chapter 10 thyroid hormones - risscontents.kocw.net/kocw/document/2015/pusan/kimnamdeuk/10.pdf ·...
TRANSCRIPT

Chapter 10
Thyroid Hormones
Nam Deuk Kim, Ph.D.
1

Timeline of Thyroid Studies (@ American Thyroid Association)
Year Event
2700
BC
Emperor Shen Nung’s prescriptions (first published in Pen Tsao, the herbal
of the Chinese pharmacopoeia, 1596) mentions the use of seaweed for the
treatment of goiter
300 BC Ayur Veda, Hindu holy text, discusses goiter.
40 BC Pliny, Vitruvius, and Juvenal describe prevalence of goiter in the Alps and
use of burnt seaweed for treatment.
138 AD Greek physician, Soranus, mentions neck swelling following pregnancy
340 Ko-Hung, Chinese alchemist, recommends seaweed for treatment of goiter
among people living in mountains
650 Sun Ssu-Mo, a Chinese physician, uses dried, powdered mollusc shells
and chopped thyroid gland for the treatment of goiter
961
Abul Kasim, personal physician to Caliph El-Hakin III of Codoba, is first to
describe thyroidectomy for goiter and to perform a needle biopsy of the
thyroid.
1170 Roger of Salerno uses seaweed in the treatment of goiter
1200 Arnaldus de Villanova reports that marine sponges could be used to treat
goiters of recent origin in the young 2

Year Event
1475 Chinese physician, Wang Hei, recommends treatment of goiter with minced
thyroid.
1500 Leonardo da Vinci is first person to recognize and draw the thyroid gland
1543 Andreas Vesalius provides first anatomic description and illustration of the
thyroid gland
1563 Eustachius introduces the term “isthmus” to describe tissue connecting the two
lobes of the thyroid
1602 Felix Platter gives first description of cretins (see 1754) found in Valais region
of Switzerland.
1656 Thomas Wharton names gland “thyroid” after the shape of an ancient Greecian
shield
1669 Albrecht van Haller describes constipation as a complication of cretinism
1754 First use of the term “cretin” in the medical literature. The term is derived from
the Latin “christianus” as affected individuals are incapable of committing a sin
1789 F.E. Fodere suggests an association between goiter and cretinism
3

1802
Giuseppe Flajani, personal physician to Pope Pius VII (1800-1823), described
association of palpitations, goiter, and bulging of the eyes. This triad was known as
Morbus Flajani.
1811 Bernard Courtois discovers iodine by oxidizing burnt seaweed (i.e. kelp 다시마류)
with sulfuric acid
1813 Gay-Lussac names the vapor discovered by Courtois iodine, from the Greek word
for violet
1818 Goiter reported in British Columbia
1820 Jean Francois Coindet concludes that iodine deficiency causes goiter and begins
treatment of goiter with iodine.
1824
Alexander von Humboldt reports endemic goiter in Andes. He observes that goiter
size decreases by 1/3 when an individual moves to an area where goiter is not
endemic
1825 C. Parry describes exophthalmic goiter
1825
Boussingault detects iodine in the natural salt from mines in the northern Andes.
Working in Bogota, he then recommends iodinated salt to prevent and treat
endemic goiter
1829
LGA Lugol recommends use of aqueous solution of iodine made from KI for
treatment of scrofula (a neck mass from a goiter and cervical adenopathy due to
tuberculosis and lymphoma were considered identical processes)
1831 Francisco Freire-Allemao, a Brazilian physician, proposes iodine prophylaxis as a
government-administered public health program, for goiter prevention.
1834 Robert Graves describes a syndrome of palpitations, goiter, and exophthalmos in
three women.
4

1848 C. von Basedow describes exophthalmic goiter
1849 J.L. Prevost adds iodine to food and water to prevent goiter
1850 T.B. Curling describes cretinism with athyreosis
1851
A. Chatin detects iodine in freshwater plants and recommends these as
prophylaxis for endemic goiter based upon his theory that goiter is due to low little
iodine in drinking water
1857 B. Niepce describes enlargement of sella turcica in cretins with hypothyroidism in
Switzerland
1857 Maurice Schiff successfully performs total thyroidectomies in animals
1860 R. Virchow suggests that cretinism and goiter are related
1862 A. Trousseau introduces the term “Graves disease”
1864 Baillarger reports occurrence of goiter in animals where goiter and cretinism are
widespread
1867 A. von Graefe describes lid lag in thyrotoxicosis (Basedow’s disease)
1873 Th. Billroth describes tetany following total thyroidectomy
1877 William Gull publishes “On a Cretinoid State Supervening in Adult Life in Women”
1882 William Ord coins term myxedema to describe middle aged women with cretinoid
features
1883 J.L. Reverdin describes cretinism following thyroidectomy.
1883 Heinrich Bircher recognizes association of endemic goiter with geologic features
characteristic of Quarternary glaciation
1883 E.T. Kocher calls attention to myxedema following thyroidectomy. He was awarded
the Nobel Prize in 1909 for his work on the thyroid gland.
5

1884
First report of the use of thyroidectomy for the treatment of Graves’ disease.
Rehn L,. Ueber die Extirpation des Krops dei Morbus basedowii. Berl Klin
Wochenschr 1884; 21: 163-166.
1886 Pierre Marie describes the characteristic tremor of hyperthyroidism
1888 Rogowitsch observes pituitary hyperplasia in rabbits following thyroidectomy
1891 F.D. von Recklinghausen reports on the occurrence of osteoporosis in
hyperthyroidism
1891 Victor Horsley, using monkeys, shows that myxedema, cretinism, and post-
thyroidectomy cachexia are all due to a deficiency of thyroid function.
1891 G.R. Murray introduces the use the thyroid extract to treat myxedema
1895 Aldolf Magnus Levy describes the influence of the thyroid on the basal metabolic
rate
1896 E. Drechsel discovers first iodine-containing protein, “gorgonin”, in the axial
skeleton of coral.
1896 Eugen Baumann discovers iodine as a natural constituent of the thyroid and
names it “iodothyrin”.
1896 B. Riedel publishes first description of chronic, fibrous thyroiditis.
1897 Pendred describes association of goiter with deaf-mutism.
1898 W. Osler publishes case reports of sporadic cretinism, some of whom had a
family history of goiter.
1898 von Notthalt describes thyrotoxicosis factitia and suggests that excess thyroid
hormone produces Graves disease. 6

1902 F. de Quervain describes subacute granulomatous thyroiditis
1905 Robert Abbe treats Graves disease by implanting radium into the patient’s goiter
1907 H.L. Wheeler and G.S. Jamieson show that gorgonia, from coral, is
diiodotyrosine.
1907 David Marine publishes that iodine is necessary for thyroid function.
1907 David Marine recommends treating Graves disease with iodine
1910
Charles H. Mayo introduces term “hyperthyroidism” to describe the clinical
conditions of primary exophthalmic goiter, toxic adenoma, and adenomatous
goiter with hyperthyroidism.
1911 D. Marine and C.H. Lenhart describe hyperthyroidism due to Graves disease
and concomitant functioning thyroid
1911 Henry Plummer from the Mayo Clinic distinguishes exophthalmic goiter from
adenomatous goiter
1912 Kocher coins term Jod Basedow for iodine over-dosage.
1912 J.F. Gudernatsch observes that thyroid extract has a specific effect on
accelerating the differentiation (metamorphosis) in amphibian larva.
1912 A. Seidell and F. Fenger describe the seasonal variation in thyroid iodine
content.
1913 Massachusetts General Hospital establishes Thyroid Unit under the direction of
J.H. Means.
1914 H. Hashimoto publishes 4 cases of a thyroid disorder characterized by a diffuse
lymphocytic infiltration and fibrosis of the gland. 7

1915 E.A. Kendall isolates thyroxine, a name he creates from a contraction of the term
“thyroxindole”.
1916 Phillip E. Smith and Bennet M. Allen independently report that Hypophysectomized
tadpoles show thyroid involution and do not undergo metamorphosis.
1916
H. Hunziker proposes that endemic goiter is due to regional iodine deficiency, which
in turn was the result of abundant precipitation in the mountains and alluvial loss of
soluble iodine salts.
1917 M. Seymour in Boston reports on the use of x-rays to treat Graves disease.
1917 thyroxine introduced into commercial distribution in the United States for $350 per
gram.
1920 Marine and Kimball successfully use iodine prophylaxis to prevent ovine and
porcine athyreosis and trout goiter.
1923 P.E. Smith and I.P. Smith show that bovine pituitary extracts could stimulate the
thyroid of a hypopituitary tadpole.
1924 H.S. Plummer at the Mayo Clinic report on the pre-operative use of iodine for the
treatment of Graves disease.
1924 George Hevesy introduces concept of radioactive tracers for the study of metabolic
pathways. He receives Nobel Prize for this work in 1943.
1926 McClendon reports that the iodine concentration in rainwater and in drinking water
decreases as one travels from the Atlantic coast to the Great Lakes.
1927 Harington determines chemical structure of thyroxine. 8

1928 Harington and Barger synthesize thyroxine.
1930 A. Chesney, T. Clawson, and B. Webster show that vegetables can cause
goiter by showing that rabbits fed cabbage develop enlarged thyroids.
1931 L. Loeb and R. Bassett extract and purify TSH from bovine pituitaries.
1932 Naffziger introduces orbital decompression for the treatment of exophthalmos.
1934 New Jones Motor Basal
1935 Roy O. Greep demonstrates that pituitary TSH differs from LH and FSH.
1936 Dr. Saul Hertz first proposes the use of radioactive iodine for the
study of the thyroid.
1936 Marine describes cyanide goiter.
1936 Barker identifies goiter as a complication of thiocyanate treatment of
hypertension.
1937-
1943
Saul Hertz, working in the Massachusetts General Hospital’s Thyroid Unit
under the direction of James Means, and Arthur Roberts, a physicist working in
the laboratory of Robley Evans at MIT, are the first to use radioactive iodine to
study thyroid physiology and treat hyperthyroidism.
1943 Kennedy observes that thiourea is goitrogenic
1946 A. Astwood used thiourea and thiouracil for the medical treatment of Graves
disease.
1947 Cope, Rawson, and McArthur report first use of radioactive iodine to
demonstrate a “hot” thyroid nodule 9

1948 H. Pemberton sends letter to The Lancet describing his eponymous sign for a
substernal goiter.
1948 T. Tempka, J. Aleksandrowicz, M. Till publish the use of fine needle thyroid
biopsy as a diagnostic method
1949 R.G. Hoskins describes negative feedback of thyroid on pituitary, a mechanism
which he termed “servo (feedback) mechanism”.
1949 J. Wolff and I. Chaikoff describe the regulatory effects of inorganic iodine on the
thyroid.
1949 Jones, Kornfeld, McLaughlin and Anderson synthesize methimazole.
1950 J.B. Stanbury describes first case of a genetic abnormality of thyroid hormone
synthesis.
1951 B. Duffy and P. Fitzgerald call attention to thyroid cancer in children following
head and neck irradiation.
1952 Lawson, Rimington, and Searle synthesize carbimazole.
1954 J. Gross and R. Pitt-Rivers isolate and synthesize T3.
1954 J.B. Stanbury, J.B. Wyngaarden, and A. Godley describe use of perchlorate in
treatment of hyperthyroidism.
1954 J.B. Stanbury provides definitive proof of Jod Basedown in course of treating
endemic goiter in Menduza, Argentena.
1956 Goldschmidt, a Norweigen geochemist, identifies Quarternary glaciation as
cause of iodine deficiency in soil.
1956 Roitt and Doniach demonstrate autoantibodies in Hashimoto’s disease. 10

1959 J.B. Hazard, W.A. Hawk, and G. Crile identify medullary thyroid cancer as a
distinct entity.
1960 Adams, Purves, and McKenzie discover LATS in the serum of Graves disease
patients.
1962 Robert Pendleton, a radiation ecologist at the University of Utah, provides first
documentation of I-131 release from atmospheric nuclear testing.
1963
D.H. Copp, A.G.F. Davidson, and B. A. Cheney provide first description of
calcitonin.
Lewis Braverman MD, receives the 1963 Van Meter Award from Theodore
Winship MD. Seated is Virginia Kneeland‐Frantz MD
1965 S. Berson and R. Yalow develop radioimmunoassay procedure, and R. Yalow
receives Nobel Prize for this work in 1977.
1965 E.D. Williams reports 17 cases of cancer of the thyroid and pheochromocytoma.
1966 R.F. Rohner, J.T. Prior, and J.H. Sipple describe the first cases of multiple
endocrine neoplasia type 2.
1969 Neonatal screening for congenital metabolic disease introduced in Switzerland.
1970 A. Schally identifies TRH and receives Noble Prize for this work in 1977.
1970 L. Braverman, S. Ingbar, and K. Sterling discover T4 to T3 conversion.
1971
Hetzel publishes his classic paper on the prenatal neuropathology of iodine
deficiency.
Pharoah POD, Butfied IH, Hetzel BS. Neurological damage to the fetus
resulting from severe iodine deficiency during pregnancy. Lancet 1971; 29: 308-
310. 11

1972 S. Berens, J. Wolff, D. Murphy show that the thyroid concentrates lithium.
1974 S. Refetoff and L. DeGroot identify thyroid hormone resistance.
1977 J Ginsberg and PG Walfish recognize the classical thyrotoxic phase preceding
the hypothyroid phase of postpartum thyroiditis.
1979 T.H. Liao and J. Pierce obtain first ultrapure TSH preparation and then demon
strate that TSH shares a common alpha subunit with LH and FSH.
1998 Recombinant human TSH approved for clinical use in the United States
2002 Thomas Scanlan discovers 3-iodo-thyronine (T1 amine).
12

Thyroid Gland
13

1. The Thyroid Gland
• Consists of two lobes of endocrine tissue joined in middle
by narrow portion of gland
• Follicular cells
– Arranged into hollow spheres
– Forms functional unit called a follicle
– Lumen filled with colloid
• Serves as extracellular storage site for thyroid
hormone
– Produce two iodine-containing hormones derived from
amino acid tyrosine
• Tetraiodothyronine (T4 or thyroxine)
• Tri-iodothyronine (T3)
• C cells
– Secrete peptide hormone calcitonin 14

Fig. 13-1. Structures of thyroxine (T4) and triiodothyronine (T3).
15

• Synthesis, storage, and secretion of thyroid hormone
– Basic ingredients • Tyrosine
– Synthesized in sufficient amounts by body
• Iodine
– Obtained from dietary intake
– Synthesis • All steps occur on thyroglobulin molecules within colloid
• Tyrosine-containing thyroglobulin is exported from follicular cells into colloid by exocytosis
• Thyroid captures iodine from blood and transfers it into colloid by iodine pump
• Within colloid, iodine attaches to tyrosine
• Coupling process occurs between iodinated tyrosine molecules to form thyroid hormones
2. Synthesis and Chemistry
16

17

Fig. 13-4.
Summary scheme
of thyroid
hormone
biosynthesis and
secretion. The
actual oxidative
coupling of
iodinated tyrosine
residues probably
takes place at the
apical surface of
the follicular cell,
rather than in the
lumen.
18

Fig. 13-5. Hypothetical coupling scheme for iodothyronine formation.
19

Fig. 13-6. Structures of some thionamide type antithyroid drugs.
Antithyroid drugs can suppress thyroid
hormone synthesis
- Inhibit iodide transport (iodide trapping)
into the thyroid gland and those that inhibit
iodine incorporation into tyrosine.
- Univalent inhibitors of iodide transport:
thiocyanate and other monovalent anions
(perchlorate, chlorate, periodate, etc.)
- Iodide uptake inhibitors: antagonize iodide
transport through competitive inhibition.
- Other antithyroid compounds:
thionamides, the sulfonamides (e.g., para-
aminobenzoic acid), and the sulfonylureas
(carbutamide, tolbutamide)
20

Fig. 13-7. Synthesis and structure of goitrin.
• Goitrogen: substances that suppress the function of the thyroid gland
by interfering with iodine uptake, which can, as a result, cause an
enlargement of the thyroid, i.e., a goiter.
• Goitrin: a sulfur-containing oxazolidine, a cyclic thiocarbamate, that
reduces the production of thyroid hormones such as thyroxine.
- found in cruciferous vegetables (십자화과 식물) such as cabbage,
brussels sprouts and oil-seed rape, and is formed by the hydrolysis
of a glucosinolate; 2-hydroxy-3-butenyl glucosinolate. The unstable
isothiocyanate (2-hydroxy-3-butenyl isothiocyanate) derived from the
latter glucosinolate spontaneously cyclizes to goitrin, because the
hydroxy group is situated in proximity to the isothiocyanate group
(allowing a five-membered ring to be formed).
21

– Storage
• Thyroid hormones remain in colloid until they are split off and
secreted
• Usually enough thyroid hormone stored to supply body’s needs
for several months
– Secretion
• Follicular cells phagocytize thyroglobulin-laden colloid
• Process frees T3 and T4 to diffuse across plasma membrane and
into blood
• Regulated by negative-feedback system between hypothalamic
TRH, anterior pituitary TSH, and thyroid gland T3 and T4
• Feedback loop maintains thyroid hormones relatively constant
3. Thyroid Hormone or Thyroid Hormone?
23
I I
CH2CH-COOH
NH2
O
I I
HO
3,5,3',5'-Tetraiodothyronine (T4)
most abundant form
Inactivation in
fasting adult
5-deiodinase CH2CH-COOH
NH2
O
I
I I
HO
3,3',5'-Triiodothyronine (reverse) (rT3)
inactive form
5'-deiodinase
Activation in
fed adult
Peripheral
target
tissue
3,5,5'-Triiodothyronine (T3)
most potent form
CH2CH-COOH
NH2
O
I
I I
HO
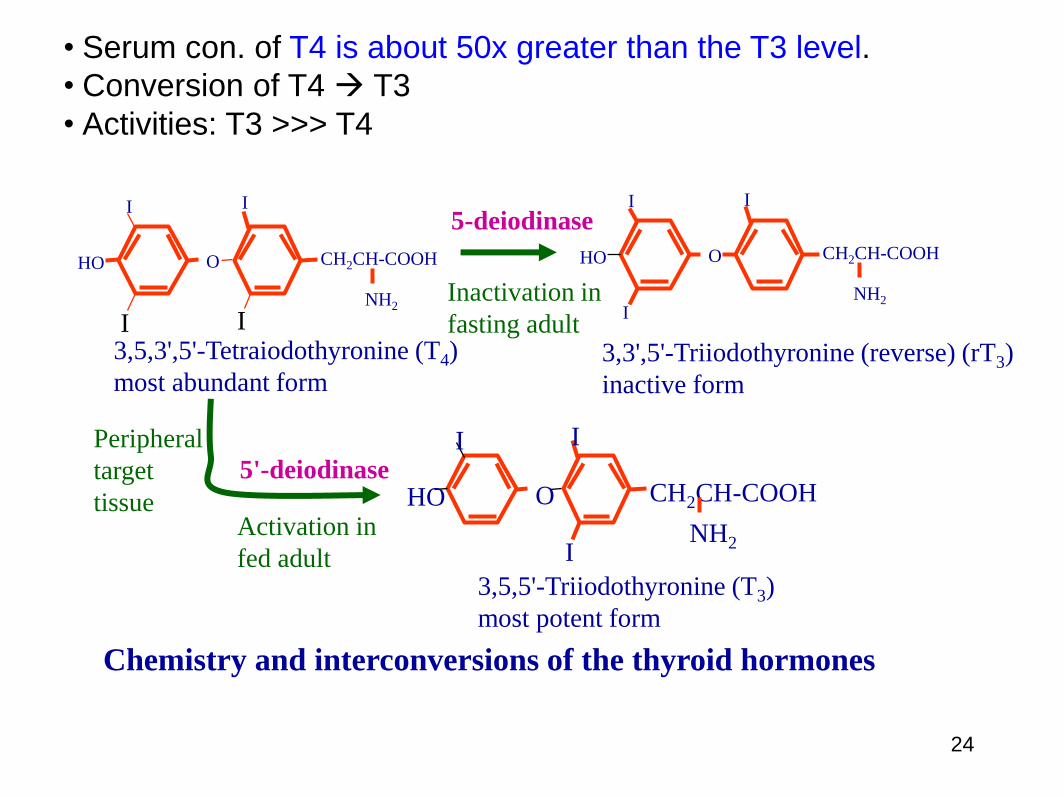
Chemistry and interconversions of the thyroid hormones
• Serum con. of T4 is about 50x greater than the T3 level.
• Conversion of T4 T3
• Activities: T3 >>> T4
24

Fig. 13-8. Structural formulas of iodothyronines found in human plasma.
• Other iodothyronines in biological fluids (Fig. 13-8).
25

4. Control of Thyroid Hormone Secretion
시상하부
뇌하수체
갑상샘 26

• Thyroid hormones: water-insoluble molecules
• Two major thyroxine-binding proteins:
- Transthyretin: 55 kDa; four identical subunits; 127 aa per
subunit
- Thyroxine-binding globulin (TBG): a single polypeptide
chain
- About 70-75% of T4: bound to TBG
- About 20%: bound to transthyretin
- 5-10%: bound to albumin
5. Circulation and Metabolism
27

6. Physiological Roles of Thyroid Gland
• Effects of thyroid hormone: major
– Main determinant of basal metabolic rate
– Influences synthesis and degradation of
carbohydrate, fat, and protein
– Increases target-cell responsiveness to
catecholamines
– Increases heart rate and force of contraction
– Essential for normal growth
– Plays crucial role in normal development of
nervous system
28

29

Fig. 13-10. Model for the action mechanism of thyroid hormone on target tissues. The active
form of thyroid hormone, triiodothyronine (T3), is produced by deiodination of thyroxine (T4) by the
enzymes T45’-deiodinase (5’-D) types I and II. Type I T45’-deiodinase is found predominantly in the
liver and kidneys; its action is responsible for the production of two-thirds of the total T3 in the body.
Type II T35’-deiodinase is responsible for most of the T3 found in the pituitary, the brain, and brown
fat. T3 enters the cell or is produced locally and then transported into the nucleus. Transcriptionally
active forms of thyroid hormone receptors (TR) include monomers, homodimers, and heterodimers
with nuclear protein partners, such as the retinoid X receptor (RXR). The T3–receptor complex
interacts with specific sequences in DNA regulatory regions and modifies gene expression. T3
causes both increases and decreases in gene expression and may also influence the stability of
messenger RNA (mRNA). 9-cis RA denotes 9-cis-retinoic acid, the ligand for RXR.
7. Mechanisms of Action
30

Thyroid Target Cell
(e.g., pituitary/brain, liver, muscle, heart)
T3 receptor
RNA Pol
Nucleus
Induced gene
Response element
New Proteins
(enzymes)
mRNA
Trans-crip- tion
Trans
lation
Circulating T4 - bound to TBG, Transthyretin, or TBPA
G3PDH
UCP
Mitochondria
deiodination T3 T4 5' deiodinase
RXR T3
Na+,K+-
ATPase
Temp. homeostasis:
heat generation from
ATP used by Na, K-
ATPase in liver and
other tissues
O2
O2 consumption
BMR (liver)
Fig. 5. Action of the thyroid hormones
Other effects of T3:
brain development, myelination
Growth (GH transcribed in
somatotrope; induction of anabolic
enzymes)
TSH in thyrotrope
(repressive pituitary effect)
1-adrenergic receptor
RXR T3 RXR T3 RXR T3
31
*UCP, uncoupling protein (Mitochondrial uncoupling
proteins (UCPs) are transporters that are important for
thermogenesis.

NUTRITIONAL CORRELATE – IODINE DEFICIENCY
Plasma T4: Weight of thyroid gland: Thyroid blood flow: Goiter (샘종): reversible hypertrophy/ hyperplasia of thyroid (intakes <10% of the
RDA, Recommended Dietary Allowance, 1일 권장량) Thyromegaly:
• adaptation to lack of iodine for synthesis of thyroid hormone • directly due to TSH, due to low plasma thyroid hormones • excessive TSH enhances number and size of thyroid cells
Cretinism:
• maternal iodine deficiency • mental and physical impairments not reversible • prevented by treating iodine-deficient mother with iodine early in pregnancy
8. Pathophysiology
32

Simple Goiter
단순 갑상샘종
비독성 갑상샘종(단순, 콜로이드 또는 다결젃성 샘종 - 갑상샘의 비대 - 갑상선샘기능은 정상 - 남녀비 = 1:8 - 콜로이드형: 사춘기, 임신 - 다결젃성: 50세 이상 노인 - 무게: 40g~수백g - 자각증상 없음 - 원인: 요오드 이용 부족 및 결함, TSH에 과민 반응 등
33

Gross Pathology of
Goiter(샘종)
•Diffuse colloid goiter
•Nodular goiter
•Long-standing nodular goiter
34

Nontoxic Goiter
•Thyroid gland enlarges
due to excessive
stimulation by TSH
•Treat by supplying
thyroid hormone
•May need to remove
surgically
35
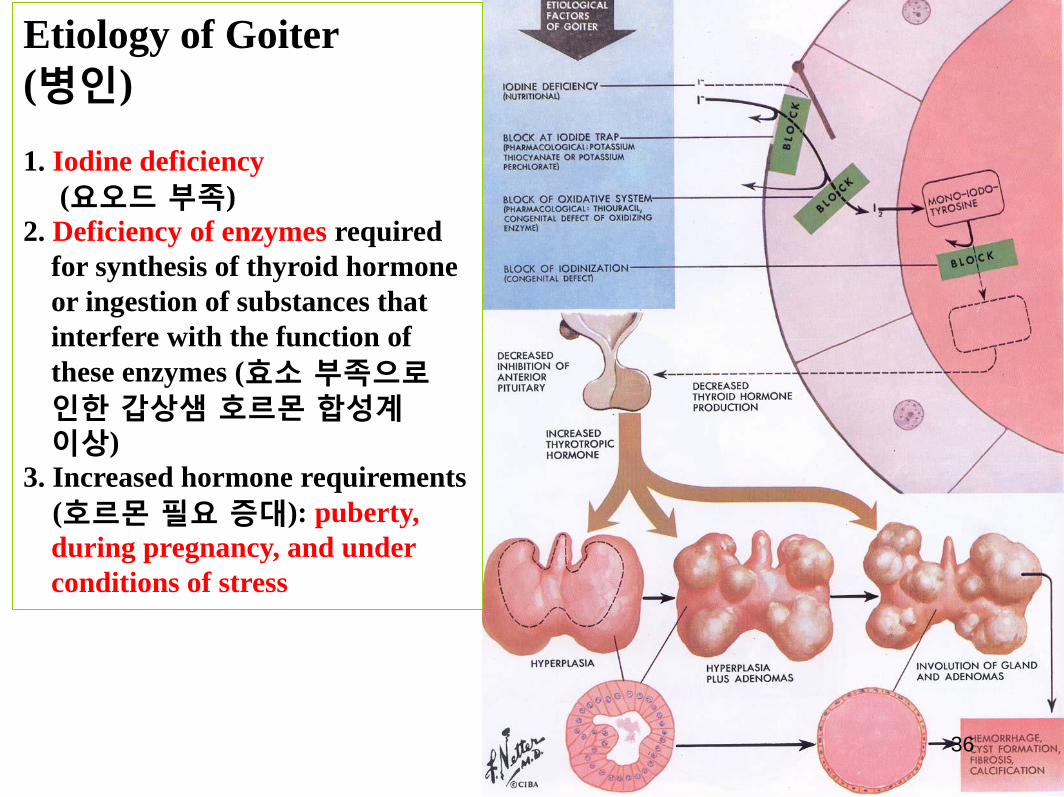
Etiology of Goiter
(병인)
1. Iodine deficiency
(요오드 부족)
2. Deficiency of enzymes required
for synthesis of thyroid hormone
or ingestion of substances that
interfere with the function of
these enzymes (효소 부족으로 인한 갑상샘 호르몬 합성계 이상)
3. Increased hormone requirements
(호르몬 필요 증대): puberty,
during pregnancy, and under
conditions of stress
36

Treatment of Nontoxic Goiter
• Administration of thyroid hormone
37

Fig. 13-12. Various endocrine disorders relating to the
overproduction or underproduction of TSH or to inadequate thyroid-
or peripheral-tissue responses to TSH or thyroid hormones.
38

39
40

Symptom of
Hyperthyroidism
Affected Enzyme, Receptor,
Hormone, Antibody, etc.
Symptom of
Hypothyroidism
Weight
BMR
Mitochondrial Uncoupling
Protein (UCP), Oxidative
Enzymes
Weight
BMR
Heat Intolerance UCP, Na/K-ATPase Cold Intolerance
Heart Rate Cardiac 1-Adrenergic
Receptor
Heart Rate
Irritable Central Sympathetic
-Adrenergic Receptor
Sluggish
Moist Skin Fluid Imbalance Dry Skin
Exophthalmos Thyroid Stimulating
Immunoglobulin (TSI)
------
Goiter TSI or TSH Goiter
------ Myelin Mental Development
------ Growth Hormone Growth
Table 1. Biochemical Basis for the Symptoms of Hyper- and Hypothyroidism.
41

• Hypothyroidism • Causes
– Primary failure of thyroid gland
– Secondary to a deficiency of TRH, TSH, or both
– Inadequate dietary supply of iodine
• Cretinism
– Results from hypothyroidism from birth
• Myxedema
– Term often used for myxedema in adults
• Treatment
– Replacement therapy
– Dietary iodine
42

Causes of Hypothyroidism
• Primary
a. Developmental (thyroid dysgenesis: PAX-8, TTF-2, TSH-receptor mutations)
b. Thyroid hormone resistance syndrome (TRβ mutations)
c. Postablative: surgery, radioiodine therapy, or external radiation
d. Autoimmune hypothyroidism: Hashimoto thyroiditis
e. Iodine deficiency
f. Drugs (lithum, iodides, p-aminosalicylic acid)
g. Congenital biosynthesis defect (dyshormonogenetic goiter)
• Secondary: Pituitary failure
• Tertiary: Hypothalamic failure (rare)
43

Adult: Myxedema 성인 갑상샘 기능 저하증
- 피부: 부풀어 오른 눈꺼풀, 손발 부종, 창백하고 찬 피부
- 신경계: 무기력증, 졳림, 기억상실, 느린 사고, 편집증, 우울증, 점액수종 정신착란
- 심장: 맥박수 및 박출량 감소, 심박출량 감소, 점액수종성 심장
- 위장관: 연동 감소로 인한 변비
- 허스키한 목소리 - 부종 - 월경불순 및 중단 - 쇠약감
44

Adult myxedema:
Clinical manifestations
and etiology
•푸석한 얼굴, 두꺼운 입술, 건조한 피부, 두꺼운 눈꺼풀, 피곤한 표정, 푸석한 머리카락 •Megaloglossia(거대 혀) •Pudgy hands(손 및 팔이 튼 피부, 팔꿈치에 심한 과각화증
45

Adult : Primary Myxedema (Thyroid Origin)
갑상샘 유래 원인 •갑상샘 젃제술 후 •갑상샘암 치료를 위한 방사선 치료 •급성 갑상샘염 후 •하시모토 갑상샘염 후
46

Adult : Secondary Myxedema (Pituitary Origin) 뇌하수체 유래 원인 Seehan 증후군에 의한 TSH 부족
47

Cretinism 선천성 갑상샘 기능 저하증
1.Young cretin with marked
stigmata 2.Elderly cretin - 풍토병, 산발적, 가족력 - 남녀비 = 1:2 - 90%가 갑상샘 발생 장애로 인함 - 어릴 때 나타남 - 무관심, 굼뜸 - 커짂 복부, 배꼽 탈장 - 낮은 체온(35oC) 이하 - 치료하지 않을 경우 난쟁이 및 지능저하 야기
48

– Hyperthyroidism
• Most common cause is Graves’ disease
– Autoimmune disease
– Body erroneously produces thyroid-stimulating
immunoglobulins (TSI)
– Characterized by exopthalmos
• Treatment
– Surgical removal of a portion of the over-
secreting thyroid
– Administration of radioactive iodine
– Use of antithyroid drugs
49

Role of Thyroid-Stimulating Immunoglobulin in Graves’ Disease
50

Hyperthyroidism – Clinical course • Hypermetabolic state
• Activated sympathetic nervous system
• Increase in the basal metabolic rate
• Cardiac manifestations are among the earliest and most consistent features of hyperthyroidism
• Diastolic dysfunction
• Thyrotoxic dilated cardiomyopathy
• Thyroid myopathy
• Ocular change
• Thyroid ophthalmopathy
• Gastrointestinal system: hypermotility, malabsorption, and diarrhea
• Skeletal system: stimulates bone resorption
• Atrophy of skeletal muscle
51

그레이브스병 임상 특징 - 초조, 감정적 변화
- 경련, 나약함 - 체중감소 - 추위에 약하고, 다한증
- 빈맥, 가슴 두근거림
- 무월경 - 안구 돌출 - 습한 피부, 피부병
52

Patients displaying
exophthalmos.
53

Diffuse hyperthyroidism
(Graves’ disease)
54

Diffuse hyperthyroidism (Graves’ disease)
55

Diffuse hyperthyroidism (Graves’ disease)
56

Diffuse hyperthyroidism (Graves’ disease)
57

Thyroid pathology in
Diffuse hyperthyroidism
(Graves’ disease)
58

Treatment of Hyperthyroidism
1. Antithyroid drugs can be administered to block the synthesis of hormone by the hyperactive gland.
2. A large portion of the gland can be removed surgically (thyroidectomy), reducing the source of the hormone.
3. A large dose of radioactive iodine can be administered to be taken up by the thyroid gland. The irradiation destroys part of the gland and reduces its hormone output.
59

Effects of therapy in
diffuse hyperthyroidism
(Graves’ disease)
60

Acute and Subacute
Thyroiditis
•Malaise
•Dysphagia
•Pain radiating to ear
•Thyroid gland visibly enlarged
(more on one side)
•Tender pretracheal lymph nodes
•Thyroid gland tender, palpable
61

Chronic Thyroiditis
(만성 갑상샘염) • 갑상샘에 염증을 동반하면서 다양한 증상을 나타내는 질환
1. 하시모토 갑상샘염 (Hashimoto thyroditis)
2. 아급성 갑상샘염 (Subacute thyroiditis)
3. 리델 갑상샘염 (Riedel thyroiditis)
62

Chronic Thyroiditis (Hashimoto’s Thyroditis)
•Autoantibody
destroys thyroid
tissue
•Often leads to
hypothyroidism
•Cellular infiltration
is the result of an
immunologic
reaction between
antigen and antibody Pathogenesis of Hashimoto thyroiditis. Three proposed
models for mechanism of thyrocyte destruction in
Hashimoto disease. Sensitization of autoreactive CD4+ T
cells to thyroid antigens appears to be the initiating
event for all three mechanisms of thyroid cell death. See
the text for details. 63

Thyroid Tumors • Benign adenoma
• Carcinoma
– Well-differentiated
– Undifferentiated
– Medullary
• Papillary Carcinoma (유두암종)
- 75% to 85% of cases
• Follicular carcinoma(여포암종)
- 10% to 20% of cases
• Medullary carcinoma(속질암종)
- 5% of cases
• Anaplastic carcinoma(미분화성암종)
- <5% of cases
64

65
<성별 10대암 조발생률, 2010년> (2013년 8월 현재)(단위: 명/10만명)
위(80.8)
대장(62.5)
폐(58.7)
간(47.3)
전립샘(31.4)
갑상샘(24.9)
방광(11.0)
췌장(10.0)
담낭 및 기타 담도(10.1)
싞장(10.1)
갑상샘(119.6)
유방(57.1)
대장(40.8)
위(39.8)
폐(24.3)
간(16.5)
자궁경부(15.5)
담낭 및 기타 담도(9.4)
췌[장(8.6)
난소(8.0)

• 목 앞 부위에 혹 • 쉰 목소리 • 경부 림프절 종대 • 연하곤란, 호흡 곤란 • 목부위 압통
Symptoms(증상) Diagnosis(진단) • History & Physical
Examination(조직 및 이화학적
검사)
• 갑상샘 기능 검사 및 호르몬 검사
• Laboratory Evaluation : blood
test(혈액 검사)
• CT/Ultrasonography(초음파)
• Imaging Studies : Radionuclide
Scanning (방사선 스캔 검사)
• Fine Needle Aspiration (FNA)
Biopsy (세침흡인세포검사-결절의
악성도 검사)
66

Scintiscans of thyroid (방사선 스캔 검사)
Left : normal Right : "cold" nodule
• less radioactivity than the surrounding thyroid tissue
(cold nodules -> benign or malignant)
• more radioactivity than the surrounding thyroid tissue
(hot nodules -> usually benign)
67

(A) Benign epithelial cells, colloid,
and occasional macrophages, typical
of a "colloid nodule".
(B) Epithelial cells in a follicular
arrangement suggesting adenoma,
but which could be from a follicular
carcinoma.
(C) Epithelial cells in a papillary
formation from a papillary thyroid
carcinoma. Nuclear grooves are also
apparent.
Fine needle aspiration cytology specimens
68

유두암종 • 가장 흔한 갑상샘암
• 20세~50세 빈발
• 남녀비 = 1:3
• 병인:
-요오드 초과 투여 혹은 섭취
-방사능 노출
-유전적 요인: HLA-DR7
69

유두암종의 임상적 특징 • 유두암종은 대체로 림프관에 침투하여 경부 쪽 국부의 림프절에 퍼짐; 환자의 ¼ 경우
• 암의 말기 때에 쉰 목소리, 연하곤란, 기침, 호흡곤란 등의 증상이 동반됨
• 예후: 매우 좋음; 10년 생존율이 95%
- 국소 재발: 5~20%
- 원위부 재발: 10~20%
- 환자 나이(45세 이상), 갑상선 외 조직 침투, 원위부 전이가 있을 경우 예후가 더욱 나쁨.
- 폐, 뇌 전이 또는 식도나 기도 방해 등으로 사망
70

Follicular Carcinoma
Of the Thyroid
(10% to 20%)
여포성 갑상샘암종 -대부분 40세 이상 -남녀비 = 1:3 -손으로 만져지는 혹 -10년 생졲율=85%
71

수질의 갑상샘암종 (Medullary thyroid carcinoma)
• 갑상샘의 부여포 또는 C 세포에서 시작
• 칼시토닌을 분비하여 혈중 칼슘 농도 낮춤
• 갑상샘암의 5% 이하
• 악성종양증후군(세로토닌)과 쿠싱(Cushing) 증후군(부싞피질자극호르몬) 같은 내분비물 증상을 앓고 있음
• 치료법: 완전갑상샘 절제술
• 5년 생존율: 75%
72

미분화성 갑상샘암종 (Anaplastic thyroid carcinoma)
• 매우 공격적이고 분화되지 않는 갑상샘암
• 급속하게 자라고 치명적
• 주로 여성에 발병(남녀비 = 1:4)
• 보통 60세 이상에서 발병
• 갑상샘암의 10%
• 대부분 장기간 지속되는 갑상샘종의 병력을 가졌음
• 국부조직을 억압하고 파괴시킴
• 연하곤란, 호흡곤란 야기
• 예후는 매우 나쁘고 전이가 잘 발생함
• 5년 생존율: 10% 이하
• Anaplastic thyroid cancer: The 5-year relative survival rate for anaplastic (undifferentiated) carcinomas, all of which are considered stage IV, is around 7% (based on patients diagnosed between 1985 and 1991).
73

Tumors Metastatic To the Thyroid 1. Breast(유방) 2. Lung(폐) 3. Kidney(신장) 4. Rectum and sigmoid colon (직장, S상 결장)
74

stage 5-year relative survival rate(%)
Papillary I 100
II 100
III 94
IV 48
Follicular
I 99
II 99
III 82
IV 47
Medullary
I 98
II 98
III 73
IV 40
Survival rates by Stage of the Thyroid Cancers
75
Anaplastic thyroid cancer: The 5-year relative survival rate for anaplastic
(undifferentiated) carcinomas, all of which are considered stage IV, is around 7% (based
on patients diagnosed between 1985 and 1991).
… Depending on the type and stage of thyroid cancer
• Surgery (수술)
(taking out the cancer)
• Radioactive Iodine (RAI) therapy(방사성 옥소 치료)
(using radioactive iodine to destroy cancer cells)
• External radiation therapy (외인성 방사선 치료)
(using high-dose x-rays or other high-energy rays to kill cancer cells)
• Hormone therapy (호로몬 억제제)
(using hormones to stop cancer cells from growing)
• Chemotherapy(항암제 치료는 아주 특별한 경우에만 사용)
(using drugs to kill cancer cells)
Treatment(치료)
76

Surgery(수술법)
• Lobectomy removes only the side
of the thyroid where the cancer is
found. Lymph nodes in the area
may be taken out (biopsied) to see
if they contain cancer.
• Near-total thyroidectomy removes
all of the thyroid except for a small
part.
• Total thyroidectomy removes the
entire thyroid.
• Lymph node dissection removes
lymph nodes in the neck that
contain cancer.
1. Partial Thyroid Lobectomy
2. Thyroid Lobectomy
3. Thyroid Lobectomy with
isthmusectomy
4. Subtotal Thyroidectomy
5. Total Thyroidectomy
1. 2.
3. 4.
77

갑상샘암 결롞
• 분화된 갑상샘암은 잘 치료됨
• 갑상샘암의 수술은 경험 있는 의사가 할 경우 큰 합병증 없이 잘 치료됨
• 재발된 경우에도 목 근처에서 재발하기 때문에 대부분 재수술로 치료 잘됨
• 비록 젂이된 경우에도 치료 방법이 있음
78