changing the paradigm: from stafffrom staff-directed ... the paradigm: from stafffrom staff-directed...
TRANSCRIPT
Changing the Paradigm:From Staff-Directed to
Changing the Paradigm:From Staff-Directed toFrom Staff-Directed to Patient-Centered CareFrom Staff-Directed to Patient-Centered Care
Beth Witten, MSW, ACSW, LSCSWMedicare Modernization Program Manager
National Kidney Foundation*****
Resource & Policy Associate
1
Resource & Policy AssociateMedical Education Institute, Inc.
ObjectivesObjectivesObjectivesObjectives
T h lTo help you:Recognize the link between patient-centered care, self-determination and participation in careUnderstand and utilize strategies to enhance patient self-managementp gEvaluate your facility's progress toward patient-centered care
2
patient centered care
Institute of Medicine: Core Needs Institute of Medicine: Core Needs for Healthcare Improvementfor Healthcare Improvement
The system should be:The system should be:Safe – error-freeEffective – evidence-based services providedEffective – evidence-based services provided to those who will benefit vs. those who won’tPatient-centered – personalized, p ,individualizedTimely – avoids delaysEfficient – avoids wasteEquitable – consistent quality without regard t d hi i bl
3
to demographic variables
Physician/Staff-Directed CarePhysician/Staff-Directed CarePhysician/Staff-Directed CarePhysician/Staff-Directed CareTrust me…
I knowI know what’s best
for you
I’ll take care of
Fear & guilt will care of
youg
make you comply
No need to ask
ti
4
questions
What Is Patient-Centered What Is Patient-Centered Care?Care?
Patient-centered care is “health care that establishes a partnership among practitioners, patients, and their families p p(when appropriate) to ensure that decisions respect patients’ needs and p ppreferences, and that patients have the education and support they need to ymake decisions and participate in their own care.”Institute of Medicine Envisioning the National Health Care Quality Report
5
Institute of Medicine, Envisioning the National Health Care Quality Report (Washington, D.C.: National Academy Press, 2001
Patient-Centered Care:Physician, Facility & Staff
Patient-Centered Care:Physician, Facility & StaffPhysician, Facility & Staff
BenefitsPhysician, Facility & Staff
BenefitsParticipation in planning ↑ motivation toParticipation in planning ↑ motivation to follow the plan • Could pay off in future P4P• Could pay off in future P4P
environmentImproved MD-patient communicationImproved MD patient communication may save money• Patient-centered care reduces risk ofPatient centered care reduces risk of
malpractice suits11Forster HP et al. Reducing legal risk by practicing patient-centered medicine. A h I t M d J 10 2002 162(11) 1217 1219)
6
Arch Intern Med Jun 10 2002; 162(11):1217-1219)
Patient-Centered Care:Physician, Facility & Staff
Patient-Centered Care:Physician, Facility & StaffPhysician, Facility & Staff
BenefitsPhysician, Facility & Staff
BenefitsFuture may hold incentives for patientFuture may hold incentives for patient-centered care
N b i d l d• New measures are being developedNew CPM measures satisfaction with care• 25% of patients leave MD due to poor p p
communication2
2Terry K. Telling patients more will save you time. Med Econ Jul 25 1994; 71(14) 40 43 46
7
71(14):40, 43, 46
Patient-Centered Care:P ti t B fit
Patient-Centered Care:P ti t B fitPatient BenefitsPatient Benefits
Better patient o tcomesBetter patient outcomesIncreased self-esteemI d f thImproved sense of worthMore empowered to care for, & about, selfMore attentive & understanding staffFamily & support system are more involved iin care
Mid-Atlantic Renal Coalition, Providing Patient-Centered Care
8
(Module 2)
Patient-Centered Care in the CfC:
Patient-Centered Care in the CfC:CfC:
A Few Patients’ RightsCfC:
A Few Patients’ RightsThe patient has the right to—The patient has the right to(1) Respect, dignity, and recognition of his or her
individuality and personal needs, and sensitivity to his or her psychological needs and ability to copehis or her psychological needs and ability to cope with ESRD; (V452)
(2) Receive all information in a way that he or she can(2) Receive all information in a way that he or she can understand; (V453)
(5) Be informed about and participate if desired in all(5) Be informed about and participate, if desired, in all aspects of his or her care, and be informed of the right to refuse treatment, to discontinue treatment, and to refuse to participate in experimental
9
and to refuse to participate in experimental research; (V456)

A Couple More Patients’ A Couple More Patients’ RightsRights
(6) Be informed about his or her right to execute d di ti d th f ilit ’ liadvance directives, and the facility’s policy
regarding advance directives; (V457)
(7) Be informed about all treatment modalities and settings, including but not limited to, transplantation, home dialysis modalities (home hemodialysis intermittent peritoneal dialysishemodialysis, intermittent peritoneal dialysis, continuous ambulatory peritoneal dialysis, continuous cycling peritoneal dialysis), and in-facility hemodialysis The patient has the right tofacility hemodialysis. The patient has the right to receive resource information for dialysis modalities not offered by the facility, including information about alternative scheduling options for working
10
g p gpatients; (V458)
Patient-Centered Care in the CfC:
Patient-Centered Care in the CfC:CfC:
Patient AssessmentCfC:
Patient Assessment(9) E l ti f th ti t’ biliti(9) Evaluation of the patient’s abilities,
interests, preferences, and goals, i l di th d i d l l fincluding the desired level of participation in the dialysis care
th f d d litprocess; the preferred modality (hemodialysis or peritoneal dialysis),
d tti (f l hand setting, (for example, home dialysis), and the patient’s
t ti f t11
expectations for care outcomes.(V512)
Patient-Centered Care in the CfC:
Patient-Centered Care in the CfC:CfC:
Patient Plan of CareCfC:
Patient Plan of Care(b) Standard: Implementation of the(b) Standard: Implementation of the
patient plan of care.(1) The patient’s plan of care must–( ) p p
(i) Be completed by the interdisciplinary team, including the patient if the patient desires; and(ii) Be signed by the team members including the(ii) Be signed by the team members, including the patient or the patient’s designee; or, if the patient chooses not to sign the plan of care, this choice must be documented on the plan of care, along p gwith the reason the signature was not provided.(V556)
12
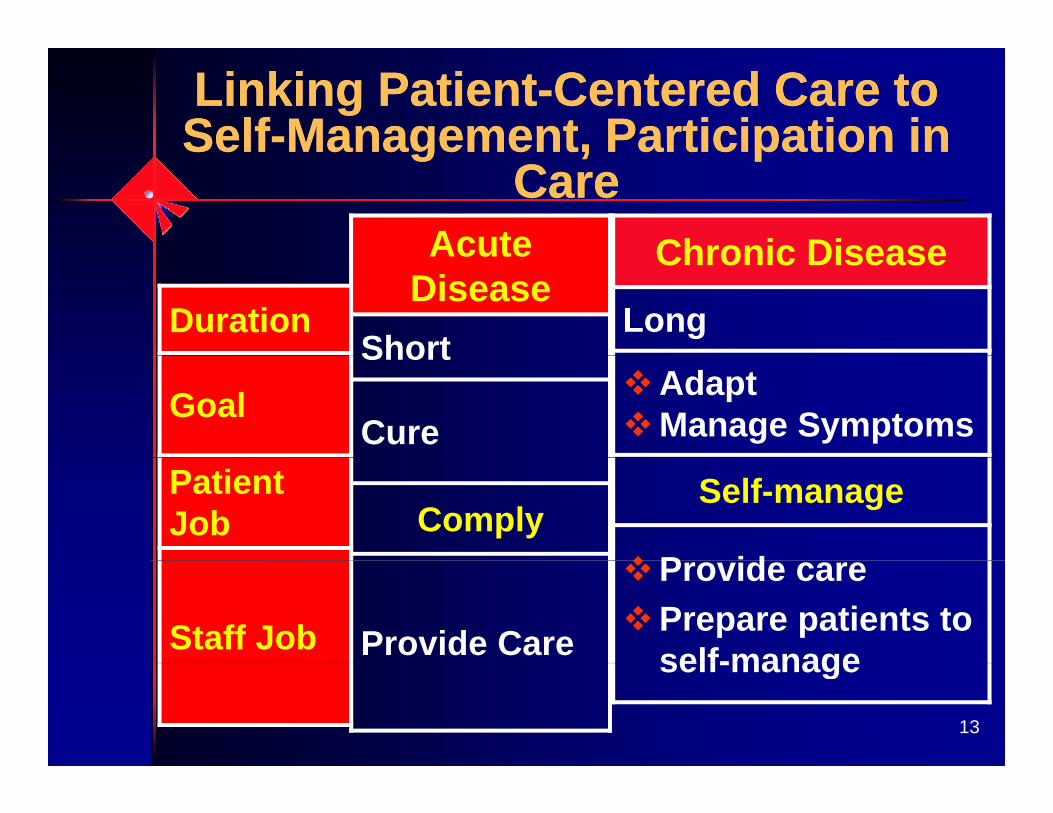
Linking Patient-Centered Care to Self-Management, Participation inLinking Patient-Centered Care to Self-Management, Participation inSelf Management, Participation in
CareSelf Management, Participation in
CareChronic DiseaseAcute Chronic Disease
LongDuration
Acute Disease
ShortAdaptManage SymptomsGoal
Short
CureSelf-manage
P id
Patient Job Comply
Provide carePrepare patients to self-manageStaff Job Provide Care
13
self-manage
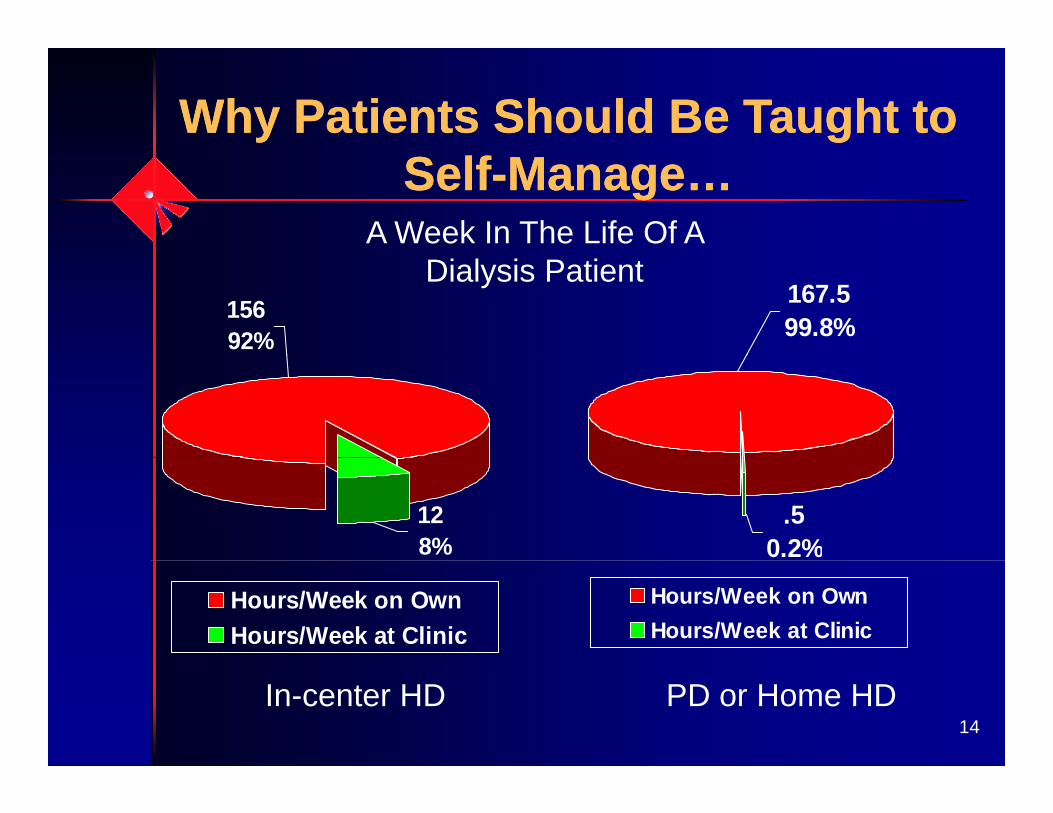
Why Patients Should Be Taught to Why Patients Should Be Taught to Self-Manage…Self-Manage…
A Week In The Life Of A
156 92%
167.5 99.8%
Dialysis Patient
12 8%
.50.2%
Hours/Week on OwnHours/Week at Clinic
Hours/Week on OwnHours/Week at Clinic
14In-center HD PD or Home HD
Promoting Autonomy & Active Promoting Autonomy & Active Participation in CareParticipation in Care
Provide information in a way patients can y punderstand (overcome learning barriers)Offer choicesUse motivational interviewing techniquesUse motivational interviewing techniques• Use reflective listening to help understand
patient’s frame of reference• Be accepting and non-judgmental• Draw out & reinforce motivational statements• Monitor readiness; avoid going beyond whereMonitor readiness; avoid going beyond where
patient is• Affirm patient’s freedom of choice & self-
direction
15
direction
If Self-Management Is Our Goal, Why Are 91 7% of Patients On
If Self-Management Is Our Goal, Why Are 91 7% of Patients OnWhy Are 91.7% of Patients On
Center HD?Why Are 91.7% of Patients On
Center HD?Do nephrologists get enough experience with PD or HHD patients in training? A t ff h t t l i t ti t llAre staff who treat only in-center patients well informed enough about home options?Are all patients provided fact based educationAre all patients provided fact-based education about home options or just “candidates?”Who decides candidacy & what isWho decides candidacy & what is considered?Is modality decision-making more patient-
16
Is modality decision-making more patient-centered than in the mid-1990s?
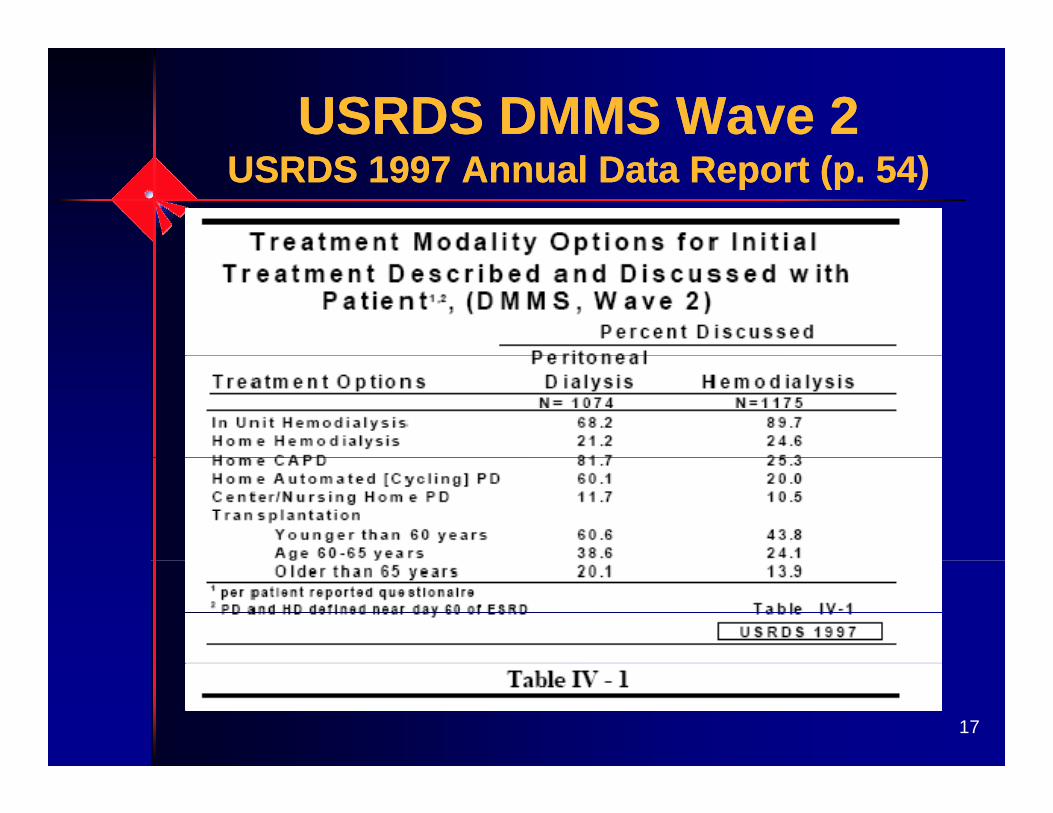
USRDS DMMS Wave 2USRDS DMMS Wave 2USRDS 1997 Annual Data Report (p. 54)USRDS 1997 Annual Data Report (p. 54)
17
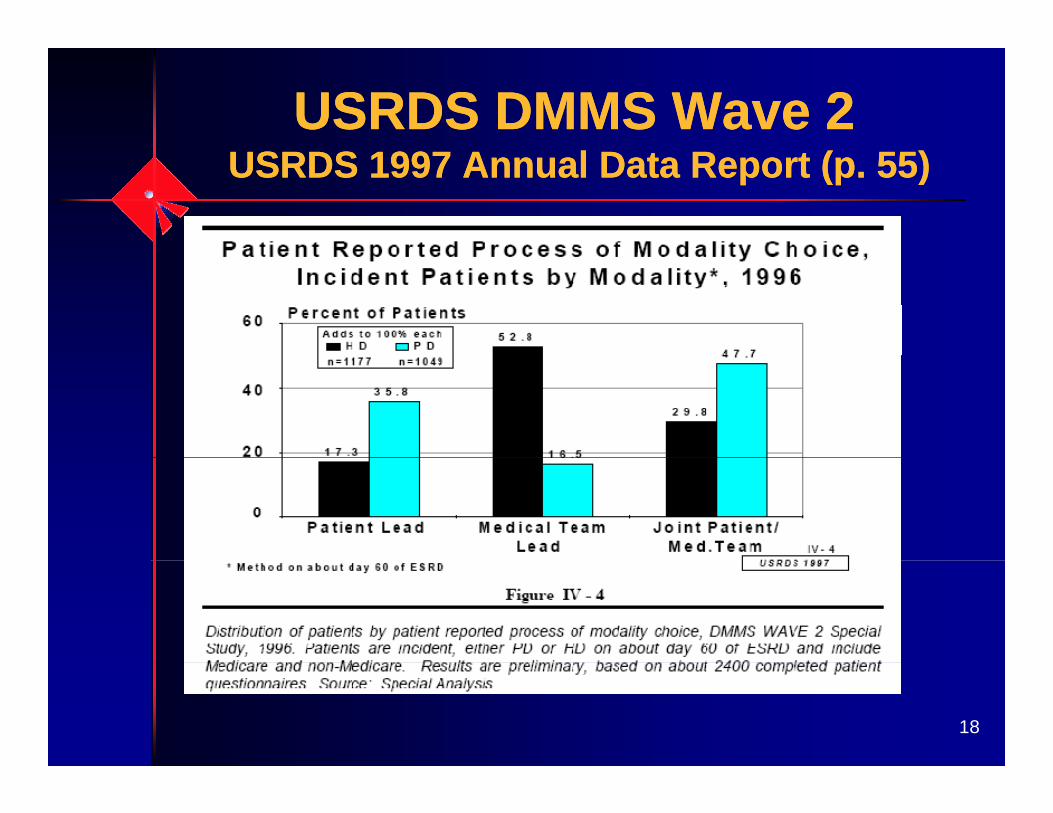
USRDS DMMS Wave 2S S ( )
USRDS DMMS Wave 2S S ( )USRDS 1997 Annual Data Report (p. 55)USRDS 1997 Annual Data Report (p. 55)
18
Systematic Bias: Modality Guidance
Systematic Bias: Modality Guidance
Who is Most Likely to be Offered Home Dialysis?
Who is Most Likely to be Offered Home Dialysis?
A B CA B C
D E FD E F
DMMS Wave 2 (n=4,025), PD more likely in:Younger Whit
EmployedM i d
19
WhiteCollege-educated
MarriedMale
Stack AG. J Amer Soc Nephrol. 2002, 13(5):1279-87
With CKD Education, More With CKD Education, More Patients Choose HomePatients Choose Home
1 88 studies done around the world1-8
All found that 45-60% of patients who received modality education chose home
1. Schreiber M et al. Nephrol News Issues. 2000, 14(12):44-62. Groovaerts T et al. Nephrol Dial Transplant. 2005, 20(9):1842-73. Mehrotra R et al. Kidney Int. 2005, 20(9):1842-74 P i h d SS P it Di l I t 1996 16(1) 69 724. Prichard SS. Perit Dial Int. 1996, 16(1):69-725. Marron B et al. Nephrol Dial Transplant. 2006, 21 Suppl. 2:ii51-56. Wuerth DB et al. Perit Dial Int. 2002, 22(2):184-907. Gomez CG et al. Perit Dial Int. 1999, 19(5):471-78 M BJ t l Kid I t 2005 68(4) 1777 83
20
8. Manns BJ et al. Kidney Int. 2005, 68(4):1777-83
Enhance Competence & Confidence with Communication
Enhance Competence & Confidence with CommunicationConfidence with Communication
& EducationConfidence with Communication
& EducationSit at the patient’s eye levelSit at the patient s eye levelListen carefully & speak slowlyAvoid jargon & use simple explanationsj g p p“A picture is worth a thousand words”Focus on areas patients want & need to kknowProvide user-friendly handoutsUse “teach-back” to assure understandingUse teach back to assure understandingEncourage patients to ask questions (Ask-Me-3)
21
• What is my main problem?• What do I need to do (about the problem)?• Why is it important for me to do this?
Kidney SchoolTMKidney SchoolTMKidney SchoolTMKidney SchoolTM
Available 24/7/365Patient chooses which of 16 topics to studyInteractive• Action plan• Certificate
PDF for those without Internet access
22
accessIdea Guide for Patient Education
Method to Assess Treatment Choices for Home Dialysis
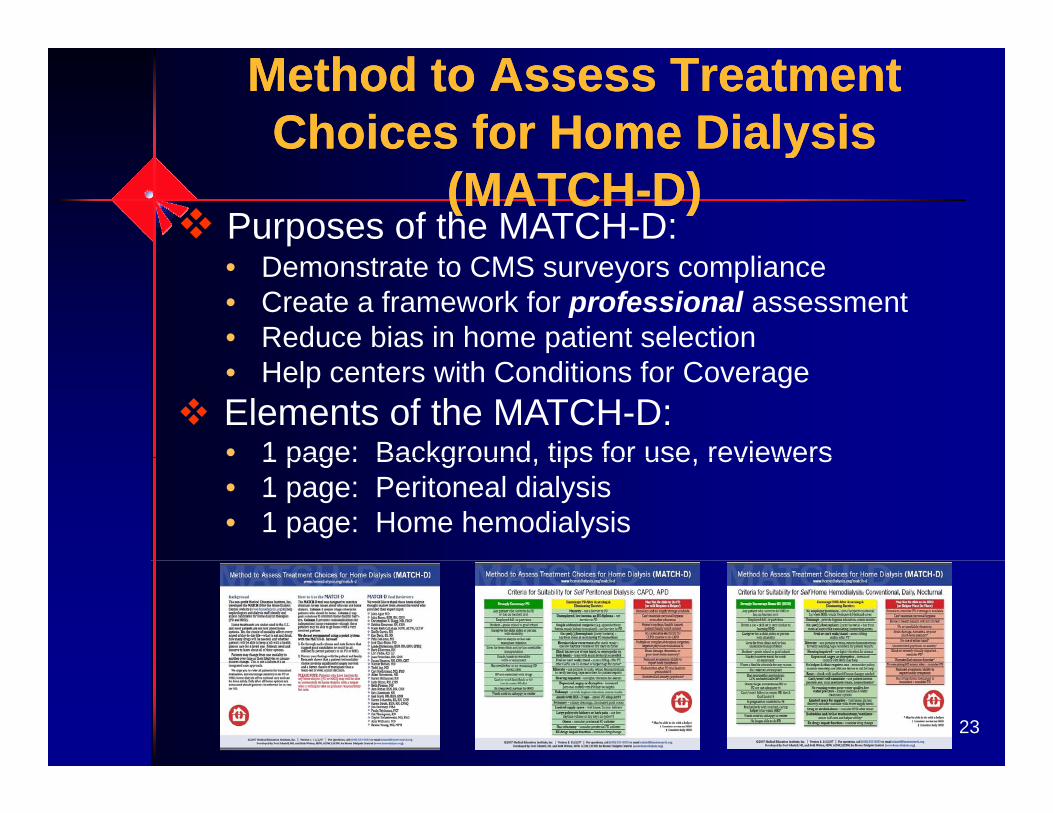
Method to Assess Treatment Choices for Home Dialysis y
(MATCH-D)y
(MATCH-D)Purposes of the MATCH-D: • Demonstrate to CMS surveyors compliance • Create a framework for professional assessment• Reduce bias in home patient selection• Help centers with Conditions for CoverageElements of the MATCH-D:• 1 page: Background tips for use reviewers1 page: Background, tips for use, reviewers• 1 page: Peritoneal dialysis• 1 page: Home hemodialysis
23
Use Mentors to Encourage & S t S lf M t
Use Mentors to Encourage & S t S lf M tSupport Self-ManagementSupport Self-Management
Face toFace-to-Face
Online
Telephone
24
Measuring &Measuring &Measuring & Tracking Progress
Measuring & Tracking Progress
25
ESRD Clinical Performance M (CPM ) P i t 2008
ESRD Clinical Performance M (CPM ) P i t 2008Measures (CPMs) Prior to 2008Measures (CPMs) Prior to 2008
Adequacy of dialysisAdequacy of dialysis (toxins from blood)Access to blood (vascular or PD)Anemia (red cells in (blood)Pressure (of blood)Electrolytes (in blood)
2626
Surveying for Health-Related Quality of Life (HRQOL)
Surveying for Health-Related Quality of Life (HRQOL)Quality of Life (HRQOL)Quality of Life (HRQOL)
New Conditions for Coverage requires use ofNew Conditions for Coverage requires use of standardized physical & mental functioning survey2008: CMS adopted KDQOL-36 for HRQOL CPMKDQOL-36 excludes some patients• <18 (use another age-appropriate survey)• <3 months on dialysis• Cognitively impairment, dementia, psychosis
D ’t k/ d E li h & t l ti27
• Don’t speak/read English & no translation or interpreter available
• Patients who refuse
S l G i SF ItS l G i SF ItSample Generic SF ItemsSample Generic SF ItemsHow much does your health limit you inHow much does your health limit you in climbing several flights of stairs?During the past 4 weeks have youDuring the past 4 weeks, have you accomplished less than you’d like?During the past 4 weeks how much didDuring the past 4 weeks, how much did pain interfere with your normal work?How much of the time during the past 4How much of the time during the past 4 weeks have you felt down or blue?
28
MOS SF S D iMOS SF S D iMOS SF Survey DomainsMOS SF Survey DomainsPhysical Component Mental Component y p
Summary (PCS)
• Physical Functioning
pSummary (MCS)
• Vitality• Physical Functioning• Role-Physical• Bodily Pain
• Vitality• Social Functioning• Role-emotional
• General Health • Mental Health
29
PCS & MCS Scores Predict M bidit & M t lit
PCS & MCS Scores Predict M bidit & M t litMorbidity & MortalityMorbidity & Mortality
1 Point in MCS1 Point in PCS 1 Point in MCSRR mortality 2%RR hosp 1%
1 Point in PCSRR mortality 2% RR hosp. 1%2%RR hosp. 2%
Lowrie EG et al Medical Outcomes Study Short Form 36: A consistent and powerful
30
Lowrie EG et al. Medical Outcomes Study Short Form-36: A consistent and powerful predictor of morbidity and mortality in dialysis patients. Am J Kidney Dis 41(6):1286-1292, 2003.
KDQOL 36 S & S lKDQOL 36 S & S lKDQOL-36: Survey & ScalesKDQOL-36: Survey & ScalesKidney-specific surveyKidney-specific survey6 pages - 15 minutes - 36 items include:
It 1 12 SF 12 (PCS & MCS)• Items 1-12: SF-12 (PCS & MCS)• Items 13-16: Burdens of Kidney Disease
It 17 28 S t /P bl• Items 17-28: Symptoms/Problems• Items 29-36: Effects of Kidney Disease
Download survey Excel spreadsheets:Download survey, Excel spreadsheets: www.gim.med.ucla.edu/kdqol
31
KDQOL-36: Burden of Kidney Disease
KDQOL-36: Burden of Kidney DiseaseBurden of Kidney DiseaseBurden of Kidney Disease
Interference with daily lifeInterference with daily lifeTime to deal with kidney diseaseFrustrationFrustrationFeeling like a burden
32
KDQOL-36: Symptoms/Problems
KDQOL-36: Symptoms/ProblemsSymptoms/ProblemsSymptoms/Problems
General healthGeneral healthActivity limitsAbility to accomplish desired tasksAbility to accomplish desired tasksDepression/anxietyEnergy levelSocial activities
33
KDQOL-36: Effects of Kidney Disease on Daily Life
KDQOL-36: Effects of Kidney Disease on Daily LifeDisease on Daily LifeDisease on Daily Life
Impact of fluid & diet limitsImpact of fluid & diet limitsAbility to work around the house/travelFeeling dependent on medical teamStress or worriesS lifSex lifePersonal appearance
34
Sample KDQOL-36 ItemsSample KDQOL-36 ItemsSample KDQOL-36 ItemsSample KDQOL-36 ItemsToo much of my time is spent dealingToo much of my time is spent dealing with my kidney disease (T/F)I feel like a burden on my family (T/F)I feel like a burden on my family (T/F) During the past 4 weeks, to what extent were you bothered by itchyextent were you bothered by itchy skin? How much does kidney disease botherHow much does kidney disease botheryou in the area of fluid restriction?
35
Using the KDQOL-36Using the KDQOL-36with Patientswith Patients
Ask for the first answer that comes to mindAvoid leading responses if helping patientReview scores with patientsReview scores with patients Brainstorm re: factors in low scoresDevelop a plan of care with your teamDevelop a plan of care with your team (e.g., counseling, PT referral, options education )Resurvey at least annually
36
KDQOL-OnlineKDQOL-OnlineKDQOL-OnlineKDQOL-OnlineUse it to get up to speed:• Read the questions• Take as if a patient• Let patients take itp• Score & print report• Read about subscales• See research-basedSee research based
interpretation & tips• Think teamwork
What it won’t doWhat it won t do• Save patient data• Compare patients’ data
A ti f ti www lifeoptions org/kdqol
37
• Assess satisfaction www.lifeoptions.org/kdqol
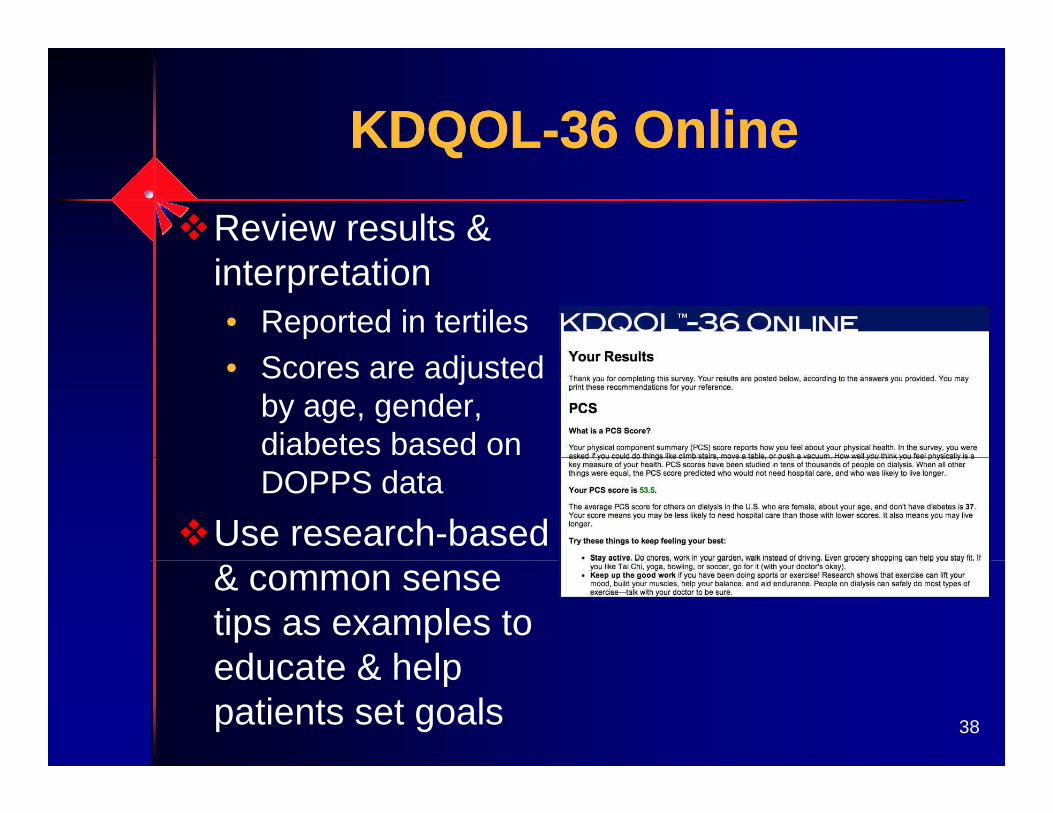
KDQOL-36 OnlineKDQOL-36 OnlineQQ
Review results & interpretation• Reported in tertiles
S dj d• Scores are adjusted by age, gender, diabetes based on DOPPS data
Use research-based & common sense tips as examples to educate & help
38
educate & help patients set goals
Coming in Spring 2009: KDQOL COMPLETE
Coming in Spring 2009: KDQOL COMPLETEKDQOL-COMPLETEKDQOL-COMPLETE
Facility-level KDQOL-y36 scoring toolEnter & track all facility patientspatientsReport by patient or by facilityyArray scores for QAPI purposesR t d t f CPMReport data for CPMSpanish translation of survey & report
39
survey & report
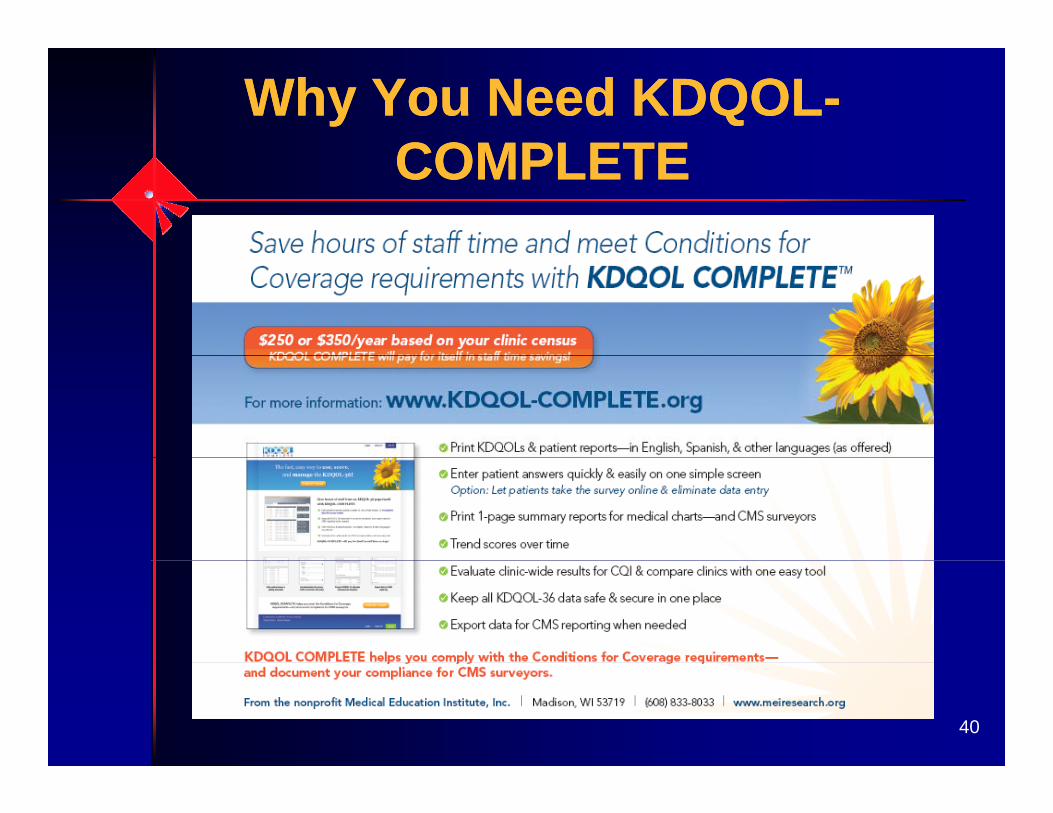
Why You Need KDQOL-COMPLETE
Why You Need KDQOL-COMPLETECOMPLETECOMPLETE
40
ScoringScoringScoring: higher score = better healthTransform linearly to 0-100 range Average items in each scale together g gIf item is skipped:• Numerator = sum of points of allNumerator sum of points of all
answered responses in scale• Denominator = maximum points per
question multiplied by questions answered in scale
• Result = score for that scale41
• Result = score for that scale
Framing the KDQOL-36(F th CNSW Li t )
Framing the KDQOL-36(F th CNSW Li t )(From the CNSW Listserv)(From the CNSW Listserv)
"The governing body that licenses and evaluates g g ydialysis clinics has changed the rules for the betterment of patient care. I am very excited about the changes and look forward to working with you under g g ythese new rules. We are going to be taking a more complete look at patients from a holistic point of view. Each of the staff who work with you will be concerned ywith your mind, body, and spirit. We want you to have the very best quality of life possible. I will be talking to you about some issues or concerns you may have and y y yasking you a lot more questions. Anything you don't want to answer is fine. Shall we begin?"
42
- Mary Calzada, MSW, LCSW, posted 11/25/08
Using the KDQOL in R h bilit ti Pl i
Using the KDQOL in R h bilit ti Pl iRehabilitation PlanningRehabilitation Planning
Review scores & responses with patients soon after survey is completedFocus on areas where things are going wellFocus on areas where scores & responses could improveresponses could improveAsk the patient to choose an area of most concern from below average
43
most concern from below average scores
Use a Patient-Centered, Solution-Oriented Approach to
Use a Patient-Centered, Solution-Oriented Approach toOriented Approach to
InterveningOriented Approach to
Intervening“What would you like to see differentWhat would you like to see different in this area a few months from now?”“How would your day-to-day life beHow would your day-to-day life be different if this were better? What would you be doing?”“What steps are needed to get you to where you want to go?”y g“How might we partner together to reach your goal?”
44
eac you goa

HRQOL is:HRQOL is:HRQOL is:HRQOL is:Patient-perceived physical & mental p p yfunctioningA way to assess chronic disease goalsA way to assess chronic disease goalsA predictor of morbidity & mortality in ESRDESRDEasy to measure using valid, reliable toolsActionable in the dialysis settingActionable in the dialysis setting
45
Surveying for Patient SatisfactionSurveying for Patient SatisfactionNew CfC requires monitoring patientNew CfC requires monitoring patient satisfaction under QAPICMS adopted the CAHPS as the survey for p ypatient satisfaction CPMCAHPS® In-Center Hemodialysis Survey Kit:y y• Survey for adult HD patients• Protocols & sample materials to administer survey • Data analysis programs & guidelines (need SAS;
SAS/STAT)• Reporting measures
46
• Reporting measures
How Are We Doing? Tool to Assess Self-Management
How Are We Doing? Tool to Assess Self-Management g
Supportg
SupportAssessment of Primary Care Resources and ySupports for Chronic Disease Self-Management
D l d f di b t b t lid & li blDeveloped for diabetes, but valid & reliable across chronic illnessesTeam self-assessmentIdentifies optimal performance & gapsPromotes discussion & planning by teamM ti 16 f t 2Measures progress over time - 16 factors, 2 categories
Patient support
47
Organizational supportUseful for QAPI
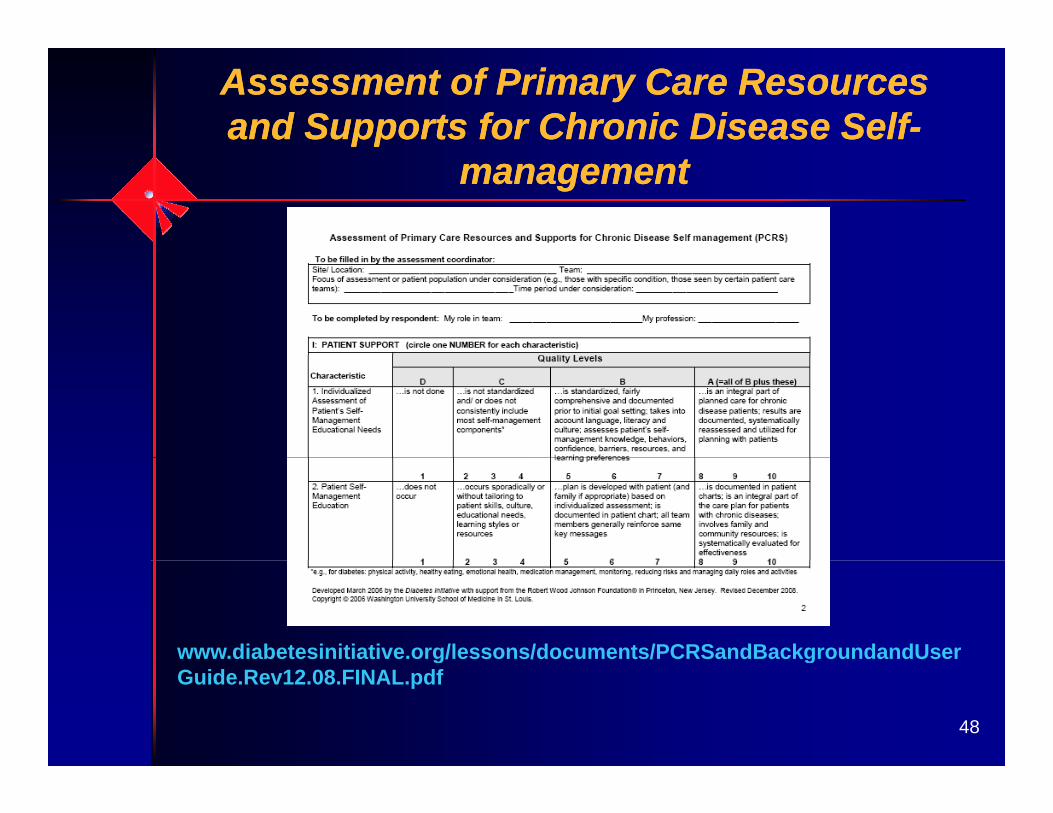
Assessment of Primary Care Resources and Supports for Chronic Disease Self-Assessment of Primary Care Resources and Supports for Chronic Disease Self-
managementmanagement
www.diabetesinitiative.org/lessons/documents/PCRSandBackgroundandUser
48
g gGuide.Rev12.08.FINAL.pdf
ConclusionConclusionConclusionConclusion
P ti t t d ffPatient-centered care offers many benefits to facilities, physicians, staff &
ti tpatientsSelf-management should be a goal for all willing patients Staff can use strategies to promote self-g pmanagement & improve functioningTracking progress toward goals is
49
Tracking progress toward goals is neededTools exist to measure progress

50