chagas disease - university of colorado · pdf fileclinical course of chagas disease •...
TRANSCRIPT
UNIVERSITY OF COLORADO | COLORADO STATE UNIVERSITY | UNIVERSITY OF NORTHERN COLORADO
Chagas Disease
Edwin J. Asturias | Senior Investigator Colorado School of Public Health
Department of Pediatrics Children’s Hospital Colorado
The burden of Chagas Disease • One of the most lethal endemic infections in the
Western Hemisphere (Latin America) • Earliest report of T. cruzi infection in mummies
from Chinchorro, Chile from ~ 9,000 years ago • Considered incurable • Kills people in rural areas in the age range of 30-
50 years • 8 million infected people (WHO)

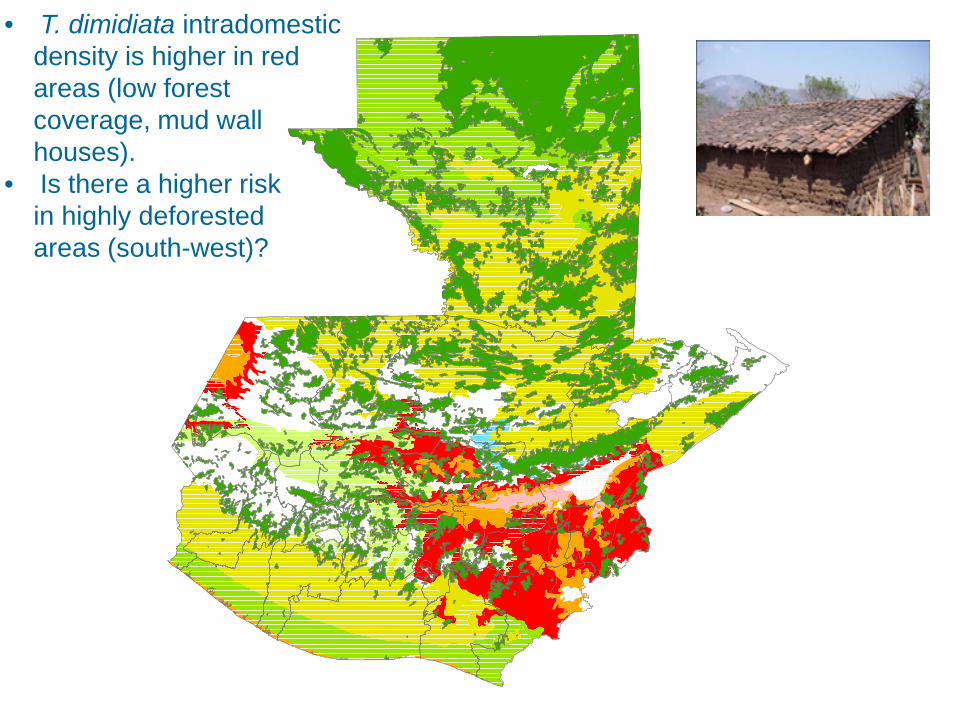
• T. dimidiata intradomestic density is higher in red areas (low forest coverage, mud wall houses). • Is there a higher risk in highly deforested areas (south-west)?
1:250,000
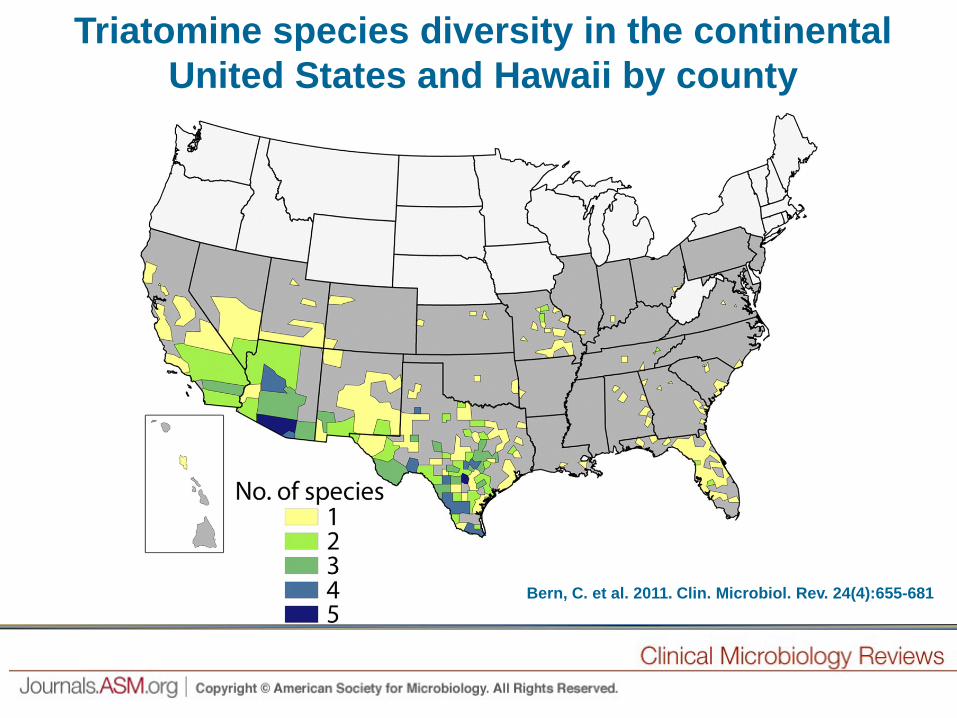
Bern, C. et al. 2011. Clin. Microbiol. Rev. 24(4):655-681
Triatomine species diversity in the continental United States and Hawaii by county

Chagas vector • Discovered by Carlos
Chagas at 28 yrs of age (Oswaldo Cruz young researcher)
• Outbreaks in Minas Gerais, Brazil
• Kissing bug – Triatomine insect
• Named the protozoan Tripanosoma cruzi
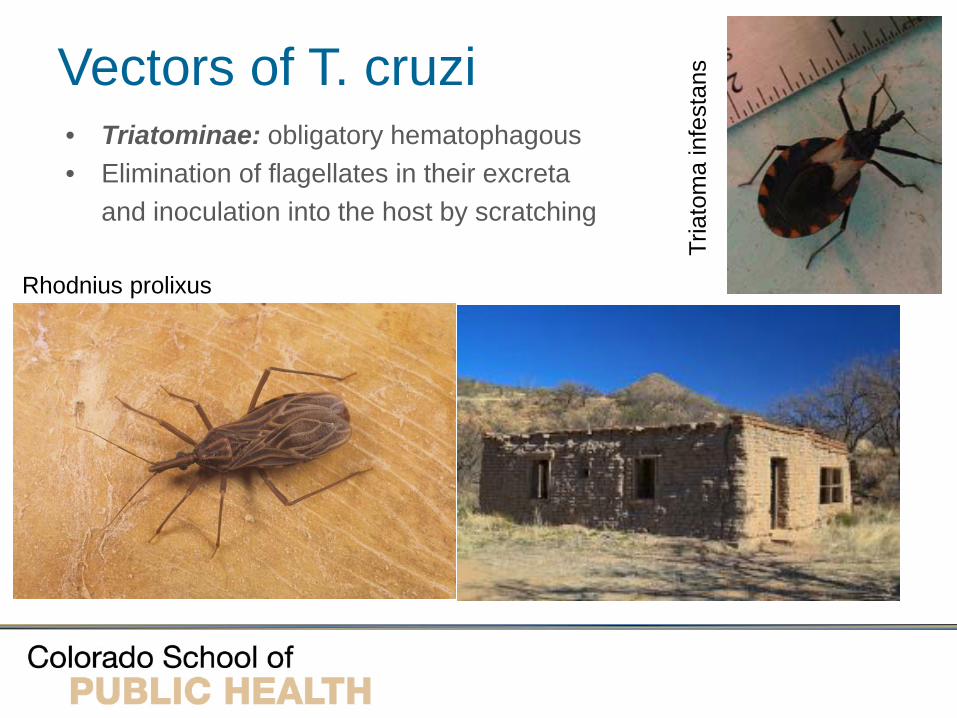
Vectors of T. cruzi
Rhodnius prolixus
Tria
tom
a in
fest
ans
• Triatominae: obligatory hematophagous • Elimination of flagellates in their excreta
and inoculation into the host by scratching

Tripanosoma cruzi
• Trypanosomatidae protozoa: genera Trypanosoma and Leishmania
• Isolated from > 150 species of wild and domestic mammals
• Long term parasitemia – zoonotic reservoir • Humans are accidental hosts after disruption of
natural habitat of Rhodnius prolixus and Triatoma infestans
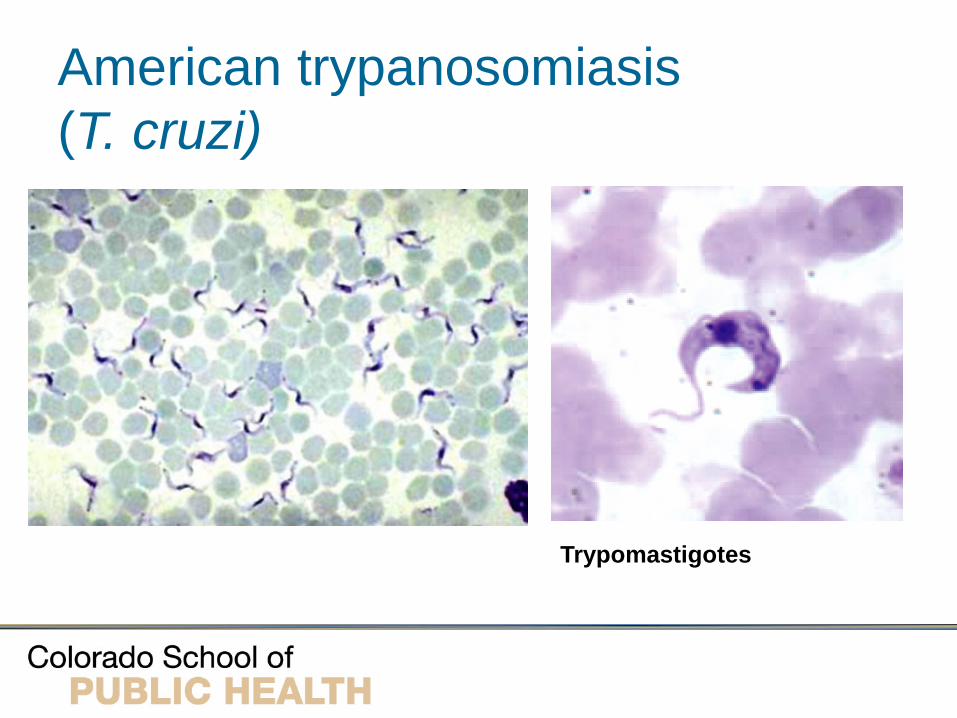
American trypanosomiasis (T. cruzi)
Trypomastigotes

Transmission of T. cruzi • Vector-borne • Oral: food
– More severe: 75% of 103 infected individuals in the Caracas outbreak were symptomatic, 59% had ECG abnormalities, 20% hospitalized, and one death from acute myocarditis
• Transfusion and organ transplant • Congenital
– Trans placental transmission in 1-10% of infected mothers (acute or intermediate
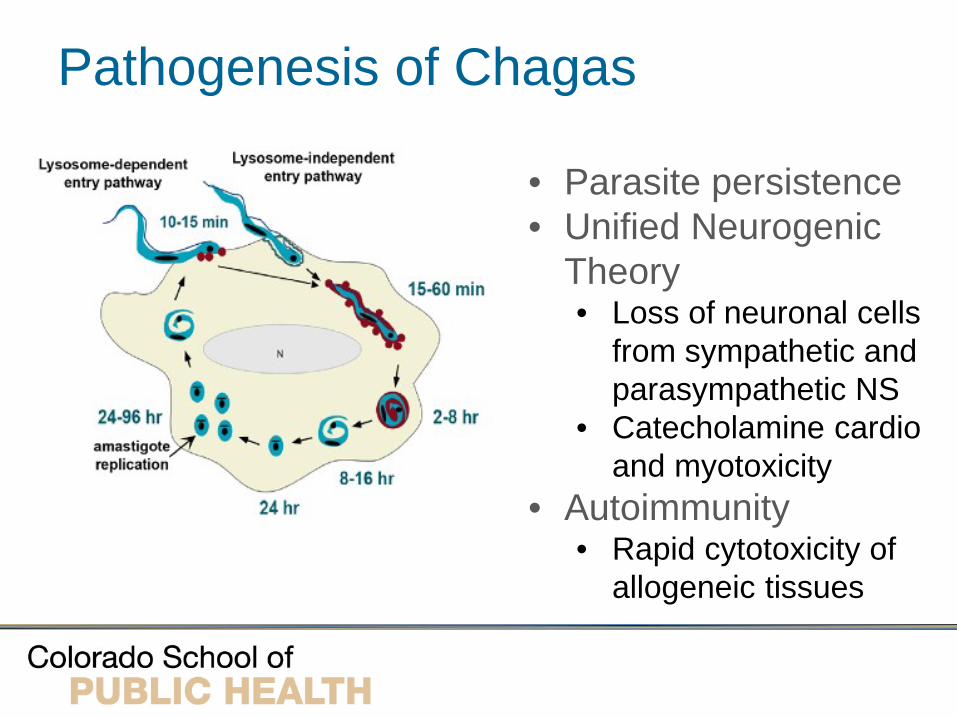
Pathogenesis of Chagas
• Parasite persistence • Unified Neurogenic
Theory • Loss of neuronal cells
from sympathetic and parasympathetic NS
• Catecholamine cardio and myotoxicity
• Autoimmunity • Rapid cytotoxicity of
allogeneic tissues
Pathology of Chagas
• Chagoma – acute inflammatory lesion in muscle and subcutaneous tissues
• Trypomastigotes can be found in the blood after rupture of host cells
• Myocarditis • Megaintestinal disease: megacolon &
megaesophagous (muscle hypertrophy and parasympathetic denervation)
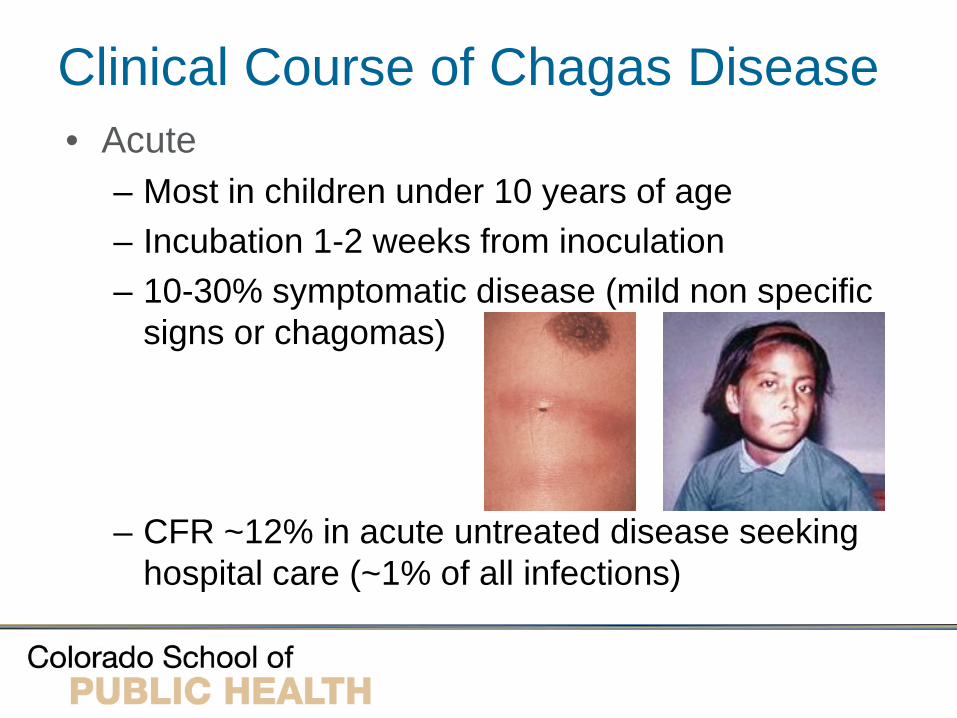
Clinical Course of Chagas Disease • Acute
– Most in children under 10 years of age – Incubation 1-2 weeks from inoculation – 10-30% symptomatic disease (mild non specific
signs or chagomas)
– CFR ~12% in acute untreated disease seeking hospital care (~1% of all infections)

Romaña sign (<5% cases)
Oculo-glandular disease Conjunctiva is the portal of entry Painless edema of palpebrae and periocular tissues Fever, edema, anorexia and edema of face and legs

Acute complications of Chagas
• Hepatosplenomegaly • Meningoenchephalitis (poor prognosis) • Severe myocarditis • Congestive heart failure
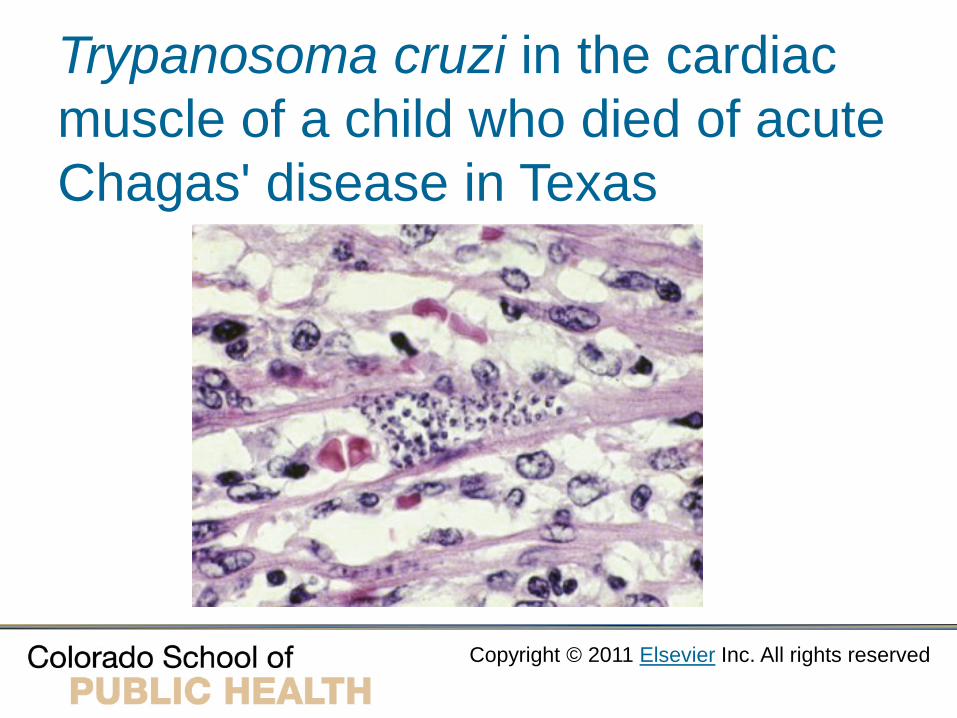
Trypanosoma cruzi in the cardiac muscle of a child who died of acute Chagas' disease in Texas
Copyright © 2011 Elsevier Inc. All rights reserved

Clinical Course of Chagas Disease • Chronic
– Develops in 1/3 of intermediate infections ~ 25 + 7 years after acute infection
– Heart is the most common organ involved (95%) • Rhythm disturbances (dizziness and syncope) • Congestive right sided heart failure
– Intestinal disease (5%) • Dysphagia, chest pain, cough, regurgitation • Recurrent aspiration pneumonitis • Chronic constipation and abdominal pain

Chronic Chagas: Intestinal disease
Megacolon Megaesophagous
Copyright: Palmer and Reeder http://www.isradiology.org/tropical_deseases
Diagnosis of Chagas • History of exposure (residence or transfusion) • Acute Chagas
– Detection of parasite in wet preparation – Anti-T. cruzi IgM not useful – Other sterile fluids and biopsy – PCR: sensitivity of 45-100% (most ~ 90%)
• Chronic Chagas – IgG serology (ELISA, IH, IF) – false positives + – USA: Chagas Hemagen & Ortho T. cruzi

Treatment of Chagas • Nifurtimox (Lampit, Bayer 2502, Leverkusen, Germany)
• Parasitologic cure in 50-70% cases • Reduces duration, severity and mortality • Adults 8-10 mg/kg, children 15-20 mg/kg/d for 90-
120 days - CDC Drug Service (404-639-3670). • Benznidazole (Rochagan, Roche 7-1051, São Paulo, Brazil)
• Nitroimidazole – second line agent • Cure rates ~ 50% • ADR: neuropathy, rash, granulocytopenia • Dose: 5 mg/kg/day for 60 days

Treatment of chronic Chagas • Cardiac
• Symptomatic • Heart transplantation • Nifurtimox prophylactic therapy appears necessary
• Intestinal • Megaesophagous – treat as achalasia • Dilation and esophagocardiomyectomy • High fiber diet and laxatives for colonic disease • Beware of volvulus (surgical decompression)
Prevention of Chagas Disease
• Population screening for early detection and prevention of congenital transmission
• Screening of blood transfusions • Avoid sleeping in dilapidated dwellings • Use insect repellent and bed nets to reduce
exposure to vectors • Vector elimination programs