cellular analysis of aspiration lung …jcp.bmj.com/content/jclinpath/2/1/49.full.pdfcellular...
TRANSCRIPT

1. clin. Path. (1949), 2, 49.
CELLULAR ANALYSIS OF THE ASPIRATION LUNGBIOPSY FROM NORMAL AND SOME
PATHOLOGICAL CONDITIONSBY
Z. Z. GODLOWSKIFrom the Department of Pathology, Edinburgh University, and
the Polish Unit at the Ballochmyle Hospital, Ayrshire
(RECEIVED FOR PUBLICATION, NOVEMBER 24, 1948)
In a previous report (Godlowski, 1948) spec'alattention was drawn to the obscure role which theeosinophils played in allergic conditions, in par-ticular in allergic bronchial asthma treated withinsulin hypoglycaemia and adrenaline infusion dur-ing which a peripheral eosinopenia occurred andin both of which the mechanism of the eosinopeniaseemed to be identical. There is on record(Bertelli and others, 1910) certain evidence thatin dogs big doses of adrenaline produce a peri-pheral eosinopenia with local eosinophilia in theliver. Analysis of the bone-marrow in allergicconditions shows no substantial alteration in theeosinophil content (Godlowski, 1948). In order totry to trace the fate of the eosinophilic cells duringthe adrenaline infusion and insulin hypoglycaemiait was decided to do a lung aspiration biopsy,assuming the lung to be the presumptive shockorgan and the place where eosinophils assembleduring the peripheral eosinopenia.
Aspiration lung biopsy has been done by manyclinicians (Stewart, 1930; Sappington and Favorite,1936) for the bacteriological identification of thebacteria causing lung infection, particularly of thepneumococcus in pneumonia for ascertaining theproper serum treatment. In spite of favourablereports given by these and other clinicians whohave used this method and who have stressed itsharmlessness and its great diagnostic value, thismethod is at present not in general use in lungdiagnosis except in cases of lung tumours (Martinand Ellis, 1930; Stewart, 1930; Sappington andFavorite, 1936; Wilson, 1945). Serious objectionsto this method are advanced only by those whohave had inadequate statistical data. Their objec-tions are based mainly on somewhat theoretical
arguments and fear of spreading infection alongthe puncture canal, of injury of the large pulmonaryvessels, and of production of pneumothorax, airembolism, etc. It has been shown, however(Stewart, 1930; Martin and Ellis, 1930; Bullowa,1936), that these complications occur so rarely thatthey need not be regarded as discrediting thismethod of diagnosis in lung diseases. Two thou-sand cases of lobar pneumonia, for example, werecomplicated by empyema in 4.6 per cent of casessubjected to lung biopsy, whereas 1,913 cases oflobar pneumonia without lung aspiration biopsyshowed empyema in 5.1 per cent-that is, the fre-quency of empyema was of the same degree inboth series. Thus the empyema must be consideredas a complication not of the lung aspiration biopsybut of the lobar pneumonia (Sappington andFavorite, 1936).
MethodSeventy-five clinically normal men and women, of
whom fifty were tobacco smokers and twenty-five non-smokers, with negative x-ray reports of the chest, andten cases with various pathological conditions of thelung, were subjected to lung aspiration biopsy. Thefirst twelve were premedicated with 0.02 g. of morphiaand 0.001 g. of atropine sulphate, injected sub-cutaneously thirty minutes before biopsy. Since acertain number of cases, however, responded withtoxic symptoms which upset them more than thebiopsy itself, the premedication was thereafter droppedand attention concentrated on a local anaesthesia, towhich very great importance is attached. The localanaesthesia consisted of 2 per cent solution of pro-caine hydrochloride. An intradermal wheal was madein the first instance and then the tissues of the chestwere gradually infiltrated as deep as the costal and
on 25 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.2.1.49 on 1 February 1949. D
ownloaded from

Z. Z. GODOWSKI
finally visceral pleura and the adjacent parts of thelung tissue itself. Very great importance is attachedto the anaesthesia of the pleura, since the literatureincludes cases in which simple tapping of the pleuracaused so-called vasovagal syncope, leading in some
cases to instantaneous death (Stewart, 1930; Sapping-ton and Favorite, 1936). Local anaesthesia of thepleura can substantially minimize the danger of thevasovagal syncope. Five to ten minutes after theinjection of procaine hydrochloride the patient's chestwas again screened by way of a repeat control. Thesite of the biopsy is of no importance in normal cases;in pathological cases the aspiration biopsy should bedone at the most easily accessible place of the radio-logically discovered pathological alteration; in thepresent series of biopsies it was made in the sixth orseventh intercostal space in the anterior axillary lineof the right lung. Two per cent tincture of iodine wasused for disinfection of the skin.
In most of the cases presented here an ordinarylarge lumbar puncture needle was used for the lungbiopsy. As, however, among the biopsy elementsthere were found cells suspected to be of skin or
,pleural origin, the two-needle method was applied inorder to avoid the inclusion of such cells and to obtaina film of pure lung elements. One short needle oflarge calibre with the stilette in it was pushed throughthe whole cheslt wall and both pleurae, and, as soonas the needle appeared in the lung itself (the wholeprocedure being controlled by radiograph), the stilettewas removed and a second needle much longer andthinner than the first and also with a stilette in it-was passed through the 'first needle. As soon as thesecond needle appeared in the lung the stilette wasremoved and a 20 ml.'syringe was connected to it.By makiing an intense, sharp aspiration the secondneedle was pushed into the lung at times as deep as20 cm. and moved in and out to the tip of the firstneedle several times. During this procedure thepatient must stop breathing in order to avoid lacera-tion of the lung by respiratory movements with subse-quent pneumothorax. The aspiration was stopped atthe point where the second needle on the way outapproached the tip of the first one; the secondneedle was then slowly drawn through the firstone. The content of the second needle was spreadon the glass slide and, if the amount was sufficient, afilm was made of it. The first needle was removedand the place of the puncture dressed. In spite ofthese precautions the lung specimen so obtained in afew cases still contained pleural cells, which meansthat the second needle was contaminated by thematerial adherent to the wall of the first needle. Toavoid any incidental contamination from the skin, anincision was, in a few cases, made in the skin andthe two-needle method used through the wound.After a week a routine x-ray control of the chestwas always made.A biopsy smear obtained in this way was dried for
a period of one to twelve hours at room temperatureand was stained by the Leishman or Jenner-Giemsa
method. Iron haematoxyjin or mucicarmine staininggives very poor differential value and for this reasonis not recommended.The precaution of using the two-needle method in
lung biopsy was necessary only for identification ofcertain cells and exclusion of cellular elements of thepleura and skin. For ordinary diagnostic purposesthe one-needle method is entitely satisfactory if it iskept in mind that the cells described below belong tothe seros'a of the pleura. The detailed descriptionof the one-needle method may be found elsewhere(Martin and Ellis, 1930, 1934).
If the local anaesthesia is well performed themajority of the patients feel only negligible painduring the whole procedure. More sensitive indi-viduals, however, sometimes feel a short stabbing painwhich in one or two cases may persist for a few hours;such pain is not intensive and can easily be allayedby light analgesics. Out of eighty-five normal andpathological men and women in the present series, onehad a slight haemoptysis which ceased after twelvehours. Pneumothorax occurred in 'three: it was small
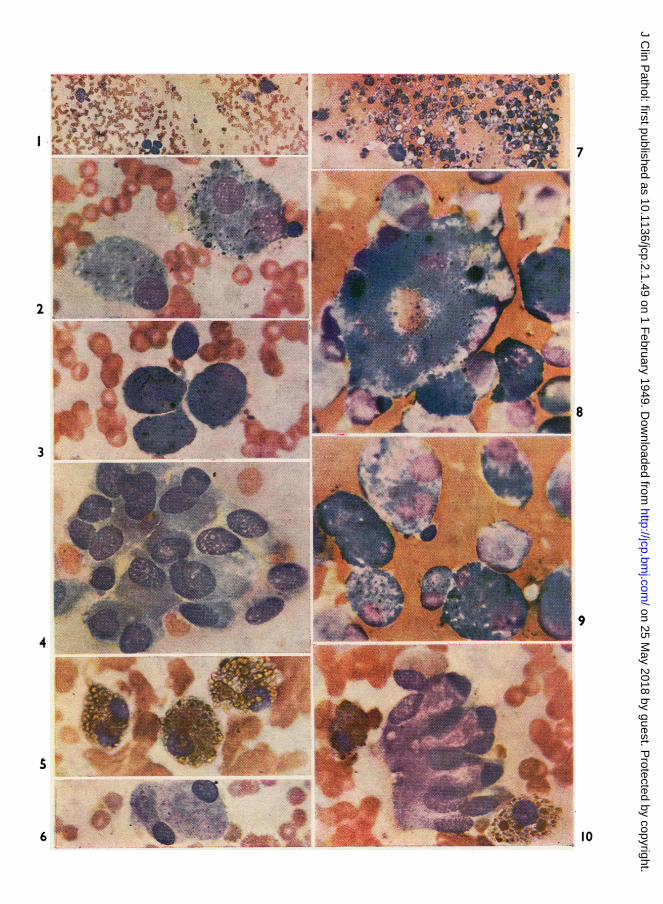
FIG. 1 -Normal pulmogram of a non-smoker show-ing few macrophages (" dust cells "), large cellswith pale-blue cytoplasm, and alveolar histio-cytes with dark-blue cytoplasm; in both type3 ofcells are seen few particles in their cytoplasm.The other cells seen in the film are of the typeseen in the peripheral blood. (Leishman, x 100.)
FIG. 2.-Two macrophages (" dust cells ") fromFig. 1. (x800.)
FIG. 3.-Alveolar histiocytes from Fig. 1. (x 800.)
FIG. 4.-Sheet of nucleated alveolar epithelium froma normal pulmogram; their cytoplasm free fromany particles, there are some vacuoles seen in thecytoplasm. (Leishman, x 800:)
FIG. 5.-Two macrophages loaded with haemosiderin(" heart-failure cells ") from a case with chronicvenous congestion in the lung (mitral stenosis).(Jenner-Giemsa, x 800.)
FIG. 6.-Two mesothelial cells fronr the pleura froma normal pulmogram. (Leishnman, x 800.)
FIG. 7.-Pulmogram of a heavy tobacco-smokershowing very numerous macrophages with pale-blue cytoplasm (" tobacco cells ") and alveolarhistiocytes with dark-blue cytoplasm, both heavilypacked with particles. There is also one giantcell. (Leishman, x 100.)
FIG. 8.-One giant cell surrounded with " tobaccocells " and alveolar histiocytes from the case seenin Fig. 7. (Leishman, x 800.)
FIG. 9.-Tobacco cells and alveolar histiocytes packedwith particles from the film seen in Fig. 7.(Leishman, x 800.)
FIG. 10.-Ciliated epithelium with three gobletelements forming a palisade layer. Also two" heart-failure" cells. From a case of chronicvenous congestion or the lung. (Jenner-Giemsa,x 800.)
50
on 25 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.2.1.49 on 1 February 1949. D
ownloaded from
7
8
9
A
3 *.
If
4
10
A? -.Ai
I
5
.-i4l,We-6
I
.IT%do-Ilk
RIF-M-'.
W0
j
-A
li
.-- --.1I
-A-
:.. IL.-
on 25 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.2.1.49 on 1 February 1949. D
ownloaded from
CELLULAR ANALYSIS OF THE ASPIRATION LUNG BIOPSY
and was discovered only by routine x-ray control;the partly collapsed lung re-expanded totally infourteen days.
Results and DiscussionA pulmogram usually consists of cells derived
from (1) lung tissue, (2) blood aspirated from thepulmonary vessels, and (3) tissues of the thoracicwall and pleura.The identification of some of the pulmonary
elements as regards origin is very difficult andsometimes impossible. Therefore the terminologyused in this paper for the cells concerned is basedonly on the close resemblance of the cells -inpulmogram to the elements described by histolo-gists. Histological terminology is, however, not inthe least unanimous about the nature of the alveo-lar lining or the origin of macrophages.
1. Elements derived from the lung tissue itselfare: (a) macrophages, (b) histiocytes of the alveo-lar lining, (c) nucleated alveolar epithelial cells,(d) "non-nucleated plates," (e) reticulum cells,(f) collagenous and elastic fibres, (g) lymphoidcells, (h) ciliated and non-ciliated epithelium fromthe bronchi and bronchioles.
(a) Macrophages vary greatly in size (15 to 50microns in their longer diameter) and in shape,being round, oval, or irregular. Their cytoplasmwith Leishman or Giemsa staining is pale blue;it may be packed with particles of different origin,shape, and size, or might have only a few granulesor none at all. Their nuclei are round or oval,may be single or multiple, and stain a violetcolour; they contain one or more nucleoli and areabundantly filled with coarse, granular chromatin.Cells with several nuclei and reaching the upperlimits of the dimensions specified above are rarelyseen in normal pulmograms; the cytoplasm of thesevery big cells often contains particles, but by thismethod of staining it is difficult to decide whetherthey include any bacteria. These macrophagesbelong to the class of giant cells (Figs. 7 and 8).The function of the macrophages is phagocytosis,and according to the phagocytized material theyhave acquired different names; if they contain dustor carbon particles they are called " dust cells "(Figs. 1 and 2), or if they include granules ofhaemosiderin derived from ingested red cells pha-gocytosed in chronic venous congestion of the lungthey are called " heart-failure cells " (Figs. 5 and10); they may also be called " tobacco cells " (Fig.9) if they contain partly or totally carbonizedtobacco.The origin of these cells is not conclusively
elucidated; Lang (1925) and Gazayerli (1936) sug-gest that they arise from the " septal cells " by losing
contact with their ground and growing in size.Others suggest an origin from the nucleated alveo-lar epithelium (Cappell, 1923, 1929; Carleton,1927) or from septal pericapillary cells or themononuclear cells of the blood (Foot, 1927).The "dust cells" in a normal pulmogram are
usually irregular in their distribution and are foundmost plentifully at the edges of the film, where theyare suitable for the observation of qualitativealterations only. To get information about quanti-tative changes in the " dust cells " it is advisable tocompare the number found in the middle fields ofthe smear with those on its edges, as is done in adifferential count of the peripheral blood. Apulmogram may be considered normal as regardsquantitative changes when the number of " dustcells" found in one high-power field (an averageof 100 fields) does not exceed three to fivemacrophages. If, however, peripheral blood wereaspirated in large quantities into the syringe, thequantitative estimation would be fallacious.
(b) Histiocytes of the alveolar lining (Fig. 3) aresmaller cells than " dust cells " and more regularin shape, with highly basophilic cytoplasm inwhich are seen particles of different size and shape.The single nucleus is as a rule eccentrally located,oval or round in shape, and densely filled withgranular chromatin.
Gazayerhi (1936) in his experiments on animalsand in human beings found cells with highphagocytic power between the nucleated alveolarepithelium. These occasionally showed mitosisand were regarded by him as capable of beingshed into the lumen of alveoli. Such cells mayresemble those reproduced in Fig. 3.
(c) Nucleated alveolar epithelial cells (Fig. 4)are the cells much smaller than " dust cells," andtheir shape is polygonal if they are in sheets ormore round if isolated. The blue cytoplasm withsmall violet patches is never granular but may befinely vacuolated. The large single nucleus filledwith coarse granules of chromatin is violet andusually contains one or more nucleoli.The lack of any particles in. their cytoplasm in
biopsies in which phagocytes are packed withgranules proves their total inability to act as phago-cytes. The amount of the nucleated alveolarepithelium might in certain normal pulmogramsbe greater than all other elements. Cells of thisnature have been identified as those which line thewalls of the alveoli themselves and are thus partof the interalveolar septum (Gazayerli, 1936;Miller, 1947).
(d) "Non-nucleated plates" (Fig. 11) are verythin structureless plates which are polygonal or
51
on 25 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.2.1.49 on 1 February 1949. D
ownloaded from

Z. Z. GODLOWSKI
TABLEAVERAGE PER CENT VALUES OF DIFFERENTIAL COUNTS MADE FROM CAPILLARY BLOOD AND FROM ASPIRATION
LUNG BIOPSY FROM THIRTEEN NORMAL CASES
Neutrophils:Young Mature j
Eosinophils Basophils MoQlocytes Lymphocytes
CplayCapill a CapillaryCair arill Caplabloo LLLungood Lung Luni{uLup ryi Lung Lungblood blood blood ng blood Lug bloo bld
Differential -- -counts:
%values .. 2.11 2.22 63.08 64.77 2.38 3.15 0.23 0.23 5.69 3.48 27.38 26.85
Standarderror ±1.1 ±1.31 ±10.14 1±7.61 ±1.73 ±2.03 ±0.42 ±0.42 ±2.49 ±2.57 ±9.9 ±9.9
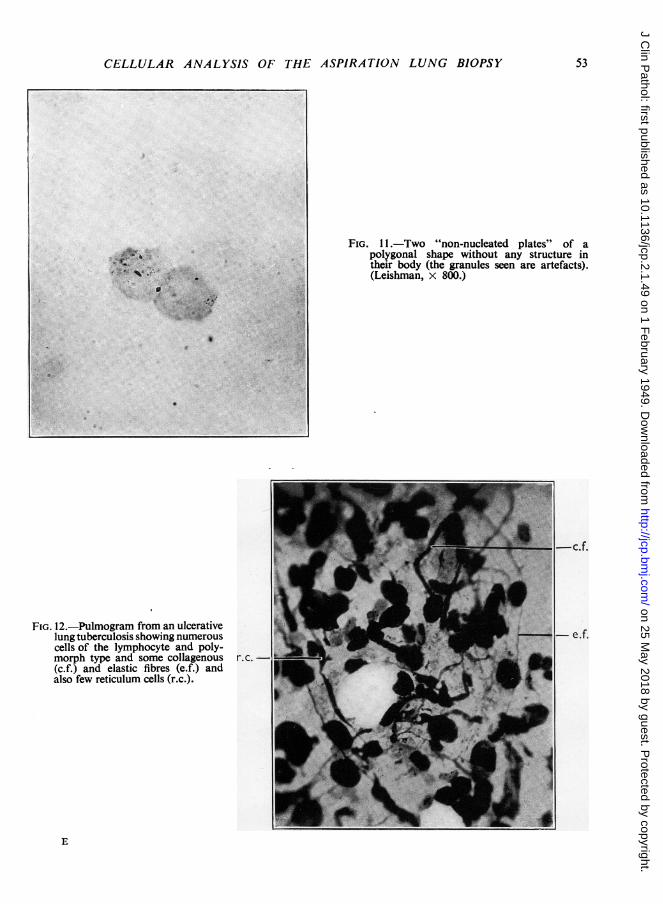
quite irregular in outline and stain very lightlybluish violet; they are usually located at thethinner end of the smear singly or in groups. Thetwo-needle method, made through the incision inthe skin, on the one hand and the aspiration lungspecimen taken at necropsy on the other provetheir lung origin conclusively.
Similar plates have been described by Kolliker(1881) and Lang (1925) as forming part or all ofthe alveolar lining. In the aspiration lung biopsy,however, they may be an artifact-for example,cells of various kinds from which the nucleus hasbeen removed by manipulation while making thefilm.
(e) The reticulum cells (Fig. 12), which are rarelyfound in a normal pulmogram, are branchingelements with deep blue non-granular cytoplasmand hyperchromatic nucleus, situated in the middleof the body of the cells. They are quite numerousin a pulmogram from pathological conditions ofthe lung entailing destruction of the pulmonarytissue.
(f) Collagenous and elastic fibres are elementsoften met in pulmograms obtained from a lunginvolving destructive processes; both are stainedviolet by this method; collagenous fibres (Fig.12, c.f.) are thick and twisted threads and theelastic fibres (Fig. 12, e.f.) are fine straight ones.
(g) Lymphoid cells are cells of young lympho-cytic type as met in the peripheral blood, with around violet nucleus and one nucleolus; the paleblue cytoplasm never contains any particles andin this respect resembles the nucleated alveolarepithelium. They are, however, much smaller insize than alveolar epithelium, while the nuclearchromatin is more compact and the nucleus itselfalso is much smaller.
(h) Ciliated and non-ciliated epithelial cells(Fig. 10) lining bronchi and bronchioles of differentcalibre are very seldom seen in a normal biopsy.Pathological conditions such as venous congestionand chronic bronchitis, however, are characterizedby the appearance of such ciliated cylindrical cellsarranged in palisade formation or singly. Cilia bythis method of staining are pink-red or violet incolour. If arranged in a layer, these cells mayinciude goblet elements (Fig. 10). The bottom ofthe row shows polygonal epithelial cells with ovalnuclei and they are the parent cells of the surfaceepithelium.
Non-ciliated epithelial cells lining respiratorybronchioles are cells of cuboidal outline with a largeoval nucleus and cytoplasm free of any granula-tion in normal conditions, whereas in pathologicalones such as inflammations the cytoplasm may bevacuolated.
2. White blood cells aspirated from the pulmon-ary vessels.-The differential count of these cellswas compared with capillary blood differentialcount. The results are shown in the Table andindicate that difference between the peripheraland pulmonary differential counts lies within thelimits of experimental error.
3. Cells derived from tissue of the thoracic walL-These are mainly those from the costal andvisceral pleura. Such mesothelial cells (Fig. 6)may be seen in the pulmogram obtainedby the one-needle method. As was mentionedbefore, however, they may also appear in pulmo-grams made by the two-needle method, butin much smaller number. They are scatteredas loose cells over the whole film. Their paleviolet-blue cytoplasm is free of granulations. Theirround, violet nucleus is centrally or eccentrallylocalized and has thick granular chromatin.
52
on 25 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.2.1.49 on 1 February 1949. D
ownloaded from
CELLULAR ANALYSIS OF THE ASPi
FIG. 12.-Pulmogram from an ulcerativelung tuberculosis showing numerouscells of the lymphocyte and poly-morph type and some collagenous r.c. -(c.f.) and elastic fibres (e.f.) andalso few reticulum cells (r.c.).
]RATION LUNG BIOPSY 53
FIG. 11. Two "non-nucleated plates" of apolygonal shape without any structure intheir body (the granules seen are artefacts).(Leishman, x 800.)
ci.aI1.IP
E
.e*.......* 4 . * e > .... .$wib *
^: ? * ^*'' '5'§.$
on 25 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.2.1.49 on 1 February 1949. D
ownloaded from

Z. Z. GODLOWSKI
Tobacco-smoker's Pulmogram
Fig. 7, a specimen from a heavy smoker (60cigarettes per day) otherwise normal, shows a
remarkably increased number of all the cellularelements. Although there are certain parts in thefilm containing a lesser number of the cells, yetthe greater part of the smear has the characterreproduced in the photomicrograph. Giant cellswhich are of common occurrence in such cases
are also present.A detailed analysis of the tobacco-smoker's
pulmogram under high magnification is seen
in Fig. 9 and makes it clear that the majorityof the cells are macrophages and in thiscase might be called "tobacco cells." They are
loaded with particles of various sizes and shapesof which some are black and some are deep blue;the black granules are the carbon particleswhich are not stained at all, and thegranules staining deep blue might be partlycarbonized tobacco or paper particles inhaledwhile smoking. Apart from the macrophagesloaded with granules, there are quite numerous
macrophages almost entirely free from any par-ticles, and this may be regarded as a sign of localirritation by smoking. The nucleated alveolarepithelial cells are also much more numerous thanin non-smoker's pulmogram.The conclusions to be drawn from a smoker's
pulmogram are: (1) their lungs are "infiltrated"with macrophages with increased production ofgiant cells; (2) there is an increased shedding ofthe alveolar epithelium. The degree of thesealterations depends, of course, on the daily amountof tobacco inhaled.
CommentsAspiration lung biopsy may be used as a
diagnostic procedure in various pathological con-
ditions of the lung such as pneumoconiotic or
chronic and acute inflammatory processes. Thepathological alterations may be viewed on thebases of quantitative and qualitative changes ofthe cellular elements as welI as changes of micro-histochemical analysis; this may be of particular
value in the various types of pneumoconiosis, whichmay offer diagnostic difficulties clinically.The most common complication of the aspira-
tion lung biopsy is pneumothorax which in thepresent series occurred in three cases in a verybenign form; pneumothorax per se, if not of verygreat degree, should not be regarded as serious.On the contrary it might even have a certain bene-ficial effect in inflammatory lung conditions. Innon-inflammatory cases it is usually a harmlessevent generally escaping notice.The few accompanying photomicrographs give
some idea of the value of this method in clinicaldiagnosis. Further investigation is needed to elicitits real value in the various pathological conditionsof the lungs.
Summary1. A cytological study is made of the aspiration
lung biopsy in normal and pathological conditions.2. The method of the biopsy is described.3. Suggestions are made for further investiga-
tions along these lines.I express my thanks to Prof. A. M. Drennan,
of the Pathology Department, Edinburgh University,for his advice and criticism; to Dr. Mackie, radio-logist to the Ballochmyle Hospital, Ayrshire, for hisready collaboration and technical advice in the carry-ing out of the aspiration biopsy in his department;to Dr. F. R. Ogilvie for criticsm and help in micro-scopic differentiation of the cellular elements; and toMr. T. C. Dodds for the photomicrographs.
REFERENCESBertelli, G., Falta, W., and Schweenger, 0. (1910). Z. klin. Med.,
71, 23.Bullowa, J. G. M. Quoted by Sappington and others.Cappell, D. F. (1923). J. Path. Bact., 26, 430.Cappell, D. F. (1929). J. Path. Bact., 32, 675.Carleton, H. M. (1927). J. Hyg., Camb., 26, 227.Foot, N. C. (1927). Amer. J. Path., 3, 413.Gazayerli, M. E. (1936). J. Path. Bact., 43, 357.Godlowski, Z. Z. (1948). Brit. med. J., 1, 46.Kolliker (1881). Quoted by Millep.Lang, F. J. (1925). J. infect. Dis., 37, 430.Martin, H. E., and Ellis, E. B. (1930). Ann. Surg., 92, 169.Martin, H. E., and Ellis, E. B. (1934). Surg. Gynec. Obstet., 59, 578.Miller, W. S. (1947). " Lung." Second Edit. C. C. Thomas, Spring-
field, Illinois.Sappington, S. W., and Favorite, G. 0. (1936). Amer. J. med. Sci.,
191, 225.Stewart, D. (1930). Lancet, 2, 520.Wilson, T. E. (1945). Med. J. Austral., 1, 268.
54
on 25 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.2.1.49 on 1 February 1949. D
ownloaded from