cell transplantation and immunoisolation
TRANSCRIPT
From the Departments of Transplantation Surgery and Pathology,Karolinska Institutet, Huddinge Hospital,
Stockholm, Sweden
CELL TRANSPLANTATION AND IMMUNOISOLATION
Studies on a macroencapsulation device
By
Ehab Rafael, B.Sc., M.D.
Stockholm 1999

2
Cover photo: Cross-section of an islet graft in a preimplanted TheraCyte™ device, 2 weeksafter islet transplantation.
ISBN 91-628-3883-0Printed in Sweden by Repro Print AB, Stockholm 1999

3
To my country, Egypt
To my church, The Coptic Orthodox

4
Abstract
Encapsulation of cellular grafts in semipermeable membranes may provide a way to
protect the graft from immune attack without the need for pharmacological
immunosuppression. In this thesis, the use of immunoisolating devices consisting of a
bilaminar PTFE membrane was evaluated. Previous experimental studies indicate that these
devices can protect cellular allografts from rejection. This thesis aims at improving our
understanding of physiological factors influencing graft survival.
In the first study, the use of macroencapsulation for protection of human parathyroid
allograft was evaluated. The following studies focused on the physiological milieu in the device
by longitudinal investigations of the exchange of insulin and glucose across the membrane and
the blood perfusion in the surrounding tissues. Finally, we evaluated whether implantation of
the device 3 months before loading with islets improves graft survival.
The results can be summarized as follows. Allogeneic parathyroid tissue encapsulated
in TheraCyte devices can survive for one year after transplantation in non-
immunosuppressed humans. However, marked growth of fibrotic tissue occurred in the
devices. The exchange between the device lumen and microcirculation was reduced 1-4 weeks
after implantation, but improved at 3 months and then no significant diffusion barrier seemed
to be present. Histologically, the number of vascular profiles within 15 µm of the device
surface was significantly increased as early as 2 weeks after implantation, while the number
within 250 µm increased up to 3 months after implantation. Only the number of vessels within
250 µm showed a significant correlation to glucose kinetics. The blood perfusion in the s.c.
tissue surrounding the device was lower at 4 weeks than on day 1 after implantation. It
recovered at 2 months and then remained at a similar level for at least one year. The last study
showed that if devices were preimplanted and loaded with islets in situ 3 months later, the
survival of encapsulated syngeneic rat islets improved and the growth of fibrotic tissue in the
device was reduced.
We conclude that microdialysis and laser Doppler are useful methods for evaluating
the performance of a macroencapsulation device in vivo. Preimplantation of the TheraCyte™
device seems to be a promising way to improve the survival of the encapsulated graft.
5
Original papers
This thesis is based on the following publications which will be referred to by their romannumerals:
I. Survival of macroencapsulated allogeneic parathyroid tissue one year after transplantationin non-immunosuppressed humans.Tibell A, Rafael E, Wennberg L, Wernerson A, Bergström M, Geller RL, Loudovaris T,Johnson RC, Brauker JH, Neuenfeldt S, Nordenström J.Submitted.
II. In vivo studies on insulin permeability of an immunoisolation device intended for islettransplantation using the microdialysis technique.Rafael E, Wernerson A, Arner P, Tibell A. Eur Surg Res 31: 249-258; 1999.
III. In vivo evaluation of glucose permeability of an immunoisolation device intended for islettransplantation: A novel application of the microdialysis technique.Rafael E, Wernerson A, Arner P, Wu GS, Tibell A.Cell Transplantation 8 (3): 317-326; 1999.
IV. Longitudinal studies on the microcirculation around the Theracyte immunoisolationdevice, using the laser Doppler technique.Rafael E, Gazelius B, Tibell A.Cell Transplantation. In press.
V. Improved survival of macroencapsulated islets of Langerhans by preimplantation of animmunoisolating device. A morphometric study.Rafael E, Wernerson A, Wu GS, Hultenby K, Tibell A.In manuscript
Copyright
Paper II: S. Karger AG, Medical and Scientific Publishers, Basel, Switzerland
Paper III: Cognizant Communication Corporation, NY, USA

6

7
Table of Contents
Introduction...................................................................................................................
Aims of the studies.........................................................................................................
Material and Methods.................................................................................................…
A. Immunoisolation devices and techniques used in various studies………………………….
B. Designs of the individual studies…………………………………………………………..
Results and Discussion...................................................................................................
Appendix with colour photographs of histological sections……………………………………....
Summary...........................................................................................…………………..
Conclusions………………………………………………………………………………
Acknowledgments..........................................................................................................
References.....................................................................................................................
Paper I - V
9
25
26
26
33
41
60
62
65
66
70
8
Abbreviations
ANOVA Analysis of variance
AUC Area under the curve
BW Body weight
Cmax Peak concentration
CMV Cytomegalovirus
HIV Human immunodeficiency virus
i.m.
i.p.
Intramuscular
Intraperitoneally
IVGTT Intravenous glucose tolerance test
Ka K-value for the ascending limb of the curve
Kd K-value for the descending limb of the curve
LDF Laser Doppler flowmetry
LDPM Laser Doppler perfusion monitoring
MLC Mixed lymphocyte culture
MNC Mononuclear cells
ns Non-significant
PBL Peripheral blood leucocytes
PTFE Polytetrafluroroethylene
PTH
PU
s.c.
SD rat
SD
STZ
TTP
Vv
Parathyroid hormone
Perfusion units
Subcutaneous
Sprague-Dawley rat
Standard deviation of the mean
Streptozotocin
Time-to-peak
Volume density
9
Introduction
A major breakthrough in transplantation occurred in 1954 when Joseph Murray performed the
first successful kidney transplant between identical twins (Merill JP et al 1956). In the early
1960s, administration of the immunosuppressive drug 6-mercaptopurine together with
corticosteroids made it possible to perform renal allotransplantation (Calne RY 1960, Zukoski
CF et al 1960). This was the first example of successful whole-organ allografting in the
treatment of patients with terminal organ failure. Today, kidneys, livers, pancreases, hearts and
lungs are grafted with good results and transplantation of the small bowel is being developed.
The first clinical trials in the field of cell transplantation were started in the late 1960s and early
1970s. Thomas and others used bone marrow transplantation to treat patients with aplastic
anemia, immune deficiencies and acute leukemia (Bach FH et al 1968, Gatti RA et al 1968,
Thomas ED et al 1972, 1977). Today, about 100 000 patients have undergone hematopoietic
stem cell transplantation and the number of indications is increasing.
The use of somatic cellular grafts for replacement of degenerated or diseased tissues has
progressed at a slower pace. Nevertheless, somatic cell therapy has potential to help patients
with chronic disabling metabolic and neurological disorders such as diabetes and Parkinson’s
disease (Björklund A et al 1979, Perlow MJ et al 1979, Lindvall O 1993, 1995 ). It has also
been suggested that transplantation of hepatocytes might be of value in the treatment of
fulminant hepatic failure or to replace a defective hepatic enzyme in patients with inborn errors
of metabolism (Morris PJ 1993). The transplantation of myoblasts as a treatment of
Duchenne´s muscular dystrophy is also being investigated (Partridge TA et al 1989).
In many of these patient groups, a cellular graft would not be immediately life-saving, but the
transplantation would aim at ameliorating symptoms and improve the quality of life. Therefore,
the risks connected with the treatment must be low. A cellular transplantation is usually a
comparatively minor procedure for the patient. However, the side-effects of chronic
immunosuppressive therapy must compare favorably with the complications of the disease
itself. For pancreatic islets and other grafts consisting of secretory cells, immunoisolation - that
is, encapsulation of the cells in semipermeable membranes - may reduce the need for

10
immunosuppressive therapy. The introductory part of my thesis focuses on studies of islet
transplantation and various methods for immunoisolation of secretory grafts.
Transplantation of the islets of Langerhans
Transplantation as a treatment for diabetes. Type-1 diabetes is caused by autoimmune
destruction of insulin-producing β-cells in the pancreas. Today, transplantation of the whole
pancreas (Abendroth D et al 1990, Stratta RJ et al 1998, Tydén G et al 1999) or of the islets
of Langerhans alone (London NJM et al 1994, Sutherland DER 1996, Hering BJ et al 1999,
Benedum J 1999) is the only treatment that can restore endogenous insulin production. Up till
now, more than 10 000 patients with diabetes have undergone pancreas transplantation while
only 353 adult islet allotransplantations have been reported to the Islet Transplantation
Register (Brendel MD et al 1999).
Pancreas transplantation is usually performed in conjunction with a renal transplantation.
Thus the recipients have long-standing diabetes and apart from nephropathy, they have
secondary complications affecting nerves, eyes and vessels. After pancreas transplantation, the
patients become insulin-independent and free from dietary restrictions. Somatic and autonomic
neuropathy improve and the pancreas graft protects the simultaneously transplanted kidney
from developing diabetic nephropathy. Mild retinopathy stabilizes or improves while advanced
lesions do not benefit from this procedure (Landgraf R 1996, Stratta RJ 1998). Pancreas graft
recipients experience an improved quality of life (Mattas AJ et al 1998, Gross CR et al 1998).
Moreover, patients given combined grafts have significantly better long-term survival than
diabetic recipients of a renal graft alone (Tydén G et al 1999, Smets YFC et al 1999). Thus,
pancreas transplantation has clearly proven the value of providing diabetic patients with new
insulin-producing tissue.
In recipients of combined grafts, the only expense for these benefits is the increased surgical
risk connected with the pancreatic grafting as these patients, due to their renal grafts, are
subjected to chronic immunosuppression anyhow. Ideally, transplantation should be performed
at an early stage in the diabetic disease, to prevent the development of secondary
complications. However, such non-uremic patients have a more vigorous immune response

11
(Tyden G et al 1990). Furthermore, in this patient group, the benefits must be weighed against
the risks connected with surgery and chronic immunosuppression.
Experimental studies on islet transplantation. Moskalewski was the first to describe the use
of collagenase to isolate islets of Langerhans from finely dispersed guinea pig pancreases
(Moskalewski S 1965). The technique was refined by Lacy and Kostianovsky who introduced
intraductal injection of collagenase and applied the technique to the rat pancreas (Lacy PE et al
1967). A few years later, the same group also reported the first successful islet transplantation
placing 500 syngeneic islets intraperitoneally in diabetic rats (Ballinger WF et al 1972). In the
early studies, the islets were handpicked from the pancreatic digest. Later, a more rapid
method for purification of the islet grafts was devised -i.e., centrifugation on density gradients.
However, the procedure developed for isolation of rodents islets was inefficient to separate
islets from the pancreas of large mammals and man. During the 1980s, modifications in the
methods of isolation and purification improved both the number and purity of islets obtained
from large animal and human pancreases (Gray DWR et al 1984, 1987, Ricordi C et al 1988,
1990, Rajotte RV et al 1987). Since then, cure of diabetes by alloislet transplantation has also
been reported in animals such as the dog and monkey (Gray DW et al 1986, Warnock GL et al
1988).
Clinical islet transplantation. More than 100 years have passed since Williams, in 1890,
attempted the first β-cell transplantation by implanting fragments of a sheep pancreas in a 15-
year-old diabetic child (Williams PW 1894). Insulin was not discovered until some 30 years
later, but the transplantation was based on the hypothesis that the pancreas contained a
”sugar-destroying substance”.
During the 1980s, clinical islet transplantation trials were initiated in several countries. The
early trials were performed using fetal allogeneic and xenogeneic tissue, due to the initial
problems with adult islet isolation. More than 1500 such cases have been reported, many of
which were performed in China and Eastern Europe. In most cases, very little information is
available. Thus, it is difficult to draw any definite conclusions from these trials but there seem
to be no confirmed cases of insulin independence after fetal islet transplantation (Federlin KF
et al 1992). However, in a number of well-documented cases, C-peptide has been secreted for
12
several months after allogeneic and xenogeneic fetal islet transplantation (Groth CG et al 1980,
1994).
The first case of long-lasting cure of a diabetic recipient using allogeneic islet transplantation
was reported by Kolb and Largadier (Kolb E et al 1980). In this patient, the islet graft was
obtained from a pediatric donor. After the methods for isolation of adult human islets were
improved, several groups started clinical trials usually performing the transplantations in
patients having diabetic nephropathy, in conjunction with or after renal grafting. In 1989,
Scharp et al achieved 15 days of insulin-independence and the next year, the same group had a
patient off insulin for >300 days after adult alloislet transplantation (Scharp DW et al 1989,
1990). Since then, several groups have reported insulin independence after transplantation of
adult human islets but on the whole, the success rates remain low (Scharp DW et al 1992,
Socci C et al 1991, Warnock GL et al 1991, Ricordi C et al 1992).
Until December 1998, 405 adult islet allografts were reported to the Islet Transplant Register.
Only 10% of the patients became insulin-independent (>1 week) during the first year while
partial function, defined as C-peptide excretion >0.5 ng/ml, was obtained in 35%. The longest
period of insulin-independence reported so far is 70 months (Brendel MD et al 1999). The
results obtained by the group in Giessen, Germany are more promising (Bretzel RG et al
1998). In a series of 17 simultaneous islet and kidney transplantations, 14 patients had
functioning islet grafts at 1 year and 4 have become insulin-independent. In the patients given
islet grafts after a previous renal transplantation, 8 of 15 had functioning islet grafts at 1 year
and 3 achieved insulin-independence.
Autologous and allogeneic islet transplantations have also been carried out in patients with
surgically-induced diabetes. In such patients, the results are better. More than 50% of patients
autotransplanted after pancreatectomy for chronic pancreatitis are insulin-independent at 1
year. In this group, the number of islets transplanted seems to be the most important factor for
cure. The longest duration of function reported was more than 7 years (Brendel MD et al,
1999). In a small series of patients undergoing combined liver and islet transplantation after
upper abdominal exenteration for malignancy, 5 of 9 patients became insulin-independent
(Tzakis AG et al 1990). These islet grafts usually functioned until the patient died because of
tumor recurrence, the longest survival being almost 5 years.
13
These results prove that the islets of Langerhans can be implanted in an ectopic site, like the
liver, and function and provide insulin-independence for long periods. Factors contributing to
the low success rate in type-1 diabetic patients may include insulin resistance in the recipient,
side-effects of the immunosuppressive drugs and islet losses due to rejection and recurrence of
diabetes in the graft.
The promise of islet transplantation. In clinical work, transplantation of the islets of
Langerhans is usually performed by an injection into the recipient´s portal vein and offers a
simple and safe technique to provide a patient with new insulin-producing tissue. Compared to
pancreas transplantation, islet transplantation may offer better possibilities to reduce or omit
the need for chronic immunosuppression e.g., by encapsulation of the islets within
semipermeable membranes (see below). Furthermore, islets can be kept in culture for several
days before grafting. During this time, the graft can be pretreated to reduce immunogenicity. In
the future, the culture period may be used for treatment of the recipient with donor antigen to
induce tolerance. Islet transplantation may also facilitate the use of xenogeneic donors.
Transplantation of parathyroid tissue
The parathyroid glands represent another type of endocrine tissue that can be transplanted as a
cellular allograft. Autotransplantation of parathyroid tissue is routinely performed in
conjunction with total parathyroidectomy in patients with parathyroid hyperplasia (Alveryd A
1968, Chou FF et al 1998, Hidi H et al 1998, Walgenbach S et al 1999). Usually these
autografts function adequately, but occasionally they fail or the parathyroid glands are removed
accidentally during thyroid surgery and chronic hypoparathyroidism develops.
Most patients with chronic hypoparathyroidism do well on vitamin D and calcium supplements.
In a few cases, the calcium levels are unstable and the patients have problems with
hypocalcemic or hypercalcemic episodes. Of the few patients who have undergone
allotransplantation of the parathyroid glands, most have been renal graft recipients who
required chronic immunosuppression anyway (Alfery EJ et al 1992, Groth CG et al 1973). A
few attempts to transplant encapsulated parathyroid tissue have also been reported (Hasse C et
al 1994, Tibell A et al 1996). However, parathyroid allotransplantation has usually not been
14
considered because its advantages were out-weighed by the need for chronic
immunosuppression.
Immunosuppression hazards
The main disadvantages of successful allotransplantation are side-effects of the
immunosuppressive therapy. While old drugs like steroids and azathioprine affect the immune
system in many ways, new drugs often interfere with specific mechanisms involved in rejection.
The side effects can be divided into those related to the immunosuppressive effect, and those
that are not.
Those related to the immunosuppressive properties include an increased susceptibility to
infections and an increased risk of malignancies. Opportunistic infections are of concern,
especially during the first year after transplantation, while malignancies often occur later in the
follow-up. Data from several large transplant centers show an overall incidence of malignant
tumors which is 4-5 times higher than that in the general population (Hisse C et al 1995, Tan-
Shalaby J et al 1995).
There are also side-effects that are specific for each compound. Corticosteroids alone or in
combination with other immunosuppressives can cause -e.g., osteoporosis, diabetes, cataracts,
weight gain and poor growth in children (Lindholm A et al 1992). Azathioprine and
mycophenolate mofetil can induce bone marrow depression and gastrointestinal disturbances
(Keown P et al 1996, Shapiro R et al 1999), whereas nephrotoxicity, hypertension, gingival
hyperplasia and hirsutism are common in patients on cyclosporine A (Starzl TE et al 1991,
Lindholm A et al 1992). Tacrolimus may cause neurotoxicity, nephrotoxicity and increase the
incidence of diabetes (Starzl TE et al 1991, Shapiro R et al 1995, Moxey-Mims M et al. 1998,
Shapiro R et al 1999) while sirolimus has been associated with hyperlipidemia, reductions in
platelet and WBC counts, increases in liver enzymes and arthralgia (Groth CG et al 1999).
Of special concern, in islet transplantation is that several of the immunosuppressive drugs,
including cyclosporine, tacrolimus and steroids, have negative effects on β−cell function and
increase insulin resistance (Gunnarsson R et al 1983, Schlumpf R et al 1986, Engfeldt P et al
1986, van Schlifgaarde R et al 1986, Tze WJ et al 1990). Studies in pancreatic graft recipients
15
and non-diabetic kidney recipients show that increased insulin secretion is needed to maintain
normal glucose metabolism in patients on immunosuppression with cyclosporine, azathioprine
and steroids (Christiansen E et al 1996a, b).
It would obviously be better if islet transplantation could be performed without any need for
chronic immunosuppression. β-cell toxicity could be avoided and the secretory demand on the
islet graft would be reduced, increasing the likelihood of insulin-independence. Furthermore,
the morbidity related to immunosuppressive therapy would be of no concern. Then the
indications for islet transplantation could be widened. Young diabetic patients would be treated
early, thereby improving their quality of life and preventing development of the secondary
complications of diabetes. Protecting the islets from the immune response by encapsulation of
the graft in semipermeable membranes may help to achieve this goal.
Immunoisolation
The term immunoisolation refers to the encapsulation of a graft in a selectively permeable
membrane. To support the graft, low molecular weight substances, such as oxygen, glucose
and other nutrients, should be exchanged across the membrane while protection against
rejection requires that immune cells and other factors detrimental to graft survival are
excluded. The possibility of using such membranes is being explored for certain types of
cellular grafts, mainly those consisting of secretory cells. Obviously, the prerequisite for a
therapeutic effect is that the cell product -e.g., insulin, will also be exchanged across the
membrane and taken up by the surrounding microcirculation.
Devices produced from synthetic membranes and loaded with viable cells have been termed
biohybrid artificial organs and are being developed as substitutes in case of failing organ or
tissue function (Colton C 1995). The graft can consist of primary allogeneic or xenogeneic
cells or be derived from a cell line.
A number of studies are in progress on the use of biohybrid artificial organs for a wide variety
of diseases including endocrine deficiencies such as diabetes (Lacy PE et al 1991, Altman JJ et
al 1990, Lanza RP et al 1997b, Reach G et al 1984, 1992, 1993, 1994, Aomatsu Y et al 1992)
and hypoparathyroidism (Sollinger HW et al 1983, Fu XW et al 1989, Hasse C et al 1994,
16
1996, Tibell A et al 1996). Devices have been filled with genetically-engineered cells to
provide a source of erythropoietin in anemia (Koo J et al 1993), human growth factor in
dwarfism (Chang PL et al 1993) and factor IX in hemophilia B (Liu HW et al 1993, Brauker
JH et al 1998). Bovine adrenal chromaffin cells producing metenkephalin and other pain-
relieving substances have been implanted in patients with morphine-resistant pain (Aebisher P
et al 1994).
Biohybrid artificial organs have also been suggested for treatment of neurodegenrative
disorders such as Parkinson’s disease (Aebischer P et al 1991, Emerich DF et al 1992, Hara K
et al 1997), Alzheimer’s disease (Winn SR et al 1994) and amyotrophic lateral sclerosis
(Aebischer P et al 1996). Encapsulated porcine hepatocytes have been incorporated in a
perfusion machine - the so-called liver-assist device - and used extracorporeally for temporary
treatment of patients with fulminant liver failure (Vanholder R et al 1991, Takebe K et al 1996,
Kanai N et al 1999). In most cases, development is still in an early phase but the liver-assist
device and the bovine cells used as a treatment for pain are undergoing phase II trials in
humans. The remaining part of this survey focuses on the possible use of encapsulated islets of
Langerhans as treatment for diabetes.
The principle of immunoisolation of islets for transplantation has two potential benefits. First, it
may permit alloislet transplantation without the use of pharmacological immunosuppression.
Secondly, encapsulation may facilitate the transplantation of islets from non-human species
(xenografts) thereby giving access to an unlimited source of insulin-producing tissue.
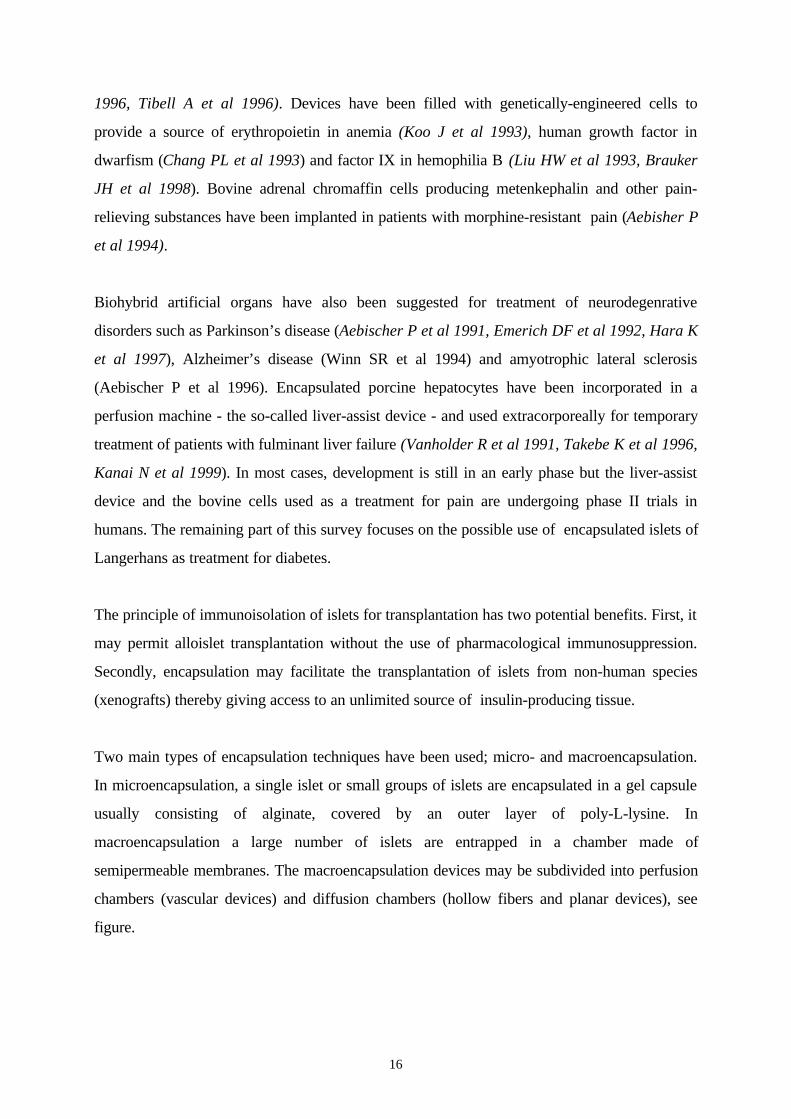
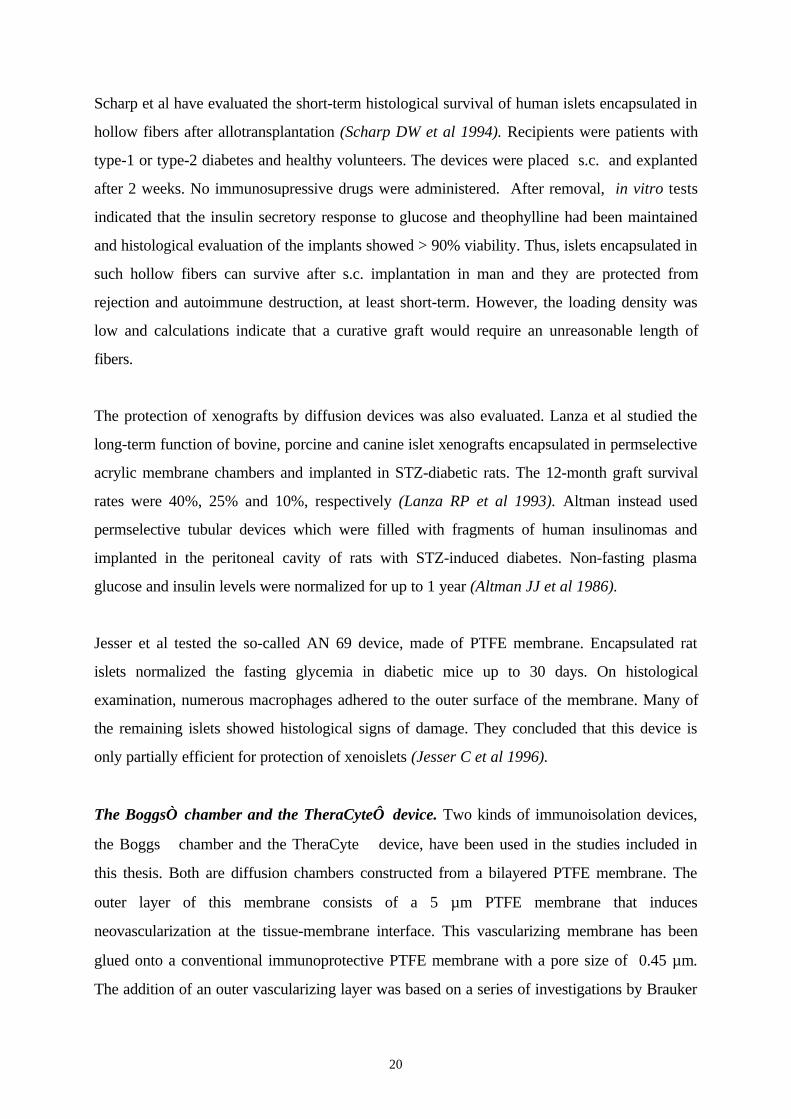
Two main types of encapsulation techniques have been used; micro- and macroencapsulation.
In microencapsulation, a single islet or small groups of islets are encapsulated in a gel capsule
usually consisting of alginate, covered by an outer layer of poly-L-lysine. In
macroencapsulation a large number of islets are entrapped in a chamber made of
semipermeable membranes. The macroencapsulation devices may be subdivided into perfusion
chambers (vascular devices) and diffusion chambers (hollow fibers and planar devices), see
figure.
17
Microcapsules Macrocapsules
1A
1B
2
3
1-2: Diffusion devices;1. planar devices (A: Boggs® chamber, B: TheraCyte™)2. hollow fibers
3: Perfusion device (vascular device)
A-V shunt
Implanted cells
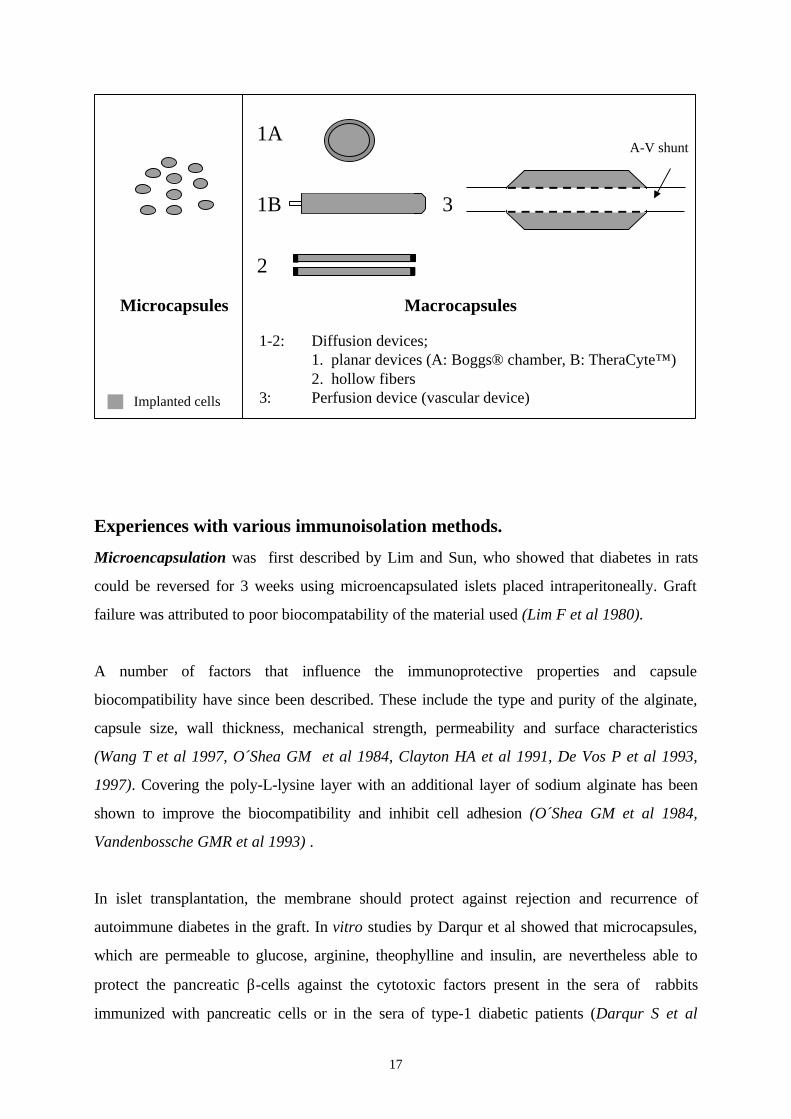
Experiences with various immunoisolation methods.
Microencapsulation was first described by Lim and Sun, who showed that diabetes in rats
could be reversed for 3 weeks using microencapsulated islets placed intraperitoneally. Graft
failure was attributed to poor biocompatability of the material used (Lim F et al 1980).
A number of factors that influence the immunoprotective properties and capsule
biocompatibility have since been described. These include the type and purity of the alginate,
capsule size, wall thickness, mechanical strength, permeability and surface characteristics
(Wang T et al 1997, O´Shea GM et al 1984, Clayton HA et al 1991, De Vos P et al 1993,
1997). Covering the poly-L-lysine layer with an additional layer of sodium alginate has been
shown to improve the biocompatibility and inhibit cell adhesion (O´Shea GM et al 1984,
Vandenbossche GMR et al 1993) .
In islet transplantation, the membrane should protect against rejection and recurrence of
autoimmune diabetes in the graft. In vitro studies by Darqur et al showed that microcapsules,
which are permeable to glucose, arginine, theophylline and insulin, are nevertheless able to
protect the pancreatic β-cells against the cytotoxic factors present in the sera of rabbits
immunized with pancreatic cells or in the sera of type-1 diabetic patients (Darqur S et al
18
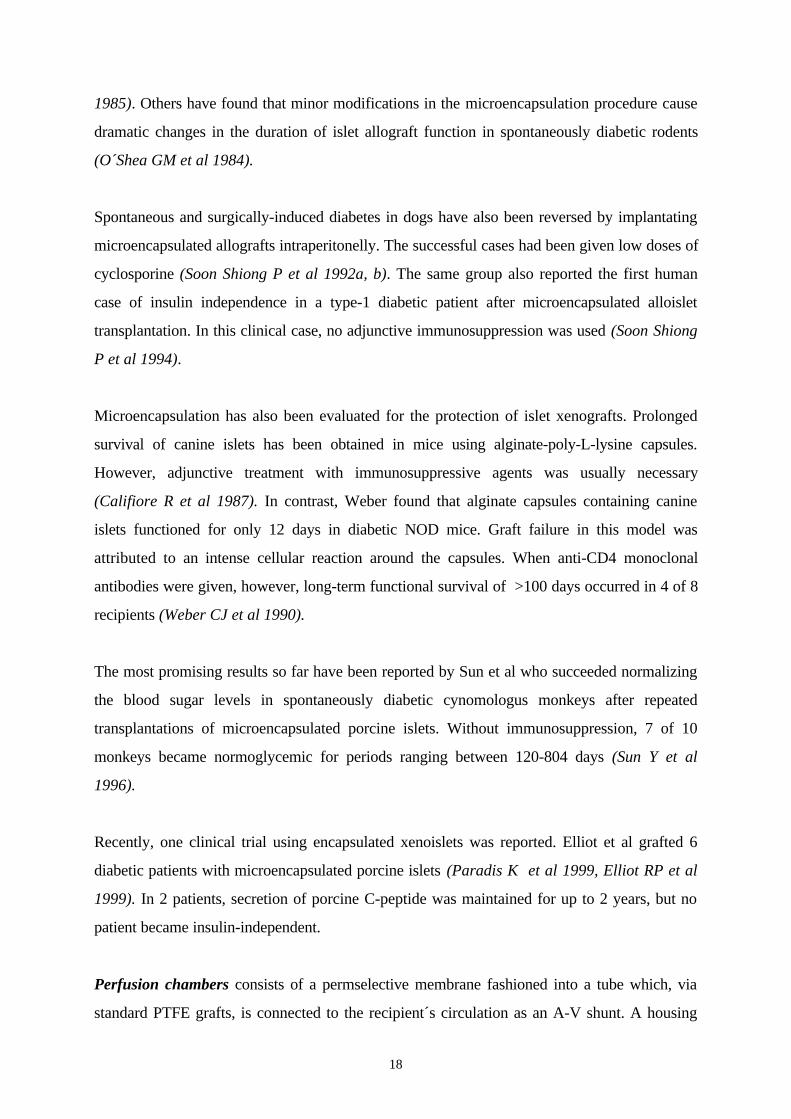
1985). Others have found that minor modifications in the microencapsulation procedure cause
dramatic changes in the duration of islet allograft function in spontaneously diabetic rodents
(O´Shea GM et al 1984).
Spontaneous and surgically-induced diabetes in dogs have also been reversed by implantating
microencapsulated allografts intraperitonelly. The successful cases had been given low doses of
cyclosporine (Soon Shiong P et al 1992a, b). The same group also reported the first human
case of insulin independence in a type-1 diabetic patient after microencapsulated alloislet
transplantation. In this clinical case, no adjunctive immunosuppression was used (Soon Shiong
P et al 1994).
Microencapsulation has also been evaluated for the protection of islet xenografts. Prolonged
survival of canine islets has been obtained in mice using alginate-poly-L-lysine capsules.
However, adjunctive treatment with immunosuppressive agents was usually necessary
(Califiore R et al 1987). In contrast, Weber found that alginate capsules containing canine
islets functioned for only 12 days in diabetic NOD mice. Graft failure in this model was
attributed to an intense cellular reaction around the capsules. When anti-CD4 monoclonal
antibodies were given, however, long-term functional survival of >100 days occurred in 4 of 8
recipients (Weber CJ et al 1990).
The most promising results so far have been reported by Sun et al who succeeded normalizing
the blood sugar levels in spontaneously diabetic cynomologus monkeys after repeated
transplantations of microencapsulated porcine islets. Without immunosuppression, 7 of 10
monkeys became normoglycemic for periods ranging between 120-804 days (Sun Y et al
1996).
Recently, one clinical trial using encapsulated xenoislets was reported. Elliot et al grafted 6
diabetic patients with microencapsulated porcine islets (Paradis K et al 1999, Elliot RP et al
1999). In 2 patients, secretion of porcine C-peptide was maintained for up to 2 years, but no
patient became insulin-independent.
Perfusion chambers consists of a permselective membrane fashioned into a tube which, via
standard PTFE grafts, is connected to the recipient´s circulation as an A-V shunt. A housing
19
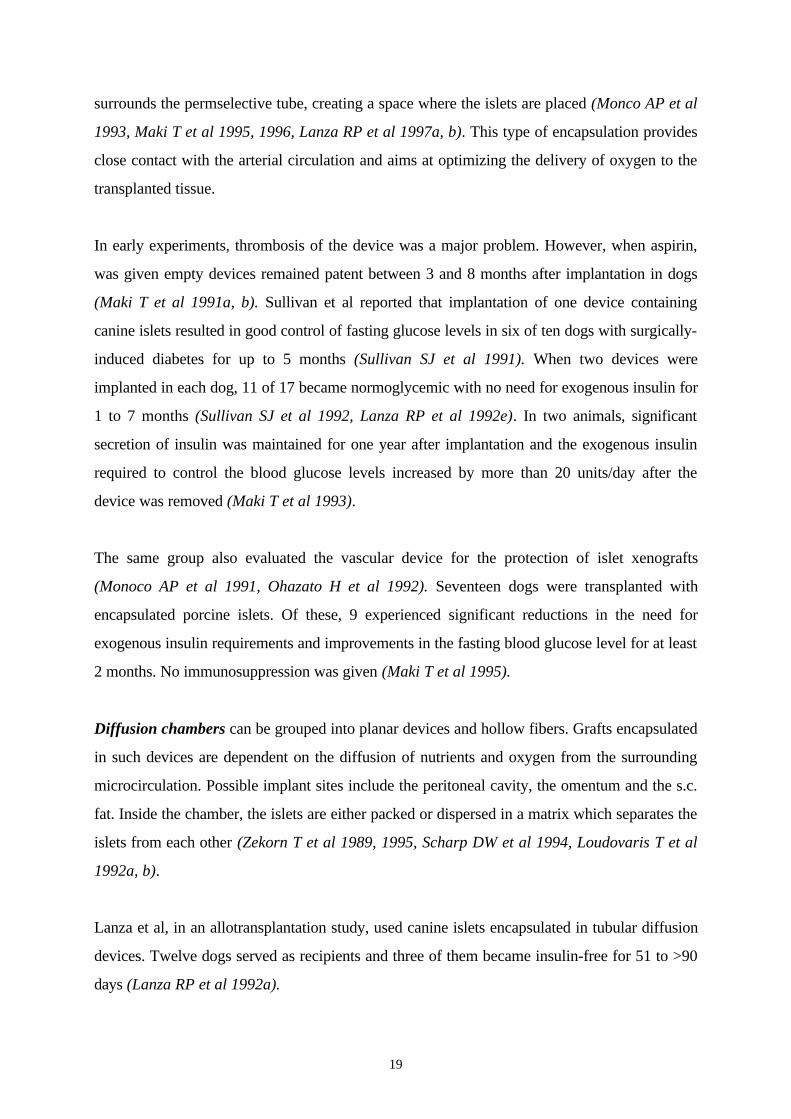
surrounds the permselective tube, creating a space where the islets are placed (Monco AP et al
1993, Maki T et al 1995, 1996, Lanza RP et al 1997a, b). This type of encapsulation provides
close contact with the arterial circulation and aims at optimizing the delivery of oxygen to the
transplanted tissue.
In early experiments, thrombosis of the device was a major problem. However, when aspirin,
was given empty devices remained patent between 3 and 8 months after implantation in dogs
(Maki T et al 1991a, b). Sullivan et al reported that implantation of one device containing
canine islets resulted in good control of fasting glucose levels in six of ten dogs with surgically-
induced diabetes for up to 5 months (Sullivan SJ et al 1991). When two devices were
implanted in each dog, 11 of 17 became normoglycemic with no need for exogenous insulin for
1 to 7 months (Sullivan SJ et al 1992, Lanza RP et al 1992e). In two animals, significant
secretion of insulin was maintained for one year after implantation and the exogenous insulin
required to control the blood glucose levels increased by more than 20 units/day after the
device was removed (Maki T et al 1993).
The same group also evaluated the vascular device for the protection of islet xenografts
(Monoco AP et al 1991, Ohazato H et al 1992). Seventeen dogs were transplanted with
encapsulated porcine islets. Of these, 9 experienced significant reductions in the need for
exogenous insulin requirements and improvements in the fasting blood glucose level for at least
2 months. No immunosuppression was given (Maki T et al 1995).
Diffusion chambers can be grouped into planar devices and hollow fibers. Grafts encapsulated
in such devices are dependent on the diffusion of nutrients and oxygen from the surrounding
microcirculation. Possible implant sites include the peritoneal cavity, the omentum and the s.c.
fat. Inside the chamber, the islets are either packed or dispersed in a matrix which separates the
islets from each other (Zekorn T et al 1989, 1995, Scharp DW et al 1994, Loudovaris T et al
1992a, b).
Lanza et al, in an allotransplantation study, used canine islets encapsulated in tubular diffusion
devices. Twelve dogs served as recipients and three of them became insulin-free for 51 to >90
days (Lanza RP et al 1992a).
20
Scharp et al have evaluated the short-term histological survival of human islets encapsulated in
hollow fibers after allotransplantation (Scharp DW et al 1994). Recipients were patients with
type-1 or type-2 diabetes and healthy volunteers. The devices were placed s.c. and explanted
after 2 weeks. No immunosupressive drugs were administered. After removal, in vitro tests
indicated that the insulin secretory response to glucose and theophylline had been maintained
and histological evaluation of the implants showed > 90% viability. Thus, islets encapsulated in
such hollow fibers can survive after s.c. implantation in man and they are protected from
rejection and autoimmune destruction, at least short-term. However, the loading density was
low and calculations indicate that a curative graft would require an unreasonable length of
fibers.
The protection of xenografts by diffusion devices was also evaluated. Lanza et al studied the
long-term function of bovine, porcine and canine islet xenografts encapsulated in permselective
acrylic membrane chambers and implanted in STZ-diabetic rats. The 12-month graft survival
rates were 40%, 25% and 10%, respectively (Lanza RP et al 1993). Altman instead used
permselective tubular devices which were filled with fragments of human insulinomas and
implanted in the peritoneal cavity of rats with STZ-induced diabetes. Non-fasting plasma
glucose and insulin levels were normalized for up to 1 year (Altman JJ et al 1986).
Jesser et al tested the so-called AN 69 device, made of PTFE membrane. Encapsulated rat
islets normalized the fasting glycemia in diabetic mice up to 30 days. On histological
examination, numerous macrophages adhered to the outer surface of the membrane. Many of
the remaining islets showed histological signs of damage. They concluded that this device is
only partially efficient for protection of xenoislets (Jesser C et al 1996).
The Boggs chamber and the TheraCyte device. Two kinds of immunoisolation devices,
the Boggs chamber and the TheraCyte device, have been used in the studies included in
this thesis. Both are diffusion chambers constructed from a bilayered PTFE membrane. The
outer layer of this membrane consists of a 5 µm PTFE membrane that induces
neovascularization at the tissue-membrane interface. This vascularizing membrane has been
glued onto a conventional immunoprotective PTFE membrane with a pore size of 0.45 µm.
The addition of an outer vascularizing layer was based on a series of investigations by Brauker
21
et al, and aimed at improving the physiological conditions in the device. When evaluating the
neovascularization at the membrane-tissue interface after s.c. implantation in rats, they found
that the PTFE membrane with a pore size of 5 µm had 80-100-fold more vascular structures
within 15 µm from the surface than a membrane with 0.02 µm pore size. The difference
occurred as early as 3 weeks after implantation and persisted for up to 1 year (Brauker JH et
al 1995). Brauker attributed this effect to the architecture of the surface of the 5 µm membrane
rather than to chemical or other properties. The improved neovascularization around implants
covered with the 5µm PTFE membrane has also been noted in humans (Tibell A et al 1992).
Brauker then studied the local inflammatory response around Boggs chambers containing
iso- allo- and xenografts. Empty devices and encapsulated isografts induced a mild
inflammatory reaction. Allografts induced a somewhat greater reaction while xenografts were
surrounded by a very severe inflammation. This difference in response is probably related to
the different immunogenicity of the antigens shed from the grafts. Brauker showed that
encapsulated mice embryonic lung xenografts were destroyed within 3 weeks while the
allografts were protected up to 1 year (Brauker JH et al 1996). This failure to protect
xenografts, may be related to the intense inflammatory reaction around such implants and to
the large pore size which allows e.g., immunoglobulins to cross the membrane (Brauker JH et
al 1992, 1996, Loudovaris T et al 1992b). Loudovaris et al also showed that if the mice were
treated with anti-CD4 antibodies, xenografts encapsulated in the Boggs chamber would
survive (Loudovaris T et al 1992a, 1996).
Andersson et al have studied human islets encapsulated in Boggs chambers and transplanted
to nude mice. Histological examination 1 to 2 months later showed well preserved islet
morphology. Maintained function was indicated by the presence of human C-peptide in mice
sera. However, encapsulated mouse and rat islets survived less well than human islets
indicating that rodent islets are more affected by the physiological milieu inside the device
(Andersson A et al 1994, 1996). Furthermore, when fetal porcine islet-like cell clusters were
transplanted to immunosuppressed C57BL/6 mice, encapsulated grafts did worse than free
grafts placed under the kidney capsule (Sandberg J-O et al 1995).
22
Weir´s group studied the number and volume of encapsulated islets required to cure diabetic
mice. They obtained cure in STZ-diabetic mice using 2 Boggs chambers with 500 islets each
(Suzuki K et al 1996, 1998a, Trivedi N et al 1997). They also showed reversal of diabetes in
nude mice, using 1200 rat islets encapsulated in the TheraCyte device and transplanted s.c.
(Tatarkiewicz K et al 1999). This group has developed a morphometric method to measure the
mass of islet tissue inside an immunoisolation device (Suzuki 1998b). Applying this technique,
they found that the amount of encapsulated islets needed to cure diabetes is equivalent to that
of a graft in an optimal transplant site, such as under the kidney capsule.
Loudovaris et al have explored the possibility of using the TheraCyte device for
encapsulation of insulinoma cell lines instead of primary islets (Loudovaris T et al 1999).
During the past 5 years, the TheraCyte device has also been extensively evaluated for
encapsulation of other tissues. Studies have been performed on genetically-engineered cells to
treat inborn errors of metabolism (Carr-Bendel VE et al 1997) and on cells secreting factor IX
in hemophilia (Brauker JH et al 1998). Another interesting application is in the field of anti-
tumor therapy. Geller et al reimplanted excised tumor tissue encapsulated in the TheraCyte
device. The shed antigens will then generate an antitumor response which, in experimental
models, can cure minimal residual disease (Geller R et al 1997a, b).
Common encapsulation problems
Despite some promising data mentioned above, a number of problems remain before islet
encapsulation can be successfully used in clinical work. Several of these problems are shared
by all the techniques used for encapsulation.
The inflammatory response to implanted devices. Implantation of artificial material in a living
body causes an inflammatory response (Icard P et al 1990, Soon-Shiong P et 1991, Fritschy
WM et al 1994, Brauker JH et al 1996). The reactions to implants could be divided into: an
acute inflammatory response, an chronic inflammatory response and the foreign body reaction
with the development of granulation tissue, foreign body giant cells, macrophages and fibrosis
(Anderson JM et al 1988). As discussed above, antigens shed from the encapsulated graft may
further enhance the reaction. For macroencapsulation devices, the surgical trauma caused by
the implantation procedure will also contribute to the inflammatory response. During the acute
23
phase, cytokines and other factors present in the surrounding tissues may cross the membrane.
These factors, as well as the avascular fibrotic capsule that usually develops around the
implant, may impair the functional capacity or even the survival of the encapsulated graft.
Poor graft survival. The ideal permeability of an immunoisolating membrane is a balance
between immunoprotection and tissue nutrition. If the pore size is too large, harmful factors
such as cytokines and antibodies or even immune cells may cross the membrane and damage
the encapsulated graft. If the pore size is too narrow, this will interfere with the nutritional
demands of the graft, jeopardizing graft survival (Colton K et al 1995, 1996). Oxygen is
considered to be one of the critical factors. Schrezenmeir et al have studied factors influencing
oxygen supply to the encapsulated graft. They suggested that the outer diameter of the device
should be less than 300 µm. Various methods to inhibit fibrous tissue formation or inducing
vascularization should also improve oxygen supply to the islets. Moreover, euglycemia
improves the chances of survival and function of the graft by preventing unnecessary oxygen
expenditure. The ratio between the diffusion distance and cell mass should also be taken into
consideration (Schrezenmeir J et al 1992, 1994).
A suitable implantation site is a problem especially for macroencapsulated grafts. In most
experiments, the epididymal fat pad, peritoneal cavity and s.c. tissue have been used for hollow
fibers and diffusion devices. For clinical trials, placement in the peritoneal cavity, the omentum,
on the surface of the liver or s.c. have been proposed. (Scharp DW et al 1991, 1992, 1994,
Juang J-H et al 1995). The latter site is known to have a poor blood supply but, on the other
hand the s.c. fat is safe and easily accessible for clinical use. As discussed above, the
physiological conditions inside the device will depend on the characteristics of the
immunoisolating membrane and on the properties of the surrounding tissue. These factors
influence the maximum loading density. If the loading density can be increased – i.e., more
islets can be packed into a given volume - the size of the device could be reduced which would
facilitate its clinical use.
The vascular devices are anastomosed as A-V shunts and require access to major vessels like
the iliac artery and vein. The need to implant several devices, the chronic treatment with
anticoagulants and the risks connected with vascular surgery especially in diabetic patients
seem to limit their usefulness in a clinical setting. For microencapsulated grafts, most groups
24
prefer implantation in the peritoneal cavity so the volume of the graft does not constitute a
problem (Soon-Shiong P et al 1992a, b, 1994). The major drawback is the risk of inducing
intraperitoneal adhesions.
Insufficient long-term stability of the immunoisolating membrane is a problem connected
especially with microencapsulated grafts. Major efforts have been made to improve the stability
of the capsule wall and the components of its structure (Wang T et al 1997, van Schilfgaarde
et al 1999). Macroencapsulation devices should be more chemically stable, but may be
susceptible to mechanical stress. Lanza et al reported that 80-90% of tubular membrane
diffusion devices transplanted into diabetic dogs had broken 5-7 months after implantation
(Lanza R et al 1992a).
In the following studies, we focused on use of the TheraCyte device for protection of
cellular allografts. Today, macroencapsulation is being explored for protection of many kinds
of secretory cells. However, in the field of islet transplantation, most recent research has
focused on microencapsulation. One important reason is the relatively great amount of tissue
needed to cure diabetes making it difficult to design reasonably-sized diffusion devices or
perfusion chambers. However, macroencapsulation devices have a number of advantages
including better physical and chemical stability and the possibility of retrieving the graft. To
facilitate the clinical use of macroencapsulation in islet transplantation, the survival of the
encapsulated graft should be improved and the loading density of these devices must be
increased.
25
Aims of the studies
The purpose of these studies were:
• To evaluate macroencapsulation as a method for protecting allogeneic parathyroid grafts in
humans.
• To assess the physiological conditions inside the TheraCyte immunoisolation device in
longitudinal studies.
• To evaluate the possible correlation between close vascular profiles and physiological
conditions in the device.
• To study the blood perfusion in the tissue surrounding the device in a longitudinal study.
• To develop strategies to improve the survival of encapsulated grafts.
26
Material and Methods
A. Immunoisolation devices and techniques used in the various studies
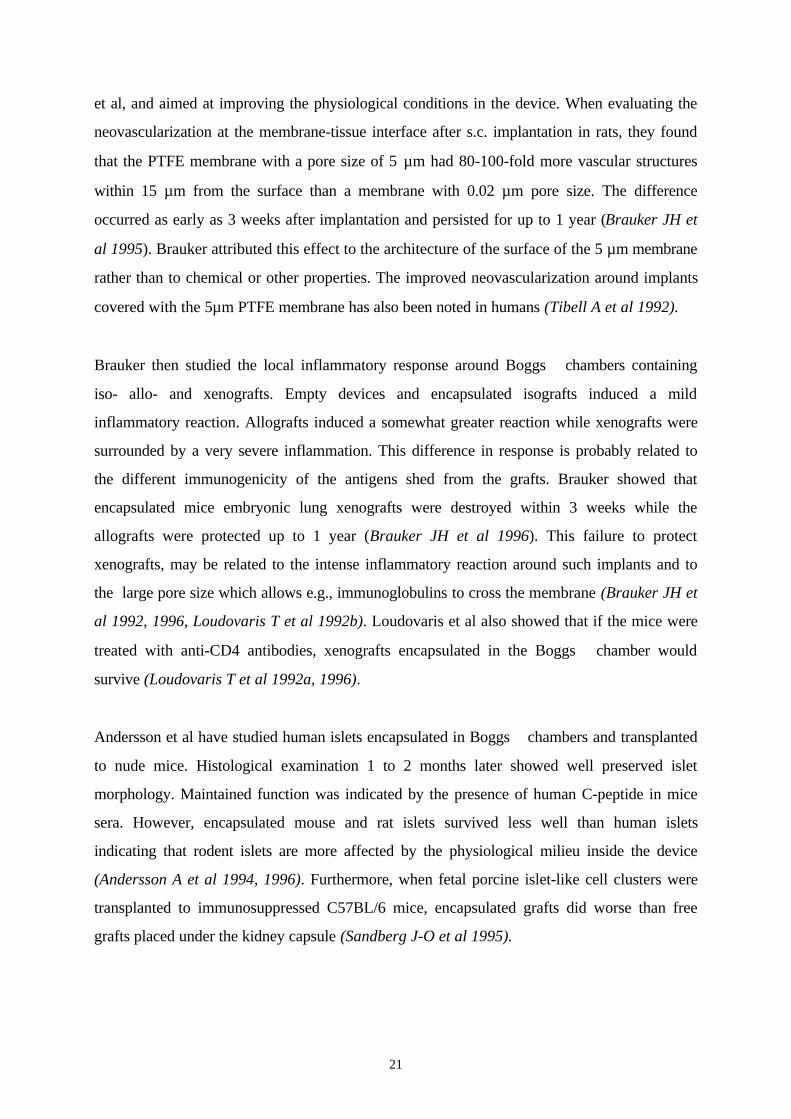
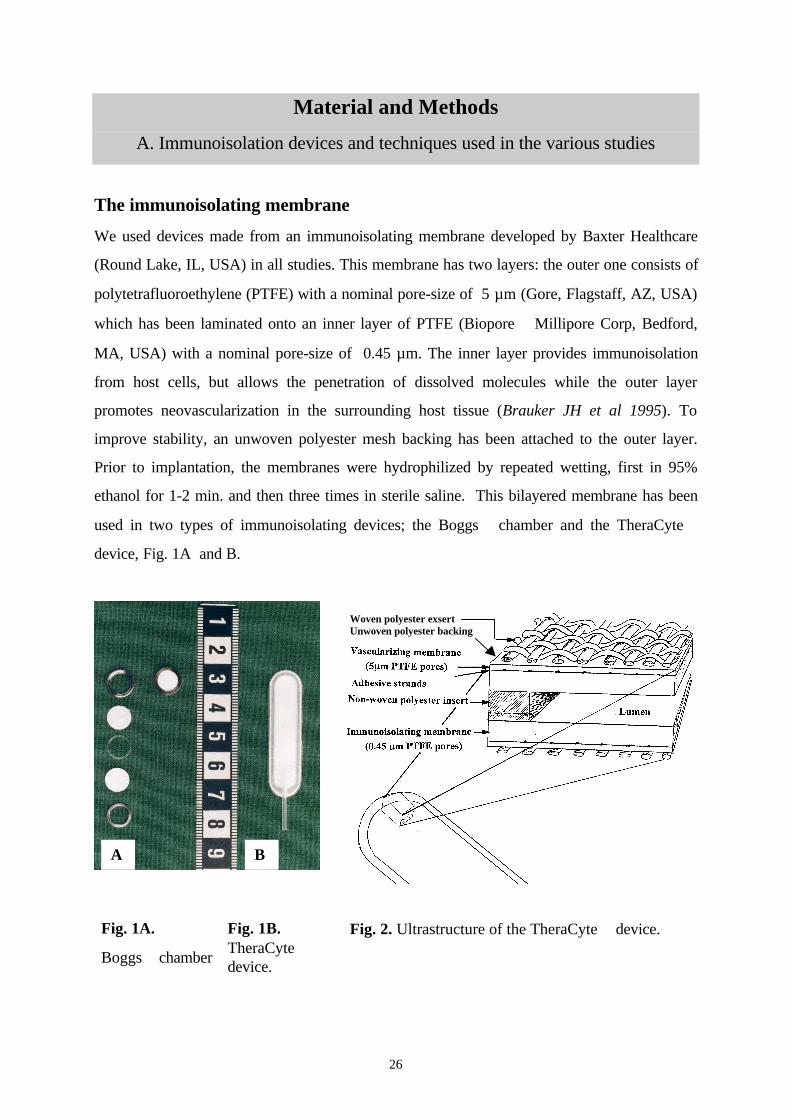
The immunoisolating membrane
We used devices made from an immunoisolating membrane developed by Baxter Healthcare
(Round Lake, IL, USA) in all studies. This membrane has two layers: the outer one consists of
polytetrafluoroethylene (PTFE) with a nominal pore-size of 5 µm (Gore, Flagstaff, AZ, USA)
which has been laminated onto an inner layer of PTFE (Biopore Millipore Corp, Bedford,
MA, USA) with a nominal pore-size of 0.45 µm. The inner layer provides immunoisolation
from host cells, but allows the penetration of dissolved molecules while the outer layer
promotes neovascularization in the surrounding host tissue (Brauker JH et al 1995). To
improve stability, an unwoven polyester mesh backing has been attached to the outer layer.
Prior to implantation, the membranes were hydrophilized by repeated wetting, first in 95%
ethanol for 1-2 min. and then three times in sterile saline. This bilayered membrane has been
used in two types of immunoisolating devices; the Boggs chamber and the TheraCyte
device, Fig. 1A and B.
Fig. 1A.
Boggs chamber
Fig. 1B.TheraCytedevice.
Fig. 2. Ultrastructure of the TheraCyte device.
Woven polyester exsertUnwoven polyester backing
A B
27
Devices used in various studies
The Boggs chamber (Baxter Health Care, Round Lake, IL, USA) belongs to the first
generation of the devices used in our trials. Its construction is shown in Fig. 1A. One
membrane is placed in a titanium ring. A silicon ring, to create a lumen, is placed on top and
the graft is loaded in the middle. The graft is then covered with another membrane and an
upper ring is pressed into the lower titanium ring to close the chamber. The volume of the
device is 5µl.
Boggs chambers were used in our first study for the encapsulation of human autologous
parathyroid grafts. These were implanted s.c. in the patient’s lower arm. Control devices were
placed s.c. in nude mice (Balbc/nu, Mollegaard Research and Breeding Center, Ry, Denmark).
The TheraCyte device is a prefabricated teabag-shaped device with a polyethylene port that
permits access to the lumen for loading, Fig. 1B. It was developed to provide a construction of
defined integrity which can be loaded with less risk of contamination of its outer surface. This
device is available in three sizes with internal volumes of 4.5 µl, 20 µl and 40 µl, respectively.
The outer surface of the TheraCyte device is covered with a woven polyester mesh in order
to improve further the stability of the construct, Fig 2.
TheraCyte devices were used in all our studies, except for the study on the autologous
parathyroid grafts (see above). In the first study, they were used to encapsulate the human
allogeneic parathyroid implants. The devices were then placed s.c. in the patient’s lower arm.
Nude mice (Balbc/nu) served as a control and received a s.c. device, loaded with the same
parathyroid tissue. In rat studies, the devices were placed s.c. on the back of male Sprague-
Dawley (SD) rats (ALAB, Sollentuna, Sweden) weighing 200-250g.
Techniques for studies of the exchange across the membrane and of blood
perfusion in tissue around the device
The microdialysis technique provides an in vivo bioanalytical sampling technique for
monitoring chemical events occurring in a living body. A great advantage of microdialysis is
that it is atraumatic and does not disturb the physiology of the tissue studied. It is based on
28
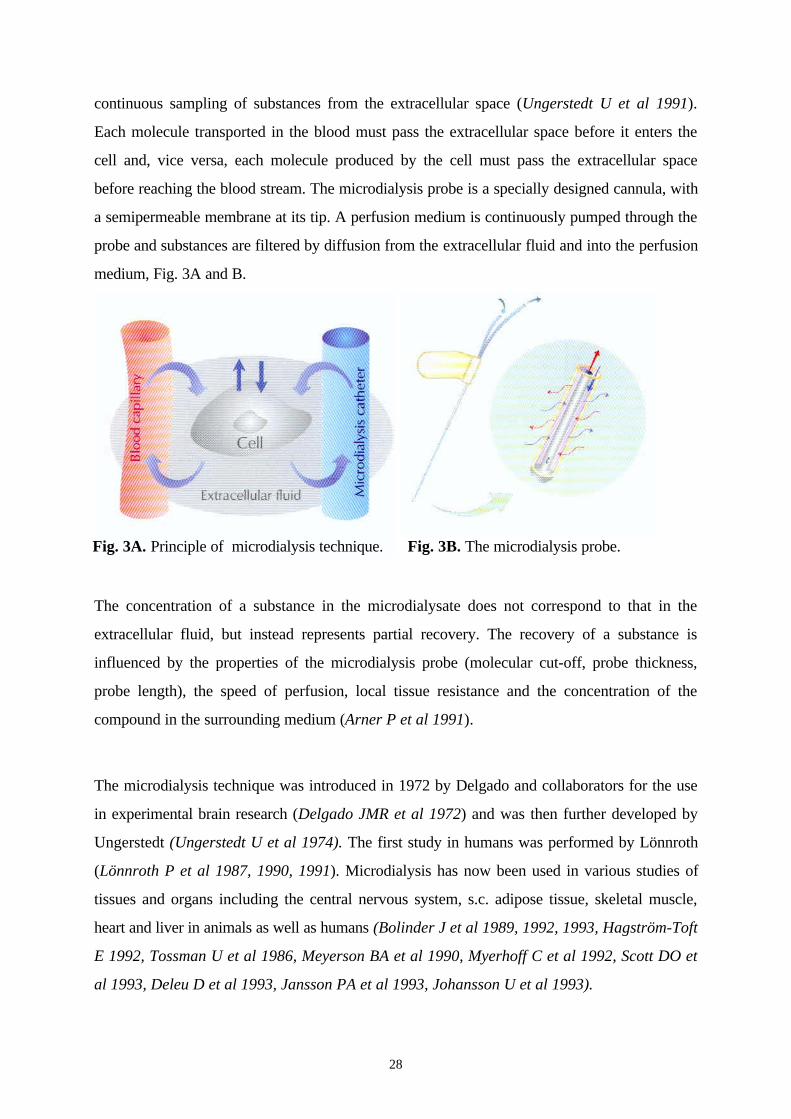
continuous sampling of substances from the extracellular space (Ungerstedt U et al 1991).
Each molecule transported in the blood must pass the extracellular space before it enters the
cell and, vice versa, each molecule produced by the cell must pass the extracellular space
before reaching the blood stream. The microdialysis probe is a specially designed cannula, with
a semipermeable membrane at its tip. A perfusion medium is continuously pumped through the
probe and substances are filtered by diffusion from the extracellular fluid and into the perfusion
medium, Fig. 3A and B.
The concentration of a substance in the microdialysate does not correspond to that in the
extracellular fluid, but instead represents partial recovery. The recovery of a substance is
influenced by the properties of the microdialysis probe (molecular cut-off, probe thickness,
probe length), the speed of perfusion, local tissue resistance and the concentration of the
compound in the surrounding medium (Arner P et al 1991).
The microdialysis technique was introduced in 1972 by Delgado and collaborators for the use
in experimental brain research (Delgado JMR et al 1972) and was then further developed by
Ungerstedt (Ungerstedt U et al 1974). The first study in humans was performed by Lönnroth
(Lönnroth P et al 1987, 1990, 1991). Microdialysis has now been used in various studies of
tissues and organs including the central nervous system, s.c. adipose tissue, skeletal muscle,
heart and liver in animals as well as humans (Bolinder J et al 1989, 1992, 1993, Hagström-Toft
E 1992, Tossman U et al 1986, Meyerson BA et al 1990, Myerhoff C et al 1992, Scott DO et
al 1993, Deleu D et al 1993, Jansson PA et al 1993, Johansson U et al 1993).
Fig. 3A. Principle of microdialysis technique. Fig. 3B. The microdialysis probe.
29
We used microdialysis to study the exchange of glucose and insulin between the device’s
lumen and the microcirculation. In our studies, the microdialysis probes had a length of 10 mm,
a thickness of 0.5 mm, and molecular cut-off of 20 000 dalton (glucose study) or 100 000
dalton (insulin study). In the glucose study, Ringer-acetate solution (Pharmacia AB,
Stockhom, Sweden) served as the perfusion medium, while an albumin-containing medium
(RIA test, Pharmacia AB, Stockholm, Sweden) was used in the insulin study. The speed of
perfusion was 2 ul min-1. The afferent part of the probe was connected to a microdialysis
pump (CMA 102, CMA Microdialysis, Stockholm, Sweden) and the efferent part was
connected to a microfraction collector (CMA 142, CMA Microdialysis, Stockholm, Sweden).
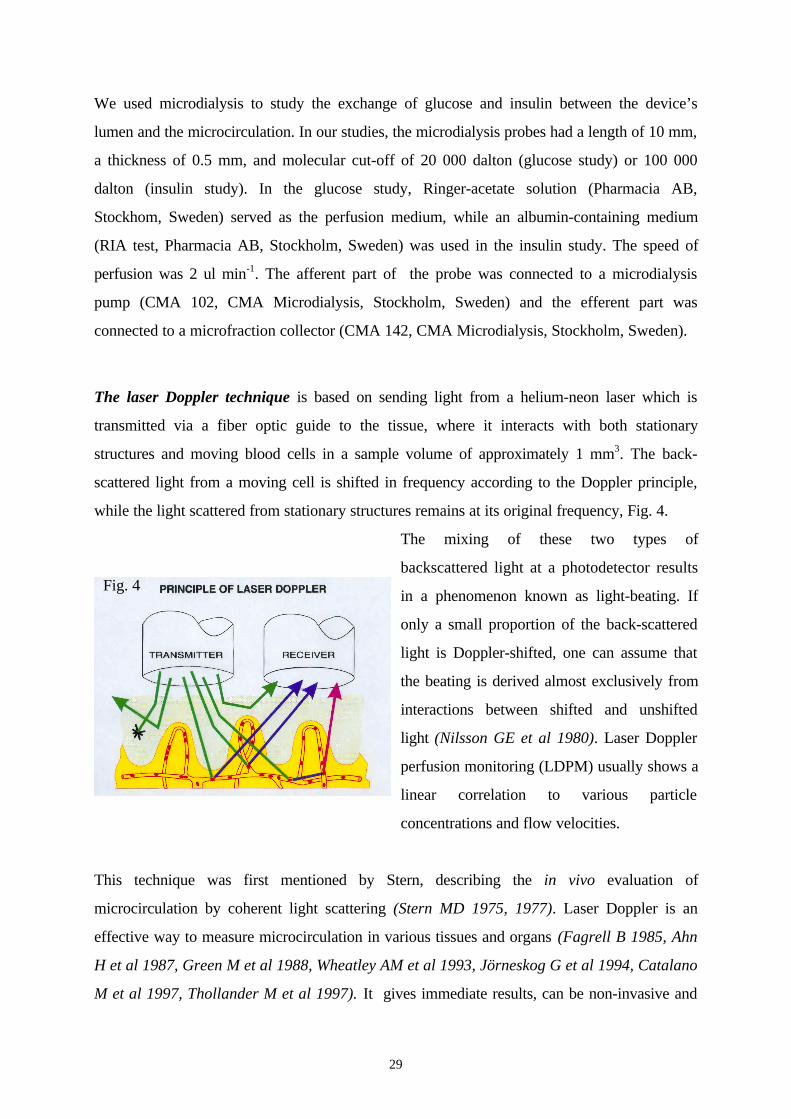
The laser Doppler technique is based on sending light from a helium-neon laser which is
transmitted via a fiber optic guide to the tissue, where it interacts with both stationary
structures and moving blood cells in a sample volume of approximately 1 mm3. The back-
scattered light from a moving cell is shifted in frequency according to the Doppler principle,
while the light scattered from stationary structures remains at its original frequency, Fig. 4.
The mixing of these two types of
backscattered light at a photodetector results
in a phenomenon known as light-beating. If
only a small proportion of the back-scattered
light is Doppler-shifted, one can assume that
the beating is derived almost exclusively from
interactions between shifted and unshifted
light (Nilsson GE et al 1980). Laser Doppler
perfusion monitoring (LDPM) usually shows a
linear correlation to various particle
concentrations and flow velocities.
This technique was first mentioned by Stern, describing the in vivo evaluation of
microcirculation by coherent light scattering (Stern MD 1975, 1977). Laser Doppler is an
effective way to measure microcirculation in various tissues and organs (Fagrell B 1985, Ahn
H et al 1987, Green M et al 1988, Wheatley AM et al 1993, Jörneskog G et al 1994, Catalano
M et al 1997, Thollander M et al 1997). It gives immediate results, can be non-invasive and
Fig. 4

30
allows repeated or continuous longitudinal measurements.
In our studies, laser Doppler was used to determine the blood perfusion in the tissue around
the TheraCyte device. A laser Doppler with a working wave length of 780 nm (PF 4001,
Perimed AB, Järfälla, Sweden) was used. The probe (PF 402 φ 0.5 mm, fiber separation 0.15
cm) was calibrated before each experiment, in accord with manufacturer’s instructions. The
laser Doppler equipment was connected to a computer and the Perisoft program (version 5.10
C2, Perimed AB, Järfälla, Sweden) was used to record data and basic calculations.
Preparation of rat islets
Pancreases were harvested from SD rats of the same inbred strain as the recipient rats. The
pancreatic islets were isolated using a modification of the technique described by Gray (Gray
DWR et al 1984 and 1986a, Hesse et al 1992) Collagenase solution (2 mg/ml, Sigma type VI,
Sigma Chemicals LTD, St. Louis, MO, USA) was injected into the bile duct until the pancreas
was well distended. The pancreatic tissue was then disintegrated at 37°C. The islets were
separated from exocrine tissue by centrifugation using a discontinuous Ficoll density gradient.
Isolated islets were then cultured at a temperature of 37 °C overnight, using RPMI 1640
medium (11.1 mM glucose, ICN Biomedicals, Costa Mesa, CA, USA), supplemented with
10% fetal calf serum and penicillin-streptomycin solution.
As a control for islet quality, implants were placed under the kidney capsule in nude mice.
Black 6 nu/nu mice (BomMice, Bomholt Gaard Breeding and Research Center LTD., Ry,
Denmark) weighing 25-30g were made diabetic by injecting streptozotocin i.v. (250 mg/kg
BW, Sigma Chemicals LTD). Diabetes was defined as a blood glucose level > 20 mmol/L for
two consecutive days. Each mouse received 450-500 rat islets, via a braking pipette, under the
left kidney capsule.
Histological studies
Preparation of histological specimens. The devices were explanted, together with a thin rim
of the surrounding s.c. tissue. Specimens were fixed in Histofix (Histolab Products AB, Västra
Frölunda, Sweden) or 4% phosphate-buffered formalin and then dehydrated and embedded in
paraffin according to routine methods. The blocks were cut in a microtome (Leica

31
Microsystems AB, Sollentuna, Sweden) with a section thickness of approximately 5 µm.
Sections were stained with hematoxylin-eosin. All histological evaluations were performed
with the light microscope by the same investigator. The sections were coded to ensure a
blinded evaluation.
Evaluation of encapsulated parathyroid tissue. All sections were qualitatively evaluated with
the light microscope. In the autologous implant study, semiquantitative estimates of
parathyroid tissue, fibrosis and necrosis were also made. On the section containing most tissue,
we estimated the volume densities (Vv´s) of these parameters by point-counting in a projection
microscope (magnification 300X), using a grid with 2.5 cm between the test points. The results
are presented as volume fractions (%). In the allogeneic implant study, the small devices
explanted from patients and nude mice were also evaluated by this semiquantitative technique.
Evaluation of vascular profiles and fibrosis around the TheraCyte device. The membranes
were divided longitudinally before embedding. We performed a semiquantitative evaluation of
vascular profiles on one central section. The number of vascular profiles within 15 µm from the
surface was counted along the entire length of the membrane on both sides (approx. 7.5 cm)
with the light microscope. In addition, in Paper III, micrographs were taken along one cm in
the middle of the membrane on both membrane surfaces (final magnification x 325). On these
micrographs, we counted the number of vascular profiles within 250 µm from the surface of
the membrane. The values were expressed as the number of vascular profiles/cm. The thickness
of the fibrous tissue reaction around the device, also measured at eight evenly distributed
points along each membrane surface, was expressed as a mean thickness (µm) for each device.
Morphometric studies of encapsulated islet grafts. After the entire membranes had been
embedded, serial transverse sectioning was performed. Sections at intervals of 400 µm were
stained with hematoxylin and eosin for histological evaluation. Approximately 25-30 section-
levels were evaluated from each membrane. Six pairs of devices were evaluated by
morphometry, using stereological techniques. From the sections containing grafted tissue in the
device, micrographs were taken, covering the entire area of the graft. The area of the tissue
was then measured on printed copies at a final magnification of 30.5x in a semiautomatic
interactive image analyzer (Videoplan, Zeiss, Oberkuchen, Germany). The total volume of the

32
encapsulated graft could then be calculated according to Cavalier’s principle (Sterio DC 1984).
Every other section containing grafted tissue was then evaluated in a computer-assisted
stereological system (Cast GRID System, Olympus, Albertslund, Denmark). At a final
magnification of 390x, point-counting was performed in every other visual field. Conventional
stereological principles were used to estimate volume densities (Vv´s) of viable endocrine cells,
fibrotic and necrotic tissue and the absolute volumes of these parameters were then calculated
(Weibel ER et al 1979).
Evaluation of subcapsular islet grafts in control nude mice. The graft-bearing kidneys from
control nude mice were evaluated qualitatively with the light microscope.
Immunohistochemistry. In the encapsulated parathyroid grafts, the presence of viable
parathyroid cells was verified by immunohistochemistry, using an antiserum against human
parathyroid hormone 1-38 (Peninsula Laboratories Inc, St. Helens, Merseyside, England). In
encapsulated islet grafts and islet graft-bearing kidneys, the presence of viable islets was
verified by using antibodies against insulin (Dako, Glostrup, Denmark).
Biochemical methods
The serum levels of human intact PTH were analyzed by an immunoradiometric assay (IRMA,
Nichols Institute of Diagnostics, San Juan Capistrano, CA, USA). This intact PTH assay has a
sensitivity of 1 ng/L and a reference interval of 8 - 51 ng/L. The insulin levels in the
microdialysates were analyzed with a RIA kit (Pharmacia AB, Uppsala, Sweden). The blood
glucose levels in capillary samples from the tail vein in rats and mice were analyzed on site
using a blood glucose meter (Glucometer Elite, Bayer Diagnostics, Gothenburg, Sweden).
The measuring range of this meter is 1.1 - 33.3 mmol/L. For analyses of glucose
concentrations in the mecrodialysates, we diluted the microdialysate samples (10µl) by adding
20 µl distilled water and performed the analyses twice, using a Select Biochemistry Analyzer
(YSI model 2700, Yellow Springs, OH, USA).
Immunological methods
33
Mixed lymphocytic culture was performed using a pool of MNC cells as the positive control.
The stimulator cells were inactivated by irradiation with 20 Gy. The tests were performed in a
microculture system and were harvested on day 6 (Solheim BG et al 1993). MLC reactivity
was expressed as relative response (RR). The RR was defined as cpm of [(R + Dx) - (R + Rx)
/ (R + Px) - (R + Rx)] *100, where P is the pooled control, R= recipient cells, D= donor cells
and X= irradiated fraction.
Analysis of panel-reactive antibodies. Analyses of antibodies against unfractionated
lymphocytes and enriched T cells was made against a panel of lymphocytes using an ordinary
microlymphocytotoxicity test with incubation for 90 minutes, at 37°C. Screening for B cell
antibodies was performed against the same panel according to the standard NIH technique,
with incubation for 195 minutes at 22°C. The cytotoxic reaction was judged to be positive
when at least 50% of the individual panel lymphocytes were killed. The patient’s serum was
judged to be positive if it reacted with more than 10% of the panel. Sera with B cell antibodies
were platelet-absorbed and retested against the T and B cell panels.
Data presentation
Results are presented as mean ± SD. A p-value of <0.05 was considered statistically
significant. The methods used for the statistical analyses are presented in each individual study.
Material and Methods
B. Designs of the individual studies
In the patient studies, informed consent was obtained from all participants. The patient study
protocols were approved by the local ethics committee. In the animal studies, study protocols
were approved by the animal ethics committee. The experimental studies were performed in
accordance with “Principals of Laboratory Animal Care” published by NIH and Swedish
Legislation for the protection of animals.
34
Paper I. Histological studies on the survival of encapsulated autologous and
allogeneic parathyroid tissue in humans.
Autologous parathyroid transplantation study. To study the survival of encapsulated
parathyroid tissue in the absence of an alloresponse, six patients received a s.c. implant of their
own parathyroid tissue in conjunction with an operation for parathyroid hyperplasia. One
patient with a parathyroid adenoma was also included. The tissue was minced with
microscissors and encapsulated in a Boggs chamber. The devices were explanted after 2 or 4
weeks for histological evaluation. For comparison, encapsulated tissue from five of seven
patients was also placed s.c. in nude mice and explanted after the same period.
Allogeneic parathyroid transplantation study. In this study, four patients with
hypoparathyroidism and unstable calcium levels, in spite of pharmacological treatment,
received macroencapsulated allogeneic parathyroid grafts. The donors were patients
undergoing parathyroidectomy due to parathyroid adenoma or parathyroid hyperplasia. They
were blood group-compatible but HLA-mismatched in relation to the recipients. The patients
received no immunosuppressive or anti-inflammatory drugs.
One to three 40µl TheraCyte devices were implanted s.c. in each patient’s lower arm. In 3
patients, a small device holding 4.5 µl was also implanted sc. and removed after 4 weeks to
evaluate early changes in the implanted tissue. The large devices were explanted 8.5-14 months
after implantation. During the follow-up period, blood samples for analyses of parathyroid
hormone were obtained from both arms at least twice monthly. Mixed lymphocyte culture
(MLC) was performed in the four donor-recipient pairs. Peripheral blood leukocytes (PBL)
from the donor were isolated and frozen at the time of donation. PBL from the recipient were
obtained before implantation and during the follow-up period, the last sample being taken at
the time of explantation. Panel reactive antibodies were analyzed in sera obtained before
implantation and at the time of explantation.
In three of the four allogeneic implant cases, a nude mouse was transplanted with encapsulated
parathyroid tissue from the same donor as a control. The mice implants were also harvested
after 4 weeks. All devices were prepared for histology and evaluated as described above.
35
Paper II. Longitudinal studies on the insulin permeability of the TheraCyte
device and histological evaluation of close vascular profiles.
In vitro studies. To determine the recovery of insulin with our microdialysis set-up, recoveries
at various insulin concentrations were studied in vitro. Solutions of human insulin (Actrapid,
Novo Nordisk, Bagsvaerd, Denmark) at concentrations of 100 (n=2), 200 (n=2) and 300 (n=3)
µU/ml were prepared by adding a dilution medium (Pharmacia RIA test, Uppsala, Sweden)
containing albumin. The microdialysis probe was immersed in a test tube containing one of the
three insulin concentrations and microdialysate samples were collected every 15 minutes up to
180 minutes in plastic tubes (CMA Microdialysis, Stockholm, Sweden) and frozen at - 20 °C,
pending analysis.
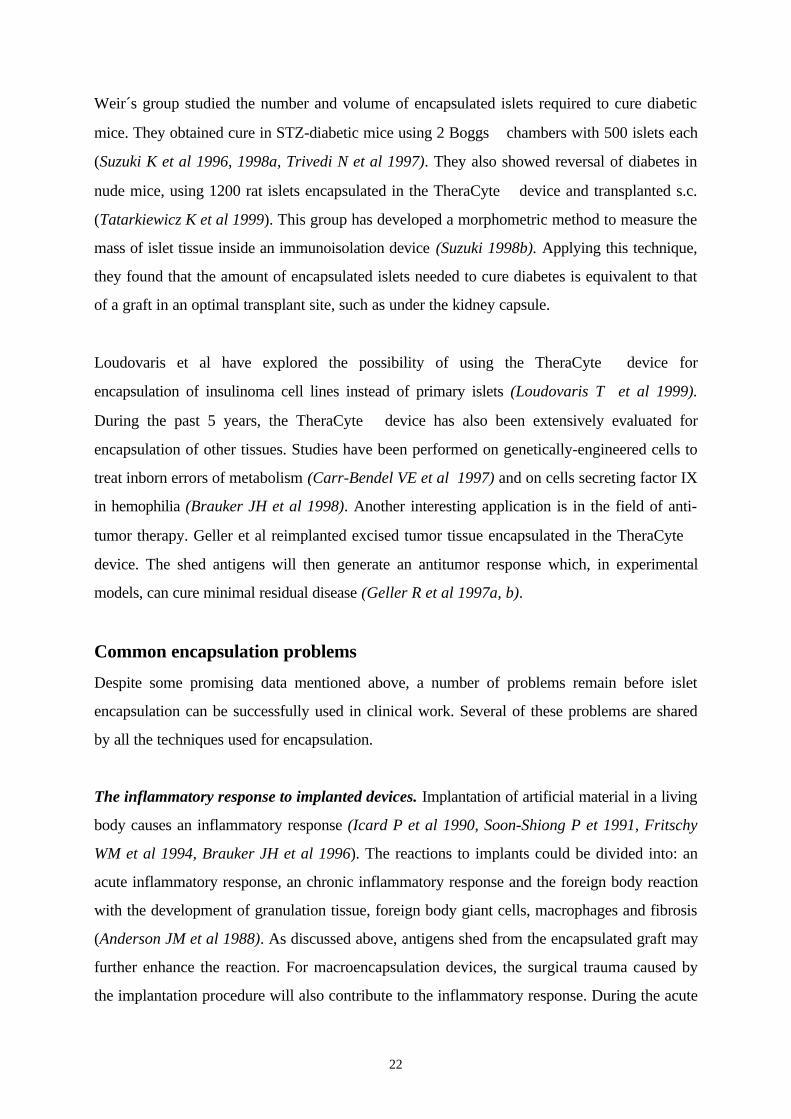
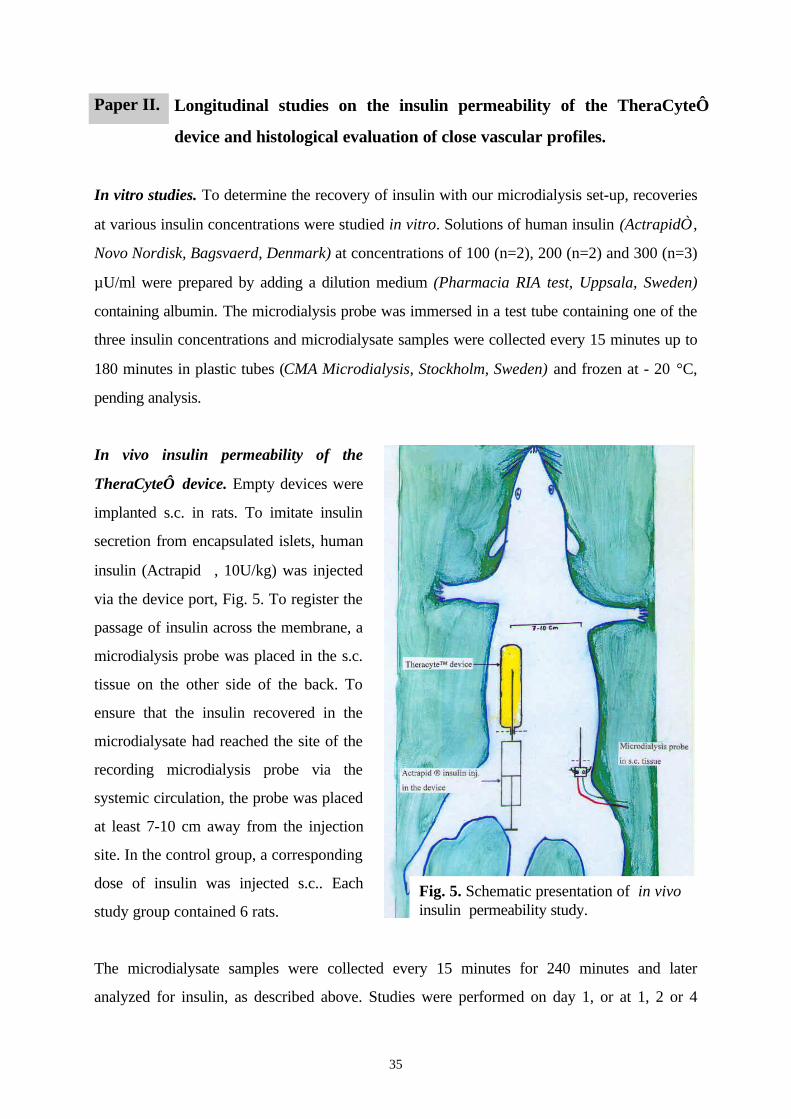
In vivo insulin permeability of the
TheraCyte device. Empty devices were
implanted s.c. in rats. To imitate insulin
secretion from encapsulated islets, human
insulin (Actrapid, 10U/kg) was injected
via the device port, Fig. 5. To register the
passage of insulin across the membrane, a
microdialysis probe was placed in the s.c.
tissue on the other side of the back. To
ensure that the insulin recovered in the
microdialysate had reached the site of the
recording microdialysis probe via the
systemic circulation, the probe was placed
at least 7-10 cm away from the injection
site. In the control group, a corresponding
dose of insulin was injected s.c.. Each
study group contained 6 rats.
The microdialysate samples were collected every 15 minutes for 240 minutes and later
analyzed for insulin, as described above. Studies were performed on day 1, or at 1, 2 or 4
Fig. 5. Schematic presentation of in vivoinsulin permeability study.
36
weeks and 3 months after implantation of the device. The blood glucose levels of the rats were
followed during the experiment. Histological evaluation of close vascular profiles was
performed on devices that had been implanted at least 1 week or more.
The area under the curve (AUC), the time-to-peak (TTP) and peak concentrations of insulin
(Cmax) were calculated for the various groups. The k-values (percentage of change in insulin
concentration/minute) were also calculated for the ascending and descending parts of the
curves. For the ascending parts, k-values (ka) were calculated between 15 and 90 minutes
while, for the descending parts of the curves, k-values (kd) were calculated from the point
where the curve started to descend until the end of the experiment. Analysis of variance
(ANOVA) and the unpaired Student’s t test, with Bonferroni’s correction were used for the
statistical evaluation.
Paper III. Longitudinal studies on the glucose permeability of the TheraCyte
device and histological evaluation of vascular profiles around the implant.
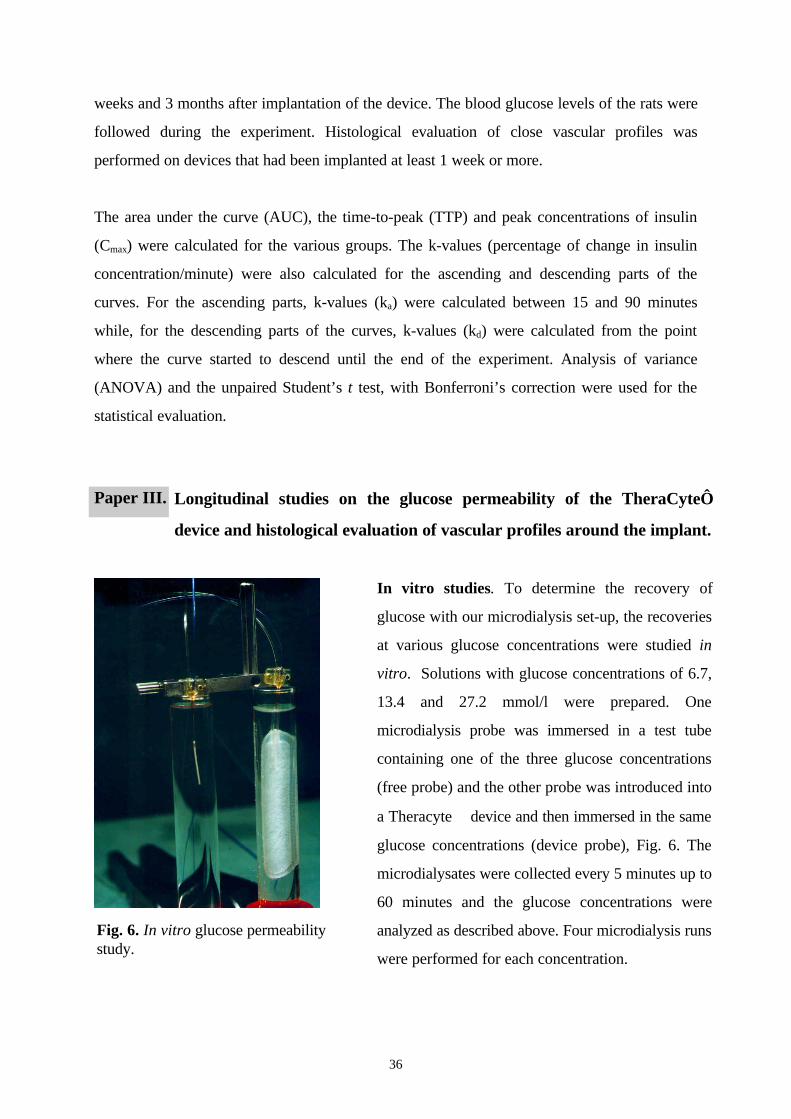
In vitro studies. To determine the recovery of
glucose with our microdialysis set-up, the recoveries
at various glucose concentrations were studied in
vitro. Solutions with glucose concentrations of 6.7,
13.4 and 27.2 mmol/l were prepared. One
microdialysis probe was immersed in a test tube
containing one of the three glucose concentrations
(free probe) and the other probe was introduced into
a Theracyte device and then immersed in the same
glucose concentrations (device probe), Fig. 6. The
microdialysates were collected every 5 minutes up to
60 minutes and the glucose concentrations were
analyzed as described above. Four microdialysis runs
were performed for each concentration.
Fig. 6. In vitro glucose permeabilitystudy.
37
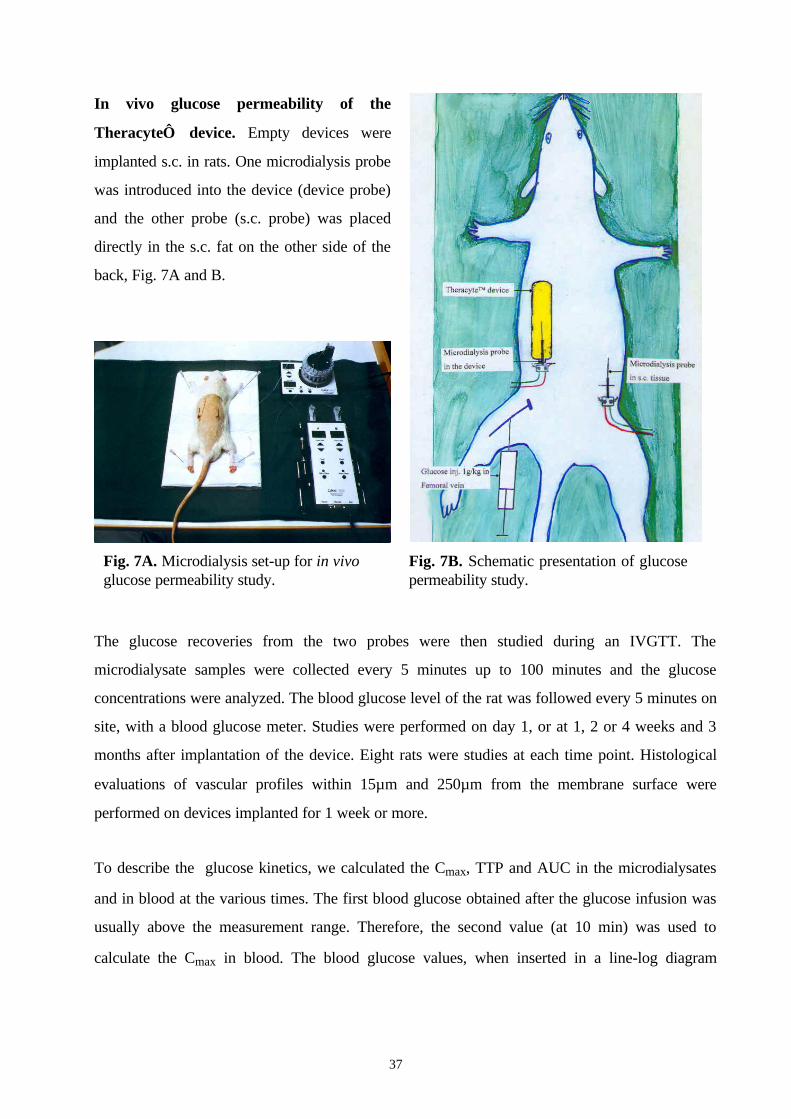
In vivo glucose permeability of the
Theracyte device. Empty devices were
implanted s.c. in rats. One microdialysis probe
was introduced into the device (device probe)
and the other probe (s.c. probe) was placed
directly in the s.c. fat on the other side of the
back, Fig. 7A and B.
The glucose recoveries from the two probes were then studied during an IVGTT. The
microdialysate samples were collected every 5 minutes up to 100 minutes and the glucose
concentrations were analyzed. The blood glucose level of the rat was followed every 5 minutes on
site, with a blood glucose meter. Studies were performed on day 1, or at 1, 2 or 4 weeks and 3
months after implantation of the device. Eight rats were studies at each time point. Histological
evaluations of vascular profiles within 15µm and 250µm from the membrane surface were
performed on devices implanted for 1 week or more.
To describe the glucose kinetics, we calculated the Cmax, TTP and AUC in the microdialysates
and in blood at the various times. The first blood glucose obtained after the glucose infusion was
usually above the measurement range. Therefore, the second value (at 10 min) was used to
calculate the Cmax in blood. The blood glucose values, when inserted in a line-log diagram
Fig. 7A. Microdialysis set-up for in vivoglucose permeability study.
Fig. 7B. Schematic presentation of glucosepermeability study.
38
showed a biphasic disappearance pattern. Therefore, we analyzed AUC for these two periods
separately, AUC 0-40 and AUC 40-100.
For longitudinal comparisons of the glucose kinetics in blood at various times, analysis of
variance (ANOVA) and the unpaired Student’s t-test, with Bonferroni’s correction, were
performed. For comparisons of the glucose kinetics in s.c. fat and in the device at each time-point,
Wilcoxon’s matched-pairs signed-rank tests were used. To compare the number of vascular
profiles in the various groups, ANOVA and the unpaired Student’s t-test with Bonferroni’s
correction were used. Relations between the numbers of vascular profiles at 1, 4 weeks and 3
months and glucose kinetics were evaluated by linear regression analysis.
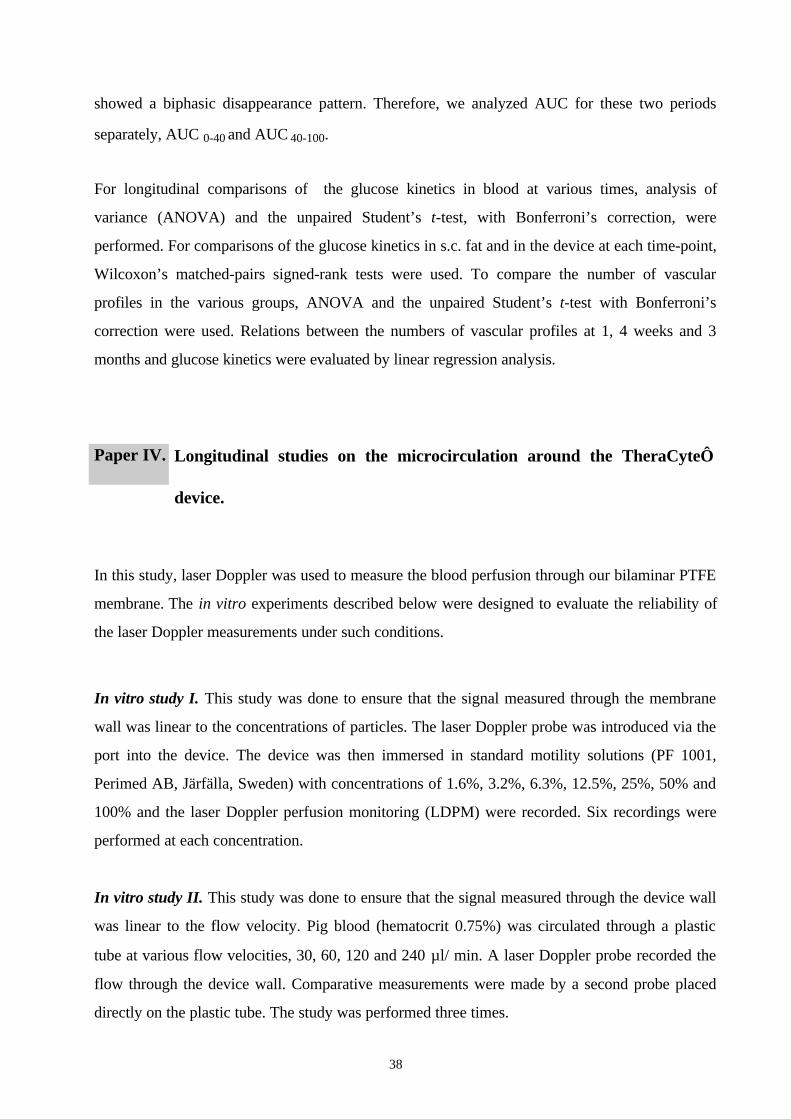
Paper IV. Longitudinal studies on the microcirculation around the TheraCyte
device.
In this study, laser Doppler was used to measure the blood perfusion through our bilaminar PTFE
membrane. The in vitro experiments described below were designed to evaluate the reliability of
the laser Doppler measurements under such conditions.
In vitro study I. This study was done to ensure that the signal measured through the membrane
wall was linear to the concentrations of particles. The laser Doppler probe was introduced via the
port into the device. The device was then immersed in standard motility solutions (PF 1001,
Perimed AB, Järfälla, Sweden) with concentrations of 1.6%, 3.2%, 6.3%, 12.5%, 25%, 50% and
100% and the laser Doppler perfusion monitoring (LDPM) were recorded. Six recordings were
performed at each concentration.
In vitro study II. This study was done to ensure that the signal measured through the device wall
was linear to the flow velocity. Pig blood (hematocrit 0.75%) was circulated through a plastic
tube at various flow velocities, 30, 60, 120 and 240 µl/ min. A laser Doppler probe recorded the
flow through the device wall. Comparative measurements were made by a second probe placed
directly on the plastic tube. The study was performed three times.

39
In vivo measurements of the perfusion around the TheraCyte device. We then evaluated the
microcirculation around empty TheraCyte devices implanted s.c. in rats. Studies were
performed on day 1 or at 1, 2, 4 weeks or at 2, 3 and 12 months after implantation. Ten rats were
studied at each time point.
A laser Doppler probe was introduced via the
device port and tissue perfusion was
measured from the bottom of the device and
every 5 mm for a total of 30 mm, Fig. 8.
Since the rats were studied at various times
after implantation, their weights at the time of
evaluation ranged between 250-450g. To
investigate whether this growth also caused
changes in the perfusion of the s.c. tissue, we
performed control studies in 2 groups of rats,
one weighing approximately 250g and
another weighing approximately 450g.
In these control studies, the laser Doppler probe was placed on the side of the back,
corresponding to the site used for device implantation, and the perfusion was measured every 5
mm for a total of 30 mm. Each control group contained 6 rats.
The rat's temperature was kept stable during the experiments (37°-38°C), using temperature
controller CMA/150 (CMA Microdialysis, Stockholm, Sweden). A catheter was introduced into
the carotid artery and the arterial blood pressure of the rats was monitored continuously during
the experiment (GRASS Polygraph, Model 7D and Gould P231D transducer, Quincy, MA,
USA). Only rats with a stable mean arterial blood pressure (85-110 mmHg) were included in the
analysis. The LDPM are presented as mean perfusion units (PU). Kruskal-Wallis and Dunn’s
multiple comparison tests were used for the analyses.
Fig. 8. Laser Doppler set-up for in vivostudies of blood perfusion around the device.

40
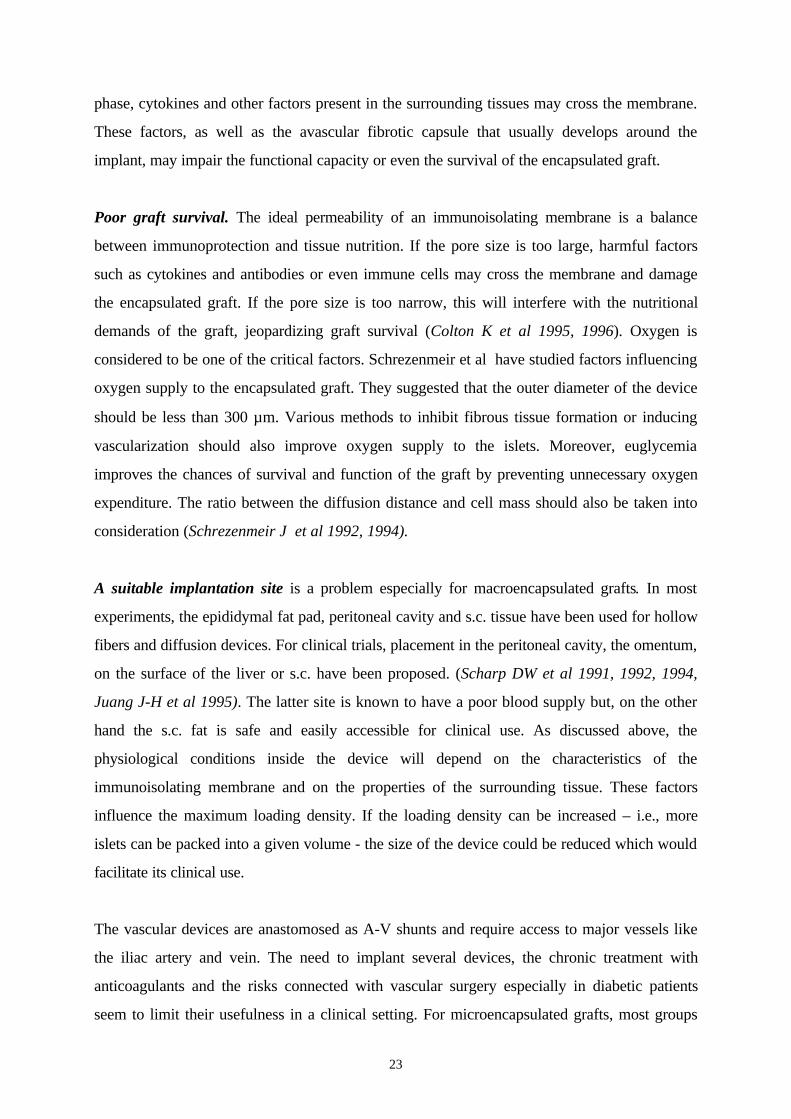
Paper V. Evaluation of preimplantation as a method to improve survival of
encapsulated islet grafts.
Empty 20µl TheraCyte devices were
implanted s.c. in SD rats. After 3 months
another device loaded with 1500 syngeneic rat
islets was implanted s.c. in the free side of the
back. The device implanted 3 months earlier
was opened and loaded in situ with 1500 islets
from the same isolation, Fig. 9. Both devices
were explanted two weeks later. The
specimens were serially sectioned and
stereological analyses of the encapsulated islet
graft were performed, as described above. The
volume densities and absolute volumes of
viable endocrine cells, fibrotic tissue and
necrosis were estimated. Six pairs of devices
were evaluated.
The Wilcoxon signed rank test was used to compare the results in the preimplanted and non-
preimplanted devices.
As a control for islet quality, islets from the same batch were also transplanted under the kidney
capsule of a diabetic nude mouse. The blood glucose levels of the mice were monitored for 8
weeks. The grafts were then explanted for histological evaluation and blood sugar levels were
followed for another three days.
Fig. 9. Schematic presentation of thepreimplantation study.
TheraCytedevice pre-implanted for3 months
TheraCyte deviceimplanted day 0
Hamilton syringeloading 1 500islets in situ.
41
Results and Discussion
Paper I. Histological studies on the survival of encapsulated autologous and allogeneic
parathyroid tissue in humans.
In the first paper of this thesis, we studied the use of a macroencapsulation device for
transplantation of human parathyroid tissue. To determine whether human parathyroid tissue
could survive under the physiological conditions present in the device, we took tissue from
patients operated on for hyperparathyroidism and implanted as encapsulated autologous grafts.
Since we wanted to evaluate graft survival in the presence of an immune response, we also
implanted encapsulated allogeneic grafts in patients with chronic hypoparathyroidism. Control
implants were performed in nude mice.
The histological findings in the autologous grafts 2-4 weeks after implantation were similar in
the devices implanted in humans, Figs. I:1A and B (see appendix), and nude mice. The mean
percentages of viable endocrine tissue were 22±7 in humans vs. 30±11 in nude mice. Fibrosis
was seen in 63±7% vs. 51±17% while the remaining parts of the grafts were necrotic.
These results indicate that the physiological conditions in the chamber can fulfill the
requirements of parathyroid tissue –i.e., in the best cases, 35-44% of the implants consisted of
viable endocrine cells.
In the following allogeneic study each patient received multiple implants. These were well
tolerated, and no local tenderness or macroscopic signs of inflammation or capsule formation
occurred around the devices. When the small control devices explanted at 4 weeks were
evaluated histologically, marked fibrosis was seen inside the devices and only 1%, 5% and 23%
of the implants, respectively, consisted of viable endocrine tissue. Similar findings were
observed in the grafts implanted in nude mice, Figs. I:2A and B (see appendix). However, the
lymphocytic inflammation around the devices was more marked in humans than in nude mice.
The large devices were explanted at 14, 13, 11 and 8.5 months after implantation, respectively.
Only a few clusters of surviving endocrine cells were identified. The rest of the grafts consisted
42
of fibrotic tissue, Fig. I:3 (see appendix). The implants were surrounded by a foreign body
reaction with fibrosis and the lymphocytic inflammation around the devices had increased
slightly, compared to that after 4 weeks. No significant improvements in calcium levels or in
serum PTH levels occurred after transplantation.
Two patients showed increases in their donor-specific mixed lymphocyte reactivity after
transplantation but no patient developed increased levels of panel reactive antibodies.
Discussion. Hypoparathyroidism will not become a common indication for allotransplantation,
but transplantation of parathyroid tissue can serve as a good model when evaluating
encapsulation techniques. The amount of tissue needed for a measurable effect is small, thereby
avoiding problems with up-scaling the size of the device and limiting the trauma to the patient.
Moreover, parathyroid tissue is easily accessible and graft function can be assessed by
measurements of PTH levels. In contrast to the diabetic population, a patient with
hypoparathyroidism is at a low risk of needing an organ transplant and thus the development of
HLA antibodies is less likely to be a disadvantage for the patient. In the future, encapsulation
may become a valuable therapeutic alternative for some of these patients who are not well
managed by conventional treatment.
The results in the autologous study indicate that this device can fulfill the physiological
requirements of parathyroid tissue. However, in the allogeneic implants the percentage of
endocrine cells at 4 weeks was usually lower than in the autologous ones - in the best case,
23%. The amount of fibrotic tissue was even greater than in the autografts. A mild-to-
moderate infiltration of mononuclear cells occurred around the allografts and two patients
increased their lymphocyte reactivity against the parathyroid donor. It is possible that
immunological factors contributed to the outcome as allo-antigens will shed through the
membrane and may activate the immune system. This should increase the production of
cytokines and other mediators of inflammation in the surrounding tissue and these factors may
cross the membrane and damage the graft (Zekorn T et al 1990, Brauker JH et al 1996).
However, experiments in rodents indicate that this membrane is alloprotective, even if it has
not been previously evaluated in humans (Brauker JH et al 1992, Loudovaris T et al 1992a,
b). Furthermore, previous experimental studies indicate that the risk of sensitization is
43
significantly reduced if islets are encapsulated instead of transplanted as free grafts (Tibell A et
al 1999). In the present study, none of the patients receiving of parathyroid allografts
developed panel reactive antibodies. Particularly note worthy is, that the amounts of surviving
endocrine tissue was similar in devices placed in T-cell-deficient mice as in those implanted in
the patients. This indicates that the quality of the parathyroid tissue or an inadequate
physiological milieu rather than immunological factors were responsible for the poor graft
survival.
The different methods used for preparation of autografts and allografts may also have affected
the results. Loading of the TheraCyte device used in the allogeneic study requires that the
tissue is broken down into smaller fragments. This procedure disrupted the tissue architecture
and may also have damaged the endocrine cells, thereby making way for the more robust
fibroblasts. In future studies, less traumatic methods for preparation of the parathyroid tissue
should be sought (Wozniewisc B et al 1996).
To improve the physiological conditions for the encapsulated cells, the TheraCyte device
was designed using a membrane with an outer layer that induces neovascularization of the
device surface (Brauker JH et al 1995). Nevertheless, survival of our encapsulated parathyroid
grafts was unsatisfactory. Likewise, in an unpublished pilot study in which encapsulated human
islets were implanted s.c. in volunteers, histological graft survival was poor (Tibell A et al,
personal communication).
Since encapsulated grafts are dependent on the diffusion of oxygen and nutrients from the
surrounding microcirculation an insufficient exchange across the membrane will negatively
affect graft survival. The permeability of immunoisolating membranes have so far usually been
defined only in vitro. However, after implantation, the exchange may be affected by additional
factors, including protein deposits in the membrane, and various degrees of edema,
vascularization and fibrosis in the surrounding tissue. Thus, in vitro testing does not necessarily
reflect the in vivo characteristics of a device. The following two studies were designed to
improve our understanding of the in vivo performance of the TheraCyte device as regards
the exchange between the device lumen and the microcirculation and how it changes over time.
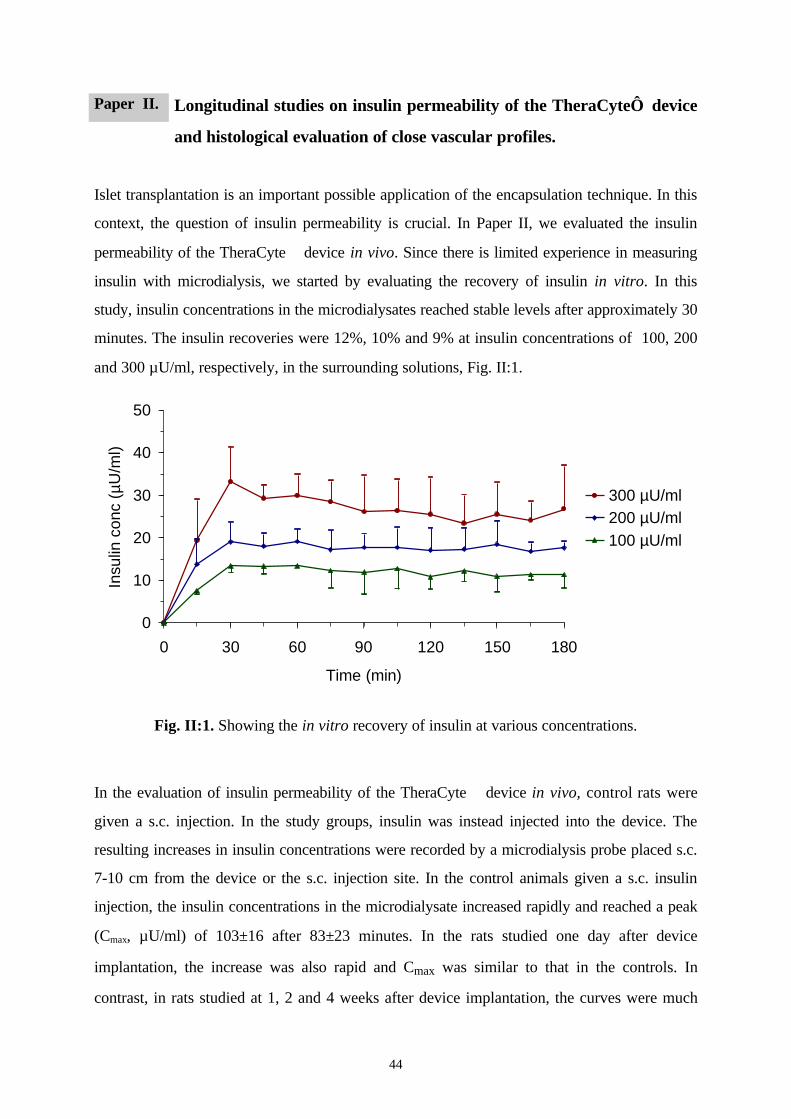
44
Paper II. Longitudinal studies on insulin permeability of the TheraCyte device
and histological evaluation of close vascular profiles.
Islet transplantation is an important possible application of the encapsulation technique. In this
context, the question of insulin permeability is crucial. In Paper II, we evaluated the insulin
permeability of the TheraCyte device in vivo. Since there is limited experience in measuring
insulin with microdialysis, we started by evaluating the recovery of insulin in vitro. In this
study, insulin concentrations in the microdialysates reached stable levels after approximately 30
minutes. The insulin recoveries were 12%, 10% and 9% at insulin concentrations of 100, 200
and 300 µU/ml, respectively, in the surrounding solutions, Fig. II:1.
0
10
20
30
40
50
0 30 60 90 120 150 180
Time (min)
Insu
lin c
onc
(µU
/ml)
300 µU/ml200 µU/ml100 µU/ml
Fig. II:1. Showing the in vitro recovery of insulin at various concentrations.
In the evaluation of insulin permeability of the TheraCyte device in vivo, control rats were
given a s.c. injection. In the study groups, insulin was instead injected into the device. The
resulting increases in insulin concentrations were recorded by a microdialysis probe placed s.c.
7-10 cm from the device or the s.c. injection site. In the control animals given a s.c. insulin
injection, the insulin concentrations in the microdialysate increased rapidly and reached a peak
(Cmax, µU/ml) of 103±16 after 83±23 minutes. In the rats studied one day after device
implantation, the increase was also rapid and Cmax was similar to that in the controls. In
contrast, in rats studied at 1, 2 and 4 weeks after device implantation, the curves were much
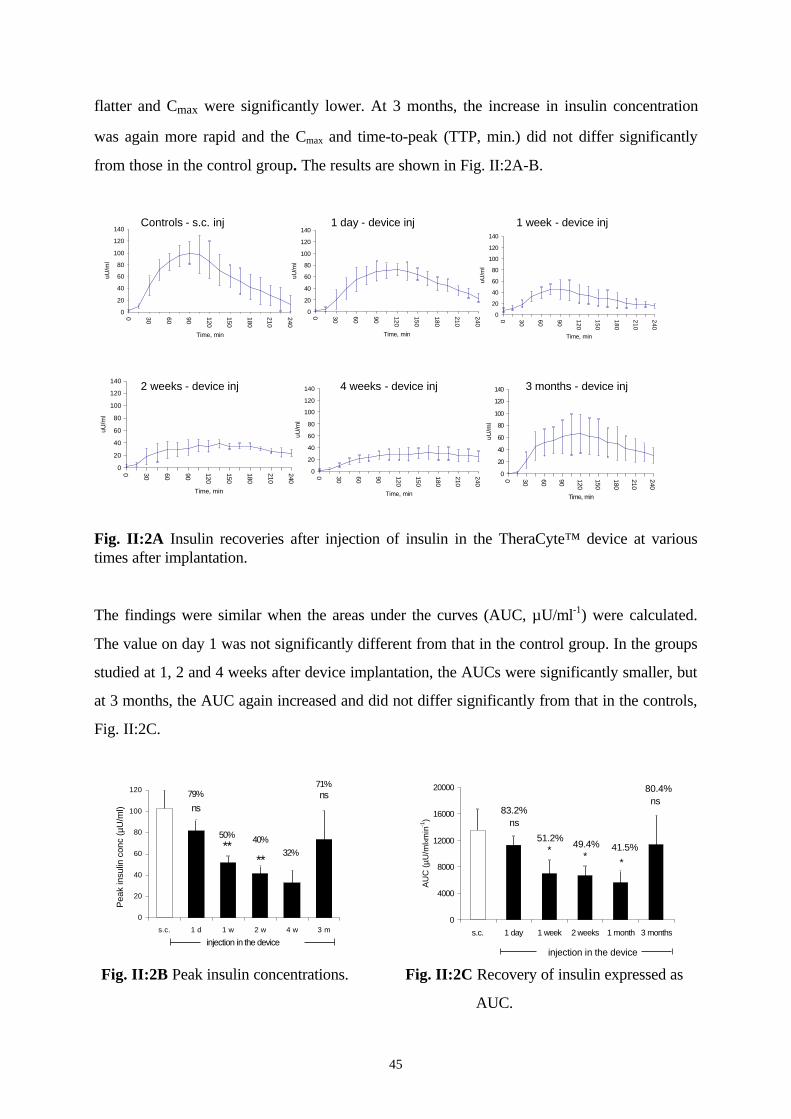
45
flatter and Cmax were significantly lower. At 3 months, the increase in insulin concentration
was again more rapid and the Cmax and time-to-peak (TTP, min.) did not differ significantly
from those in the control group. The results are shown in Fig. II:2A-B.
0
20
40
60
80
100
120
140
0 30 60 90 120
150
180
210
240
Time, min
uU/m
l
0
20
40
60
80
100
120
140
0 30 60 90 120
150
180
210
240
Time, min
uU/m
l
0
20
40
60
80
100
120
140
0 30 60 90 120
150
180
210
240
Time, minuU
/ml
0
20
40
60
80
100
120
140
0 30 60 90 120
150
180
210
240
Time, min
uU/m
l
Controls - s.c. inj
3 months - device inj
1 day - device inj 1 week - device inj
0
20
40
60
80
100
120
140
0 30 60 90 120
150
180
210
240Time, min
uU/m
l
0
20
40
60
80
100
120
140
0 30 60 90 120
150
180
210
240
Time, min
uU/m
l
2 weeks - device inj 4 weeks - device inj
Fig. II:2A Insulin recoveries after injection of insulin in the TheraCyte™ device at varioustimes after implantation.
The findings were similar when the areas under the curves (AUC, µU/ml-1) were calculated.
The value on day 1 was not significantly different from that in the control group. In the groups
studied at 1, 2 and 4 weeks after device implantation, the AUCs were significantly smaller, but
at 3 months, the AUC again increased and did not differ significantly from that in the controls,
Fig. II:2C.
0
20
40
60
80
100
120
s.c. 1 d 1 w 2 w 4 w 3 m
79%
50% 40%32%
71%
injection in the device
****
nsns
Pea
k in
sulin
con
c (µ
U/m
l)
ns
ns
* **
83.2%
51.2%49.4% 41.5%
80.4%
injection in the device
0
4000
8000
12000
16000
20000
s.c. 1 day 1 week 2 weeks 1 month 3 months
AU
C (µ
U/m
lx min
-1)
Fig. II:2B Peak insulin concentrations. Fig. II:2C Recovery of insulin expressed as
AUC.
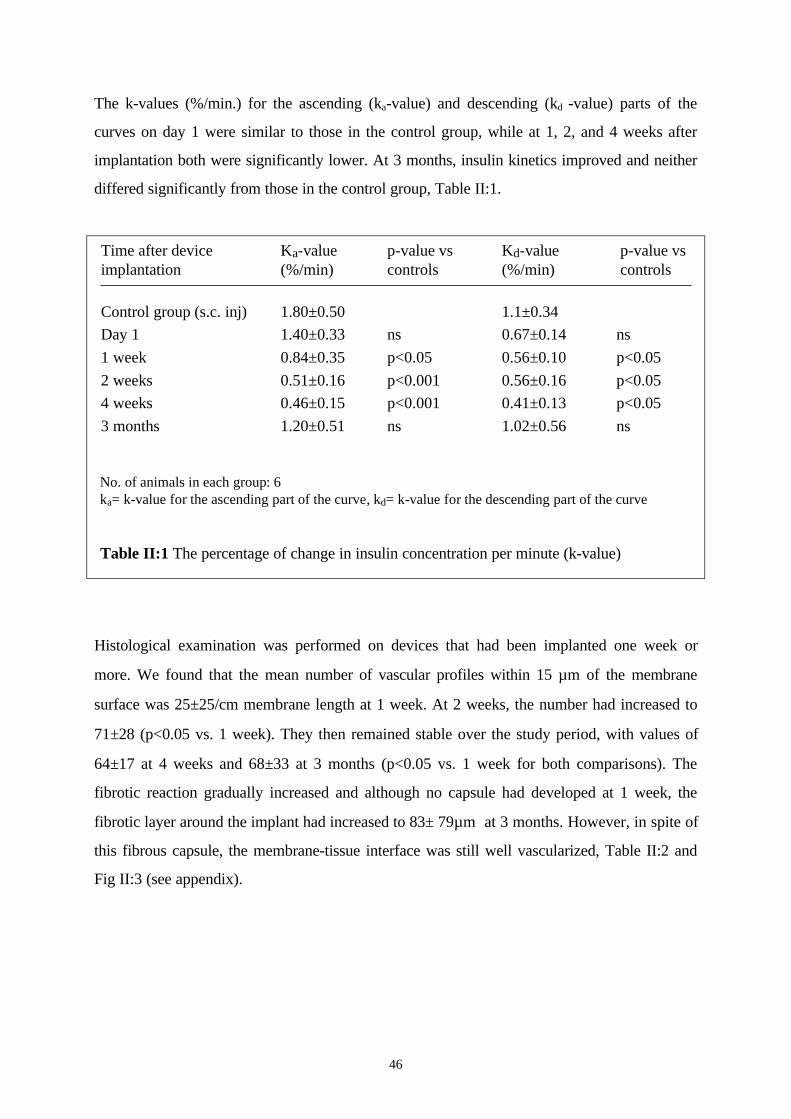
46
The k-values (%/min.) for the ascending (ka-value) and descending (kd -value) parts of the
curves on day 1 were similar to those in the control group, while at 1, 2, and 4 weeks after
implantation both were significantly lower. At 3 months, insulin kinetics improved and neither
differed significantly from those in the control group, Table II:1.
Time after device Ka-value p-value vs Kd-value p-value vsimplantation (%/min) controls (%/min) controls
Control group (s.c. inj) 1.80±0.50 1.1±0.34Day 1 1.40±0.33 ns 0.67±0.14 ns1 week 0.84±0.35 p<0.05 0.56±0.10 p<0.052 weeks 0.51±0.16 p<0.001 0.56±0.16 p<0.054 weeks 0.46±0.15 p<0.001 0.41±0.13 p<0.053 months 1.20±0.51 ns 1.02±0.56 ns
No. of animals in each group: 6ka= k-value for the ascending part of the curve, kd= k-value for the descending part of the curve
Histological examination was performed on devices that had been implanted one week or
more. We found that the mean number of vascular profiles within 15 µm of the membrane
surface was 25±25/cm membrane length at 1 week. At 2 weeks, the number had increased to
71±28 (p<0.05 vs. 1 week). They then remained stable over the study period, with values of
64±17 at 4 weeks and 68±33 at 3 months (p<0.05 vs. 1 week for both comparisons). The
fibrotic reaction gradually increased and although no capsule had developed at 1 week, the
fibrotic layer around the implant had increased to 83± 79µm at 3 months. However, in spite of
this fibrous capsule, the membrane-tissue interface was still well vascularized, Table II:2 and
Fig II:3 (see appendix).
Table II:1 The percentage of change in insulin concentration per minute (k-value)

47
Time point No of vascular p vs Fibrosisprofiles within 15µ 1 week
1 week 25±10.3 - none2 weeks 70.6±11.5 p<0.05 4±74 weeks 64.3±6.9 p<0.05 53±413 months 68.2±10.9 p<0.05 83±79
Discussion. This study was designed to investigate the in vivo performance of an
immunoisolating device designed for encapsulation of secretory cells, such as pancreatic islets.
Normalization of the glucose metabolism in a diabetic recipient requires a rapid exchange of
insulin and glucose across the immunoisolating membrane. Thus, the diffusion barrier is
important not only for survival but also for the functional characteristics of the encapsulated
graft.
The in vivo diffusion barrier depends partly on the immunoisolating membrane but also on the
tissue reaction in the recipient. The development of an avascular foreign body reaction around
an implant, a common problem in the fields of macro- and microencapsulation, interferes with
the survival and function of the encapsulated islets, while well vascularized surrounding tissue
should be favorable (Anderson JM 1988). Thus, good biocompatability will facilitate graft
survival (Lum ZP et al 1991, Reach G et al, 1992, 1993, 1994, Lanza RP et al 1992b, c, d,
1996 and 1997a, Fan MY et al 1992, Clayton HA et al 1993, Zekorn T et al 1996).
In this study, insulin permeability of the TheraCyte device was studied in vivo at various
times after s.c. implantation of the device in rats. On day 1 after implantation, neither the
membrane nor the surrounding tissue reaction constituted a significant diffusion barrier for
insulin. However, in the studies performed between 1 and 4 weeks after device implantation,
the amounts of insulin recovered were lower and the changes in insulin concentrations
occurred more slowly than in the control group.
Table II:2. Histological evaluation of vascularization and fibrosis around the TheraCyte™ device.
48
Our main finding was, that although the diffusion barrier increased during the first 4 weeks, the
insulin recovery then improved. At 3 months after implantation, the insulin kinetics had almost
returned to baseline and was not significantly different from that in the control group. This is a
rather unexpected finding, since several publications have reported that an avascular fibrotic
capsule develops around the implant during the first months after implantation (Theodorou NA
et al 1988, Icard P et al 1990, Brauker JH et al 1996).
One explanation might be changes in, or even degradation of, the membrane material.
However, this is unlikely, since the devices have proved alloprotective for up to one year after
implantation. (Brauker JH et al 1996, own unpublished data). Changes in the surrounding
tissue seemed to be a more likely explanation. The neovascularization observed may improve
the transfer of insulin from the device to the systemic circulation. However, there was a time
lag between the occurrence of an increased number of vessels and the improved recovery of
insulin. This finding may indicate that the function of these new capillaries takes time to
develop fully.
Our results underline the importance of defining the functional characteristics of
macroencapsulation devices, not only in vitro but also in vivo, at various times after
implantation. To substantiate our findings further, we decided to study the permeability of a
low molecular weight substance of great importance in islet transplantation -i.e., glucose.
Paper III. Longitudinal studies on glucose permeability of the TheraCyte device and
histological evaluation of the vascular profiles around the implant.
In this study, we used microdialysis to evaluate glucose permeability of the TheraCyte device
at various times after s.c. implantation in rats. By introducing a microdialysis probe into the
device and another probe into the s.c. tissue, we compared the environment in the device to
that outside it during IVGTT. Thus, the in vivo diffusion barrier of the immunoisolation device
was evaluated.
First, the glucose permeability of the TheraCyte device was studied in vitro. The mean
glucose levels in the microdialysates recovered from free probes perfused in vitro were 36%,
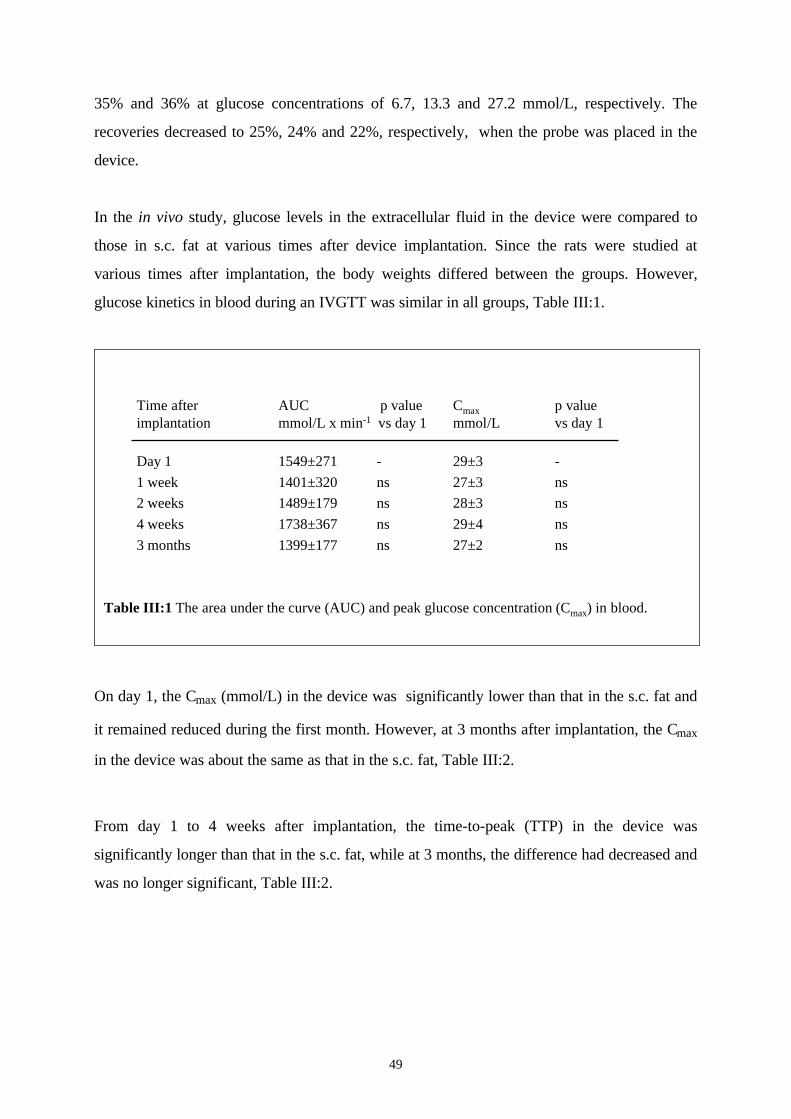
49
35% and 36% at glucose concentrations of 6.7, 13.3 and 27.2 mmol/L, respectively. The
recoveries decreased to 25%, 24% and 22%, respectively, when the probe was placed in the
device.
In the in vivo study, glucose levels in the extracellular fluid in the device were compared to
those in s.c. fat at various times after device implantation. Since the rats were studied at
various times after implantation, the body weights differed between the groups. However,
glucose kinetics in blood during an IVGTT was similar in all groups, Table III:1.
Time after AUC p value Cmax p valueimplantation mmol/L x min-1 vs day 1 mmol/L vs day 1
Day 1 1549±271 - 29±3 -1 week 1401±320 ns 27±3 ns2 weeks 1489±179 ns 28±3 ns4 weeks 1738±367 ns 29±4 ns3 months 1399±177 ns 27±2 ns
Table III:1 The area under the curve (AUC) and peak glucose concentration (Cmax) in blood.
On day 1, the Cmax (mmol/L) in the device was significantly lower than that in the s.c. fat and
it remained reduced during the first month. However, at 3 months after implantation, the Cmax
in the device was about the same as that in the s.c. fat, Table III:2.
From day 1 to 4 weeks after implantation, the time-to-peak (TTP) in the device was
significantly longer than that in the s.c. fat, while at 3 months, the difference had decreased and
was no longer significant, Table III:2.
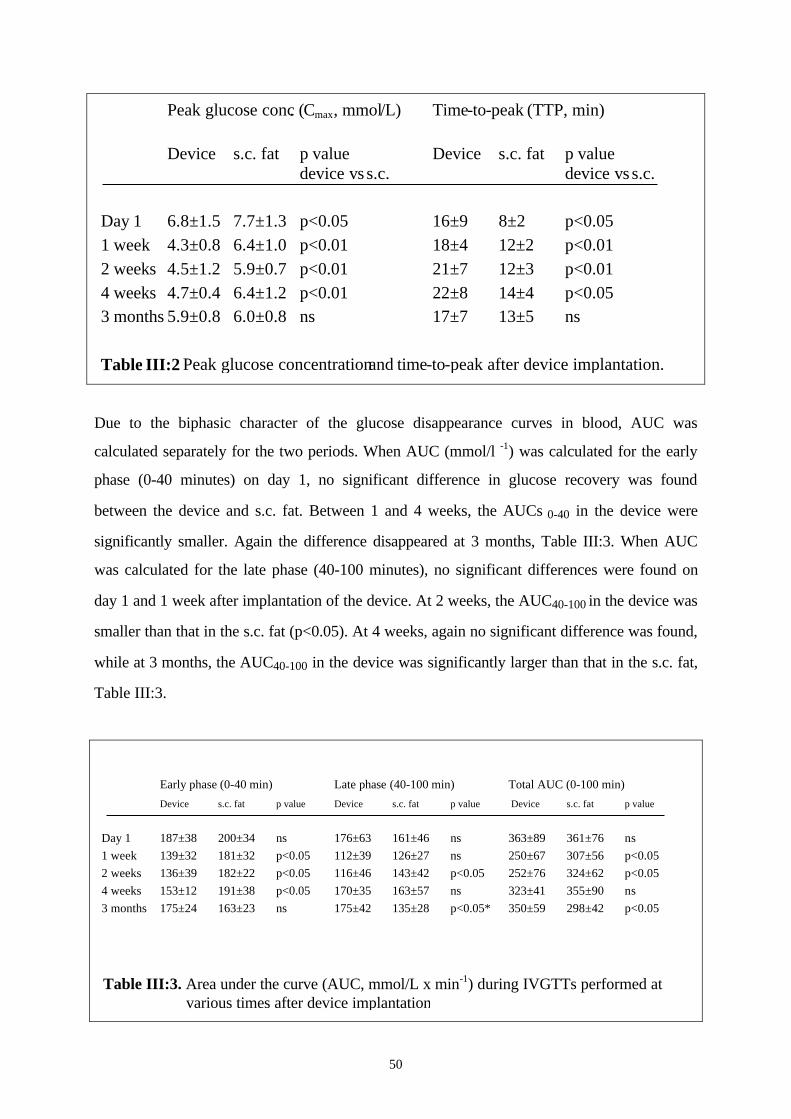
50
Peak glucose conc. (Cmax, mmol/L) Time-to-peak (TTP, min)
Device s.c. fat p value Device s.c. fat p valuedevice vs s.c. device vs s.c.
Day 1 6.8±1.5 7.7±1.3 p<0.05 16±9 8±2 p<0.051 week 4.3±0.8 6.4±1.0 p<0.01 18±4 12±2 p<0.012 weeks 4.5±1.2 5.9±0.7 p<0.01 21±7 12±3 p<0.014 weeks 4.7±0.4 6.4±1.2 p<0.01 22±8 14±4 p<0.053 months 5.9±0.8 6.0±0.8 ns 17±7 13±5 ns
Table III:2 Peak glucose concentrationand time-to-peak after device implantation.
Due to the biphasic character of the glucose disappearance curves in blood, AUC was
calculated separately for the two periods. When AUC (mmol/l -1) was calculated for the early
phase (0-40 minutes) on day 1, no significant difference in glucose recovery was found
between the device and s.c. fat. Between 1 and 4 weeks, the AUCs 0-40 in the device were
significantly smaller. Again the difference disappeared at 3 months, Table III:3. When AUC
was calculated for the late phase (40-100 minutes), no significant differences were found on
day 1 and 1 week after implantation of the device. At 2 weeks, the AUC40-100 in the device was
smaller than that in the s.c. fat (p<0.05). At 4 weeks, again no significant difference was found,
while at 3 months, the AUC40-100 in the device was significantly larger than that in the s.c. fat,
Table III:3.
Early phase (0-40 min) Late phase (40-100 min) Total AUC (0-100 min)
Device s.c. fat p value Device s.c. fat p value Device s.c. fat p value
Day 1 187±38 200±34 ns 176±63 161±46 ns 363±89 361±76 ns1 week 139±32 181±32 p<0.05 112±39 126±27 ns 250±67 307±56 p<0.052 weeks 136±39 182±22 p<0.05 116±46 143±42 p<0.05 252±76 324±62 p<0.054 weeks 153±12 191±38 p<0.05 170±35 163±57 ns 323±41 355±90 ns3 months 175±24 163±23 ns 175±42 135±28 p<0.05* 350±59 298±42 p<0.05
Table III:3. Area under the curve (AUC, mmol/L x min-1) during IVGTTs performed at various times after device implantation
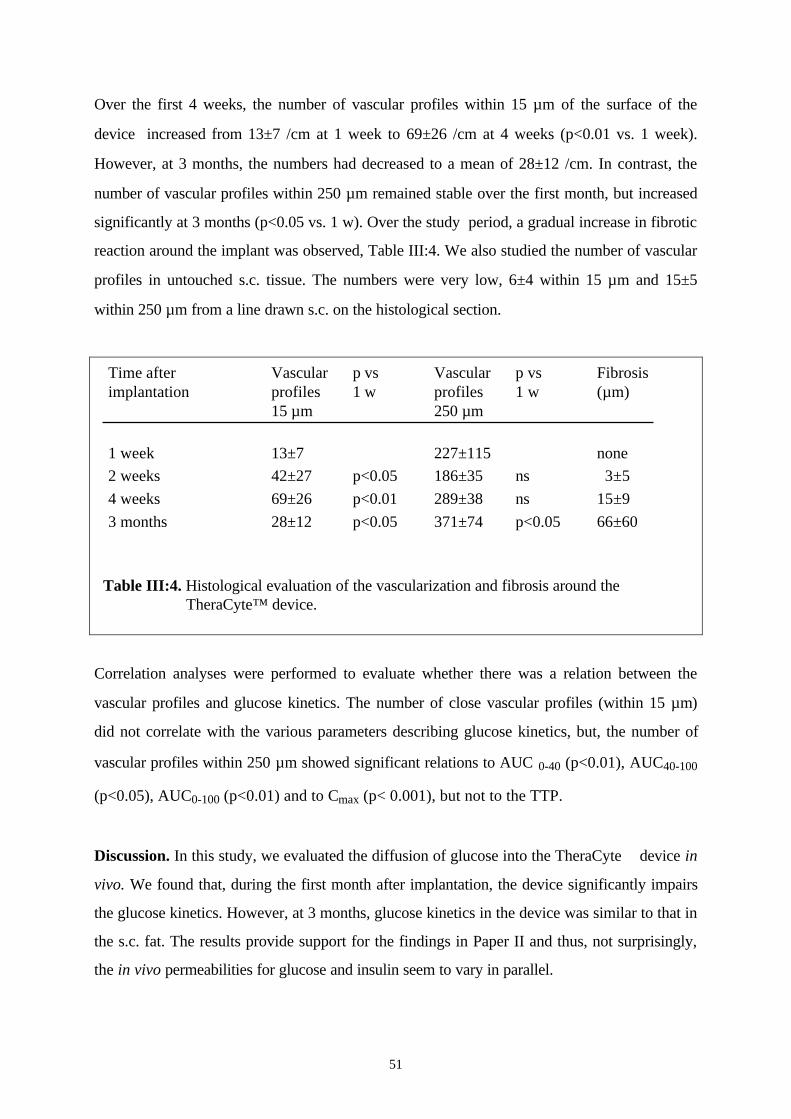
51
Over the first 4 weeks, the number of vascular profiles within 15 µm of the surface of the
device increased from 13±7 /cm at 1 week to 69±26 /cm at 4 weeks (p<0.01 vs. 1 week).
However, at 3 months, the numbers had decreased to a mean of 28±12 /cm. In contrast, the
number of vascular profiles within 250 µm remained stable over the first month, but increased
significantly at 3 months (p<0.05 vs. 1 w). Over the study period, a gradual increase in fibrotic
reaction around the implant was observed, Table III:4. We also studied the number of vascular
profiles in untouched s.c. tissue. The numbers were very low, 6±4 within 15 µm and 15±5
within 250 µm from a line drawn s.c. on the histological section.
Time after Vascular p vs Vascular p vs Fibrosisimplantation profiles 1 w profiles 1 w (µm)
15 µm 250 µm
1 week 13±7 227±115 none2 weeks 42±27 p<0.05 186±35 ns 3±54 weeks 69±26 p<0.01 289±38 ns 15±93 months 28±12 p<0.05 371±74 p<0.05 66±60
Correlation analyses were performed to evaluate whether there was a relation between the
vascular profiles and glucose kinetics. The number of close vascular profiles (within 15 µm)
did not correlate with the various parameters describing glucose kinetics, but, the number of
vascular profiles within 250 µm showed significant relations to AUC 0-40 (p<0.01), AUC40-100
(p<0.05), AUC0-100 (p<0.01) and to Cmax (p< 0.001), but not to the TTP.
Discussion. In this study, we evaluated the diffusion of glucose into the TheraCyte device in
vivo. We found that, during the first month after implantation, the device significantly impairs
the glucose kinetics. However, at 3 months, glucose kinetics in the device was similar to that in
the s.c. fat. The results provide support for the findings in Paper II and thus, not surprisingly,
the in vivo permeabilities for glucose and insulin seem to vary in parallel.
Table III:4. Histological evaluation of the vascularization and fibrosis around the TheraCyte™ device.
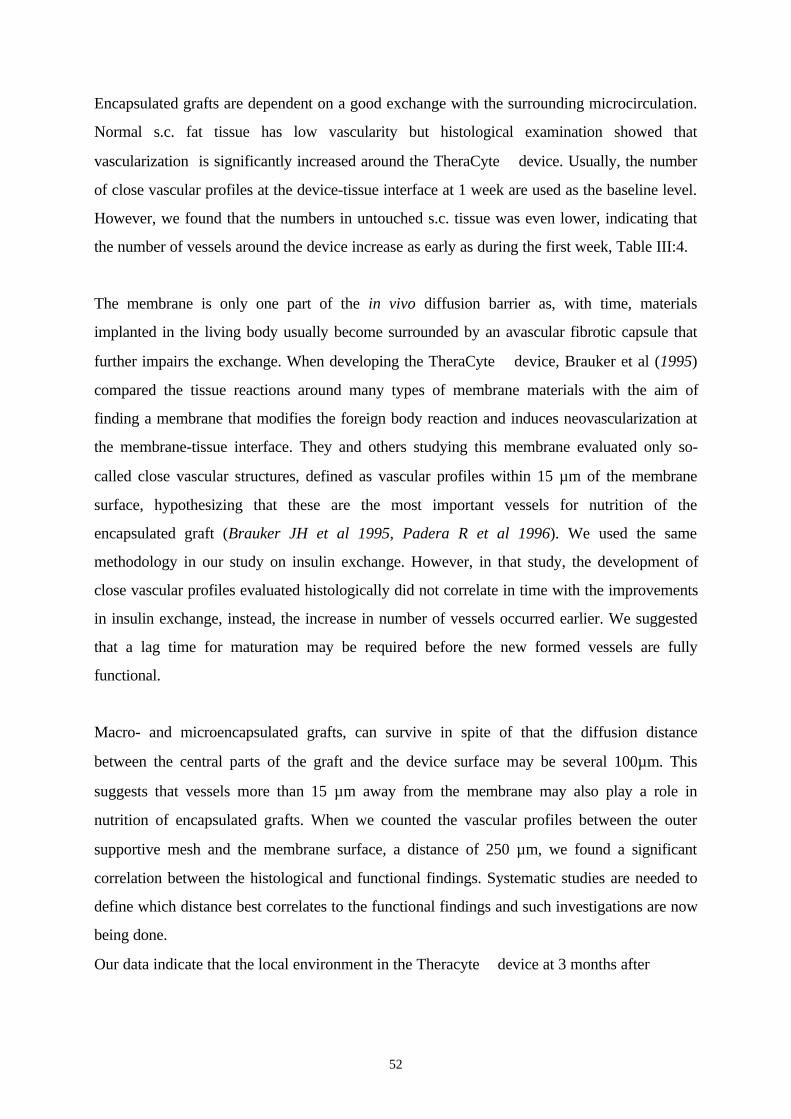
52
Encapsulated grafts are dependent on a good exchange with the surrounding microcirculation.
Normal s.c. fat tissue has low vascularity but histological examination showed that
vascularization is significantly increased around the TheraCyte device. Usually, the number
of close vascular profiles at the device-tissue interface at 1 week are used as the baseline level.
However, we found that the numbers in untouched s.c. tissue was even lower, indicating that
the number of vessels around the device increase as early as during the first week, Table III:4.
The membrane is only one part of the in vivo diffusion barrier as, with time, materials
implanted in the living body usually become surrounded by an avascular fibrotic capsule that
further impairs the exchange. When developing the TheraCyte device, Brauker et al (1995)
compared the tissue reactions around many types of membrane materials with the aim of
finding a membrane that modifies the foreign body reaction and induces neovascularization at
the membrane-tissue interface. They and others studying this membrane evaluated only so-
called close vascular structures, defined as vascular profiles within 15 µm of the membrane
surface, hypothesizing that these are the most important vessels for nutrition of the
encapsulated graft (Brauker JH et al 1995, Padera R et al 1996). We used the same
methodology in our study on insulin exchange. However, in that study, the development of
close vascular profiles evaluated histologically did not correlate in time with the improvements
in insulin exchange, instead, the increase in number of vessels occurred earlier. We suggested
that a lag time for maturation may be required before the new formed vessels are fully
functional.
Macro- and microencapsulated grafts, can survive in spite of that the diffusion distance
between the central parts of the graft and the device surface may be several 100µm. This
suggests that vessels more than 15 µm away from the membrane may also play a role in
nutrition of encapsulated grafts. When we counted the vascular profiles between the outer
supportive mesh and the membrane surface, a distance of 250 µm, we found a significant
correlation between the histological and functional findings. Systematic studies are needed to
define which distance best correlates to the functional findings and such investigations are now
being done.
Our data indicate that the local environment in the Theracyte device at 3 months after
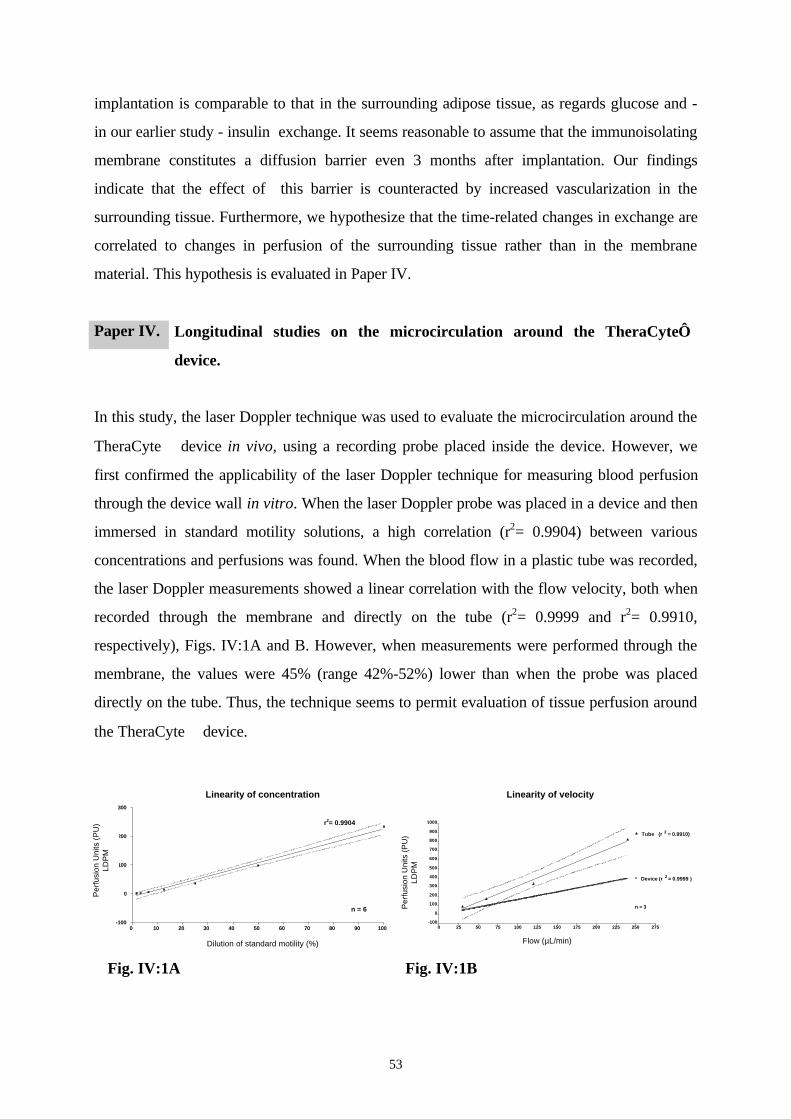
53
implantation is comparable to that in the surrounding adipose tissue, as regards glucose and -
in our earlier study - insulin exchange. It seems reasonable to assume that the immunoisolating
membrane constitutes a diffusion barrier even 3 months after implantation. Our findings
indicate that the effect of this barrier is counteracted by increased vascularization in the
surrounding tissue. Furthermore, we hypothesize that the time-related changes in exchange are
correlated to changes in perfusion of the surrounding tissue rather than in the membrane
material. This hypothesis is evaluated in Paper IV.
Paper IV. Longitudinal studies on the microcirculation around the TheraCyte
device.
In this study, the laser Doppler technique was used to evaluate the microcirculation around the
TheraCyte device in vivo, using a recording probe placed inside the device. However, we
first confirmed the applicability of the laser Doppler technique for measuring blood perfusion
through the device wall in vitro. When the laser Doppler probe was placed in a device and then
immersed in standard motility solutions, a high correlation (r2= 0.9904) between various
concentrations and perfusions was found. When the blood flow in a plastic tube was recorded,
the laser Doppler measurements showed a linear correlation with the flow velocity, both when
recorded through the membrane and directly on the tube (r2= 0.9999 and r2= 0.9910,
respectively), Figs. IV:1A and B. However, when measurements were performed through the
membrane, the values were 45% (range 42%-52%) lower than when the probe was placed
directly on the tube. Thus, the technique seems to permit evaluation of tissue perfusion around
the TheraCyte device.
Linearity of concentration
0 10 20 30 40 50 60 70 80 90 100-100
0
100
200
300
r2= 0.9904
n = 6
PerfusionUnits(
PU)
LDPM
Dilutionof standardmotility (%)
Linearity of velocity
0 25 50 75 100 125 150 175 200 225 250 275-100
0
100
200
300
400
500
600
700
800
900
1000
Device (r 2 = 0.9999 )
Tube (r 2 = 0.9910)
n = 3
Flow (µ l/min)
Per
fusi
on
Un
its
(PU
)L
DP
M
Fig. IV:1A Fig. IV:1B
Per
fusi
on U
nits
(P
U)
LDP
M
Linearity of concentration
Dilution of standard motility (%)
Linearity of velocity
Per
fusi
on U
nits
(P
U)
LDP
M
Flow (µL/min)
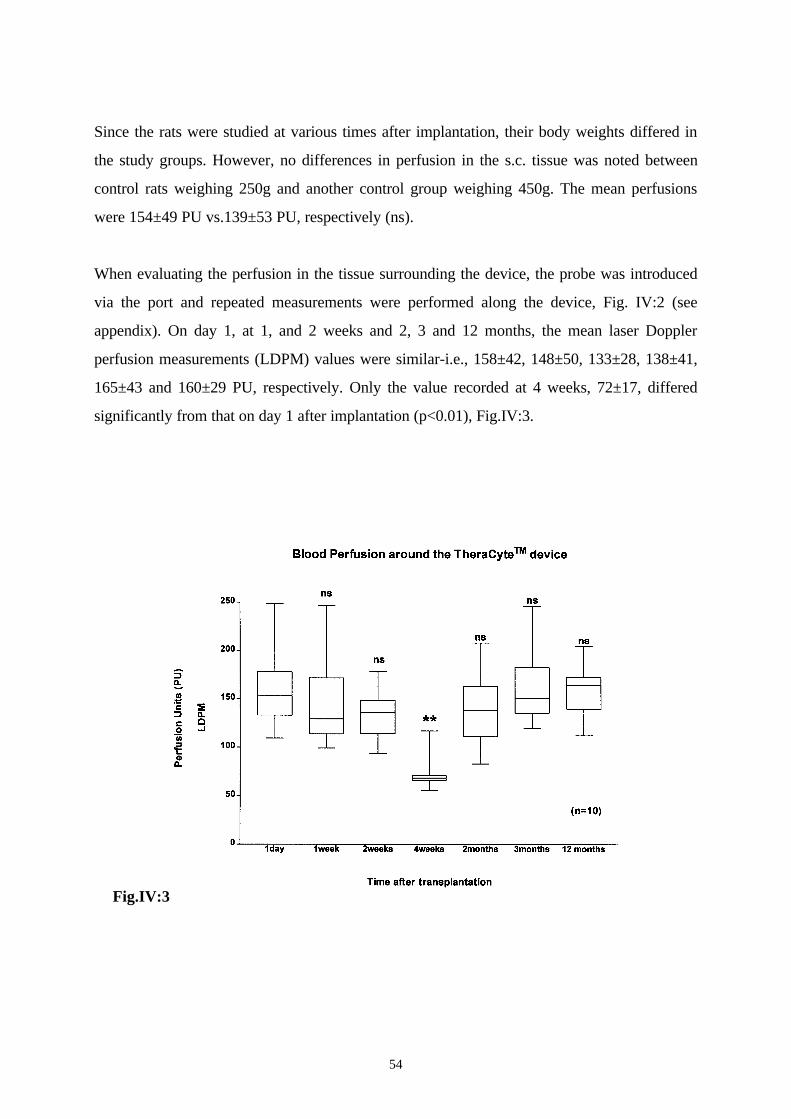
54
Since the rats were studied at various times after implantation, their body weights differed in
the study groups. However, no differences in perfusion in the s.c. tissue was noted between
control rats weighing 250g and another control group weighing 450g. The mean perfusions
were 154±49 PU vs.139±53 PU, respectively (ns).
When evaluating the perfusion in the tissue surrounding the device, the probe was introduced
via the port and repeated measurements were performed along the device, Fig. IV:2 (see
appendix). On day 1, at 1, and 2 weeks and 2, 3 and 12 months, the mean laser Doppler
perfusion measurements (LDPM) values were similar-i.e., 158±42, 148±50, 133±28, 138±41,
165±43 and 160±29 PU, respectively. Only the value recorded at 4 weeks, 72±17, differed
significantly from that on day 1 after implantation (p<0.01), Fig.IV:3.
Fig.IV:3
55
Discussion. The TheraCyte device was designed to improve the physiological conditions for
the graft by increasing the perfusion in the surrounding tissue. Up till now, the effectiveness of
the outer vascularizing membrane has mainly been evaluated by histological methods that
involve counting the number of vascular profiles within 15 µm of the device surface. These
increase significantly already during the first 2 weeks, while our functional studies indicate a
nadir in the exchange around 4 weeks after implantation followed by an improvement at 3
months. This laser Doppler study showed significantly lower perfusion around the device at 4
weeks after implantation, supporting the view that the physiological conditions around this
time may be suboptimal for the encapsulated cells. From 2 months onwards, the perfusion
remained stable for at least one year. This is a promising finding indicating a long-term effect
of the outer vascularizing membrane.
Laser Doppler is an effective way to measure the microcirculation in various tissues and organs
(Stern MD 1975, Fagrell B 1985, Ahn H et al 1987, Green M et al 1988, Wheatly AM et al
1993, Jörneskog G et al 1994, Catalano Met al 1997, Thollander M et al 1997). It gives
immediate results, can be non-invasive and allows repeated or continuous longitudinal
measurements. Compared to histology, it is less laborious, less time-consuming and less
investigator-dependent. Moreover, while microscopy permits detailed evaluation of various
histological features of the foreign body reaction, the laser Doppler technique provides
additional functional information- namely, data on tissue perfusion. To our knowledge, laser
Doppler has not been used previously to study macroencapsulation devices. Our findings
suggest that this is a quick and effective method for screening the biocompatibility of
macroencapsulation devices.
The TheraCyte device is ported and thus allows cells to be transplanted at a given time after
implantation. The device is usually loaded outside the body, but in view of our findings, we
suggest that it should instead be filled in situ 2-3 months after implantation. Such an approach
would allow time for neovascularization of the tissue around the device and may improve early
graft survival and function.
56
Paper V. Evaluation of preimplantation as a method to improve survival of encapsulated
islet grafts.
In this study, the effect of preimplantation of the TheraCyte device on the survival of a later
implanted islet graft was evaluated using morphometric methods.
Syngeneic rat islets were placed in preimplanted and non-preimplanted devices and the
implants were removed after 2 weeks. The total volume (mm3) of the graft in the preimplanted
devices was 4.8±3.0 vs. 6.1±1.2 in non-preimplanted devices (ns). The volume density (Vv) of
viable islets was 0.22±0.04 in the preimplanted devices vs. 0.06±0.03 in the devices loaded
without preimplantation (p<0.05). The volume densities of fibrosis and necrosis were
0.64±0.13 vs.0.85±0.08 (p<0.05) and 0.11±0.14 vs. 0.09±0.07 (ns), respectively, Figs. V:1A
and V:2A (see appendix).
When the absolute volumes (mm3) of the various components were calculated, preimplanted
and non-preimplanted devices contained 1.1±0.7 endocrine cells vs. 0.4±0.2 (p<0.05). The
corresponding volumes of fibrotic tissue were 3.0±1.8 vs. 5.2±1.2 (p<0.05), while the amounts
of necrotic tissue did not differ significantly, Tables V:1.
Immunohistochemical evaluation of the encapsulated grafts showed viable endocrine tissue
staining positive for insulin, Figs. V:1B and V:2B (see appendix). Both pre-implanted and non-
preimplanted devices were surrounded by a foreign body reaction but the fibrosis was more
pronounced around the preimplanted ones. Still, preimplanted devices seemed to have more
vascular profiles in the vicinity of the membrane-tissue interface. Furthermore, vascular profiles
were more homogeneously distributed while in non-preimplanted devices vessels were seen
mainly on the side of the device facing the fascia.
The diabetic nude mice transplanted with free islets, all achieved normoglycemia within a few
days. After removal of the graft-bearing kidney they again became diabetic within 24 hours.
Histological evaluation showed viable endocrine tissue staining positive for insulin.
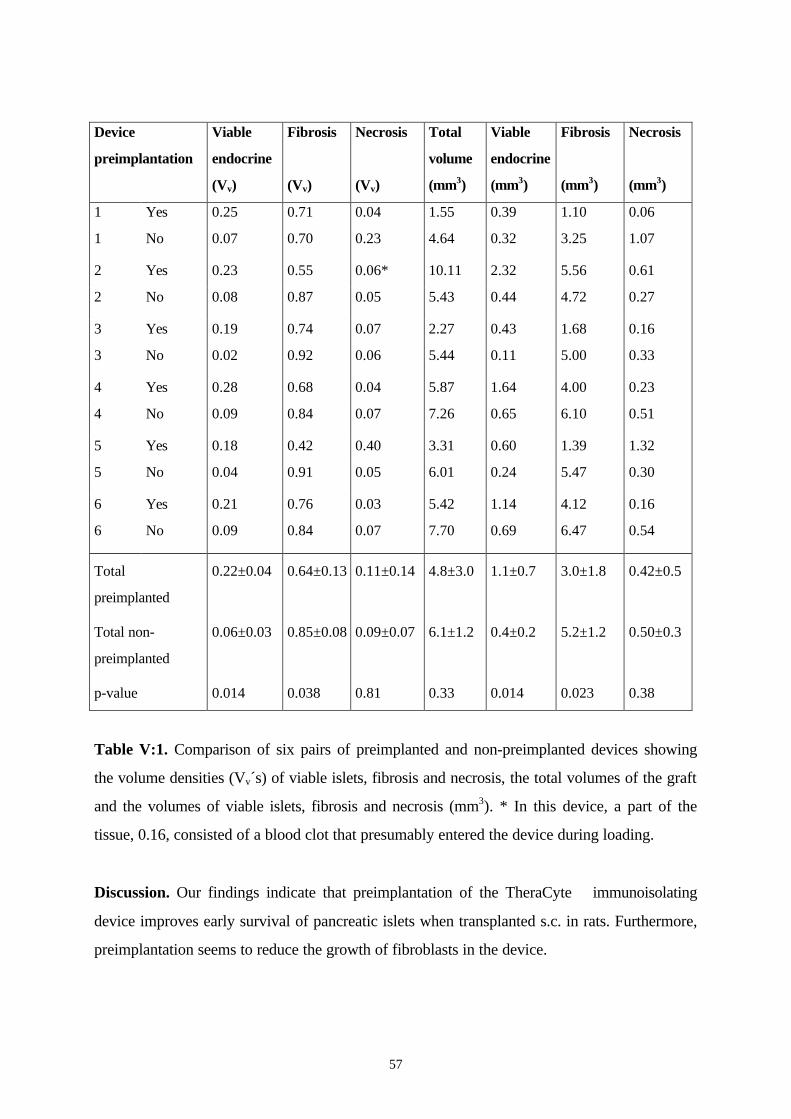
57
Device
preimplantation
Viable
endocrine
(Vv)
Fibrosis
(Vv)
Necrosis
(Vv)
Total
volume
(mm3)
Viable
endocrine
(mm3)
Fibrosis
(mm3)
Necrosis
(mm3)
1 Yes 0.25 0.71 0.04 1.55 0.39 1.10 0.06
1 No 0.07 0.70 0.23 4.64 0.32 3.25 1.07
2 Yes 0.23 0.55 0.06* 10.11 2.32 5.56 0.61
2 No 0.08 0.87 0.05 5.43 0.44 4.72 0.27
3 Yes 0.19 0.74 0.07 2.27 0.43 1.68 0.16
3 No 0.02 0.92 0.06 5.44 0.11 5.00 0.33
4 Yes 0.28 0.68 0.04 5.87 1.64 4.00 0.23
4 No 0.09 0.84 0.07 7.26 0.65 6.10 0.51
5 Yes 0.18 0.42 0.40 3.31 0.60 1.39 1.32
5 No 0.04 0.91 0.05 6.01 0.24 5.47 0.30
6 Yes 0.21 0.76 0.03 5.42 1.14 4.12 0.16
6 No 0.09 0.84 0.07 7.70 0.69 6.47 0.54
Total
preimplanted
Total non-
preimplanted
p-value
0.22±0.04
0.06±0.03
0.014
0.64±0.13
0.85±0.08
0.038
0.11±0.14
0.09±0.07
0.81
4.8±3.0
6.1±1.2
0.33
1.1±0.7
0.4±0.2
0.014
3.0±1.8
5.2±1.2
0.023
0.42±0.5
0.50±0.3
0.38
Table V:1. Comparison of six pairs of preimplanted and non-preimplanted devices showing
the volume densities (Vv´s) of viable islets, fibrosis and necrosis, the total volumes of the graft
and the volumes of viable islets, fibrosis and necrosis (mm3). * In this device, a part of the
tissue, 0.16, consisted of a blood clot that presumably entered the device during loading.
Discussion. Our findings indicate that preimplantation of the TheraCyte immunoisolating
device improves early survival of pancreatic islets when transplanted s.c. in rats. Furthermore,
preimplantation seems to reduce the growth of fibroblasts in the device.
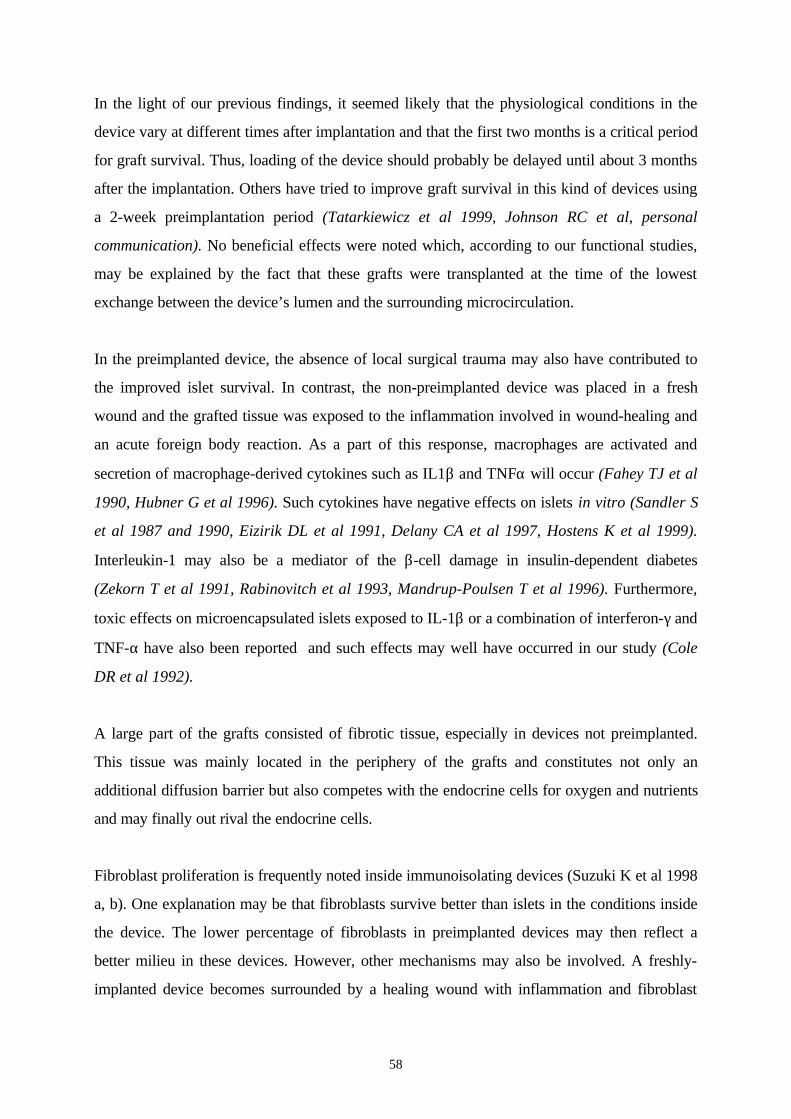
58
In the light of our previous findings, it seemed likely that the physiological conditions in the
device vary at different times after implantation and that the first two months is a critical period
for graft survival. Thus, loading of the device should probably be delayed until about 3 months
after the implantation. Others have tried to improve graft survival in this kind of devices using
a 2-week preimplantation period (Tatarkiewicz et al 1999, Johnson RC et al, personal
communication). No beneficial effects were noted which, according to our functional studies,
may be explained by the fact that these grafts were transplanted at the time of the lowest
exchange between the device’s lumen and the surrounding microcirculation.
In the preimplanted device, the absence of local surgical trauma may also have contributed to
the improved islet survival. In contrast, the non-preimplanted device was placed in a fresh
wound and the grafted tissue was exposed to the inflammation involved in wound-healing and
an acute foreign body reaction. As a part of this response, macrophages are activated and
secretion of macrophage-derived cytokines such as IL1β and TNFα will occur (Fahey TJ et al
1990, Hubner G et al 1996). Such cytokines have negative effects on islets in vitro (Sandler S
et al 1987 and 1990, Eizirik DL et al 1991, Delany CA et al 1997, Hostens K et al 1999).
Interleukin-1 may also be a mediator of the β-cell damage in insulin-dependent diabetes
(Zekorn T et al 1991, Rabinovitch et al 1993, Mandrup-Poulsen T et al 1996). Furthermore,
toxic effects on microencapsulated islets exposed to IL-1β or a combination of interferon-γ and
TNF-α have also been reported and such effects may well have occurred in our study (Cole
DR et al 1992).
A large part of the grafts consisted of fibrotic tissue, especially in devices not preimplanted.
This tissue was mainly located in the periphery of the grafts and constitutes not only an
additional diffusion barrier but also competes with the endocrine cells for oxygen and nutrients
and may finally out rival the endocrine cells.
Fibroblast proliferation is frequently noted inside immunoisolating devices (Suzuki K et al 1998
a, b). One explanation may be that fibroblasts survive better than islets in the conditions inside
the device. The lower percentage of fibroblasts in preimplanted devices may then reflect a
better milieu in these devices. However, other mechanisms may also be involved. A freshly-
implanted device becomes surrounded by a healing wound with inflammation and fibroblast
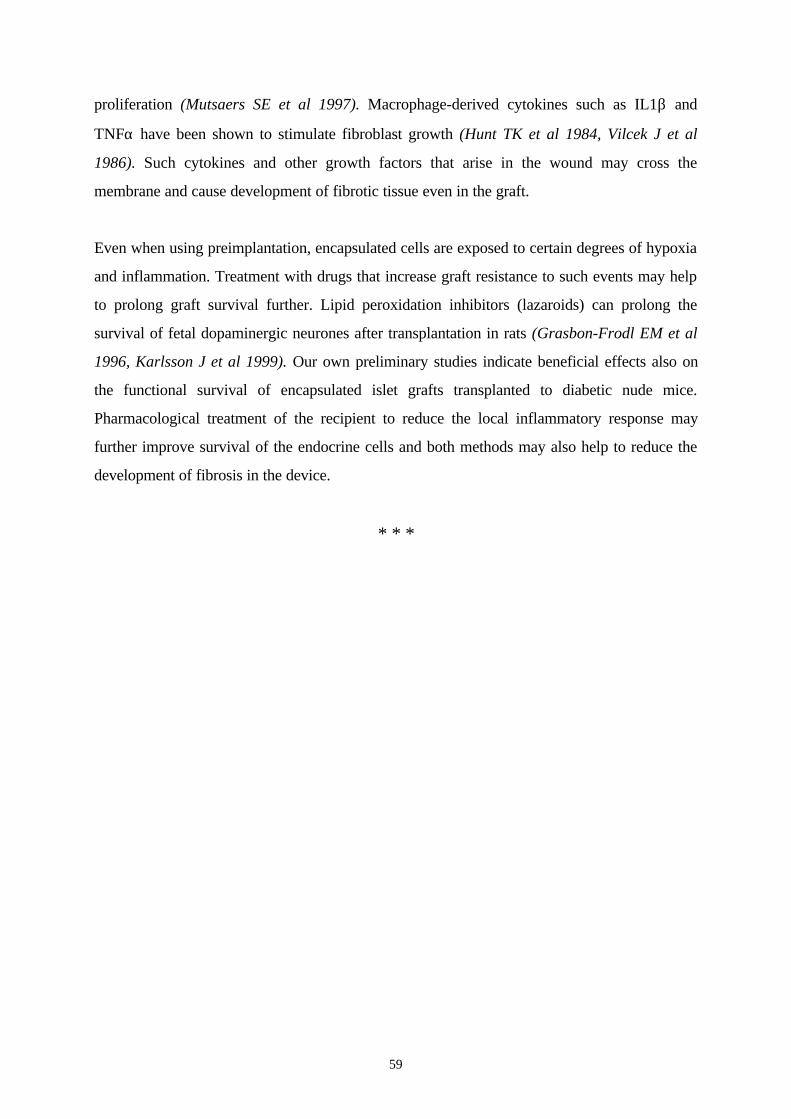
59
proliferation (Mutsaers SE et al 1997). Macrophage-derived cytokines such as IL1β and
TNFα have been shown to stimulate fibroblast growth (Hunt TK et al 1984, Vilcek J et al
1986). Such cytokines and other growth factors that arise in the wound may cross the
membrane and cause development of fibrotic tissue even in the graft.
Even when using preimplantation, encapsulated cells are exposed to certain degrees of hypoxia
and inflammation. Treatment with drugs that increase graft resistance to such events may help
to prolong graft survival further. Lipid peroxidation inhibitors (lazaroids) can prolong the
survival of fetal dopaminergic neurones after transplantation in rats (Grasbon-Frodl EM et al
1996, Karlsson J et al 1999). Our own preliminary studies indicate beneficial effects also on
the functional survival of encapsulated islet grafts transplanted to diabetic nude mice.
Pharmacological treatment of the recipient to reduce the local inflammatory response may
further improve survival of the endocrine cells and both methods may also help to reduce the
development of fibrosis in the device.
* * *
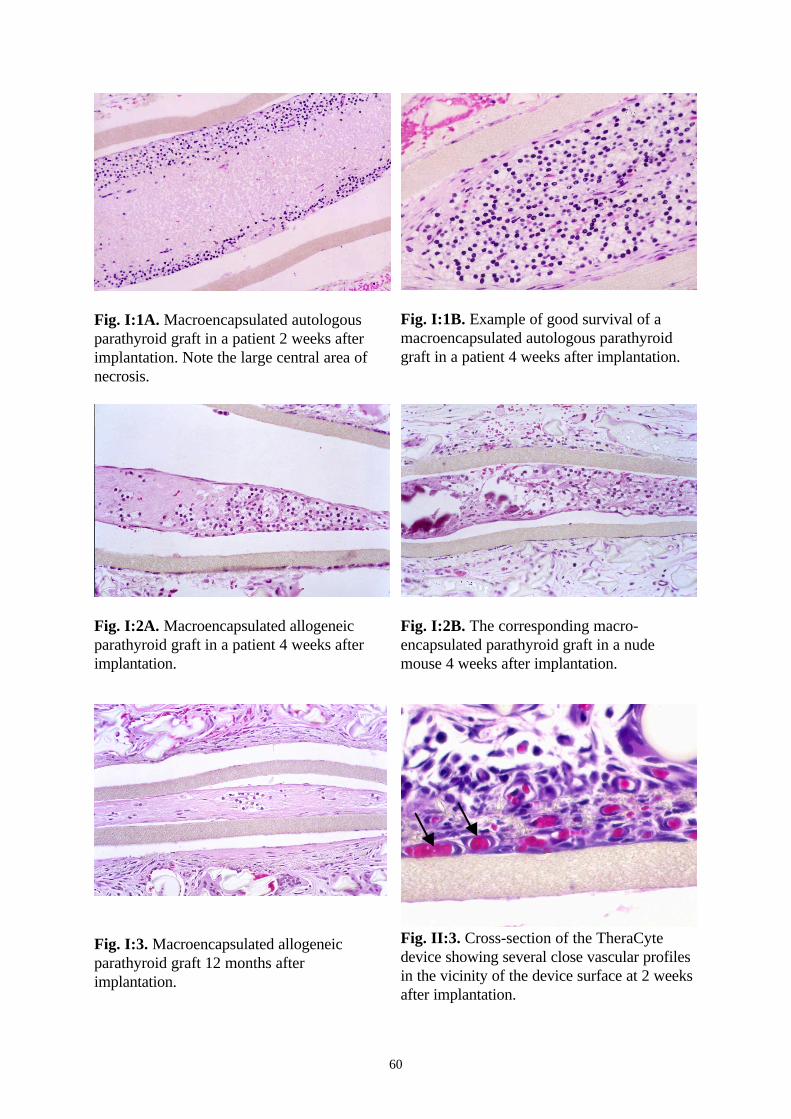
60
Fig. I:1A. Macroencapsulated autologousparathyroid graft in a patient 2 weeks afterimplantation. Note the large central area ofnecrosis.
Fig. I:1B. Example of good survival of amacroencapsulated autologous parathyroidgraft in a patient 4 weeks after implantation.
Fig. I:2A. Macroencapsulated allogeneicparathyroid graft in a patient 4 weeks afterimplantation.
Fig. I:2B. The corresponding macro-encapsulated parathyroid graft in a nudemouse 4 weeks after implantation.
Fig. I:3. Macroencapsulated allogeneicparathyroid graft 12 months afterimplantation.
Fig. II:3. Cross-section of the TheraCytedevice showing several close vascular profilesin the vicinity of the device surface at 2 weeksafter implantation.
61
The TheraCyte™ immunoisolation device. Fig. IV:2. The blood perfusion around theTheraCyte™ device was measured at theintervals shown above.
Fig. V:1A. Cross-section of an islet graft in anon-preimplanted TheraCyte™ device twoweeks after s.c. implantation in a rat.
Fig. V:1B. Immunohistochemical staining forinsulin of the graft shown in Fig. V:1A.
Fig. V:2A. Cross-section of an islet graft in apreimplanted TheraCyte™ device two weeksafter islet transplantation.
Fig. V:2B. Immunohistochemical staining forinsulin of the graft shown in Fig. V:2A.
62
Summary
Immunosuppressive therapy is a major cause of morbidity and mortality in recipients of
allografts and limits the use of transplantation as treatment. For cellular grafts, encapsulation in
semipermeable membranes may provide another way to protect the graft from immune attack
and thus allow transplantation without need for pharmacological immunosuppression.
In the studies included in this thesis, we used immunoisolating devices consisting of a bilaminar
PTFE membrane. The inner layer of the membrane provides immunoprotection; the outer one
has been added to induce neovascularization in the surrounding tissue, the aim being to
improve the physiological conditions in the device. Experimental studies indicate that cellular
allografts encapsulated in this bilayered membrane are not rejected.
Paper I describes our first experiences with transplanting human macroencapsulated
parathyroid tissue into patients. Encapsulated autologous grafts were studied 2-4 weeks after
implantation to determine whether the physiological conditions in the device allowed survival
of parathyroid tissue. Graft survival in the presence of an immune response was then evaluated
by implanting encapsulated allogeneic grafts. The autologous implants were placed in the first-
generation device - the Boggs chamber- while allografts were placed in the more recently
designed ported TheraCyte device. Both devices were made from the membrane described
above.
Histological evaluation of the autologous implants indicated that parathyroid tissue could
survive in this device when implanted s.c.. In the allogeneic study, small amounts of the
parathyroid tissue survived for one year in these non-immunosuppressed patients. However,
the vast majority of the grafts were fibrotic. The similar histological picture in control grafts
implanted in nude mice indicated that factors related to the preparation of the grafts or the
physiological conditions in the device rather than immunological damage was responsible for
the poor survival of the endocrine cells.
63
Islet transplantation is one important future clinical application of the encapsulation technique.
To improve our knowledge of the physiological conditions inside the device at various times
after transplantation, we evaluated the exchange of insulin and glucose between the device
lumen and the microcirculation in vivo, using the microdialysis technique (Paper II and III).
In both studies, empty TheraCyte devices were implanted s.c. in rats and we determined the
exchange across the membrane. In Paper II, insulin was injected into the device on day 1 or at
1, 2, 4 weeks or 3 months after implantation. The recovery was measured by inserting a
microdialysis probe s.c. 7-10 cm from the membrane. In the control group, insulin was injected
s.c. At 1, 2 and 4 weeks after implantation, the recovery of insulin after injection into the
device was significantly lower than that after s.c injection. However, at 3 months, recovery
improved and did not differ significantly from that in controls.
In paper III, the glucose kinetics in the device was compared to glucose kinetics in the s.c.
tissue during IVGTT. The results were similar to those in the insulin study, showing a
significant diffusion barrier during the first 4 weeks and an improved exchange 3 months after
implantation.
In both microdialysis studies, the histological examination showed an increased number of
vascular profiles within 15 µm of the membrane surface at 2, 4 weeks and 3 months after
transplantation, when compared to the number at 1 week. In the glucose study, the number of
vascular profiles within 250 µm was also counted and this number of vessels correlated
significantly to glucose kinetics whereas the number within 15 µm did not. Thus, vessels at a
distance more than 15 µm from the surface probably play an important role in nutrition of the
encapsulated graft.
We interpreted the variations in exchange with time noted in both microdialysis studies as
related to changes in blood perfusion in the tissue surrounding the device rather than to
changes in the membrane material. In Paper IV, laser Doppler was used to evaluate further the
blood perfusion around the device at various times after implantation. Again, empty devices
were implanted s.c. in rats. A laser Doppler probe was introduced via the port and the
microcirculation was measured along the device at different times between 1 day and 12
64
months after implantation. At 4 weeks, the perfusion was significantly reduced, but at 2
months, it had improved again and was the same as that on day 1. It then remained at a similar
level for at least one year. This is a promising observation indicating, together with our other
studies, that after an early period of reduced exchange between the device and
microcirculation, conditions improve about 2-3 months after implantation and then remain
stable.
Our findings also suggest that if the critical period of reduced exchange can be avoided,
survival of the encapsulated graft may be prolonged. By first implanting empty devices and
then loading the cells in situ 2-3 months later, the physiological conditions during the early
posttransplantation period should be improved.
In Paper V, this hypothesis was evaluated in a syngeneic rat model. Empty TheraCyte
devices were implanted s.c. and after 3 months, the device was filled in situ with 1500 islets. At
the same time, another device was filled with the an equal number of islets and implanted on
the other side of the back. Two weeks later, both implants were explanted and evaluated by
morphometry, using stereological techniques. The volume densities (Vv´s), and the absolute
volumes of viable islet tissue were larger in the preimplanted devices, while the Vv´s and the
total volumes of fibrotic tissue were smaller. As discussed above, these favorable effects may
be related to better physiological conditions in the preimplanted devices. Preimplantation also
avoids placing the encapsulated cells in a fresh wound and should thereby reduce the negative
effects caused by exposure to the inflammatory cytokines and fibroblast growth factors
involved in wound healing.
* * *
65
Conclusions
Allogeneic parathyroid tissue encapsulated in TheraCyte devices can survive for one year
after transplantation in non-immunosuppressed humans. However, marked growth of fibrotic
tissue occurs in the devices.
The exchange of insulin and glucose between the lumen of the device and blood is low 1-4
weeks after implantation but after 3 months, it improves and there seems to be no significant
diffusion barrier.
The number of vascular profiles within 15 µm of the device surface is significantly increased as
early as 2 weeks after implantation, while the number within 250 µm increases up to 3 months
after implantation. Only the number of vessels within 250 µm shows a significant correlation
to glucose exchange.
The blood perfusion in the s.c. tissue surrounding the device is lower at 4 weeks than that on
day 1 after implantation. It recovers at 2 months and then stays at a similar level for at least
one year.
Preimplantation of the device improves the survival of encapsulated syngeneic rat islets and
reduces the growth of fibrotic tissue inside the device.
Microdialysis and laser Doppler are useful techniques for evaluating the performance of
macroencapsulation devices in vivo. Such functional studies provides additional information to
that obtained by conventional methods such as in vitro testing of membrane permeability and
histological studies on biocompatibility.

66
Acknowledgments
I wish to express my sincere gratitude and appreciation to all those who have helped and
encouraged me throughout these studies and especially to:
My supervisor, tutor and friend, Annika Tibell for introducing me to the world of research
and sharing her great experience, for her enthusiastic guidance and invaluable advice in the
preparation of this thesis. For the nice memories during the long hours of standing and
operating on both humans and animals everywhere in Sweden.
My co-supervisor, Annika Wernerson for always being friendly and able to simplify all the
complicated histological techniques. For encouragement when everything seems impossible.
My mentor, Professor Carl-Gustav Groth who welcomed me to Sweden. For his generosity,
vision for the future and continuous support and who made me feel that I was doing the same
things he did 30 years ago.
My friends in the Xeno-islet transplantation group, Olle Korsgren, Lars Wennberg, William
Bennet, Torbjörn Lundgren, Guosheng Wu, Zhenshung Song, Jianguo Zhang and
Martin Wikström, for always being kind, helpful and sharing good and bad experiences in
islet transplantation and research.
My close friend and co-author Bertil Gazelius, for offering his valuable time to teach me
about laser-Doppler, for his big heart and high spirits which I shall never forget.
Our Xeno-lab maestro, Berit Sundberg for always being available to explain, help and support
the beginners, for the friendly attitude and high spirits. Silvia Nava, for glucose analyses and
preparation of the devices.
Professor Lennart Eriksson, head of the Department of Pathology for kindly providing
research facilities.
67
Anneli Hansson and Maria Jepsen for skillful preparation of the histological sections.
Marie Larsson our data expert, for excellent graphs and figures even at a distance.
My co-authors, Peter Arner and Kjell Hultenby, for their contributions and valuable advice.
Göran Lundgren, Gunnar Tydén and Bo-Göran Ericzon, for accepting me as a visiting
fellow in kidney and liver transplantation sections.
My senior colleagues on the transplantation ward, Christina Brattström, Frans Duraj,
Håkan Gäbel, Professor Olle Ringdén, Johan Sandberg, Jan Tollmer and Henryk
Wilczek, excellent teachers in transplantation surgery, immunosuppressives and research.
My senior colleagues from other Departments Professor Erna Möller, Professor Finn
Reinholt, Lennart Eleborg, Ulrika Broomé, Ingla Fehrman for extending my knowledge of
their specialties.
My friends and junior colleagues, Stefan Carlens, Ashok Gadré, Mikael Hartman, Patrik
Hentscke, Gustaf Herlenius, Hans Högglund, Jonas Mattsson, Grzegorz Nowak and
Gunnar Söderdahl, for accepting me in their group, improving my Swedish and for
unforgettable memories and laughs.
Ann-Christin Croon and Lena Svensson, transplantation coordinators, for the sightseeing in
the early mornings and late nights, and for making organ harvesting an enjoyable trip.
All the staff in the animal department especially Ingvild Halbig and Marina Nyborg, for the
friendship and good care of my rats and mice.
Ewa Söderberg, for her excellent secretarial work and for efficiently handling all my
administration.
68
Our friends from Baxter Healthcare Corporation in USA, Robert Johnson, James Brauker,
Tom Loudovaris, Robin Geller, Steven Neuenfeldt and Len Czuba for always being helpful
and for valuable advice.
Mr. Francis and Dr. Zoe Walsh, for their English corrections and for accepting that I am
always in a hurry to get it done.
Bo Nilsson, an excellent statistician, for his time, help and advice in all the studies.
Baxter Health Care for providing the immunoisolation devices and for economical support
for parts of Study I.
The staff in CMA microdialysis AB, Perimed AB and Agntho´s AB for providing
information, equipment and technical help.
My Mother, Rakyah Rafael, for being my first teacher and example, for providing me with
unlimited love, care and support.
My father, Saad Rafael, for unfailing support and friendship, for his care at a distance-for
dedicating his life to his family.
My brother, Ashraf, and My sister, Ellen, and their families for their care, support, warm
feelings and understanding.
My family in Sweden, my father-and mother-in-law, Ezat and Mervat, my sisters-and brother-
in-law, Nancy, Josef and Marina, who provided me with a very enjoyable social life, and took
good care of my son while I was busy.
Anton, my son, and the most precious treasure I have, who gave value to my life.
Riham, my life-companion, for pure love, patience, understanding, encouragement and for
accepting that I am away often. I am happy having you.
69
The studies included in thesis were supported by:
Karolinska Institutet,
the Swedish Medical Research Council,
the Swedish Institute,
the Foundation for International Surgical Co-operation,
the Swedish Medical Society,
the Swedish Society for Medical Research,
the Wiberg Foundation,
Jeansson Foundation,
Juvenile Diabetes Foundation,
the Knut and Alice Wallenberg Foundation,
Torsten and Ragnar Söderberg Foundation
and Martin Rind’s Foundation.

70
References
Abendroth D, Landgraf R, Illner WD, et al. Beneficial effect of pancreatic transplantation ininsulin-dependent diabetes mellitus patients. Transplant Proc, 1990. 22(2): p. 696-697.
Aebischer P, Wahlberg L, Tresco PA, et al. Macroencapsulation of dopamine-secreting cells bycoextrusion with an organic polymer solution. Biomaterials, 1991. 12: p. 50-56.
Aebischer P, Buchser E, Joseph JM, et al. Transplantation in humans of encapsulatedxenogeneic cell without immunosuppression. Transplantation, 1994. 58: p. 1275-1277.
Aebischer P, Schluep M, Deglon N. Intrathecal delivery of CNTF using encapsulatedgenetically-modified xenogeneic cells in amyotrophic lateral sclerosis patients. Nat Med, 1996. 2:p. 3-5.
Ahn H, Johansson K, Lundgren O, et al. In vivo evaluation of signal processors for laser-Doppler tissue flowmetry. Med & Biol Eng & Comp, 1987. 260: p. 207-211.
Alfrey EJ, Perloff LJ, Asplund MW. Normocalcemia 13 years after successful parathyroidallografting in a recipient of a renal transplant. Surgery, 1992. 111(2): p. 234-236.
Altman JJ, Houlbert D, Callard P. Long-term plasma glucose normalization in experimentaldiabetic rats with macroencapsulated implants of benign human insulinoma. Diabetes, 1986. 35:p. 625-633.
Altman JJ. Bioartificial pancreas. Transplant Proc, 1990. 22(2): p. 698-699.
Alveryd A. Parathyroid glands in thyroid surgery. I. Anatomy of parathyroid. II. Postoperativehyperparathyroidism: identification and autotransplantation of parathyroid glands. Acta ChirScand, 1968. 389: p. 1-49.
Anderson JM. Inflammatory response to implants. Trans Am Soc Artif Intern Organs, 1988. 34:p. 101-107.
Andersson A, Eizirik DL, Hellerström C, et al. Morphology of Encapsulated human pancreaticislets transplanted into nude mice. Transplant Proc, 1994. 26(2): p. 802-803.
Andersson A, Eizirik DL, Bremer C, et al. Structure and function of macroencapsulated humanand rodent islets transplanted into nude mice. Horm Metab Res, 1996. 28: p. 306-309.
Aomatsu Y, Iwata H, Takagi T, et al. Microencapsulated islets in agarose gel as bioartificialpancreas for discordant xenotransplantation. Transplant Proc, 1992. 24(6): p. 2922-2923.
Arner P, Bolinder J. Microdialysis of the adipose tissue. J Intern Med, 1991. 230: p. 381-386.
Bach FH, Albertini RJ, Joo P, et al. Bone marrow transplantation in a patient with the Wiskott-Aldrich syndrome. Lancet, 1968. 2(7583): p. 1364-1366.
Ballinger WF. Transplantation of intact pancreatic islets in rats. Surgery, 1972. 72: p. 175-186.
Benedum J. The early history of endocrine cell transplantation. J Mol Med, 1999. 77: p. 30-35.
71
Björklund A, Stenevi U. Reconstruction of the nigrostriatal pathway by intracerebral nigraltransplants. Brain Res, 1979. 177: p. 555-560.
Bolinder J, Hagström E, Ungerstedt U, et al. Microdialysis of subcutaneous adipose tissue invivo for continuous glucose monitoring in man. J Clin Lab Invest, 1989. 49: p. 465-474.
Bolinder J, Ungerstedt U, Arner P. Microdialysis measurements of the absolute glucoseconcentration in subcutaneous adipose tissue allowing glucose monitoring in diabetic patients.Diabetologia, 1992. 35: p. 1177-1180.
Bolinder J, Ungerstedt U, Arner P. Long-term continuous glucose monitoring with microdialysisin ambulatory insulin-dependent diabetic patients. The Lancet, 1993. 342: p. 1080-1085.
Brauker J, Martinson LA, Loudovaris T, et al. Immunoisolation with large pore membrane:Allografts are protected under conditions that results in destruction of xenografts. CellTransplantation, 1992. 1: p. 164(Abstract).
Brauker J, Carr- Brendel V, Martinson L, et al. Neovascularization of synthetic membranedirected by membrane microarchitecture. J Biomed Mater Res, 1995. 29: p. 1517-1524.
Brauker JH, Martinson LA, Young SK, et al. Local inflammatory response around diffusionchambers containing xenografts. Transplantation, 1996. 61: p. 1671-1677.
Brauker J, Frost GH, Dwarki V, et al. Sustained expression of high levels of human factor IXfrom human cells implanted within immunoisolation device into athymic rodents. Hum Gene Ther,1998. 9(6): p. 879-888.
Brendel MD, Hering BJ, Schultz AO, et al. (International Islet Transplant Registry). Newsletter8, 1999. Geissen, Germany: Justus-Liebig- University of Giessen: p. 1-20.
Bretzel RG, Eckhard M, Brandhorst D, et al. Simultaneous and after kidney or after livertransplantation of islets of Langerhans at Gissen university in 45 consecutive patients withinsulin-dependent diabetes mellitus (IDDM). Horm Metab Res, 1998. 30: p. A9 (Abstract).
Califiore R, Janjic D, Koh N. Transplantation of microencapsulated canine islets into NODmice: prolongation of survival with superoxide dismutase and catalase. Clin Res, 1987. 35: p.499A.
Calne RY. Lancet, 1960. i: p. 417-418.
Carr-Brendel VE, Geller RL, Thomas TJ, et al. Transplantation of cells in an immunoisolationdevice for gene therapy. Methods Mol Biol., 1997. 63: p. 373-387.
Catalano M, Schioppa S, Sampietro G, et al. Skin blood flow during vasoconstrictive andvasodilative stimuli in essential hypertension patients: A laser-Doppler f lowmetry study. Int JMicrocirc, 1997. 17: p. 80-85.
Chang PL, Shen N, Westcott AJ. Delivery of recombinant gene products with microencapsulatedcells in vivo. Hum Gene Ther, 1993. 4: p. 443-440.
Chou FF, Chan HM, Houng TJ, et al. Autotransplantation of parathyroid glands intosubcutaneous forearm tissue for renal hyperparathyroidism. Surgery, 1998. 124(1): p. 1-5.
72
Christiansen E, Vestergaard H, Tibell A, et al. Impaired Insulin- stimulated Nonoxidativeglucose metabolism in pancreas-kidney transplant recipients. Diabetes, 1996 a. 45: p. 1267-.
Christiansen E, Tibell A, Volund A, et al. Pancreatic endocrine function in recipients ofsegmental and whole pancreas transplantation. J Clin Endocrinol Metab, 1996 b. 81: p. 3972-3979.
Clayton HA, London NJM, Colloby PS, et al. The effect of capsule composition on thebiocompatibility of alginate-poly-L-lysine capsule. J Microencapsulation, 1991. 8: p. 221-233.
Clayton HA, James RFL, London NJM. Islet microencapsulation: a review. Acta Diabetol,1993. 30: p. 181-189.
Cole DR, Waterfall M, McIntyre M, et al. Microencapsulated islet grafts in the BB/E rat: apossible role for cytokines in graft failure. Diabetologia, 1992. 35(3): p. 231-237.
Colton C, Avgoustiniatos E. Bioengineering in the development of the hybrid artificial pancreas.Transections of the ASME, 1991. 113: p. 152-170.
Colton C. Implantable biohybrid artificial organs. Cell Transplantation, 1995. 4(4): p. 415-436.
Colton C. Engineering challenges in cell- encapsulation technology. TIBTECH, 1996. 14: p. 158-162.
Darqur S, Reach G. Immunoisolation of pancreatic β-cells by microencapsulation. An in vitrostudy. Diabetologia, 1985. 28: p. 776-780.
De Vos P, Wolters GHJ, Fritschy WM. Obstacles in the application of microencapsulation inislet transplantation. Int J Artif Organs., 1993. 16: p. 205-212.
De Vos P, De Haan BJ, Wolters GHJ, et al. Improved biocompatability but limited graftsurvival after purification of alginate for microencapsulation of pancreatic islets. Diabetologia,1997. 40: p. 262-270.
Delany CA, Pavlovic D, Hoorens A, et al. Cytokines induce deoxyribonucleic acid strand breaksand apoptosis in human pancreatic islet cells. Endocrinology, 1997. 138(6): p. 2610-2614.
Deleu D, Sarre S, Ebinger G, et al. Simultaneous monitoring of levodopa, Dopamine and theirmetabolites in skeletal muscle and subcutaneous tissue in different pharmacological conditionsusing microdialysis. J Pharmaceut Biomed Anal, 1993. 11(7): p. 577-585.
Delgado JMR, Feudis FV, Roth RH, et al. Dialytrode for long-term intravertebral perfusion inawake monkeys. Arch Int Pharmacodyn Ther, 1972. 198: p. 9-21.
Eizirik DL, Bendtzen K, Sandler S. Short exposure of rat pancreatic islets to interleukin-1binduces a sustained but reversible impairment in b-cell function: influence of protease activation,gene transcription and protein synthesis. Endocrinology, 1991. 128(3): p. 1611-1616.
Elliot RP, Garkavenko O, Schroeder BA, et al. No evidence of infection with porcineendogenous retrovirus in recipients of encapsulated porcine islet-cell xenograft. Abstract book,7th World Congress of the IPITA., 1999 (229): p. 143 (Abstract).
73
Emerich DF, Winn SR, Christenson L, et al. A novel approach to neural transplantation inParkinson’s disease: use of polymer encapsulated cell therapy. Neurosci Biobehav Rev, 1992. 16:p. 437-474.
Engfeldt P, Tydén G, Gunnarsson R, et al. Impaired glucose tolerance with cyclosporine.Transplant Proc, 1986. 18: p. 65-66.
Fagrell B. Dynamics of skin microcirculation in humans. J Cardiovasc Pharmacol, 1985. 7(S3): p.S53-S58.
Fahey TJ, Sherry B, Tracey KJ, et al. Cytokine production in a model of wound healing: theappearance of MIP-1, MIP-2, cachectin/ TNF and IL-1. Cytokine, 1990. 2(2): p. 92-99.
Fan MY, Lum ZP, Fu XW, et al. Reversal of diabetes in BB rats by transplantation ofencapsulated pancreatic islets. Diabetes, 1992. 39: p. 519-522.
Federlin KF, Bretzel RG, Hering BJ. Islet transplant registry. In: Pancreatic islet celltransplantation, Ricordi C, Ed. R.G. Landes Company, Austin, TX, USA, 1992: p. 462-472.
Fritschy WM, de Vos P, Groen H, et al. The capsular overgrowth on microencapsulatedpancreatic islet grafts in streptozotocin and autoimmune diabetic rats. Transpl Int, 1994. 7: p.264-271.
Fu WX, Sun AM. Microencapsulated parathyroid cells as a bioartificial parathyroid.Transplantation, 1989. 47(3): p. 432-4355.
Gatti RA, Meuwissen HJ, Allen HD, et al. Immunological reconstitution of a sex-linkedlymphopenic immunological deficiency. Lancet, 1968. 2(7583): p. 1366-1369.
Geller RL, Loudovaris T, Neuenfeldt S, et al. Use of an immunoisolation device for celltransplantation and tumor immunotherapy. Ann N Y Acad Sci, 1997a. 831: p. 438-451.
Geller RL, Neuenfeldt S, Levon SA, et al. Immunoisolation of tumor cells: generation ofantitumor immunity through indirect presentation of antigen. J Immunother, 1997b. 20(2): p. 131-137.
Grasbon-Frodl EM, Nakao N, Brundin P. The lazaroids U- 83836E improves the survival of ratembryonic mesencephalic tissue stored at 4 degrees C and subsequently used for cultures orintracerebral transplantation. Brain Res Bull, 1996. 39(6): p. 341-347.
Gray DWR, McShane P, Grant A, et al. A method for isolation of islets of Langerhans from thehuman pancreas. Diabetes, 1984. 33: p. 1055- 1061.
Gray DWR, Morris PJ. Isolation of rat pancreatic islets by ductal injection of collagenase.Transplantation, 1986 a. 42(6): p. 689-691.
Gray DW, Warnock G, Sutton R, et al. Successful autotransplantation of isolated islets ofLangerhans in the cynomolgus monkey. Br J Surg, 1986 b. 1986(73): p. 850-857.
Gray DWR, Morris PJ. Developments in isolated pancreatic islet transplantation.Transplantation., 1987. 43: p. 321-326.
74
Green M, Holloway AG, Heimbach DM. Laser-Doppler monitoring of microcirculatory changesin acute burn Wounds. JBCR, 1988. 9(1): p. 57-62.
Gross CR, Limwattananon C, Matthees BJ. Quality of life after pancreas transplantation: areview. Clinical Transplantation, 1998. 12: p. 351-361.
Groth CG, Popovtzer M, Hammond WS, et al. Survival of homologous parathyroid implant inan immunosuppressed patient. Lancet, 1973. 1: p. 1082-1085.
Groth CG, Andersson A, Björkén R, et al. Transplantation of fetal pancreatic microfragmentsvia the portal vein to a diabetic patient. Diabetes, 1980. 29(1): p. 80-83.
Groth CG, Korsgren O, Tibell A, et al. Transplantation of porcine fetal pancreas to diabeticpatients. Lancet, 1994. 344: p. 1402-1404.
Groth CG, Bäckman L, Morales J-M, et al. Sirolimus (Rapamycin)-Based therapy in humanrenal transplantation. Transplantation, 1999. 67(7): p. 1036-1042.
Gunnarsson R, Klintmalm G, Lundgren G, et al. Deterioration in glucose metabolism inpancreatic transplant recipients given cyclosporine A. Lancet, 1983. 2: p. 571-572.
Hagström-Toft E, Arner P, Johansson U, et al. Effect of insulin on human adipose tissuemetabolism in situ. Interactions with b-adrenoreceptors. Diabetologia, 1992. 35: p. 664-670.
Hara K, Uchida K, Fukunaga A, et al. Implantation of xenogeneic transgeneic neural platetissues into parkinsonian rat brain. Cell Transplantation, 1997. 6(5): p. 515-519.
Hasse C, Schrezenmeir J, Stinner B, et al. Successful allotransplantation of microencapsulatedparathyroid in rats. World J Surg, 1994. 18: p. 630-634.
Hasse C, Klock G, Zielke A, et al. Transplantation of parathyroid tissue in experimentalhypoparathyroidism: in vitro and in vivo function of parathyroid tissue microencapsulated with anovel amitogeneic alginate. Int J Artif Organs, 1996. 19(12): p. 735-741.
Hering BJ, Ricordi C. Islet transplantation for patients with type-1 diabetes. Graft, 1999. 2(1): p.12-27.
Hesse UJ, Schmitz-Rode M, Voss S. Islet counting by staining with Dithizone in variousconcentrations. Transplant Proc, 1992. 24(6): p. 2989.
Hidi H, Chiba T, Takagi Y, et al. Percutaneous autotransplantation of parathyroid tissue intothe forearm muscle. Surgery Today, 1998. 28(1): p. 114-116.
Hesse C, Kriaa F, Rieu JR, et al. Incidence and type of malignancies occurring after renaltransplantation in conventionally and cyclosporine-treated recipients: Analysis of a 20 yearperiod in 1600 patients. Transplant Proc, 1995. 27(972-974).
Hostens K, Pavlovic D, Zambre Y, et al. Exposure of human islets to cytokines can result indisproportionately elevated proinsulin release. J Clin Invest, 1999. 104(1): p. 67-72.

75
Hunber G, Brauchle M, Smola H, et al. Differential regulation of pro-inflammatory cytokinesduring wound healing in normal and glucocorticoid-treated mice. Cytokines, 1996. 8(7): p. 548-556.
Hunt TK, Knighton DR, Thakral KK, et al. Studies of inflammation and wound healing:Angiogenesis and collagen synthesis stimulated in vivo by resident and activated woundmacrophages. Surgery, 1984. 96: p. 48-54.
Icard P, Penfornis F, Gotheil C, et al. Tissue reaction to implanted bioartificial pancreas in pigs.Transplant Proc, 1990. 22(2): p. 724-726.
Jansson P-A, Fowelin JP, Von Schenck HP, et al. Measurement by microdialysis of the insulinconcentration in subcutaneous interstitial fluid. Importance of the endothelial barrier for insulin.Diabetes, 1993. 42: p. 1469-1473.
Jesser C, Kessler L, Lambert L, et al. Pancreatic islet macroencapsulation: a new device for theevaluation of artificial membrane. Artif Organs, 1996. 20(9): p. 997-1007.
Johansson U, Arner P, Bolinder J, et al. Influence of insulin on glucose metabolism and lipolysisin adipose tissue in situ in a patient with liver cirrhosis. Euro J Clin Invest, 1993. 23: p. 837-844.
Jörneskog G, Lins P-E, Adamson U, et al. Patients with type-1 diabetes lack vasoconstrictorresponse in skin microcirculation during insulin-induced hypoglycaemia. Int J Microcirc, 1994.14: p. 262-268.
Juang J-H, Bonner-Weir S, Vacanti J, et al. Outcome of subcutaneous islet transplantationimproved by a polymer device. Transplant Proc, 1995. 27(6): p. 3215-3216.
Kanai N, Hagihara M, Nagamachi Y, et al. Beneficial effects of immunoisolated fetal andneonatal pig liver fragments on acute liver failure in large animals. Cell Transplantation, 1999. 8:p. 413-417.
Karlsson J, Love RM, Clarke DJ, et al. Effects of anaesthetics and lazaroid U- 83836E onsurvival of transplanted rat dopaminergic neurones. Brain Res, 1999. 821(2): p. 546-550.
Keown P, Häyry P, Mathew T, et al. A blinded, randomized clinical trial of MycophenolateMofetil for the prevention of acute rejection in cadeveric renal transplantation. Transplantation,1996. 61(7): p. 1029-1037.
Kolb E, Largiader F. Clinical islet transplantation. Transplant Proc, 1980. 12: p. 205-208.
Koo J, Chang TMS. Secretion of erythropoietin from microencapsulated rat kidney cells.Preliminary results. Int J Artif Organs, 1993. 16: p. 557-560.
Lacy PE, M. K. Method for the isolation of intact islets of Langerhans from the rat pancreas.Diabetes, 1967. 16: p. 35-38.
Lacy PE, Hegre OH, Gerasimide-Vazeou A. Subcutaneous xenografts of rat islets in acryliccopolymer capsules maintain normoglycemia in diabetic mice. Science, 1991. 254: p. 1782-1784.
Lanza RP, Borland KM, Lodge P, et al. Pancreatic islet transplantation using membranediffusion chambers. Transplant Proc, 1992a. 24: p. 2935-2936.
76
Lanza RP, Sullivan SJ, Chick WL. Islet transplantation with immunoisolation. Diabetes, 1992b.41: p. 1503-1510.
Lanza RP, Bulter DH, Borland KM, et al. Successful xenotransplantation of a diffusion-basedbiohybrid artificial pancreas: a study using canine, bovine, and porcine islets. Transplant Proc,1992c. 24(2): p. 669-671.
Lanza RP, Borland KM, Staruk JE, et al. Transplantation of encapsulated canine islets intospontaneously diabetic BB/wor rats without immunosuppressive. Endocrinology, 1992d. 131(2): p.637-642.
Lanza RP, Borland KM, Lodge P, et al. Treatment of severely diabetic pancreatectomized dogsusing a diffusion-based hybrid pancreas. Diabetes, 1992e. 41: p. 886-889.
Lanza RP, Beyer AM, Staruk JE, et al. Biohybrid artificial pancreas. Long-term function ofdiscordant islet xenograft in streptozotocin diabetic rats. Transplantation, 1993. 56(5): p. 1067-1072.
Lanza RP, Hayes J, Chick WL. Encapsulated cell technology. Nature Biotechnology, 1996. 14:p. 1107-1111.
Lanza RP, Chick WL. Transplantation of encapsulated cells and tissues. Surgery, 1997a. 121(1):p. 1-9.
Lanza RP, Chick WL. Immunoisolation strategies for the transplantation of pancreatic islets.Ann NY Acad Sci, 1997b. 831: p. 323-331.
Lim F, Sun AM. Microencapsulated islets as bioartificial endocrine pancreas. Science, 1980.210: p. 908-910.
Lindholm A, Albrechtsen D, Tufveson G, et al. A randomized trial of Cyclosporine andPrednisolane versus Cyclosporine, Azathioprine, and Perdnisolane in primary cadaveric renaltransplantation. Transplantation, 1992. 54(4): p. 624-631.
Lindvall O. Restoration of brain function by tissue transplantation. Berlin Heidelberg: Springer-Verlag, 1993: p. 1-74
Lindvall O. Neural Transplantation. Cell Transplantation, 1995. 4(4): p. 393-400.
Liu HW, Ofosu FA, Chang PL. Expression of human factor IX by microencapsulatedrecombinant fibroblasts. Hum Gene Ther, 1993. 4: p. 291-301.
London NJM, Robertson GSM, Chadwick DR, et al. Human pancreatic islet isolation andtransplantation. Clinical Transplantation, 1994. 8: p. 421-459.
Loudovaris T, Charlton B, Mandel T. The role of T-cells in the destruction of xenografts withincell-impermeable membranes. Transplant Proc, 1992. 24(6): p. 2938.
Loudovaris T, Charlton B, Hodgson RJ, et al. Destruction of xenografts but not allograftswithin cell impermeable membrane. Transplant Proc, 1992. 24(5): p. 2291-2292.
77
Loudovaris T, Mandel T, Charlton B. CD4 +T-cell-mediated destruction of xenografts withincell-impermeable membranes in the absence of CD8+T-cells and B-cells. Transplantation, 1996.61(12): p. 1678-1684.
Loudovaris T, Jacobs S, Young S, et al. Correction of diabetic NOD mice with insulinomaimplanted within Baxter immunoisolation devices. J Mol Med, 1999. 77: p. 219-222.
Lönnroth P, Jansson PA, Smith U. A microdialysis method allowing characterization of theintercellular water space in humans. Am J Physiol, 1987. 253: p. E228-231.
Lönnroth P, Smith U. Microdialysis- a novel technique for clinical investigation. J Intern Med,1990. 227: p. 295-300.
Lönnroth P. Microdialysis - a new promising method in clinical medicine. J Intern Med, 1991.230: p. 363-364.
Lum ZP, Tait IT, Krestaw M, et al. Prolonged reversal of the diabetic state in NOD mice byxenograft microencapsulated rat islets. Diabetes, 1991. 40: p. 1511-1516.
Maki T, Ubhi CS, Sanchez-Farpon H, et al. The biohybrid artificial pancreas for treatment ofdiabetes in totally pancreatectomized dogs. Transplant Proc, 1991a. 23 (1): p. 754-755.
Maki T, Ubhi CS, Sanchez- Farpon H, et al. Successful treatment of diabetes with the biohybridartificial pancreas in dogs. Transplantation, 1991b. 51 (1): p. 43-51.
Maki T, Lodge PA, Carretta M, et al. Treatment of severe diabetes mellitus for more than oneyear using a vascularized hybrid artificial pancreas. Transplantation, 1993. 55(4): p. 713-718.
Maki T, Mullon C, Solomon B, et al. Novel delivery of pancreatic islet cells to treat insulin-dependent diabetes mellitus. Clin Pharmacokinet., 1995. 28(6): p. 471-482.
Maki T, Otsu I, O´Neil JJ, et al. Treatment of diabetes by xenogeneic islets withoutimmunosupressive. Diabetes, 1996. 45: p. 342-347.
Mandrup-Poulsen T. The role of interleukin-1 in the pathogenesis of IDDM. Diabetologia, 1996.39: p. 1005-1029.
Mattas AJ, McHugh L, Payne WD, et al. Long-term quality of life after kidney and simultaneouspancreas-kidney transplantation. Clinical Transplantation, 1998. 12: p. 233-242.
Merill JP, Murray JE, Harrison JH, et al. Successful homotransplantation of human kidneybetween identical twins. JAMA, 1956. 160: p. 227-231.
Meyerson BA, Linderoth B, Karlsson H, et al. Microdialysis in the human brain: extracellularmeasurements in the thalamus of parkinsonian patients. Life Sci, 1990. 46: p. 301-309.
Monaco AP, Maki T, Ozato H, et al. Transplantation of islet allografts and xenografts in totallypancreatectomized diabetic dogs using the hybrid artificial pancreas. Ann Surg, 1991. 214(3): p.339-361.
Monaco AP. Transplantation of pancreatic islets with immunoexclusion membranes. TransplantProc, 1993. 25: p. 2234-2236.
78
Morris PJ. The immunobiology of cell transplantation. Cell Transplantation, 1993. 2: p. 7-12.
Moskalewski S. Isolation and culture of the islets of Langerhans of the guinea pig. Gen CompEndocrin, 1965. 5: p. 342-345.
Moxey-Mims M, Kay C, Light JA, et al. Increased incidence of insulin-dependent diabetesmellitus in pediatric renal transplant patients receiving Tacrolimus (FK 506). Transplantation,1998. 65(5): p. 617-619.
Mutsaers SE, Bishop JE, Mc Grouther G, et al. Mechanisms of tissue repair: from woundhealing to fibrosis. Int J Biochem Cell Biol, 1997. 29(1): p. 5-17.
Myerhoff C, Bischof F, Sternberg F, et al. On-line continuous monitoring of subcutaneous tissueglucose in men by combining portable glucose sensor with microdialysis. Diabetologia, 1992. 35:p. 1087-1092.
Nilsson GE, Tenland T, Öberg PÅ. Evaluation of laser-Doppler flowmeter for measurement oftissue blood flow. IBID., BME, 1980. 27: p. 597-604.
Ohazato H, Carretta M, Maki T, et al. Use of xenogeneic islets in hybrid artificial pancreas fortreatment of diabetes without immunosuppression. Transplant Proc, 1992. 24(2): p. 661-662.
O′Shea GM, Goosen MFA, Sun AM. Prolonged survival of transplanted islets of Langerhansencapsulated in a biocompatible membrane. Biochim Biophys Acta, 1984. 804: p. 133-136.
Padera R, Colton C. Time course of membrane microarchitecture-driven neovascularization.Biomaterials, 1996. 17: p. 277-284.
Paradis K, Langford G, Long Z., et al. Search for cross-species transmission of porcineendogenous retrovirus in patients treated with living pig tissue. Science, 1999. 285: p. 1236-1241.
Partridge TA, Morgan JE, Coulton GR, et al. Conversion of mdx myofibers from dystropin-negative to- positive by injection of normal myoblasts. Nature, 1989. 337: p. 176-179.
Perlow MJ, Freed WJ, Hoffer BJ, et al. Brain grafts reduce motor abnormalities produced bydestruction of nigrostriatal dopamine system. Science, 1979. 204: p. 643-647.
Rabinovitch A. Role of cytokines in IDDM pathogenesis and islet b-cell destruction. DiabetesRev, 1993. 1: p. 215-240.
Rajotte RV, Warnock GL, Evans M, et al. Isolation of viable islets of Langerhans fromcollagenase-perfused canine and human pancreata. Transplant Proc, 1987. 19(916-918).
Reach G. Bioartificial pancreas, present state and future prospects. Biomed Biochim Acta, 1984.43(5): p. 569-576.
Reach G. Artificial and bioartificial replacement of the endocrine pancreas. Artif Organs, 1992.16(1): p. 61-70.
Reach G. Bioartificial pancreas. Diabet Med, 1993. 10: p. 105-109.
79
Reach G. Bioartificial pancreas. Transplant Proc, 1994. 26(2): p. 397-398.
Ricordi C, Lacy PE, Finke EH, et al. An automated method for the isolation of humanpancreatic islets. Diabetes, 1988. 37: p. 413-420.
Ricordi C, Socci C, Davalli AM, et al. Isolation of the elusive pig islet. Surgery, 1990. 107: p.688-692.
Ricordi C, Tzakis A, Carroli P, et al. Human islet isolation and allotransplantation in 22consecutive cases. Transplantation, 1992. 53: p. 407-414.
Sandberg J-O, Olsson N, Johanson RC, et al. Immunosuppression, macroencapsulation andultraviolet-B irradiation as immunoprotection in porcine pancreatic islet xenotransplantation.Pharmac & Toxic, 1995. 76: p. 400-405.
Sandler S, Andersson A, Hellerström C. Inhibitory effects of interleukin-1 on insulin secretion,insulin biosynthesis, and oxidative metabolism of isolated rat pancreatic islets. Endocrinology,1987. 121(4): p. 1424-1431.
Scharp DW, Lacy PE, Ricordi C, et al. Human islet transplantation in patients with type-1diabetes. Transplant Proc, 1989. 21(1): p. 2744-2745.
Scharp DW, Lacy PE, Santiago JV, et al. Insulin-independence after islet transplantation intotype-1 diabetic patient. Diabetes, 1990. 39: p. 515.
Scharp DW, Lacy PE, Santiago JV, et al. Results of our first nine intraportal islet allografts intype 1, insulin-dependent diabetic patients. Transplantation, 1991. 51: p. 76-85.
Scharp DW, Marchetti P, Swanson C, et al. The effect of transplantation site and islet mass onlong-term survival and metabolic and hormonal function of canine purified islet autografts. CellTransplantation, 1992. 1: p. 245-254.
Scharp DW, Swanson CJ, Olack BJ, et al. Protection of encapsulated human islets implantedwithout immunosuppression in patients with type -I or type II diabetes and nondiabetic controlsubjects. Diabetes, 1994. 43: p. 1167-1170.
Schlumpf R, Largiader F, Uhlschmid G.K., et al. Is cyclosporine toxic for transplantedpancreatic islets? Transplant Proc, 1986. 28: p. 1175-1176.
Schrezenemeir J, Gerö L, Laue C, et al. The role of oxygen supply in islet transplantation.Transplant Proc, 1992. 24(6): p. 2925-2929.
Schrezenemeir J, Kirchgessner J, Gerö L. Effects of microencapsulation on oxygen distributionin islet organs. Transplantation, 1994. 57: p. 1308-1314.
Scott DO, Lunte CE. In vivo microdialysis sampling in the bile, blood, and liver of rats to studythe dispositional of phenol. Pharmaceut Res, 1993. 10(3): p. 335-342.
Shapiro R, Jordan ML, Scantlebury VP, et al. A prospective randomized trial of FK506-basedimmunosuppression after renal transplantation. Transplantation, 1995. 59(4): p. 485-490.
80
Shapiro R, Jordon ML, Scantlebury VP, et al. A prospective, randomized trial of Tacrolimus/Prednisone versus Tacrolimus/ Prednisone/Mycophenolate Mofetil in renal transplant recipients.Transplantation, 1999. 67(3): p. 411-415.
Smets YFC, Westendorp RGJ, van der Pijl JW, et al. Effect of simultaneous pancreas-kidneytransplantation on mortality of patients with type-1 diabetes mellitus and end-stage renal failure.The Lancet., 1999. 353: p. 1915-1919.
Socci C, Falqui L, Falorni J, et al. Fresh human islet transplantation to replace pancreaticendocrine function in type-1 diabetic patients. Acta Diabetol, 1991. 28: p. 151.
Solheim BG, Ferrone S, Moller E. The HLA system in clinical transplantation. Springer-Verlag,Berlin, Heidelberg, 1993.
Sollinger HW, Mack E, Cook K, et al. Allotransplantation of human parathyroid tissue withoutimmunosuppression. Transplantation, 1983. 36: p. 599-602.
Soon- Shiong P, Otterlie M, Skjak-Braek G, et al. An immunological basis for the fibroticreaction to implanted capsules. Transplant Proc, 1991. 23(1): p. 758-759.
Soon- Shiong P. Treatment of type-1 diabetes using encapsulated islets. Adv. Drug Deliv. Rev.,1999. 35: p. 259-270.
Soon-Shiong P, Feldman E, Nelson R. Successful reversal of spontaneous diabetes in dogs byintraperitoneal microencapsulated islets. Transplantation, 1992a. 54(5): p. 769-774.
Soon-Shiong P, Feldman E, Nelson R, et al. Long-term reversal of diabetes in the large animalmodel by encapsulated islet transplantation. Transplant Proc, 1992b. 24(6): p. 2946-2947.
Soon-Shiong P, Heintz RE, Merideth N. Insulin-independence in a type-1 diabetic patient afterencapsulated islet transplantation. The Lancet, 1994. 343: p. 950-951.
Starzl TE, Abu-Elmagd K, Tzakis. A., et al. Selected Topics on FK 506, with special referencesto rescue of extrahepatic whole organ grafts, transplantation of " forbidden organs," side effects,mechanism, and practical pharmacokinetics. Transplant Proc, 1991. 23(1): p. 914-919.
Sterio DC. The unbiased estimation of number and sizes of arbitary particles using the dissector.J Microsc, 1984. 134: p. 127-136.
Stern MD. In vivo evaluation of microcirculation by coherent light -scattering. Nature, 1975.254(5495): p. 56-8.
Stern MD, Lappe DL, Bowen PD. Continuos measurement of tissue blood flow by laser-Dopplerspectroscopy. Am J Physiol, 1977. 232(4): p. H441-H444.
Stratta RJ. Impact of pancreas transplantation on the complication of diabetes. Curr Opinion inOrgan Transplant, 1998. 3: p. 258-273.
Sullivan SJ, Maki T, Borland KM, et al. Biohybrid artificial pancreas: long-term implantationstudies in diabetic, pancreatectomized dogs. Science, 1991. 252: p. 718-721.
81
Sullivan SJ, Maki T, Carretta M, et al. Implantation of A hybrid artificial pancreas in diabeticdogs. Transplant Proc, 1992. 24(3): p. 942-944.
Sun Y, Ma X, Zhou D, et al. Normalization of diabetes in spontaneously diabetic cynomologusmonkey by xenografts of microencapsulated porcine islets without immunosuppression. J ClinInvest, 1996. 98(6): p. 1417-1422.
Sutherland DER. Pancreas and islet transplantation: now and then. Transplant Proc, 1996.28(4): p. 2131-2133.
Sutherland DER, Cecka M, Gruessner AC. Report from the international pancreas transplantregistry. Transplant Proc, 1999. 31: p. 597-601.
Suzuki K, Bonner-Weir S, Hollister J, et al. A method for estimating number and mass of isletstransplanted within a membrane device. Cell Transplantation, 1996. 5(6): p. 613-625.
Suzuki K, Bonner-Weir S, Trevidi N, et al. Function and survival of macroencapsulatedsyngeneic islets transplanted into streptozocin-diabetic mice. Transplantation, 1998a. 66(1): p. 21-28.
Suzuki K, Bonner-Weir S, Hollister-Lock J, et al. Number and volume of islets transplanted inimmunobarrier devices. Cell Transplantation, 1998b. 7(1): p. 47-52.
Takebe K, Shimura T, Munkhbat B, et al. Xenogeneic (pig-to-rat) fetal liver fragmentstransplantation using macrocapsules for immunoisolation. Cell Transplantation, 1996. 5(S51): p.S31-S33.
Tan-Shalaby J, Tempero M. Malignancies after liver transplantation. Seminars in liver disease,1995. 15: p. 1156-1164.
Tatarkiewicz K, Hollister-Lock J, Quickel RR, et al. Reversal of hyperglycemia in mice aftersubcutaneous transplantation of macroencapsulated islets. Transplantation, 1999. 67(5): p. 665-671.
Theodorou NA, Vrbova H, Tyhurst M. Problems in the use of polycaronate diffusion chambersfor syngeneic pancreatic islet transplantation in rats. Diabetologia, 1988. 31: p. 54-57.
Thollander M, Hellström PM, Gazelius B. Semi-invasive laser-Doppler flowmetry technique. IntJ Microcirc, 1997. 17: p. 15-21.
Thomas ED, Storb R, Fefer A, et al. Aplastic anaemia treated by marrow transplantation. TheLancet, 1972. 1(7745): p. 284-289.
Thomas ED, Buckner CD, Banaji M, et al. One hundred patients with acute leukemia treated bychemotherapy, total body irradiation, and allogeneic marrow transplantation,. Blood, 1977.49(4): p. 511-533.
Tibell A, Brauker JH, Johnston W, et al. Tissue reactions to implanted membranes: A study inhuman subjects. Cell Transplantation, 1992. 1(3): p. 174 (Abstract).
Tibell A, Rafael E, Wennberg L, et al. Transplantation of macroencapsulated parathyroid tissuein man. Cell Transplantation, 1996. 5(5S-2): p. 54 (Abstract).
82
Tibell A, Wu GS, Zhu S, et al. Macroencapsulation reduces the risk of sensitization after islettransplantation. 7 Th. World congress of the IPITA, Sydney, Australia, 1999: p. 153 (Abstract).
Tossman U, Ungerstedt U. Microdialysis-principles and applications for studies in animals andman. J Intern Med, 1991. 230: p. 365-373.
Trivedi N, Suzuki K, Bonner-Weir S, et al. Islet number in an immunobarrier device required totreat diabetes in mice. Transplant Proc, 1997. 29: p. 2142-2143.
Tydén G, Tibell A, Bolinder J, et al. High incidence of late rejections in preuremic recipients ofpancreas transplants given alone or in combination with renal transplants. Transplant Proc, 1990.222: p. 398-401.
Tydén G, Bolinder J, Solders G, et al. Improved survival in patients with insulin-dependentdiabetes mellitus and end-stage diabetic nephropathy 10 years after combined pancreas andkidney transplantation. Transplantation, 1999. 67(5): p. 645-648.
Tzakis AG, Ricordi C, Alejandro R, et al. Pancreatic islet transplantation after upperabdominal exenteration and liver replacement. Lancet, 1990. 336: p. 402.
Tze WJ, Tai J, Cheung S. In vitro effects of FK-506 on human rat islets. Transplantation, 1990.49: p. 1172-1174.
Ungerstedt U, Pycock C. Functional correlates of dopamine neurotransmission. Bull SchweizAkad Med Wiss, 1974. 1278: p. 1-5.
Ungerstedt U. Microdialysis - principle and applications for studies in animal and man. J InternMed, 1991. 230: p. 365-373.
van Schilfgaarde R, van der Burg MPM, van Suylichem PTR, et al. Does Cyclosporineinfluence B-cell function? Transplant Proc, 1986. 28(5): p. 1175-1176.
van Schilfgaarde R, de Vos P. Factors influencing the properties and performance ofmicrocapsules for immunoprotection of pancreatic islets. J Mol Med, 1999. 77: p. 199-205.
Vandenbossche GMR, Bracke ME, Cuvelier CA, et al. Host reaction against empty alginate-polylysine microcapsule. Influence of preparation procedure. J Pharm Pharmacol, 1993. 45: p.115-120.
Vanholder R, Rigoir S. Bioartificial pancreas and liver: a review. Intern J of Artif Organs, 1991.14(7): p. 398-402.
Vilcek J, Palombella VJ, Henriksen-Destefano D, et al. Fibroblast growth-enhancing activity oftumor necrosis factor and its relationship to other polypeptide growth factors. J Exp Med, 1986.163: p. 632-643.
Walgenbach S, Hommel G, Junginger T. Prospective study of parathyroid graft function inpatients with renal hyperparathyroidism after total parathyroidectomy and heterotopicautotransplantation by measurements of the intact parathyroid hormone concentrations in bothantecubital veins. Eur J Surg, 1999. 165: p. 343-350.

83
Wang T, Lacik I, Brissova M, et al. An encapsulation system for the immunoisolation ofpancreatic islets. Nature Biotechnology, 1997. 15: p. 358-362.
Warnock GL, Rajotte RV. Critical mass of purified islets that induce normoglycemia afterimplantation into dogs. Diabetes, 1988. 37: p. 467-471.
Warnock GL, Kneteman NM, Ryan EA. Normoglycemia after transplantation of freshlyisolated and cryopreserved pancreatic islets in type-I (insulin-dependent) diabetes mellitus.Diabetologia, 1991. 34: p. 55-58.
Weber CJ, Zabiniski S, Koschitzky T, et al. The role of CD4+ helper T-cells in the destructionof microencapsulated islet xenograft in NOD mice. Transplantation, 1990. 49: p. 396-404.
Weibel ER. Stereological methods, Practical methods for biological morphometry. AcademicPress, London, New York, Toronto, Sydney, San Francisco, 1979.
Wheatley AM, Zhao D. Intraoperative assessment by laser-Doppler flowmetry of hepaticperfusion during orthotopic liver transplantation in the rat. Transplantation, 1993. 56(5): p. 1315-1318.
Williams PW. Notes on diabetes treated with extract and by grafts of sheep’s pancreas. Br Med J,1894. 2: p. 1303-1306.
Winn SR, Hammang JP, Emerich DF, et al. Polymer-encapsulated cells genetically modified tosecrete human growth factors promote the survival of axotomized septal cholineargic neurones.Proc Natl Acad.Sci, 1994. 91: p. 2324-2328.
Wozniewisc B, Migaj M, Giera B, et al. Cell Culture preparation of human parathyroid cells forallotransplantation without immunosuppressives. Transplant Proc, 1996. 28(6): p. 3542-3544.
Zekorn T, Sieberes U, Filip L, et al. Bioartificial pancreas: the use of different hollow fibers as adiffusion chamber. Transplant Proc, 1989. 21(1): p. 2748-2750.
Zekorn T, Siebers U, Bretzel RG, et al. Protection of islets of Langerhans from interleukin-1toxicity by artificial membranes. Transplantation, 1990. 50(3): p. 391-394.
Zekorn T, Horcher U, Siebers K, et al. Islet transplantation in immunoseparating membranesfor treatment of insulin-dependent diabetes mellitus. Exp Clin Endocrinol Diabetes, 1995. 103: p.136-139.
Zekorn T, Horcher A, Mellert J, et al. Biocompatability and immunology in the encapsulation ofislets of Langerhans (bioartificial pancreas).Intern J Artif Organs, 1996. 19(4): p. 251-257.
Zukosoki CF, Lee HM, Hume DM. Surg. Forum, 1960. 11: p. 470-472.