprotein.Diuretics
Diuretics are often prescribed for cardiac conditions. Many patients with heart problems have fluid retention that is treated with diuretics. The most frequently used diuretics are the loop diuretics such as furosemide (Lasix), the thiazide diuretics such as hydrochlorothiazide (Esidrix, HCTZ) and the potassium-sparing diuretics such as spironolactone (Aldactone). Information about these and other diuretics is presented in the Drug Therapy table on p. 850.
Anticoagulants

Anticoagulants are used to prevent clot formation. Heparin, low-molecular-weight heparin (LMWH), and warfarin are the most commonly used preventive anticoagulants.
Heparin
Heparin interferes with factor III in the clotting process. It is administered by continuous intravenous drip or subcutaneously. When a patient has a clotting episode, a heparin bolus is administered and a continuous infusion is started. The infusion rate is set to deliver a prescribed number of heparin units per hour. The physician adjusts the heparin dosage based on the activated partial thromboplastin time (aPTT). When the aPTT has stabilized (generally at 1.5 to 2.0 times the control level), the drug can be changed to the subcutaneous route. Because heparin cannot be administered orally, the patient must remain hospitalized during its administration. Heparin is recommended for use with acute coronary syndrome (ACS), during percutaneous coronary interventions (PCI) and surgical revascularization, and in conjunction with fibrinolytic therapy (Ante, 2004; Deglin & Vallerand, 2005).
Low-Molecular-Weight Heparin.
Low-molecular-weight heparins (LMWHs), such as enoxaparin (Lovenox), are fragments derived from heparin that work by blocking the formation of thrombin and preventing the development of a clot. The advantages of using LMWHs are that the anticoagulant effect is more predictable, they are administered subcutaneously once or twice a day, and they do not require such close monitoring of aPTT. LMWHs are recommended for patients with deep vein thrombosis, with unstable angina, and in some cases of acute myocardial infarction (before a thrombus occludes the coronary vessel) (Ante, 2004; Deglin & Vallerand, 2005).
Warfarin
The anticoagulant that may be administered orally, warfarin (Coumadin), is started as soon as possible. The warfarin dosage is regulated by the prothrombin time and international normalized ratio (INR). The prothrombin time is kept in a therapeutic range of 1.5 to 2.0 times the normal level. The INR may be kept at 2.0 to 4.5. Patients who have had artificial valve replacements must remain on anticoagulant therapy for life.
All patients on anticoagulants must be monitored closely for any signs of bleeding. Also, patients should be taught how to reduce the risk of bleeding, such as to use an electric razor and a soft-bristle toothbrush.
Pharmacology Capsule
Heparin dosage is adjusted based on the patient's activated partial thromboplastin time (aPTT). Warfarin dosage is adjusted based on the patient's prothrombin time (PT) and international normalized ratio (INR).
Antiplatelet Agents

Antiplatelet therapy is often used after an AMI to prevent additional myocardial infarction and strokes. The dosage of aspirin as an antiplatelet agent in stroke prevention is under investigation. Some studies have shown that one baby aspirin (81 mg) a day is sufficient, and other studies indicate that an even smaller dosage may produce a therapeutic effect. Dipyridamole (Persantine), ticlopidine (Ticlid), and clopidogrel (Plavix) also exhibit antiplatelet effects and may be prescribed for patients who are unable to tolerate aspirin.
Glycoprotein (GP) IIb/IIIa inhibitors block the platelet receptor sites that bind with fibrinogen and lead to platelet aggregation. GP IIb/IIIa inhibitors such as abciximab (ReoPro) and eptifibatide (Integrilin) are used in combination with heparin and aspirin as part of the medical treatment for unstable angina and acute myocardial infarction. They are also being used in conjunction with fibrinolytic therapy and/or percutaneous coronary interventions after acute myocardial infarction.
Pharmacology Capsule
Anticoagulants and antiplatelet agents prevent formation of new clots, but fibrinolytic agents destroy clots that have already formed.
Fibrinolytic Agents
Whereas anticoagulants and antiplatelet agents prevent the continued formation of clots, the fibrinolytic agents (also called thrombolytics) act to destroy clots that have already formed. Streptokinase, Reteplase, and tissue plasminogen activator are examples of thrombolytics. They are best used as soon as there is evidence of clot formation. They are administered intravenously when certain criteria have been met. Administration is continued until there is evidence of reperfusion or until the maximum dosage has been given.
Information about anticoagulant, antiplatelet, and fibrinolytic agents is presented in the Drug Therapy tables on pp. 464 and 465 and pp. 697 and 698. Selected antiplatelet agents are also listed in the Drug Therapy table on p. 645.
Lipid-Lowering Agents
Lipid-lowering medications are frequently part of the overall treatment plan, along with diet and exercise, for many patients with heart disease. The goal of therapy is for the patient to have decreased serum triglyceride and LDL levels and an improved HDL level. Patients on this group of medications need to be encouraged to adhere to diet restrictions, exercise, and quit smoking. Serial laboratory tests (lipid profile and liver function) will be closely monitored. Selected lipid-lowering medications are included in the Drug Therapy table on p. 645.
Analgesics
The patient who has an AMI experiences severe chest pain. The first medication administered to a patient with chest pain is nitroglycerin, which is a vasodilator. When this drug does not relieve the pain, morphine is the preferred analgesic. Morphine relieves pain, reduces anxiety, and

reduces the workload of the heart by trapping some of the venous blood in the periphery of the body. An alternative to morphine is meperidine hydrochloride (Demerol). Meperidine is less effective in relieving anxiety and cardiac workload than morphine. Morphine and meperidine are most effective when administered intravenously.
DIET THERAPY
Reduction of body weight lessens the workload on the heart. A low-fat, high-fiber diet usually is recommended for cardiac patients. Patients would be encouraged to eat a well-balanced diet that includes an emphasis on fruits, vegetables, grains, and proteins low in fat (fish, legumes, poultry and lean meats). Cholesterol intake should be limited to 200 mg/day for individuals with heart disease or at high risk for heart disease. It is also recommended that foods with trans fatty acids be limited ( American Heart Association, 2007 ). An exercise program may help the patient achieve optimal weight.
Sodium
If fluid retention accompanies the cardiac problem, the physician may order sodium restriction. A diet containing sodium 2 g/day is most often prescribed. Restrictions greater than this are difficult to achieve, and studies have shown that patients quickly become noncompliant with the dietary regimen. Salt substitutes are available.
Potassium
Patients taking potassium-wasting diuretics (e.g., furosemide, hydrochlorothiazide) need to include adequate potassium in the diet to counteract the depletion. Patients taking large doses of potassium-wasting diuretics need to have potassium supplements prescribed.
Pharmacology Capsule
Potassium-wasting diuretics such as furosemide and hydrochlorothiazide may cause hypokalemia, which can lead to dangerous dysrhythmias.
Consider the Alternative
Some people use garlic to reduce plasma lipids and lower blood pressure. The best garlic preparation is an enteric-coated dried preparation that contains adequate allicin and allinase—the “active ingredients” in the preparation. Most of the allicin and allinase are destroyed when fresh garlic is cooked or eaten raw. Garlic irritates the GI tract and increases the effects of anticoagulants and insulin.
OXYGEN THERAPY
The myocardium needs an adequate blood supply to function properly. Any patient complaining of chest pain unrelieved by nitroglycerin should have supplemental oxygen administered. A

nasal cannula or facemask should be applied and set to deliver the prescribed liter flow, and the patient's response to this therapy should be monitored.
PACEMAKERS
Pacemakers were first introduced in 1958. Their purpose is to restore regular rhythm and to improve cardiac output and tissue perfusion. Pacemakers may be temporary or permanent. Methods for temporary pacing are transcutaneous, transvenous, or epicardial. Transcutaneous pacemakers deliver impulses through the skin from externally placed electrode pads. A transvenous pacemaker has a pacing electrode that is threaded through a vein into the right side of the heart. Epicardial pacing wires are placed into the epicardial wall of the heart during cardiac surgery and the wires are brought through the chest wall. Temporary pacemakers all require an external pulse generator to provide the electrical energy needed to stimulate depolarization. A permanent pacemaker is surgically place subcutaneously in the wall of the chest, with the electrical lead placed into the heart through a vein. Impulses are conducted from the power source (external pulse generator or implanted pacemaker) to the heart to stimulate contraction of the myocardium.
Pacemakers can be used to stimulate the atrium or ventricle (called single-chamber pacing), or they can be used to stimulate both chambers (called dual-chamber pacing). Dual-chamber pacing produces conduction and contraction that is near normal.
Table 35-6 Revised NASPE/BPEG Generic Code for Antibradycardia Pacing*
I II III IV V
Chamber(s) Paced Chamber(s) Sensed
Response to Sensing Rate Modulation Multisite
Pacing O = None O = None O = None O = None O = None
A = Atrium A = Atrium T = Triggered R = Rate modulation A = Atrium
V = Ventricle V = Ventricle I = Inhibited V = Ventricle
D = Dual (A+V) D = Dual (A+V) D = Dual D = Dual (A+V)
S = Single (A or V)† S = Single (A or V)† (T+I)From Bernstein, A.D., Daubert, J.C., Fletcher, R.D., Hayes, D.L., Luderitz, B., Reynolds, D.W., Schoenfeld, M.H., & Sutton R. (2002). The revised NASPE/BPEG generic code for antibradycardia, adaptive-rate, and multisite pacing. Pacing and Clinical Electrophysiology, 25 (2), 261.
Table 35-7 Pertinent Definitions Related to Pacemakers
SensingAbility of the pacemaker to detect intrinsic myocardial electrical activityThe pacemaker either is inhibited from delivering a stimulus or initiates an electrical impulse, based on the programmed response
Pulse generation
Occurs when the pacemaker produces a programmed current for a set durationThis energy travels through the transvenous lead wires to the myocardium—this is known as pacemaker firing and usually produces a line or spike on the ECG

recording
Capture
Refers to the successful stimulation of the myocardium by the pacemaker impulse that results in depolarizationEvidenced on the ECG by a pacemaker spike/stimulus followed by either an atrial or ventricular complex, depending on the chambers being paced
Failure of pulse generation
Pacemaker does not discharge a pacing stimulus at its programmed time to the myocardiumEvidenced by the absence of a pacemaker spike on the ECG where expected
Sensing failure
Pacemaker has either detected extraneous signals that mimic intrinsic cardiac activity (oversensing) or did not accurately identify intrinsic activity (undersensing)Oversensing is recognized on the ECG by pauses where paced beats were expected and prolongation of the interval between paced beatsUndersensing is recognized on the ECG by inappropriate pacemaker spikes relative to the intrinsic electrical activity (pacemaker spikes occurring within the P wave, QRS complex, or T wave) and shortened distances between paced beats)
Failure to capture
Pacemaker has delivered a pacing stimulus that was unable to initiate depolarization of the myocardium and subsequent myocardial contractionEvidenced on the ECG by pacemaker spikes that are not followed by a P wave for atrial pacing or spikes not followed by a QRS complex for ventricular pacing
ECG, Electrocardiogram.
Pacemakers have multiple settings related to pacing and sensing. A coding system was developed in the 1970s and has undergone a number of revisions. The most recent revision is found in Table 35-6. A set of pertinent definitions related to pacemakers is found in Table 35-7.
Temporary Pacemakers
Temporary pacemakers can be used electively or for emergency situations. Elective uses include gaining control of very rapid supraventricular tachycardic rhythms, assessing the need for permanent pacing in patients with bradycardias, and following cardiac surgery.
Permanent Pacemakers
Permanent pacemakers are indicated in a number of patient situations in which conduction defects or dysrhythmias compromise the normal function of the heart. Several clinical conditions indicate the need for permanent pacing. A few of these conditions are the following: acquired atrioventricular (AV) block, sinus node dysfunction, chronic bifascicular or trifascicular block, symptomatic tachycardias, and carotid sinus syndrome. A permanent implantable pacemaker is inserted under local anesthesia. The batteries, usually lithium, have an 8- to 10-year expected life. Permanent pacemakers are inserted in the operating room, catheterization laboratory, or special procedures area. The pacing lead is positioned (through the subclavian or cephalic vein) in the right atrium, right ventricle, left ventricle, or a combination of these (depending on the patient's problem). The generator is placed in a subcutaneous pocket, usually under the clavicle or in the abdomen.

Table 35-7 Pertinent Definitions Related to Pacemakers
SensingAbility of the pacemaker to detect intrinsic myocardial electrical activityThe pacemaker either is inhibited from delivering a stimulus or initiates an electrical impulse, based on the programmed response
Pulse generation
Occurs when the pacemaker produces a programmed current for a set durationThis energy travels through the transvenous lead wires to the myocardium—this is known as pacemaker firing and usually produces a line or spike on the ECG recording
Capture
Refers to the successful stimulation of the myocardium by the pacemaker impulse that results in depolarizationEvidenced on the ECG by a pacemaker spike/stimulus followed by either an atrial or ventricular complex, depending on the chambers being paced
Failure of pulse generation
Pacemaker does not discharge a pacing stimulus at its programmed time to the myocardiumEvidenced by the absence of a pacemaker spike on the ECG where expected
Sensing failure
Pacemaker has either detected extraneous signals that mimic intrinsic cardiac activity (oversensing) or did not accurately identify intrinsic activity (undersensing)Oversensing is recognized on the ECG by pauses where paced beats were expected and prolongation of the interval between paced beatsUndersensing is recognized on the ECG by inappropriate pacemaker spikes relative to the intrinsic electrical activity (pacemaker spikes occurring within the P wave, QRS complex, or T wave) and shortened distances between paced beats)
Failure to capture
Pacemaker has delivered a pacing stimulus that was unable to initiate depolarization of the myocardium and subsequent myocardial contractionEvidenced on the ECG by pacemaker spikes that are not followed by a P wave for atrial pacing or spikes not followed by a QRS complex for ventricular pacing
ECG, Electrocardiogram.
Pacemakers have multiple settings related to pacing and sensing. A coding system was developed in the 1970s and has undergone a number of revisions. The most recent revision is found in Table 35-6. A set of pertinent definitions related to pacemakers is found in Table 35-7.
Temporary Pacemakers
Temporary pacemakers can be used electively or for emergency situations. Elective uses include gaining control of very rapid supraventricular tachycardic rhythms, assessing the need for permanent pacing in patients with bradycardias, and following cardiac surgery.
Permanent Pacemakers
Permanent pacemakers are indicated in a number of patient situations in which conduction defects or dysrhythmias compromise the normal function of the heart. Several clinical conditions indicate the need for permanent pacing. A few of these conditions are the following: acquired atrioventricular (AV) block, sinus node dysfunction, chronic bifascicular or trifascicular block,

symptomatic tachycardias, and carotid sinus syndrome. A permanent implantable pacemaker is inserted under local anesthesia. The batteries, usually lithium, have an 8- to 10-year expected life. Permanent pacemakers are inserted in the operating room, catheterization laboratory, or special procedures area. The pacing lead is positioned (through the subclavian or cephalic vein) in the right atrium, right ventricle, left ventricle, or a combination of these (depending on the patient's problem). The generator is placed in a subcutaneous pocket, usually under the clavicle or in the abdomen.
Table 35-7 Pertinent Definitions Related to Pacemakers
SensingAbility of the pacemaker to detect intrinsic myocardial electrical activityThe pacemaker either is inhibited from delivering a stimulus or initiates an electrical impulse, based on the programmed response
Pulse generation
Occurs when the pacemaker produces a programmed current for a set durationThis energy travels through the transvenous lead wires to the myocardium—this is known as pacemaker firing and usually produces a line or spike on the ECG recording
Capture
Refers to the successful stimulation of the myocardium by the pacemaker impulse that results in depolarizationEvidenced on the ECG by a pacemaker spike/stimulus followed by either an atrial or ventricular complex, depending on the chambers being paced
Failure of pulse generation
Pacemaker does not discharge a pacing stimulus at its programmed time to the myocardiumEvidenced by the absence of a pacemaker spike on the ECG where expected
Sensing failure
Pacemaker has either detected extraneous signals that mimic intrinsic cardiac activity (oversensing) or did not accurately identify intrinsic activity (undersensing)Oversensing is recognized on the ECG by pauses where paced beats were expected and prolongation of the interval between paced beatsUndersensing is recognized on the ECG by inappropriate pacemaker spikes relative to the intrinsic electrical activity (pacemaker spikes occurring within the P wave, QRS complex, or T wave) and shortened distances between paced beats)
Failure to capture
Pacemaker has delivered a pacing stimulus that was unable to initiate depolarization of the myocardium and subsequent myocardial contractionEvidenced on the ECG by pacemaker spikes that are not followed by a P wave for atrial pacing or spikes not followed by a QRS complex for ventricular pacing
ECG, Electrocardiogram.
Pacemakers have multiple settings related to pacing and sensing. A coding system was developed in the 1970s and has undergone a number of revisions. The most recent revision is found in Table 35-6. A set of pertinent definitions related to pacemakers is found in Table 35-7.
Temporary Pacemakers

Temporary pacemakers can be used electively or for emergency situations. Elective uses include gaining control of very rapid supraventricular tachycardic rhythms, assessing the need for permanent pacing in patients with bradycardias, and following cardiac surgery.
Permanent Pacemakers
Permanent pacemakers are indicated in a number of patient situations in which conduction defects or dysrhythmias compromise the normal function of the heart. Several clinical conditions indicate the need for permanent pacing. A few of these conditions are the following: acquired atrioventricular (AV) block, sinus node dysfunction, chronic bifascicular or trifascicular block, symptomatic tachycardias, and carotid sinus syndrome. A permanent implantable pacemaker is inserted under local anesthesia. The batteries, usually lithium, have an 8- to 10-year expected life. Permanent pacemakers are inserted in the operating room, catheterization laboratory, or special procedures area. The pacing lead is positioned (through the subclavian or cephalic vein) in the right atrium, right ventricle, left ventricle, or a combination of these (depending on the patient's problem). The generator is placed in a subcutaneous pocket, usually under the clavicle or in the abdomen.
NURSING CARE of the Patient with a Pacemaker
Patients with inserted pacemakers recover in the postanesthesia care unit and then go to a unit with telemetry capability. Monitor the patient for proper pacemaker functioning. Examine the ECG for rhythm, pacemaker spike, and dysrhythmias (premature ventricular contractions and ventricular tachycardia are seen most often). The pacemaker spike is a mark observed on the ECG tracing that represents the impulse generated by the pacemaker. Assess vital signs and inspect the incision frequently. Patients rest for 24 hours after the insertion of a permanent pacemaker. Following that, patients are ambulated and are encouraged to resume normal activities.
After insertion of a temporary pacemaker, microshock precautions should be followed. Monitor the ECG and transport the patient with a portable cardiac monitor and a nurse in attendance. Assess the pacemaker for misfiring. Plan a gradual increase in activities.
There are three major problems that can occur with pacing. The first problem, failure to pace, means that the pacemaker did not initiate the electrical stimulus when it was due to fire. Frequently caused by battery failure or lead wire displacement, it is recognized by the lack of a pacer spike on the ECG tracing. The second problem, failure to capture, means that the electrical stimulus from the pacemaker is not followed by electrical activity in the patient's heart. Caused by dislodgement of the lead or the pacemaker output setting set too low, failure to capture is recognized by noting the presence of a pacer spike without ECG activity following the spike. The third problem, failure to sense, means that the pacemaker does not sense the patient's cardiac rhythm and initiates an electrical impulse when it is not needed. Failure to sense is most often caused by displacement of the electrode and can be recognized by pacer spikes that fall too close to the patient's rhythm.
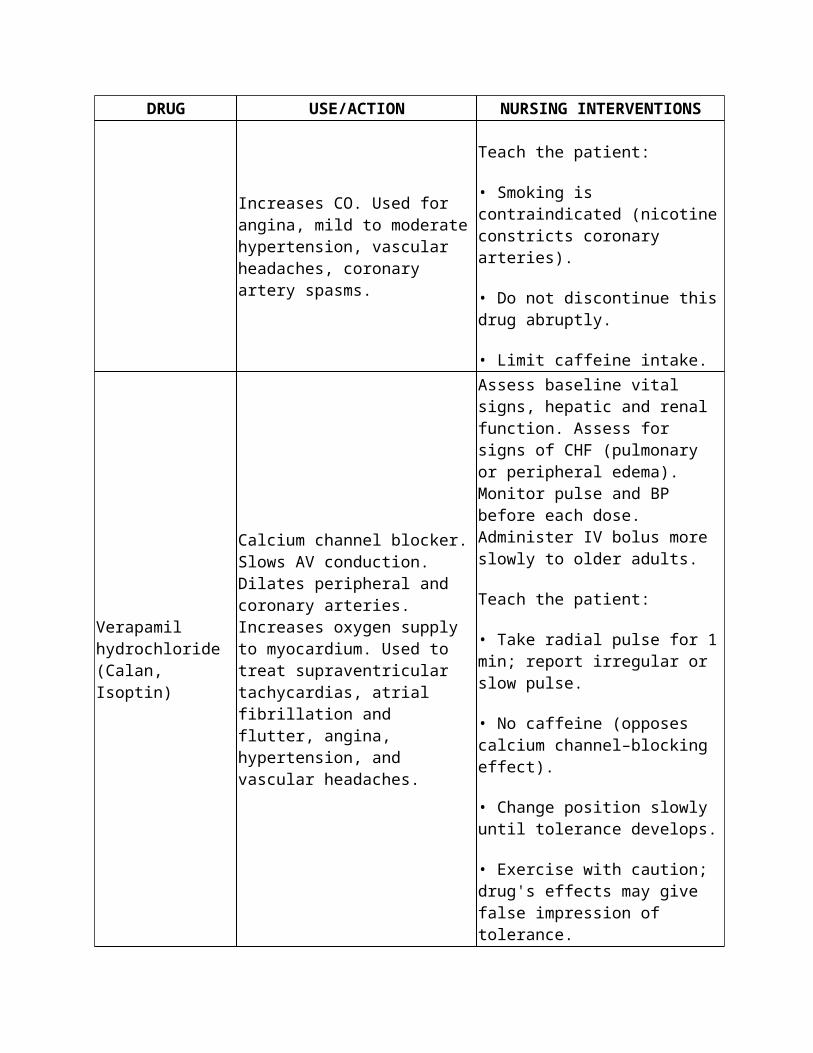
When a permanent pacemaker has been inserted, teach the patient how to count the pulse for 1 full minute daily. Explain wound care and the healing process. Advise the patient to notify the physician of symptoms of decreased cardiac output: dyspnea, dizziness, syncope, weakness, fatigue, and chest pain. Also instruct the patient to carry an identification card describing the type of pacemaker implanted.
CARDIOVERSION
Cardioversion is the delivery of a synchronized shock to terminate atrial or ventricular tachydysrhythmias (rapid abnormal heart rhythms). It may be done as an emergency or elective procedure. The shock is synchronized with the R wave to avoid shocking during the vulnerable period of the T wave. A shock delivered during ventricular relaxation can initiate ventricular fibrillation.
If the patient is receiving digoxin, the drug is withheld for 24 hours before the procedure. Emergency drugs are made available, and the patient has a patent intravenous line in place before the procedure. Explain the procedure, and obtain informed consent. A short-acting sedative is usually given. The cardioverter is set to the synchronized mode, and two electrodes are placed on the chest. One electrode is placed to the right of the sternum just below the clavicle and the other is placed at the apex of the heart. The initial impulse varies from 25 to 100 joules depending on the type of dysrhythmia. If the initial impulse does not convert the dysrhythmia to normal sinus rhythm, the impulse energy is increased and the procedure is repeated.
After cardioversion, the patient usually recovers very quickly from the sedation and does not remember the event. Inspect the skin under the electrodes for irritation. Monitor the patient's heart rate and rhythm, vital signs, and neurologic status. Transient dysrhythmias and a drop in blood pressure are common. Be especially alert for atrial fibrillation, which can contribute to the formation of atrial wall thrombus and emboli.
CARDIOPULMONARY RESUSCITATION
Cardiopulmonary resuscitation is the restoration of heart and lung function after cardiac arrest. The procedure is used in basic cardiac life support and advanced cardiac life support. The reader is referred to materials prepared by the American Heart Association for current, in-depth coverage of the procedure. See Chapter 16 for an overview.
CARDIAC SURGERY
The most common surgical procedures involving the heart are pacemaker insertion, heart surgery to repair or replace valves or septa or remove tumors, and coronary artery bypass surgery. Pacemaker insertion is described earlier in this section. Coronary artery bypass surgery is described as a surgical treatment for AMI on pp. 657 and 658.
With some of the surgical procedures on the heart, the heart muscle must be at rest during the procedure. This requires placing the patient on a machine to direct the blood away from the heart and lungs and to maintain appropriate oxygen and carbon dioxide levels. The heart's rhythm is

interrupted by an electrolyte solution and may be restarted after the surgery by electrical stimulation. During this type of surgery, the patient's core temperature usually is reduced to decrease the oxygen needs of the entire body, especially the brain.
PREOPERATIVE NURSING CARE of the Cardiac Surgery PatientAssessment
Nursing assessment of the patient with cardiac disorders is summarized in Box 35-1. When a patient is facing cardiac surgery, also assess the patient's fears and anxiety. Patients are usually upset and very concerned when heart surgery is recommended. Determine what patients know about the surgery and what more they would like to know.
Nursing Diagnoses, Goals, and Outcome Criteria: Preoperative Cardiac SurgeryNursing Diagnoses Goals and Outcome Criteria
Fear related to perceived threat of death or unfamiliarity with setting and procedures
Reduced fear: patient states is less fearful, demonstrates relaxed manner
Anxiety related to threat to health status or uncertain outcome
Reduced anxiety: patient states is less anxious, is calmer
InterventionsFear and Anxiety
Encourage the patient to identify feelings and then explore the basis of those feelings. Do not assume you know how the patient feels. Accept the patient's feelings and do not give trite reassurance (“Don't worry; everything will be fine.”). Accurate information about what to expect helps reduce fear of the unknown. Physical comfort measures such as a massage or back rub may also be soothing. If the patient's anxiety level remains high, notify the physician.
Good patient teaching is essential to address fear and anxiety. The physician reviews necessary diagnostic tests, the surgical procedure itself, and what to expect after surgery. Nevertheless, the nurse must be able to clarify and further explain what the patient will experience. If the surgery is to be done as an emergency, little time is available to do preoperative teaching. Planned cardiac surgery allows time for the patient to accept the need for surgery and to explore why the procedure is necessary. Include the family in the preoperative teaching to decrease their anxiety and allow them to participate in the patient's recovery. The patient teaching plan must be individualized for the type of surgical procedure.
Patient Teaching PlanCardiac Surgery, Preoperative
The specifics of the teaching plan depend on the exact procedure and agency/surgeon procedures. General content of the teaching plan incudes the following:
•Preoperative routines: NPO, monitoring, diagnostic tests, any special preparation •Where the patient will be after surgery: in intensive care unit after extensive procedures;
to regular units after pacemaker insertion •The postoperative care setting: the room and the equipment

•Postoperative routines: how to turn, cough, deep breathe, and exercise the leg muscles; monitoring; procedures
•Postoperative pain: amount of pain to expect, relief measures such as splinting, positioning, medication
•Communication: because most patients are intubated for 4 to 8 hours after surgery, establish a means of communication before surgery
Put on Your Thinking Cap! A patient is scheduled for extensive cardiac surgery and will be on a ventilator for up to 8
hours postoperatively. What means of communication can you establish in advance? What if the patient is illiterate? What if the patient is deaf?
POSTOPERATIVE NURSING CARE of the Cardiac Surgery Patient Nursing care needs vary considerably depending on the type of surgical procedure. Care
specific to certain conditions is discussed with those conditions. In addition, see Chapter 17 for thorough coverage of care of the surgical patient. This section addresses needs common to many patients having cardiac surgery.
Assessment Assessment of the cardiac patient is summarized in Box 35-1. After surgery, be
especially alert to changes in vital signs, breath sounds, urine output, mental alertness, and color. In the intensive care unit, monitor cardiac rhythm, arterial blood gases, and hemodynamic pressures. Assess chest tube function. Frequently inspect all dressings for type and amount of drainage. Examine the surgical wound and insertion sites of tubes and cannulas for increasing redness, swelling, and purulent drainage. Assess urine amount, appearance, and odor.
Nursing Diagnoses, Goals, and Outcome Criteria: Postoperative Cardiac SurgeryNursing Diagnoses Goals and Outcome Criteria
Ineffective Breathing Pattern related to mechanical ventilation, general anesthesia, pain, or restrictive surgical dressings
Adequate oxygenation: arterial blood gases within normal limits
Acute Pain related to tissue trauma Pain relief: patient states pain reduced or relieved, relaxed manner
Ineffective Thermoregulation related to cooling during surgery
Normal body temperature: temperature of at least 36.7° C (98° F) orally
Decreased Cardiac Output related to fluid loss or decreased fluid intake
Normal cardiac output: fluid intake equal to output
Risk for Infection related to altered skin integrityAbsence of infection: no fever; decreasing drainage, redness, and swelling of wound
Anxiety related to unfamiliar routines and stressful experience
Reduced anxiety: patient states anxiety is reduced
InterventionsIneffective Breathing Pattern
Patients with open heart or bypass surgery are unresponsive on arrival in the intensive care unit. Ventilatory assistance is of prime importance. Reassess breath sounds and arterial blood gases
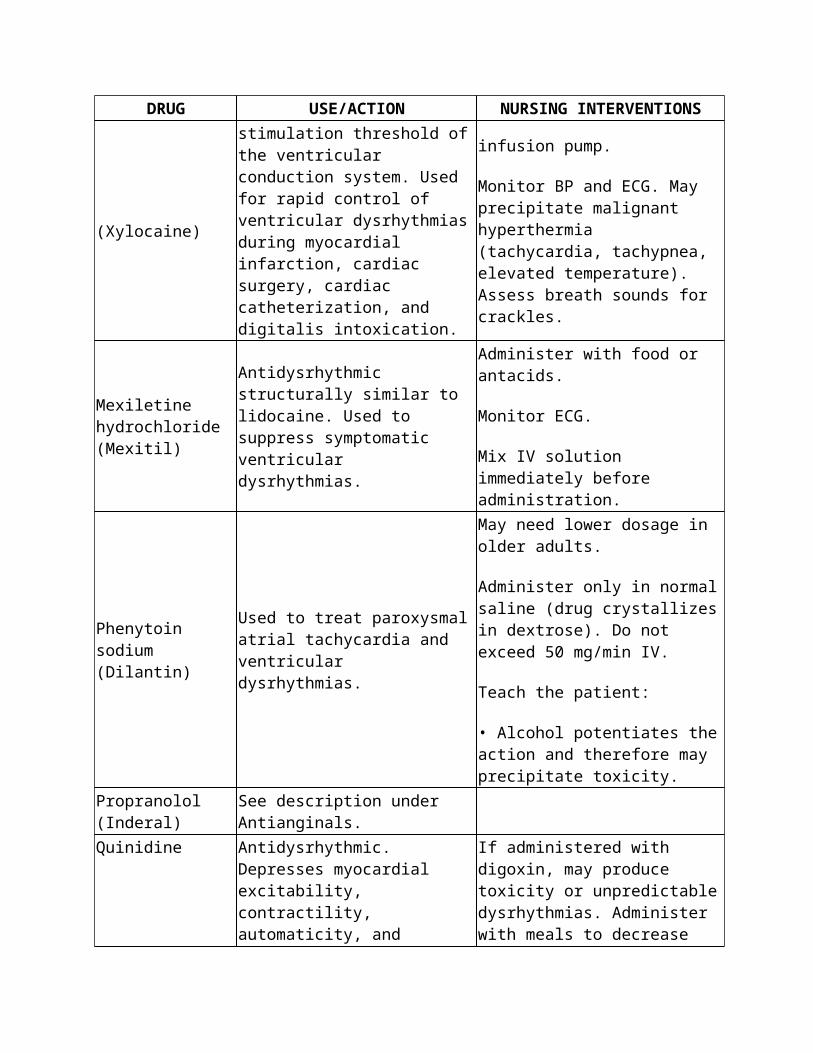
frequently. Connect chest tubes to underwater seal drainage. (See Chapter 30 for the care of chest tubes.) Reposition the patient often to promote removal of pulmonary secretions and improve respiratory excursion.
When the patient is extubated, provide an oxygen mask or nasal cannula as ordered to provide supplemental oxygen. Assist the patient to cough and deep breathe frequently. A pillow or a blanket in a pillowcase can be used as an incisional splint during coughing. An incentive spirometer is usually ordered. Monitor its use, and remind the patient to use it. Assist with early ambulation, as ordered, to reduce the risk of pulmonary complications.
Acute Pain
Effective pain relief makes it easier for the patient to turn, cough, and deep breathe. Assess the patient's pain: location, severity, aggravating factors, and relieving factors. Administer analgesics as ordered. Intravenous morphine in small doses is most frequently prescribed for analgesia. You may also use independent measures, including position changes, back rubs, relaxation techniques, and imagery. Assess the effectiveness of the interventions in managing pain. Provide for periods of rest and sleep after pain relief efforts.
Ineffective Thermoregulation
Warmed blankets, heating blankets, and warming lights may be used to assist rewarming. Monitor body temperature continuously until the patient is stable.
Decreased Cardiac Output
Monitor cardiac pressures continuously in the intensive care unit until they stabilize. Prescribed medications are adjusted based on vital signs, hemodynamic pressures, and cardiac rhythms. Pacing wires are connected to a temporary pacemaker. Monitor fluid and blood administration, and assess urinary and other drainage outputs. Volume expanders (albumin, dextran, hetastarch) and vasoactive drugs may be necessary to maintain blood pressure. Oral fluids are ordered shortly after extubation.
Risk for Infection
The patient is at risk for incisional, respiratory tract, and urinary tract infections. In addition, the presence of multiple tubes and cannulas provides additional sites for potential nosocomial infection. To reduce the risk of infection, practice good hand-washing technique and use aseptic technique when handling dressings and invasive equipment. Provide wound care as ordered or per agency policy. Administer antibiotics as ordered. Before discharge, begin teaching the patient how to care for the surgical wound. Emphasize signs or symptoms that should be reported to the physician: fever, increasing or purulent wound drainage, increasing redness or swelling, and separation of wound margins.
Anxiety
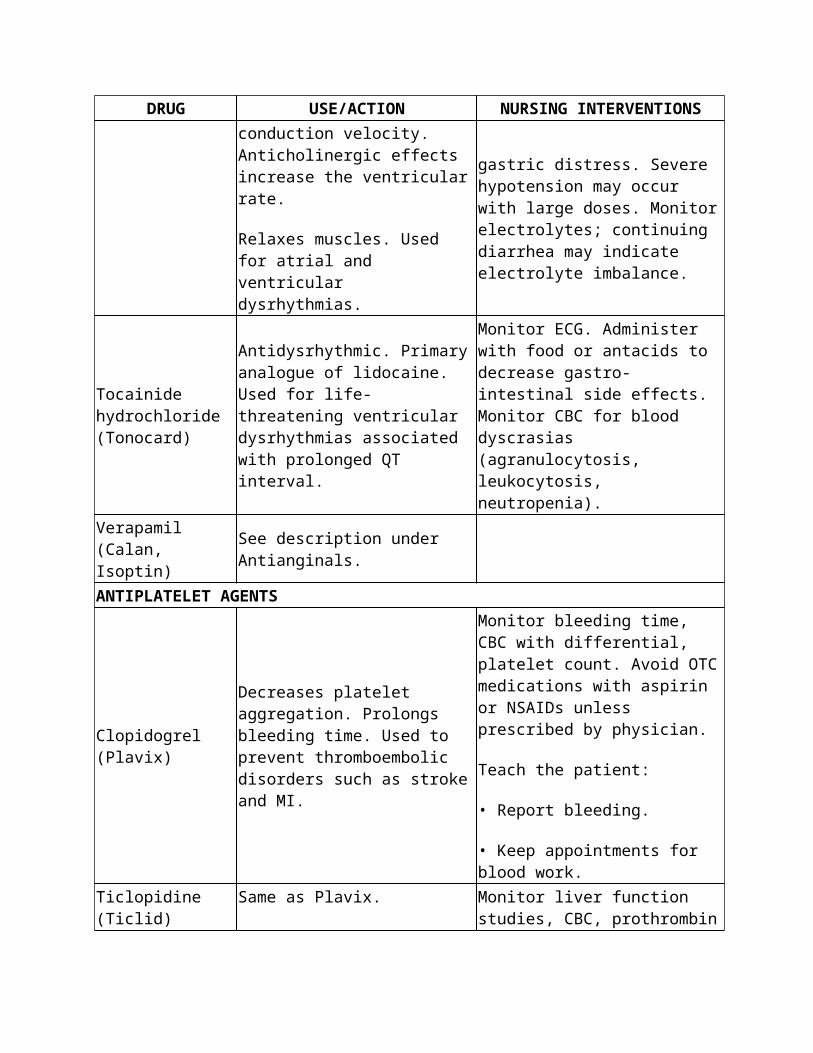
Inform the patient and the family what is being done and how the patient is responding. Remember to talk to the patient and offer reassurance. When the patient is on a ventilator, use the previously established nonverbal means of communication. It is often necessary to repeat instructions because of the effects of pain, medications, and anxiety. As the patient improves, explain the importance of follow-up care and rehabilitation.
Consider the Alternative
For pain relief, many complementary therapies are used with analgesics. Some examples are massage, relaxation techniques, and imagery.
CARDIAC DISORDERSCORONARY ARTERY DISEASE
Coronary artery disease (CAD) occurs when the major coronary arteries supplying the myocardium are partially or completely blocked. Blockage of the arteries is caused by coronary artery spasm, arteriosclerosis, or atherosclerosis and may result in ischemia or infarction of myocardial tissue. In 1998, there were 208 deaths per 100,000 population. A Healthy People 2010 objective is to reduce that number by 20 percent (Centers for Disease Control and Prevention/National Institutes of Health, 2005). See the Health Promotion Considerations box on p. 653 for a review of cardiac risk factor modification.
Arteriosclerosis
Arteriosclerosis is an abnormal thickening, hardening, and loss of elasticity of arterial walls. Smooth muscle cells and collagen migrate into the tunica intima (innermost layer of the artery) and cause the arterial wall to stiffen and thicken and the lumen to decrease in diameter. Lipids, cholesterol, calcium, and thrombi adhere to the damaged arterial wall. This process limits the elasticity of the wall and decreases the flow of oxygen-carrying blood to tissues. Some effects of arteriosclerosis are hypertension, impaired tissue perfusion, and aneurysms.
Health Promotion ConsiderationsRisk Factor Modification
Risk factor modification will help reduce an individual's risk for developing CAD, angina, and acute coronary syndromes. Controlling HTN, reducing serum cholesterol and LDLs, smoking cessation, participating in regular, moderate exercise, obtaining/maintaining ideal body weight, and learning to handle stress are recommended lifestyle changes that can help decrease risk.
Signs and Symptoms
Coronary artery disease usually is asymptomatic until the tissue's blood supply is reduced by at least 50%. Then, the clinical manifestations of CAD include angina pectoris, acute coronary syndrome (unstable angina and acute myocardial infarction), and sudden cardiac death. Acute myocardial infarction has been further categorized into non–ST-segment elevation myocardial infarction (NSTEMI) and ST-segment elevation myocardial infarction (STEMI).
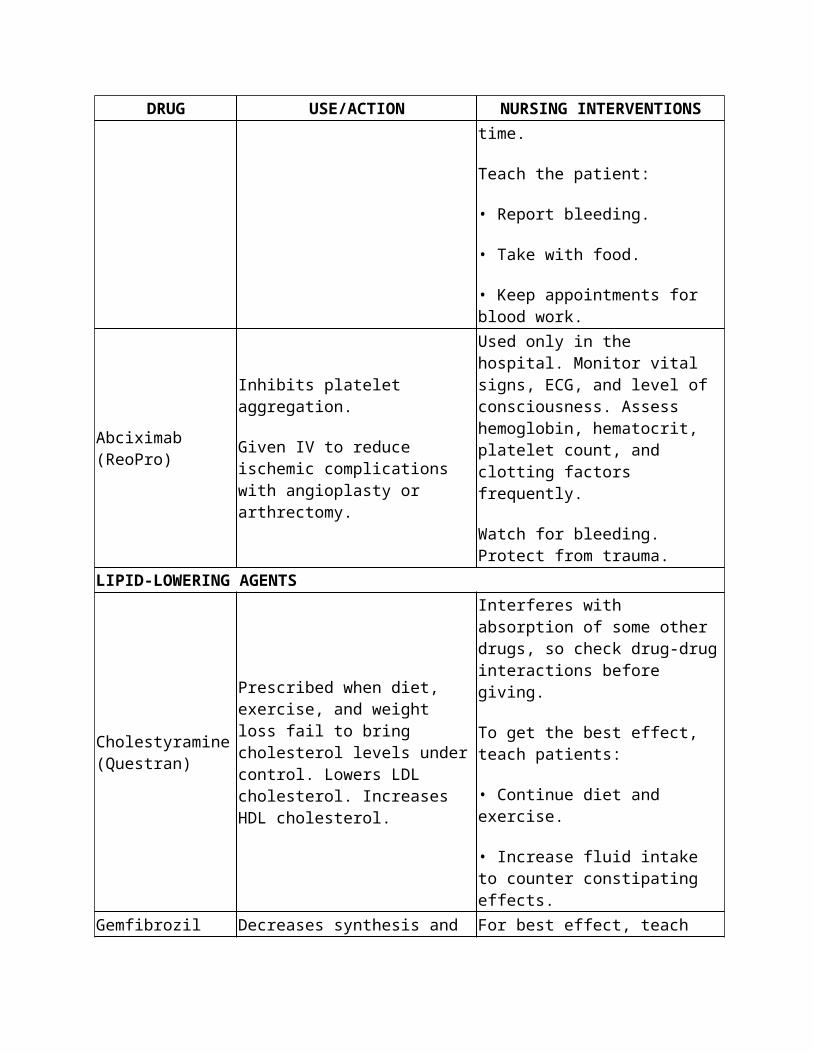
ANGINA PECTORIS
Angina pectoris (shortened to angina), or chest pain, the most common symptom of CAD, results when the demand for oxygen by the myocardial cells exceeds the supply of oxygen delivered. There are different types of angina: stable, unstable, and variant. Stable angina (also called chronic angina or exertional angina) occurs most often with exercise or activity and usually subsides with rest. Other precipitating factors are smoking, physical exertion, emotional stress, and heavy meals. The pain is usually substernal and described by the patient as viselike, burning, squeezing, or smothering. The pain may radiate to either arm, the shoulder, the jaw, the neck, or the epigastrium. Accompanying symptoms are diaphoresis, dyspnea, nausea, and vomiting. Stable angina occurs intermittently and is often predictable. Usually, stable angina lasts only a few minutes and is relieved by rest or with nitroglycerine (NTG).
Unstable angina (categorized and treated as an acute coronary syndrome) is also called crescendo angina or preinfarction angina. The pain of unstable angina is more severe, occurs at rest or with minimal exertion, is often not relieved by NTG or requires more frequent NTG administration, and is not predictable. Unstable angina may occur in a patient with a history of stable angina. The patient may describe a change in the pain pattern or in the severity of the pain. Or, unstable angina may be the first clinical manifestation of CAD that a patient experiences. In either case, unstable angina is considered more serious than stable angina and will be treated differently. Patients with unstable angina are at higher risk for acute myocardial infarction (AMI) and are often hospitalized for diagnostic workup and treatment.
Variant angina (also known as Prinzmetal's angina) is caused by coronary artery spasm and may not be associated with CAD. This type of angina is unpredictable and often occurs at rest. When the coronary spasm occurs, the patient experiences angina and, if the patient is being monitored, transient ST elevation may be seen. When the spasm subsides, the pain goes away and the ST segment returns to normal. The treatment for variant angina is usually administration of calcium channel blockers to prevent the spasms from occurring.
Medical Treatment
Treatment of CAD includes diet therapy, drug therapy, and reduction of modifiable risk factors (e.g., smoking, obesity, hypertension). Recommendations for medical therapy have been developed for both stable and unstable angina. Initial therapy for patients with angina should follow the mnemonic below (Braunwald, et al., 2002; Gibbons, et al., 2002):
A Aspirin and antianginal therapyB Beta blocker and blood pressureC Cigarette smoking and cholesterolD Diet and diabetesE Education and exercise
Low-dose aspirin is administered to interfere with platelet aggregation and it can reduce the risk of myocardial infarction. If the patient cannot tolerate aspirin, another antiplatelet medication (e.g., Ticlid, Plavix) will be prescribed. Antianginal therapy includes nitrates, beta-adrenergic

blockers, and calcium channel blockers. Nitrates such as NTG are used to treat actual episodes of angina and to prevent the occurrence of angina. Various forms of nitroglycerin are prescribed for treatment of acute angina. These are administered sublingually or buccally at the onset of pain. They are quickly absorbed and usually effective. Oral, topical, and transdermal nitrates may be ordered to prevent angina attacks. Beta-adrenergic blockers and calcium channel blockers are
prescribed in the long-term management of angina.
After the initial relief and control of the anginal pain, the focus of therapy will turn to risk reduction to include optimizing blood pressure, smoking cessation, lipid control (diet alone or diet plus lipid-lowering medications), healthy diet and tight glucose control for diabetic patients, exercise training, and patient education (i.e., medication therapy, risk reduction, and what to do if symptoms of an AMI occur).
ACE inhibitors may also be prescribed to patients with stable angina to reduce the risk of AMI. In addition, some patients may be recommended for further treatment with percutaneous coronary interventions (PCI), such as angioplasty, stent placement, or atherectomy (Gibbons, et al., 2002).
Additional information about various drug therapies is presented in the Drug Therapy table on p. 646.
Unstable angina may be treated conservatively or more aggressively, depending on the situation. Because unstable angina may be a “warning” of more serious events, it has been classified as an acute coronary syndrome. In current recommendations, unstable angina and NSTEMI are addressed together because they are so closely related. Patients with unstable angina should receive the A-B-C-D-E's discussed in the previous section. However, in addition to antiplatelet therapy, anticoagulation therapy with LMWH may be administered. For patients who will be undergoing cardiac catheterization and PCI, a platelet GP IIb/IIIa antagonist will also be administered (Braunwald, et al., 2002).
Surgical Intervention
Surgical procedures to treat CAD are discussed on pp. 656 and 657.
What Does Culture Have to Do with Heart Disease?
American Indians and African Americans develop CAD at an earlier age than other Americans. The incidence of CAD is highest among middle-aged Caucasian males. Latinos have lower death rates from CAD than non-Latinos. Nurses can educate high-risk patients about risk factors that can be modified: obesity, hypertension, and stress. Role models from the target population are especially influential.
ACUTE MYOCARDIAL INFARCTION
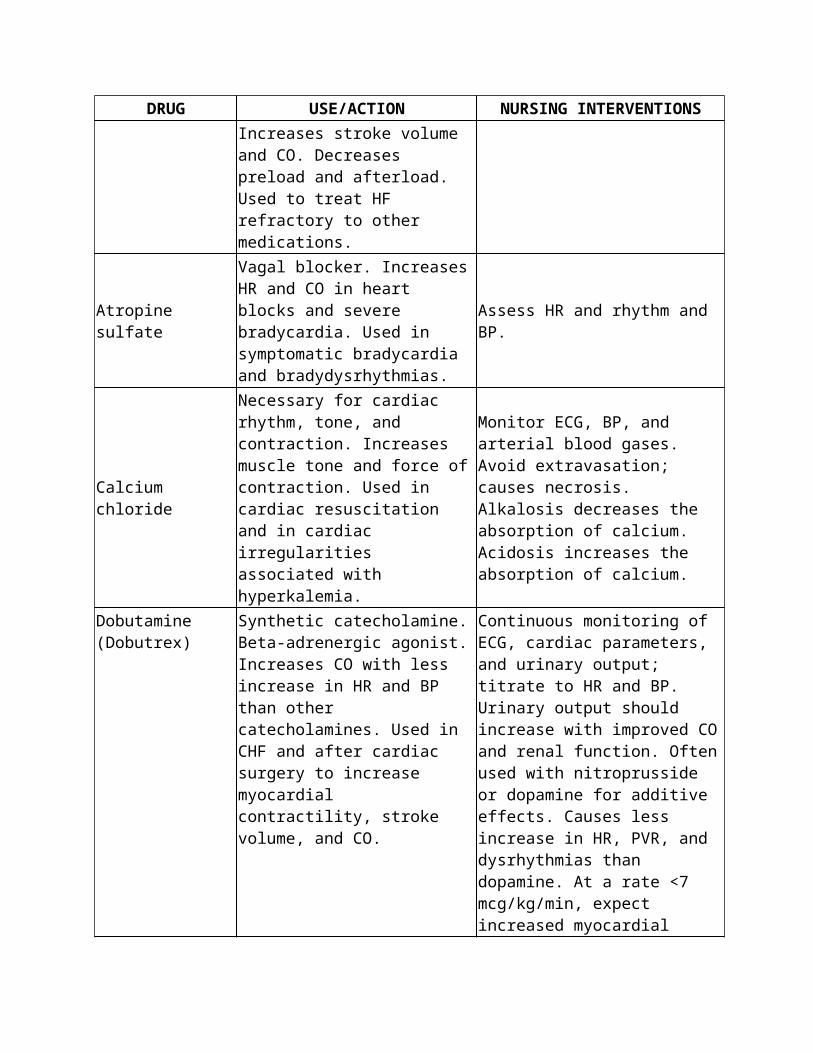
An AMI is the death of myocardial tissue as a result of prolonged lack of blood and oxygen supply. Approximately 700,000 Americans have a new myocardial infarction every year and 500,000 Americans have recurrent attacks annually. Approximately 225,000 individuals in the United States will die each year from myocardial infarction. The average age for men having a first heart attack is 65 to 66 years, and the average age in women for a first heart attack is 70 years (American Heart Association, 2007).
Risk Factors
Risk factors for AMI include obesity, smoking, a high-fat diet, hypertension, family history, male gender, diabetes mellitus, sedentary lifestyle, and excessive stress. Smoking, a high-fat diet, hypertension, sedentary lifestyle, and stress are considered modifiable risk factors. This means that risk can be reduced by cessation of smoking, diet modification, management of hypertension, regular exercise, and stress reduction.
Pathophysiology
An AMI begins with the occlusion of a coronary artery. Over a period of 4 to 6 hours, a process of ischemia, injury, and infarction develops. Ischemia results from a lack of blood and oxygen to a portion of the heart muscle. If ischemia is not reversed, injury occurs. Deprived of blood and oxygen, the affected tissue becomes soft and loses its normal color. With continued ischemia, an infarction, or death of myocardial tissue, occurs. Ischemia lasting 20 minutes or more is sufficient to produce irreversible tissue damage.
Within 24 hours after an infarction, the healing process begins. By the third day, necrotic tissue has been broken down by enzymes and removed by macrophages. Collateral circulation develops to supply the injured area, and scar tissue begins to form. About 10 to 14 days after the AMI, the myocardium is especially vulnerable to stress because of the weakness of the healing tissue. Complete healing takes about 6 weeks.
An AMI is considered an acute coronary syndrome, along with unstable angina as mentioned earlier. Health care providers divide AMI into two types: non–ST-elevation MI (NSTEMI) and ST-elevation MI (STEMI) for purposes of diagnosis and treatment. The ST segment of an ECG is usually flat or isoelectric (see the Interpretation of Electrocardiograms section on p. 673). Because the ST segment can be displaced when there is partial or complete lack of oxygen flow to the myocardial cells, the appearance of a patient's ST segment is an important component of the assessment of an AMI. Patients with NSTEMI usually have transient or partial occlusion of a coronary artery, whereas patients with STEMI have total occlusion of a coronary artery from coronary thrombosis.
Complications
The major complications of AMI are dysrhythmias, heart failure, cardiogenic shock, thromboembolism, and ventricular aneurysm/rupture.
Dysrhythmias.

Dysrhythmias are disturbances in heart rhythm, including excessively rapid, slow, or irregular heartbeats. They occur in approximately 80% of all patients with AMI. Because some dysrhythmias are life-threatening, continuous cardiac monitoring is usually ordered for patients with AMI. This permits early detection and prompt treatment of dysrhythmias. Recognition and treatment of specific dysrhythmias are addressed on pp. 673 to 682.
Heart Failure.
The AMI may cause the heart to fail as a pump if the injured LV is unable to meet the body's circulatory demands. The ventricle fails to empty efficiently. Increased preload leads to systemic and pulmonary edema. Cardiac output and blood pressure fall. Untreated cardiac failure progresses to cardiogenic shock and death. Early symptoms of congestive failure are dyspnea, restlessness, and increasing heart rate.
Cardiogenic Shock.
Cardiogenic shock is the most frequent cause of death after an AMI. It is usually related to extensive injury to the LV and is more common when the patient has had a previous infarction. Cardiogenic shock is marked by hypotension; cool, moist skin; oliguria; and decreasing alertness.
Thromboembolism.
After an AMI, thrombi may form in the injured heart chambers or in the veins of the legs. The thrombi may break loose, travel through the circulation, and lodge in the lung. Pallor, cyanosis, and heart failure may be caused by pulmonary emboli. Massive pulmonary embolism is characterized by sudden, severe dyspnea. It is usually fatal. Pulmonary emboli are discussed in detail in Chapter 30.
Ventricular Aneurysm/Rupture.
Weakened areas of the ventricular wall may bulge during contractions. If scar tissue is inadequate to strengthen the wall, an aneurysm may develop and rupture. Ventricular rupture is fatal.
Signs and Symptoms
Pain is the classic symptom of AMI. It is typically a heavy or constrictive pain located below or behind the sternum, as described with angina. It may radiate to the arms, back, neck, or jaw. The pain may begin with or without exertion. If not relieved by rest and nitroglycerin, it progresses. The patient becomes diaphoretic and lightheaded and may experience nausea, vomiting, and dyspnea. The skin is frequently cold and clammy. The patient experiences great anxiety and often a feeling of impending doom. Not all patients experience the more classic signs and symptoms. Women, older adults, and diabetic patients often have atypical symptoms. Women may complain of fatigue, shortness of breath, and atypical chest pain. Older adults and diabetic

patients may not experience chest pain but will complain of other symptoms such as shortness of breath, dizziness, and nausea.
Medical Diagnosis
The diagnosis of an AMI is based primarily on the patient's history and the physical signs and symptoms. The AMI can be confirmed by laboratory evidence and ECG changes.
Cardiac MarkersTroponin.
Troponin T (cTnT) and troponin I (cTnI) are proteins released from cardiac muscle when the muscle is damaged. Troponin levels elevate in 3 hours after myocardial injury, peak in 24 hours, and remain in the circulation for up to 2 weeks (cTnI remains elevated for 5 to 7 days; cTnT for 10 to 14 days). Troponin levels may be drawn in the emergency room, helping to establish an early diagnosis.
Myoglobin.
Myoglobin is released within 1 hour after an acute myocardial infarction, and levels rise before CK-MB levels; therefore myoglobin levels can be helpful in the early diagnosis of AMI. Myoglobin levels will also be increased after strenuous exercise or renal failure and in the presence of neuromuscular disease.
Cardiac Enzymes.
A blood sample is drawn from anyone with prolonged chest pain to measure cardiac enzymes. With sustained ischemia, the cell membrane is impaired and enzymes are released from their intracellular location into the interstitial fluid. These enzymes can be measured in the serum and are assessed at regular intervals to confirm an AMI. CPK and its isoenzyme CPK-MB (myocardial) elevate rapidly with infarction. Beginning 4 to 6 hours after infarction, the CPK rises to 5 or more times the normal level within 12 to 24 hours and returns to normal in 2 to 3 days.
Electrocardiogram.
Changes in the normal waveform and dysrhythmias can be seen on an ECG. With ischemia, the ST segment is often depressed and the T wave is inverted. If there has been total occlusion of a coronary artery, the ECG will show ST elevation (STEMI). This is the more common occurrence. If there has been transient or partial occlusion of the artery, the ECG may not show ST elevation (NSTEMI). After infarction, another change often seen on the ECG waveforms is a significant Q wave (Fig. 35-8). A significant Q wave is one that is greater than one-third the height of the R wave. The most frequently observed dysrhythmias are premature ventricular contractions, ventricular tachycardia, and ventricular fibrillation.
Medical Treatment

The goals of medical therapy after an AMI are to limit the amount of cardiac muscle injury, to relieve symptoms, and to prevent or minimize complications.
Drug Therapy.
Sublingual or intravenous nitroglycerin is administered to dilate coronary arteries and increase blood flow to the damaged area. If the nitroglycerin relieves the pain, the infarction may not extend. Morphine sulfate is also used for chest pain. It has many effects in addition to analgesia. Morphine causes peripheral pooling of blood, which decreases the blood returning to the heart and lungs. It also diminishes anxiety, decreases tachypnea, and relaxes bronchial smooth muscles, thereby improving gas exchange. If the patient cannot tolerate morphine, meperidine (Demerol) may be ordered, but it does not have all the other beneficial properties of morphine and may increase the heart rate.
Oxygen is administered at 4 to 6 L/min to assist in oxygenating myocardial tissue to support pumping activity and to repair damaged tissue.
Fibrinolytic therapy is recommended for patients with STEMI (patients with total occlusion) (Ante, et al., 2004). Streptokinase and tissue plasminogen activator are administered intravenously or into the coronary arteries (during cardiac catheterization) to dissolve the thrombus. This treatment is most effective when initiated early but may be administered up to 12 hours from the onset of chest pain. The patient must meet strict criteria (no recent surgery or active bleeding; no history of a stroke; no bleeding disorders) and provide informed consent before the administration of fibrinolytics. After administration of the fibrinolytics, heparin is administered to prevent further clot formation.
FIGURE 35-8 Electrocardiographic changes with myocardial infarction.

Aspirin and beta-adrenergic blockers should be administered as soon as the patient can tolerate them and if not contraindicated. Beta-adrenergic blockers improve survival rates by decreasing the heart rate, reducing the work of the heart, and lessening the oxygen demand of the myocardium. ACE inhibitors may be prescribed for some patients to minimize the abnormal shaping or remodeling that can occur in the damaged ventricular muscle. Unstable patients may require dopamine or dobutamine, or both, as inotropic agents (Ante, et al., 2004). As the myocardium receives blood and oxygen, reperfusion dysrhythmias that require treatment may be noted.
Percutaneous Coronary Intervention.
Emergency percutaneous coronary intervention (PCI) is an option for treatment after AMI, either instead of fibrinolytic therapy or after fibrinolytic therapy (Ante, et al., 2004). There are several PCI procedures that can be performed in the cardiac catheterization laboratory: percutaneous transluminal coronary angioplasty (PTCA), intracoronary stent placement, atherectomy, laser angioplasty, and radiation therapy. PTCA involves passage of a catheter through a peripheral

artery (usually the femoral artery) into the occluded coronary artery. The tip of the catheter contains a balloon that is inflated to compress the atherosclerotic plaque and dilate the artery. PTCA is often utilized when there is single-vessel disease, non-calcified lesions, or lesions that are not at bifurcations. PTCA is not recommended for lesions of the left main coronary artery.
When appropriate, this procedure is preferred over coronary artery bypass surgery because it can be done under local anesthetic, it is less invasive, and the recovery time is faster. The procedure is safer than bypass surgery but is not without risks. Complications of PTCA include coronary artery dissection, dysrhythmias, coronary spasm, hematoma at the catheter site, restenosis, and death. In approximately 30% of patients, the vessel narrows again within 6 months.
Intracoronary stents are devices that are positioned within the blockage through a balloon-tipped catheter, expanded into place, and left to support the arterial wall. Over time, endothelial cells will completely line the inner wall of the stent to produce a smooth inner lining (Fig. 35-9). After an intracoronary stent is placed, the patient will be on antiplatelet or anticoagulant agents to decrease the chance of occlusion in the stent. Complications of stents are injury to the vessel wall and bleeding.
The coronary atherectomy is a procedure that widens the coronary artery by removing the atherosclerotic plaque using a device that shaves the plaque off the vessel walls.
FIGURE 35-9 Intracoronary stent.
A newer procedure is laser angioplasty. It uses a catheter with a laser on the tip. The laser is used to widen the lumen of the artery by destroying atherosclerotic plaque.
Radiation therapy is used primarily to treat restenosis of intracoronary stents. Radiation is delivered to the area of stenosis for several minutes. The patient requires no special precautions after the procedure related to the radiation.
Coronary Artery Bypass Graft Surgery.
Coronary artery bypass graft surgery may be performed to improve the blood supply to the myocardium. Arterial bypass surgery uses the patient's own vasculature as replacement for occluded coronary arteries. From one to six vessels may be bypassed. The saphenous veins and

the internal mammary artery are most commonly used. The saphenous veins are removed from one or both legs, inspected for patency, and reversed so that the valves do not inhibit blood flow. The replacement vessels are attached above and below the occlusions in the coronary arteries and serve as new conduits for oxygenated blood to the myocardium (Fig. 35-10). This is major surgery requiring the heart beat to be stopped and the patient to be placed on a cardiopulmonary bypass (CPB) machine during the surgery. The survival rate is higher in patients who are in stable condition.
Another approach to surgical revascularization is being used on patients requiring surgery on the arteries of the anterior heart. This procedure is called minimally invasive direct coronary artery bypass grafting and is performed through a small anterior thoracotomy incision. The patient's internal mammary artery is used to bypass the stenosed vessel, and the bypass is accomplished on a beating heart. The patient does not have to be placed on CPB. Postoperative care is similar to that of other cardiac surgery, although patients do not require as lengthy ventilatory support and total length of hospital stay is shorter.
A third option, off-pump coronary artery bypass (OPCAB), usually uses a full sternotomy incision (as with the traditional CABG) to provide the surgeon access to all coronary vessels (anterior and posterior). The OPCAB surgery is then accomplished on a beating heart without the use of CPB. Specially developed vacuum-assisted stabilizers are used by the surgeon to stabilize the graft site.
A new approach to CABG is done endoscopically. Called totally endoscopic CAB (TECAB), three tiny incisions are made on the patient's chest between ribs, and a small camera and two robotic arms are inserted. The surgeon sits at a console to view the surgical area and manipulates the robotic arms with his or her hands/wrists. The surgery is done on a beating heart, is less traumatic to the patient due to the small incisions, and is easier to recover from.
Another method of revascularization, used for patients with diffuse coronary vessel disease, is transmyocardial laser revascularization. Tiny holes are drilled in the myocardium using a laser, which helps provide collateral circulation to the ischemic myocardial muscle (Fig. 35-11).
FIGURE 35-10 Coronary artery bypass graft surgery.
NURSING CARE of the Patient with Acute Myocardial InfarctionAssessment
General assessment of the cardiac patient is summarized in Box 35-1. When a patient has AMI, be especially concerned with assessment of pain. When chest pain is present, early evaluation and treatment are paramount. Ask the patient to describe the pain, including type, location, duration, and severity. It is recommended that chest pain be assessed using the mnemonic PQRST.
P Precipitating factors, palliative: What was the patient doing when the pain began? Did anything make the pain better? Worse?Q Quality: Have the patient describe what the pain feels like (in his or her own words).
R Region, radiation: Where is the pain located? Does it hurt anywhere else?S Severity, symptoms: Have the patient rate the pain. Use the pain scale 0-10. Note other symptoms (e.g., nausea, diaphoresis).T Time: When did the pain start? How long did it last?
Record what the patient was doing when the pain started, what action was taken, and the effects of any actions or treatments. Inspect the patient's skin for color and palpate for temperature and moisture. Frequently assess vital signs. Document the mental status and level of anxiety. When cardiac monitoring is initiated, evaluate the rate and rhythm.
Nursing Diagnoses, Goals, and Outcome Criteria: Acute Myocardial InfarctionNursing Diagnoses Goals and Outcome Criteria
Anxiety related to feeling of impending doom, lack of understanding of routines
Reduced anxiety: patient statement of lessened anxiety, calm manner and self-care
Acute Pain related to lack of oxygen to the myocardium
Pain relief: patient statement of relieved pain, relaxed manner
Decreased Cardiac Output related to dysrhythmia and abnormal heart rate
Normal cardiac output: normal pulse, blood pressure, and cardiac rhythm
InterventionsAcute Pain
Administer analgesics as ordered, and monitor for relief of pain. Morphine is usually administered in small amounts (2 to 4 mg) intravenously every few minutes until pain relief is evident. Provide supplemental oxygen as ordered through nasal cannula at 2 to 4 L/min to provide adequate oxygen to the heart muscle. The head of the bed is usually elevated at least 30 degrees. Inform the physician if the patient has an increasing respiratory rate or dyspnea.
Decreased Cardiac Output
Monitor vital signs hourly or more frequently until stable. Monitor the ECG for changes in normal waveform (inverted T wave, ST elevation, and Q wave) and for dysrhythmias. Notify the physician of changes in the rhythm. In an intensive care unit, standing orders prescribe drug therapy for specific dysrhythmias. An intravenous line is usually established so that emergency drugs can be administered quickly and directly. Prompt treatment of dysrhythmias may prevent fatal alterations in rhythm. Monitor the patient for fluid volume excess (crackles, cough, jugular vein distention), and report any such evidence to the physician.
FIGURE 35-11 Transmyocardial laser revascularization.
Interventions to decrease demands on the heart include assisting the patient to rest, spacing activities and providing rest periods, providing adequate ventilation and oxygenation, relieving pain, and maintaining a calm, quiet environment.
Anxiety

Provide as calm an environment as possible. Explain procedures and equipment to the patient and family, using simple terms. Keep family members informed of the patient's progress. They can be helpful in calming the patient during the acute episode.
During the acute phase of AMI, provide simple explanations of the procedures and routines. Reinforce information given by the physician about the diagnosis and treatment. Patient teaching is especially important in the rehabilitation phase.
Cardiac Rehabilitation
As soon as the patient is stable, begin rehabilitation by teaching the patient and family about exercise, medications, and diet. If surgical intervention has been proposed, you may also teach the patient about that procedure.
The purpose of rehabilitation is to minimize the risk of repetition of adverse cardiac events. The goal of rehabilitation is to enable patients to attain the highest level of wellness and work ability.
The program is individualized to the patient for maximal success. The four phases of cardiac rehabilitation are (1) inpatient management; (2) immediately after discharge, using telemetry monitoring during exercise; (3) later rehabilitation, which is unmonitored; and (4) maintenance. A team of medical professionals (e.g., nurse, physician, physical therapist, nutritionist, social worker) plans the individual program. Education during the rehabilitation process should include normal anatomy and physiology of the heart; pathophysiology of coronary artery disease, angina, and AMI; risk factor modification; activity and exercise; medications; diet; and when to seek medical advice. See the Nutrition Concepts box below for a discussion of dietary considerations for patients with heart disease.
Patient Teaching PlanAcute Myocardial Infarction
After AMI, the following are some key points in the discharge teaching plan:
•It is very important to take your medications as prescribed and to contact the physician if you have any problems. (Provide written information about drug names, dosages, purpose, interactions with other medications and foods, and adverse effects that should be reported.)
•Your physician may prescribe a low-fat, low-sodium diet to decrease weight and to reduce the workload on your heart.
•Participation in cardiac rehabilitation will help you become active again in a safe manner.
•Stop smoking. Smoking stimulates the heart rate and causes blood vessels to constrict, which makes the heart work harder.
•Maintain normal weight (or lose weight if obese) to decrease the work of the heart. •The local chapter of the American Heart Association is a helpful resource for
information and guidance on diet, smoking cessation, and exercise.

Put on Your Thinking Cap!A new patient is being seen in the physician's office. Basic information and health history data include the following: 58-year-old white male, height 599°, weight 190 lbs; vital signs: T, 98° F; P, 82; R, 14; BP, 152/84.SOCIAL HISTORY
Real estate salesman (describes himself as “pretty successful” and able to maintain a good quality of life). Plays tennis 3 times a week; walks 2 miles, 4 times a week. Divorced father of three adult children; one son who recently was admitted to rehabilitation for substance abuse has no insurance. Patient has conflict with ex-wife related to son's situation. Enjoys a “few beers” in the evening. Has eggs, bacon, biscuits, coffee for breakfast, has lunch (sandwich, fries) at fast-food restaurant, and cooks dinner (usually “meat and potatoes”). Sleeps 7 to 8 hrs; usually rested on arising. Some recent trouble sleeping because of son's problems. No current significant other.
HEALTH HISTORY
Hypertension for 5 years treated with daily antihypertensive drug; chronic sinusitis; arthritis in left knee related to sports injury.
FAMILY HISTORY
Mother, age 78, living and in moderately good health. Had mild stroke last year without permanent effects. Has diabetes. Father died suddenly at age 66 of acute myocardial infarction. Two living brothers, ages 52 and 49. Both are hypertensive.
ANALYSIS
1. Based on the data available, identify modifiable and unmodifiable risk factors for coronary artery disease.
2. Identify one strategy to address each modifiable factor. 3. Identify current factors that reduce his risk of coronary artery disease.
HEART FAILURE
Heart failure is the inability of the heart to meet the metabolic demands of the body. The pumping ability of the heart is ineffective.
Etiology and Risk Factors
Heart failure (HF) is the preferred term used to describe the clinical picture of failure. Congestive heart failure (CHF) is a commonly used term for heart failure; it describes the symptoms seen when the heart fails to pump effectively and blood “backs up” into the vasculature of the lungs, producing congestion. The two terms (HF and CHF) are often used interchangeably in the clinical setting. Causes of heart failure are primarily of two types: disorders that increase the workload of the heart and disorders that interfere with the pumping ability of the heart. Therefore patients at risk for HF include those with CAD, AMI, cardiomyopathy, hypertension, COPD,

pulmonary hypertension, anemia, disease of the heart valves, and fluid volume overload. Other conditions that increase metabolic needs, such as fever and pregnancy, may also precipitate heart failure. Approximately 4.9 million Americans have heart failure and over half a million new cases of heart failure are diagnoses every year. After age 65, 10 of every 1000 individuals have heart failure, and 75% of heart failure patients have a history of hypertension (American Heart Association, 2007).
Nutrition Concepts
1. A major part of treatment for people with heart disease is reduction of fat and cholesterol in the diet.
2. When fats are used in cooking or eating, unsaturated fats (vegetable oil such as corn oil, canola oil, or olive oil) should be substituted for saturated fats (animal fat such as butter or lard).
3. Fats and oils used in cooking or eating should be limited to five to eight servings daily in normal adults.
4. Saturated fat can be limited by eating only 5 to 7 ounces of meat daily. 5. Foods that contain omega-3 fatty acids (certain fish, walnuts, and soybeans) lower
serum triglycerides and decrease the number of deaths resulting from heart disease.
Pathophysiology
The LV, RV, or both fail as pumps. Usually the left side of the heart fails first. In time, the right side fails as a result of the left-sided failure. Heart failure can be classified as systolic HF resulting from ineffective pumping of the ventricles or as diastolic HF resulting from impaired filling of the ventricles. With either classification, cardiac output is decreased. Heart failure can occur acutely, with onset over several hours or days, or it can be chronic, with onset over months to years.
Compensation.
Compensation is a term used to describe the cardiac and circulatory adjustments that maintain or restore cardiac output to normal or near normal. Compensation occurs through three mechanisms: sympathetic nervous system stimulation, regulation of blood volume by the kidneys, and enlargement of the ventricular myocardium.
Sympathetic Compensation.
The sympathetic nervous system responds to decreased cardiac output and blood pressure. Catecholamines are released that increase heart rate, stroke volume, cardiac output, and venous tone. Increased venous tone increases systemic vascular resistance, venous return, and ventricular filling.
Renal Compensation.

The second mechanism that responds to decreased cardiac output is renal compensation. When cardiac output falls, so does renal perfusion. This initiates the renin-angiotensin-aldosterone (RAA) mechanism. Renin, secreted by the kidneys, activates angiotensinogen to convert to angiotensin I. Angiotensin I is converted to angiotensin II, which causes vasoconstriction and triggers release of aldosterone. Vasoconstriction raises the blood pressure by increasing peripheral resistance to blood flow. Aldosterone causes the kidneys to retain sodium and water, which increases blood volume.
Natriuretic Peptides.
Natriuretic peptides are neurohormonal substances released with heart failure. Atrial natriuretic peptide (ANP) is released in response to increased volume and stretch in the cardiac atria. B-type natriuretic peptide (BNP) is released when the cardiac ventricles stretch, usually from increased blood volume. The natriuretic peptides are thought to counter the vasoconstrictive and volume-increasing effects of the SNS and RAA systems. BNP levels can be measured in the blood and can be used as a diagnostic tool for HF (Saul & Shatzer, 2003).
Ventricular Hypertrophy.
The final mechanism is enlargement of the ventricular myocardium, called ventricular hypertrophy, which results from strain. The increased blood volume raises the pressure in the ventricles, which can also cause the ventricles to dilate. The ventricle changes in size and shape, which impairs pumping effectiveness. This process is called ventricular remodeling.
After a period, the compensatory mechanisms may no longer be able to meet the increased demands. Contractility decreases; the heart muscle can stretch just so far before becoming inefficient. The force of contraction of the LV decreases. Stroke volume and cardiac output decrease as pumping action fails. Afterload increases with left-sided heart failure. Blood backs up in the LA and then the pulmonary veins. Because of the high pressure in the pulmonary veins (pulmonary hypertension), fluid leaks from the capillaries, causing pulmonary edema. Pulmonary hypertension eventually causes the right side of the heart to fail as well. Then, blood returning to the heart from the body meets resistance, which causes systemic pressure to rise. This results in peripheral edema and enlargement of the liver and spleen. If heart failure is not corrected, death eventually ensues.
With left-sided HF, there is increased left ventricular end-diastolic pressure, increased left atrial pressure, increased pulmonary pressure, and resulting pulmonary edema as the excess fluid leaks into the lung tissues. In right-sided HF, right ventricular pressure increases, right atrial pressure increases, and fluid accumulates in the systemic vasculature.
Put on Your Thinking Cap!
1. Explain why a patient with heart failure might (1) feel anxious, and (2) gain weight. 2. A patient with heart failure is advised to try to lose 30 pounds. What nursing strategies
would help her achieve this goal?

3. You suspect that a patient with HF and hypertension is not taking her blood pressure medication regularly as prescribed. What strategies might improve her compliance?
Signs and Symptoms
The patient with left-sided heart failure is typically very anxious, pale, and tachycardic. Consecutive blood pressure readings may show a downward trend. Auscultation of the lung fields may reveal crackles, wheezes, dyspnea, and cough. When assessing heart sounds, S3 and S4
may be heard as a result of the backup of fluid and the heart's inability to handle the excess fluids.
With right-sided heart failure, there is increased central venous pressure, jugular venous distention, abdominal engorgement, and dependent edema. Anorexia, nausea, and vomiting may result from the abdominal engorgement. Fatigue, weight gain, and decreased urinary output are common complaints.
Medical Diagnosis
The diagnosis of HF is made on the basis of the history, physical examination, radiographs, and laboratory test results. A chest radiograph may reveal hazy lung fields, distended vasculature, and cardiomegaly. An echocardiogram may reveal heart enlargement and ineffective ventricular contraction. Laboratory tests indicative of HF are decreased serum sodium and Hct from hemodilution and decreased saturated arterial oxygenation from poor pulmonary perfusion. The blood urea nitrogen (BUN) and creatinine are elevated with decreased renal function. BNP levels are elevated in HF, and the higher the levels, the more severe the failure. Liver function test results are elevated with hepatomegaly (liver enlargement). The patient who is critically ill with HF may require more intensive monitoring of hemodynamics parameters.
Medical Treatment
Medical treatment includes management of the underlying cause, drug therapy to improve cardiac output and eliminate excess fluid, and conservative measures to decrease demands on the heart. Sodium restriction is prescribed for most HF patients.
Treatment of the underlying problem may involve such interventions as correction of dysrhythmias, management of hypertension, and valve replacement or repair.
Drug Therapy.
A number of drugs are used to treat heart failure. Current recommendations include ACE inhibitors, diuretics, beta-adrenergic blockers, inotropic agents, cardiac glycosides, and nitrates. In addition, certain patients will benefit from B-type natriuretic peptide. ACE inhibitors decrease preload and afterload by blocking the RAA system, resulting in vasodilation, decreased blood volume, and lower blood pressure. In addition, ACE inhibitors are thought to limit the progression of ventricular remodeling. Diuretics are prescribed to decrease circulating fluid volume and decrease preload. Loop diuretics such as furosemide (Lasix) are usually used in HF.

Spironolactone, a weak potassium-sparing diuretic, may be prescribed for some patients because it acts by blocking aldosterone and may slow the process of remodeling. Beta-adrenergic blockers improve survival rates by decreasing the heart rate, reducing the work of the heart, and lessening the oxygen demand of the myocardium. Inotropic agents such as dopamine, dobutamine, and amrinone are prescribed to improve cardiac contractility, improve renal perfusion and decrease fluid retention. Digoxin, a cardiac glycoside with inotropic effects, is prescribed to improve pump function by increasing contractility and decreasing heart rate. Nesiritide (Natrecor) is a recombinant human B-type natriuretic peptide that is often prescribed in patients with decompensated HF. Nesiritide counteracts the vasoconstriction and fluid retention of the RAA system and relieves the severe dyspnea seen in these patients. Nitrates, such as NTG, are venodilators and reduce preload for patients with HF. This helps reduce the workload on the heart. Morphine may be used to decrease anxiety, dilate the vasculature, and reduce myocardial oxygen consumption in the acute stage. The Drug Therapy table on pp. 642 to 646 provides additional information about drugs used to treat HF.
Other Therapy.
Other therapies are available for decreasing cardiac workload and increasing myocardial oxygenation. The intra-aortic balloon pump (IABP), ventricular assist devices (VADs), and biventricular pacing may be utilized. The intra-aortic balloon pump is a temporary device used in the intensive care unit to increase cardiac output and coronary artery perfusion. VADs can partially or completely support a patient's failing heart. Currently considered a temporary intervention, VADs are used as a “bridge” to transplantation. Biventricular pacing is useful in approximately 30% of HF patients who have conduction delays in the right or left bundle branch. These conduction delays result in the ventricles being depolarized and contracting out of synchrony. This reduces cardiac output and can contribute to the worsening of HF. In biventricular pacing, leads are placed in both ventricles and they are stimulated at the same time. Cardiac contraction occurs in both ventricles at the same time and cardiac output is improved (Lagrotteria, 2003).
Surgery.
Coronary artery bypass grafting is recommended in HF patients who experience angina. Valve repair or replacement is recommended when valve dysfunction contributes to the HF. Partial left ventriculectomy may be useful in some patients. Cardiac transplantation is often the last option for patients with end-stage HF whose symptoms are not responding to conventional therapy.
Complications
Dysrhythmias, pulmonary edema, and cardiogenic shock are possible complications.
NURSING CARE of the Patient with Heart FailureAssessment
Complete assessment of the cardiac patient is outlined in Box 35-1 (see also Nursing Care Plan: The Patient with Heart Failure on p. 663). It is especially important to assess heart sounds, rate,
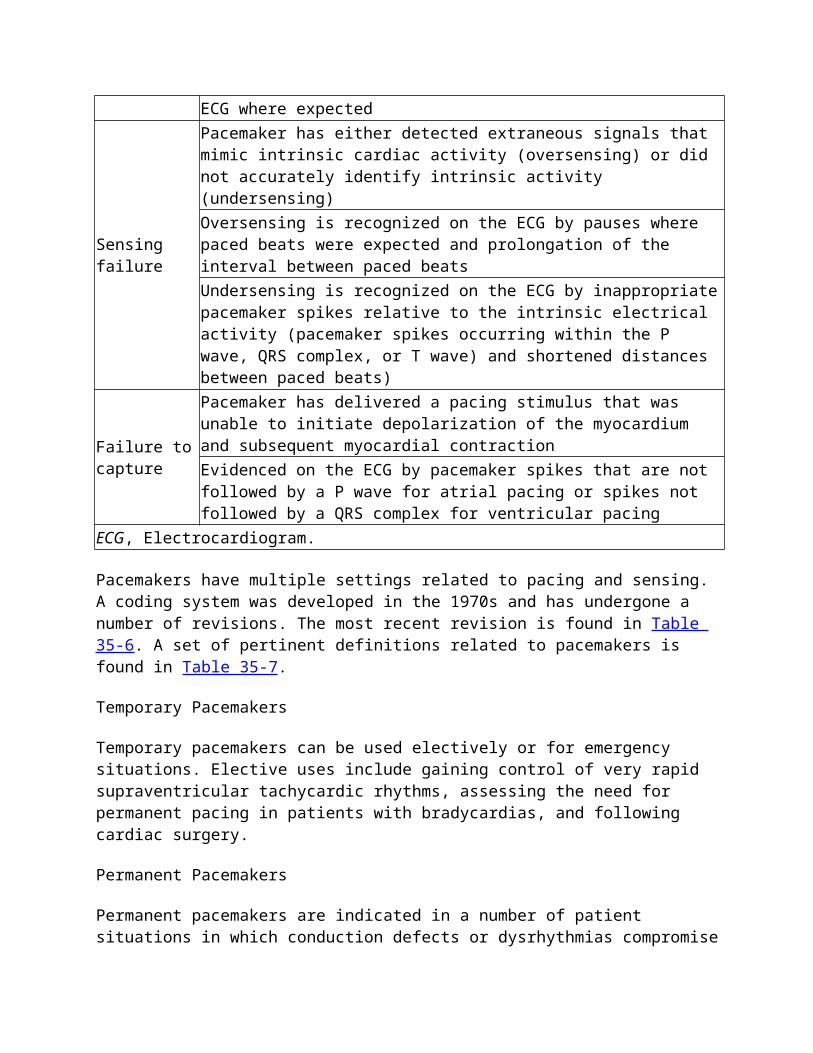
and rhythm. The point of maximum impulse is noted. Assess the apical and radial pulses frequently. Inspect for jugular vein distention. A baseline respiratory assessment of rate, rhythm, and breath sounds is vital. Measure weight and blood pressure accurately. Inspect the skin and palpate for turgor and edema. Intake and output records and daily weights may be done to evaluate fluid retention or loss. If ordered, take central venous pressure and hemodynamic readings as well. If cardiac monitoring is done, observe for dysrhythmias. Nurses who work in intensive care units routinely interpret ECGs. Interpretation is discussed on pp. 673 to 675.
Nursing Diagnoses, Goals, and Outcome Criteria: Heart FailureNursing Diagnoses Goals and Outcome Criteria
Fluid Volume Excess related to ineffective cardiac pumping
Normal fluid volume: no edema or dyspnea, blood pressure consistent with patient norms
Impaired Gas Exchange related to decreased pulmonary perfusion
Adequate oxygenation: clear breath sounds, respiratory rate 12 to 20/min without dyspnea
Anxiety related to edema and difficulty breathing
Reduced anxiety: patient statement of reduced anxiety, calm manner
Decreased Cardiac Output related to mechanical failure
Improved cardiac output: normal heart rate and rhythm, fluid intake and output equal
Activity Intolerance related to inability to meet oxygen demands
Increase activity tolerance: performance of activities of daily living without fatigue
InterventionsDecreased Cardiac Output
Give medications as ordered, and monitor the patient for therapeutic and adverse effects. Older adult patients are more susceptible to adverse drug effects because they may metabolize and excrete drugs more slowly. This is especially true when the older patient is taking digitalis. Advise the patient to report early signs of digitalis toxicity: anorexia, nausea, and visual disturbances. Bed rest and stress reduction decrease the cardiac workload. When the patient is acutely ill, eliminate unnecessary activity. Give partial baths rather than complete bed baths. Assist the patient to change positions at least every 2 hours so that the skin can be inspected for signs of pressure. Visitors may be permitted, but advise them to sit quietly with the patient for short periods.
NURSING CARE PLANThe Patient with Heart FailureASSESSMENT
Health History: A 73-year-old Chinese-American woman is admitted through the Emergency Department. She is a retired business owner who lives alone and has no immediate family in the area. She began having dyspnea and orthopnea that has become progressively worse over the past 3 days. Her past medical history includes a myocardial infarction 1 year ago and a 10-year history of hypertension treated with diet and verapamil 240 mg daily. In addition to the

verapamil, she takes only an occasional laxative. She complains of fatigue, restlessness, nervousness, irritability, insomnia, anorexia, and a productive cough with pink sputum.
Physical Examination: Vital signs: temperature 98° F orally; pulse 104, slightly irregular; respirations 24; blood pressure 168/96. Height 5′2′; weight 152 lbs (a 7-lb increase in 1 week). She is alert but appears anxious. Her skin is pale and diaphoretic. An S3 is present. Jugular vein distention is noted. Auscultation of the lungs reveals crackles in the lower lobes of both lungs. The abdomen is distended. Bowel sounds are present in all four quadrants. There is 3+ pitting edema in both feet and ankles.
She is being admitted to the telemetry unit for treatment, where she will have continuous electrocardiography and be placed on oxygen.
Nursing Diagnosis Goals and Outcome Criteria Interventions
Decreased Cardiac
The patient's cardiac output will improve, as evidenced by normal heart rate and rhythm, normal blood pressure, normal hemodynamic measure, and breath sounds clear to auscultation.
Monitor vital signs, heart and lung sounds, level of consciousness, electrocardiography. Enforce bed rest with head of bed elevated. Schedule activities to allow rest. Request small, frequent meals. Administer cardiotonics, vasodilators, and ACE inhibitors as ordered.
Output related to decreased myocardial contractilityFluid Volume Excess related to decreased glomerular filtration rate, increased aldosterone, sodium and water retention, and increased antidiuretic hormone release
The patient will have normal fluid balance as evidenced by weight of 145 lbs, absence of edema, absence of crackles and wheezes in lungs, and ability to participate in activities of daily living without dyspnea.
Monitor for jugular venous distention and peripheral edema. Auscultate heart and lung sounds q 4 hr. Measure weight daily and intake and output accurately. Maintain intravenous lines and correct fluid infusion rate. Administer diuretics as ordered. Teach about sodium restriction and rationale. Protect edematous extremities from pressure or injury.
Impaired Gas Exchange related to pulmonary congestion
The patient's gas exchange will be evidenced by pulse oximetry >95%, normal skin color, absence of dyspnea, and clear lung sounds.
Assess lung sounds and respiratory status q 4 hr. Monitor O2 saturation. Elevate head of bed. Administer oxygen as ordered. Assist to cough and deep breathe q 2 hr. Administer diuretics and morphine sulfate as ordered.
Activity Intolerance related to imbalance between oxygen supply and demand
The patient's activity tolerance will improve, as evidenced by performance of activities of daily living without excessive fatigue or dyspnea.
Assess response to activity when permitted. Monitor for dyspnea, changes in vital signs. Limit fatiguing activities. Gradually increase activity as tolerance improves.

Nursing Diagnosis Goals and Outcome Criteria Interventions
Anxiety related to hypoxia, life-threatening situation
The patient's anxiety will be reduced, as evidenced by calm demeanor and statement that she feels less anxious.
Explain procedures and equipment. Tell patient about congestive heart failure and how it is being treated. Point out signs of improvement. Visit often, and respond to call bell promptly. Offer spiritual counselor if desired.
Deficient Knowledge of condition, treatment, self-care, and resources
The patient will verbalize information about her condition, treatment, self-care measures, and resources.
Provide simple explanation of congestive heart failure, its effects, and its treatment. As discharge nears, discuss diet, exercise, and drug therapy. Explain signs and symptoms that should be reported to physician. Advise of services of American Heart Association for information. Explore sources of support and need for visiting nurse or home health services.
CRITICAL THINKING QUESTIONS
▪ What is the rationale behind sodium restriction in patients with heart failure? ▪ Describe three signs of improvement in a patient with heart failure.
Pharmacology Capsule
Before each dose of digitalis, the apical pulse is counted for 1 full minute. If the heart rate is less than 60 bpm, the drug is withheld and the physician is notified.
Pharmacology Capsule
The most common adverse effects of diuretic therapy are fluid and electrolyte imbalances.
Impaired Gas Exchange
Hypoxia is a common finding with left-sided heart failure because of pulmonary edema. It is common with right-sided heart failure because of decreased blood flow to the lungs. The patient with HF usually breathes more easily in a semi- or high-Fowler's position. Elevation of the upper body facilitates breathing by reducing pressure of the abdominal organs on the diaphragm. Supplemental oxygen is usually prescribed at 4 to 6 L/min per nasal cannula. The flow rate is reduced to 2 L/min for patients with chronic hypoxia. Assess respiratory status and blood gases frequently.
Prescribed bed rest can lead to other pulmonary complications related to immobility: hypostatic pneumonia and pulmonary emboli. Teach the patient to cough and deep breathe at least every 2 hours to promote respiratory excursion and to mobilize secretions. Other interventions to prevent complications of immobility are detailed in Chapter 21.

On discharge, the physician may order portable oxygen for use at home. The nurse or a respiratory therapist instructs the patient in the use of the equipment and the safety precautions to take when using oxygen (see Chapter 30).
Fluid Volume Excess
Fluid retention is a response to HF, an attempt to maintain normal cardiac output. Unfortunately, it compounds the problem by increasing the workload on the heart. Therefore measures are taken to reduce the fluid volume to normal while improving the function of the heart. Administer diuretics as ordered, and monitor the patient for adverse effects. The most common adverse effects of diuretic therapy are fluid and electrolyte disturbances. Signs and symptoms that may indicate fluid or electrolyte disturbances include cardiac dysrhythmias, muscle weakness or twitching, cramps, changes in mental status, and abdominal distention. Frequent serum electrolyte measurements are usually ordered. Note the results and notify the physician of abnormal findings. If hourly urine output is being measured, report an output of less than 30 mL/hr to the physician as well. The patient should be weighed daily.
An intravenous catheter is usually placed to provide a line for drug administration. If intravenous fluids are administered, monitor the rate of administration very carefully. If fluid retention is not relieved by other means, fluid restriction may be instituted. All staff should know the exact amount of fluid allowed and must record all intake. Fluid restriction can be very uncomfortable for the patient. Even with fluid volume excess, the patient may feel thirsty because of electrolyte imbalances. Present oral fluids in small containers, and offer them at reasonable intervals. Frequently provide mouth care. The patient and family must understand why fluids are restricted so that the patient does not exceed the prescribed intake.
The most common therapeutic dietary measure for CHF is sodium restriction. The patient may be limited to 2 g of sodium/day. In severe cases, a limitation of 500 to 1000 mg/day may be prescribed. Reduced sodium intake decreases fluid retention, thereby reducing the cardiac workload. For a 2-g sodium diet, advise the patient to avoid foods high in sodium (a list should be provided), not to add salt before or after cooking, and to use no more than 2 cups of milk products daily. Patients often have difficulty changing their use of seasonings. Acknowledge the difficulty, and explain how sodium limitation contributes to improvement of cardiac function.
It is best to identify the type of diet to be prescribed on discharge as early as possible. This allows time for a dietary consultation to be arranged, which should be followed by reinforcement by the nurse. The person who prepares the patient's meals at home must be included in the teaching sessions.
Activity Intolerance
Frequent rest periods, pacing of activities, and relaxation techniques help the patient conserve energy. As the fluid volume is decreased and the cardiac output is increased, the patient can expect to be less fatigued.

The patient may be referred to a rehabilitation facility for exercise training. In general, the patient is advised to plan rest periods before and after tiring activities. Activity should be increased gradually, with rest periods taken when fatigue or dyspnea occurs. The physician may prescribe vasodilators for patients who experience chest pain with some activities. If monitoring is indicated after discharge, request a referral to a home nursing agency.
Instruct the patient to notify the physician if the following problems develop: increasing dyspnea or edema, excessive fatigue, or pain that is not relieved by rest or prescribed medications. Early recognition of signs and symptoms that the patient's condition is deteriorating is crucial to avoiding rehospitalization (see the Health Promotion Considerations box above). In addition, advise the patient to avoid smoking and smoky environments and to refrain from wearing constricting clothing on the lower extremities.
Health Promotion ConsiderationsHeart Failure: Discharge Instructions
A major goal for heart failure patients is to prevent rehospitalization. A critical factor in reaching this goal is for the patient or family member to recognize early signs and symptoms of worsening failure and to contact their provider. Examples of what to call about are the following: difficulty breathing (especially with activity); dry, hacking cough; weakness, increased fatigue; foot/ankle swelling; dizziness; and weight gain of 3-5 lbs in a week or less.
Anxiety
Factors that may cause the patient to become anxious are dyspnea, unfamiliar setting and routines, and uncertainty about what is happening. Acknowledge the patient's anxiety and attempt to identify the basis. While taking immediate measures to relieve dyspnea, calmly explain what is being done. It may be helpful to tell the patient how specific measures help relieve symptoms. The presence of family members may have a calming effect if the relatives understand that they, too, must remain calm.
Patient Teaching PlanChronic Heart Failure
• Reducing sodium in your diet will help control swelling and reduce the workload on your heart.
• Excess weight makes your heart work harder. Your physician may prescribe a weight-loss diet for you.
• Take your medications as prescribed to improve your heart function. (Provide written information about drug names, actions, dosage, schedule, side and adverse effects, special aspects of administration, and interactions with other medications and food.)
• Gradually increase your activity. Avoid activity that causes shortness of breath or severe fatigue.
• Weigh yourself each morning, before breakfast, on the same scale and with the same amount of clothing.

• Contact your physician if you gain 2 or more pounds in a week, develop a persistent cough, or have shortness of breath or chest pain.
• Resources: The American Heart Association provides information about diet and exercise. The Visiting Nurses Association or a home health agency can monitor your home.
Pharmacology Capsule
Older adults are more susceptible to adverse drug effects because they metabolize and excrete drugs more slowly.
INFLAMMATORY DISORDERS
Inflammation of the heart most often results from systemic infections. The endocardium, myocardium, and pericardium may be affected.
Infective EndocarditisEtiology and Risk Factors
Microbial infections of the endocardium affect primarily the valves. Organisms present in the blood easily colonize valves damaged by rheumatic heart disease or congenital defects or a mitral valve that is prolapsed.
Although the incidence of infective endocarditis (IE) has decreased with the use of antibiotics, there has been a resurgence of the problem in intravenous drug abusers. The more frequent use of invasive intravascular catheters for severely compromised patients has also contributed to the frequency with which IE occurs.
Patients with known valvular disease are also at risk for IE. They should be treated with prophylactic antibiotics before dental or invasive procedures. Immunosuppression or any source of bacterial contamination (lacerations, pneumonia, invasive procedures, intravenous drug use with contaminated needles) places patients at risk.
Pathophysiology
Pathogens, usually bacteria, enter the bloodstream by any of the previously mentioned means. The pathogen accumulates on the heart valves and/or the endocardium and forms vegetations. The mitral valve is the most common site for these vegetations. The turbulence of the blood flow through the heart weakens the vegetations and causes pieces to break off. These emboli can then obstruct circulation and impair tissue perfusion in the lungs, brain, kidneys, and heart.
Complications
Complications of IE include HF and embolization. HF is the most frequent cause of death with IE.

Signs and Symptoms
Patients usually present with fever, chills, malaise, fatigue, and weight loss. The fever may be low grade (37.2° to 38.9° C [99° to 102° F]) or higher (38.9° to 40.6° C [102° to 105° F]). The fever is accompanied by chills and night sweats. Chest or abdominal pain may be reported, possibly indicating embolization. Vegetative fragments and microembolizations can produce petechiae inside the mouth and on the ankles, feet, and antecubital areas. Pea-size, tender, red-to-purple lesions known as Osler's nodes may be on the patient's fingertips or toes.
Medical Diagnosis
The diagnosis of IE is based on the history, physical examination, and results of laboratory studies. A history of recent dental or surgical procedures may precede IE. Auscultation may reveal a heart murmur. Echocardiography helps visualize lesions and valvular regurgitation. Right-sided or left-sided heart failure may be evident. Serial blood cultures may give clues to the causative organism or organisms. The WBC count may be elevated.
Medical Treatment
Antimicrobials, rest, and limitation of activities are the primary therapeutic measures for IE. Antimicrobials are given intravenously for 2 to 6 weeks, depending on the organism. The patient is usually hospitalized for at least 1 week and then receives home intravenous therapy if that is available. Prophylactic anticoagulants may be necessary. Surgery may be necessary to replace an infected valve.
NURSING CARE of the Patient with Infective EndocarditisAssessment
Complete assessment of the cardiac patient is summarized in Box 35-1. With IE, review the patient's history for risk factors, recent invasive procedures, known pathologic cardiac conditions, and onset of symptoms. Assess for temperature elevation, heart murmur, evidence of HF (cough, peripheral edema), and embolization.
Nursing Diagnoses, Goals, and Outcome Criteria: Infective EndocarditisNursing Diagnoses Goals and Outcome Criteria
Decreased Cardiac Output related to impaired valve function
Normal cardiac output: normal pulse and blood pressure
Impaired Physical Mobility related to fatigue and prolonged intravenous therapy
Resumption of usual physical activities without symptoms: performance of activities of daily living without fatigue
Ineffective Tissue Perfusion related to embolization
Normal tissue perfusion: absence of dyspnea or signs of circulatory obstruction
Interventions
Administer prescribed antibiotics. Throughout the course of the illness, continue to assess cardiac output and monitor for complications. Teach the patient about the medications prescribed and any restrictions imposed. Encourage adequate rest, which is necessary during the healing process. Range-of-motion exercises may be necessary during the acute stage and until the patient is ambulatory.
PericarditisEtiology and Risk Factors
Pericarditis is an inflammation of the pericardium. It may be a primary disease or associated with another inflammatory process. The disease may be acute or chronic. Acute pericarditis is caused by viruses, bacteria, fungi, chemotherapy, or AMI (Dressler's syndrome). Chronic pericarditis is caused by tuberculosis, radiation, or metastases.
Pathophysiology
In acute pericarditis, the inflammatory process causes an increase in the amount of pericardial fluid and inflammation of the pericardial membranes. In chronic pericarditis (also called constrictive pericarditis), scarring of the pericardium fuses the visceral and parietal pericardia together. Loss of elasticity results from the scarring. This constrictive process prevents adequate ventricular filling.
Complications
The major complication of pericarditis is pericardial effusion or accumulation of fluid in the pericardial space. This may lead to cardiac tamponade when sufficient fluid accumulation decreases ventricular filling. The resulting drop in cardiac output is an emergency. It is treated with pericardiocentesis to remove the accumulated fluid.
Signs and Symptoms
Chest pain is the hallmark symptom of pericarditis. The pain is most severe on inspiration. It is most often sharp and stabbing but may be described as dull or burning. It is relieved by sitting up and leaning forward. Dyspnea, chills, and fever accompany pericarditis. ST segment elevation may be noted on the ECG. A pericardial rub may be present. Slowly progressing pericardial effusion does not result in hemodynamic compromise until 400 to 500 mL of fluid has accumulated. Rapidly accumulating fluid may precipitate sudden symptoms with only 250 mL of fluid.
Medical Diagnosis
The diagnostic challenge is to differentiate pericarditis from AMI. Serial ECGs show that the ST segment elevation resolves in several weeks. QRS voltage may decrease because of the accumulated fluid in the pericardial space. An echocardiogram may show pericardial thickening and effusion. Atrial fibrillation may occur because of the irritation. The CPK-MB may be elevated. Blood cultures may identify the causative organism or organisms. One differentiating
feature to consider is that ischemic chest pain or angina is not relieved by position change and the chest pain that accompanies pericarditis often is relieved by change in position.
Medical Treatment
The patient is treated with analgesics, antipyretics, anti-inflammatory agents, and antibiotics. With constrictive pericarditis, the patient would be treated as for HF. Surgical creation of a pericardial window (removal of a segment of parietal pericardium to allow continuous drainage of pericardial fluid) may be necessary for treating chronic pericarditis with effusion.
NURSING CARE of the Patient with PericarditisAssessment
General nursing assessment of the cardiac patient is summarized in Box 35-1. With pericarditis, assessment of heart sounds is especially important.
Nursing Diagnoses, Goals, and Outcome Criteria: PericarditisNursing Diagnoses Goals and Outcome Criteria
Acute Pain related to pericardial inflammation
Pain relief: patient statement that pain is reduced, relaxed manner
Decreased Cardiac Output related to pericardial constriction
Improved cardiac output: normal pulse and blood pressure
Anxiety related to illness Decreased anxiety: patient statement that anxiety is reduced, calm manner
Interventions
Rest and reduction of activity decrease the workload of the heart. Administer medications and teach the patient about the medications. Emotional support from the nursing staff and significant others is vital. The patient can be instructed in relaxation techniques. Monitor vital signs and auscultate for a pericardial friction rub. The rub is heard during inspiration with the diaphragm of the stethoscope placed between the second and the fourth intercostal spaces at the left sternal border. It is heard when there is no fluid accumulation. Distant heart sounds may be heard when there is fluid accumulation. Note pain characteristics and response to analgesics and anti-inflammatory agents. Monitor the ECG for dysrhythmias.
What Does Culture Have to Do with Cardiomyopathy?
African-American males are at increased risk for dilated cardiomyopathy. Be alert to complaints of decreasing exercise tolerance and dyspnea in this population.
FIGURE 35-12 Cardiomyopathy. A, Dilated cardiomyopathy. B, Hypertrophic cardiomyopathy. C, Restrictive cardiomyopathy.
CARDIOMYOPATHYEtiology and Risk Factors

Cardiomyopathy (CMP) is disease of the heart muscle. The cause of CMP is often unknown or CMP may be secondary to another disease process. The disease usually leads to heart failure. Three types of cardiomyopathy are recognized: dilated, hypertrophic, and restrictive (Fig. 35-12). Dilated cardiomyopathy is the most common type, accounting for 87% of cases (American Heart Association, 2007). There are three risk factors associated with dilated CMP: excessive use of alcohol, pregnancy, and infections. A relatively poor prognosis exists for dilated cardiomyopathy, with a 50% mortality in 5 years. Hypertrophic CMP often results from valvular heart disease or HTN. There also appears to be a genetic autosomal dominant link. Hypertrophic CMP is more common in younger individuals; approximately 36% of young athletes who died suddenly were found to have hypertrophic CMP. Restrictive cardiomyopathy is the least common type of CMP. Amyloidosis, sarcoidosis, and other immunosuppressive disorders may predispose individuals to restrictive cardiomyopathy.
Pathophysiology
With dilated cardiomyopathy, there is dilation of the ventricle and severely impaired systolic function. This causes decreased contractility, decreased ejection fraction and stroke volume, and increased left ventricular end-diastolic pressure. Pressure backup results in dilation of all four chambers and is most pronounced in the ventricles. Left ventricular failure and resulting HF are seen as the result of excessive back pressure (see Fig. 35-12, A ).
In hypertrophic cardiomyopathy, the LV hypertrophies and there is thickening of the ventricular septum. The left ventricular capacity decreases, and the outflow track of the left ventricle is decreased in size. The size of the LA increases as a result of the back pressure. The exterior heart size may appear to be normal. Ventricular dysrhythmias are common (see Fig. 35-12, B ).
In restrictive cardiomyopathy, the myocardium becomes rigid and noncompliant. This reduces ventricular filling and cardiac output. Pulmonary and systemic congestion result (see Fig. 35-12, C).
Signs and Symptoms
Dilated cardiomyopathy is a progressive, chronic disease. The onset is gradual, with dyspnea, fatigue, left-sided heart failure, and moderate-to-severe cardiomegaly. Mitral valve regurgitation and S3 and S4 sounds are evident.
With hypertrophic cardiomyopathy, the progression of symptoms is slow. Dyspnea, orthopnea, angina, fatigue, syncope, palpitations, ankle edema, and S4 sounds are found.
With restrictive cardiomyopathy, the primary symptom is exercise intolerance. Dyspnea, fatigue, right-sided HF, S3 and S4 sounds, and mitral valve regurgitation are also noted.
Medical Diagnosis
Diagnosis of dilated cardiomyopathy is made primarily on the basis of echocardiography results. Cardiac enlargement may be noted on chest radiography. The echocardiogram and chest

radiograph are also used to diagnose hypertrophic cardiomyopathy. Other findings include a systolic murmur and atrial and ventricular dysrhythmias. An enlarged LV may be accompanied by left atrial enlargement. The diagnosis of restrictive cardiomyopathy is demonstrated by decreased cardiac output and HF. It must be differentiated from pericarditis. An echocardiogram may show thickened ventricular walls and small ventricular cavities.
Medical Treatment
Supportive measures are used for dilated cardiomyopathy. Positive inotropic drugs to improve cardiac output, diuretics to decrease preload, and ACE inhibitors and vasodilators to decrease afterload provide this type of therapy. Anticoagulants may be used to prevent thrombi. If all other measures fail, the patient needs a heart transplant. Medical treatment for hypertrophic cardiomyopathy includes antidysrhythmics, antibiotics, anticoagulants, calcium channel blockers, and beta-blockers. Surgical incision of the hypertrophied septal muscle and resection of some of the hypertrophied muscle may be considered for hypertrophic cardiomyopathy An alternative for select patients, nonsurgical reduction of the hypertrophied septum with alcohol ablation, may be done percutaneously in the cardiac catheterization laboratory. Some patients with hypertrophic CMP may benefit from an implantable cardioverter-defibrillator placed to prevent sudden cardiac death. Treatment of restrictive cardiomyopathy is similar to that of HF therapy. Heart transplantation may be considered. Complications observed with all types of cardiomyopathy are dysrhythmias, HF, and death. There is a poor prognosis with cardiomyopathy. Mortality from CMP is highest in older adults, men, and blacks.
NURSING CARE of the Patient with CardiomyopathyAssessment
These patients are primarily assessed for heart failure. Be alert for dyspnea, cough, edema, dysrhythmias, and decreased cardiac output.
Nursing Diagnoses, Goals, and Outcome Criteria: CardiomyopathyNursing Diagnoses Goals and Outcome Criteria
Decreased Cardiac Output related to ventricular failure Improved cardiac output: normal pulse and blood pressure
Activity Intolerance related to poor tissue perfusion
Increased activity intolerance: performance of daily activities without excessive fatigue
Hopelessness related to poor prognosis
More positive outlook: patient's expression of feelings about condition and hopeful statements
Interventions
The care of these patients is similar to that of patients with HF. In addition, a hopeful atmosphere and a careful explanation of care requirements are necessary. Encourage the family to support the patient. The teaching plan guides the patient to make lifestyle changes. Encourage the patient to make decisions and choices.
CARDIAC TRANSPLANTATION

The first heart transplantation was performed in 1967 in South Africa by Dr. Christiaan Barnard. Today, heart transplantations in the United States, approximately 2500 per year, are done for end-stage heart disease. Most of the cases of end-stage heart disease that require transplantation are caused by cardiomyopathy. Psychological makeup is carefully assessed before transplantation. Patients with a history of depression, noncompliance, and inability to cope with stress are poor candidates. In the United States, there are federal regulations that prohibit the sale of human organs.
The donor must meet the criteria for brain death, have no malignancies outside the central nervous system, be free of infection, and not have experienced severe chest trauma. Prolonged advanced life support measures are avoided. The donor and recipient organs must be carefully matched. The donor heart size must be sufficient to meet the needs of the recipient. The donor heart may be preserved for 4 to 6 hours before transplantation.
FIGURE 35-13 Heart transplantation. A, After the recipient is placed on cardiopulmonary bypass, the heart is removed. B, The posterior walls of the recipient's left and right atria are left intact. C, The left atrium of the donor heart is anastomosed to the recipient's residual posterior atrial walls, and the other atrial walls, the atrial septum, and the great vessels are joined. D, Postoperative result.
The recipient must be free of infection at the time of transplantation. The patient is prepared for surgery as with any open-heart procedure. Cardiopulmonary bypass is initiated and the recipient's heart is removed except for the posterior portions of the atria (Fig. 35-13). The donor heart is trimmed and anastomosed to the remaining native heart. The patient is removed from bypass, the heart is restarted, and the chest is closed.
Aftercare of the patient with a heart transplant is similar to that of the patient after coronary artery bypass surgery. Hemodynamic monitoring, ventilation, cardiac assessment, care of chest tubes, and accurate intake and output measurements are vital. Immediately after surgery, the patient is placed in a private room in the intensive care unit. Modified protective isolation is used. The use of gowns, masks, and careful hand washing has been found to be superior to strict isolation techniques. Invasive lines/tubes (e.g., endotracheal tube, pulmonary artery catheter, Foley catheter, chest tubes) are removed as rapidly as possible to decrease the chance of infection. The prevention of postoperative infection is a major goal. Pulmonary infections are most frequently found after heart transplantations. Moving the patient from the intensive care unit to a private room and to home as soon as possible decreases the incidence of nosocomial infections. Patients and families are taught the signs and symptoms of infection and to avoid crowds and others with infections.
In addition, the patient with a transplant receives immunosuppressive medications. Lifelong immunosuppression is administered to prevent the body from rejecting the donated heart, which it recognizes as foreign tissue. Initially, large doses of corticosteroids are administered, and the dose is decreased over time. At the first indication of rejection (increased temperature, infection, dyspnea, malaise, fatigue, dysrhythmia), the steroid dose usually is increased. Other drugs used to prevent and treat rejection are azathioprine (Imuran) and cyclosporine (Sandimmune).

Protocols using several immunosuppressive agents are considered most effective. Reduced dosages of each drug provide for a lower incidence of toxicity.
Rejection is monitored through endomyocardial biopsies. These are performed frequently in the immediate period after transplantation and less frequently over time. Patients are taught to monitor their own progress and to report problems promptly. Patients are followed closely by the transplant team and are observed for infection, rejection, quality of life, and complications. Common complications noted after heart transplantation are hypertension, elevated cholesterol, obesity, and malignancies.
SUDDEN CARDIAC DEATH
Sudden cardiac death occurs when heart activity and respirations cease abruptly. The most common underlying reason for sudden cardiac death is coronary heart disease.
Pharmacology Capsule
Patients taking immunosuppressive drugs to prevent rejection of transplanted tissue have reduced resistance to infection.
The sudden cardiac death event usually occurs during ordinary activity. It is often preceded by ventricular tachycardia or ventricular fibrillation and occasionally by severe bradydysrhythmias (slow, abnormal cardiac rhythms). An episode of sudden cardiac death may be the first indication of CAD. Other causes include left ventricular dysfunction, cardiomyopathy, hypokalemia, antidysrhythmics, liquid protein diets, and high alcohol consumption.
Those who survive an episode of sudden cardiac death need to have extensive testing done to determine the nature and cause of the sudden cardiac death. Many of these people will need treatment of CAD (medical therapy, PTCA, or coronary artery bypass grafting). Most of these patients have a lethal dysrhythmia that requires intervention. Diagnostic tests include 24-hour Holter monitoring and/or ILR, stress testing, and electrophysiology study. During the electrophysiology study, pacing electrodes are placed in the heart and electrical stimuli are used to elicit the dysrhythmia. This helps the physician determine appropriate medical therapy. In some patients, the dysrhythmia may be treated during the electrophysiology study with catheter ablation. The ablation (removal or “burning”) of abnormal conduction pathways or irritable sites in the heart can prevent the dysrhythmia from recurring. Still other patients are treated effectively with antidysrhythmics such as amiodarone (Cordarone). If these therapies are ineffective, the patient may be considered a candidate for an implantable cardioverter/defibrillator (ICD).
Implantable Cardioverter/Defibrillator
The implantable cardioverter/defibrillator (ICD) is used to treat patients with life-threatening recurrent ventricular fibrillation who are unresponsive to medications or pacemakers. Its use has greatly decreased the mortality from sudden cardiac death. The device senses heart rate, diagnoses rhythm changes, and treats ventricular dysrhythmias. The ICD generator is implanted

in the subcutaneous tissue over the pectoral muscle. The lead system is placed via a subclavian vein into the endocardium. The cardioverter recognizes ventricular fibrillation and ventricular tachycardia and uses the shocks to convert the dysrhythmia to normal sinus rhythm. When the ICD senses these lethal dysrhythmias, it delivers a shock of up to 35 joules to defibrillate. If the heart rhythm does not return to normal, the device can continue to deliver shocks. The patient is instructed to sit or lie down when experiencing a shock and to keep a record of the number of shocks delivered. Patients report that the shocks feel like a blow to the chest. In addition to defibrillation, the newer generation of ICDs are also able to function as antitachycardia and antibradycardia pacemakers, have event memory/retrieval, and are capable of programmed self-testing.
Complications.
Complications associated with the ICD are inappropriate shocks, broken or displaced leads, and failure to deliver shocks as a result of battery failure or failure to recognize a dysrhythmia.
NURSING CARE of the Patient with an Implantable Cardioverter/Defibrillator
Nurses can promote psychosocial adaptation in patients with ICDs. The patient may be concerned with body image change and a fear of shocks. It is important to decrease anxiety about being shocked. Some patients become very dependent on the machine. These patients and families need much teaching and support. People who touch the patient during a shock will feel a tingling sensation, which is not harmful. An established support group for the patient and family is very helpful. The family must be instructed in cardiopulmonary resuscitation. An identification bracelet and a card with instructions about the ICD setting are carried at all times. Advise patients to avoid strong magnetic fields (metal detectors, power plants, MRI). The device and batteries should be checked every 2 months. Batteries should last 4 to 7 years.
VALVULAR DISEASE
The purpose of the heart valves is to maintain blood flow in one direction. If the valves are damaged through a congenital defect or acquired disease, their function is compromised. Stenosis and regurgitation are the two major valve problems. Stenosis is narrowing of the valvular opening. A stenotic valve limits the amount of blood ejected from one chamber to the next. Regurgitation, the inability of the valve to close completely, allows the blood to flow backward when a valve does not close efficiently. The left side of the heart is affected most often, and the mitral valve is the most frequently affected of all the valves. The pulmonic valve in the right side of the heart is infrequently affected. Only left-sided valvular disease is discussed here.
Antibiotics have decreased the incidence of valvular disease from rheumatic fever, but the incidence of nonrheumatic valvular disease has increased. Longer life span and intravenous drug abuse are the primary causes of the increasing incidence of nonrheumatic valvular disease.
Mitral Stenosis

Mitral stenosis is a narrowing of the opening in the mitral valve that impedes blood flow from the LA into the LV. The mitral valve leaflets become thickened and fibrotic. Rheumatic heart disease is the leading cause of mitral stenosis. Congenital malformations of the mitral valve occur but are not common. Other causes are calcium accumulation on valve leaflets and atrial myxomas (tumors).
Pathophysiology
The thickening of the valve structures reduces the outflow of blood from the LA to the LV. The LA dilates to accommodate the amount of blood not ejected, and left atrial pressure increases. As left atrial pressure increases, the blood volume backs up into the pulmonary system, increasing pulmonary pressures. This increases the workload on the right side of the heart, leading to right ventricular hypertrophy. Eventually, the RV fails, and cardiac output decreases because less blood is delivered to the LV.
Signs and Symptoms
Symptoms may begin soon after the disease process or may be delayed for many years. Dyspnea, fatigue, cough, chest pain, and activity intolerance are the most frequent symptoms. Exertional dyspnea and pulmonary edema occur as blood backs up in the pulmonary system and serous fluid leaks into the pulmonary tissues. Because stenosis causes turbulent blood flow through the valve, a murmur is present during diastole (best heard at the apex of the heart).
Medical Diagnosis
Diagnosis is made on the basis of the patient history, physical examination, and results of diagnostic procedures. The chest radiograph shows left atrial, right ventricular, and pulmonary vascular enlargement. Echocardiography, often transesophageal echocardiography, is used to visualize the mitral valve. Cardiac catheterization is used to confirm the diagnosis and determine the extent of the disease process.
Medical Treatment
When symptomatic, the patient with mitral stenosis is treated as for CHF with drug therapy, sodium and fluid restrictions, and activity restriction. Digoxin, diuretics, beta-blockers, and antidysrhythmics may be prescribed. If the patient has atrial fibrillation, anticoagulants also may be prescribed. Prophylactic antibiotics are prescribed before any invasive procedure for patients with mitral stenosis because bacteria tend to cluster on the damaged valves.
Surgical Treatment
Surgical treatment includes commissurotomy, mitral valve replacement, and balloon valvuloplasty. Commissurotomy is excision of parts of the leaflets to enlarge the opening. The mitral valve may be replaced with a biologic or synthetic valve (Fig. 35-14). Both commissurotomy and mitral valve replacement require major surgery with cardiopulmonary bypass.
Balloon valvuloplasty, a procedure done in the cardiac catheterization laboratory, has been very successful in dilating stenosed heart valves. It is less invasive than valve replacement or commissurotomy. To dilate the mitral valve, a balloon catheter (like the one used for PTCA) is threaded from the femoral artery to the mitral valve. The balloon is positioned in the valve and inflated until the valve opens sufficiently. After the procedure, the patient is observed closely in an intensive care unit for dysrhythmias and complications. Complications include valve regurgitation, restenosis, perforation of the myocardium, and, rarely, systemic embolization.
FIGURE 35-14 Types of prosthetic and tissue valves. A, Bileaflet mechanical valve. B, Porcine heterograft. C, Carpentier-Edwards aortic pericardial valve.
NURSING CARE of the Patient with Mitral StenosisAssessment
It is most important to obtain a complete history as summarized in Box 35-1 and a record of signs and symptoms being experienced. Take the vital signs, and auscultate for heart murmurs. The murmur of mitral stenosis is described as rumbling and low pitched. It is heard best at the apex of the heart. The ECG may show a notched P wave, indicating left atrial enlargement. Atrial fibrillation is frequently seen. Tachycardia and tachypnea are common signs. The pulse pressure may be decreasing, indicating low cardiac output. Jugular venous distention and crackles are found with pulmonary congestion.
Nursing Diagnoses, Goals, and Outcome Criteria: Mitral Stenosis
The nursing diagnoses and goals for mitral stenosis are the same as those for CHF and for all valvular diseases:
Nursing Diagnoses Goals and Outcome CriteriaDecreased Cardiac Output related to narrowing or insufficiency of valvular competence
Increased cardiac output: normal pulse and blood pressure
Impaired Gas Exchange related to pulmonary congestion Improved gas exchange: clear breath sounds, normal arterial blood gases
Activity Intolerance related to imbalance between oxygen supply and demand
Improved activity tolerance: performance of daily activities without excessive fatigue
Fluid Volume Excess related to decreased glomerular filtration rate, increased aldosterone, sodium and water retention, and increased antidiuretic hormone release
Normal fluid balance: no edema, clear breath sounds, fluid output equal to or exceeds fluid intake
Interventions
See the Nursing Care of the Patient with Heart Failure section on pp. 662 to 665 for the remainder of the nursing process.
Mitral Regurgitation
Mitral regurgitation (insufficiency) allows blood to flow back into the LA during diastole. The valve does not close completely because one or both of the valve leaflets becomes rigid and shortens.
The LA and LV hypertrophy as a result of the backflow of blood against the incompetent valve. Left ventricular hypertrophy is compensatory in an attempt to maintain cardiac output. Eventually, the left side of the heart fails, and symptoms are then the same as those with mitral stenosis.
The murmur of mitral regurgitation is high pitched and blowing and occurs during systole. It is best heard at the apex and may radiate to the axilla. With severe disease, S3 and S4 sounds may be auscultated. Atrial fibrillation occurs as the LA enlarges.
Mitral regurgitation is treated with vasodilators to decrease the afterload and therefore the regurgitation. Other medical treatment includes activity restriction, dietary sodium limitation, diuretics, and digitalis. Surgical treatment includes annuloplasty and mitral valve replacement. Annuloplasty is reconstruction of the leaflets and the annulus.
Mitral Valve Prolapse
The mitral valve prolapses when one or both leaflets enlarge and protrude into the LA during systole. It has a tendency to run in families and may be caused by heart infections, rheumatic fever, or a wide variety of congenital anomalies. The disease is usually benign but may progress to mitral insufficiency. Mitral valve prolapse occurs in approximately 3% of the population (American Heart Association, 2007). Most victims are women 20 to 55 years of age.
In most patients, symptoms do not occur or may occur with stress. Symptoms include chest pain, palpitations, dizziness, and syncope. Some patients exhibit dysrhythmias. The ECG usually shows normal findings. Evidence of mitral valve prolapse may be found on echocardiography. The problem is often controlled with stress-reduction techniques. Beta-blockers may be prescribed to decrease syncope, palpitations, and severe chest pain. Therapeutic management is matched to the degree of symptoms.
Aortic StenosisEtiology and Risk Factors
Stenosis of the aortic valve occurs when the valve cusps become fibrotic and calcify. It may be caused by a congenital malformation or result from rheumatic fever, syphilis, or the aging process (atherosclerosis and calcification). When seen in younger patients, it is most often caused by a congenital malformation. The aortic valve is most commonly diseased in the aging population.
Pathophysiology
The valve opening decreases to one-third normal size before symptoms occur. As flow is impeded through the narrowed valve, the LV hypertrophies to compensate for the extra pressure

needed to eject blood. The LA also compensates by delivering a strong atrial kick. These compensatory mechanisms allow normal function until atrial fibrillation disrupts the atrial kick or until the LV hypertrophies to the point of dysfunction, with decreased cardiac output and myocardial ischemia. With left ventricular dysfunction, blood backs up into the LA and the pulmonary system. If uncorrected, eventually the right side of the heart fails.
Signs and Symptoms
The patient complains of dyspnea on exertion, angina, and syncope. Fatigue, orthopnea, and paroxysmal nocturnal dyspnea are late symptoms and indicate heart failure. A systolic murmur may occur.
Medical Diagnosis
The chest radiograph shows atrial and ventricular enlargement, which are late signs. The murmur of aortic stenosis is heard best in the aortic area, the second intercostal space to the right of the sternum. The echocardiogram shows left ventricular wall thickening. An exercise tolerance test may be ordered to evaluate heart function.
Medical Treatment
Prophylactic antibiotics are prescribed to prevent IE with dental and invasive procedures. Heart failure is treated with digoxin, diuretics, a low-sodium diet, and activity restriction. Surgical treatment includes balloon valvuloplasty and aortic valve replacement.
NURSING CARE of the Patient with Aortic Stenosis
Monitor for a bounding arterial pulse and widened pulse pressure. The nursing process is the same as for HF (see Nursing Care Plan: The Patient with Heart Failure on p. 663).
Aortic Regurgitation
Fibrosis and thickening of the aortic cusps progress until the valve no longer maintains unidirectional blood flow. Aortic regurgitation (insufficiency) is caused primarily by rheumatic fever. Other causes include IE, blunt chest trauma, calcification of the valve, and chronic hypertension.
Regurgitation of blood into the LV during diastole increases the amount of blood in the LV. The LV dilates and hypertrophies. Myocardial ischemia and left ventricular failure occur. Blood backs up into the pulmonary system and eventually right ventricular failure occurs.
The murmur of aortic regurgitation is high pitched and blowing and occurs in diastole. It is auscultated best at the aortic area. The point of maximal impulse may be shifted to the left and down. Tachycardia and palpitations are compensatory mechanisms. Later signs of HF such as fatigue, dyspnea, and ascites develop. A widened pulse pressure (increased difference between

systolic and diastolic pressures) results from a low diastolic pressure. S3 and S4 sounds are often auscultated.
Left atrial and ventricular dilation are noted on chest radiography. The echocardiogram shows left ventricular dilation. Cardiac catheterization is used to determine the extent of incompetence.
As with other patients with valve disease, these patients have prophylactic antibiotics prescribed before invasive procedures. Digoxin and diuretics are prescribed for left ventricular hypertrophy. Aortic valve replacement provides long-term correction.
ELECTROCARDIOGRAM MONITORING
Nurses working in critical care areas are responsible for monitoring and interpreting ECGs. Patients usually are monitored continuously at the bedside and have intermittent monitoring through a 12-lead ECG.
12-LEAD ELECTROCARDIOGRAM
A 12-lead ECG looks at the heart from 12 directions or perspectives. This permits more precise evaluation of the heart's electrical activity. Three leads are placed on the limbs (leads I, II, and III), three leads are augmented (aVR, aVL, and aVF), and there are six chest, or precordial, leads (V1 to V6). Electricity flows from the negative to the positive lead. If the depolarization wave flows toward the positive pole (electrode), the deflection is upright. If the wave flows away from the positive pole, the deflection is negative.
CONTINUOUS MONITORING
For continuous ECG monitoring, only one or two single leads are used. Most units that perform continuous monitoring use the five-lead system with four limb electrodes and a chest electrode (which is placed at one of the V lead sites). The electrodes are held in place by adhesive pads. Thoroughly clean the electrode sites before applying the pads. Change the pads according to agency policy. Monitor the skin for irritation or breakdown. The lead monitored depends on the purpose of the monitoring (e.g., detect dysrhythmias, detect ischemia).
INTERPRETATION OF ELECTROCARDIOGRAMS
To interpret an ECG strip, the reader is referred to Figure 35-15. The graph paper consists of horizontal and vertical small and large squares. The horizontal axis measures time; the vertical axis measures voltage. Each small square represents 0.04 second on the horizontal axis and 1 mm on the vertical axis. Each large square, bounded by heavy lines, is made up of five small squares and represents 0.20 second and 5 mm. The electrical activity of the heart is represented by deflections, positive and negative, from the baseline. A deflection is an upward or downward movement from the baseline. The baseline is called the isoelectric line. The first positive deflection (upward movement) is the small, rounded P wave that represents atrial depolarization. The second positive deflection is the peaked QRS complex that represents ventricular depolarization. The Q is the first negative deflection, meaning the line moves below the

isoelectric line. The R wave corresponds to the patient's pulse. Atrial repolarization occurs during ventricular depolarization and is obscured by the QRS complex. The third deflection is the rounded T wave, which represents ventricular repolarization. The fourth deflection, if present, is the U wave. It is small, rounded, and usually indicates electrolyte imbalance (hypokalemia).
The PR interval represents the time it takes the impulse to travel from the atria through the AV node to the ventricles. The PR interval is measured from the beginning of the P wave to the Q wave. The normal PR interval is from 0.12 to 0.20 second. The QRS complex is measured from the point at which the Q leaves the isoelectric line to the point at which the S returns to the isoelectric line. The normal QRS complex is 0.06 to 0.10 second. The ST segment represents the time from ventricular depolarization to ventricular repolarization. The ST segment should be along the isoelectric line. The QT segment represents ventricular refractory time. It is measured from the beginning of the QRS complex to the end of the T wave. The normal QT segment time range varies with heart rate; therefore it is necessary to compare the QT obtained with a table (QT tables are available in most textbooks dealing with dysrhythmias). The QT segment is affected by age, gender, and heart rate.
FIGURE 35-15 Relationship between the cardiac cycle and the heart sounds.
Criteria for Interpreting Electrocardiograms
Criteria have been established for interpreting an ECG strip. The ECG is evaluated for rate, regularity, P waves, PR interval, and QRS complexes (Table 35-8).
Rate Calculation.
Most ECG strips have tic marks indicating 3-second time periods. There are several ways to calculate heart rate from the ECG strip. The quickest but least accurate method is to count the number of P waves (for atrial rate) or R waves (for ventricular rate) in a 6-second strip (between 3 tic marks or 30 large squares) and multiply by 10 for the estimate of the number of beats per minute. For example, if there are six R waves in a 6-second strip, the heart rate is 60 bpm.

The more accurate method uses the number of small squares between two P waves (atria) or two R waves (ventricles). Divide 1500 by the number of small squares. For example, if there are 25 small squares between two R waves, the rate is 60 bpm (1500 divided by 25). The atrial rate is determined by the number of P waves and the ventricular rate by the number of QRS complexes. The normal rate is from 60 to 100 bpm.
Rhythm.
The consecutive P-P intervals for the atria and the consecutive R-R intervals for ventricles are measured for consistency. Using calipers or a blank piece of paper, note the distance between R waves. If the distances do not vary more than one small square, the rhythm is considered regular. If the distances are greater than one small square, the rhythm is irregular.
Table 35-8 Criteria for Electrocardiogram Interpretation
Rate Are the atrial and ventricular rates the same as measured by the P-P and R-R intervals?
Rhythm Is the rate regular or irregular? If irregular, is there a pattern? Are these ectopic beats? Where do they occur?
P waves Is there a P wave before every QRS complex? Does each P wave have the same size and shape?
PR interval (PRI)
Are all the PRIs the same length? If not, is there a pattern to the irregularity? Are the PRIs within normal range?
QRS complexes
Do all the QRS complexes look alike? Are all the QRS complexes within the normal range (0.06-0.10 sec)?
ST segment Is the ST segment isoelectric, depressed, or elevated?T waves Do all the T waves look alike? Are the T waves upright or inverted?FIGURE 35-16 Normal sinus rhythm. Each segment between the dark lines (above the monitor strip) represents 3 seconds, when the monitor is set at a speed of 25 mm/sec. Characteristics: Rate—60 to 100 bpm; Regularity—essentially regular (P-to-P and R-to-R intervals are regular with only minor variation); P wave, PR interval—there is a P before every QRS; each P wave is the same size and shape; PR interval is between 0.12 and 0.20 sec; QRS—falls between 0.06 and 0.10 sec; T wave—rounded, all the same shape. Interpretation: Normal sinus rhythm.
P Waves.
The next evaluation is of P waves. Is there a P wave before each QRS complex? If so, the rhythm originates in the SA node. Do all the P waves appear the same size and shape? If so, the impulse originates in the SA node.
PR Interval.
Does the PR interval fall within the normal range of 0.12 to 0.20 second? If so, there is no interference in conduction from the SA to the AV node.
QRS Complex.

Does the QRS complex fall within the 0.06- to 0.10-second range? If the QRS is prolonged (0.12 second or greater), there is a delay in conduction through the ventricles.
ST Segment.
Examine the ST segment. Is it isoelectric? Or is it depressed or elevated?
T Waves.
Are the T waves rounded and the same size and shape? Do the T waves follow the QRS complexes?
QT Interval.
Measuring the QT interval is not always part of dysrhythmia interpretation. The QT interval, if measured, should be compared with the QT interval table. The QT interval may be affected by electrolyte imbalances and drugs.
Normal Sinus Rhythm
The most common cardiac rhythm is sinus in origin because the impulse originates in the SA node, is conducted normally, and meets all of the criteria established earlier. Normal sinus rhythm is displayed in Figure 35-16.
Common Dysrhythmias
A dysrhythmia is a disturbance of the rhythm of the heart caused by a problem in the conduction system. Dysrhythmias are categorized according to the site of the origin of the impulse formation. Dysrhythmias originating in the atria are called atrial dysrhythmias. Dysrhythmias originating in the AV node are called junctional or escape rhythms. Dysrhythmias originating below the AV node are called ventricular. Blocks are interruptions in impulse conduction. Dysrhythmias and blocks have characteristics that are noted on the ECG. See Figures 35-17 through 35-30 for examples. Antidysrhythmic drugs are used to treat dysrhythmias and restore normal sinus rhythm.
HEMODYNAMIC MONITORING
In addition to noninvasive cardiac assessment and ECG monitoring, more sophisticated measures may be needed to determine what is going on within the heart or vascular system. Nurses who work in intensive care areas frequently work with patients who have central venous catheters, pulmonary artery catheters, or arterial lines.
FIGURE 35-17 Sinus bradycardia. Characteristics: Rate—less than 60 bpm; Regularity—normal; P wave, PR interval—normal; QRS—normal; T wave—normal. Interpretation: All characteristics are within normal ranges except for the rate, which is slow. Causes: Drugs, including digitalis and beta-blockers, vagal stimulation (Valsalva maneuver), severe pain,
hyperkalemia, infection, and myocardial infarction. Frequently seen in athletes as a result of conditioning. Symptoms: Dizziness, syncope, chest pain, hypotension, sweating, nausea, dyspnea, and disorientation; sometimes no symptoms. Treatment: Not treated unless the patient is symptomatic. The underlying cause is treated. Atropine may be given to increase the heart rate. Isoproterenol is used with extreme caution. A pacemaker may be needed.FIGURE 35-18 Sinus tachycardia. Characteristics: Rate—greater than 100; usually less than 150 bpm; Regularity—regular; P wave, PR interval—P waves may be buried in T wave of preceding beat with very rapid rates, more than 140 bpm; QRS—normal; T wave—normal. Interpretation: All characteristics are within normal range except for the rate, which is excessive. Causes: Fever, dehydration, hypovolemia, increased sympathetic nervous system stimulation, stress, exercise, and acute myocardial infarction. Symptoms: Palpitations most common. Angina and decreased cardiac output from the decreased ventricular filling time may also occur. Treatment: Correction of underlying cause. Elimination of caffeine, nicotine, and alcohol. Vagal stimulation may decrease the rate but does not treat the cause. Treatment: Beta-blockers.
CENTRAL VENOUS CATHETER
The central venous catheter is placed through the skin, into a venous access (brachial, femoral, subclavian, or jugular sites), and threaded into the RA. The catheter may have one to three lumens. With this catheter, the pressure in the RA (called right atrial pressure [RAP] or central venous pressure [CVP]) can be measured. This measurement is used as an indication of fluid volume. The normal CVP or RAP is 2 to 6 mm Hg. Measurements below normal indicate hypovolemia, and measurements above normal indicate hypervolemia. This catheter may also be used to infuse fluids, blood and blood products, and medications as well as to withdraw blood for analysis.
PULMONARY ARTERY CATHETER
The pulmonary artery (PA) catheter, frequently called a Swan-Ganz catheter, is longer than the central venous catheter. It is inserted like the central venous catheter and is threaded through the RA, the tricuspid valve, the RV, the pulmonic valve, and into the pulmonary artery. The catheter is balloon tipped and flows with the blood. Different waveforms are seen on an oscilloscope as the catheter moves through the different areas of the heart. Pulmonary artery catheters have multiple lumens and are approximately 110 cm (44 inches) long. Various lumens are used to measure the pulmonary capillary wedge pressure, inflate the balloon, measure RAP, determine cardiac output, and administer fluids and drugs. Newer catheters incorporate fiberoptics for continuous monitoring of saturated venous oxygenation (SvO2), a measure of tissue perfusion or continuous cardiac output.
FIGURE 35-19 Sinus dysrhythmia. Characteristics: Rate—normal; Regularity—slightly irregular, varies with respirations; P wave, PR interval—P-to-P intervals vary, the difference between the shortest and longest P-to-P interval is greater than 0.12 sec; the PR interval is normal; QRS—normal; T wave—normal. Interpretation: The rate varies with respirations. Considered normal when the rhythm varies in relation to the respiratory cycle: The R-to-R interval is shorter during inspiration; therefore the rate is increased; the R-to-R interval is longer during expiration; therefore the rate is decreased. Causes: When unrelated to respirations, is

often the result of digoxin toxicity, increased intracranial pressure, or inferior wall myocardial infarction. In older adults, marked variation may indicate a condition known as sick sinus syndrome. Symptoms: Usually none. Treatment: If treatment is necessary, atropine is used and the underlying problem is treated.
FIGURE 35-20 First-degree atrioventricular (AV) block. Characteristics: Rate—normal; Regularity—regular; P wave, PR interval—all P waves are conducted to the ventricles, but AV conduction is prolonged through the AV node; PR interval is greater than 0.20 sec and constant; QRS—normal; T wave—normal. Interpretation: The PR interval is prolonged. Causes: Increased vagal tone, coronary artery disease, digoxin toxicity, heart infections, and quinidine. Symptoms: Usually none, may be bradycardic. Treatment: Correction of underlying cause.
The purpose of a pulmonary artery catheter is to measure right-sided heart pressures and pulmonary artery pressures and to assess left-sided heart function. The proximal port is used to measure the RAP or CVP (normal value, 2-6 mm Hg). The distal port measures the pulmonary artery pressure (normal value, 20-30/0-10). The lungs are low-pressure organs unless the patient has COPD.
The pulmonary capillary wedge pressure is used to assess the function of the left side of the heart. To determine the pulmonary capillary wedge pressure, the balloon is inflated with up to 1.5 mL of air. This allows the tip of the catheter to float into a pulmonary capillary until it occludes the capillary. This measures the pressure ahead of the catheter, therefore the left ventricular heart function. The normal pulmonary capillary wedge pressure is 4 to 12 mm Hg. Once the pressure is recorded, the balloon is deflated. This pressure is lower when fluid is restricted, when diuretics are being administered, and when patients are receiving vasodilators such as nitroglycerin or morphine. The pressure is elevated with excess fluid, when fluid volume expanders such as albumin, dextran, or hetastarch are being administered, or in left heart dysfunction.
FIGURE 35-21 Second-degree atrioventricular block: type I (Mobitz I; Wenckebach). Characteristics: Rate—atrial rate is greater than ventricular rate; Regularity—atrial rate is regular; ventricular rate is irregular; P wave, PR interval—there are more P waves than QRS complexes; the PR interval increases until a P wave is not followed by a QRS; QRS—some are absent; T wave—absent when the QRS is dropped. Interpretation: Progressively lengthening PR interval and a dropped beat. Causes: Myocardial ischemia with progressive increase in conduction time through the sinoatrial node, inferior wall myocardial infarction, digoxin toxicity, and electrolyte imbalance. Symptoms: Decreased blood pressure and syncope, if any. Treatment: Atropine, pacemaker.Cardiac Output
With a pulmonary artery catheter in place, cardiac output can be measured continuously or by the thermodilution method. The normal cardiac output is 4 to 8 L/min. Stress increases the cardiac output. Cardiac output may decrease with AMI, HF, bradycardia, tachycardia, and some drugs. It is important for the nurse to use consistent technique in measuring cardiac output.

Mixed Venous Oxygen Saturation
PA catheters may have sensors in place that allow for measurement of mixed venous oxygen saturation (SvO2) or, if the sensor is not part of the catheter, a blood sample can be obtained from the distal port (which opens in the pulmonary artery). Blood in the pulmonary artery is the blood returned from all of the organs and tissues in the body and mixed in the PA. When the oxygen saturation of this mixed venous blood is measured (in a laboratory or through fiberoptics), the results reflect the degree of oxygen use by the body tissues. SvO2can be decreased when oxygen delivery is decreased or the body has increased the use of oxygen (fever, pain, stress). SvO2can be increased when oxygen delivery is increased or when oxygen utilization is decreased (hypothermia, general anesthesia). Normal SvO2is 60% to 75%.
FIGURE 35-23 Third-degree atrioventricular (AV) block. Characteristics: Rate—atrial rate is faster than ventricular rate; ventricular rate is generally less than 45 bpm; Regularity—irregular; P wave, PR interval—no relationship exists between the P waves and the QRS complexes; QRS—atria and ventricles are beating independently; the QRS is ventricular in origin; T wave—normal. Interpretation: Impulses originating in the sinoatrial node are blocked at the AV node. The ventricles respond to a secondary pacemaker. Causes: Digoxin toxicity, conduction damage during mitral valve replacement, hypoxia, and rheumatic fever. Symptoms: Hypotension, syncope, decreased cardiac output. The underlying cause is treated. Treatment: Atropine, pacemaker, isoproterenol with extreme caution. Do not administer lidocaine, which could suppress ventricular response.
ARTERIAL LINE
An arterial line may be inserted (most often in the radial artery) to provide a direct measurement of systolic and diastolic blood pressures. Once the line is inserted, it is connected to a pressurized solution to keep the catheter patent and to a transducer to assess pressure. The mean arterial pressure is an indication of tissue perfusion. This pressure is elevated with sympathetic stimulation and increased heart rate.
Key Points
• The primary function of the heart is to pump blood through the pulmonary and systemic circulation.
• The heartbeat has two phases: systole (contraction) and diastole (relaxation). • Cardiac output is the amount of blood ejected per minute by each ventricle; stroke
volume is the amount of blood ejected by a ventricle in a single contraction. The factors that affect stroke volume are preload, contractility, and afterload.
• The heart sounds are “lub,” heard during systole, and “dub,” heard during diastole. • The most common cardiac surgical procedures are pacemaker insertion, valve repair or
replacement, and coronary artery bypass surgery. • Nursing concerns after cardiac surgery include Ineffective Breathing Pattern, Acute
Pain, Ineffective Thermoregulation, Decreased Cardiac Output, Risk for Infection, and Anxiety.

• Pacemakers are electronic devices that deliver impulses to stimulate contraction of the myocardium.
• Coronary artery disease is treated with drug therapy, diet modifications, lifestyle modifications, surgical intervention, or a combination of these.
• Risk factors for atherosclerosis are age, gender, race, heredity, diabetes mellitus with elevated blood glucose, increased serum lipids, nicotine, hypertension, obesity, sedentary lifestyle.
• Angina pectoris is the pain that results from myocardial ischemia. It is treated with vasodilators and rest.
• Procedures used to improve myocardial blood flow include percutaneous coronary balloon angioplasty, laser angioplasty, atherectomy, stent placement, coronary artery bypass grafts, and transmyocardial laser revascularization.
• Acute myocardial infarction, caused by partial or complete occlusion of a coronary artery, can lead to dysrhythmias, heart failure, cardiogenic shock, thromboembolism, and ventricular aneurysm/rupture.
• Nursing care of the patient with myocardial infarction addresses Anxiety, Acute Pain, and Decreased Cardiac Output.
• Patients with acute cardiac conditions often have continuous cardiac monitoring to detect potentially fatal dysrhythmias for prompt treatment.
• Cardiac rehabilitation begins with a cardiac incident, lasts throughout life, and includes the patient and family in teaching about exercise, diet, and medications.
• Heart failure, the inability of the heart to meet the metabolic demands of the body, may be caused by disorders that increase the heart's workload or interfere with its pumping action.
• Treatment of heart failure may include correction of underlying causes, drug therapy to improve cardiac function and eliminate excess fluid, and measures to decrease demands on the heart.
• Complications of heart failure are dysrhythmias, pulmonary edema, and cardiogenic shock.
• Nursing care of the patient with heart failure focuses on Fluid Volume Excess, Impaired Gas Exchange, Anxiety, Decreased Cardiac Output, and Activity Intolerance.
• Cardiac inflammatory conditions (endocarditis and pericarditis) are treated with drug therapy and rest.
• Cardiomyopathy is a disease of the heart muscle that is treated with supportive measures but may lead to heart failure that eventually requires cardiac transplantation.
• Patients who have received heart transplants require immunosuppressive drugs for the remainder of their lives to prevent rejection of the foreign tissue.
• Signs and symptoms of cardiac transplant rejection are fever, dyspnea, fatigue, and dysrhythmias.
• An implantable cardioverter/defibrillator is an im-planted device that monitors cardiac activity, detects life-threatening dysrhythmias, and delivers a shock to convert the rhythm to a normal one.
• The primary disorders of the heart valves are stenosis, which interferes with blood movement from one chamber to the next, and regurgitation, which allows blood to flow backward.

• Valve disease may be treated with drug therapy to improve cardiac function, with balloon valvuloplasty to dilate stenosed valves, with commissurotomy to enlarge the opening, and with valve replacement using a biologic or synthetic valve.
• General measures to maintain perfusion of vital organs are modified Trendelenburg's position, oxygen, intravenous fluids, and drugs to maintain or restore blood pressure.
• A dysrhythmia (also called an arrhythmia) is a disturbance of the heart rhythm caused by a problem in the conduction system.
REVIEW QUESTIONS Choose the best answer
1. Normally, the impulse that stimulates a myocardial contraction begins in the: o 1.AV nodeo 2.Bundle of Hiso 3.Purkinje cellso 4.SA node
2. Which statement correctly describes one of the three factors that affect stroke volume? o 1.Contractility is the ability of cardiac muscle fibers to shorten and produce a
muscle contraction.o 2.Preload is the amount of blood remaining in the atria at the end of diastole.o 3.Cardiac output is the amount of blood ejected by the heart with each ventricular
contraction.o 4.Afterload is the amount of blood remaining in the ventricles at the end of
systole. 3. Which of the following age-related changes in the circulatory system can cause heart
murmurs? o 1.Decreased elasticity of connective tissue in the heart muscleo 2.Arterial stiffening caused by changes in connective tissue and elastic fiberso 3.Heart valves that are stiff and do not close properlyo 4.Stretching and dilation of veins resulting in impaired venous return
4. Before administering digoxin, you count a patient's apical heart rate and find that it is 62 bpm. The patient's usual rate ranges from 65 to 75 bpm. What should you do?
o 1. Withhold the digoxin and notify the physician. o 2. Administer the digoxin and document the heart rate. o 3. Hold the drug and recheck the heart rate in an hour. o 4. Give half of the prescribed dose of digoxin.
5. An adverse effect common to all antidysrhythmic drugs is: o 1.Fluid and electrolyte imbalanceo 2.Drowsinesso 3.Diarrheao 4.Additional dysrhythmias
6. The usual dietary recommendations for cardiac patients include the following: o 1.No more than 10% saturated fatso 2.Low fiber and carbohydrateso 3.Sodium restricted to 1 g/dayo 4.20% or less of total fat intake
7. Risk factors for atherosclerosis that can be modified include the following:

o 1. Gender o 3. Heredity o 2. Race o 4. Sedentary lifestyle
8. Characteristics of angina pectoris include that it: o 1.Most often occurs at resto 2.Is accompanied by drop in blood pressureo 3.Is usually substernal but may radiateo 4.Is commonly treated with digitalis
9. Which of the following drugs may be administered after acute myocardial infarction to dissolve thrombi?
o 1.Heparino 2.Tissue plasminogen activatoro 3.Aspirino 4.Lidocaine
10. When cardiac output falls, compensatory mechanisms include the following: o 1. Elimination of excess fluid by the kidneys o 2. Dilation of blood vessels in the extremities o 3. Stimulation of the parasympathetic nervous system o 4. Enlargement of the ventricular myocardium
11. Discharge teaching for a patient with heart failure should include instructions to: o 1.Immediately begin a vigorous program of exerciseo 2.Inform the physician if you gain more than 2 pounds in a weeko 3.Weigh yourself before going to bed each nighto 4.Expect to continue having shortness of breath, chest pain, and cough
12. Before invasive procedures including dental work, patients with valvular heart disease usually are prescribed antibiotics to prevent:
o 1.Pericarditiso 2.Abscess formationo 3.Infective endocarditiso 4.Cardiomyopathy
13. A patient who has had heart transplantation comes into the physician's office complaining of fever, fatigue, shortness of breath, and an irregular heart beat. You should suspect:
o 1. Infection in the surgical wound o 2. Congestive heart failure o 3. Rejection of the transplanted heart o 4. Postoperative anxiety and depression
14. Which of the following findings would you expect in a patient with mitral stenosis? o 1.Increased left atrial pressureo 2.Decreased pulmonary pressureo 3.Increased cardiac outputo 4.Decreased right ventricular pressure
