ceased, provided that the exercise had lasted for many hours
TRANSCRIPT
J. Phy8iol. (1973), 229, pp. 77-85 77With 1 text-figurePrinted in Great Britain
ELEVATION IN SET POINT FOR BODY TEMPERATUREREGULATION AFTER PROLONGED EXERCISE
BY J. S. J. HAIGHT* AND W. R. KEATINGEFrom the Department of Physiology, London Hospital
Medical College, Turner Street, London El 2AD
(Received 17 July 1972)
SUMMARY
1. In nine healthy men, after prolonged exercise (approximately 37 kmwalk and 2-5 km ascent and descent in 9 hr) deep body temperature at reststabilized at a higher level than in the absence of previous exercise.
2. The increase, approximately 0.36° C, was recorded at both oral andrectal sites. It persisted while the subjects rested in warm and in coolsurroundings, and disappeared about 11 hr after the end of exercise.
3. The increase in body temperature after exercise was accompaniedby a similar increase in the body temperature at which sweating startedduring body heating.
4. After exercise the subjects' metabolic response to cold air (13.60 C)was normal or increased in spite of the elevation in body temperature.
5. Blood glucose concentration was never lower than 3-1 mm duringthese experiments.
6. The temperature changes are most easily explained by mild pyrexiadue to the release of endogenous pyrogen associated with minor tissuedamage.
INTRODUCTION
This study was undertaken to see whether prolonged physical exertionwas followed by any disturbance in the regulation of body temperature.People who collapse on hill-walks in cold surroundings often do so afterexercising to the point of exhaustion (Mountain Rescue Committee, 1969)and hypothermia is thought to be responsible for the deaths which some-times ensue (Pugh, 1966; Grieve, 1968; Strang, 1969). Any disturbance intemperature regulation produced by prolonged exercise could be of in-terest in relation to these deaths.
Preliminary studies suggested that exercise produced an elevation ofbody temperature which persisted for long periods after the exercise hadceased, provided that the exercise had lasted for many hours. The experi-
* M.R.C. Scholar.

J. S. J. HAIGHT AND W. R. KEATINGE
ments described in this paper were made to establish the existence ofsuch an elevation in stable body temperature after exercise under closelycontrolled conditions, and to determine its size, duration and probablecause. Measurements were made of metabolic rate as well as body tem-perature in warm and cold surroundings, of the body temperature at whichthe subjects began to sweat when they were heated artificially, and of thewhite blood cell count and blood glucose concentration. A sustainedelevation in temperature after exercise does not seem to have been recordedbefore, although a fatigue fever was postulated without real evidence inthe last century (Rendon, 1888; Knott, 1888; Peter, 1889). Since that timea number of essentially negative findings have been reported, probablybecause measurements were made after relatively short periods of exercise.For example Bardswell & Chapman (1911) found that a 9 6 km run, andDouglas & Koch (1951) that a 16 km walk, was followed by a return ofrectal temperature to control levels within 1 hr. Downey & Darling (1962)showed that salicylates did not accelerate significantly the fall in bodytemperature after about 30 min exercise on a treadmill.The present studies were made under conditions in which hypoglycaemia
would not be expected and did not occur. The following paper (Haight &Keatinge, 1973) describes disturbances in temperature regulation duringhypoglycaemia produced by ethanol in association with shorter thoughmore intense exercise. A preliminary account of the present findings hasbeen published (Haight & Keatinge, 1970).
METHODS
SubjectsThe subjects were nine male volunteers aged 19-25 (mean 22.5) yr. They were
initially given a routine medical examination for cardiovascular and respiratorydisease and found to be healthy. Most of them had experience of hill-walking orstrenuous games but none was in a high state of training at the time of the experi-ments, having taken no more exercise than one or two games of Rugby football inthe previous 3 weeks. All of them understood the nature of the study and consentedto be subjects in the experiments.
General procedureThe heights, weights and skinfold thicknesses of the subjects were measured
immediately before the first experiment. Each subject was then studied twice withan interval of 21-28 days. For one of these studies (test experiment) they spent theday walking and doing stepping exercises that were designed to mimic a strenuoushill walk, before being subjected to body temperature, sweat and metabolic ratemeasurements while at rest in warm and cold surroundings. Blood and urine sampleswere also taken. For the other study, which served as a control, the subject spentthe day in sedentary activities after which similar measurements were made of bodytemperature, sweating and metabolic rate, and blood and urine composition. Thecontrol measurements on each subject were made at the same time of day as the test
78

PYREXIA AFTER PROLONGED EXERCISE 79
measurements so that the comparison would not be distorted by diurnal fluctuations.The order in which the two studies were made was varied between subjects tominimize any changes due to habituation or training. Test studies were made firstin subjects 1, 5, 6 and 8, and control studies first in the remainder.
Details of procedure
Exercise. At approximately 8.30 a.m. the subjects started to walk a level outdoorcircuit (10-4 km long) as fast as possible wearing whatever clothing they found mostcomfortable for the air temperature, which varied between 0-4 and 15-50 C. Aftercompleting this and resting for 10 min they stepped on and off a box (height 18 cm)for 20-30 min, initially at 31 cycles/min, but slowing as they became tired. Theythen repeated the whole procedure until they were too stiff and tired to continue,8-10 hr after exercise was started. During this time they covered 31-2-41-6 (mean37-1) km walking, and ascended and descended 1-86-3-56 (mean 2-49) km box-stepping.
Diet. Subjects 1-6 ate only carbohydrate (calorie value about 240 keal) on theevening of experiments, in order to minimize any disturbance of the subsequentmeasurements as carbohydrate has little specific dynamic action and no significanteffect on body temperature (Rubner, 1902; Lusk, 1912-13). For the same reasonsubjects 7, 8 and 9 ate nothing from 18 hr before the start of each experiment untilthe experiment finished. All subjects were allowed unlimited water, with addition ofsmall amounts of salt (up to 14 g) if they wished.Measurement of stable body temperature. After exercise, or after a control day of
sedentary activities, the subject sat fully clothed in still air at 21 + 20 C with an oraland rectal thermocouple in position until the temperatures stabilized. This point wasdefined by neither temperature changing more than 0-05° C in 15 min.Measurement of sweat onset temperature. The subject's legs were then immersed
up to the knees in warm (40-430 C) water to raise the deep body temperature, andthe temperatures at which sweating started were noted. Sweat was detected bypainting tincture of iodine on the forehead, allowing it to dry, sprinkling it withstarch powder, and noting the appearance of blue dots when sweating began.
Blood sampling and metabolic rate in the warm room. The left arm (subjects 4-9only) was immersed in warm water (40-430 C) for 5 min to raise local blood flow, anda blood sample taken from the antecubital vein. Expired air was then collected for10 min to measure metabolic rate, and rectal temperature noted.
Cold exposure. The subject then sat for 30 min, wearing only shorts, in a refri-gerated room at 13-6 + 1-5° C containing a fan which propelled the air towards himat 15-3 + 0-8 km/hr. Rectal temperature was noted after 15 and 30 min and all of theair expired during the cold exposure was collected and used to determine metabolicrate. Immediately afterwards a urine sample was collected.
Measurements during the night. The subject then slept on an air bed wearingpyjamas and wrapped in a blanket, in still air at 15-0 + 2° C; rectal temperature wasnoted at 2 hr intervals.
Measurements after waking. At 6.00 a.m., 91-111 hr after exercise ended, expiredair was collected with the subject still lying down, for metabolic rate determination.The subject dressed and sat in still air at 21 + 20 C to enable stable rectal and oraltemperatures to be recorded as before. His legs were then immersed in water at40-430 C to enable sweat onset temperatures to be measured, and a venous bloodsample and urine sample were collected as before.

J. S. J. HAIGHT AND Wf. R. KEATINGE
Techniques of measurementSkinfold thickness and surface area. Skinfold thickness was measured with
Harpenden Calipers (Edwards, Hammond, Healy, Tanner & Whitehouse, 1955).Points of measurement were triceps mid-way between tip of acromion and olecranonprocesses, subscapular over the lower angle of the scapula, subcostal over the costalmargin vertically below the centre of the clavicle, and abdominal at the level of theintertubercular plane vertically below the centre of the clavicle. Four readings weremade from each site and the mean taken. These sites give a good indication of over-all surface fat thickness (Hammond, 1955). Surface area was obtained from heightand weight by the nomogram of Weir (1949).
Temperature measurement. Air temperature was measured by calibrated mercurythermometers. Oral and rectal temperatures were measured by a thermocoupleassembly (Ellab, TE3). After allowing for a small calibration error the readings wereaccurate to + 0.0250 C. Oral temperature was recorded from a probe placed under thetongue, after the mouth had been closed for at least 10 min. Rectal temperature wasrecorded from a probe that had been inserted 10 cm from the anus for at least10 min.
Metabolic rate. The subjects, wearing a nose clip, breathed through a valve assemblyfor a measured time into modified Douglas bags of 5001 capacity made of polvinylchloride (Plysu Co.). The oxygen percentage of the collected gas was measured by aparamagnetic 02 analyser (Beckman E2), its volume by a dry gas meter (Parkinson),and the temperature of the gas flowing into it by a mercury thermometer in the in-take tube of the meter. Metabolic rates were calculated from the measurements bythe method of Weir (1949).
Blood determinations. A standard white cell count was made with an improvedNeubauer Haemocytometer after diluting the venous blood samples in 167 mm aceticacid and 4 1 mm gentian violet solution. Differential counts were made on smearsof the blood stained by Leishman dye.For blood glucose determinations 1 ml. venous blood taken into a citrate tube
was analysed for glucose on an autoanalyser, using the glucose oxidase method.Urine examination. Haemocombistix papers (Ames Co.) were used to test for the
presence of haemoglobin and protein in urine. A fresh drop of urine was placed on aslide under a cover slip and examined by microscope for the presence of blood cells.
Statistics. Comparisons were made by the paired Student t test.
RESULTS
The subjects. The subjects' heights were between 163 and 182 (mean175) cm; weight between 50-0 and 82-7 (mean 70.0) kg; surface areabetween 1-52 and 2-04 (mean 1.85) M2; and average skinfold thickness atthe four sites between 7 0 and 13-8 (mean 9.3) mm. The mean weight andskinfold thickness are close to the standard weight of 69 1 kg quoted byBrozek & Keys (1951) and skinfold thickness close to the value of 7-6 mmquoted by Hammond (1955) for men aged 20.
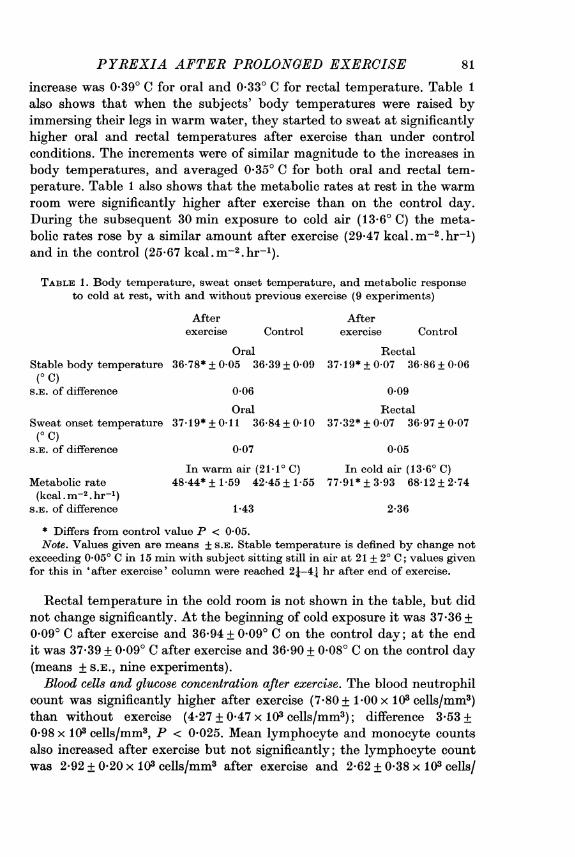
Stable body temperature, sweat onset temperature, and metabolic responseto cold after exercise. Table 1 shows that when the subjects sat quietly inwarm air after a day of exercise their oral and rectal temperature stabilizedat a significantly higher level than after a day of sedentary activities. The
80
PYREXIA AFTER PROLONGED EXERCISE
increase was 0.390 C for oral and 0,330 C for rectal temperature. Table 1also shows that when the subjects' body temperatures were raised byimmersing their legs in warm water, they started to sweat at significantlyhigher oral and rectal temperatures after exercise than under controlconditions. The increments were of similar magnitude to the increases inbody temperatures, and averaged 0 35° C for both oral and rectal tem-perature. Table 1 also shows that the metabolic rates at rest in the warmroom were significantly higher after exercise than on the control day.During the subsequent 30 min exposure to cold air (13-6' C) the meta-bolic rates rose by a similar amount after exercise (29.47 kcal. M-2. hr-1)and in the control (25-67 kcal.m-2.hr-1).
TABLE 1. Body temperature, sweat onset temperature, and metabolic responseto cold at rest, with and without previous exercise (9 experiments)
After Afterexercise Control exercise Control
Oral RectalStable body temperature 36-78* + 0-05 36-39 + 0 09 37-19* + 0 07 36-86 + 0-06(O C)
S.E. of difference 0-06 0 09
Oral RectalSweat onset temperature 37.19* +0-11 36-84+ 0 10 37-32* + 0 07 36-97+ 0 07(O C)
S.E. of difference 0-07 0 05
In warm air (21.10 C) In cold air (13-60 C)Metabolic rate 48.44* + 1-59 42-45+ 1-55 77-91* + 3.93 68-12+ 2.74(kcal . m-2. hr-L)
S.E. of difference 1*43 2-36
* Differs from control value P < 0-05.Note. Values given are means + S.E. Stable temperature is defined by change not
exceeding 0.050 C in 15 min with subject sitting still in air at 21 + 20 C; values givenfor this in 'after exercise' column were reached 21-41 hr after end of exercise.
Rectal temperature in the cold room is not shown in the table, but didnot change significantly. At the beginning of cold exposure it was 37-36 +0 09° C after exercise and 36-94 + 0 09° C on the control day; at the endit was 37-39 + 0 090 C after exercise and 36-90 + 0 08° C on the control day(means + sE., nine experiments).Blood cells and glucose concentration after exercise. The blood neutrophil
count was significantly higher after exercise (7x80 + 1 00 x 103 cells/mm3)than without exercise (4.27 + 0 47 x 103 cells/mm3); difference 3*53 +0-98 x 103 cells/mm3, P < 0-025. Mean lymphocyte and monocyte countsalso increased after exercise but not significantly; the lymphocyte countwas 2-92 + 0-20 x 103 cells/mm3 after exercise and 2-62 + 0*38 x 103 cells/
81

J. S. J. HAIGHT AND W. R. KEATINGEmm3 in the controls; the monocyte counts 0*35 + 0-08 x 103 cells/mm3 afterexercise and 0-20 + 0-03 x 103 cells/mm3 in the controls.
Blood glucose concentration remained within normal limits. It was3*77 + 0*22 mm after exercise and 3 70 + 0*18 mm in the controls; no valuewas lower than 3-1 mm, and the difference between test and control experi-ments was not significant.
All of the above values are means + S.E. of six experiments (subjects4-9).
370
u 36.5 -
a.~ ~~Tmeam
E0
36.0
35.5
3 5 7Time a.m.
Fig. 1. Rectal temperature during night after prolonged exercise. 0-0 Afterexercise. 0- Control. Values are means + S.E. of nine experiments.
Urine changes after exercise. After a day of sedentary activity none ofthe six urine samples (subjects 4-9) gave a clear positive reaction forprotein or haemoglobin, or contained erythrocytes or leucocytes. Afterexercise all gave positive reactions for protein; the urine of two subjects(nos. 5 and 9) also gave positive reactions for haemoglobin, and containedlarge numbers of red and white cells. None of the others gave a clearpositive reaction for haemoglobin after exercise but with subjects 4 and 7a few red and white cells could be seen. Similar urine changes to these havebeen observed after marathon races (Barach, 1910).
Duration of the disturbances. The mean rectal temperature remainedhigher throughout the 6 hr night's rest after exercise than under controlconditions (Fig. 1). However, the difference gradually decreased during thistime and was no longer significant by 7 a.m., on average 10 hr 52 min afterthe end of exercise.
Other measurements 10-16 hr after the end of exercise showed that allabnormalities had virtually disappeared by this time. Metabolic rate(kcal . m-2. hr-1) measured during the last 30 min of the night's rest was
82

PYREXIA AFTER PROLONGED EXERCISE
almost the same after exercise as in the control experiment: 44-34 + 1-25compared to 41-59 + 176. Stable oral temperature in the warm room14-15 hr after exercise was 36-32 + 0.080 C compared to 36-32 + 0-15' C inthe control. Sweat onset temperatures were 36-78 + 0-13° C (oral) and36-82 + 0.08° C (rectal) after exercise compared to 36-99 + 0.120 C (oral)and 37-00 + 0.140 C (rectal) in the control. All of these values are means+ S.E., nine experiments, and show no significant differences between afterexercise and control values. Urine samples (subjects 4-9) at this time afterexercise showed a weak positive reaction for protein in only 1 case (subject5) and no positive reaction of haemoglobin. None contained excess cellsexcept the sample from subject 5 which contained a few leucocytes.
Subjective observations. The subjects complained of muscle and jointpains and sore feet at the end of the day's exercise. Most of them had smallabrasions on the feet. The morning after exercise muscle stiffness per-sisted, but otherwise they had few complaints.
DISCUSSION
The main findings were that after prolonged exercise in cool surround-ings body temperature was regulated at a higher level than normal forapproximately 11 hr. Body temperature stabilized at a higher level at rest,the body temperature needed to produce sweating was increased by thesame amount, and the metabolic response to a standard cold stress was atleast as large as normal in spite of the increase in body temperature. Theseare the changes seen in pyrexia. As long ago as the last century Stern(1892) showed that during fever the stable body temperature in a tem-perate environment, and the body temperature needed to produce sweating,were both increased by a similar amount. The body temperature needed toinduce vasodilatation is also raised in stable pyrexia (Cooper, Cranston &Snell, 1964). No studies ofthe metabolic response to cold seem to have beenmade under these conditions but shivering at the onset of pyrexia is wellknown, and this fact leaves little doubt that pyrexia increases the bodytemperature at which a given metabolic response is produced. The smallelevation in resting metabolic rate that was observed in warm surroundingsafter -exercise must have a different explanation. It was comparable inmagnitude with that seen in the stable phase of mild pyrexia (DuBois,1921), and is attributable at least in part to the direct effect of an im-creased temperature on the rate of cellular metabolism.
It is unlikely that the raised stable body temperature (mean increase0.36° C) after prolonged exercise was due to the slight dehydration thatcan be produced by prolonged outdoor exercise when water is freelyavailable (Pugh, 1969). The subjects had at least 2- hr to correct any
83

J. S. J. HAIGHT AND W. R. KEATINGE
dehydration. Relatively severe fluid loss has only been reported to raisebody temperature by 0.10 C (Senay & Christensen, 1965). Nor is it likelythat the increase in body temperature needed to cause sweating resultedfrom fatigue of the sweat glands due to sweating during the period ofexercise; sweat rate has been reported to decline during exercise in severeheat (Gerking & Robinson, 1946) but there was no evidence that this wasaccompanied by an increase in the threshold body temperature forsweating. The subjects of the present experiments exercised in cool sur-roundings and did not sweat excessively.
There are a number of ways in which prolonged exercise might havecaused the release of endogenous pyrogen in the body. After exercise thesubjects had minor abrasions of their feet, their muscles and joints werepainful, and their urine always contained protein and sometimes leuco-cytes, erythrocytes and haemoglobin. The reason for most of thesechanges is uncertain, but repeated minor trauma is likely to account forthe muscle pain (see Asmussen, 1956), as well as for the other limb pains,while the urine changes may be due to ischaemic damage from the lowrenal blood flow that is known to be produced by exercise (Chapman,Henschel, Minckler, Forsgren & Keys, 1948). This would imply some degreeof cellular damage in each case, and damage to muscle and kidney cells isknown to release endogenous pyrogen from the tissue (Snell & Atkins,1965). Leucocytes also release endogenous pyrogen during phagocytosis(Berlin & Wood, 1964). The well known mobilization of neutrophils intothe circulation during exercise (e.g. Larrabee, 1902), which was seen to amarked degree in the present experiments, will have made large numbersof these cells available for phagocytosis of damaged tissue and releaseof pyrogen.
We are indebted to the Department of Clinical Biochemistry at the RadcliffeInfirmary, Oxford for measuring the blood glucose concentrations in these experi-ments.
REFERENCES
AsMuSSEN, E. (1956). Observations on experimental muscular soreness. Acta rheum.Scand. 2, 109-116.
BARACH, J. H. (1910). Physiological and pathological efiects of severe exertion (themarathon race) on the circulatory and renal systems. Arche intern. Med. 5,382-405.
BARDSWELL, N. D. & CHAPMAN, J. E. (1911). Some observations upon the deeptemperature of the human body at rest and after muscular exertion. Br. med. J.1, 1106-1110.
BERLIN, R. D. & WOOD, W. B. JR. (1964). Studies on the pathogenesis of fever.XIII. The effect of phagocytosis on the release of endogenous pyrogen by poly-morphonuclear leucocytes. J. exp. Med. 119, 715-726.
84

PYREXIA AFTER PROLONGED EXERCISE 85
BROZEK, J. & KEYS, A. (1951 ). The evaluation of leanness-fatness in man: norms andinterrelationships. Br. J. Nutr. 5, 194-206.
CHAPMAN, C. B., HENSCHEL, A., MINCKLER, J., FORSGREN, A. & KEYS, A. (1948).The effect of exercise on renal plasma flow in normal male subjects. J. clin.Invest. 27, 639-644.
COOPER, K. E., CRANSTON, W. I. & SNELL, E. S. (1964). Temperature regulationduring fever in man. Clin. Sci. 27, 345-356.
DOUGLAS, C. G. & KOCH, A. C. E. (1951). Carbohydrate metabolism and muscularexercise. J. Physiol. 114, 208-221.
DOWNEY, J. A. & DARLING, R. C. (1962). Effect of salicylates on elevation of bodytemperature during exercise. J. apple. Physiol. 17, 323-325.
DuBois, E. F. (1921). The basal metabolism in fever. J. Am. med. Ass. 77, 352-355.EDWARDS, D. A. W., HAMMOND, W. H., HEALY, M. J. R., TANNER, J. M. & WXHITE-
HOUSE, R. H. (1955). Design and accuracy of calipers for measuring subcutaneoustissue thickness. Br. J. Nutr. 9, 133-143.
GERKING, S. D. & ROBINSON, S. (1946). Decline in the rates of sweating of menworking in severe heat. Am. J. Physiol. 147, 370-378.
GRIEVE, R. R. (1968). An incident on Ingleborough. Climber 6, 183-184.HAIGHT, J. S. J. & KEATINGE, W. R. (1970). Human temperature regulation after
prolonged intermittent exercise. J. Physiol. 206, 20-21 P.HAIGHT, J. S. J. & KEATINGE, W. R. (1973). Failure of thermoregulation in the cold
during hypoglycaemia induced by exercise and ethanol. J. Physiol. 229, 87-97.HAMMOND, W. H. (1955). Measurement and interpretation of subcutaneous fat, withnorms for children and young adult males. Br. J. prev. soc. Med. 9, 201-211.
KNOTT, J. F. (1888). The fever of over-exertion. Trans. R. Soc. Med. in Ireland 6,77-99.
LARRABEE, R. C. (1902). Leucocytosis after violent exercise. J. med. Res. 2, 76-82.LUSK, G. (1912-13). Animal calorimetry. III. Metabolism after the ingestion of
dextrose and fat, including the behaviour of water, urea and sodium chloridesolutions. J. biol. Chem. 13, 27-47.
MOUNTAIN RESCUE COMMITTEE (1969). Accident report of 1968. Mountaineering 5,49-51.
PETER, (1889). De la fievre de surmenage. J. Med. Paris 2nd series 1, 663-665.PUGH, L. G. C. E. (1966). Clothing insulation and accidental hypothermia in youth.
Nature, Lond. 209, 1281-1286.PUGH, L. G. C. E. (1969). Blood volume changes in outdoor exercise of 8-10 hour
duration. J. Physiol. 200, 345-351.RENDON, V. (1888). Fievres de surmenage. Thesis de la faculty de midecine, Paris,
159 pp. no. 87.RUBNER, M. (1902). Die Gesetze des Energieverbrauchs bei der Ernihrung. Leipzigund Wien: Franz Deuticke.
SENAY, L. C. JR. & CHRISTENSEN, M. L. (1965). Cutaneous circulation duringdehydration and heat stress. J. appl. Physiol. 20, 278-282.
SNELL, E. S. & ATKINS, E. (1965). The presence of endogenous pyrogen in normalrabbit tissues. J. exp. Med. 121, 1019-1038.
STERN, R. (1892). Ueber das Verhalten der Wirmeregulation im Fieber und unterder Einwirkung von Antipyreticis. Z. klin. Med. 20, 63-97.
STRANG, P. J. H. (1969). Death due to exposure to cold in theNew Zealand Mountains.N.Z. med. J. 69, 4-11.
WEIR, J. B. DE V. (1949). New methods for calculating metabolic rate with specificreference to protein metabolism. J. Physiol. 109, 1-9.