cervical lymphadenitis in the pediatric age group
TRANSCRIPT

Cervical Lymphadenitis in the Pediatric Age Group
by
SAHAR AWADA, MDPediatric Resident
Lebanese University Medical School

Case Presentation• 1y 2m old boy previously healthy presenting for Right
Neck mass• 4 days ptp, pt started to develop HGF with no other sx • In the next day, HGF continued and the mother noticed a
right neck swelling with edema and erythema • 2 days ptp, mass increased progressively in size, the
parents seeked medical advice and the pt was started on antibiotic(Amoclan)

Case Presentation
• Despite antibiotic therapy, pt continued to be febrile with no decrease in mass size
• On the day of presentation, U/S neck was done in another hospital and showed:
A right submandibular cystic mass of 2.5 cm in diameter resembeling an abscess collection just next to a lymph node of 1 cm in diameter
Case Presentation
• No chills, night sweat, rinorrhea , cough , dyspnea, drooling, dysphagia or any other GI Sx, no change in voice quality, arthralgia, weight loss , fatigue
• No hx of trauma, insect bite, ingestion of unpasteurized animal milk, undercooked meat or new drug intake
• No hx of Dental problems or mouth sores• No hx of animal exposure or recent travel

Case Presentation
• PMH: ftb, nvd, no ICN admission, no hx of recurrent infection
• PSH: neg• PFH: simultaneous acute viral illness(sister)• Diet: regular for age• Home med: Amoclan, Profinal, Panadol• Vaccination: uptodate until the age of 1 yr( 1st
MMR dose not yet received)

Physical exam
• Pt looked ill, NAD, febrile(39.2) • Anicteric sclera, well injected conjunctiva,no mouth sore
or apthous lesions, nrl tonsills • Ears: nrl • Right submandibular mass, hard, non mobile, tender,
warm and erythemateous, measuring 3x3 cm• Heart: rr, nrl s1s2• Lungs: GBAE, no adventitious sounds• Abdomen : non distended, +BS, non tender, no HSM• Normal genitaliae, no palpable axillary or inguinal LN

Lab tests
• Cbcd– WBC 24000– Neutro 70%– Lympho 20%– Hb 11– Hct 34– MCV 80– Plt 518
• Electrolytes nrl• CRP 22

Imaging
• CXR nrl
• CT neck with contrast:– Right submandibular abscess measuring 3.4cm in
diameter next to a small centimetric LN with several small bilateral LN

Pediatric Neck Masses

Classification
• Congenital• Acquired
– Inflammatory• Infectious • Non infectious
– Neoplastic • Benign • Malignant

Classification
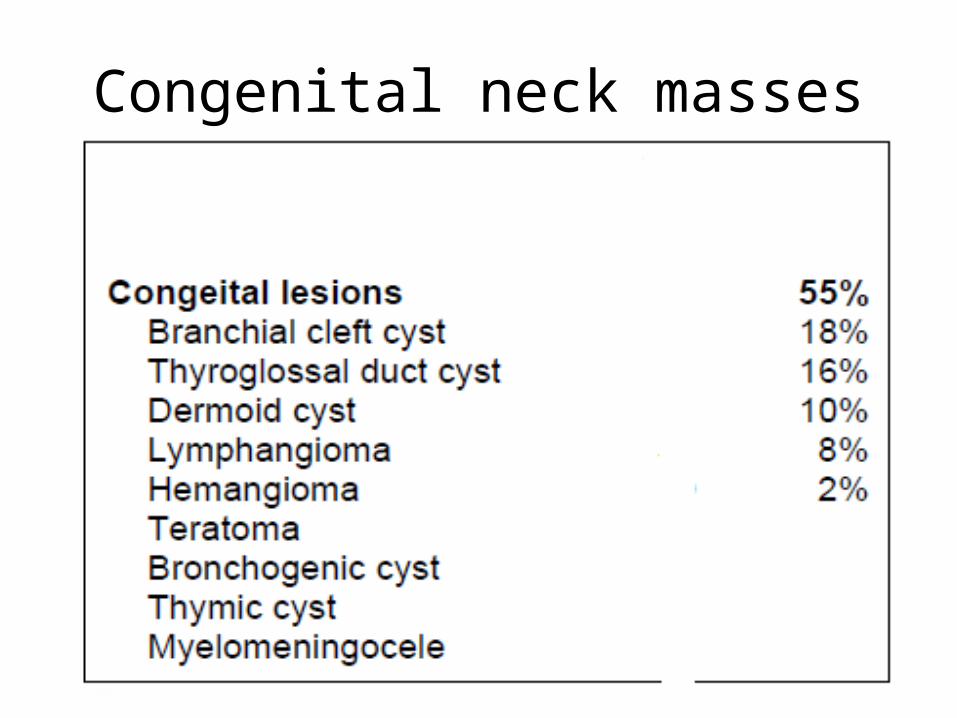
Congenital neck masses
Inflamatory neck masses
• Infectious– Reactive viral lymphadenopathy – Bacterial lymphadenopathy – Parasitic lymphadenopathy
• Non infectious– Connective tissue disorder– Sarcoidosis– Kawasaki disease
Neoplastic neck masses
• Metastatic head and neck carcinomas• Thyroid mass• Salivary gland neoplasms• Schwanoma • Lymphoma • Lipoma and benign skin cysts

Initial evaluation(History)• Age(BIRTH=CONGENITAL)• Onset• Rapidity of growth(rapid enlargement=inflammatory)• Fluctuation in size• Pain• Infection• Trauma• Skin lesion(HS, staph, cat scratch disease) • Associated symptoms (weight loss, fever, arthralgias, sore throat)• Dental problems(anaerobes)• mouth sores(HSV, Enterovirus herpangina)

Initial evaluation(History)• Travel• Ingestion of unpasteurized animal
milk(brucellosis, mycobacterium bovis)• Animal exposures(cat scratch disease,
toxoplasmosis [cats], brucellosis [especially goats], tularemia [especially rabbits])
• Immunization status(diphtheria, measles, mumps)
• Medications (phenytoin, carbamazepine)

Initial evaluation(physical exam)
• Size• Multiplicity• Laterality• Consistency(firm, rubbery, matted)• Color• Mobility(fixed or mobile)• Tenderness• Fluctuation
Initial evaluation(physical exam)
• "Reactive" LN are usually discrete, mobile, rubbery, and minimally tender
• Infected LN are usually isolated, asymmetric, tender, warm, and erythematous; they may be fluctuant; less mobile and discrete than reactive LN
• Malignant LN often are hard, nontender, and fixed to the underlying structures
Initial evaluation(physical exam)
• Oral cavity: search for evidence of periodontal disease, herpangina, HSV gingivostomatitis, or pharyngitis
• Eyes : conjunctival injection may indicate Parinaud oculoglandular syndrome (associated with cat scratch disease) or Kawasaki disease
• Skin : a generalized rash may suggest a viral illness, whereas a localized skin lesion may indicate a more specific etiology(cat scratch disease, HSV, etc.)
• Less common infections in which a papular or pustular lesion is suggestive of an inoculation site
Initial evaluation(physical exam)Location location location
Midline • Thyroglossal cyst
• Submental
lymphadenopathy• Dermoid and
epidermoid cysts• Teratoma• Cervical cleft
Lateral• Branchial cleft anomaly• Lymphatic/vascular
malformation• Lymphadenopathy• Thyroid nodule• Thymic cyst• Laryngocele• Sialadenitis• Soft tissue tumor

Initial evaluation(lab tests)
• Cbcd with differential• Electrolytes: high ca level ->sarcoidosis• Serology testing for EBV, CMV, toxo, syphilis, cat
scratch disease• Thyroid function test• PPD• Urinary collection for VMA (vanillylmandelic acid)
->neuroblastoma

Initial evaluation(imaging)
• CXR to R/O malignancy, TB, Sarcoidosis • Lateral neck Xray essential in evaluation of
nasopharynx, cervical spine and retro-pharyngeal region
• U/S to differentiate cystic structure from solid mass and to evaluate thyroid mass
• CT WITH CONTRAST to differentiate cellulitis from abscess and to identify vascular mass
Initial evaluation(surgical diagnosis)
• FNA to decompresse the mass and to provide material for cx
• If malignancy suspected => incisional or exicional bx indicated

Congenital neck masses
Branchial cleft cysts• 1/3 of congenital neck masses• Nontender, fluctuant masses that may become inflamed
and lead to abscess formation during an upper respiratory infection
• First branchial cleft cysts, rare, typically present near the angle of the mandible
• Second branchial cysts are found high in the neck and deep to the anterior border of the sternocleidomastoid muscle
• Third branchial cleft cysts, also rare, are seen near the upper pole of the thyroid gland
Branchial cleft cyst
• Ultrasound shows a fluid-filled cyst and can differentiate cystic lesions from solid masses
• CT and MRI also confirm the cystic characteristics of the mass and, more importantly, delineate the relationship of the cyst to surrounding structures
• Management of branchial cleft cysts is surgical excision

Branchial cleft cyst

Thyroglossal duct cyst• Forms in a persistent thyroid descent tract that
begins as an elongation of the thyroid diverticulum• Most in the midline near the level of the hyoid
bone, elevate with swallowing, and can rarely present laterally
• A thyroglossal duct cyst usually presents as an asymptomatic mass but may be associated with mild dysphagia
• infrequently, may get infected and rapidly enlarge

Thyroglossal duct cyst

Dermoid cyst
• Dermoid cysts consist of epithelium-lined cavities filled with skin appendages (e.g., hair, hair follicles, sebaceous glands)
• Typically, dermoid cysts are seen in the midline of the neck, usually in the submental region
• They are attached to and move with the overlying skin and are painless unless infected
• Management is by complete surgical excision

Dermoid cyst

Lymphatic malformation
• Previously termed lymphangioma• Congenital malformations of lymph tissue that result from
the failure of lymph spaces to connect to the rest of the lymphatic system
• Soft, smooth, nontender mass that is compressible and can be transilluminated
• Macrocystic lymphatic malformations (previously termed cystic hygroma) contain large thickwalled cysts that have less infiltration of surrounding tissue
• lymphatic malformations fluctuate in size as a result of infection or hemorrhage

Cystic Hygroma
Infectious neck masses
Acute unilateral cervical
lymphadenitis
Subacute/chronic unilateral lymphadenitis
Acute bilateral cervical
lymphadenitis
Subacute/chronic bilateral lymphadenitis

Acute bilateral cervical lymphadenitis
• Is the most common infectious neck mass• Viral
– Caused by a benign, self-limited viral upper respiratory infection (eg, enterovirus, adenovirus, influenza virus)
– The LN(reactive LN) typically are small, rubbery, mobile, discrete, minimally tender, and without erythema or warmth
-Baterial: GAS pharyngitis is a common cause of bilateral cervical lymphadenitis, which is often tender

Acute unilateral cervical Lymphadenitis
Acute unilateral cervical lymphadenitis is usually caused by bacteria
-S. Aureus-GAS
-In young infants, Streptococcus agalactiae (group B streptococcus)

S. aureus and GAS
-Between 40 and 80 % of cases-Most of these infections occur in children younger than
5 years of age-Patients may have a history of a recent URI or impetigo
-Submandibular nodes are affected in more than 50 %
-The lymph node usually is 3 to 6 cm in diameter, tender, warm, erythematous, nondiscrete, and poorly mobile
-One-fourth to one-third of infected nodes suppurate and become fluctuant
Other causes
-Acute unilateral cervical lymphadenitis in older children with history of periodontal disease usually is caused by an infection with
anaerobic bacteria
-Tularemia

Subacute/chronic bilateral cervical lymphadenitis
-Most often caused by EBV or CMV infection-EBV causes infectious mononucleosis that may
manifest as fever, exudative pharyngitis, lymphadenopathy, and hepatosplenomegaly
-CMV also can cause a mononucleosis-like illness
Subacute/chronic unilateral cervical lymphadenitis
-Nontuberculous mycobacteria (NTM) infections
-Bartonella henselae-cat scratch disease (CSD)
-TB -Toxoplasmosis

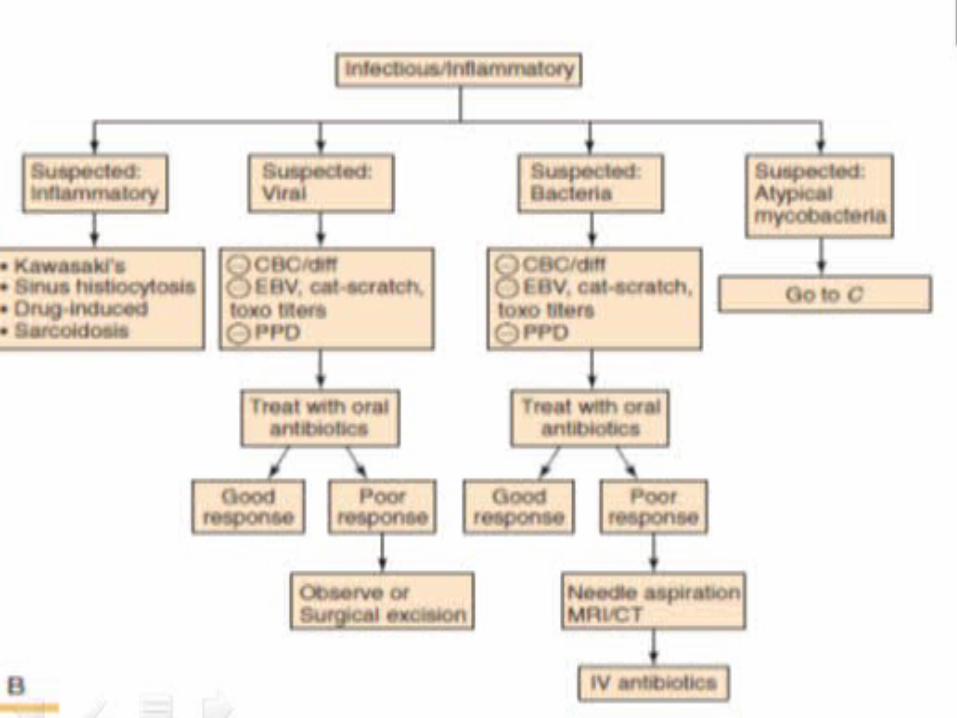
Treatement
• Acute bilateral LN — Treatment is not usually necessary for acute bilateral lymphadenitis (LN), which most frequently is related to a self-limited viral illness. The treatment of those with severe, progressive, or persistent cervical lymphadenitis depends upon the etiology
Treatement• Acute unilateral LN — The initial treatment depends upon the
severity of symptoms• In well-appearing children with a slightly enlarged and minimally
tender cervical lymph node, it is suggested to measure the lymph node and monitoring it over time
• In children with moderate symptoms (eg, fever, warm and/or tender adenitis without evidence of fluctuance), a course of oral antimicrobial therapy is recomended. FNA of the inflamed node before initiation of oral therapy may help to guide antimicrobial coverage
• In children with severe symptoms (eg, fever, fluctuant node, cellulitis), parenteral antimicrobial therapy after incision and drainage of the inflamed node is recomended

Treatement
• Treatment failure — If the child fails to respond to empiric therapy, the differential diagnosis needs to be expanded to include uncommon causes of acute unilateral cervical adenitis, including noninfectious causes. The history needs to be re-reviewed. Surgical excision, drainage, or biopsy may be necessary
Back to our case • Acute unilateral cervical lymphadenitis• ENT consult was ordered• A decision to drain the abscess was taken in the same day of
presentation• Pus cx was taken intraoperatively • A 2 weeks course of Augmentin was started• The patient did very well postoperatively and was free of
symptoms• Cx was positive for Staph Aureus• Pt was discharged home on oral Augmentin 4 days after his
admission to the hospital