changing trends in gastrointestinal disease in the asia–pacific region
TRANSCRIPT

179
Journal of Digestive Diseases 2007; 8; 179–185 doi: 10.1111/j.1443-9573.2007.00304.x
Blackwell Publishing AsiaMelbourne, AustraliaCDDChinese Journal of Digestive Diseases1443-9611© 2007 The AuthorsJournal compilation © 2007 Chinese Medical Association Shanghai Branch, ChineseXXXReview ArticleGastrointestinal disease in the Asia–PacificKL Goh
Changing trends in gastrointestinal disease in the Asia–Pacific region
KL GOH
Department of Medicine, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia
The new millennium has seen distinct changes in thepattern of gastrointestinal disease in the Asia–Pacificregion. These changes are important as more than halfof the world’s population come from the region andtherefore impact significantly on the global diseaseburden. The highest incidence of gastric cancer (GCA)has been reported from Asia and GCA remains a veryimportant cancer. However time-trend studies haveshown a decrease in GCA incidence in several countriesin Asia. A rise in cardio-esophageal cancers as seen inthe West has not been reported. On the other hand,colorectal cancer has been steadily increasing in Asiawith age-standardized incidence rates of some countriesapproaching that of the West. The pattern of acid-relateddiseases has also changed. Gastroesophageal refluxdisease is a fast emerging disease with an increasingprevalence of reflux esophagitis and reflux symptoms.
The prevalence of peptic ulcer disease has at the sametime declined in step with a decrease in H. pylori infec-tion. Many of the changes taking place mirror theWestern experience of several decades ago. Astuteobservation of the epidemiology of emerging diseasescombined with good scientific work will allow aclearer understanding of the key processes underlyingthese changes. With rapid modernization, lifestylechanges have been blamed for an increase in severaldiseases including gastroesophageal reflux disease,nonalcoholic fatty liver disease and colorectal cancer.A worrying trend has been the increase in obesityamong Asians, which has been associated with anincrease in metabolic diseases and various gastro-intestinal cancers. Conversely, an improvement in livingconditions has been closely linked to the decrease inGCA and H. pylori prevalence.
KEY WORDS: colorectal cancer, gastric cancer, gastroesophageal reflux disease, Helicobacter pylori, peptic ulcerdisease, time trends.
INTRODUCTION
More than half the world’s population or approxi-mately 4 billion people live in Asia. Changes in trendsof disease in Asia would therefore impact significantlyon the global heath burden. Major changes in disease
and health is inevitable in the Asia–Pacific region as aresult of dramatic socio-economic changes in the regionand concomitant lifestyle changes.
For all diseases, an increased prevalence could be dueto better diagnosis as well as a true increase in thefrequency of disease. Observations of a decrease indisease prevalence are interesting and important aswell. The changing epidemiology of a disease oftenprovides valuable insights as to possible pathogenicmechanisms and the changing epidemiology in Asiaallows us an opportunity to make such observations.
The purpose of this review is to study and summarizethe changes that have taken place in the epidemiologyof major gastrointestinal diseases: gastric cancer (GCA)and colorectal cancer (CRC), as well as that of acid-peptic
Correspondence to: KL Goh, Department of Medicine, Faculty of Medicine, University of Malaya, 50603, Kuala Lumpur. Malaysia. Email: [email protected]
This article is a write-up of a State of the Art Lecture presented by Professor KL Goh at the Asian Pacific Digestive Week 2005, held in Seoul, Korea from 25th–28th September 2005
2007 The AuthorJournal compilation 2007 Chinese Medical Association Shanghai Branch, Chinese Society of Gastroenterology and Blackwell Publishing Asia Pty Ltd.

180 KL Goh Journal of Digestive Diseases 2007; 8; 179–185
2007 The AuthorJournal compilation 2007 Chinese Medical Association Shanghai Branch, Chinese Society of Gastroenterology and Blackwell Publishing Asia Pty Ltd.
diseases, including peptic ulcer disease (PUD) andgastroesophageal reflux disease (GERD) based onpublished data in the Asia–Pacific region.
GASTRIC CANCER
Gastric cancer remains one of the most common cancersin the Asia–Pacific region. In 2002, two Asia–Pacificcountries, Korea and Japan, recorded the highest gastriccancer incidence in the world for both men andwomen.1 In absolute numbers, for the same year, closeto 1 million new cases of GCA were diagnosed, morethan half the cases were from East Asia, 41% fromChina and 11% from Japan. However Asia is a diversecontinent and incidence rates vary greatly from coun-try to country as well as between ethnic groups. Agestandardized incidence rates in India, Thailand andthe Philippines are among the lowest in the world andrange from 10 to 15 per 100 000 per year.2 In multiracialSingapore, Chinese have the highest incidence ratescompared to low incidence rates among Malays andIndians.2 Similarly in a case-control study from Malay-sia, Chinese race was identified as a significant inde-pendent predictive factor for GCA.3
Food has been often implicated as cause of the highGCA incidence rates among Chinese, Koreans andJapanese. High salt content of oriental foods and theintake of preserved foods such as soya-bean paste soupand Kim-chi among Japanese and Koreans have beenimplicated as a cause.4–6 On the other hand, Indiansappear to be protected because of the high intake ofcurries and chillies, which may contain gastro-protectivefactors such as curcurmin.7,8 Ultimately, causation ofdisease would depend on the interaction between hostgenetic factors and environmental factors includingdiet and H. pylori infection.
Broadly, ecologic comparison studies in Asian popula-tions have shown a close association between H. pyloriinfection and GCA.9 Some anomalies exist. There is ahigh prevalence of H. pylori among both Chinese andIndians in a multiracial Asian population in Malaysiabut an inordinately low GCA incidence among thelatter has been observed and has been called the‘Indian’ enigma.3 This fact is reiterated by the wellreported high prevalence of H. pylori in the Indianpopulation and the relatively low cancer incidencenoted in Indian cancer registries.10,2
While the burden of GCA remains high in the Asia–Pacific region, age-standardized incidence rates (ASR)have started to show a decline. ASR from cancer regis-tries in Osaka, Japan, Qidong county, China and
Singapore for example, show a steady decline over thepast 20 years (Fig. 1).11 Cancer statistics collected fromthe urban districts of Shanghai by the Shanghai CancerInstitute, showed a marked decline in ASR in menfrom 62 to 35.8 and in women from 23.9 to 17.5 per100 000 population from 1979 to 1999.12,13 This is inkeeping with observed trends noted in Western countrieswhere GCA has been observed to have declined sincethe 1940s (Fig. 1).14
This decline is thought to be due to the decreasedintake of salt and food preservatives following thewidespread use of refrigeration of food in the West.Refrigeration has allowed greater intake of fresh fruitsand vegetables with a higher level of antioxidants.15,16
This has been well shown in a study by Fei and Xiaofrom Shanghai where consumption of fresh fruits andvegetables and availability of home refrigeration wasassociated with a lower incidence of gastric cancer.17
H. pylori has now been identified as a critical factor ingastric carcinogenesis.18 With increasing awareness,diagnosis and treatment of the infection, prevalencerates of H. pylori have now also decreased throughoutthe world.19–21 However the decline in GCA precededthe discovery of H. pylori. Paradoxically, the prevalenceof H. pylori, may in fact have also started to declinebefore its discovery. H. pylori is a marker of socioeco-nomic status and improvement in status with betterpersonal and community hygiene has probably been amore important factor in the decrease in the prevalenceof infection.22
Another important change with regard to GCA hasbeen the change in the topography of GCA in Westernpatients which was first noted in the early 1990s.Cardia cancer has been reported to be the fastest growinggastrointestinal cancer in the West.23 However, such achange has not been noted in Asian countries wheredistally located tumors still predominate (Fig. 2).24,25
Although incidence rates of GCA have declined, greaterlife expectancy and an increase in the elderly popula-tion, as is seen in Japan, would mean that the healthburden in terms of actual numbers of GCA patientswould remain the same or even increase.26
COLORECTAL CANCER
Colorectal cancer has long been considered a Westerndisease. There has however, been clear evidence thatCRC incidence rates have been increasing in Asians.11
In the recent Globocan figures of 2002, ASR rates ofCRC have increased markedly in Japan and among

Journal of Digestive Diseases 2007; 8; 179–185 Gastrointestinal disease in the Asia–Pacific 181
2007 The AuthorJournal compilation 2007 Chinese Medical Association Shanghai Branch, Chinese Society of Gastroenterology and Blackwell Publishing Asia Pty Ltd.
Singapore Chinese and are reported to be among thehighest in the world.2 In several Asian countries, theASR of colon and rectal cancer has now surpassed thatof GCA.2
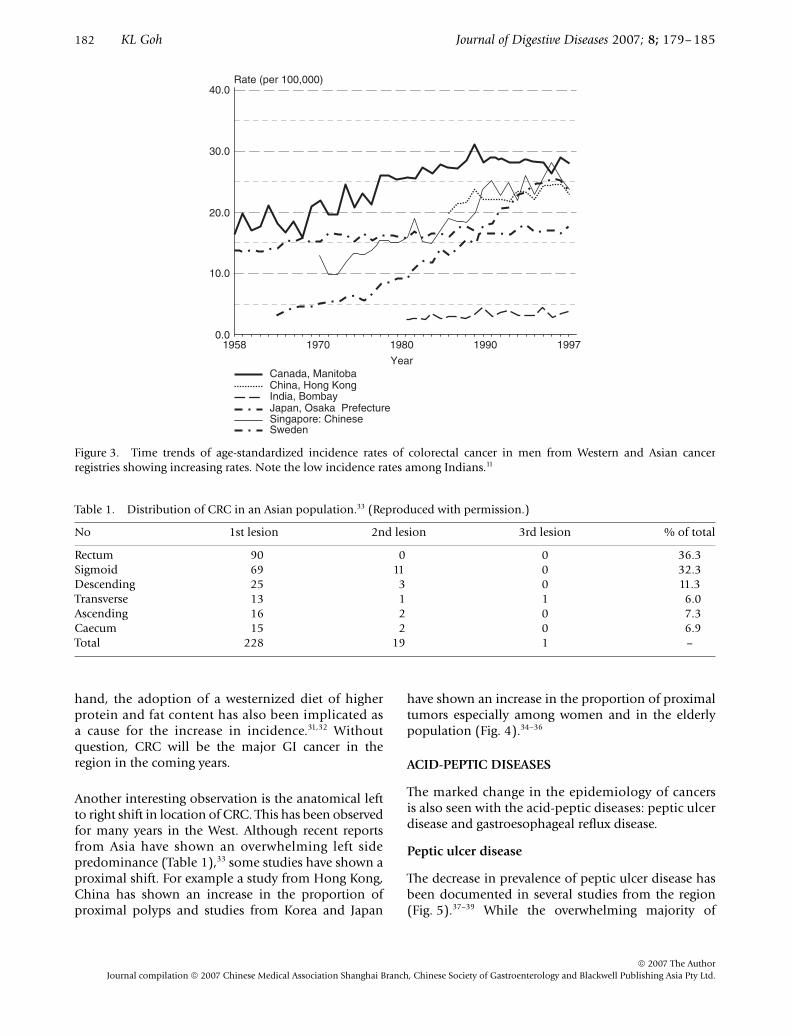
This changing epidemiology follows that of the Westwhere CRC had been steadily over the past 40 to 50years (Fig. 3). The increased incidence of CRC could be
due to better detection and diagnosis of the cancer.With widespread availability of better health care servicesin Asia, flexible colonoscopy has become more readilyavailable. However, the continuing rise in CRC ratespoints to a true increase in CRC.27 The reasons arelikely to be similar to those in the West. Rising afflu-ence with an increase in obesity and a decrease in physicalactivity have been implicated in CRC.28–30 On the other
Figure 1. Time trends age-standardized incidence rates of gastric cancer in men from Western and Asian cancer registriesshowing declining incidence rates. Note the low incidence rates among Indians.11
Figure 2. Comparison of subsite distribution of gastric cancer (men and women) from Western and Asian cancer registries.25
182 KL Goh Journal of Digestive Diseases 2007; 8; 179–185
2007 The AuthorJournal compilation 2007 Chinese Medical Association Shanghai Branch, Chinese Society of Gastroenterology and Blackwell Publishing Asia Pty Ltd.
hand, the adoption of a westernized diet of higherprotein and fat content has also been implicated asa cause for the increase in incidence.31,32 Withoutquestion, CRC will be the major GI cancer in theregion in the coming years.
Another interesting observation is the anatomical leftto right shift in location of CRC. This has been observedfor many years in the West. Although recent reportsfrom Asia have shown an overwhelming left sidepredominance (Table 1),33 some studies have shown aproximal shift. For example a study from Hong Kong,China has shown an increase in the proportion ofproximal polyps and studies from Korea and Japan
have shown an increase in the proportion of proximaltumors especially among women and in the elderlypopulation (Fig. 4).34–36
ACID-PEPTIC DISEASES
The marked change in the epidemiology of cancersis also seen with the acid-peptic diseases: peptic ulcerdisease and gastroesophageal reflux disease.
Peptic ulcer disease
The decrease in prevalence of peptic ulcer disease hasbeen documented in several studies from the region(Fig. 5).37–39 While the overwhelming majority of
Figure 3. Time trends of age-standardized incidence rates of colorectal cancer in men from Western and Asian cancerregistries showing increasing rates. Note the low incidence rates among Indians.11
Table 1. Distribution of CRC in an Asian population.33 (Reproduced with permission.)
No 1st lesion 2nd lesion 3rd lesion % of total
Rectum 90 0 0 36.3Sigmoid 69 11 0 32.3Descending 25 3 0 11.3Transverse 13 1 1 6.0Ascending 16 2 0 7.3Caecum 15 2 0 6.9Total 228 19 1 –

Journal of Digestive Diseases 2007; 8; 179–185 Gastrointestinal disease in the Asia–Pacific 183
2007 The AuthorJournal compilation 2007 Chinese Medical Association Shanghai Branch, Chinese Society of Gastroenterology and Blackwell Publishing Asia Pty Ltd.
patients were diagnosed to have associated H. pyloriinfection, one study from Philippines has noted asteady decline in prevalence of H. pylori-associatedulcers.40 Reports on the prevalence of NSAID useand the increase in NSAID-associated ulcers have alsobeen noted.41
Gastroesophageal reflux disease
Gastroesophageal reflux disease has been considereda rare disease in the East previously. Indeed earlierstudies have shown an inordinately low prevalence ofreflux esophagitis.42 Community-based studies havealso shown a low prevalence of reflux symptoms. Thesituation has changed dramatically. More and betterstudies are now available, which have shown pre-valence of reflux esophagitis approaching 20% and
prevalence of reflux symptoms of 10–15%. More severegrades of esophagitis have also been noted althoughBarrett’s esophagus remains uncommon.43
Helicobacter pylori infection
H. pylori underlies several gastrointestinal disordersincluding GCA and peptic ulcer disease. Reports fromAsia have shown a steady decline of H. pylori over theyears.44–47 Studies from Japan have linked the decreasein H. pylori incidence with an increase in GERD.48
OTHER GASTROINTESTINAL DISEASES
Inflammatory bowel disease (IBD): ulcerative colitisand Crohn’s disease have also been thought to be veryuncommon diseases in Asians. Studies from Japan andChina have, however shown marked increases in prev-alence rates as well as absolute numbers of patientswith IBD.49–52 Data from one study from northernIndia show inordinately high rates of ulcerative colitiscomparable to that seen in the West.53 There is nowenough evidence to show that IBD may be the nextemerging GI disease in the Asia–Pacific region.54
DISCUSSION
The epidemiological changes that have taken placeover a relatively short interval of time point to theinfluence of exogenous factors. Broadly, changes tothat result in a more ‘westernized’ lifestyle, havebeen blamed. Such changes that are relevant to ourdiscussion include dietary changes, improved livingconditions and a decrease in physical activity.
A change in diet to one that is rich in fat and proteinhas been implicated in the rise in incidence of CRC aswell as GERD. This process could be brought aboutdirectly by the change in diet or through associatedproblems such as obesity. Dietary change compoundedby a decrease in the level of physical activity has madeobesity the fastest growing problem in the Asia–Pacificregion.55 An epidemic of obesity-associated diseasessuch as ‘fatty liver’ has already been predicted.56
Paradoxically, dietary change has also meant a changeto a better diet – one that contains less salt and preserv-atives. This has been thought to be the single mostimportant factor in the decline in GCA rates. Animprovement in living conditions and better personaland community hygiene has also resulted in the rapiddecrease in the prevalence in H. pylori and as a conse-quence, a decline in the prevalence of associatedgastroduodenal disease: peptic ulcer and GCA. A decrease
Figure 4. Time trends of the proportion (%) of patients= 70 years of age with proximal tumors.36 (Reproduced withpermission.)
Figure 5. Time trends – proportion of patients withduodenal ulcer, esophagitis and H. pylori infection in anendoscopy-based study.39 (Reproduced with permission.)

184 KL Goh Journal of Digestive Diseases 2007; 8; 179–185
2007 The AuthorJournal compilation 2007 Chinese Medical Association Shanghai Branch, Chinese Society of Gastroenterology and Blackwell Publishing Asia Pty Ltd.
in H. pylori infection has resulted in a healthier stomachwith an increase in acid producing capacity which willcontribute to the increase in GERD.57 An improvementin hygiene has conversely been implicated in theincrease in IBD in Western populations.58 This mayalso be the case in the Asian population where anincrease in prevalence has already been observed.
An important demographic factor to consider is theincrease in the proportion of population that is elderlyin the Asia–Pacific region. Apart from degenerative dis-eases, cancers including gastrointestinal cancers wouldincrease and patterns of cancer will also change. Higherconsumption of non-steroidal anti-inflammatory drugsin the elderly will result in an increase in gastrointestinalulceration and associated complications particularlygastrointestinal bleeding despite the decrease inH. pylori associated ulcers.
Epidemiological change in disease is inevitable withtime. The challenge for everyone is to identify putativefactors and implement modifiable or remedial actionto prevent the full deleterious effects of such changes.
REFERENCES
1 Ferlay J, Bray F, Pisani P, Parkin DM. GLOBOCAN 2002: Cancer Incidence, Mortality and Prevalence Worldwide, Version 2.0. Lyon: IARC Press, 2004.
2 Parkin DM, Whelan SL, Ferlay J, Teppo L, Tomas DB, eds. Cancer Incidence in Five Continents, Vol. VIII. Lyon: IARC Scientific Publication no. 155, 2002.
3 Goh KL, Cheah PL, Noorfaridah M, Parasakthi N. Ethnic differences in gastric cancer in a multiracial Asian popoulation: a case-controlled study. Am J Gastroenterol 2007; 102: 40–5.
4 Hirayama T. Relationship of soybean paste soup intake to gastric cancer risk. Nutr Cancer 1982; 3: 223–33 .
5 You WC, Blot W, Chang YS et al. Diet and high risk of stomach cancer in Shandong. China Cancer Res 1988; 48: 3518–23 .
6 Nan H, Park J, Song Y et al. Kimchi and soybean pastes are risk factors of gastric cancer. World J Gastroenterol 2005; 11: 3175–81.
7 Azuine MA, Kayal JJ, Bhide SV. Protective role of aqueous turmeric extract against mutagenicity of direct-acting carcinogens as well as benzo [alpha] pyrene-induced genotoxicity and carcinogenicity. J Cancer Res Clin Oncol 1992; 118: 447–52.
8 Nagabhushan M, Bhide SV. Curcumin as an inhibitor of cancer. J Am Coll Nutr 1992; 11: 192–8.
9 Forman D, Sitas F, Newell DG et al. Geographic association of Helicobacter pylori antibody prevalence and gastric cancer mortality in rural China. Int J Cancer 1990; 46: 608–11.
10 Graham DY, Adam E, Reddy GT et al. Seroepidemiology of Helicobacter pylori infection in India. Comparison of developing and developed countries. Dig Dis Sci 1991; 36: 1084–8.
11 IARC (International Agency for Research on Cancer). Cancer Mondial. Cited: 1st January 2007. Available from URL: http://www-dep.iarc.fr.
12 Jin F, Zhou SZ, Tao RF et al. Cancer incidence trend in Shanghai 1972–94. Tumor 1999; 19: 255–8.
13 The Epidemiological Department of Shanghai Cancer Institute. The incidence of malignant tumors in Shanghai urban districts in 1999. Tumor 2002; 22: 259.
14 Howson CP, Hiyama T, Wynder EL. The decline in gastric cancer: epidemiology of an unplanned triumph. Epidemiol Rev 1986; 8: 1–27.
15 Coggon D, Barker DJ, Cole RB, Nelson M. Stomach cancer and food storage. J Natl Cancer Inst 1989; 81: 1178–82.
16 La Vecchia C, Negri E, D’Avanzo E, Franceschi S. Electric refrigerator use and gastric cancer risk. Br J Cancer 1990; 62: 136–7.
17 Fei SJ, Xiao SD. Diet and gastric cancer: a case-control study in Shanghai urban districts. Ch J Dig Dis 2006; 7: 83–8.
18 IARC (International Agency for Research on Cancer). Schistosomes, liver flukes, and Helicobacter pylori. In: IARC Monographs Programme on the Evaluation of Carcinogenic Risks to Humans, Vol 61. Lyon: IARC, 1994. Cited: December 2006. Available from URL: http://monographs.iarc.fr
19 Everhart JE. Recent developments in the epidemiology of Helicobacter pylori. Gastroenterol Clin North Am 2000; 29: 559–78.
20 Rehnberg-Laiho L, Rautelin H, Koskela P et al. Decreasing prevalence of helicobacter antibodies in Finland, with reference to the decreasing incidence of gastric cancer. Epidemiol Infect 2001; 126: 37–42.
21 Jacobson K. The changing prevalence of Helicobacter pylori infection in Canadian children: should screening be performed in high-risk children? Can J Gastroenterol 2005; 19: 412–14.
22 Plummer M, Franceschi S, Munoz N. Epidemiology of gastric cancer. IARC Sci Publ 2004; 157: 311–26.
23 Botterweck AA, Schouten LJ, Volovics A, Dorant E, van Den Brandt PA. Trends in incidence of adenocarcinoma of the oesophagus and gastric cardia in ten European countries. Int J Epidemiol 2000; 29: 645–54.
24 Lee JY, Kim HY, Kim KH et al. No Changing Trends in Incidence of Gastric Cardia Cancer in Korea. J Korean Med Sci 2003; 18: 53–7.
25 Inoue M, Tsugane S. Epidemiology of gastric cancer in Japan. Postgrad Med J 2005; 81: 419–24.
26 Tajima K, Kuroishi T, Oshima A, eds. Monograph on Cancer Research no. 51. Cancer Mortality and Morbidity Statistics. Japan and the World. Tokyo: Japanese Cancer Association/Karger, 2004.
27 Sung JJ, Lau JY, Goh KL, Leung WK; Asia Pacific Working Group on Colorectal Cancer. Increasing incidence of colorectal cancer in Asia: implications for screening. Lancet Oncol 2005; 6: 871–6.
28 Le Marchand L, Wilkens LR, Kolonel LN, Hankin JH, Lyu LC. Associations of sedentary lifestyle, obesity, smoking, alcohol use, and diabetes with the risk of colorectal cancer. Cancer Res 1997; 57: 4787–94.
29 Slattery ML, Edwards SL, Boucher KM, Anderson K, Caan BJ. Lifestyle and colon cancer: an assessment of factors associated with risk. Am J Epidemiol 1999; 150: 869–77.
30 Wang YY, Lin SY, Lai WA, Liu PH, Sheu WH. Association between adenomas of rectosigmoid colon and metabolic syndrome features in a Chinese population. J Gastroenterol Hepatol 2005; 20: 1410–15.
31 Whittemore AS, Wu-Williams AH, Lee M et al. Diet, physical activity, and colorectal cancer among Chinese in North America and China. J Natl Cancer Inst 1990; 82: 915–26.
32 Levi F, Pasche C, La Vecchia C, Lucchini F, Franceschi S. Food groups and colorectal cancer risk. Br J Cancer 1999; 79: 1283–7.

Journal of Digestive Diseases 2007; 8; 179–185 Gastrointestinal disease in the Asia–Pacific 185
2007 The AuthorJournal compilation 2007 Chinese Medical Association Shanghai Branch, Chinese Society of Gastroenterology and Blackwell Publishing Asia Pty Ltd.
33 Goh KL, Quek KF, Yeo GTS et al. Colorectal cancer in Asians – A Demographic and Anatomic Survey In Malaysian Patients Undergoing Colonoscopy. Aliment Pharmacol Ther 2005; 22: 859–64.
34 Sung JJY, Leung WK, Suen BY et al. Proximal migration of adenomas in the colon: a survey of 3,126 cases of colorectal adenoma over 10 years. Gut 2004; 53 (Suppl. 36): A30.
35 Kim DJ, Shin MH, Alun YO. Incidence pattern of colorectal cancer in Korea by subsite of origin. J Korean Med Sci 2000; 15: 675–81.
36 Takada H, Ohsawa A, Iwamoto S et al. Changing site distribution of colorectal cancer in Japan. Dis Colon Rectum 2002; 45: 1249–54.
37 Xia HH, Phung N, Altiparmak E, Berry A, Matheson M, Talley NJ. Reduction of peptic ulcer disease and Helicobacter pylori infection but increase of reflux esophagitis in Western Sydney between 1990 and 1998. Dig Dis Sci 2001; 46: 2716–23.
38 Rosaida MS, Goh KL. Opposing time trends in the prevalence of duodenal ulcer and reflux esophagitis in a multiracial Asian population. Gastroenterology 2004; 126: A443 (Abstract).
39 Ho KY, Chan YH, Kang JY. Increasing trend of reflux esophagitis and decreasing trend of Helicobacter pylori infection in patients from a multiethnic Asian country. Am J Gastroenterol 2005; 100: 1923–8.
40 Wong SN, Sollano JD, Chan MM et al. Changing trends in peptic ulcer prevalence in a tertiary care setting in the Philippines: a seven-year study. J Gastroenterol Hepatol 2005; 20: 628–32.
41 Ong TZ, Ho KY. The increasing frequency of non- Helicobacter pylori peptic ulcer disease in an Asian country is related to NSAID use. [Abstract] Gastrointest Endosc 2003: 57: AB153.
42 Goh KL, Chang SC, Fock KM, Ke MY, Park HJ, Lam SK. Gastro-oesophageal reflux disease in Asia. J Gastroenterol Hepatol 2000; 15: 230–8.
43 Goh KL. Changing epidemiology of gastroesophageal reflux disease in the Asia–Pacific region: an overview. J Gastroenterol Hepatol 2004; 19 (Suppl. 3): S22–5.
44 Haruma K, Okamoto S, Kawaguchi H et al. Reduced incidence of Helicobacter pylori infection in young Japanese persons between the 1970s and the 1990s. J Clin Gastroenterol 1997; 25: 583–6.
45 Xia B, Xia HH, Ma CW et al. Trends in the prevalence of peptic ulcer disease and Helicobacter pylori infection in family physician-referred uninvestigated dyspeptic patients in Hong Kong. Aliment Pharmacol Ther 2005; 22: 243–9.
46 Shimatani T, Inoue M, Iwamoto K et al. Prevalence of Helicobacter pylori infection, endoscopic gastric findings and dyspeptic symptoms among a young Japanese population born in the 1970s. J Gastroenterol Hepatol 2005; 20: 1352–7.
47 Chen J, Bu XL, Wang QY, Hu PJ, Chen MH. Decreasing seroprevalence of Helicobacter pylori infection during 1993–2003 in Guangzhou, southern China. Helicobacter 2007; 12: 164–9.
48 Haruma K, Hamada H, Mihara M et al. Negative association between Helicobacter pylori infection and reflux esophagitis in older patients: case-control study in Japan. Helicobacter 2000; 5: 24–9.
49 Yoshida Y, Murata Y. Inflammatory bowel disease in Japan: studies of epidemiology and etiopathogenesis. Med Clin North Am 1990; 74: 67–90.
50 Morita N, Toki S, Hirohashi T et al. Incidence and prevalence of inflammatory bowel disease in Japan: nationwide epidemiological survey during the year. J Gastroenterol 1995 1991; 30: 1–4.
51 Jiang XL, Cui HF. An analysis of 10218 ulcerative colitis cases in China. World J Gastroenterol 2002; 8: 158–61.
52 Hu RW, Ouyang Q, Chen X et al. An analysis of clinical presentation, diagnosis and treatment of inflammatory bowel disease from literature in China. J Gastroenterol Hepatol 2004; 18: A382 (Abstract).
53 Sood A, Midha V, Sood N et al. Incidence and prevalence of ulcerative colitis in Punjab, North India. Gut 2003; 52: 1587–90.
54 Ouyang Q, Tandon R, Goh KL, Ooi CJ, Ogata H, Fiocchi C. The emergence of inflammatory bowel disease in the Asia–Pacific region. Curr Opin Gastroenterol 2005; 21: 408–13.
55 Gu DF, Reynolds K, Wu X et al. for the interASIA collaborative group. Prevalence of the metabolic syndrome and overweight among adults in China. Lancet 2005; 365: 1398–405.
56 Farrell GC. Non-alcoholic steatohepatitis: what is it, and why is it important in the Asia-Pacific region? J Gastroenterol Hepatol 2003; 18: 124–38.
57 Kinoshita Y, Kawanami C, Kishi K, Nakata H, Seino Y, Chiba T. Helicobacter pylori independent chronological change in gastric acid secretion in the Japanese. Gut 1997; 41: 452–8.
58 Gent AE, Hellier MD, Grace RH et al. IBD and domestic hygiene in infancy. Lancet 1994; 343: 766–7.