chapter 14 injuries to the tissues. oa 10.21 differentiate between a primary injury and secondary...
TRANSCRIPT

Chapter 14
Injuries to the Tissues

2
OA 10.21
• Differentiate between a primary injury and secondary injury

Objectives
• Introduce the terminology associated with injury classification
• Introduce biomechanical forces that cause injuries
• Explain biomechanical concepts for various tissues

Injury classification
• Intrinsic– Infection (viral, bacterial)
• Extrinsic– Tissue stressed to the point of mechanical
failure due to excessive force

Extrinsic injury classification
• Primary Injury– Direct immediate consequence of
excessive force (trauma)
• Secondary Injury– Delayed injury some time after initial
trauma– An accommodation to the primary injury

Extrinsic injury classification
• Acute Injury– Mechanical failure of soft tissue due to
excessive force occurring in a single bout– Sudden onset of short duration

Extrinsic injury classification
• Chronic Injury– Mechanical failure of soft tissue due to
repeated micro-trauma occurring over an extended period of time
– Gradual onset and are of prolonged duration
Injury classification
• Microtrauma– Occurs with repeated submaximal forces
over time, and the tissues are unable to adapt
• Macrotrauma– Occurs when a single force exceeds the
tissue’s failure point

Open vs. closed
• Open– Exposed – Breaks the surface of the skin
• Closed– Unexposed – Any injury that does not involve disruption
of the skin surface

Mechanical stresses
• Load/Stress– External/internal force acting on the tissue– Force = Mass x Acceleration (F=ma)
• Deformation/Strain– Extent of deformation under loading

load/deformation
• Mechanical force causes deformation
• Degree of deformation depends on:– Tissue composition– Speed of applied
load– Frequency of loading– Direction of loading
Deformation
Load

Yield point
• Load is greater than mechanical capabilities of the tissue
• Elastic limit of the tissue has been reached
• Mechanical failure occurs
Deformation
Load YieldPoint
UltimateFailurePoint
ElasticRegion
PlasticRegion

Tissue stresses
• Five primary mechanical forces that cause injury– Tension– Compression– Bending– Shear– Torsion

Tissue stresses
• Can occur alone or in combination
• Type of force = Mechanism of Injury (MOI)

tension
• Creates a pulling action trying to elongate the structure– Longitudinal “tearing” stress– Overstretched tissue (i.e. valgus force)
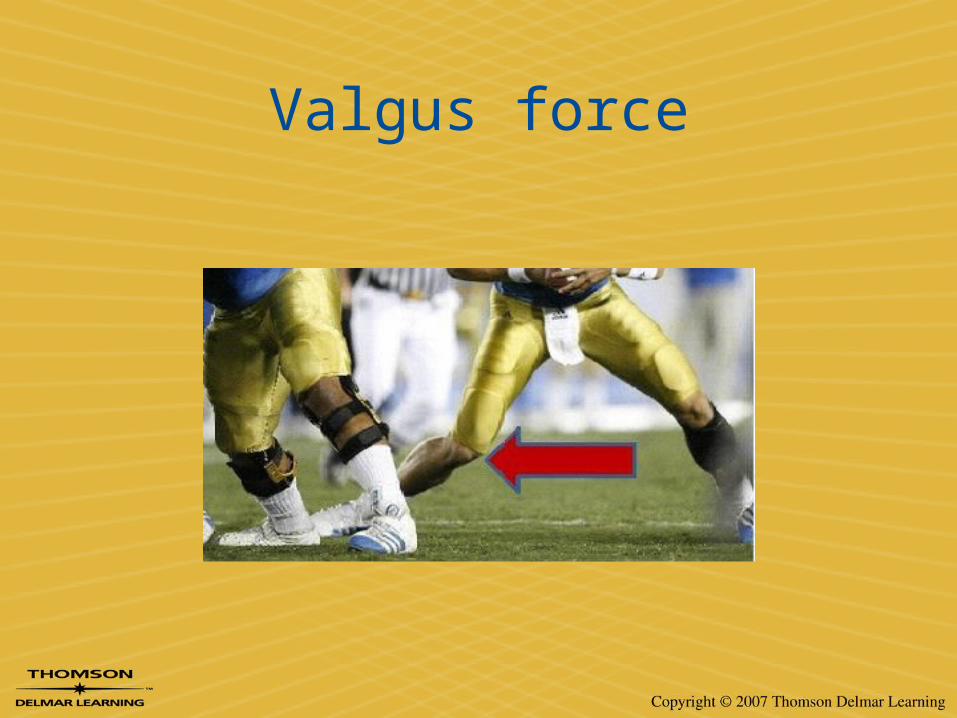
Valgus force

compression
• Creates a pushing action tending to shorten the structure– Stress is applied at each end (i.e. FOOSH)

FOOSH

bending
• Loading about an axis – Combination of tension and compression

Shear force
• Force that acts perpendicular to the surface of a structure

Shear force

torsion
• Load applied causing structure to twist about an axis

23

Combined loading
• Tissue is seldom loaded in one mode only
• Subjected to multiple indeterminate loads
• Geometric structure is irregular

forces

26
OA 10.22
• Give an example of each of the 5 mechanical forces that cause injury.

SUPERFICIAL INJURIES

Integumentary System
• Skin and structures derived from it– Hair, nails, sweat
and oil glands

Functions
– Regulate body temperature– Protects body– Receives stimuli
• Temp, pressure, pain
– Eliminates waste • Sweat

Three Layers
• Epidermis:– Most Superficial

Three Layers
• Dermis: – Tough, Leathery
Fibrous Connective Tissue
– Partly Vascularized

Three Layers
• Subcutaneous (Hypodermis):– Superficial Fascia– Mostly Fat (Insulate
& Absorb Shock)– Anchors Skin to
Underlying Structures

Three Layers

Injurious Mechanical Forces
• Friction• Scraping• Compression• Tearing• Cutting• Penetrating

Open Vs. Closed
• Open– Exposed – Breaks the surface of the skin
• Closed– Unexposed – Any injury that does not involve disruption
of the skin surface

Abrasions
• Scraping away of the superficial tissue– Sliding or skidding across a surface
• Superficial in depth, large in area• Bleeding is minimal, risk of infection is
great


Laceration
• Irregular cut caused by tearing forces– Jagged wound edges– Can be minor or very deep


Puncture
• Penetration of the skin by an object– Most susceptible to infection– why?– Impaling = object is embedded & partially
sticks out


Incision
• A clean, straight, knife-like cut– Commonly caused by a surgeon


Avulsion
• Tearing away of tissue, commonly paired with a laceration.– Flap avulsion – tissue is still connected


Calluses
• Skin thickening due to increased friction or intermittent pressure


Blister
• Excessive friction combined with shear forces causing fluid build-up under the skin
General Principles Of Wound Care

Chain of infectionRESERVOIR HOST
• Infected individual
PORTAL OF EXIT• Nose, mouth, eyes,
urinary/reproductive system, open wounds
ROUTE OF TRANSMISSION
• Direct or indirect contact
PORTAL OF ENTRY• Nose, mouth, eyes,
urinary/reproductive system, open wounds
SUSCEPTIBLE HOST• Very young and elderly are most
susceptible
pathogen

Universal Precautions
• Those in direct contact must use protective equipment– Non-latex gloves, gowns, aprons, masks & face
shield, eye protection, CPR barriers– Emergency kits should include gloves, CPR
barrier, alcohol prep pads at minimum

Universal Precautions
• Doubling gloves is suggested with severe bleeding

Universal precautions
• Use Personal Precautions– Extreme care must be used with glove
removal– Glove Removal

Universal precautions
• Use Personal Precautions– Wash hand & skin surfaces
• Proper Hand Washing

Supplies to have on hand
• Non-latex gloves• Sterile 4”x4” gauze
pads/sponges• Sterile saline solution• Non-adherent pads• Antiseptic/antibiotic
ointment• Non-adherent
cohesive tape
• Optional: soap, water, hand sanitizer, hydrogen peroxide, cinder suds, nitrotan

bleeding
• 3 types of external bleeding– Venous – dark red blood, slowly flowing– Capillary – bright red, seeping/oozing– Arterial – bright red, spurts or streams

Controlling bleeding
• For all types of bleeding direct pressure must be applied to the area– Blood takes 4-6 minutes to clot

Controlling bleeding
• Use a sterile gauze pad/compress to collect the blood– If saturated, add additional gauze as
needed• Never remove and replace, always add!
Controlling bleeding
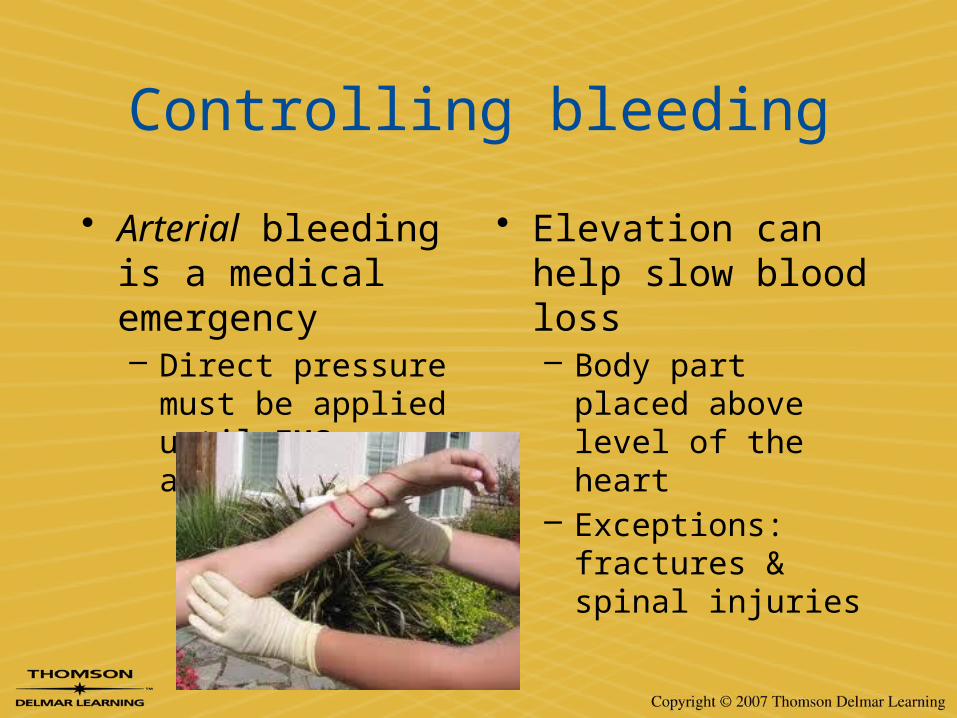
• Arterial bleeding is a medical emergency– Direct pressure must
be applied until EMS arrives
• Elevation can help slow blood loss– Body part placed
above level of the heart
– Exceptions: fractures & spinal injuries

Controlling bleeding
• Indirect pressure can slow blood loss– Pressure points proximal to the injury must
be compressed

Controlling bleeding
• An ice pack causes vasoconstriction (narrowing of blood vessels), slowing bleeding

Wound cleansing
• Debridement - removal of dead, damaged, or infected tissue to improve the healing potential of the remaining healthy tissue.

Wound cleansing
• Cleansing and debriding a wound prevents infections and increases healing time.

64
OA 10.23
• List in order the four methods for controlling bleeding.

Wound cleansing
1. Remove any dirty bandages, clothing, etc. from the wound
2. Apply a solution to irrigate the wound1. Saline, sterile water, etc.
3. Clean the wound with circular motion starting at the center and working outwards
4. Irrigate the wound once more to remove all dirt & debris
5. Dry the area with sterile gauze
6. Cover the wound with a sterile dressing


Applying bandages & dressings
• Dressing = contact with the wound• Bandage = holds dressing in place

Applying bandages & dressings
• Bandages and dressings decrease the risk of infection if properly applied and maintained– Must cover the wound entirely and stay in
place– Allow for normal movement and activity– Absorb blood and drainage– Protect the wound from
further injury

Bandage & dressing types
• Dressings:– Non-adherent pads– Vasiline gauze– Telfa pads– Adaptic pads– Xeroform gauze

Bandage & dressing types
• Bandages– Sterile gauze– ABD dressings– Rolled gauze– Oval eye pads– Adhesive bandages

Applying dressings
1. Select the proper dressing
2. Ensure the wound is cleansed
3. Apply antibiotic ointment to the dressing
4. Place dressing directly over the wound

Applying bandages
1. Select appropriate bandage1. Allows movement
2. Remains sturdy
2. Remove jewelry, clothing, etc. near bandage site1. Circulation can be impaired with swelling
3. Leave fingers & toes exposed1. To check circulation

Applying bandages
4. Cover the dressing entirely
5. Apply bandage snugly, but not too tightly1. Apply in the position they will remain in
6. Secure loose ends with tape, or tuck them in


Wound care management
• Patient instructions– Keep wound clean and dry– Change dressings daily– Remove and replace if wet– Watch circulation of the limb; seek medical
help if circulation is impaired– Watch for signs of infection

Signs of infection
• Redness• Swelling• Increased pain• Red streak up the arm or leg• Foul-smelling odor• Elevation in temperature
over the wound or surrounding tissue

77
OA 10.24
• List the 6 signs of infection

Tissue stresses
• Five primary mechanical forces that cause injury– Tension– Compression– Bending– Shear– Torsion

Tissue stresses
• Can occur alone or in combination
• Type of force = Mechanism of Injury (MOI)


Five Major Functions Of The Skeleton
• Protection of vital soft tissues• Support human posture• Movement by serving as points of
attachment for muscles• Storage for minerals• Hemopoiesis – the process of blood
formation that occurs in the red bone marrow

Mechanical properties of bone
• Wolff’s Law: bone will adapt to the loads under which it is placed.

Mechanical properties of bone
• Direction of Loading– Strongest in compression– Weak in tension– Weakest in shear
Compression > Tension > Shear

Mechanical properties of bone
• Bone size– ↑ size of bone (mass) = ↑ bone strength– Greater area to distribute mechanical
stresses

Mechanical properties of bone
• Bone shape– Sudden shape changes are areas where
mechanical stresses are most concentrated• Weak points/Stress risers

Bone growth
• Epiphyseal growth plate– Cartilaginous disk near
the end of each long bone
– Dependent on plate– Injury can prematurely
close the plate causing loss of length

Mechanisms of bone injuries
• Pure tensile forces
• Compression forces
• Bending

Three-point bending
• ↑ distance from center = ↑ bending moment
Tensile Force
Compressive Force


90
SKELETAL INJURIES

Bone injuries
• Periostitis– Inflammation of the periosteum, usually
from contusion
• Bone contusion– Bruising of the bone tissue– Very painful– Slow to heal – typically 6-8 weeks
Live Injuries
• Proper Field Set-Up• Femur• ACL• Knee• Broken Leg

93
OA 10.28
• Describe the properties of bone that make it strongest, weakest, and most prone to injury.

Bone injuries
• Fracture– Any disruption in the continuity of the bone
or periosteum

Bone injuries
• Description of Fracture– Site– Extent – partial, complete, hairline– Configuration - type– Relationship of fragments – displaced,
non-displaced– Relationship to external environment –
closed, compound

Incomplete Fracture

Undisplaced Fracture

Displaced Fracture

Open (Compound) Fracture

Bone trauma classificationType EtiologyTransverse Direct BlowSpiral Rotation on planted footOblique One end fixed, other sudden
torsionComminuted Blow or fall in awkward positionDepressed Flat bones, direct blow

Bone trauma classificationType EtiologyGreenstick Incomplete Fx, skeletally
immature (convex)Longitudinal Splits along length, jumping
from heightSerrated Direct blow, jagged edgesContrecoup Side opposite to point of impactImpacted Compressive force on long axis
of bone

Transverse Fracture
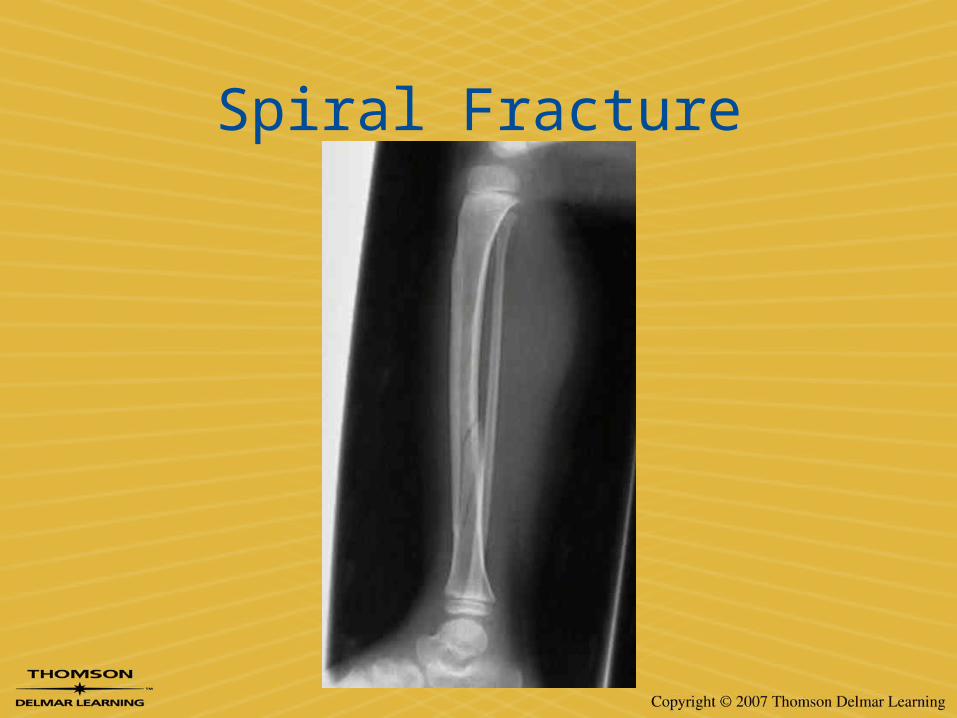
Spiral Fracture

Oblique Fracture

Comminuted Fracture

Depression Fracture
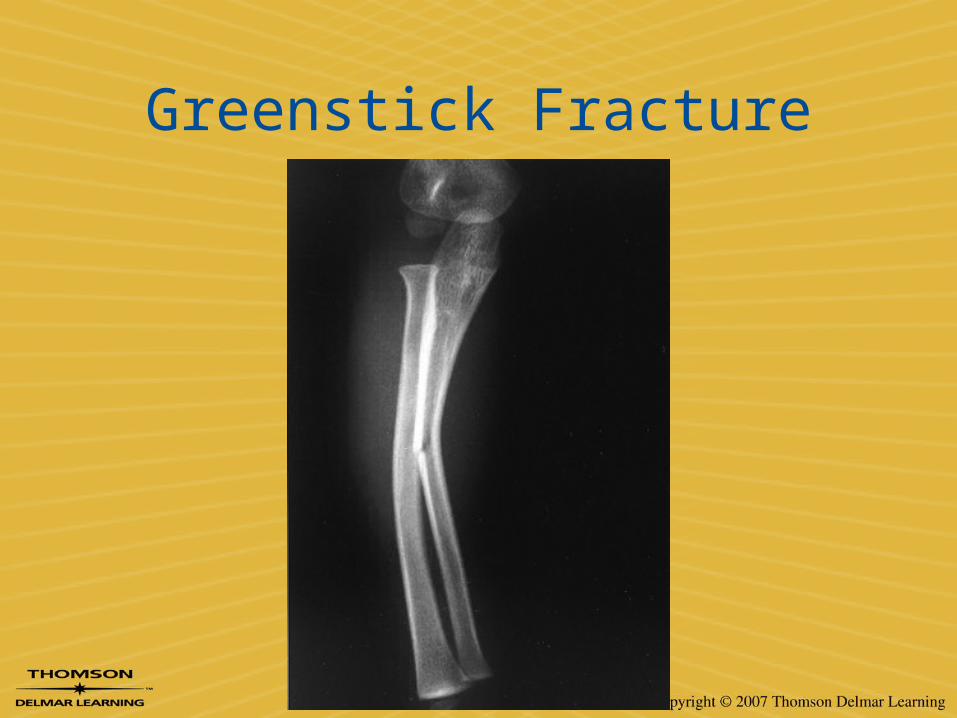
Greenstick Fracture

Longitudinal fracture

Serrated fracture

Impacted Fracture

Other fractures
• Some fractures have names based on founder, mechanism, common type– Bennett’s fracture– Maisonneuve fracture– Boxer’s fracture– Bankart fracture– Pott’s fracture– Many, many more

Bennett’s fracture

Maisonneuve fracture

Boxer’s fracture

Bankart fracture

Pott’s fracture

Stress Fractures
• Also called march, fatigue, & spontaneous fractures
• Weight bearing bones become weaker before they become stronger

Stress Fractures
• Typical causes in sports:– Coming back too soon after injury or illness– Changing events without proper training– Starting initial training too quickly– Changing habits or the environment

Stress Fracture

Avulsion Fracture

Avulsion Fracture

Joints (Articulations)
• All joints are comprised of capsular tissue surrounding the joint itself– Strong, fibrous tissue
• Synovial joints– Capsular tissue– Articular cartilage at ends of bones– Synovial membrane & fluid– Muscles affecting the joint

Synovial Joints
• Synovial Membrane & Fluid– Membrane made of connective tissue for
articular capsule– Fluid is secreted & absorbed in membrane;
acts as lubricant

Synovial Joints
• Articular Cartilage– Connective tissue providing support– Hyaline (nasal septum), fibrous (vertebral
disks & menisci), & elastic (ear)– Aids in motion control, stability, and load
transmission for joints


Functional Synovial Joint Characteristics
• Synovial Joint Stabilization– Provided by skeleton, ligaments, joint
capsules and muscles– Reflex contraction of muscles to prevent
overstretch

Functional Synovial Joint Characteristics
• Articular Capsule & Ligaments– Elastic fibers as opposed to contractile– Fast protective response time– Ligaments are strongest in center of
ligament

Synovial Joint Trauma
• Constant compression or tension can lead to ligament or capsular deterioration
• Intermittent compression or stress can increase strength

Synovial Joint Trauma
• Tension, torsion, or twisting forces that exceed yield point will lead to injury
• Articular cartilage failing to properly transmit load may lead to failure

Synovial Joint Injury Classification
• Acute Joint Injuries– Joint Sprains
• Stretch or tear of stabilizing connective tissue
• Severity Grading

Synovial Joint Injury Classification
• Acute Joint Injuries– Acute synovitis
• Injury to synovial membrane of joint
• Result of contusion or sprain

Synovial Joint Injury Classification
• Acute Joint Injuries– Subluxations &
dislocations• Disruption of the joint
capsule & membraneor joint surfaces

Synovial Joint Injury Classification
• Chronic Joint Injuries– Osteochondrosis
• Degenerative changes in ossification centers of epiphyses of bones
• Joint (OCD) or tuberosity (apophysitis)

Synovial Joint Injury Classification
• Chronic Joint Injuries– Osteoarthritis
• Wearing down of cartilage• Most often in weight-bearing
joints

135
OA 10.30

Synovial Joint Injury Classification
• Chronic Joint Injuries– Bursitis
• Caused by overuse or external compression/trauma

Synovial Joint Injury Classification
• Chronic Joint Injuries– Capsulitis & synovitis
• Degenerative tissue changes
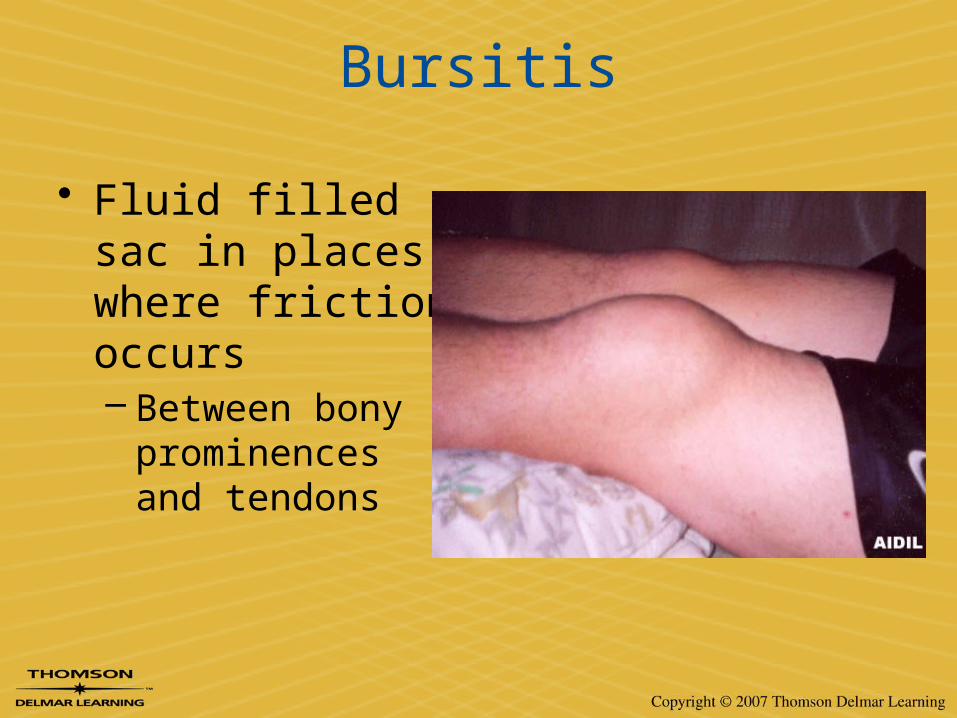
Bursitis
• Fluid filled sac in places where friction occurs– Between bony
prominences and tendons

Tendons and Ligaments
• Functions– Tendons
• Execute joint motion by transmitting mechanical forces from muscles to bones
– Ligaments• Join bones and provide stability to joints
• Inert Structures– Non-contractile structures (passive tissues)– Unable to actively generate forces
Mechanical Properties of Tendon
• Composed of mostly collagen fibers– High resistance to tensile forces
• Location– Strongest in mid-point– Weakest at myo-tendinous and osteo-
tendinous junctions• Due to changes in tissue composition

Tendon Injuries
• Tendinitis – inflammation of the tendon– Chronic injury due to repetitive motion or
overuse– Appears as dull, aching pain
before/during/after exercise– Occurs with crepitus

Tendon Injuries
• Tenosynovitis – inflammation of the synovial sheath– More severe form of “-itis” injury

Tendon Injuries
• Strain / Rupture – overload of the tendinous junction
• Contusion

Tendon Injury
• Attaches muscle to bone
• Usually double the strength of the muscle it serves
• Acute strain• Tendonitis

Mechanisms of Tendon Injuries
• High magnitude, single load, tensile forces– Acute strain or rupture
• Low magnitude, repetitive load, tensile forces– Tendinitis or tenosynovitis
Dynamite vs. Axe

Mechanical Properties of Ligaments
• Greater proportion of elastic collagen fibers than in tendon– Less resistant to
tensile forces– Greater deformation
occurs prior to mechanical failure

Mechanical Properties of Ligaments
• Frequency of Loading– Repeated loading Mechanical Weakening
instability
• Direction of Loading– Resists tensile forces

Mechanisms of Ligament Injuries
• High magnitude, single load, tensile forces– Acute sprain or rupture
• Low magnitude, repetitive load, tensile forces– Constant tensile forces lead to ligamentous
deterioration– Chronic instability

Mechanisms of Ligament Injuries

Grades of Ligamentous Injury
Degree Etiology End Feel Instability
First Mild overstretching, no tissue disruption
Firm None
Second Partial disruption or macrotearing of the ligament
Definite (soft) Slight to Moderate
Third Complete disruption None Severe

Skeletal Muscle
• Composed of contractile cells• Function
– Generates force to drive motion– Dynamic stability of joints

Skeletal Muscle
• Tensile Forces– Produces active and passive tensile forces– Active tension contraction– Passive tension stretched past resting
length

Skeletal Muscle Injuries
• Strains• Contusions• Muscle
lacerations• Myositis
• Atrophy• Contracture• DOMS• Spasm

Muscle Injury
• Acute– Contusions
• Sudden traumatic blow with compressive force
• Superficial or deep tissue affected
• Rated by the ability of muscle to produce ROM

Muscle Injury
• Acute– Strains
• Stretch or tear in muscle• Abnormal muscle contraction
– Mineral imbalance or dehydration
– Fatigue– Strength imbalance

Muscle Injury
• Acute– Muscle spams (cramps)
• Clonic - intermittent• Tonic – constant• Contracture• May lead to strains• DOMS

Muscle Injury
• Chronic– Myositis
• Inflammation of muscle
– Fasciitis• Inflammation of fascia
within the muscle
– Myositis ossificans• Repeat trauma• Calcium deposits within
the muscle• Can resorb in 9-12
months

Mechanisms of Muscle Injuries
• High magnitude, single load, tensile forces– Acute strains or ruptures
• Low magnitude, repetitive load, tensile forces– Degenerative effect
Dynamite vs. Axe

Grades of Muscle Injuries
Degree Etiology Signs/Symptoms
First Overstretching or microtearing of muscle or tendon
Mild loss of strength, swelling, ecchymosis, point tenderness
SecondFurther stretching and partial tearing of muscle or tendon fibers
Symptoms are more severe, greater function loss
Third Complete ruptureSevere symptoms, loss of muscle function, possible palpable defect
Nerve Injuries
• Compression or tensioning of neural structure– Secondary to direct blow– Acute swelling in enclosed space– Pathology which compromises space for
nerve
Nerve Injuries
• Anesthesia – absent sensation• Paresthesia – diminished sensation• Hyperesthesia – over-sensation

Neuropraxia
• “Burners” or “stingers”• Transient and reversible loss in nerve
function • Secondary to trauma or irritation• Mechanical deformation of the nerve• Disruption of nerve fibers & signals• Short-lived sensory and motor deficits
(seconds-two weeks)

A shortstop is hit in the shin by a batted ball that took a bad hop
• What kind of force is involved?• What type of injury is likely to have
occurred?

A football player sustains repeated blows to his left quadriceps muscle
• What type of injury could be sustained from repeated compressive forces to the muscle?

A basketball player steps on another player’s foot and sustains a lateral ankle injury
• What forces are applied?• What type of injury has occurred?

An alpine skier catches his right ski tip and severely twists the lower leg
• What type of serious injury could be created by this mechanism?