central iowa healthcare - … · warrant the intervention within their scope of ... abdominal pain...
TRANSCRIPT

CENTRAL IOWA HEALTHCARE
Marshalltown, IA
EMERGENCY DEPARTMENT POLICY & PROCEDURES
Policy Number P-17
Subject: Triage Protocol
Purpose: To provide a pathway of timely, coordinated care for patients with urgent/emergent symptoms, determined
through assessment by an Registered Nurse (RN) that correspond to a specific triage protocol delegated by a
medical provider to reduce delays in medical treatment and care.
Policy: The Emergency Department (ED) RN will initiate the triage protocols if the patient assessment findings
warrant the intervention within their scope of competency and licensure. Protocols are complaint specific and
were developed to be within the critical thinking skill set of a bedside emergency room RN.
Procedures: Patient presents to the ED with specific symptoms that align with the current ED triage protocols, the RN
assessment confirmation of symptom(s) or condition that warrants initiation of protocols, then RN initiates
corresponding protocol(s) and consults with ED provider if additional clarification as needed.
Additional information:
The following triage protocols are applicable to all adult/pediatric patients experiencing the following
symptom(s) and/or condition(s):
Abdominal pain
Behavioral Health
Chest pain Adult
Diarrhea
Dyspnea
Pediatric Asthma
Dysuria
Eye problems
Fever
Flank pain
Flu-like symptoms
GI Bleeding
Laceration
Medical Imaging
Musculoskeletal pain
Nausea & vomiting
Seizure
Sepsis
Shortness of breath
Sore Throat
Stroke-like symptoms/Altered Mental Status
Syncope/Near Syncope (Fainting)
Vaginal bleeding
Nebulizer Treatment
Pediatric Fever
Allergic Reaction

Diabetic Emergency
Fever Adult
Neutropenic Fever
Pneumonia
Trauma-Minor
Trauma-Major
Pediatric-Simple Fever
Originated by: Emergency Department
Effective date: 6/15
Authorized by: ________________________________________________________
ER Medical Staff Director Date
________________________________________________________
Administration Date
Revision date: 10/15
Review date:
Appendix: Appendix A: Emergency Department Triage Protocols
Appendix B: Asthma Respiratory Severity Score
Appendix C: Oral Rehydration Therapy Guidelines

Appendix A:
Abdominal Pain
Nursing Saline Lock IV
DIET NPO (except medications) NPO (including medications)
Laboratory CBC w/Diff UA
CMP
Epigastric or RUQ Pain and age > 12 Add:
Lipase Serum
With Jaundice and/or on Warfarin Add:
PT(includes INR)
If Female of Menstruating Age and No Hysterectomy Add:
HCG Quant, Serum
Possible Cardiac Component or Upper Abdominal Pain > 40 years old, Add:
Troponin I Assay STAT EKG
MEDICATIONS (for patients > 12 years of age)
Zofran 4mg IVP x 1 PRN nausea
Or Zofran 4 mg ODT x 1 PRN nausea
GI cocktail PO x1 PRN upper abd pain
Behavioral Health
LABORATORY CBC CMP UDS ETOH TSH Acetaminophen Level Salicylates Level Urinalysis
SOCIAL WORK Consult Social Services
ABG’s
LABORATORY ABGs
Arterial Puncture

Chest Pain Adult
NURSING Suspect Cardiac Origin: Saline Lock IV (Antecubital)
Cardiac Monitoring Oximeter Continuous Oxygen- 2L /min Nasal Cannula titrate to keep O2 Sat > 92% Nurse Communication: Obtain old records including any EKG’s
DIET NPO (except medications) NPO (including medications)
LABORATORY CBC w/Diff
CMP Troponin I Assay
If on Warfarin Add: PT(includes INR) DIAGNOSTIC TESTING EKG (within 10 minutes of arrival) (To EDP STAT after completion) MEDICAL IMAGING Chest Single View Adult Portable
MEDICATIONS Aspirin initial 324 mg. PO chew tab x1 NGT 0.4 mg SL x3 PRN chest pain (Notify EDP if CP not relieved with 3 doses) (HOLD if SPB <90) Morphine 2mg IVP PRN chest pain up to 10 mg
Diarrhea
Nursing Saline Lock IV
LABORATORY Elderly Patients with Orthostatic Changes, or Any Patient with Suspected Volume Deficit:
CBC w/Diff CMP Nurse Communication: Collect & save stool specimen if possible UA Urine Culture (UR Culture Urine) if indicated
Nebulizer Treatments
MEDICATIONS Albuterol 1UD x 1 Atrovent 1UD x 1 Duoneb 1UD x 1 Pulmicort 0.25mg x 1 or 0.5mg x 1 Racemic epi 1UD x 1 Xopenex 0.31mg x 1 0.63mg x 1 1.25mg x 1
Nursing Nebulizer Treatment
1UD = 1 Unit Dose

Dyspnea
NURSING RNs may use their clinical judgment to initiate an SVN (small volume nebulizer) based on signs and symptoms including:
-Dyspnea and/or wheezing - Oxygen saturation <90% -Oximeter Continuous -Oxygen-2L/min NC, titrate to keep O2 Sat >90% (or Pediaflow for infants, titrate to > 92% SPO2)
For patients ages 1 year- 17 years old, RNs may initiate the ED Pediatric Asthma protocol based on an Asthma Respiratory Severity Score (RSS) as applicable
Call / request Respiratory to respond
RT Suction- age appropriate suction bulb or BBG nasal aspirator (Reserve deep suction for airway obstruction causing significant respiratory compromise)
RT SVN- Albuterol 2.5 mg SVN, Soln, 1 x ONLY Shortness of Breath or wheezing
RT Peak Flow Measurement 2 times- Perform Peak Expiratory Flow Rate (PEFR) before and after treatment if able (Exception infants and small children)
PEDIATRIC PATIENTS ONLY:
Mild: Barky Cough
MEDICATION
Dexamethasone (Decadron) 0.6mg/kg po, not to exceed 10 mg, 1 x only
Moderate/Severe: Barky Cough with active stridor, retractions at rest, retractions with severe respiratory distress, hypoxia, or cyanosis
If child is under 6 months of age:
RT SVN-Racemic epinephrine 0.3ml of 2.25% solution diluted in 3mL NS SVN, 1x ONLY
Pulmicort 0.25 neb x1 If child is 6 months of age or older:
RT SVN-Racemic epinephrine 0.5mL of 2.25% solution diluted in 3 mL NS SVN, 1x ONLY
Pulmicort 0.25 neb x1 If child is no longer moderate/severe:
Medication Dexamethasone (Decadron) 0.6mg/kg po, not to exceed 10 mg, 1 x ONLY Dexamethasone (Decadron) 0.6mg/kg IM, not to exceed 10 mg, 1 x ONLY. For use only if patient vomits oral dose.
Document patient assessment and notify provider as soon as possible after treatment has begun
Repeated SVNs are given only after the provider has been consulted or per ED Pediatric Asthma protocol

Pediatric Respiratory Distress
FIRST HOUR OF TREATMENT IN ED
Patients with a respiratory severity score 1-5: MEDICATION
RT-Duoneb (Albuterol 2.5 mg/0.5 ml and ipratropium 500 mcg in 3 ml solution)
Consult with provider prior to administering: Prednisolone 1 mg/kg PO once
Consult with provider prior to administering: Repeat Albuterol 2.5 mg/0.5 ml nebulized
Patients with a respiratory severity score 6-12: MEDICATION
RT-Duoneb treatment (Albuterol 2.5 mg/0.5 ml and ipratropium 500 mcg in 3 ml solution) then consult provider for further treatment
Titrate oxygen to keep SPO2 > 92%
Consult with provider prior to administering: Prednisolone 1 mg/kg PO once SECOND HOUR OF TREATMENT IN ED Patients with a respiratory severity score 1-4:
NURSING
Prepare for discharge
If a patient just received continuous Albuterol they should be observed for a minimum of 1 hour and rescored Patients with a respiratory severity score 5-8:
NURSING Observe for 1 hour and rescore after medication administered and report to ED Provider
MEDICATION
RT -Albuterol MDI 8 puffs
Patients with a respiratory severity score 9-12:
MEDICATION
RT-Duoneb treatment (Albuterol 2.5 mg/0.5 ml and ipratropium 500 mcg in 3 ml solution) then consult provider for further treatment
Titrate oxygen to keep SPO2 > 92%
Consider Magnesium sulfate IV 50 mg/kg (max dose 2 grams) x2 for patients not responsive to the 1st
hour of treatment

Dysuria
LABORATORY UA
Urine Culture (UR Culture Urine) if indicated)
If Female of Menstruating Age and No Hysterectomy Add:
HCG Quant, Serum Eye Problems
MEDICATIONS FOR SEVERE PAIN DUE TO POSSIBLE CORNEAL ABRASION OR FOREIGN BODY
CONSIDERATION: Do NOT use topical anesthetic (tetracaine or proparacaine) if there is a possible globe perforation.
tetracaine ophthalmic 3 drops, 1x ONLY
proparacaine ophthalmic 3 drops, 1 x ONLY NURSING
Visual Acuity Evaluation CHEMICAL SPLASH TO THE EYE(s) Check pH, but do not delay irrigation CONSIDERATION: Do NOT use topical anesthetic (tetracaine or proparacaine) if there is a possible globe perforation, if not contraindicated:
tetracaine ophthalmic 3 drops, 1x ONLY
proparacaine ophthalmic 3 drops, 1x ONLY
S-Sol Irrigation Sodium Chloride 1L (S-Solution Irrign NaCl 0.9 1L), use ocular irrigation set NURSING
Visual Acuity Evaluation
Pediatric Fever
Nursing Saline Lock IV
LABORATORY
Toxic appearance: CBC w/Diff
CMP Lactic Acid
Blood Culturex1
UA Nurse Communication: urinalysis – clean catch or catheter
MEDICATION
Consider Acetaminophen when: 1. the child's temperature is 38.0 C or higher 2. The child was under dosed according to weight guidelines 3. Or the last dose was vomited regardless of the time it was given. Consider Ibuprofen when Acetaminophen was given within the last 4 hours and if the child’s temperature to 38.0 C or greater.
14 years and younger:
Acetaminophen 15 mg/kg PO or rectal x1 For children age 6 months to 14 years:
Ibuprofen 10 mg/kg PO x1
If Neonatal Fever:
IV Saline Lock
Straight Catheter Insert NEO UA catheterize
Urine Culture - catheterize Blood Culture x 1

Draw red top to hold
Lidocaine 4% cream (LMX /Ela-max)- apply up to 5 gm to lumbar spine area
PEDIATRIC – SIMPLE FEVER LABS: RSV Influenza Rapid Strep MEDICATIONS: Motrin: 10mg/kg all children > 6 months if no med within 6 hours. Tylenol: 15 mg/kg all children if no med within 4 hours.
Flank Pain
NURSING Saline Lock IV
LABORATORY
CBC w/Diff
Comprehensive Metabolic Panel
UA
Urine Culture (UR Culture Urine) if indicated) If Female of Menstruating Age and No Hysterectomy Add:
HCG Qual, Serum
Flu-like Symptoms
LABORATORY Strep Influenza A/B
GI Bleeding NURSING
Saline Lock IV
LABORATORY
CBC w/Diff
CMP
PT/PTT (include INR)
If Hemodynamically Unstable, add:
Type and Screen
If Chest Pain, see Chest Pain
Musculoskeletal Pain
Nurse Communication: Provider comfort measures i.e. Ice, pillow, elevation and consult MD for pain medication
MEDICATION
For patients under 18 years old presenting with pain associated with minor closed head injury and/or musculoskeletal injury Consider Ibuprofen for pain when child is over 6-months-of-age: 1. If the child was not already given ibuprofen Consider acetaminophen for pain if: 1. Ibuprofen was given within the last 6 hours, 2. the child is allergic to ibuprofen, 3. The child is under 6-months-of age
Ibuprofen 10mg/kg PO, not to exceed 800mg, 1 x ONLY Acetaminophen 15mg/kg PO, not to exceed 1000mg, 1 x ONLY

Allergic Reaction
LABORATORY CBC with Diff BMP
Nursing Cardiac Monitor Pulse Oximeter Oxygen Nebulizer Treatment
Medications IV Saline Lock 0.3ml/1:1000 Epinephrine IM x 1 Xopenex Benadryl PO 50mg x 1 0.31mg x 1 nebulizer Benadryl IM 50mg x 1 0.63mg x 1 nebulizer Benadryl IV 25mg x 1 1.25mg x 1 nebulizer Pepcid IV 20 mg IV x 1 0.3ml/1:1000 Epinephrine SQ x 1
Diabetic Emergency
LABORATORY CBC with Diff CMP
Nursing Accucheck – Glucose Diet Medications IV Saline Lock IV NS TKO D50 IV 1 AMP
Fever Adult
LABORATORY CBC with Diff CMP UA Urine Culture Blood Culture Flu Strep
Medical Imaging X-Ray Medications Tylenol 650mg or 1000mg PO/PR
Ibuprofen 400mg PO IV NS TKO
Neutropenic Fever

LABORATORY CBC with Diff CMP Lactate Blood Culture Urine Culture UA
Medical Imaging X-ray Nursing IV Saline Lock Tylenol 1000mg PO/PR Motrin 400mg PO
Pneumonia
LABORATORY CBC with Diff CMP UA Urine Culture Blood Culture CRP – quant Lactate
Medical Imaging X-Ray Nursing IV Saline Lock
IV NS TKO Tylenol 650mg or 1000mg PO/PR Ibuprofen 400mg PO
Trauma-Minor
Medical Imaging: X-Ray Nursing ICU
Elevate Suture Set-Up
Medication Adacel IM 0.5ml IM x 1
Trauma-Major LABORATORY CBC with Diff
CMP PT/PTT ETOH Pregnancy Qualitative Pregnancy Quantitative Urine Drug Screen UA Blood Bank Lactate Lipase

Medical Imaging X-ray Ultrasound CT Scan
Nursing Cardiac Monitor Pulse Oximeter NPO Oxygen C-Collar NG Tube Foley Catheter Chest Tube Set Up
Medication: IV NS with Bolus IV #2 NS IV RL Zofran IV 4mg x 1, may repeat x 1 for total of 8mg Fentanyl IV Adacel 0.5ml IM x 1
Nausea and Vomiting
Nursing Saline Lock IV For pediatric patients greater than 6 months old, may start Oral Rehydration Therapy (ORT) per protocol as applicable
LABORATORY UA
CMP CBC w/Diff
If Female of Menstruating Age and No Hysterectomy Add: HCG Quant, Serum
MEDICATIONS 2 mg for weight from 8 to 16 kg 4 mg for weight >16 kg
Ondansetron (Zofran®) mg PO ODT (Disintegrating) Tablet or liquid now
If Abdominal pain follow Abdominal pain care set
Seizure
NURSING Saline Lock IV Nurse Communication, place seizure pads around patient. Telemetry
LABORATORY
Glucose Point-of-Care (Finger-Stick Glucose)
With Prior Seizure History and On One Of These Medications Add: Carbamazepine (Tegretol) Level Dilantin Level
Valproic Acid (Depakane) Level Phenobarbitol Level
If Fever or Obtunded Add:
UA
Urine Culture (UR Culture Urine) if indicated CBC w/Diff CMP
If Female of Menstruating Age and No Hysterectomy Add:
HCG Quant, Serum

Sepsis Patients who present with at least 2 of the following: □ Temperature < 36 or > 38 ⁰ C □ HR > 90 □ Respirations > 20
AND SBP < 90 AND at least one of the following risk factors: □ Diabetic □ Indwelling Catheters □ Immunosuppressed □ Transfer for SNF □ Decreased LOC □ Age > 50
NURSING Saline Lock IV x2 Cardiac Monitoring
Oximeter Continuous Oxygen- 2L /min Nasal Cannula titrate to keep O2 Sat > 90%
LABORATORY CBC w/Diff
CMP
Lactic Acid Blood Culturex2 UA Urine Culture
MEDICATIONS Normal Saline 2 liter bolus x1 Acetaminophen 15mg/kg PO, not to exceed 1000mg, 1 x ONLY Ibuprofen 10mg/kg PO, not to exceed 800mg, 1 x ONLY MEDICAL IMAGING Portable Chest X-Ray
Shortness of Breath
Does Not Apply to Uncomplicated Asthma in a Young Patient, see Dyspnea
NURSING Saline Lock IV
Oximeter Continuous Oxygen- 2L /min Nasal Cannula titrate to keep O2 Sat > 90%
LABORATORY CBC w/Diff
CMP
If Cardiac Origin Add: BNP Troponin I Assay
DIAGNOSTIC TESTING EKG
MEDICAL IMAGING Chest Single View Adult Portable
Chest PA + Lat
Sore Throat
LABORATORY Strep

Stroke-like Symptoms/Altered Mental Status (Facial droop, arm drift, abnormal speech, etc.) NURSING Saline Lock IV
Oximeter Continuous Continuous Cardiac Monitoring Oxygen- 2L /min Nasal Cannula titrate to keep O2 Sat > 90% AccuCheck
DIET NPO (except medications)
NPO (including medications)
Laboratory CBC w/Diff UA
CMP PT/PTT
Glucose Point-of-Care (Finger-Stick Glucose)
DIAGNOSTIC TESTING EKG Head CT non-contrast (To be determined after EDP evaluates)
Syncope/Near Syncope (Fainting)
NURSING Notify Physician if Hemodynamically unstable Continuous cardiac monitoring Orthostatic vitals Saline Lock IV AccuCheck
LABORATORY Draw Extra Tubes for Possible Cardiac Enzymes, PT, INR, PTT, Toxicology Studies, Type and Screen
CBC w/Diff CMP UA
If Female of Menstruating Age and No Hysterectomy Add:
HCG Quant, Serum Apply Blood Band ID to Specimens
DIAGNOSTIC TESTING EKG
Vaginal Bleeding
LABORATORY UA
CBC w/Diff
If Female of Menstruating Age and No Hysterectomy Add:
HCG Qualitative, Serum
If Patient Reports a Positive Pregnancy Test or has a Positive Pregnancy Test Add:
Type and Rh HCG Quant, Serum
If on Warfarin Add: PT(includes INR)
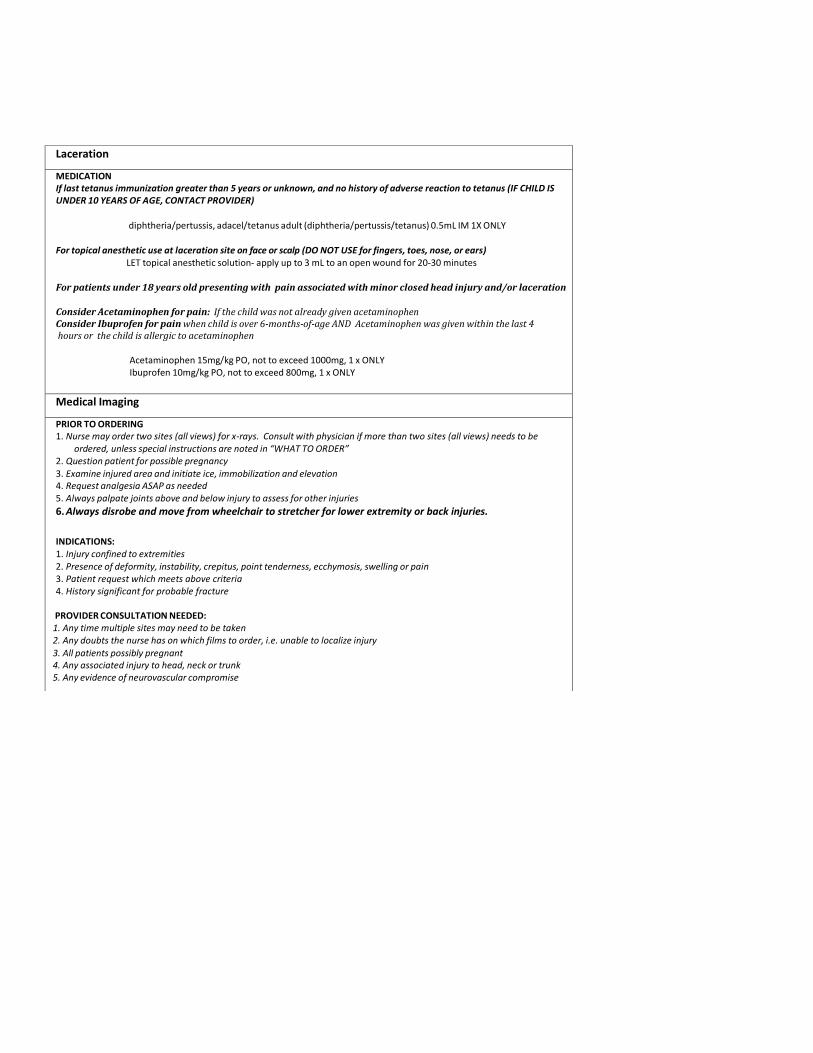
Laceration
MEDICATION If last tetanus immunization greater than 5 years or unknown, and no history of adverse reaction to tetanus (IF CHILD IS UNDER 10 YEARS OF AGE, CONTACT PROVIDER)
diphtheria/pertussis, adacel/tetanus adult (diphtheria/pertussis/tetanus) 0.5mL IM 1X ONLY
For topical anesthetic use at laceration site on face or scalp (DO NOT USE for fingers, toes, nose, or ears)
LET topical anesthetic solution- apply up to 3 mL to an open wound for 20-30 minutes
For patients under 18 years old presenting with pain associated with minor closed head injury and/or laceration Consider Acetaminophen for pain: If the child was not already given acetaminophen Consider Ibuprofen for pain when child is over 6-months-of-age AND Acetaminophen was given within the last 4 hours or the child is allergic to acetaminophen
Acetaminophen 15mg/kg PO, not to exceed 1000mg, 1 x ONLY Ibuprofen 10mg/kg PO, not to exceed 800mg, 1 x ONLY
Medical Imaging
PRIOR TO ORDERING 1. Nurse may order two sites (all views) for x-rays. Consult with physician if more than two sites (all views) needs to be
ordered, unless special instructions are noted in “WHAT TO ORDER” 2. Question patient for possible pregnancy
3. Examine injured area and initiate ice, immobilization and elevation 4. Request analgesia ASAP as needed 5. Always palpate joints above and below injury to assess for other injuries
6. Always disrobe and move from wheelchair to stretcher for lower extremity or back injuries.
INDICATIONS: 1. Injury confined to extremities 2. Presence of deformity, instability, crepitus, point tenderness, ecchymosis, swelling or pain 3. Patient request which meets above criteria 4. History significant for probable fracture
PROVIDER CONSULTATION NEEDED: 1. Any time multiple sites may need to be taken 2. Any doubts the nurse has on which films to order, i.e. unable to localize injury
3. All patients possibly pregnant 4. Any associated injury to head, neck or trunk 5. Any evidence of neurovascular compromise

WHAT TO ORDER "Heard a pop", inversion or eversion ankle injury; swelling at malleoli. Palpate fifth metatarsal and if pain present, order a foot x-ray also. Ankle film does not visualize the metatarsals well.
Ankle 3 Or More Views Lt Ankle 3 Or More Views Rt
Post traumatic pain if associated with decrease or loss of supination, pronation, flexion or extension. ** In a child of 5 years or less with unexplained loss of arm function and no apparent soft tissue swelling, a radial head subluxation must be considered and x-rays should not be obtained prior to physician evaluation.
Elbow 3 Or More Views Lt Elbow 3 Or More Views Rt
If swelling or pain on top of foot.
Foot 3 Or More Views Lt Foot 3 Or More Views Rt
Clear hand injury distal to wrist
Hand 3 Or More views Lt Hand 3 Or More Views Rt
Order special calcaneal films if fracture suspected
Calcaneus [Heel] Lt Calcaneus [Heel] Rt
1. Inability to stand or walk with localized knee pain 2. Post traumatic joint effusion 3. A fall or blow to the knee/patellar area with subsequent inability to flex or extend the knee fully. If pain over patellar
area, add order for sunrise (patellar) view
Knee 23 View Lt Knee 23 View Rt
Tenderness above the shoulder or on top of the shoulder; may or may not have swelling/deformity.
Shoulder 2 Or More Views Lt Shoulder 2 Or More Views Rt
1. Fall on an outstretched hand with swelling and tenderness to the wrist
2. If snuffbox tenderness, a comment of "navicular view" in the order comments.
Wrist 3 Or More Views Lt Wrist 3 Or More Views Rt
Post traumatic pain in hip area if associated with rotated and shortened leg
Hip 2 Or More Views Lt Hip 2 Or More Views Rt Pelvis 1 or more views
Post traumatic pain in thigh area with swelling or pain to thigh area
Femur 2 Or More Views Lt Femur 2 Or More Views Rt
Pain, Swelling, or deformity to affected joint: Tibia/fibula 2 views Lt Tibia/fibula 2 views Rt
Formatted: Indent: Left: 0.31"
Formatted: Indent: Left: 0.56"
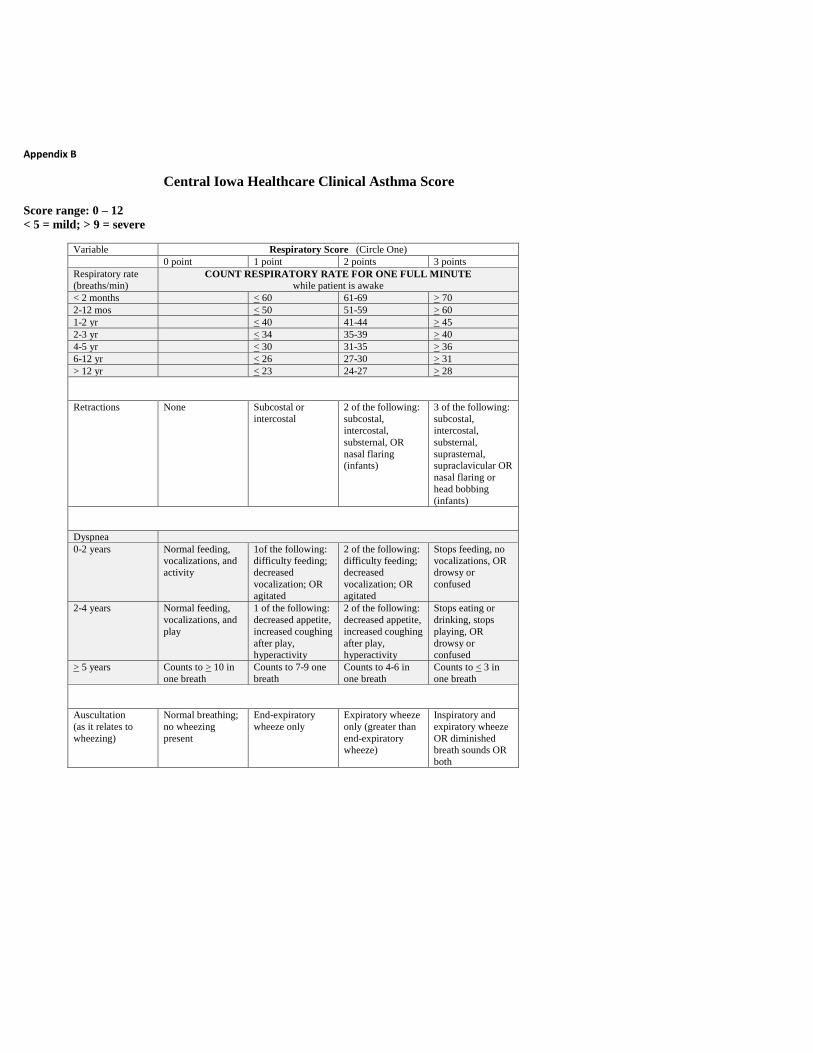
Appendix B
Central Iowa Healthcare Clinical Asthma Score
Score range: 0 – 12
< 5 = mild; > 9 = severe
Variable Respiratory Score (Circle One)
0 point 1 point 2 points 3 points
Respiratory rate
(breaths/min)
COUNT RESPIRATORY RATE FOR ONE FULL MINUTE
while patient is awake
< 2 months < 60 61-69 > 70
2-12 mos < 50 51-59 > 60
1-2 yr < 40 41-44 > 45
2-3 yr < 34 35-39 > 40
4-5 yr < 30 31-35 > 36
6-12 yr < 26 27-30 > 31
> 12 yr < 23 24-27 > 28
Retractions None Subcostal or
intercostal
2 of the following:
subcostal,
intercostal,
substernal, OR
nasal flaring
(infants)
3 of the following:
subcostal,
intercostal,
substernal,
suprasternal,
supraclavicular OR
nasal flaring or
head bobbing
(infants)
Dyspnea
0-2 years Normal feeding,
vocalizations, and
activity
1of the following:
difficulty feeding;
decreased
vocalization; OR
agitated
2 of the following:
difficulty feeding;
decreased
vocalization; OR
agitated
Stops feeding, no
vocalizations, OR
drowsy or
confused
2-4 years Normal feeding,
vocalizations, and
play
1 of the following:
decreased appetite,
increased coughing
after play,
hyperactivity
2 of the following:
decreased appetite,
increased coughing
after play,
hyperactivity
Stops eating or
drinking, stops
playing, OR
drowsy or
confused
> 5 years Counts to > 10 in
one breath
Counts to 7-9 one
breath
Counts to 4-6 in
one breath
Counts to < 3 in
one breath
Auscultation
(as it relates to
wheezing)
Normal breathing;
no wheezing
present
End-expiratory
wheeze only
Expiratory wheeze
only (greater than
end-expiratory
wheeze)
Inspiratory and
expiratory wheeze
OR diminished
breath sounds OR
both

Appendix C
Dehydration/Oral Rehydration Clinical Practice Guidelines This guideline has been developed to ensure proper rehydration in patients 1 to 60 months of age with acute gastroenteritis (diarrheal illness of rapid onset with or without nausea, vomiting, fever, abdominal pain) and with no other diagnosed disorders. The guideline is not to be used in patients with diarrhea for over 10 days, diarrhea associated failure to thrive, or vomiting without diarrhea. The recommendation to withhold antibiotics should be modified if a protozoal illness is suspected or if dysenteric signs and symptoms (fever, bloody stool, pus in stool) are present. Contra-indications to oral rehydration are outlined on page 2. Please direct questions to Dr. Lance VanGundy at 641-754-5040.
EVALUATION OF DEHYDRATION The most accurate way to estimate dehydration is to compare a recent weight (when the patient was well) and the current weight. Clinical parameters to assess hydration status are outlined below. The appropriate method of rehydration depends on the percent dehydration.
Mild (3-5%) Moderate (6-9%) Severe (>10%) General Alert Restless, Irritable Lethargic/unconscious Blood Pressure Normal Normal Normal, decreased Quality of Pulse Normal Normal, slightly decreased Moderately decreased Heart Rate Normal Increased Increased Skin Turgor Normal Decreased Decreased Fontanelle Normal Sunken Sunken Mucus Membranes Slightly dry Dry Dry Eyes Normal Sunken Deeply sunken Extremities Warm, normal cap refill Delayed cap refill Cool, mottled Urine Output Slightly decreased < 1 ml/kg/hr << 1 ml/kg/hr Thirst Slightly Increased Moderately increased Increased/Decreased
ORAL REYDRATION THERAPY (ORT) is appropriate for patients with mild and moderate dehydration. Compared to IV rehydration, ORT is safer, less costly, and able to be administered in various clinical settings.
Oral rehydration solutions (ORS) should contain 45-90 mmol/L of sodium and 74-140 mmol/L of glucose. Acceptable, commercially available ORS include: Naturalyte, Pedialyte, Infalyte, Rehydralyte, WHO Oral Rehydration Salts, and Pediatric Electrolytes. Cereal-based ORS is also available and has been shown to decrease diarrhea by 20-30% compared to glucose-containing ORS. Rehydralyte is the most appropriate ORS that is easily available.
Fluid replacement should be accomplished over 3-4 hours; additionally, 10 ml/kg for each episode of vomiting or watery stool will prevent further dehydration. For patients who are vomiting, 5 ml of ORS every 1-2 minutes should be attempted. For patients who refuse to take ORS orally or who continue to vomit, continuous nasogatric tube (NGT) rehydration should be considered.
Less than 3% dehydration (determined by weight or estimation): Encourage PO liquids and solids. Milk products and breastfeeding should be continued. There is little indication for ORS. Close monitoring for worsening dehydration is recommended and ORS to replace ongoing losses may be recommended (10ml/kg for each episode of vomiting or watery diarrhea).
MILD = 3-5% dehydration (determined by weight or estimation): Use ORS (orally or by NGT) to replace 50 ml/kg (or the exact losses if known by weight change) plus ongoing losses (10 ml/kg for each episode of vomiting or watery diarrhea) over 4 hours. Reevaluate every 2 hours. Begin age-appropriate diet after rehydration is accomplished. Continue to replace ongoing losses with ORS (10ml/kg for each episode of vomiting or watery diarrhea).
MODERATE = 6-9% dehydration (determined by weight or estimation): Use ORS (orally or by NGT) to replace 100 ml/kg (or the exact losses if known by weight change) plus ongoing losses (10 ml/kg for each episode of vomiting or watery diarrhea) over 4 hours. Reevaluate every hour. Begin age-appropriate diet after rehydration is accomplished. Continue to replace ongoing losses with ORS (10ml/kg for each episode of vomiting or watery diarrhea).
SEVERE = Over 9% dehydration (determined by weight or estimation): Arrange hospital admission, initiate IV fluids (20ml/kg lactated Ringer’s or normal saline), order appropriate laboratory studies, and begin ORT when patient is stable and improved. Age-appropriate feedings may be resumed after rehydration is accomplished.

EARLY REFEEDING is recommended. Patients who are not dehydrated may continue their typical age- appropriate diet. Dehydrated patients may resume their typical age-appropriate diet after being rehydrated. Most patients tolerate lactose-containing milk/formula safely. If a patient has worsening diarrhea with the resumption of lactose-containing products, consider checking stool for pH and reducing substances and instituting a lactose-free diet for 2 weeks. Breastfeeding should be continued during acute diarrheal illnesses. Foods that are well tolerated include: rice, wheat, potatoes, bread, cereal, lean meat, fruit, yogurt, vegetables. Poorly tolerated foods include: fatty foods, food or drinks high in simple sugars (juice, soft drinks/soda).
TYPICAL COURSE: The usual course of a diarrheal illness includes one to two days of fever and vomiting, followed by three to four days of diarrhea. Even severely dehydrated children are willing to attempt PO intake on the second or third day of illness. Discharge criteria from an in-patient hospital stay should include rehydration accomplished, oral intake of fluids adequate to maintain hydration status and follow-up arranged. For patients rehydrated in the ED or out-patient setting, follow-up should include: a phone call by the primary care provider the following day for cases of mild dehydration or a phone call the same day and an office visit the following day for moderate dehydration.
HYPERNATREMIC DEHYDRATION is dehydration associated with serum sodium over 150 mEq/L. It is associated with a doughy feeling of the skin and mental status changes. Patients with hypernatremic dehydration can be safely rehydrated orally. However, if the patient requires IV rehydration, the sodium deficit should be replaced slowly (over 48 hours) to prevent CNS complications. Frequent serum sodium levels are indicated.
SERUM ELECTROLYTES are helpful in patients with: signs and symptoms of hypernatremic dehydration, severe dehydration, or a history/physical exam that is inconsistent with straightforward acute gastroenteritis. STOOL STUDIES may be considered based on the clinical situation; C. diff toxin, culture, WBC, O&P, Giardia antigen may be considered but are not recommended if a virus is the most obvious source. Rotavirus antigen testing is rarely required, except for epidemiology studies and cohorting purposes.
CONTRA-INDICATIONS TO ORAL REHYDRATION AND ADMISSION CRITERIA Over 9% dehydrated (determined by weight or estimation) Signs of shock Ileus or intestinal obstruction (proven or suspected) Comatose or unconscious Unable to tolerate ORT/NGT rehydration (persistent vomiting) Unclear diagnosis Significant psychosocial situation
ANTI-DIARRHEAL THERAPIES are not recommended. ANTI-EMETIC THERAPIES are not routinely recommended; however, studies have demonstrated short-term benefits with PO or IV ONDANSETRON.
ANTIBIOTICS are not typically recommended for acute gastroenteritis except for patients with a proven or highly suspicious diagnosis of a parasite/Giardia or patients with dysentery and the following: less than 6 months of age, systemic illness, proven or high suspicion of Shigella.
REFERENCES
1. American Academy of Pediatrics. Practice parameter: the management of acute gastroenteritis in young
children. Pediatrics 1996;97:424-35. 2. Burkhart DM. Management of acute gastroenteritis in children. American Family Physician 1999;60:2555-66. 3. Nager AL, Wang VJ. Comparison of nasogastric and intravenous methods of rehydration in pediatric patients with
acute dehydration. Pediatrics 2002;109:566-72. 4. Ramsook C, Sahagun-Carreon I, Kozinetz CA, Moro-Sutherland D. A randomized clinical trial comparing oral
ondansetron with placebo in children with vomiting from acute gastroenteritis. Annals of Emergency Medicine 2002;39:397-403.
5. Sandhu BK. Practical guidelines for the management of gastroenteritis in children. Journal of Pediatric Gastroenterology and Nutrition 2001;33:S36-9.
Algorithms are not intended to replace providers’ clinical judgment or to establish a single protocol. Some clinical problems may not be adequately addressed in this guideline. As always, clinicians are urged to document management strategies. Last revised March 2005 by The Barbara Bush Children’s Hospital at Maine Medical Center.