cerebrovascular diseases background basic manifestations ... iv presentations... · af and cva 6000...
TRANSCRIPT

Medicine for Psychiatrists
TIA/Stroke updates
2018
• Cerebrovascular Diseases
� Background
� Basic manifestations
� Risk Factors/Investigations� Risk Factors/Investigations
� Assessment/Triage/treatment
� Grey zone
• When to refer
�Updates
TIME IS BRAIN
But “Do No Harm” still applies

Cerebrovascular Disease
Spectrum..TIA/Stroke/Death
• Worst acquired adult neurological disease Affects significant others 1
Will increase – aging pop
Every minute 2 million neurons 2,3Every minute 2 million neurons 2,3
• A neurological emergency 4!!
• Treatment/outcomes- time dependant !!
1. Life after stroke .www.stroke.org .NZ
2. Hacke et al NEJM 2008;359:1317
3. NINDS Study Group NEJM 1995;333:1581
4. Karen Furie et al Up To Date , Initial evaluation and management of TIA and minor ischemic stroke , Mar 2017

STROKETIA
Ischaemic Hge
70-85%
15-30%

Transient Ischemic attack (TIA)
Definition
Classical – Time based “A TIA is defined as stroke symptoms and signs that resolve within 24 hours”5
Problematic!!
1. Most TIA symptoms very short lived6
2. If longer symptoms, minimal resolve7,8 2. If longer symptoms, minimal resolve7,8
3. 1/2 with TIA have evidence of recent infarction on MRI (DWI)
Current
• AHA/ASA - Tissue based , focal neurological dysfunction, brain, spinal cord, retinal ischemia without infarction 6
5. Easton JD et al Stroke 2009;40:2276
6. Caplan LR et al Curr Atheroscler Rep 2006;8:276
7. Albers GW et al NEJM 2002;347:1713
8. Caplan LR et al Arch Neuo 2007;64:1080
TIA/ Stroke
pathophysiology
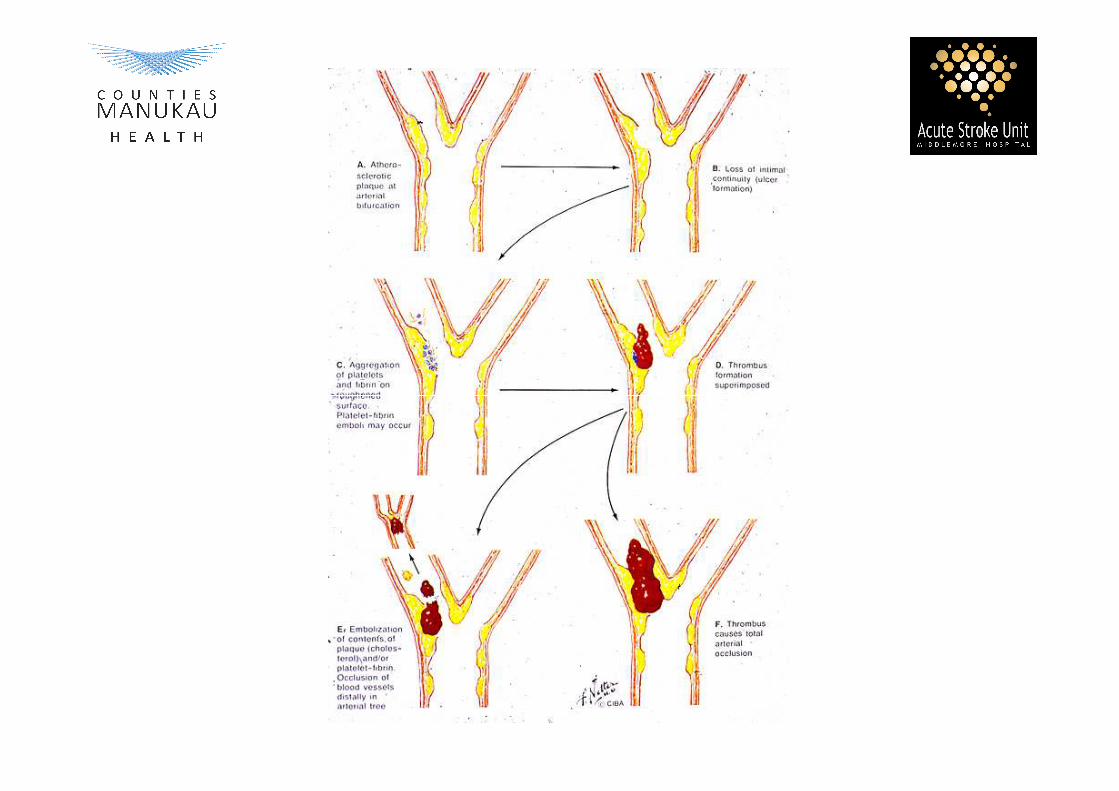
• Ischemic 9,11
� Low flow TIA- atherothrombotic stenotic 10
� Embolic , Cardiac, artery to artery, ESUS(embolic source of unknown origin).
� Small vessel TIA� Small vessel TIA
– Aim: Identify and r/o large artery stenotic lesion � (LVO)…revascularization Surgery ( CEA)
• Haemorrhage� ICH- intraparenchymal
� SAH- CSF
9. Karen Furie et al Up To Date , Initial evaluation and management of TIA and minor ischemic stroke , Mar 201710. Caplan LR Caplan’s Stroke 4th ed 2009.p22 11. Adams HP Stroke 1993;24:35 (TOAST)
TIA
characteristics
Funny turns/isolated symptoms 12
• Dizziness
• Light headedness• Light headedness
• Blurry vision
• Gen weakness
� Stroke risk <2%
� Tumour <1%
� ICH <1%
12. Hankey et al Stroke 1997; 28:2126

TIA
characteristics 13
� TIA/Stroke
• Sudden
• Focal - vascular territory
• Maximal deficit
XXX Mimics• Gradual
• No vascular territory
• No focal symptoms
• Gain in function• Maximal deficit
• Loss of function
– Motor
– Sensory
– Vision
– Speech
– Cognition
• Gain in function
• Migratory secs, mins
• Tell tale signs
– Tongue biting
– Abnormal movements
– Incontinence
– Post event confusion
13. Louis Caplan et al, Up To Date, Differential diagnosis of TIA and stroke , Mar 2017
Cerebrovascular disease
Localising lesions
Anterior circulation
• ACA
� Leg >> arm
� Unilateral Motor, sensory
• MCA
� Motor/sensory
� Cortical
� Speech
� Vision
� Cognition

Cerebrovascular disease
Localising lesions
Posterior circulation
VA
BA
• Cerebellar
� Nystagmus
� Dysarthria
� Dysmetria
� Dysdiadokokinesia
� Ataxia
• Brain Stem – Eye signs
• Medulla – Cerebellar,
crossed signs
• Pons – motor/sensory

Cerebrovascular Disease
Risk factors 14
• Modifiable:
�Hypertension
�Diabetes
� Smoking
• Non-modifiable:
�Age
�Gender
� Family history� Smoking
�Dyslipidemia
�AF
�Other - lifestyle
� Family history
�Genetics

Cerebrovascular Disease
Risk factor differs 15
Young (<45 yrs)
• PFO
• Dissection
• Connective tissue disease
Older (Traditional RF)
• HT
• DM
• Smoking
– SLE
– Anti Phospholipid
– Other vasculitis
• Moyamoya disease
• Familial - CADASIL
• AF
• Dyslipidemia
• Others
15. Karen Furie et al ,Up To Date, Secondary prevention for specific causes of ischemic stroke and TIA ,May 2017

Other risk factors
• Age, risk of CVS increases with age
• Gender
• Family history - CADASIL
• Obesity
• Connective tissue disease- SLE,APL
• Life style, ETOH, Light 1-2/day beneficial, heavy harms 16• Life style, ETOH, Light 1-2/day beneficial, heavy harms 16
• APOE issue unresolved 17,18,19
• Hyperhomocysteinemia , inc levels ass with inc risk of CAD,C VS, Isch, lacunar 20
16 Furie KL et al Stroke 2011;42:227
17. McCarron MO et al Neurology 1999;53:1308
18. Schneider JA et al Stroke 2005 ;36:954
19 Sturgeon JD et al Stroke 2005;36:2484
20. Eikelboom JW et al Stroke 2000;31:1069
Hypertension
• Single biggest risk factor !!- 50% CAD, Heart failure
- 62% Strokes 21
• Target range,<140/80,DM<130/80 22
• Evidence for treatment, BP reduction 12/5 mmHg, 30-40% • Evidence for treatment, BP reduction 12/5 mmHg, 30-40%
RRR, both Secondary and Primary event rate 5yrs 23
• NNT: 11 patients for 5 yrs : 1 fatal or non-fatal major vascular
event 24
21. Anic G et al, Oct 2013,vol31,Journal of Hypertension, ESH/ESC, 2013 Practice Guidelines.
22. Aburto Net al BMJ,2013 346
23. PROGRESS Collaborative Group, Lancet 2001;358:13;1033
24. INERACT II,SAMMPRIS
Diabetes• Risk x 2
– vascular events
– associated - dyslipidemia, endothelial dysfunction, platelet and coagulation abnormalities 26
• IGT may be a risk factor 26
• Metabolic syndrome– Prediabetic
– insulin resistance, 3 or more, high FBS ,HT, low HDL, and obesity may confer – insulin resistance, 3 or more, high FBS ,HT, low HDL, and obesity may confer increased risk 28
• Strict Glycemic control reduces –– Microvascular complications- retinopathy, nephropathy, neuropathy25 –
DCCT,UKPDS
– Macrovascular**- Type I yes ,Type II ?? RCTs no consistent evidence, MI, Strokes –DCCT/EDIC
• Life style changes – weight reduction!! …benefits28
25. AHA/ASA 2011 Guidelines
26. Arvanitakis Z et al,Neurology 2006;67:1960
27. Vermeer SE et al Stroke 2006;37:1413
28. Koren—Morag et al Stroke 2005;36:1366

Smoking
• Risk increased for all stroke subtypes, dose dependant29-32
• Evidence: Observational studies
- Nurses Health Study, smokers RR 2.58, Disappears 2-4yrs30
- Framingham Heart Study, OR 1.08 for moderate Carotid stenosis for every 5 pack yrs31
- Prospective Swedish cohort study (11,000 pts),~40% strokes - Prospective Swedish cohort study (11,000 pts),~40% strokes attributable to smoking32
• Cessation – Medicine+ therapy 33,34
29. Ockene IS et al AHA Task force on risk reduction . Circulation 1997;96:3243
30. Kawachi I et al JAMA1993;269:232
31. Wison PW et al NEJM 1997;337:516
32. Li C et al Stroke 2005;36:234
33 Stead LF et al. Cochrane Database Systemic Rev 2012;10 CD008286
34. Suls JM et al Am J preventive Med 2012;42:655

Dyslipidemia
• Major risk– CAD- Atherosclerotic disease
– Stroke – relationship - complex, appears weak risk factor35
• evidence of ischemic stroke attributable to cholesterol- inconsistentand conflicting, PITFALLS**
• Association is weakly positive with high levels > 7mmol36,37
• Ass with hge Strokes, 4.14 mmol37
• Dyslipidemia statin therapy and hge**• Dyslipidemia statin therapy and hge**38
• Other lipid lowering therapy ??
– Lowers cholesterol levels but … No significant impact on stroke incidence
35. Piechowski-J et al Stroke 2004;35:152336. Iso H et al NEJM 1989;320:90437. Lindenstrom E et al BMJ 1994;309:1138 Amarenco P et al NEJM 2006; 355:549
Atrial Fibrillation
• Prevalence – increases with age• Evidence, BAATAF, SPINAF, AFASAK, CAFA, SPAF39
– Primary prevention – risk stratification CHA2DS2VASc– Secondary prevention – Rx, 2011 ..(ASA/AHA27)
• Agents– OAG, NOACS (Dabigatran , rivaroxaban , apixaban)– Benefits: Reduce baseline risk by 2/3 44
– Risk: ICH <1% pa45– Risk: ICH <1% pa45
• Cardio embolic strokes– Are larger and more severe40,41
• Silent cerebral infarcts– TIAs– Cognitive impairment42,43
39. Sturgeon JD et al Stroke 2005;36:248440. Eikelboom JW et al Stroke 2000;31:106941. J Neurosurg 1994 Jan;80(1):51-7 41. Cerebrovasc Dis 1999 Mar-Apr;9(2):102-8 43. Caplan LR Caplan’s Stroke 4th ed 2009.p2244. BamfordJ et al Lancet22;337(8756):1521-6,199145. NEJM 333:1581-7
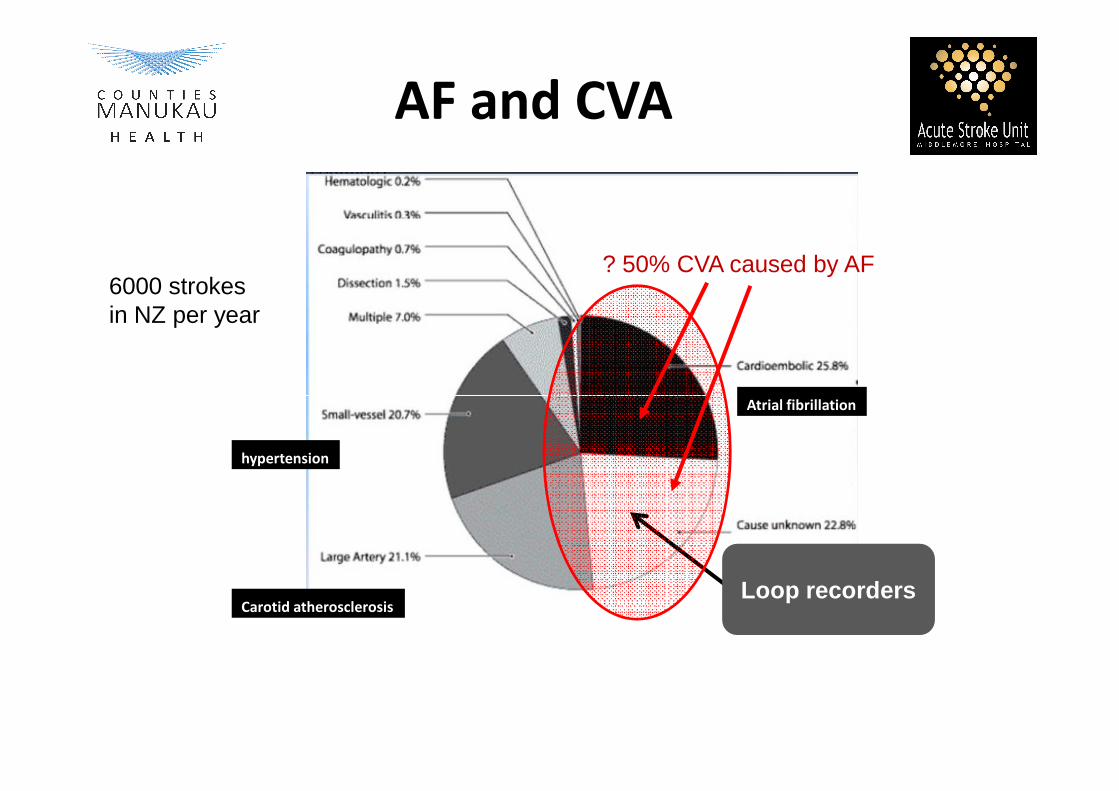
Atrial fibrillation
? 50% CVA caused by AF
AF and CVA
6000 strokes in NZ per year
hypertension
Carotid atherosclerosis
Atrial fibrillation
Loop recorders

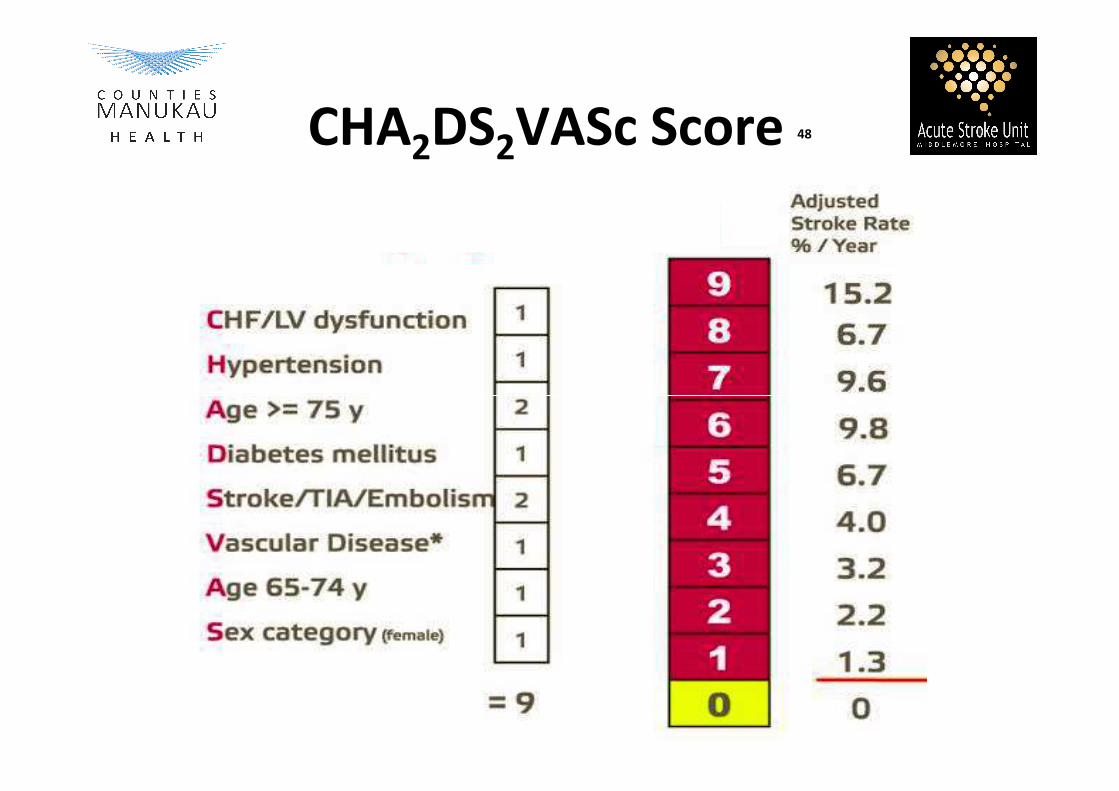
CHA2DS2VASc Score 48

Treatment Options for AFib
Cardioversion
• Pharmacological
• Electrical
Drugs to prevent AFib
• Antiarrhythmic drugs
• Non-antiarrhythmic drugsNon-antiarrhythmic drugs
Drugs to control ventricular rate
Drugs to reduce thromboembolic risk
Non-pharmacological options
• Electrical devices (implantable pacemaker and defibrillator)
• AV node ablation and pacemaker implantation (ablate & pace)
• Catheter ablation
• Surgery (Maze, mini-Maze)

Non-Pharmacological Treatment
Options for AFib
• Pacemakers not curative and must be worn for life
• Surgical procedures may be effective but are not a practical solution for the millions of sufferers of AFib
• Catheter ablation is potentially curative
SurgeryElectrophysiologicalDevices
Pacemaker(single or dual chamber)
Internal atrialdefibrillators
Catheter ablation
AV node ablation
Maze procedure
Modified Maze
(mini-Maze)
50.ACC/AHA/ESC 2006 Guidelines for the Management of Patients With Atrial FibrillationJ Am Coll Cardiol (2006) 48: 854

Medicine for Psychiatrists
TIA/Stroke updates
2018
• Cerebrovascular Diseases
� Background
� Basic manifestations
� Risk Factors/Investigations� Risk Factors/Investigations
� Assessment/Triage/treatment
� Grey zone
• When to refer
• Updates

Investigations
Labrotarory14
� FBC - Hb, Hct ,Wcc, Plt
� U&E, Na
� Glucose , lipids -LDL/HDL,CRP
• ECG• ECG
• Brain Imaging, CT/CTA/CTP, MRI/MRA,MR perfusion, Carotid
Duplex( >70% stenosis)
• Other Investigations in selected cases
• Treatment !!!!!( Express study)9
14. Rothwell PM et al Lancet 2007;370:1432


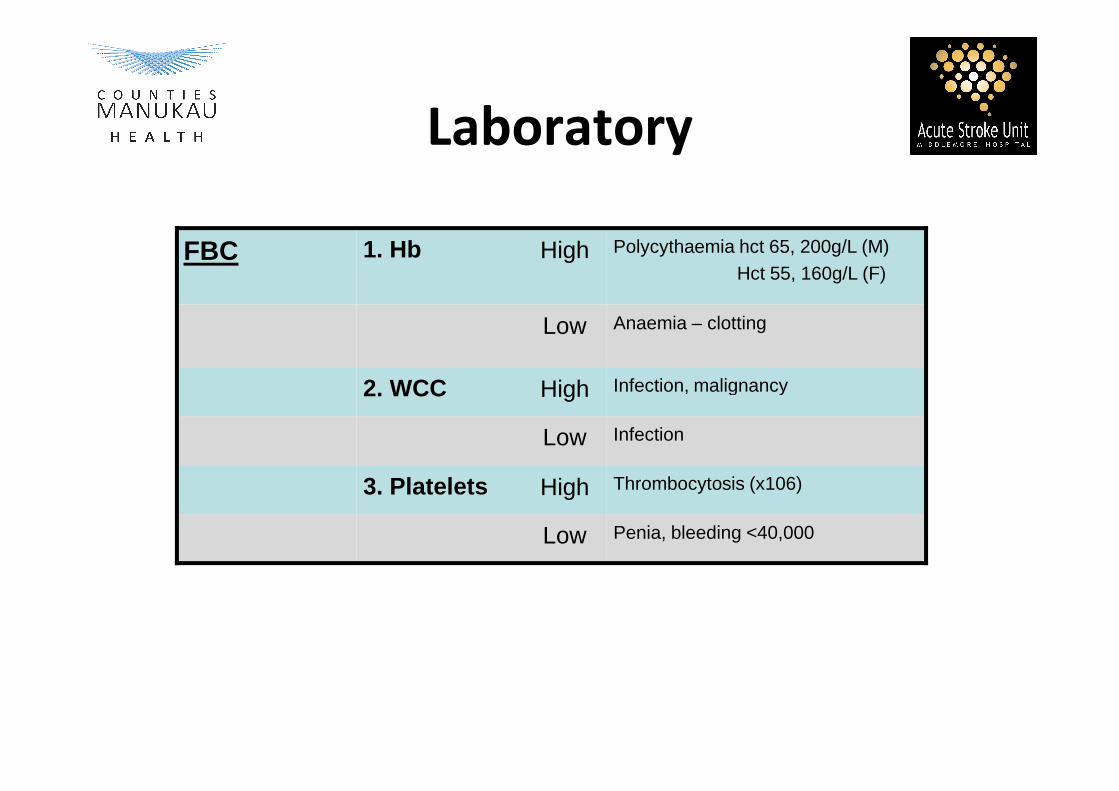
Laboratory
FBC 1. Hb High Polycythaemia hct 65, 200g/L (M)Hct 55, 160g/L (F)
Low Anaemia – clotting
2. WCC High Infection, malignancy2. WCC High
Low Infection
3. Platelets High Thrombocytosis (x106)
Low Penia, bleeding <40,000
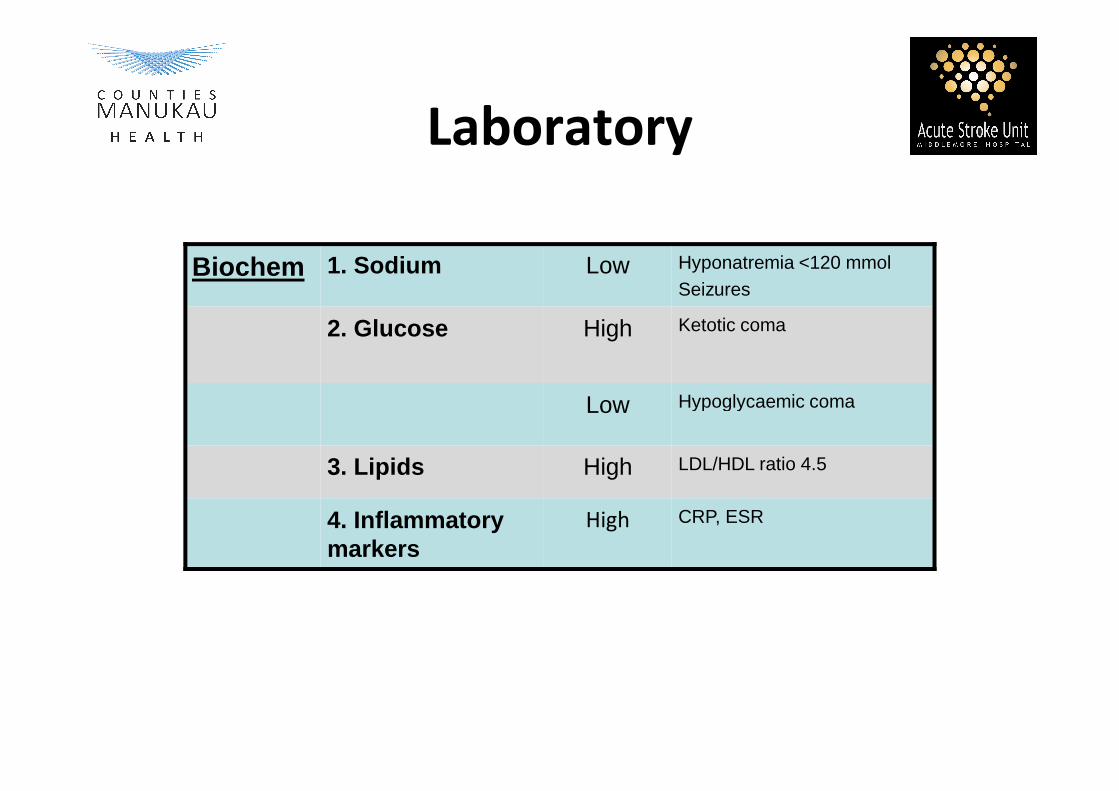
Laboratory
Biochem 1. Sodium Low Hyponatremia <120 mmolSeizures
2. Glucose High Ketotic coma
Low Hypoglycaemic comaLow Hypoglycaemic coma
3. Lipids High LDL/HDL ratio 4.5
4. Inflammatory markers
High CRP, ESR

Other Investigations 5
ECG 1. Arrhythmia (AF) Loop monitoring
2. MI
Young Patients
1. Stroke Screen
2. Connective tissue
5. Easton JD et al Stroke 2009 ;40:2276
51. Flemming KD et al Mayo Clin Proc 2004;79:1071
2. Connective tissue
3. Bubble study (PFO)
Imaging 1. Neuroimaging Surgical lesion -
2. Carotids > 70% lesion
3. Cardiac Echo LA/LV thrombus

STROKETIA
Ischaemic Hge
70-85%
15-30%

TIA –not benign !!
• ABCD2 is a Diagnostic tool
� Practical, use anywhere
� Applicable, validated
� Helps prognosticate� Helps prognosticate
� Score <3 OP,>4 IP
• Aim: Rule out LVO (Large vessel occlusion)
CMDHB

ABCD2 Score 9
Parameter Criteria PointsAge >60 yrs 1
BP >140/90 1
Clinical symptomsFace, arm, leg weakness 2
(max 2 pts)Speech
(max 2 pts)1
Duration >60 mins
10-59 mins
2(max 2 pts)
1
Diabetes 1
Total 7
9 Rothwell PM et al Neurology 2005; 64:817

ABCD2 ScoreStroke Risk
Moderate Risk 4%
High Risk 8%
4
5
6
7Risk Category Day 2 Day 7 Day 90
12% 18%
10% 6%
Low Risk 1%
0
1
2
3
4
ABCD2
1% 3%
STROKETIA
Ischaemic Hge
70-85%
15-30%
Intracranial Haemorrhage
• Causes
�Hypertension
�Amyloid angiopathy
�Raptured aneurysm
�Vascular Malformations
] MAJORITY
�Vascular Malformations
�Others; vasculitis , haemorrhagic infarction (Venous Sinus
Thrombosis), septic emboli (SBE), brain tumour, bleeding
disorders, anticoagulants, thrombolytic therapy, CNS
infection (HSV encephalitis), moya moya, drugs (cocaine
and amphetamines), phenylpropanolamine (appetite
suppressants)
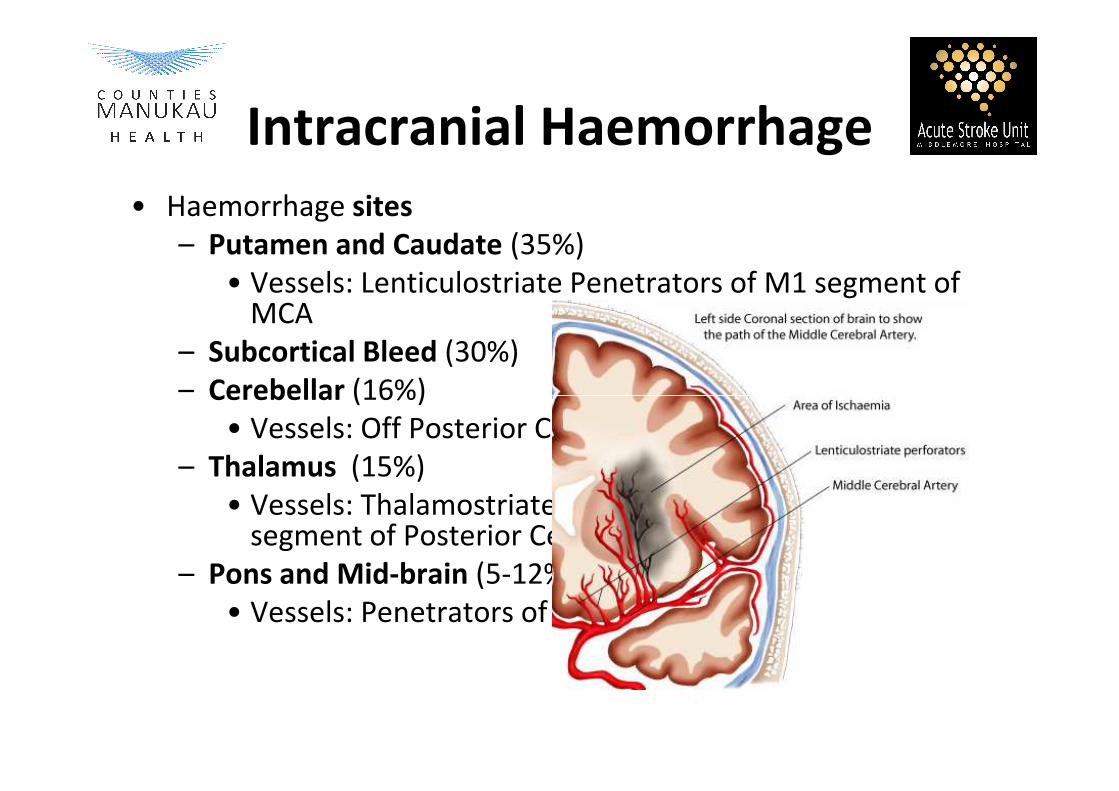
Intracranial Haemorrhage
• Haemorrhage sites
– Putamen and Caudate (35%)
• Vessels: Lenticulostriate Penetrators of M1 segment of MCA
– Subcortical Bleed (30%)
– Cerebellar (16%)– Cerebellar (16%)
• Vessels: Off Posterior Cerebral Artery
– Thalamus (15%)
• Vessels: Thalamostriate Penetrators of P1 & P2 segment of Posterior Cerebral Artery
– Pons and Mid-brain (5-12%)
• Vessels: Penetrators of Basilar Artery

Amyloid angiopathy


Ischaemic Strokes
Classification/Prognosis 55
• Oxfordshire (OSCP,
Bamford) Classification
�TACI – total anterior
circulation infarct
• 1 yr mortality
� 60%
� 19%circulation infarct
�PACI – partial anterior
circulation infarct
�POCI – posterior
cerebral infarct
� LACI – lacunar infarct
� 19%
� 16%
� 11%
55. Bamford J et al Lancet22;337(8756):1521-6,1991

Medicine for Psychiatrists
TIA/Stroke updates
2018
• Cerebrovascular Diseases
� Background
� Basic manifestations
� Risk Factors/Investigations� Risk Factors/Investigations
� Assessment/Triage/treatment
� Grey zone
• When to refer
• Updates

Recommend carotid
endarterectomy
• If symptomatic carotid stenosis of 56
�>80% NNT 5
�70-80% NNT 8
�*50-69% NNT 15 (men)
�on same side as stroke�on same side as stroke
�patient otherwise well
� low surgical risk
• Early intervention!! After 3 mths NNT 125 !! to prevent 1 disabling stroke/death – NASCET, Swedish Stroke Registry
36. Rothwell PM et al Lancet 2004; 363:915
Secondary prevention
TIA/Ischemic events
• Antiplatelet , acute
� DAP – 3 weeks
� SAP
� TAP - no role� TAP - no role
• Statins – Class effect
• BP Lowering - tailor make , choices
• Treat all other risk factors- DM , smoking ,
others

Antiplatelet therapy
Secondary prevention
• SAP- Single
- (A) Aspirin RRR 18% NNT 83
- (C) Clopidogrel
- (D)Dipyridamole RRR 17%
• DAP Dual • DAP Dual
- (A+C) RRR, CHANCE- 3 Weeks, then Single
- up to 3 mo MATCH, CAPRIE
- (A + D) RRR 33%, ESPSII, ESPIRIT – life long
• TAP - Tripple
- No role,…TARDIS,POINT
• ACCP recommend Antiplatelet sec prevention, level I
Antiplatelet therapy58,59
• Secondary prevention• Aspirin (A) RRR ~ 20% NNT 83 ,IST,CAST trials• Clopidogrel (C) RRR ~9% better cf Aspirin CAPRIE**• Dipyridamole (D) RRR 17%• DAP Dual (A+C) RRR, CHANCE , SAMPARIS, MATCH,CHARISMA,CAPRIE
(A+D) RRR 33%, ESPS 2, ESPIRIT OthersOthers
• Cilostazol- CASISP ,CSPSII ,Asian patients
• Trifusil Europe ,Latin America
• Others – Ticlopidine , Ticregalor
• ACCP recommend Antiplatlet sec prevention, level I evidence• Combination A+C 3 months ( MATCH ,SAMMPRIS)
A+C 21 days dual , mono agent(CHANCE)
58 IST,CAST, Group .LANCET 1997;349:1569-164159.Jamary Filho et al Up To Date ; Mar 2017

Life style
Modifications
• Smoking
– incremental to #
– back to base line around 3-5 yrs– back to base line around 3-5 yrs
• ETOH – J shaped
• High Salt intake- lobbying manufactures/Govt
• Weight reduction ….
• Moderate Exercise x 3 /week




Haemorrhagic
Time is Brain
• Same urgency !!
• Prognosis
– Volume
– GCS
• Expansion
– first 4-6 hrs by 40%
(in 1/3rd of patients)
– next 18 hrs 15%– GCS
• Treatment
– Medical
– Surgical: Posterior Circulation , Complications
– next 18 hrs 15%
– after 48-72hrs <5%


ICH Hematoma expansion& MortalityICH Hematoma expansion& Mortality
40%40%
RIS
K O
F H
AE
MA
TO
MA
EX
PA
NS
ION
RIS
K O
F H
AE
MA
TO
MA
EX
PA
NS
ION
60mls vol 60% mortality
TTIMEIME FFROMROM OONSETNSET
00--5 hours5 hours 66--24 hours24 hours 2 weeks2 weeks 1 year1 year
10%10%
5%5%
1%1%
RIS
K O
F H
AE
MA
TO
MA
EX
PA
NS
ION
RIS
K O
F H
AE
MA
TO
MA
EX
PA
NS
ION
65 J 65 J NeurosurgNeurosurg 1994 Jan;80(1):511994 Jan;80(1):51--7 . 7 . 66 66 CerebrovascCerebrovasc Dis 1999 MarDis 1999 Mar--Apr;9(2):102Apr;9(2):102--8 . 8 .


Post Stroke
cognitive impairment
• Issues :
�Detection tools- accurate??meaningful
�Quantification- MMSE , MoCA ,RUDAS ,ACERQuantification- MMSE , MoCA ,RUDAS ,ACER
�How best to treat??
• Serial measurements ,longitudinal follow up ,
team work .. support Pt, family, safety net
• Signals.. treatment helps/works – BP lowering

Post Stroke depression
• Prevalence ~ 30% - methodological issues 68
• Predictors – stroke severity, disability, pre-stroke depression,
cognitive impairment, anxiety69,70
• Prognosis- correlated with poorer functional outcomes 70/
perhaps mortality 71perhaps mortality 71
• Remission assoc. with better functional outcomes72
• Screening - Depression scales vs single question “Do you often
feel sad or depressed?” 86% sensitivity,78% specificity73
68. Ayerbe L et al Br J Psychiatry 2013; 202:14
69.Ng KC et al Acta Psychiatr Scand 1995; 92:75-79
70.Nys GM et al J Neurol Sci. 2005;228:27-33
71.Towfighi A et al Stroke 2017; 48:e30
72.Chemerinski E Stroke 2001;32:113
73.Watkins C BMJ 2001;323:1159

Post Stroke
Depression
• Treatment - effectiveness 74
� Pharmacotherapy
� Psychotherapy
� Combination not established - but mounting evidence that
interventions are beneficial 75interventions are beneficial 75
� No definite evidence to guide specific choice of therapy 74
• Prevention – no clear benefit 76
• Treatable illness –structured, monitoring F/U74
74.Towfighi A et al Stroke 2017; 48:e30
75.Hackett ML Cochrane Sys Rev 2008; CD003437
76.Hackett ML Cochrane Sys Rev 2008 CD003689
Post Stroke Fatigue
• Exists…Problematic
• Emerging evidence
• Str &metabolic changes at level of skeletal muscle77
� Atrophy
� Alteration in myosin expression� Alteration in myosin expression
� Chronic inflammatory signalling..oxidative damage
� Progressive wasting, impairment
• Resistance training
� reducing limitations
� long term gain persists 78
77. Hafer –Macko et al J Rehabil Res Dev 2008;45:261
78. Wist S et al Ann Phys Rehabil Med 2016; 59:114

Post Stroke
Sexual dysfunction• Moderate/complete dissatisfaction ~ 50% 79,80
• Changes in sexual function - physical/psychological 81
� Fear of stroke recurrence
� Fear of impotence
� Fear of medication effects� Fear of medication effects
� Physical disability
� Sensory deficits
� Cognitive deficits
• Treatment- as normal pop,…incontinence , CVS status
79.Korpelainen JT et al Acta Neurol Scand 1998; 98:400
80. Korpelainen JT et al Stroke 1999; 30: 715
81.Marinkovic et al J Urol 1996; 165:1748
When to refer??
� High risk TIA,
� ABCD2>4, crescendo, longer lasting
� All strokes- urgent!!
� When in doubt� When in doubt
� Multiple co morbidities

“Action is salvation”
Acute Phase Treatment- rTPA, PSI,Surgery- Antiplatelet ,DAP- Comprehensive Stroke unit,HASU,ASU…
Risk Factors
StrokeTIA ResidualDeficitX X X X X X
Primary Prevention
SecondaryPrevention
unit,HASU,ASU…
Updates
• TAP - no role
• PSI- 24 hrs
• MISTIE trial
• Neuroprotection- resurgence• Neuroprotection- resurgence
• Trials in the grey zone !!
• ECASS IV
• STICH III
• New Thrombolysis agent Tenectaplase

Thank you
• Questions???
• Doubts??
• Collaboration suggestions??