chapter 193: digitalis glycosides - wordpress.com · 2018-08-07 · 8/7/2018 1/ 14 tintinalli’s...
TRANSCRIPT

8/7/2018
1/14
Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e >
Chapter 193: Digitalis GlycosidesMichael Levine; Aaron B. Skolnik
FIGURE 193–1.
INTRODUCTION
The medicinal benefits of cardiac glycosides have been recognized for centuries, and even with otheralternative medications, digitalis preparations, such as digoxin, are still used for the treatment of atrial
fibrillation and symptomatic congestive heart failure.1 In addition to availability as pharmaceuticals, cardiacglycosides are also found in plants such as foxglove, oleander, red squill, and lily of the valley. Similarcardioactive steroids are also found in the skin of toads in the Bufonidae family and in some herbalmedications. Despite declining use of digoxin, the prevalence of patients diagnosed with digoxin toxicity has
remained constant, and the use of digoxin-specific antibody fragments has increased.2 Digitoxin, a cardiacglycoside similar in structure to digoxin but with a longer half-life, is no longer commercially available in theUnited States, but is available in Canada and elsewhere in the world.
PATHOPHYSIOLOGY
Digoxin is a cardiac glycoside available for oral or intravenous use. Following oral absorption, digoxin reachesa maximal serum concentration 1 to 3 hours a�er ingestion. It is approximately 25% protein bound and has alarge volume of distribution (6 to 7 L/kg). The drug is primarily eliminated through the kidneys.
Digoxin, like other cardiac glycosides, inhibits sodium-potassium ATPase.3 This inhibition results in increasedintracellular sodium and increased extracellular potassium. As a result of the increased intracellular sodium,the sodium-calcium antiporter is not able to e�ectively remove calcium from the myocyte. Consequently,there is an increase in intracellular calcium, which augments inotropy. The increased intracellular calciumcan contribute to delayed a�er-depolarizations, which may lead to premature ventricular contractions anddysrhythmias. In addition, there is a decreased refractory period of the myocardium, which increasesautomaticity and hence is associated with an increased risk of dysrhythmias. Furthermore, cardiacglycosides shorten atrial and ventricular repolarization, thereby decreasing the refractory period and thusincreasing automaticity.
Cardiac glycosides also increase vagal tone via action at the carotid body, thereby reducing conductionthrough the sinoatrial and atrioventricular nodes. In toxic concentrations, cardiac glycosides can increasesympathetic tone. Digoxin can reduce plasma renin concentrations in patients with advanced heart failure,
8/7/2018
2/14
thereby resulting in peripheral vasodilation.4 In contrast, in those without heart failure, digoxin can causevasoconstriction. This di�erence is likely due to increased sensitivity of the carotid baroreceptors in patients
with advanced, chronic heart failure.5
CLINICAL FEATURES
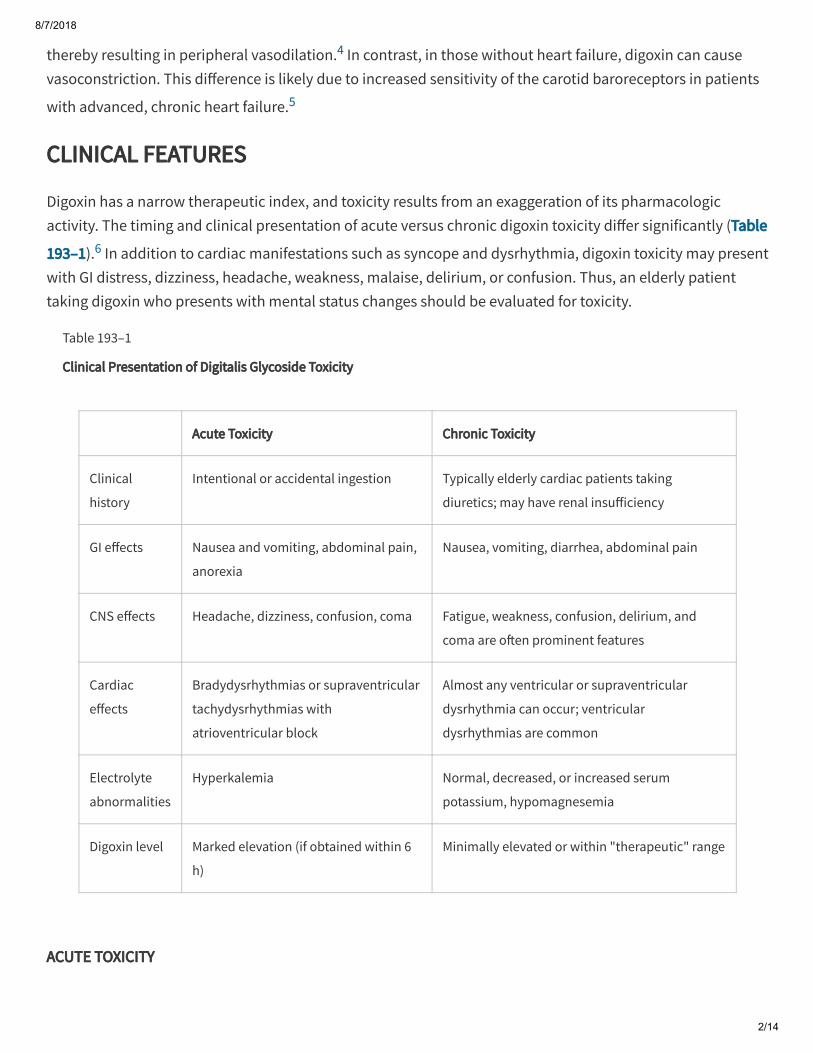
Digoxin has a narrow therapeutic index, and toxicity results from an exaggeration of its pharmacologicactivity. The timing and clinical presentation of acute versus chronic digoxin toxicity di�er significantly (Table
193–1).6 In addition to cardiac manifestations such as syncope and dysrhythmia, digoxin toxicity may presentwith GI distress, dizziness, headache, weakness, malaise, delirium, or confusion. Thus, an elderly patienttaking digoxin who presents with mental status changes should be evaluated for toxicity.
Table 193–1
Clinical Presentation of Digitalis Glycoside Toxicity
Acute Toxicity Chronic Toxicity
Clinical
history
Intentional or accidental ingestion Typically elderly cardiac patients taking
diuretics; may have renal insu�iciency
GI e�ects Nausea and vomiting, abdominal pain,
anorexia
Nausea, vomiting, diarrhea, abdominal pain
CNS e�ects Headache, dizziness, confusion, coma Fatigue, weakness, confusion, delirium, and
coma are o�en prominent features
Cardiac
e�ects
Bradydysrhythmias or supraventricular
tachydysrhythmias with
atrioventricular block
Almost any ventricular or supraventricular
dysrhythmia can occur; ventricular
dysrhythmias are common
Electrolyte
abnormalities
Hyperkalemia Normal, decreased, or increased serum
potassium, hypomagnesemia
Digoxin level Marked elevation (if obtained within 6
h)
Minimally elevated or within "therapeutic" range
ACUTE TOXICITY

8/7/2018
3/14
Patients with acute digoxin toxicity tend to have more abrupt onset of symptoms than those with chronictoxicity. In acute cardiac glycoside poisoning, there may be an asymptomatic period of several hours beforethe onset of symptoms. GI symptoms, such as nausea, vomiting, anorexia, and vague abdominal pain, areo�en the earliest manifestations of acute toxicity. Increased central vagal tone typically produces cardiacmanifestations such as bradydysrhythmias or atrioventricular block. Neurologic manifestations such asweakness or confusion can occur independently of the blood pressure. The classic description of digoxintoxicity includes viewing yellow-green halos around objects, termed xanthopsia. However, patients more
frequently describe nonspecific changes in their color vision.7
Hyperkalemia is an important finding in acute toxicity and may develop due to inhibition of sodium-potassium ATPase. Digoxin levels obtained with the first 6 hours following an acute ingestion may be falselyelevated as the level represents a predistribution level rather than reflecting the amount ingested. Overall,the severity of acute toxicity correlates most closely with the degree of hyperkalemia and correlates poorly
with the early serum digoxin levels.8
CHRONIC TOXICITY
Chronic toxicity occurs most typically in the elderly and is o�en the result of drug–drug interactions ordeclining renal function. Some of the more common drug interactions that predispose to chronic digoxintoxicity include calcium channel antagonists, amiodarone, β-receptor antagonists, diuretics, indomethacin,clarithromycin, quinidine, procainamide, and erythromycin. In particular, interaction between digoxin and
clarithromycin contributes to increased hospitalizations for digoxin toxicity in elderly patients.9 A commonscenario involves a patient starting to take a diuretic, which results in mild dehydration and hypokalemia;dehydration reduces the clearance of digoxin, and hypokalemia increases susceptibility to digoxin, resultingin chronic toxicity.
Decreases in renal function and lean body mass associated with aging may alter the pharmacokinetics of
digoxin, leading to toxicity at normally therapeutic doses.10 This population may also possess a higher risk
due to coexisting diseases and polypharmacy.10,11
The patient with chronic digoxin toxicity o�en has vague and nonspecific signs and symptoms compared tothe patient with acute digoxin toxicity. GI symptoms may occur but may be less pronounced. Neurologicmanifestations, such as weakness, fatigue, confusion, or delirium, are more prominent features in chronic
toxicity.6,12
DIAGNOSIS
The diagnosis of digoxin toxicity is a composite picture, using history, physical examination, and laboratorystudies; no single element excludes or confirms the diagnosis. In patients with heart failure and normal renalfunction, daily digoxin doses are usually between 125 and 250 micrograms. Digoxin toxicity can occur with a

8/7/2018
4/14
single ingestion of 1 to 2 milligrams in an adult, and fatalities have been reported following an acuteingestion of 10 milligrams in an adult and 4 milligrams in a child.
Di�erential diagnosis includes other toxins that may induce bradydysrhythmias such as calcium channelantagonists, β-receptor antagonists, class IA antidysrhythmics (procainamide and quinidine), class ICantidysrhythmics (flecainide and encainide), clonidine and other imidazolines, and organophosphate orcarbamate insecticide poisoning. Glycoside-containing and other cardiotoxic plants should also beconsidered (e.g., foxglove, squill, lily of the valley, oleander, rhododendron, monkshood, tobacco, falsehellebore, and yew berry). Sick sinus syndrome, with its combination of supraventricular dysrhythmias andcardiac conduction blocks, can also mimic digoxin toxicity. Hyperkalemia from any cause may producebradycardia and abnormal cardiac conduction and should be considered in the di�erential diagnosis.
ELECTROCARDIOGRAM
Almost any cardiac dysrhythmia may be observed in digoxin toxicity, with the exception of rapidly conducted
atrial dysrhythmias.13,14 The most common dysrhythmia in digoxin toxicity is premature ventricularcontractions. Ventricular dysrhythmias occur more frequently in chronic than in acute poisonings. Althoughrare and not pathognomonic for digoxin toxicity, bidirectional ventricular tachycardia should be investigatedfor possible toxicity because only a few xenobiotics are known to produce this unique dysrhythmia, digoxinincluded.
Four specific electrocardiographic findings are seen with therapeutic levels of digoxin and are not indicatorsof toxicity, although they may also be seen in poisoned patients. These findings include T-wave changes suchas flattening or inversion, QT-interval shortening, a "scooped" appearance of the ST segment with ST-
segment depression, and an increase in U-wave amplitude (Figure 193–1).14
FIGURE 193–1.
ECG demonstrating findings seen with digoxin use. A. ECG shows scooping of ST segments and small U waveswith a serum digoxin level of 0.9 nanogram/mL (1.15 nmol/L). B. ECG shows scooping of ST segments,flattening of T waves, and first-degree atrioventricular block with a serum digoxin level of 1.2 nanograms/mL(1.54 nmol/L).

8/7/2018
5/14
LABORATORY
In acute poisonings, the serum potassium and digoxin levels can provide useful diagnostic information.15 Asnoted, acute poisoning of the sodium-potassium ATPase pump may result in markedly elevated serum

8/7/2018
6/14
potassium levels, and the serum potassium level is a better indicator of end-organ toxicity and a better
prognostic indicator than the serum digoxin level in this circumstance.8
With chronic toxicity, in contrast to acute poisoning, the serum potassium and digoxin levels are lessdiagnostic. In these patients, the serum potassium is usually normal or low due to concomitant diuretictherapy, but may be elevated due to renal insu�iciency. Thus, in the setting of chronic toxicity, measuredserum potassium is more reflective of underlying comorbidities than the degree of inhibition of sodium-potassium ATPase by digoxin. Also, the serum digoxin level does not correlate with the clinical manifestationsand may be within therapeutic ranges despite significant cardiac toxicity.
Serum digoxin levels should be interpreted in the overall clinical context and not relied upon as the soleindicator of the presence or absence of toxicity. Generally accepted therapeutic digoxin levels are 0.5 to 2.0nanograms/mL (1.0 to 2.6 nmol/L), with corresponding toxic levels above 2.5 nanograms/mL (above 3.2nmol/L). Due to a relatively slow distribution phase, high digoxin levels sampled from the serum following arecent acute ingestion are not always an accurate indicator of concentration at receptor sites. Serum levels
are most reliable when obtained 6 hours a�er ingestion, when distribution is complete.15 However, given thepreceding limitations, it is still common that the higher the serum level, the greater is the likelihood of
toxicity.16 Importantly, the serum digoxin level should not be the sole factor in establishing the diagnosis ofdigoxin toxicity, so do not wait for a digoxin level before implementing therapy in an unstable patient.
Digoxin-like immunoreactive substances are substances that can be found in certain individuals that cross-react with the digoxin assay, artificially elevating the serum digoxin level, even in the absence of cardiacglycosides. Digoxin-like immunoreactive substances may be found in neonates, third-trimester pregnantwomen, patients with subarachnoid hemorrhage, and patients with renal or hepatic dysfunction. In addition,naturally occurring cardiac glycosides and cardioactive steroids from plants and animals may cross-reactwith digoxin assays. The degree of cross-reactivity is variable, and no reproducible correlation has been
established between serum levels of these substances and toxicity.17
TREATMENT
Management of a digoxin-poisoned patient includes general supportive care, treatment of specificcomplications of toxicity, prevention of further drug absorption, enhancement of drug elimination, antidote
administration when indicated, and safe disposition (Table 193–2).6 Although patients with intentional oraccidental ingestions may present with no symptoms, life-threatening complications of toxicity should beanticipated. Management of the asymptomatic patient should focus on preventing drug absorption andclosely monitoring for the development of toxicity. Continuous cardiac monitoring, IV access, and frequentreevaluations should be provided for any patient with a potentially toxic ingestion of digoxin.

8/7/2018
7/14
Table 193–2
Overview: Treatment of Digitalis Glycoside Poisoning
Asymptomatic patients
Obtain accurate history
Secure IV access
Initiate continuous cardiac monitoring
GI decontamination: activated charcoal, 1 gram/kg PO, can be considered in an awake, alert, cooperative
patient who presents within 1 h of ingestion
Frequent reevaluation
Symptomatic patients
Obtain accurate history
Secure IV access
Initiate continuous cardiac monitoring
GI decontamination: activated charcoal, 1 gram/kg PO, in an awake, alert, cooperative patient who presents
within 1 h of ingestion
Bradydysrhythmias
Atropine: 0.5–1.0 milligram IV as a temporizing measure for bradydysrhythmias while awaiting digoxin-
specific Fab antibodies
Transcutaneous pacing while awaiting digoxin-specific Fab antibodies for symptomatic bradycardia that does
not respond to atropine
Digoxin-specific antibody fragments: IV infusion (see discussion below for dose)
Cardiac arrest
CPR with current advanced cardiac life support protocols
Digoxin-specific antibody fragments: IV bolus (5–10 vials if amount ingested is unknown)
For the patient with life-threatening dysrhythmias, identify and rapidly correct conditions such as hypoxia,hypoglycemia, hypovolemia, and electrolyte abnormalities. IV magnesium may counteract ventricular
irritability seen with cardiac-glycoside toxicity.18 Use atropine and/or transvenous cardiac pacing as atemporizing treatment for bradydysrhythmias while preparing or obtaining digoxin-specific antibody
fragments.19
Digoxin-specific antibody fragments (digoxin-Fab) are the treatment of choice in acute poisoning withhyperkalemia (potassium >6.0 mEq/L) and in acute or chronic toxicity with any life-threatening
dysrhythmia.20,21,22 Hyperkalemia is not typically the cause of the death; it is a predictor of severe poisoningand increased mortality. Treatment of digoxin-induced hyperkalemia with insulin, dextrose, sodium
bicarbonate, or exchange resins does not reduce mortality.8

8/7/2018
8/14
Administration of calcium salts in cardiac glycoside–induced hyperkalemia is controversial. Older literatureindicated an increased incidence of ventricular dysrhythmias and a higher mortality when calcium wasadministered to digoxin-toxic patients. However, data from an animal model and retrospective review of alimited number of human patients with digoxin toxicity who received IV calcium found no increase in
ventricular dysrhythmias or mortality.23,24,25 In summary, hyperkalemia in acute digoxin poisoning indicatessevere toxicity and digoxin-Fab should be given to reduce mortality.
In chronic toxicity, hypokalemia and hypomagnesemia should be corrected, because both predispose todigoxin toxicity.
GI DECONTAMINATION AND ENHANCED ELIMINATION
Administrating activated charcoal may have utility in early acute ingestion of digoxin.22 Activated charcoalmay be of benefit following the acute ingestion of yellow oleander, although results of large, randomized
trials have been mixed.26 Gastric lavage is not recommended; asystole has been reported in a digoxin-toxicpatient, presumably from vagal stimulation during lavage, and no clinical benefit has been demonstrated.Cathartics, forced diuresis, hemodialysis, and hemoperfusion have no role in enhancing elimination ofdigitalis glycosides. In patients with chronic renal failure who develop digoxin toxicity, there are limited data
for the use of binding resins such as cholestyramine to help enhance elimination.27,28
DIGOXIN-SPECIFIC ANTIBODY FRAGMENTS (DIGOXIN-FAB)
Digoxin-Fab are derived from ovine antibodies to digoxin. Following IV infusion, the antibody fragments binddigoxin in the plasma and distribute widely throughout the body, removing digoxin from tissues. In severelypoisoned patients a�er digoxin-Fab administration, 90% will show reversal or significant improvement in life-threatening dysrhythmia; in most cases, clinical improvement occurs within 1 hour. Patients in cardiac arresthad a 50% survival when receiving digoxin-Fab during the resuscitation, which is significantly better than
historical survival with treatment with conventional therapies.20 Because of cross-reactivity with othercardiac glycosides, digoxin-Fab are also beneficial in treating digitoxin, foxglove, and oleander poisonings,
although large doses have sometimes been required.17,26 Indications for digoxin-Fab are life-threateningdysrhythmias (including hemodynamically significant bradydysrhythmias unresponsive to standard therapy)and hyperkalemia in excess of 6 mEq/L associated with acute poisoning.
Digoxin-Fab administration is associated with few adverse e�ects.20,21 Cardiogenic shock has been reported
in patients dependent on digoxin for inotropic support.29 In addition, ventricular response to atrialfibrillation may be increased. Hypokalemia may develop rapidly as digoxin toxicity is reversed. Mild, acutehypersensitivity reactions, including rash, flushing, and facial swelling, have been reported. No incidences of
serum sickness or anaphylaxis have been observed, even in patients with repeated administration.29 Skintesting has not proven to be useful in predicting allergic responses and may delay urgently needed

8/7/2018
9/14
*0.95 should be used instead of 0.8 if the preparation is an elixir or gel tablet; 1 should be used if the cardiac glycoside is
digitoxin.
treatment.30 Failures to digoxin-Fab therapy have been attributed to inadequate dosing, moribund state
before administration, and incorrect diagnosis of digoxin toxicity.29
A full neutralizing dose of digoxin-Fab is based on an estimation of the total-body load of digoxin, which canbe calculated from either the dose ingested or a steady-state serum digoxin level (Table 193–3). In an acutepoisoning, each vial of digoxin-Fab reverses approximately 0.5 milligram of ingested digoxin. Inhemodynamically stable patients, half the calculated full neutralizing dose is infused, and the other half is
given if an adequate clinical response is not seen in 1 to 2 hours.31 Observational studies report that a total of200 to 480 milligrams of digoxin-Fab (5 to 12 vials) were required to e�ectively treat severely digoxin-toxic
patients.20 When the ingested dose is unknown and serum level is unavailable, 10 vials are recommended asinitial treatment in life-threatening situations. Digoxin-Fab are administered IV through a 0.22-mm filter over30 minutes, except in cardiac arrest, when the dose is given as an IV bolus.
Table 193–3
Calculation of Digoxin-Specific Antibody Fragment Full Neutralizing Dose
Based on suspected amount
ingested
Digoxin body load (milligrams) = 0.8 × suspected ingested amount
(milligrams)*
Digoxin body load (milligrams) = serum digoxin concentration
(nanograms/mL) × 5.6 L/kg × weight (kg)/1000
One vial (about 40 milligrams) of digoxin-Fab neutralizes 0.5 milligram of
digoxin ingested
Based on total serum digoxin
concentration
Number of vials = serum concentration (nanograms/mL) × patient weight
(kg)/100
Calculations of a full neutralizing dose may overestimate the amount of digoxin-Fab necessary, and smaller
doses may adequately eliminate digoxin from the central compartment.32 An alternative approach in acutepoisoning with a hemodynamically stable patient is to give an 80-milligram (two vials) bolus of digoxin-Fab,evaluate the e�ect, and repeat the dose every 30 to 60 minutes as necessary until dysrhythmias haveresolved and potassium has normalized. Such a protocol may reverse toxicity with less than half of acalculated full neutralizing dose.
In chronic toxicity, an acceptable approach in the hemodynamically stable patient is to give a 40-milligram(one vial) bolus of digoxin-Fab and repeat a�er 1 hour if the patient is still symptomatic. One to three vials (40
to 120 milligrams) of digoxin-Fab are o�en adequate in reversing chronic toxicity.32

8/7/2018
10/14
1.
2.
3.
Total serum digoxin levels obtained following digoxin-Fab administration have little correlation with clinicaltoxicity. Because most laboratory assays do not distinguish between antibody-bound and unbound digoxin,
total serum levels obtained following digoxin-Fab administration may increase 10- to 20-fold.20 However,because the Fab-digoxin complex is not pharmacologically active, this increased level does not correlate with
clinical toxicity. The Fab-digoxin complex is eliminated by renal excretion.33
In the presence of renal failure, the Fab-digoxin complex may persist in the circulation for prolonged
periods.34 Recurrent toxicity can occur up to 10 days a�er digoxin-Fab administration in patients with renalfailure as the complex degrades. Due to the large molecular weight of the Fab-digoxin complex (45,000 to50,000 Da), hemodialysis does not enhance its elimination, although plasma exchange may be of
benefit.33,35,36 New liver support devices incorporating albumin-based dialysis and plasma filtration wouldbe expected to be able to clear the Fab-digoxin complex on the basis of molecular weight alone; some
devices have been reported to clear substances up to 100 kDa.37 However, there is no experience using thistechnique with digoxin-poisoned patients.
DISPOSITION AND FOLLOW-UP
Extended observation with serial digoxin and potassium levels is recommended for anyone with a confirmedacute ingestion. Asymptomatic patients should be observed until the serum digoxin level is decreasing onserial measurements and the potassium level has remained normal. Patients with signs of toxicity or ahistory of a large (>6 milligrams in an adult) ingested dose should be admitted to a monitored unit.Consultation with a medical toxicologist or the regional poison control center is recommended. Patients
receiving digoxin-Fab require intensive care unit observation for 6 to 12 hours.31 Patients in renal failure whoreceive digoxin-Fab may be at risk of delayed toxicity, as the Fab-digoxin complex can dissociate several dayslater. Finally, patients with suspected suicidality should undergo behavioral health or psychiatric evaluationbefore discharge.
REFERENCES
Ehle M, Patel C, Giugliano RP: Digoxin: clinical highlights: a review of digoxin and its use in contemporarymedicine. Crit Pathw Cardiol . 2011; 10: 93.
[PubMed: 21988950]
Hussain Z, Swindle J, Hauptman PJ: Digoxin use and digoxin toxicity in the post-DIG trial era. J Card Fail .2006; 12: 343.
[PubMed: 16762795]
Smith TW: Digitalis. Mechanisms of action and clinical use. N Engl J Med . 1988; 318: 358. [PubMed: 3277052]

8/7/2018
11/14
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
Ribner HS, Plucinski DA, Hsieh AM, et al. : Acute e�ects of digoxin on total systemic vascular resistance incongestive heart failure due to dilated cardiomyopathy: a hemodynamic-hormonal study. Am J Cardiol .1985; 56: 896.
[PubMed: 3904388]
Tisdale JE, Gheorghiade M: Acute hemodynamic e�ects of digoxin alone or in combination with othervasoactive agents in patients with congestive heart failure. Am J Cardiol . 1992; 69: 34G.
[PubMed: 1626491]
Kanji S, MacLean RD: Cardiac glycoside toxicity: more than 200 years and counting. Crit Care Clin . 2012;28: 527.
[PubMed: 22998989]
Piltz JR, Wertenbaker C, Lance SE, Slamovits T, Leeper HF: Digoxin toxicity. Recognizing the varied visualpresentations. J Clin Neuroophthalmol . 1993; 13: 275.
[PubMed: 8113441]
Bismuth C, Gaultier M, Conso F, E�hymiou ML: Hyperkalemia in acute digitalis poisoning: prognosticsignificance and therapeutic implications. Clin Toxicol . 1973; 6: 153.
[PubMed: 4715199]
Juurlink DN, Mamdani M, Kopp A, Laupacis A, Redelmeier DA: Drug-drug interactions among elderlypatients hospitalized for drug toxicity. JAMA . 2003; 289: 1652.
[PubMed: 12672733]
Vivo RP, Krim SR, Perez J, Inklab M, Tenner T Jr, Hodgson J: Digoxin: current use and approach totoxicity. Am J Med Sci . 2008; 336: 423.
[PubMed: 19011400]
Schmiedl S, Szymanski J, Rottenkolber M, Hasford J, Thurmann PA: Re: Age- and gender-specificincidence of hospitalisation for digoxin intoxication. Drug Saf . 2007; 30: 1171.
[PubMed: 18035869]
Bhatia SJ: Digitalis toxicity—turning over a new leaf? West J Med . 1986; 145: 74. [PubMed: 3529634]
Moorman JR, Pritchett EL: The arrhythmias of digitalis intoxication. Arch Intern Med . 1985; 145: 1289. [PubMed: 4015280]
Ma G, Brady WJ, Pollack M, Chan TC: Electrocardiographic manifestations: digitalis toxicity. J EmergMed . 2001; 20: 145.

8/7/2018
12/14
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
[PubMed: 11207409]
Dawson AH, Whyte IM: Therapeutic drug monitoring in drug overdose. Br J Clin Pharmacol . 1999; 48:278.
[PubMed: 10510137]
Selzer A: Role of serum digoxin assay in patient management. J Am Coll Cardiol . 1985; 5 (5 Suppl A):106A.
[PubMed: 3886746]
Dasgupta A, Emerson L: Neutralization of cardiac toxins oleandrin, oleandrigenin, bufalin, andcinobufotalin by digibind: monitoring the e�ect by measuring free digitoxin concentrations. Life Sci . 1998;63: 781.
[PubMed: 9740315]
French JH, Thomas RG, Siskind AP, Brodsky M, Iseri LT: Magnesium therapy in massive digoxinintoxication. Ann Emerg Med . 1984; 13: 562.
[PubMed: 6742564]
Chen JY, Liu PY, Chen JH, Lin LJ: Safety of transvenous temporary cardiac pacing in patients withaccidental digoxin overdose and symptomatic bradycardia. Cardiology . 2004; 102: 152.
[PubMed: 15334025]
Antman EM, Wenger TL, Butler VP Jr, Haber E, Smith TW: Treatment of 150 cases of life-threateningdigitalis intoxication with digoxin-specific Fab antibody fragments. Final report of a multicenter study.Circulation . 1990; 81: 1744.
[PubMed: 2188752]
Lapostolle F, Borron SW, Verdier C, et al. : Digoxin-specific Fab fragments as single first-line therapy indigitalis poisoning. Crit Care Med . 2008; 36: 3014.
[PubMed: 18824911]
Roberts DM, Buckley NA: Antidotes for acute cardenolide (cardiac glycoside) poisoning. CochraneDatabase Syst Rev . 2006; 4: CD005490.
[PubMed: 17054261]
Hack JB, Woody JH, Lewis DE, Brewer K, Meggs WJ: The e�ect of calcium chloride in treatinghyperkalemia due to acute digoxin toxicity in a porcine model. J Toxicol Clin Toxicol . 2004; 42: 337.
[PubMed: 15461240]
Levine M, Nikkanen H, Pallin DJ: The e�ects of intravenous calcium in patients with digoxin toxicity. JEmerg Med . 2011; 40: 41.

8/7/2018
13/14
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
[PubMed: 19201134]
Van Deusen SK, Birkhahn RH, Gaeta TJ: Treatment of hyperkalemia in a patient with unrecognizeddigitalis toxicity. J Toxicol Clin Toxicol . 2003; 41: 373.
[PubMed: 12870880]
Rajapakse S: Management of yellow oleander poisoning. Clin Toxicol (Phila) . 2009; 47: 206. [PubMed: 19306191]
Henderson RP, Solomon CP: Use of cholestyramine in the treatment of digoxin intoxication. Arch InternMed . 1988; 148: 745.
[PubMed: 3341874]
Roberge RJ, Sorensen T: Congestive heart failure and toxic digoxin levels: role of cholestyramine. VetHum Toxicol . 2000; 42: 172.
[PubMed: 10839325]
Hickey AR, Wenger TL, Carpenter VP, et al. : Digoxin immune Fab therapy in the management of digitalisintoxication: safety and e�icacy results of an observational surveillance study. J Am Coll Cardiol . 1991; 17:590.
[PubMed: 1993775]
Kirkpatrick CH: P Allergic histories and reactions of patients treated with digoxin immune Fab (ovine)antibody. The Digibind Study Advisory Panel. Am J Emerg Med . 1991; 9 (2 Suppl 1): 7.
[PubMed: 1997020]
Bateman DN: Digoxin-specific antibody fragments: how much and when? Toxicol Rev . 2004; 23: 135. [PubMed: 15862081]
Chan BS, Buckley NA: Digoxin-specific antibody fragments in the treatment of digoxin toxicity. ClinToxicol (Phila) . 2014; 52: 824.
[PubMed: 25089630]
Cli�on GD, McIntyre WJ, Zannikos PN, Harrison MR, Chandler MH: Free and total serum digoxinconcentrations in a renal failure patient a�er treatment with digoxin immune Fab. Clin Pharm . 1989; 8: 441.
[PubMed: 2743737]
Ujhelyi MR, Robert S: Pharmacokinetic aspects of digoxin-specific Fab therapy in the management ofdigitalis toxicity. Clin Pharmacokinet . 1995; 28: 483.
[PubMed: 7656506]

8/7/2018
14/14
35.
36.
37.
Zdunek M, Mitra A, Mokrzycki MH: Plasma exchange for the removal of digoxin-specific antibodyfragments in renal failure: timing is important for maximizing clearance. Am J Kid Dis . 2000; 36: 177.
[PubMed: 10873888]
Rajpal S, Beedupalli J, Reddy P: Recrudescent digoxin toxicity treated with plasma exchange: a casereport and review of literature. Cardiovasc Toxicol . 2012; 12: 363.
[PubMed: 22618329]
Krisper P, Stadlbauer V, Stauber RE: Clearing of toxic substances: are there di�erences between theavailable liver support devices? Liver Int . 2011; 31 (Suppl 3): 5.
[PubMed: 21824275]
McGraw HillCopyright © McGraw-Hill Global Education Holdings, LLC.
All rights reserved. Your IP address is 50.26.48.115
Terms of Use • Privacy Policy • Notice • Accessibility
Access Provided by: Brookdale University Medical CenterSilverchair