cerebrovascularsystem patient cases perfusion territories perfusion territories venous drainage...
TRANSCRIPT

CerebrovascularCerebrovascularSystemSystem
PatientPatientCasesCases
Perfusion TerritoriesPerfusion Territories
Venous DrainageVenous Drainage
VertebrobasilarVertebrobasilarSystemSystem
Cardiovascular DiseaseCardiovascular Disease
Map of EssentialMap of EssentialConceptsConcepts
CircleCircleOf WillisOf Willis
Blood SupplyBlood SupplyTo BrainTo Brain
Carotid SystemCarotid System
Blood Supply toBlood Supply toSpinal CordSpinal Cord
Oxygen DemandsOxygen DemandsAnd MetabolismAnd Metabolism
DM McKeough© 2008

The Cerebrovascular SystemThe Cerebrovascular SystemThe Cerebrovascular SystemThe Cerebrovascular System Oxygen demands and metabolism Cerebrovascular disease Blood supply to the brain Carotid system
Stroke effects Vertebrobasilar system
Stroke effects Circle of Willis Perfusion Territories Venous drainage Blood supply to the spinal cord Patient cases
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Oxygen Demands 1/2Oxygen Demands 1/2Oxygen Demands 1/2Oxygen Demands 1/2 The CNS (brain and spinal cord) is the best The CNS (brain and spinal cord) is the best
protected organ in the human body including protected organ in the human body including mechanisms to protect its blood supply.mechanisms to protect its blood supply.
At approximately 3 pounds, the brain accounts At approximately 3 pounds, the brain accounts for about 2% of body mass.for about 2% of body mass.
Consumes 17% of cardiac output. Consumes 17% of cardiac output.
Responsible for 20% of oxygen consumption Responsible for 20% of oxygen consumption at rest.at rest.
The CNS (brain and spinal cord) is the best The CNS (brain and spinal cord) is the best protected organ in the human body including protected organ in the human body including mechanisms to protect its blood supply.mechanisms to protect its blood supply.
At approximately 3 pounds, the brain accounts At approximately 3 pounds, the brain accounts for about 2% of body mass.for about 2% of body mass.
Consumes 17% of cardiac output. Consumes 17% of cardiac output.
Responsible for 20% of oxygen consumption Responsible for 20% of oxygen consumption at rest.at rest.
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Metabolism 2/2Metabolism 2/2Metabolism 2/2Metabolism 2/2
Brain’s sole source of energy is aerobic or Brain’s sole source of energy is aerobic or oxidative metabolism.oxidative metabolism.
Therefore, the brain requires a constant supply Therefore, the brain requires a constant supply of Oof O22 and glucose, 24 hours a day. and glucose, 24 hours a day.
Brain’s sole source of energy is aerobic or Brain’s sole source of energy is aerobic or oxidative metabolism.oxidative metabolism.
Therefore, the brain requires a constant supply Therefore, the brain requires a constant supply of Oof O22 and glucose, 24 hours a day. and glucose, 24 hours a day.
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Cerebrovascular DiseaseCerebrovascular DiseaseCerebrovascular DiseaseCerebrovascular Disease
While the blood supply to the brain is highly While the blood supply to the brain is highly protected, cerebrovascular disease is the third protected, cerebrovascular disease is the third leading cause of death in American adults and leading cause of death in American adults and the number one cause of chronic functional the number one cause of chronic functional disability requiring rehabilitative intervention.disability requiring rehabilitative intervention.
While the blood supply to the brain is highly While the blood supply to the brain is highly protected, cerebrovascular disease is the third protected, cerebrovascular disease is the third leading cause of death in American adults and leading cause of death in American adults and the number one cause of chronic functional the number one cause of chronic functional disability requiring rehabilitative intervention.disability requiring rehabilitative intervention.
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Blood Supply to the Brain Blood Supply to the Brain 1/61/6
Blood Supply to the Brain Blood Supply to the Brain 1/61/6
Approximately 1,000 ml/min Approximately 1,000 ml/min delivered via two systems.delivered via two systems.
Anterior (Anterior (CarotidCarotid) system:) system: 70% of supply (35% from 70% of supply (35% from
each internal carotid artery)each internal carotid artery) Supplies the superior 2/3 of Supplies the superior 2/3 of
the brainthe brain Posterior (Posterior (VertebrobasilarVertebrobasilar) )
system:system: 30% of supply30% of supply Supplies the inferior 1/3 of Supplies the inferior 1/3 of
the brain and brainstemthe brain and brainstemLast ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Blood Supply to the Brain Blood Supply to the Brain 2/62/6
Blood Supply to the Brain Blood Supply to the Brain 2/62/6
CarotidPerfusionTerritory(Superior 2/3)
A.
Verterbo-BasilarPerfusionTerritory(Inferior 1/3)
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Anterior (Anterior (CarotidCarotid) ) system:system:
70% of supply (35% 70% of supply (35% from each internal from each internal carotid artery)carotid artery)
Supplies the Supplies the superior 2/3 of the superior 2/3 of the brainbrain
Click to animateClick to animate
Carotid SystemCarotid System 3/6
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map
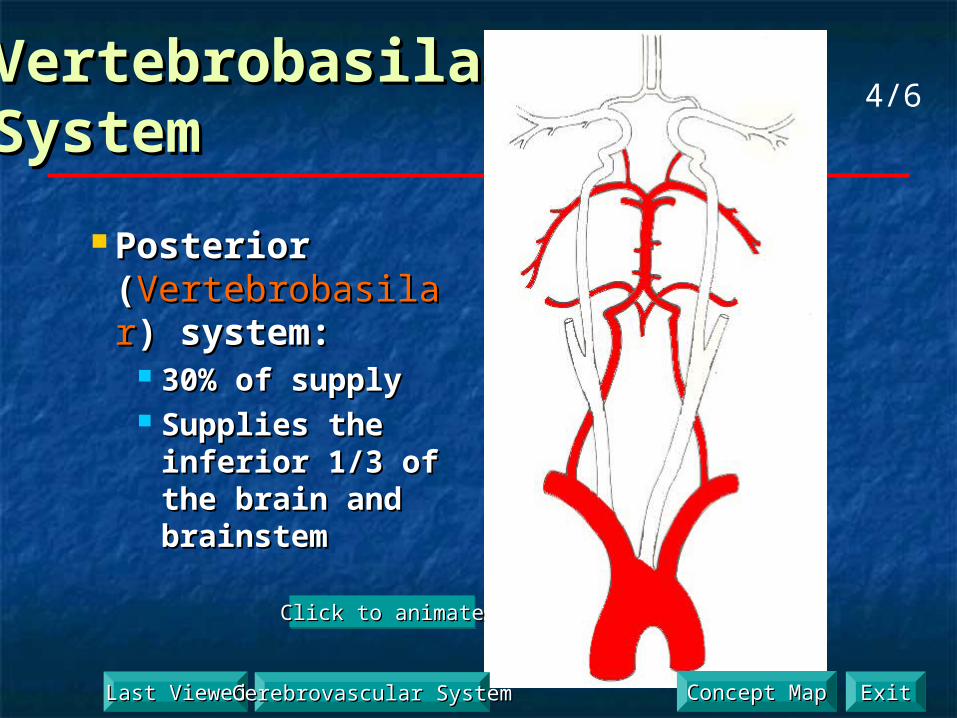
VertebrobasilarVertebrobasilarSystemSystem
Click to animateClick to animateClick to animateClick to animate
Posterior Posterior ((VertebrobasilarVertebrobasilar) ) system:system:
30% of supply30% of supply Supplies the inferior Supplies the inferior
1/3 of the brain and 1/3 of the brain and brainstembrainstem
4/6
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Blood SupplyBlood Supply to the Brain to the Brain
Blood SupplyBlood Supply to the Brain to the Brain
5/6
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Blood Supply to the Brain 6/6Blood Supply to the Brain 6/6Blood Supply to the Brain 6/6Blood Supply to the Brain 6/6
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Carotid System 1/12Carotid System 1/12Carotid System 1/12Carotid System 1/12
Click to AnimateClick to AnimateClick to AnimateClick to Animate
Anterior cerebral a.
Middle cerebral a.
Anterior communicating a.
Internal carotid a.
Anterior (Anterior (CarotidCarotid) ) system:system:
70% of supply (35% 70% of supply (35% from each internal from each internal carotid artery)carotid artery)
Supplies the superior Supplies the superior 2/3 of the brain2/3 of the brain
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Carotid System 2/12Carotid System 2/12Carotid System 2/12Carotid System 2/12
Bilateral system, each Bilateral system, each hemisphere has its own carotid hemisphere has its own carotid artery.artery.
Supplies the superior two thirds Supplies the superior two thirds of the brain.of the brain.
Derived from: aorta, common Derived from: aorta, common carotid, internal carotid, carotid carotid, internal carotid, carotid foramen (adjacent to optic foramen (adjacent to optic chiasm)chiasm)
Anterior cerebral arteryAnterior cerebral artery (ACA) (ACA) Middle cerebral arteryMiddle cerebral artery (MCA) (MCA)
Bilateral system, each Bilateral system, each hemisphere has its own carotid hemisphere has its own carotid artery.artery.
Supplies the superior two thirds Supplies the superior two thirds of the brain.of the brain.
Derived from: aorta, common Derived from: aorta, common carotid, internal carotid, carotid carotid, internal carotid, carotid foramen (adjacent to optic foramen (adjacent to optic chiasm)chiasm)
Anterior cerebral arteryAnterior cerebral artery (ACA) (ACA) Middle cerebral arteryMiddle cerebral artery (MCA) (MCA)
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Carotid System 3/12Carotid System 3/12Carotid System 3/12Carotid System 3/12
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Carotid System 4/12Carotid System 4/12Carotid System 4/12Carotid System 4/12
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Carotid System 5/12Carotid System 5/12Carotid System 5/12Carotid System 5/12
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Anterior Cerebral Artery 6/12Anterior Cerebral Artery 6/12Anterior Cerebral Artery 6/12Anterior Cerebral Artery 6/12
ADAM
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Middle Cerebral Artery 7/12Middle Cerebral Artery 7/12Middle Cerebral Artery 7/12Middle Cerebral Artery 7/12
ADAM
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Carotid System 8/12Carotid System 8/12Carotid System 8/12Carotid System 8/12
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Middle Cerebral Artery 9/12Middle Cerebral Artery 9/12Middle Cerebral Artery 9/12Middle Cerebral Artery 9/12
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Carotid System 10/12Carotid System 10/12Carotid System 10/12Carotid System 10/12
Perfusion territory by artery
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Stroke EffectsStroke EffectsStroke EffectsStroke EffectsS&S of ACA occlusionDistribution
Contralateral legPrecentral gyrus
Paresis/ paralysisPostcentral gyrus
Sensory impairment
S&S of MCA occlusionDistribution
Contralateral face & armPrecentral gyrus
Paresis/ paralysisPostcentral gyrus
Sensory impairment
11/12
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Middle Cerebral Artery Occlusion 12/12Middle Cerebral Artery Occlusion 12/12Middle Cerebral Artery Occlusion 12/12Middle Cerebral Artery Occlusion 12/12
Most common strokeMost common stroke L MCAL MCA
Most common effectsMost common effects Right hemiplegia Face & UE > LERight hemiplegia Face & UE > LE
If MCA perfuses lateral aspect of If MCA perfuses lateral aspect of hemisphere, how is the LE hemisphere, how is the LE affected?affected?
Occlusion occurs in the internal Occlusion occurs in the internal capsulecapsule
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

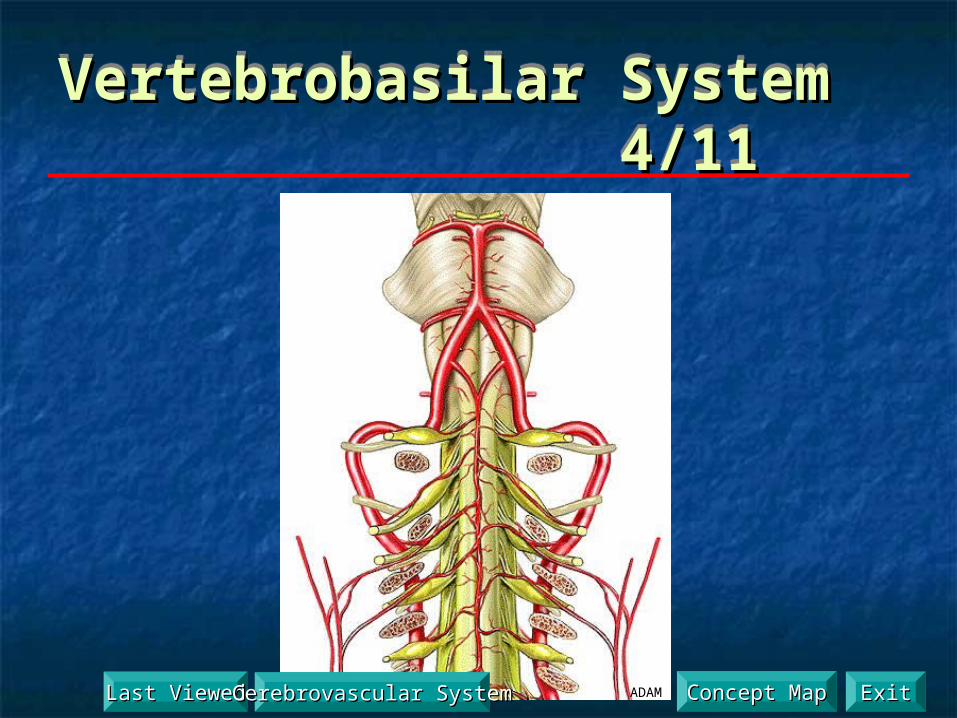
Vertebrobasilar System 1/11Vertebrobasilar System 1/11Vertebrobasilar System 1/11Vertebrobasilar System 1/11 Supplies the inferior one third of Supplies the inferior one third of
the brain; inferior surface of the the brain; inferior surface of the temporal and occipital lobes and temporal and occipital lobes and brainstem.brainstem.
Derived from: subclavian, Derived from: subclavian, vertebral, foramen magnum, vertebral, foramen magnum, anterior spinal, posterior inferior anterior spinal, posterior inferior cerebellar, basilar, anterior cerebellar, basilar, anterior inferior cerebellar, internal inferior cerebellar, internal auditory, superior cerebellar, auditory, superior cerebellar, posterior cerebral arteryposterior cerebral artery
Supplies the inferior one third of Supplies the inferior one third of the brain; inferior surface of the the brain; inferior surface of the temporal and occipital lobes and temporal and occipital lobes and brainstem.brainstem.
Derived from: subclavian, Derived from: subclavian, vertebral, foramen magnum, vertebral, foramen magnum, anterior spinal, posterior inferior anterior spinal, posterior inferior cerebellar, basilar, anterior cerebellar, basilar, anterior inferior cerebellar, internal inferior cerebellar, internal auditory, superior cerebellar, auditory, superior cerebellar, posterior cerebral arteryposterior cerebral artery
Click to animateClick to animate
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Vertebrobasilar System 2/11Vertebrobasilar System 2/11Vertebrobasilar System 2/11Vertebrobasilar System 2/11
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Vertebrobasilar System 3/11Vertebrobasilar System 3/11Vertebrobasilar System 3/11Vertebrobasilar System 3/11
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map
Vertebrobasilar System 4/11Vertebrobasilar System 4/11Vertebrobasilar System 4/11Vertebrobasilar System 4/11
ADAMLast ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Vertebrobasilar System 5/11Vertebrobasilar System 5/11Vertebrobasilar System 5/11Vertebrobasilar System 5/11
ADAM
Vertebral a.
Basilar a.
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Vertebrobasilar System 6/11Vertebrobasilar System 6/11Vertebrobasilar System 6/11Vertebrobasilar System 6/11
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Posterior Cerebral ArteryPosterior Cerebral Artery 7/11 7/11Posterior Cerebral ArteryPosterior Cerebral Artery 7/11 7/11
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Posterior Cerebral Artery 8/11Posterior Cerebral Artery 8/11Posterior Cerebral Artery 8/11Posterior Cerebral Artery 8/11
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Posterior Cerebral Artery 9/11Posterior Cerebral Artery 9/11Posterior Cerebral Artery 9/11Posterior Cerebral Artery 9/11
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

3 Cerebellar Arteries 3 Cerebellar Arteries 10/1110/11
3 Cerebellar Arteries 3 Cerebellar Arteries 10/1110/11
Superior cerebellar a.
Anterior inferior cerebellar a.
Posterior inferior cerebellar a.
Pons
Medulla
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Stroke Effects 11/11Stroke Effects 11/11Stroke Effects 11/11Stroke Effects 11/11
S&S of vertebrobasilar occlusion (brainstem stroke)S&S of vertebrobasilar occlusion (brainstem stroke) Impaired life support systems (HR, RR, BP, consciousness)Impaired life support systems (HR, RR, BP, consciousness)
S&S of basilar artery occlusionS&S of basilar artery occlusion Impaired CN functionsImpaired CN functions Impaired long tract functions (motor/ sensory)Impaired long tract functions (motor/ sensory)
S&S of PICA occlusionS&S of PICA occlusion Impaired pain sensation in ipsilateral face and contralateral Impaired pain sensation in ipsilateral face and contralateral
bodybody
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Circle of Circle of WillisWillis
Circle of Circle of WillisWillis
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Perfusion TerritoriesPerfusion TerritoriesPerfusion TerritoriesPerfusion TerritoriesWatershed Territory
Primary Artery Territory
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Venous Drainage 1/2Venous Drainage 1/2Venous Drainage 1/2Venous Drainage 1/2
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Venous Drainage 2/2Venous Drainage 2/2Venous Drainage 2/2Venous Drainage 2/2
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

BloodBloodSupplySupplyto theto the
Spinal Spinal CordCord
BloodBloodSupplySupplyto theto the
Spinal Spinal CordCord
1/2
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Spinal Arteries 2/2Spinal Arteries 2/2Spinal Arteries 2/2Spinal Arteries 2/2Anterior Posterior
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

Patient CasesPatient CasesPatient CasesPatient Cases
Sudden inability to speakSudden inability to speak Left leg weaknessLeft leg weakness Worst headache of lifeWorst headache of life Decreased vision in one eyeDecreased vision in one eye Left neglectLeft neglect Anterior cord syndromeAnterior cord syndrome
Last ViewedLast Viewed Cerebrovascular SystemCerebrovascular System ExitExitConcept MapConcept Map

MinicaseMinicaseSudden Inability to Speak 1/5Sudden Inability to Speak 1/5
MinicaseMinicaseSudden Inability to Speak 1/5Sudden Inability to Speak 1/5While standing in the check-out line at the store, 55 year-While standing in the check-out line at the store, 55 year-old retired nurse realized she was suddenly unable to old retired nurse realized she was suddenly unable to speak. Consciousness, attention, voluntary movement, speak. Consciousness, attention, voluntary movement, and the ability to understand speech were all unaffected. and the ability to understand speech were all unaffected. Incredulous, but believing she knew what is happening to Incredulous, but believing she knew what is happening to her. She left the store and drove herself directly to the her. She left the store and drove herself directly to the emergency room. In the ER she communicated to emergency room. In the ER she communicated to doctors what she thought was occurring. With difficulty doctors what she thought was occurring. With difficulty she uttered two words: “stroke” and “speech”.she uttered two words: “stroke” and “speech”.
While standing in the check-out line at the store, 55 year-While standing in the check-out line at the store, 55 year-old retired nurse realized she was suddenly unable to old retired nurse realized she was suddenly unable to speak. Consciousness, attention, voluntary movement, speak. Consciousness, attention, voluntary movement, and the ability to understand speech were all unaffected. and the ability to understand speech were all unaffected. Incredulous, but believing she knew what is happening to Incredulous, but believing she knew what is happening to her. She left the store and drove herself directly to the her. She left the store and drove herself directly to the emergency room. In the ER she communicated to emergency room. In the ER she communicated to doctors what she thought was occurring. With difficulty doctors what she thought was occurring. With difficulty she uttered two words: “stroke” and “speech”.she uttered two words: “stroke” and “speech”.
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

MinicaseMinicase Sudden Inability to Speak 2/5Sudden Inability to Speak 2/5
MinicaseMinicase Sudden Inability to Speak 2/5Sudden Inability to Speak 2/5 Her past medical history was notable for overweight, Her past medical history was notable for overweight,
hypertension and type II diabetes. hypertension and type II diabetes. Examination revealed loss of the nasal-labial fold on Examination revealed loss of the nasal-labial fold on
the left and weakness in the left cheek and jaw. the left and weakness in the left cheek and jaw. Her jaw-jerk reflex was hyperactive. Her jaw-jerk reflex was hyperactive. All other movement, sensation, and reflexes were All other movement, sensation, and reflexes were
within normal limits. within normal limits.
Where is the lesion causing these symptoms?Where is the lesion causing these symptoms?
Her past medical history was notable for overweight, Her past medical history was notable for overweight, hypertension and type II diabetes. hypertension and type II diabetes.
Examination revealed loss of the nasal-labial fold on Examination revealed loss of the nasal-labial fold on the left and weakness in the left cheek and jaw. the left and weakness in the left cheek and jaw.
Her jaw-jerk reflex was hyperactive. Her jaw-jerk reflex was hyperactive. All other movement, sensation, and reflexes were All other movement, sensation, and reflexes were
within normal limits. within normal limits.
Where is the lesion causing these symptoms?Where is the lesion causing these symptoms?
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

Minicase Follow-UpMinicase Follow-Up Sudden Inability to Speak 3/5Sudden Inability to Speak 3/5
Minicase Follow-UpMinicase Follow-Up Sudden Inability to Speak 3/5Sudden Inability to Speak 3/5 As confirmed by CT image, this woman was having a As confirmed by CT image, this woman was having a
stroke. stroke.
The occlusion involved a deep penetrating branch of The occlusion involved a deep penetrating branch of the the middle cerebral arterymiddle cerebral artery supplying the inferior frontal supplying the inferior frontal gyrus on the gyrus on the leftleft causing weakness in the lower part of causing weakness in the lower part of the right face and tongue and Broca’s aphasia. the right face and tongue and Broca’s aphasia.
As confirmed by CT image, this woman was having a As confirmed by CT image, this woman was having a stroke. stroke.
The occlusion involved a deep penetrating branch of The occlusion involved a deep penetrating branch of the the middle cerebral arterymiddle cerebral artery supplying the inferior frontal supplying the inferior frontal gyrus on the gyrus on the leftleft causing weakness in the lower part of causing weakness in the lower part of the right face and tongue and Broca’s aphasia. the right face and tongue and Broca’s aphasia.
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

Productive (Broca’s) Aphasia 4/5Productive (Broca’s) Aphasia 4/5Productive (Broca’s) Aphasia 4/5Productive (Broca’s) Aphasia 4/5
Produced by a lesion of Produced by a lesion of the inferior frontal gyrus the inferior frontal gyrus of the dominant of the dominant hemisphere.hemisphere.
Play recordingPlay recording
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

Minicase Follow-UpMinicase Follow-Up Sudden Inability to Speak 5/5Sudden Inability to Speak 5/5
Minicase Follow-UpMinicase Follow-Up Sudden Inability to Speak 5/5Sudden Inability to Speak 5/5
The key signs and symptoms in this case are:The key signs and symptoms in this case are: Suddenly unable to speakSuddenly unable to speak Consciousness, attention, voluntary movement, and Consciousness, attention, voluntary movement, and
the ability to understand speech were all unaffectedthe ability to understand speech were all unaffected Loss of the nasal-labial fold on the left and weakness in Loss of the nasal-labial fold on the left and weakness in
the left cheek and jawthe left cheek and jaw Her jaw-jerk reflex was hyperactiveHer jaw-jerk reflex was hyperactive
The key signs and symptoms in this case are:The key signs and symptoms in this case are: Suddenly unable to speakSuddenly unable to speak Consciousness, attention, voluntary movement, and Consciousness, attention, voluntary movement, and
the ability to understand speech were all unaffectedthe ability to understand speech were all unaffected Loss of the nasal-labial fold on the left and weakness in Loss of the nasal-labial fold on the left and weakness in
the left cheek and jawthe left cheek and jaw Her jaw-jerk reflex was hyperactiveHer jaw-jerk reflex was hyperactive
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

MinicaseMinicaseLeft Leg Weakness 1/5Left Leg Weakness 1/5
MinicaseMinicaseLeft Leg Weakness 1/5Left Leg Weakness 1/5
On attempting to stand after finishing breakfast, a On attempting to stand after finishing breakfast, a 67-year-old woman fell to the ground, hitting the 67-year-old woman fell to the ground, hitting the table on the way down, because she was unable table on the way down, because she was unable to support her body weight on her left leg. She to support her body weight on her left leg. She called for help from her husband who was unable called for help from her husband who was unable to get her off the floor and called for emergency to get her off the floor and called for emergency assistance. assistance.
On attempting to stand after finishing breakfast, a On attempting to stand after finishing breakfast, a 67-year-old woman fell to the ground, hitting the 67-year-old woman fell to the ground, hitting the table on the way down, because she was unable table on the way down, because she was unable to support her body weight on her left leg. She to support her body weight on her left leg. She called for help from her husband who was unable called for help from her husband who was unable to get her off the floor and called for emergency to get her off the floor and called for emergency assistance. assistance.
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

MinicaseMinicaseLeft Leg Weakness 2/5Left Leg Weakness 2/5
MinicaseMinicaseLeft Leg Weakness 2/5Left Leg Weakness 2/5
Her past history was positive for obesity, hypertension, Her past history was positive for obesity, hypertension, peripheral vascular disease, and smoking one pack per day for peripheral vascular disease, and smoking one pack per day for 52 years. 52 years.
She had hyperactive deep tendon reflexes in her left knee and She had hyperactive deep tendon reflexes in her left knee and ankle, and a positive Babinski sign in her left foot. ankle, and a positive Babinski sign in her left foot.
The left leg was flaccid and she had no voluntary control of The left leg was flaccid and she had no voluntary control of movement. movement.
She had mild impairment of light touch, pain, and temperature She had mild impairment of light touch, pain, and temperature sensation in her left leg. sensation in her left leg.
Voluntary movement, reflexes, and sensation were intact in all Voluntary movement, reflexes, and sensation were intact in all other regions of the body. other regions of the body.
Where is the lesion causing these symptoms?Where is the lesion causing these symptoms?
Her past history was positive for obesity, hypertension, Her past history was positive for obesity, hypertension, peripheral vascular disease, and smoking one pack per day for peripheral vascular disease, and smoking one pack per day for 52 years. 52 years.
She had hyperactive deep tendon reflexes in her left knee and She had hyperactive deep tendon reflexes in her left knee and ankle, and a positive Babinski sign in her left foot. ankle, and a positive Babinski sign in her left foot.
The left leg was flaccid and she had no voluntary control of The left leg was flaccid and she had no voluntary control of movement. movement.
She had mild impairment of light touch, pain, and temperature She had mild impairment of light touch, pain, and temperature sensation in her left leg. sensation in her left leg.
Voluntary movement, reflexes, and sensation were intact in all Voluntary movement, reflexes, and sensation were intact in all other regions of the body. other regions of the body.
Where is the lesion causing these symptoms?Where is the lesion causing these symptoms?
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

Minicase Follow-UpMinicase Follow-Up Left Leg Weakness 3/5Left Leg Weakness 3/5
Minicase Follow-UpMinicase Follow-Up Left Leg Weakness 3/5Left Leg Weakness 3/5 A head CT scan was done and the results A head CT scan was done and the results
suggested a probable rightsuggested a probable right anterior cerebral anterior cerebral artery infarct. artery infarct.
Follow-up hear CT scan one month later Follow-up hear CT scan one month later confirmed the presence of a hypodense area on confirmed the presence of a hypodense area on the anterior medial aspect of the right the anterior medial aspect of the right hemisphere consistent with a hemisphere consistent with a right anterior right anterior cerebral arterycerebral artery infarct infarct
A head CT scan was done and the results A head CT scan was done and the results suggested a probable rightsuggested a probable right anterior cerebral anterior cerebral artery infarct. artery infarct.
Follow-up hear CT scan one month later Follow-up hear CT scan one month later confirmed the presence of a hypodense area on confirmed the presence of a hypodense area on the anterior medial aspect of the right the anterior medial aspect of the right hemisphere consistent with a hemisphere consistent with a right anterior right anterior cerebral arterycerebral artery infarct infarct
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

Minicase Follow-UpMinicase Follow-Up Left Leg Weakness 4/5Left Leg Weakness 4/5
Minicase Follow-UpMinicase Follow-Up Left Leg Weakness 4/5Left Leg Weakness 4/5
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

Minicase Follow-UpMinicase Follow-Up Left Leg Weakness 5/5Left Leg Weakness 5/5
Minicase Follow-UpMinicase Follow-Up Left Leg Weakness 5/5Left Leg Weakness 5/5The key signs and symptoms in this case are:The key signs and symptoms in this case are: Unable to support her body weight on her left legUnable to support her body weight on her left leg Hyperactive deep tendon reflexes in her left knee and ankle, and Hyperactive deep tendon reflexes in her left knee and ankle, and
a positive Babinski sign in her left foota positive Babinski sign in her left foot The left leg was flaccid and she had no voluntary control of The left leg was flaccid and she had no voluntary control of
movementmovement She had mild impairment of light touch, pain, and temperature She had mild impairment of light touch, pain, and temperature
sensation in her left legsensation in her left leg Voluntary movement, reflexes, and sensation were intact in all Voluntary movement, reflexes, and sensation were intact in all
other regions of the bodyother regions of the body
The key signs and symptoms in this case are:The key signs and symptoms in this case are: Unable to support her body weight on her left legUnable to support her body weight on her left leg Hyperactive deep tendon reflexes in her left knee and ankle, and Hyperactive deep tendon reflexes in her left knee and ankle, and
a positive Babinski sign in her left foota positive Babinski sign in her left foot The left leg was flaccid and she had no voluntary control of The left leg was flaccid and she had no voluntary control of
movementmovement She had mild impairment of light touch, pain, and temperature She had mild impairment of light touch, pain, and temperature
sensation in her left legsensation in her left leg Voluntary movement, reflexes, and sensation were intact in all Voluntary movement, reflexes, and sensation were intact in all
other regions of the bodyother regions of the body
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

MinicaseMinicaseSudden-onset Worst Headache of Life 1/7Sudden-onset Worst Headache of Life 1/7
MinicaseMinicaseSudden-onset Worst Headache of Life 1/7Sudden-onset Worst Headache of Life 1/7
A 68-year-old man suddenly developed “the worst of A 68-year-old man suddenly developed “the worst of my life.” On the morning of admission he was sitting my life.” On the morning of admission he was sitting watching TV when at 9:00 am he suddenly developed watching TV when at 9:00 am he suddenly developed an explosive headache worse than anything he had an explosive headache worse than anything he had ever experienced. The headache began in the bifrontal ever experienced. The headache began in the bifrontal area and over the next few minutes all over the head area and over the next few minutes all over the head and down the neck. He denied loss of consciousness, and down the neck. He denied loss of consciousness, nausea, vomiting or vision changes. nausea, vomiting or vision changes.
A 68-year-old man suddenly developed “the worst of A 68-year-old man suddenly developed “the worst of my life.” On the morning of admission he was sitting my life.” On the morning of admission he was sitting watching TV when at 9:00 am he suddenly developed watching TV when at 9:00 am he suddenly developed an explosive headache worse than anything he had an explosive headache worse than anything he had ever experienced. The headache began in the bifrontal ever experienced. The headache began in the bifrontal area and over the next few minutes all over the head area and over the next few minutes all over the head and down the neck. He denied loss of consciousness, and down the neck. He denied loss of consciousness, nausea, vomiting or vision changes. nausea, vomiting or vision changes.
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

MinicaseMinicaseSudden-onset Worst Headache of Life 2/7Sudden-onset Worst Headache of Life 2/7
MinicaseMinicaseSudden-onset Worst Headache of Life 2/7Sudden-onset Worst Headache of Life 2/7
History was positive for severe diffuse History was positive for severe diffuse atherosclerosis, including coronary disease and atherosclerosis, including coronary disease and peripheral vascular disease requiring multiple peripheral vascular disease requiring multiple bypass surgeries. bypass surgeries.
He was obese and smoked two packs a day for He was obese and smoked two packs a day for 43 years. 43 years.
Examination was unremarkable except for mild Examination was unremarkable except for mild nuchal rigidity. nuchal rigidity.
History was positive for severe diffuse History was positive for severe diffuse atherosclerosis, including coronary disease and atherosclerosis, including coronary disease and peripheral vascular disease requiring multiple peripheral vascular disease requiring multiple bypass surgeries. bypass surgeries.
He was obese and smoked two packs a day for He was obese and smoked two packs a day for 43 years. 43 years.
Examination was unremarkable except for mild Examination was unremarkable except for mild nuchal rigidity. nuchal rigidity.
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

Minicase Follow-UpMinicase Follow-UpSudden-onset Worst Headache of Life 3/7Sudden-onset Worst Headache of Life 3/7
Minicase Follow-UpMinicase Follow-UpSudden-onset Worst Headache of Life 3/7Sudden-onset Worst Headache of Life 3/7
Nuchal rigidity is often a sign of meningeal Nuchal rigidity is often a sign of meningeal irritation caused by inflammation, infection, or irritation caused by inflammation, infection, or hemorrhage in the subarachnoid space.hemorrhage in the subarachnoid space.
Nuchal rigidity is often a sign of meningeal Nuchal rigidity is often a sign of meningeal irritation caused by inflammation, infection, or irritation caused by inflammation, infection, or hemorrhage in the subarachnoid space.hemorrhage in the subarachnoid space.
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

Minicase Follow-UpMinicase Follow-UpSudden-onset Worst Headache of Life 4/7Sudden-onset Worst Headache of Life 4/7
Minicase Follow-UpMinicase Follow-UpSudden-onset Worst Headache of Life 4/7Sudden-onset Worst Headache of Life 4/7
The man underwent emergency head CT which The man underwent emergency head CT which demonstrated regions of hyperdensity in the demonstrated regions of hyperdensity in the subarachnoid space consistent with subarachnoid subarachnoid space consistent with subarachnoid hemorrhage layering in the medial longitudinal hemorrhage layering in the medial longitudinal fissure, lateral fissure, and around the brainstem. fissure, lateral fissure, and around the brainstem.
Next he was taken for an angiogram which clearly Next he was taken for an angiogram which clearly revealed an revealed an aneurysmaneurysm arising from the region of the arising from the region of the anterior communicating arteryanterior communicating artery. .
The man underwent emergency head CT which The man underwent emergency head CT which demonstrated regions of hyperdensity in the demonstrated regions of hyperdensity in the subarachnoid space consistent with subarachnoid subarachnoid space consistent with subarachnoid hemorrhage layering in the medial longitudinal hemorrhage layering in the medial longitudinal fissure, lateral fissure, and around the brainstem. fissure, lateral fissure, and around the brainstem.
Next he was taken for an angiogram which clearly Next he was taken for an angiogram which clearly revealed an revealed an aneurysmaneurysm arising from the region of the arising from the region of the anterior communicating arteryanterior communicating artery. .
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

The circle of Willis has been dissected, and three berry aneurysms are seen. Multiple aneurysms are seen in about 20-30% of cases of berry aneurysm. Such aneurysms are "congenital" in the sense that the defect in the arterial wall is present from birth, but the actual aneurysm takes years to develop, so that rupture is most likely to occur in young to middle age adults.
Berry Aneurysm Berry Aneurysm 5/75/7
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

The white arrow on the black card marks the site of a ruptured berry aneurysm in the circle of Willis. This is a major cause for subarachnoid hemorrhage.
Berry Aneurysm Berry Aneurysm 6/76/7
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

Minicase Follow-UpMinicase Follow-UpSudden-onset Worst Headache of Life 7/7Sudden-onset Worst Headache of Life 7/7
Minicase Follow-UpMinicase Follow-UpSudden-onset Worst Headache of Life 7/7Sudden-onset Worst Headache of Life 7/7
The key signs and symptoms in this case are:The key signs and symptoms in this case are: Suddenly developed “the worst of my life”Suddenly developed “the worst of my life” Headache began in the bifrontal area and over the next Headache began in the bifrontal area and over the next
few minutes was all over the head and down the neckfew minutes was all over the head and down the neck Examination was unremarkable except for mild nuchal Examination was unremarkable except for mild nuchal
rigidityrigidity
The key signs and symptoms in this case are:The key signs and symptoms in this case are: Suddenly developed “the worst of my life”Suddenly developed “the worst of my life” Headache began in the bifrontal area and over the next Headache began in the bifrontal area and over the next
few minutes was all over the head and down the neckfew minutes was all over the head and down the neck Examination was unremarkable except for mild nuchal Examination was unremarkable except for mild nuchal
rigidityrigidity
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

MinicaseMinicase Decreased Vision in One Eye 1/8Decreased Vision in One Eye 1/8
MinicaseMinicase Decreased Vision in One Eye 1/8Decreased Vision in One Eye 1/8 A 63-year-old woman went to an A 63-year-old woman went to an
ophthalmologist complaining of episodes of ophthalmologist complaining of episodes of decreased vision in her “right eye” over the decreased vision in her “right eye” over the past several weeks. past several weeks.
A 63-year-old woman went to an A 63-year-old woman went to an ophthalmologist complaining of episodes of ophthalmologist complaining of episodes of decreased vision in her “right eye” over the decreased vision in her “right eye” over the past several weeks. past several weeks.
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

MinicaseMinicase Decreased Vision in One Eye 2/8Decreased Vision in One Eye 2/8
MinicaseMinicase Decreased Vision in One Eye 2/8Decreased Vision in One Eye 2/8 Her medical history was notable for type II diabetes, Her medical history was notable for type II diabetes,
hypercholesterolemia, and coronary artery disease.hypercholesterolemia, and coronary artery disease. About 5-6 weeks ago the patient began having About 5-6 weeks ago the patient began having
“episodes of sudden blurry wavy” appearance of her “episodes of sudden blurry wavy” appearance of her vision. vision.
She believed this was mostly in the right eye but never She believed this was mostly in the right eye but never tried looking with only one eye at a time. tried looking with only one eye at a time.
Her medical history was notable for type II diabetes, Her medical history was notable for type II diabetes, hypercholesterolemia, and coronary artery disease.hypercholesterolemia, and coronary artery disease.
About 5-6 weeks ago the patient began having About 5-6 weeks ago the patient began having “episodes of sudden blurry wavy” appearance of her “episodes of sudden blurry wavy” appearance of her vision. vision.
She believed this was mostly in the right eye but never She believed this was mostly in the right eye but never tried looking with only one eye at a time. tried looking with only one eye at a time.
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

MinicaseMinicase Decreased Vision in One Eye 3/8Decreased Vision in One Eye 3/8
MinicaseMinicase Decreased Vision in One Eye 3/8Decreased Vision in One Eye 3/8 Episodes would last for 15-20 minutes, resolved with Episodes would last for 15-20 minutes, resolved with
no visual impairment, repeated 3-4 times per week, and no visual impairment, repeated 3-4 times per week, and were never accompanied by pain. were never accompanied by pain.
Previously she was able to recognize faces during the Previously she was able to recognize faces during the episodes but was unable to read. episodes but was unable to read.
The current episode, that began two days ago, has The current episode, that began two days ago, has resulted in persistent decreased vision on the right.resulted in persistent decreased vision on the right.
Episodes would last for 15-20 minutes, resolved with Episodes would last for 15-20 minutes, resolved with no visual impairment, repeated 3-4 times per week, and no visual impairment, repeated 3-4 times per week, and were never accompanied by pain. were never accompanied by pain.
Previously she was able to recognize faces during the Previously she was able to recognize faces during the episodes but was unable to read. episodes but was unable to read.
The current episode, that began two days ago, has The current episode, that began two days ago, has resulted in persistent decreased vision on the right.resulted in persistent decreased vision on the right.
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

MinicaseMinicase Decreased Vision in One Eye 4/8Decreased Vision in One Eye 4/8
MinicaseMinicase Decreased Vision in One Eye 4/8Decreased Vision in One Eye 4/8
Neurologic examination revealed fluent speech. Neurologic examination revealed fluent speech. Pupils 3 mm, constricting to 2 mm bilaterally. Pupils 3 mm, constricting to 2 mm bilaterally. Normal fundi. Visual acuity 20/30 right and 20/25 left. Normal fundi. Visual acuity 20/30 right and 20/25 left. Visual field testing revealed a right homonymous hemianopia. Visual field testing revealed a right homonymous hemianopia. Extraocular movements intact. Extraocular movements intact. Facial sensation intact to light touch and pinprick. Facial sensation intact to light touch and pinprick. Face symmetrical. Normal palate elevation. Face symmetrical. Normal palate elevation. Normal shoulder shrug. Tongue midline. Normal shoulder shrug. Tongue midline.
Where is the lesion causing these symptoms?Where is the lesion causing these symptoms?
Neurologic examination revealed fluent speech. Neurologic examination revealed fluent speech. Pupils 3 mm, constricting to 2 mm bilaterally. Pupils 3 mm, constricting to 2 mm bilaterally. Normal fundi. Visual acuity 20/30 right and 20/25 left. Normal fundi. Visual acuity 20/30 right and 20/25 left. Visual field testing revealed a right homonymous hemianopia. Visual field testing revealed a right homonymous hemianopia. Extraocular movements intact. Extraocular movements intact. Facial sensation intact to light touch and pinprick. Facial sensation intact to light touch and pinprick. Face symmetrical. Normal palate elevation. Face symmetrical. Normal palate elevation. Normal shoulder shrug. Tongue midline. Normal shoulder shrug. Tongue midline.
Where is the lesion causing these symptoms?Where is the lesion causing these symptoms?
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

MinicaseMinicase Follow-UpFollow-UpDecreased Vision in One Eye 5/8Decreased Vision in One Eye 5/8
MinicaseMinicase Follow-UpFollow-UpDecreased Vision in One Eye 5/8Decreased Vision in One Eye 5/8 The transient episodes of 15-20 minutes of decreased The transient episodes of 15-20 minutes of decreased
right-sided vision occurring over several weeks, right-sided vision occurring over several weeks, followed by a sudden-onset persistent deficit is followed by a sudden-onset persistent deficit is suggestive of TIAs preceding a cerebral infarct. suggestive of TIAs preceding a cerebral infarct.
A right homonymous hemianopia can be caused by a A right homonymous hemianopia can be caused by a lesion in the left hemisphere visual pathway anywhere lesion in the left hemisphere visual pathway anywhere from the left optic tract to the primary visual cortex. from the left optic tract to the primary visual cortex.
The patient’s age and past medical history raise the The patient’s age and past medical history raise the suspicion of cerebrovascular disease of the cause. suspicion of cerebrovascular disease of the cause.
The transient episodes of 15-20 minutes of decreased The transient episodes of 15-20 minutes of decreased right-sided vision occurring over several weeks, right-sided vision occurring over several weeks, followed by a sudden-onset persistent deficit is followed by a sudden-onset persistent deficit is suggestive of TIAs preceding a cerebral infarct. suggestive of TIAs preceding a cerebral infarct.
A right homonymous hemianopia can be caused by a A right homonymous hemianopia can be caused by a lesion in the left hemisphere visual pathway anywhere lesion in the left hemisphere visual pathway anywhere from the left optic tract to the primary visual cortex. from the left optic tract to the primary visual cortex.
The patient’s age and past medical history raise the The patient’s age and past medical history raise the suspicion of cerebrovascular disease of the cause. suspicion of cerebrovascular disease of the cause.
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

MinicaseMinicase Follow-UpFollow-UpDecreased Vision in One Eye 6/8Decreased Vision in One Eye 6/8
MinicaseMinicase Follow-UpFollow-UpDecreased Vision in One Eye 6/8Decreased Vision in One Eye 6/8 The patient was sent to the hospital where an initial CT scan The patient was sent to the hospital where an initial CT scan
suggested a suggested a left posterior cerebral arteryleft posterior cerebral artery infarct, and a follow-up infarct, and a follow-up MRI confirmed the presence of a left PCS infarct involving the MRI confirmed the presence of a left PCS infarct involving the left primary visual cortex. left primary visual cortex.
An magnetic resonance angiogram (MRA) revealed several An magnetic resonance angiogram (MRA) revealed several stenoses of the cerebral vessels compatible with diffuse stenoses of the cerebral vessels compatible with diffuse intracranial atherosclerotic disease. intracranial atherosclerotic disease.
She was treated with long-term oral anticoagulation. She was treated with long-term oral anticoagulation. Her right hemianopia did not improve, but over time she learned Her right hemianopia did not improve, but over time she learned
to adapt to her visual deficit. to adapt to her visual deficit.
The patient was sent to the hospital where an initial CT scan The patient was sent to the hospital where an initial CT scan suggested a suggested a left posterior cerebral arteryleft posterior cerebral artery infarct, and a follow-up infarct, and a follow-up MRI confirmed the presence of a left PCS infarct involving the MRI confirmed the presence of a left PCS infarct involving the left primary visual cortex. left primary visual cortex.
An magnetic resonance angiogram (MRA) revealed several An magnetic resonance angiogram (MRA) revealed several stenoses of the cerebral vessels compatible with diffuse stenoses of the cerebral vessels compatible with diffuse intracranial atherosclerotic disease. intracranial atherosclerotic disease.
She was treated with long-term oral anticoagulation. She was treated with long-term oral anticoagulation. Her right hemianopia did not improve, but over time she learned Her right hemianopia did not improve, but over time she learned
to adapt to her visual deficit. to adapt to her visual deficit.
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

MinicaseMinicase Follow-UpFollow-UpDecreased Vision in One Eye 7/8Decreased Vision in One Eye 7/8
MinicaseMinicase Follow-UpFollow-UpDecreased Vision in One Eye 7/8Decreased Vision in One Eye 7/8
MRI axial T2 weighted image of left posterior cerebral artery (PCA) infarction
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

MinicaseMinicase Follow-UpFollow-UpDecreased Vision in One Eye 8/8Decreased Vision in One Eye 8/8
MinicaseMinicase Follow-UpFollow-UpDecreased Vision in One Eye 8/8Decreased Vision in One Eye 8/8
The key signs and symptoms in this case are:The key signs and symptoms in this case are: Episodes of sudden “blurry/ wavy” appearance of her Episodes of sudden “blurry/ wavy” appearance of her
vision in her “right eye” over the past several weeksvision in her “right eye” over the past several weeks Right homonymous hemianopiaRight homonymous hemianopia
The key signs and symptoms in this case are:The key signs and symptoms in this case are: Episodes of sudden “blurry/ wavy” appearance of her Episodes of sudden “blurry/ wavy” appearance of her
vision in her “right eye” over the past several weeksvision in her “right eye” over the past several weeks Right homonymous hemianopiaRight homonymous hemianopia
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

MinicaseMinicase Left Neglect 1/5Left Neglect 1/5
MinicaseMinicase Left Neglect 1/5Left Neglect 1/5
A 61-year-old right-handed man was witnessed A 61-year-old right-handed man was witnessed slumping to the floor in the grocery store. slumping to the floor in the grocery store.
A 61-year-old right-handed man was witnessed A 61-year-old right-handed man was witnessed slumping to the floor in the grocery store. slumping to the floor in the grocery store.
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

MinicaseMinicase Left Neglect 2/5Left Neglect 2/5
MinicaseMinicase Left Neglect 2/5Left Neglect 2/5
On examination in the hospital he denied anything was wrong On examination in the hospital he denied anything was wrong but said, “They called an ambulance because they said I had a but said, “They called an ambulance because they said I had a stroke.” stroke.”
He was unaware of having any impairment and wanted to go He was unaware of having any impairment and wanted to go home. home.
He had profound left visual field neglect , no blink to threat on He had profound left visual field neglect , no blink to threat on the left, and no voluntary gaze to the left past midline. the left, and no voluntary gaze to the left past midline.
When trying to right, he moved the pen in the air off to the right When trying to right, he moved the pen in the air off to the right of the page. of the page.
When shown his left hand and asked what it was, he replied When shown his left hand and asked what it was, he replied “Someone’s hand.”“Someone’s hand.”
On examination in the hospital he denied anything was wrong On examination in the hospital he denied anything was wrong but said, “They called an ambulance because they said I had a but said, “They called an ambulance because they said I had a stroke.” stroke.”
He was unaware of having any impairment and wanted to go He was unaware of having any impairment and wanted to go home. home.
He had profound left visual field neglect , no blink to threat on He had profound left visual field neglect , no blink to threat on the left, and no voluntary gaze to the left past midline. the left, and no voluntary gaze to the left past midline.
When trying to right, he moved the pen in the air off to the right When trying to right, he moved the pen in the air off to the right of the page. of the page.
When shown his left hand and asked what it was, he replied When shown his left hand and asked what it was, he replied “Someone’s hand.”“Someone’s hand.”
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

MinicaseMinicase Left Neglect 3/5Left Neglect 3/5
MinicaseMinicase Left Neglect 3/5Left Neglect 3/5
When asked who’s hand it was he replied, “The When asked who’s hand it was he replied, “The doctor’s.” doctor’s.”
He had a marked right gaze preference. He had a marked right gaze preference. He had marked weakness in the lower portion of the He had marked weakness in the lower portion of the
left face. left face. Strength was 0/5 in the left arm and leg, the left plantar Strength was 0/5 in the left arm and leg, the left plantar
response was upgoing, and there was no response to response was upgoing, and there was no response to pinprick on the left side.pinprick on the left side.
What lesion is causing this man’s symptoms? What lesion is causing this man’s symptoms?
When asked who’s hand it was he replied, “The When asked who’s hand it was he replied, “The doctor’s.” doctor’s.”
He had a marked right gaze preference. He had a marked right gaze preference. He had marked weakness in the lower portion of the He had marked weakness in the lower portion of the
left face. left face. Strength was 0/5 in the left arm and leg, the left plantar Strength was 0/5 in the left arm and leg, the left plantar
response was upgoing, and there was no response to response was upgoing, and there was no response to pinprick on the left side.pinprick on the left side.
What lesion is causing this man’s symptoms? What lesion is causing this man’s symptoms?
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

MinicaseMinicase Follow-UpFollow-UpLeft Neglect 4/5Left Neglect 4/5
MinicaseMinicase Follow-UpFollow-UpLeft Neglect 4/5Left Neglect 4/5 The patient exhibits several forms of neglect. The patient exhibits several forms of neglect. In addition to anosognosia, he has left sensory neglect, to In addition to anosognosia, he has left sensory neglect, to
visual and tactile stimuli, as well as left motor neglect. visual and tactile stimuli, as well as left motor neglect. These signs and symptoms are most commonly seen in These signs and symptoms are most commonly seen in
patients with nondominant (usually right) parietal lobe lesions. patients with nondominant (usually right) parietal lobe lesions.
Given the sudden onset of the deficits, involvement of the left Given the sudden onset of the deficits, involvement of the left arm and leg, the presence of sensory and motor deficits, and arm and leg, the presence of sensory and motor deficits, and the patient’s age, the most likely cause is ischemic infarction the patient’s age, the most likely cause is ischemic infarction of the of the right internal carotidright internal carotid arteryartery. .
The patient exhibits several forms of neglect. The patient exhibits several forms of neglect. In addition to anosognosia, he has left sensory neglect, to In addition to anosognosia, he has left sensory neglect, to
visual and tactile stimuli, as well as left motor neglect. visual and tactile stimuli, as well as left motor neglect. These signs and symptoms are most commonly seen in These signs and symptoms are most commonly seen in
patients with nondominant (usually right) parietal lobe lesions. patients with nondominant (usually right) parietal lobe lesions.
Given the sudden onset of the deficits, involvement of the left Given the sudden onset of the deficits, involvement of the left arm and leg, the presence of sensory and motor deficits, and arm and leg, the presence of sensory and motor deficits, and the patient’s age, the most likely cause is ischemic infarction the patient’s age, the most likely cause is ischemic infarction of the of the right internal carotidright internal carotid arteryartery. .
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

MinicaseMinicase Follow-UpFollow-UpLeft Neglect 5/5Left Neglect 5/5
MinicaseMinicase Follow-UpFollow-UpLeft Neglect 5/5Left Neglect 5/5
The key signs and symptoms in this case are:The key signs and symptoms in this case are: AnosognosiaAnosognosia Left face, arm and leg plegia with positive Babinski’s Left face, arm and leg plegia with positive Babinski’s
signsign No blink to threat on the leftNo blink to threat on the left No voluntary gaze to the left past midlineNo voluntary gaze to the left past midline No response to pinprick on the leftNo response to pinprick on the left
The key signs and symptoms in this case are:The key signs and symptoms in this case are: AnosognosiaAnosognosia Left face, arm and leg plegia with positive Babinski’s Left face, arm and leg plegia with positive Babinski’s
signsign No blink to threat on the leftNo blink to threat on the left No voluntary gaze to the left past midlineNo voluntary gaze to the left past midline No response to pinprick on the leftNo response to pinprick on the left
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

Occlusion of the anterior spinal artery (anterior cord Occlusion of the anterior spinal artery (anterior cord syndrome) in the cervical region would produce syndrome) in the cervical region would produce what impairments?what impairments?
Occlusion of the anterior spinal artery (anterior cord Occlusion of the anterior spinal artery (anterior cord syndrome) in the cervical region would produce syndrome) in the cervical region would produce what impairments?what impairments?
Click for answer
The anterior spinal artery perfuses the anterior 2/3 of the spinal cord including the ventral horns as well as all tracts in the lateral and anterior columns, bilaterally. Damage to the lateral corticospinal tracts cause upper motor neuron signs, bilaterally, below the lesion level. Damage to lower motor neurons in the ventral horns cause lower motor neuron signs, bilaterally, at the lesion level. Damage to the lateral spinothalamic tracts cause absence of pain and temperature sensation, bilaterally, below the lesion level. Sparing of the dorsal columns leaves light touch, vibration, and position sense intact throughout.
Click for explanation
1/2
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

UMN
DRG
UMN
DRG
R L
Anterior cord lesion
Lateral corticospinal tract lesionIpsilateral upper motor neurons signs
Contralateral loss of pain and temperature sense
Lateral spinothalamic tract lesion
Anterior Cord Syndrome
Common causes include anterior spinal artery infarct, trauma, and MS.
Click to animate
2/2
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map

The EndThe EndThe EndThe End
© DM McKeough 2008© DM McKeough 2008© DM McKeough 2008© DM McKeough 2008
Last ViewedLast Viewed Patient CasesPatient Cases ExitExitConcept MapConcept Map