ce spectrum handout -...
TRANSCRIPT


Disclaimer
• This slide deck in its original and unaltered format is for educational purposes and is current as of December 2016.6.The content and views presented in this educational activity are those of the authors and do not necessarily reflect those of Creative Educational Concepts or the supporter.
• These materials may discuss therapeutic products that havenot been approved by the US Food and DrugAdministration and off‐label uses of approved products. Aqualified healthcare professional should be consultedbefore using any therapeutic product discussed. Readersshould verify all information and data before treatingpatients or employing any therapies described in thiseducational activity.

Usage Rights
• This slide deck is provided for educationalpurposes and slides may be used for personal,non‐commercial presentations only as long ascontent and references remain the same.
• No part of this slide deck may be published ordistributed in print or electronic formatwithout prior written permission fromCreative Educational Concepts.

• Learning Objective 1. Explore LDL‐C‐lowering:– Data supporting aggressive LDL‐C control for patients at highASCVD risk
– Obstacles to tight control• Statin intolerance• Statin phobia and other reasons for poor adherence• High baseline and low response (e.g. HeFH)
• Learning Objective 2. Examine PCSK9:– Discovery of the protein– Development of anti‐PCSK9 mAb– MoA for anti‐PCSK9 mAb– Lipid efficacy– Safety/tolerability
Outline

2013 ACC/AHA Cholesterol Guidelines: Summary
1. Heart healthy lifestyle habits are the foundationto CVD prevention
2. Assess 10‐year CVD risk every 4‐6 years in adults40‐75 y/o and w/o CVD, DM, not yet on lipidtherapy and w/ LDL 70‐189 mg/dl
3. Recommend high‐intensity statin in those withCVD and age <75 years (statin category 1)
Stone NJ, et al. Circulation. 2013.

4. Recommend high‐intensity statin in those with LDL‐C >190 mg/dl (statin category 2)
5. Recommend moderate‐ or high‐ intensity statin for DM‐1 or DM‐2 aged 40‐75 (statin category 3)
6. Recommend moderate‐ to high‐intensity statin for 40‐75 y/o with >7.5% 10‐year CVD risk (statin category 4)
2013 ACC/AHA Cholesterol Guidelines: Summary – Cont.
Stone NJ, et al. Circulation. 2013.

Treatment Goals for Non‐HDL‐C,LDL‐C, and Apo B in mg/dl
Risk Category Treatment GoalsNon‐HDL‐C LDL‐C Apo B
Low <130 <100 <90
Moderate <130 <100 <90
High <130 <100 <90
Very High <100 <70 <80
NLA 2014 Lipid Recommendations
Jacobson, TA. J Clinical Lipidology. 2015.

https://professional.heart.org/professional/GuidelinesStatements/PreventionGuidelines/UCM_457698_Prevention-Guidelines.jsp
ACC/AHA ASCVD Risk Estimator

https://professional.heart.org/professional/GuidelinesStatements/PreventionGuidelines/UCM_457698_Prevention-Guidelines.jsp
ACC/AHA ASCVD Risk Estimator
App Download
Computer:http://tools.acc.org/ASCVD‐Risk‐Estimator/
Smart phone: https://itunes.apple.com/us/app/ascvd‐risk‐estimator/id808875968?mt=8&ign‐mpt=uo%3D2
https://play.google.com/store/apps/details?id=org.acc.cvrisk&hl=en

• Framingham risk calculator• ACC/AHA risk estimator• MESA CAC risk calculator: https://www.mesa‐nhlbi.org/MESACHDRisk/MesaRiskScore/RiskScore.aspx
• Q‐Risk —DM • UKPDS —DM • 1o vs 2o, DM & RF counting – ATP, NLA
ASCVD Risk Assessment
www.framinghamheartstudy.org/risk‐functions/cardiovascular‐disease/10‐year‐risk.php#;www.dtu.ox.ac.uk/riskengine/; www.qrisk.org/2016/; http://tools.acc.org/ASCVD‐Risk‐Estimator/;
www.lipid.org/recommendations/app; www.mesanhlbi.org/MESACHDRisk/MesaRiskScore/RiskScore.aspx.

Non‐HDL‐C: A Neglected Risk Factor

HDL
LDL
IDL
VLDL
Ath
erog
enic
Lipo
proteins
Non
–HD
L-C
(lip
id);
Apo
B (p
rote
in)
Intermediate‐density lipoprotein• Formed from VLDL with loss of TG• TG ≈ CE• Also known as a VLDL remnant
Low‐density lipoprotein • Formed from IDL with loss of TG• CE >> TG• Main plasma cholesterol carrier
High‐density lipoprotein• Removes cholesterol from peripheral tissues• Other anti‐athero effects
Lp(a)Lipoprotein (a)
• Formed from LDL plus Apo (a)• Very atherogenic/pro‐oxidative
Very‐low‐density lipoprotein• Made in the liver• TG >> CE• Takes lipids from the liver to periphery
Non‐HDL‐C (& Apo B) Include All Atherogenic Lipoproteins
Non–HDL‐C = Cholesterol Component
Non–HDL‐C = TC – HDL‐C
CE=cholesterol ester
Apo B = Protein
Component
www.nhlbi.nih.gov/files/docs/guidelines/atp3xsum.pdf.

Liu J, et al. Am J Cardiol. 2006.
0
0.5
1
1.5
2
2.5
Relativ
e CH
D Risk
LDL‐C, mg/dL
Non‐HDL‐C, mg/dL
<130 130‐159 ≥160
≥190160‐189
<160
Non‐HDL‐C Is Stronger than LDL‐C in Predicting CHD Risk
CHD=coronary heart disease; HDL‐C=high‐density lipoprotein cholesterol; LDL‐C=low‐density lipoprotein cholesterol;NEPTUNE=National Cholesterol Education Program Evaluation ProjecT Utilizing Novel E‐Technology; RE=risk equivalent.
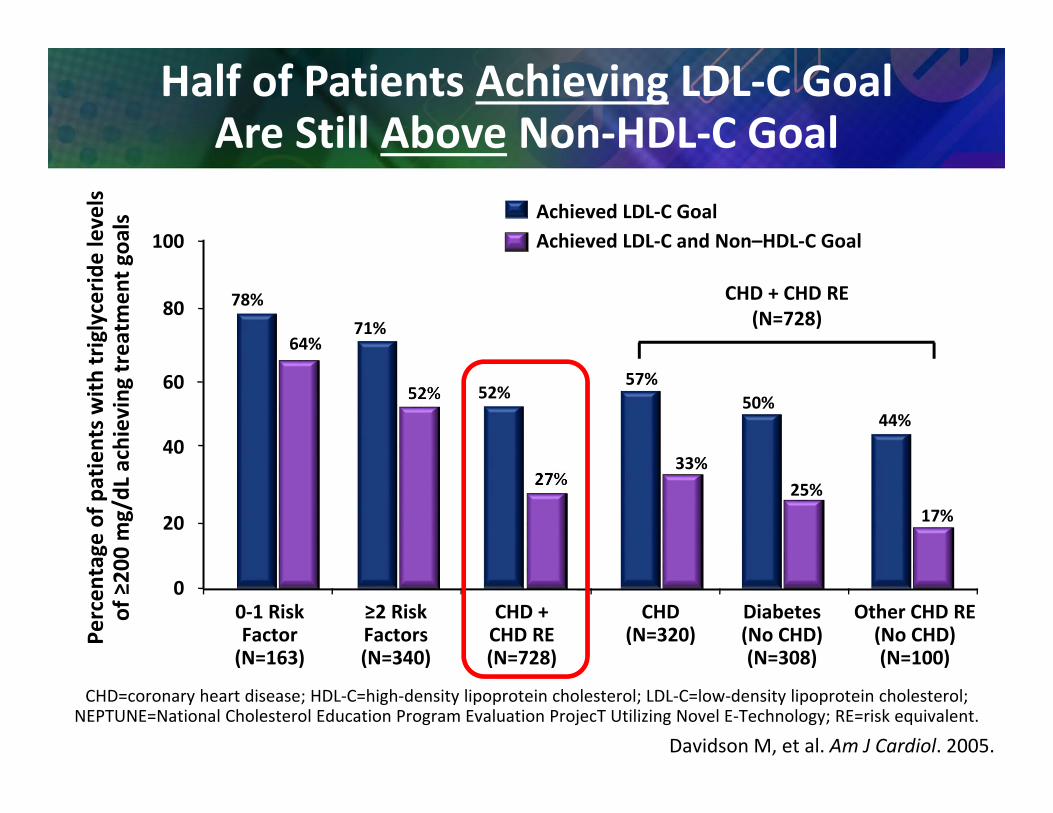
Half of Patients Achieving LDL‐C Goal Are Still Above Non‐HDL‐C Goal
Percen
tage
of p
atients w
ith triglycerid
e levels
of ≥200 mg/dL achieving
treatm
ent g
oals Achieved LDL‐C Goal
Achieved LDL‐C and Non–HDL‐C Goal
0
20
40
60
80
100
78%71%
52%
64%
52%
27%
57%50%
44%
33%25%
17%
0‐1 RiskFactor(N=163)
≥2 RiskFactors(N=340)
CHD +CHD RE(N=728)
CHD(N=320)
Diabetes(No CHD)(N=308)
Other CHD RE(No CHD)(N=100)
CHD + CHD RE(N=728)
Davidson M, et al. Am J Cardiol. 2005.

To Fast or Not to Fast?
Fasting Lipid Panel• Better accuracy for TG• TG cutoffs are based on
fasting values• Slightly better for LDL‐C• Can get fasting glucose
Non‐Fasting Lipid Panel• Can get on any visit• OK Accuracy for TG• Good Non‐HDL‐C accuracy• Reasonable accuracy for other
lipid levels• Could do A1c to follow DM2 risk
Bottom line: fasting panel is slightly better but non‐fasting is more practical

Advanced Lipid Panels
Pros• Lp(a)• Plant sterols • Apo B/LDL‐P• LDL size• HDL size?• HDL‐P?• hsCRP?
Cons• Cost/effort• May not impact clinical decisions
• Might mislead?• Empiric medication trial better?
Bottom line: OK if careful re: cost,if use to decrease over‐Rx

CAC Score Strongly Predicts Coronary Events
Sharma RK, et al. Vascular Health & Risk Mgmt. 2010.Slide courtesy of Thomas White, MD, Cherryville, NC.

CARDIA: CAC >0 in 23‐45% of Asymptomatic Individuals
Age 33‐45 (10 y FRS >2.5% to >10%)
Rozanksi A, Berman DS. JACC Cardiovasc Imaging. 2012.

CAC Predicts Mortality Better than AgeAll‐C
ause M
ortality
per 1
000 pe
rson
‐yrs
Tota‐Maharaj R, et al. Eur Heart J. 2012.

Practical Application of CAC
• Cost not paid by insurance (~$70‐$300)
• Not needed/helpful in 2o prevention
• Best in men 40‐70 y/o, women 50‐70 y/o
• OK in low‐intermed. risk (FRS>2.5%) 33‐45 y/o
• Good in HeFH >20‐30 y/o
• MESA CAC score very helpful: https://www.mesanhlbi.org/MESACHDRisk/MesaRiskScore/RiskScore.aspx

LDL‐C Lowering Treatment

Diet and Exercise

Slide adapted from Thomas White, MD, Cherryville, NC.
Diet too high in calories, sat’d fat, fructose*
*See Brinton EA. Atherosclerosis. 2016.
ExerciseOur Machines & electronics are
“killing us”

April 2, 2016Chicago, Illinois
Slide courtesy of Thomas White, MD, Cherryville, NC.
“Physician heal thyself” (Luke 4:23)

0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
1 2 3 4 5
2nd Least Fit
Most Fit
Least Fit1.0 to 6.0 M
ETS
6.0 to 8.0 M
ETS
8.0 to 10.0
METS
10 to
13
METS
>13
METS
Exercise Benefits Are Greatest at Lowest Fitness
Relativ
e Risk of D
eath
Categories of Exercise Capacity
Slide adapted from Thomas White, MD, Cherryville, NC. Myers J. Circulation. 2003.

0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
1 2 3 4 5
2nd Least Fit
Most FitRelativ
e Risk of D
eath
Least Fit1.0 to 6.0 M
ETS
6.0 to 8.0 M
ETS
8.0 to 10.0
METS
10 to
13
METS
>13
METS
Exercise Benefits Are Greatest at Lowest Fitness
Categories of Exercise Capacity
Slide adapted from Thomas White, MD, Cherryville, NC.
Guidelines set high exercise benefit thresholds, but nearly half of all mortality benefit comes at the 2nd lowest
fitness level!
Myers J. Circulation. 2003.

Statins
Why Not Just Use a High‐Intensity Statin?
Isn’t that what the 2013 ACC/AHA Guidelines Say?
Let’s look at the evidence

Moderate‐Intensity Statin Decreases MACE & MI After 2‐3 years (HOPE‐3)
2nd Co‐1o=CV Mort, NFMI, NF stroke, C‐arrest, CHF, Cor revasc.
↓35%
N=12,705: Age 66, 54% men, BMI 27; Base lipids: LDL‐C 128, TG 128, HDL‐C 45; ~Half had ≥2 RFs: ^WHR>>HBP≈ low HDL‐C> smoker≈ +FHx>>IFG>DM2>CKD.
Yusuf S, et al. N Engl J Med. 2016.
↓25%
Second Co‐primary Outcome Myocardial Infarction

Lower On‐Treatment LDL‐C IS Better!
*Adjusted for age, gender, baseline LDL-C, diabetes mellitus, and prior MI.
Lower Better Higher Better
>80‐100>60‐80>40‐60≤40
Referent0.80 (0.59, 1.07)0.67 (0.50, 0.92)0.61 (0.40, 0.91)
Hazard Ratio
Achieved
LDL‐C
(mg/
dL) N=256
N=631
N=576
N=193
Wiviott SD, et al. J Am Coll Cardiol. 2005.*Similar results reported in 8‐study meta‐analysis: Boekholdt SM, et al. J Am Coll Cardiol. 2014.
Atorvastatin 80 mg vs pravastatin 40 mg, N=2099 ACS pts, 24 mos, f/u.Endpoint: CHD death, nonfatal MI, CVA, recurrent ischemia, revascularization
0 1 2

0
5
10
15
20
25
Achieved LDL‐C (mg/dL)
But LDL‐C Can Still be Elevated on a High‐Intensity Statin!
LDL‐C levels at 4 months on Atorvastatin 80 mg
% of S
ubjects
37.1% of patients ≥70 mg/dL (1.81 mmol/L)
0.1
15.2
19.2
8.2
1.70.5
18
13.3
8.3
5.6
3.22.1 1.4
3.2
Wiviott SD, et al. J Am Coll Cardiol. 2005.*Similar results reported in 8‐study meta‐analysis: Boekholdt SM, et al. J Am Coll Cardiol. 2014.

37%46%
63%72%
0
20
40
60
80
100
Low to ModerateIntensity Statin
Increase to High PotencyStatin
High Potency Statin +Non‐statin
High Potency Statin +2 Non‐statin therapies
Patie
nts A
chieving
LD
L‐C <70 mg/dL
(%)
Many Patients with CAD Do Not Achieve LDL‐C Targets
Estimated Percentage of Patients with a History of CAD Attaining LDL‐C <70mg/dL*
• High‐potency statins include atorvastatin (40 mg or 80 mg), rosuvastatin (20 mg or 40 mg), or simvastatin 80 mg. Moderate‐potency statins include atorvastatin (10 mg or 20 mg), rosuvastatin 10 mg, simvastatin 40 mg, lovastatin 80 mg, or pravastatin 80mg. All other statins were considered low‐potency.
• Non‐statin LDL‐lowering therapies include ezteimbe, niacin, or bile acid sequestrant.
Karalis DG, et al. Cholesterol. 2012.
*Data obtained from a cohort of 9950 patients with a history of CAD at a large cardiology subspecialty practice in Philadelphia, PA area.

Why Not Just Use a High‐Intensity Statin?
Isn’t that what the 2013 ACC/AHA Guidelines Say?
Lower is betterGoals help us direct treatment with statins and statin‐adjuncts
to get lower LDL‐C

Statin Intolerance and Statin Phobia

• Reasons for discontinuation (12% of patients)• Side effects – 62% (mainly muscle Sx: ~50% of all D/C)
• Average of 2 statins tried before stopping• Cost ‐ 17% • Lack of efficacy ‐ 12%
• When/how they stopped• Promptly after a side effect (no further Rx) – 57%• Stopped without asking or telling their HCP – 33%
• Current statin users (88% of patients)• Muscle pain or weakness in 25%, but they continued anyway (with or without
switching)• Muscle Sx↑ w/Metabolic Syndrome (esp↑TG, ↓HDL‐C)• Most patients had potential drug‐drug interaction
Statin Side‐Effects are Common(By Patient Report)
Cohen J, et al. J Clin Lipidol. 2012; Brinton EA, et al. J Clin Lipidol. 2016.
USAGE survey (Understanding Statin Use in America and Gaps in Education)N=10,138: w/ HCP Dx↑chol, Rx statin, ≥18 y/o (internet survey)

Statin % Patients with muscle complaints (N=832)
Pravastatin 40 mg 10.9Atorvastatin 40–80 mg 14.9Simvastatin 40–80 mg 18.2Fluvastatin XL 80 mg 5.1
Muscle Symptoms on High‐Dose Statin Therapy (PRIMO)
N=7924
Bruckert E, et al. Cardiovasc Drugs Ther. 2005.
Note: the XL formulation of fluvastatin greatly reduces statin muscle exposure!

Statin Intolerance: ConclusionsWorking Definition: • Can’t tolerate at least 2 statins (1 at lowest appr. dose)
Manifestations:• Muscle: myalgia, weakness, cramps, stiff, rhabdomyolysis
• Cogni ve (↓memory, “fog”) or mood disturbance (?)• Arthralgia, tendon pain• Other (GI Sx, rash, peripheral neuropathy, ↑transaminase)
After Arca M, Pigna G. Diabetes Metab Syndr Obes. 2011;https://www.acc.org/latest‐in‐cardiology/articles/2015/08/11/09/16/statin‐intolerance‐not‐a‐myth.

Statin Intolerance: ConclusionsWorkup and Management:• If sx persist ~2 m post‐statin D/C, w/u for 1o myop (IMNM) • Test for and treat treatable causes
– Hypothyroidism (measure TSH)– Drug‐drug interaction (change either drug)– Vitamin D deficiency?– CoQ‐10 deficiency??
• Sx often NOT reproducible on blinded re‐challenge, but HCP can’t do this, so should persuade pts to try alternate statins/non‐statins– Trial of XL fluvastatin (or prava, pitava, or very low‐dose rosuva)– Trial of less‐than‐daily statin treatment– Treat with non‐statins (Ezetimibe, PCSK9‐I, BAS, NA)
After Arca M, Pigna G. Diabetes Metab Syndr Obes. 2011;https://www.acc.org/latest‐in‐cardiology/articles/2015/08/11/09/16/statin‐intolerance‐not‐a‐myth.
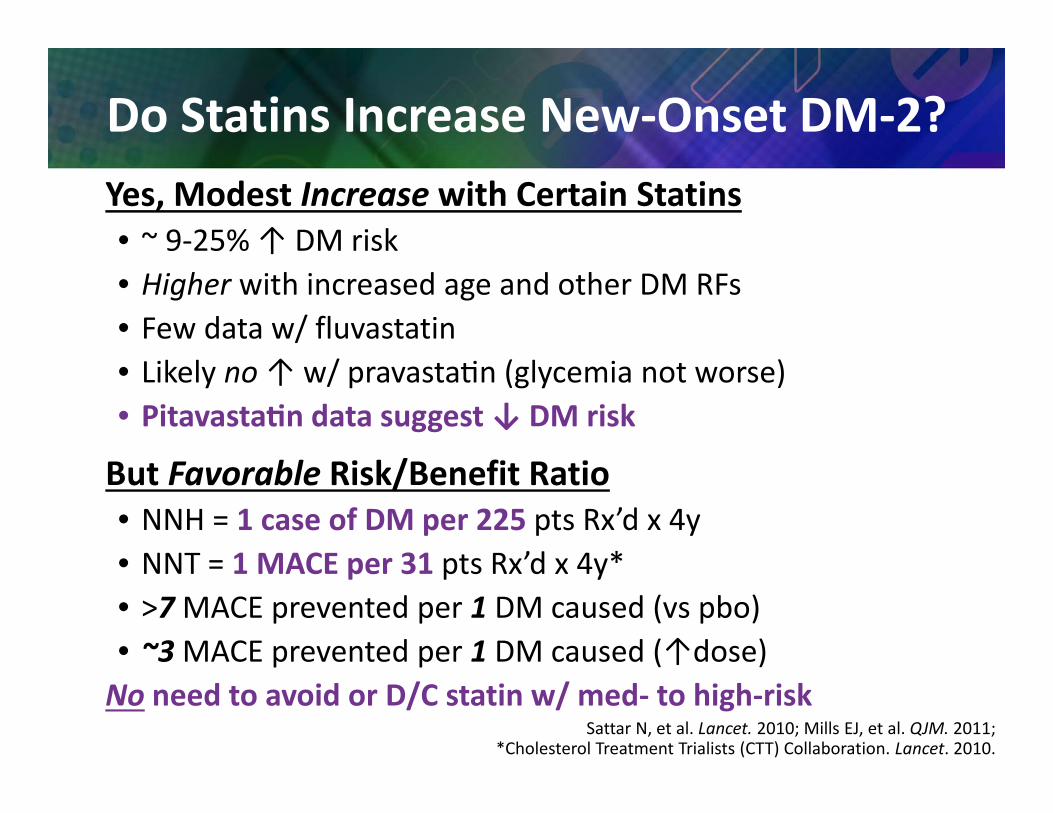
Do Statins Increase New‐Onset DM‐2?Yes, Modest Increase with Certain Statins• ~ 9‐25% ↑ DM risk• Higher with increased age and other DM RFs• Few data w/ fluvastatin• Likely no ↑ w/ pravasta n (glycemia not worse)• Pitavasta n data suggest ↓ DM risk
But Favorable Risk/Benefit Ratio• NNH = 1 case of DM per 225 pts Rx’d x 4y• NNT = 1 MACE per 31 pts Rx’d x 4y*• >7MACE prevented per 1 DM caused (vs pbo)• ~3MACE prevented per 1 DM caused (↑dose)No need to avoid or D/C statin w/ med‐ to high‐risk
Sattar N, et al. Lancet. 2010; Mills EJ, et al. QJM. 2011;*Cholesterol Treatment Trialists (CTT) Collaboration. Lancet. 2010.

Statin Phobia• Defini on: irra onal fear → unwilling to try sta n treatment• Causes:
– Negative information on internet– Distrust of big corporations/big pharma– Distrust of Western medicine, “natural” Rx wanted– Adverse experiences of family and friends
• Suggested management: – Listen to/empathize with patient– Negotiate extra diet/lifestyle effort then statin trial– “Natural” statin: red yeast rice?
• Variable potency • Potential harm from non‐statin content
– “Natural” non‐statins• Rx Omega‐3 (avoid non‐marine, check potency) • Niacin (no “flush‐free” or multi‐dose sustained‐release)
Brinton EA. 2016; unpublished.

GI‐Acting (Oral)Non‐Statins

IMPROVE‐IT: Primary Endpoint – ITT
Cannon CP, et al. N Engl J Med. 2015.
7‐year event rates
Simva 34.7%2,742 events
EZ/Simva 32.7% 2,572 events
00
10
20
30
40
1 2 3 4 5 76
Time Since Randomization (years)
Even
t Rate (%
)
Cardiovascular death, MI, documented unstable angina requiring rehospitalization, coronary revascularization (≥30 days), or stroke
Includes 42% who STOPPED study med!
↓6.4%HR 0.936
CI (0.887, 0.988)
P=.016
NNT=50

Cannon CP, et al. N Engl J Med. 2015.
7‐year event rates
Simva 34.7%2,742 events
EZ/Simva 32.7% 2,572 events
00
10
20
30
40
1 2 3 4 5 76
Time Since Randomization (years)
Even
t Rate (%
)
Cardiovascular death, MI, documented unstable angina requiring rehospitalization, coronary revascularization (≥30 days), or stroke
HR 0.936 CI (0.887, 0.988)
P=.016 NNT=50
IMPROVE‐IT: No CVD Benefit at 1 Year
No ↓ACS

Cannon CP, et al. N Engl J Med. 2015.
7‐year event rates00
10
20
30
40
1 2 3 4 5 76
Time Since Randomization (years)
Even
t Rate (%
)
Cardiovascular death, MI, documented unstable angina requiring rehospitalization, coronary revascularization (≥30 days), or stroke
HR 0.936 CI (0.887, 0.988)
P=.016 NNT=50
IMPROVE‐IT: No CVD Benefit at 1 year, But↓10% (11% OT) From 1‐7 years

IMPROVE‐IT: Major Pre‐Specified Subgroups
Overall
MaleFemale
Age <65 yearsAge ≥ 65 years
CaucasianNon‐Caucasian
No DiabetesDiabetes
SmokerNon‐Smoker
HTNNo HTN
Prior PCLNo Prior PCL
Simva† EZ/Sima†34.7 32.7
34.9 33.334.0 31.0
30.8 29.939.9 36.4
35.0 33.132.9 31.1
30.8 30.245.5 40.0
32.9 32.335.5 32.9
39.0 36.028.4 27.8
49.8 50.031.2 28.8
0.7 1.0 1.3Ezetimibe/Simva Better
Simva BetterCannon CP, et al. N Engl J Med. 2015.
*P‐interaction=.023, otherwise >.05
†7‐year event rates

IMPROVE‐IT: Major Pre‐Specified Subgroups
Overall
MaleFemale
Age <65 yearsAge ≥ 65 years
CaucasianNon‐Caucasian
No DiabetesDiabetes
SmokerNon‐Smoker
HTNNo HTN
Prior PCLNo Prior PCL
Simva† EZ/Sima†34.7 32.7
34.9 33.334.0 31.0
30.8 29.939.9 36.4
35.0 33.132.9 31.1
30.8 30.245.5 40.0
32.9 32.335.5 32.9
39.0 36.028.4 27.8
49.8 50.031.2 28.8
0.7 1.0 1.3Ezetimibe/Simva Better
Simva BetterCannon CP, et al. N Engl J Med. 2015.
*P‐interaction=.023, otherwise >.05
†7‐year event rates
~3x Benefit in DM2

Statin + Intestinally‐Acting Agent (CAI or BAS) = 2 to 3 Statin Doublings
Adapted from Bays H, et al. Expert Opin Pharmacother. 2003.
1‐STEP COADMINISTRATION
3‐STEP TITRATION
% Reduction in LDL‐C
5%‐6% 5%‐6%
Statin – starting dose 1st 2nd 3rd
5%‐6%
Statin – starting dose + CAI or BAS
15%‐18%
Dose Doublings
Statin Adjunct
0 10 20 30 40 50 60

PCSK9‐Inhibitors

PCSK9‐I Indications, Limitations Key Side Effects & Precautions
• Indications: “On diet and lifestyle and maximally tolerated statin” (and traditional non‐statin?), and “requiring additional LDL‐C lowering”, and– Prior clinical ASCVD (cor, cerebrovasc, or peripheral)—subclinical is off
label, or– Heterozygous FH (≈pre‐Rx LDL‐C >190)– Homozygous FH (≈ pre‐Rx LDL‐C >400)—evoloc. only
• Contraindication: hypersensitivity (+/‐ autoantibodies)• Most common adverse events:
– Nasopharyngitis, URI, influenza, back pain, injection site reactions (no ↑neurocogni ve but some ↑musculoskeletal)
• No immunomodulatory effects • No dose adjustment for age, sex, renal, hepatic, other meds• Limita on of use: No proof yet of ↓ASCVD
www.accessdata.fda.gov/scripts/cder/drugsatfda/; www.accessdata.fda.gov/scripts/cder/drugsatfda/.
HeFH: Pathophysiology and Dx Criteria

Physical Characteristics of FH

Familial Hypercholesterolemia: Two Degrees of Severity
Homozygous (HoFH)• Prevalence 1‐4:Million• FH in both parents• Un‐Rx’d LDL‐C >400• Childhood onset skin & tendon xanthomas & ASCVD
• Rx extremely difficult
Heterozygous (HeFH) • Prevalence ~1:200 to 1:500
• FH in one parent• Un‐Rx’d LDL‐C 200‐400• Middle‐age onset of tendon xanthomas and ASCVD
• Rx may be difficult

Relationship Between Cumulative LDL‐C Exposure and Age of ASCVD Onset
Horton J, et al. J Lipid Res. 2009.

6 Classes of LDL‐Receptor Mutations
AHA Scientific Statement on FH
Gidding SS, et al. Circulation. 2015.

6 Classes of LDL‐Receptor Mutations
AHA Scientific Statement on FH
Gidding SS, et al. Circulation. 2015.
~2/3 of FH is 2o to LDL‐R mutation, but thousands of mutations
vary in severity → huge overlap in LDL‐C: HoFH >= HeFH >= Polygenic ↑Chol

Simplified Dx Criteria for HeFH
• Baseline (un‐treated) LDL‐C >190 (>160 if <20 y/o)
• Very helpful if can find 1o relatives with:–↑LDL‐C (>190/160)– Tendon xanthomas–Premature ASCVD
Stone NJ, et al. Circulation. 2013;Onorato A, Sturm AC. Circulation. 2016.

How do mAb PCSK9‐Inhibitors Work?

PCSK9 Causes Intra‐hepatocyte Degradation of LDL‐Receptor
McKenney J. Presented at ACC 2012.

PCSK9‐Inhibitors (mAb) Prevent PCSK9‐mediated LDL‐Receptor Degradation
McKenney J. Presented at ACC 2012.

Dynamic Relationship Between mAb Levels, Free PCSK9, and LDL‐C
0 6 120
20Free
/ Total PCSK9
Con
c. (n
g/mL)
Total A
lirocum
ab(ng/mL) x 0.01
200
40
120
160
80
3 159-70
-60
LDL‐C M
ean Change (%)
0
-50
-30
-20
-40
Free PCSK9, Total Alirocumab Concentration,and LDL‐c Mean % Change vs Time
60
140
180
100
-10
Total AlirocumabFree PCSK9LDL‐C
3 6 9 12 15Weeks
Shimada YJ, Cannon CP. Eur Heart J. 2015; Stein EA, et al. N Engl J Med. 2012.

Phase 3 Data from Alirocumab and Evolocumab

PCSK9‐I mAb LDL‐C Dose‐Response
Drug Dosage % LDL‐C Lowering
Alirocumab 75 mg every 2 wks. ~40‐45%
150 mg every 2 wks. ~50‐60%
Evolocumab 140 mg every 2 wks. ~50‐65%
420 mg every 4 wks. ~50‐65%
https://www.accessdata.fda.gov/scripts/cder/drugsatfda/;https://www.accessdata.fda.gov/scripts/cder/drugsatfda/.

Alirocumab: Significant LDL‐C Reduction Across All Phase 3 Trials*
Study Population Duration(Weeks)
% LDL‐C ReductionAlirocumab Comparator
MONO Hypercholesterolemia and moderate ASCVD risk 24 47% 16% (ezetimibe)
FH I HeFH 24 49% 9% (placebo)FH II HeFH 24 49% 3% (placebo)HIGH FH HeFH 24 46% 7% (placebo)LONG TERM High ASCVD risk/HeFH 78 52% +4% increase (placebo)
ALTERNATIVEHigh ASCVD risk and history of intolerance to at least twostatins
24 45% 15% (ezetimibe)
OPTIONS I High ASCVD risk 24 44‐54%21‐23% (ezetimibe)
5% (double dose statin)21% (statin switch)
OPTIONS II High ASCVD risk 24 36‐51% 11‐14% (ezetimibe)16% (double statin dose)
COMBO I High ASCVD risk 24 48% 2% (placebo)COMBO II High ASCVD risk 24 51% 21% (ezetimibe)
Shapiro MD, et al. Curr Atheroscler Rep. 2015; Robinson JG, et al. N Engl J Med. 2015.
*P value <.0001 for all trials except OPTIONS I (P=.01) and OPTIONS II (P=.0125).
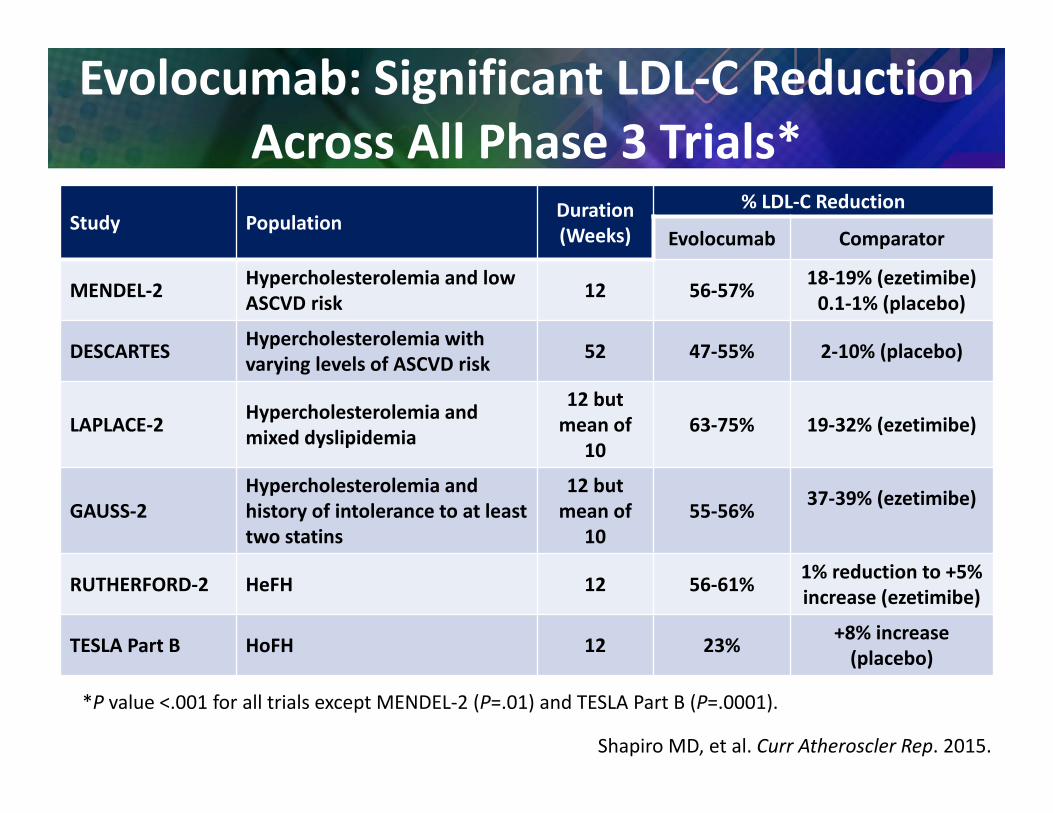
Evolocumab: Significant LDL‐C Reduction Across All Phase 3 Trials*
Study Population Duration(Weeks)
% LDL‐C Reduction
Evolocumab Comparator
MENDEL‐2 Hypercholesterolemia and low ASCVD risk 12 56‐57% 18‐19% (ezetimibe)
0.1‐1% (placebo)
DESCARTES Hypercholesterolemia with varying levels of ASCVD risk 52 47‐55% 2‐10% (placebo)
LAPLACE‐2 Hypercholesterolemia and mixed dyslipidemia
12 but mean of
1063‐75% 19‐32% (ezetimibe)
GAUSS‐2Hypercholesterolemia and history of intolerance to at least two statins
12 but mean of
1055‐56% 37‐39% (ezetimibe)
RUTHERFORD‐2 HeFH 12 56‐61% 1% reduction to +5% increase (ezetimibe)
TESLA Part B HoFH 12 23% +8% increase (placebo)
*P value <.001 for all trials except MENDEL‐2 (P=.01) and TESLA Part B (P=.0001).
Shapiro MD, et al. Curr Atheroscler Rep. 2015.

PCSK9‐I Maintain Consistent LDL‐C Reductions over 1 Year
39
53
67
81
95
109
123
137
151
1
1.5
2
2.5
3
3.5
4
0 4 8 12 16 20 24 28 32 36 40 44 48 52Week
3.1 mmol/L118.9 mg/dL
1.3 mmol/L48.3 mg/dL
3.2 mmol/L123.0 mg/dL
1.4 mmol/L53.1 mg/dL
mg/dL
PlaceboAlirocumab
LDL‐C, LS mean mmol/L
LDL‐C Levels to 52 Weeks on Alirocumab 150 mg q 2 wksAll patients on background of maximally‐tolerated statin ±other lipid‐lowering therapy
Intent‐to‐treat (ITT) analysis Robinson JG, et al. N Engl J Med. 2015.

Sabatine MS, et al. N Eng J Med. 2015.
PCSK9‐I Maintain Consistent LDL‐C Reductions over 1 Year
LDL‐C Levels to 48 Weeks on Evolocumab 140 mg q 2 wks (or 420 mg q 4 wks)Most patients on background of maximally‐tolerated statin ±other

Treatment‐Emergent Adverse EventsMedian 48 weeks treatment with evolocumab
Sabatine MS, et al. N Eng J Med. 2015.
Adverse Events % (N) Evolocumab(N=2976)
Standard Therapy(N=1489)
Any AE 69.2% (2060) 64.8 (965)
Serious AE 7.5% (222) 7.5% (111)
AE leading to treatment discontinuation 2.4% (71) NA
Muscle Related AE 6.4% (190) 6% (90)
Injection‐site reaction 4.3% (129) NA
Neurocognitive event 0.9% (27) 0.3% (4)
Other AEs
Arthralgia 4.6% (137) 3.2% (48)
Headache 3.6% (106 2.1% (32)
Limb pain 3.3% (99) 2.1% (32)
Fatigue 2.8% (83) 1% (15)
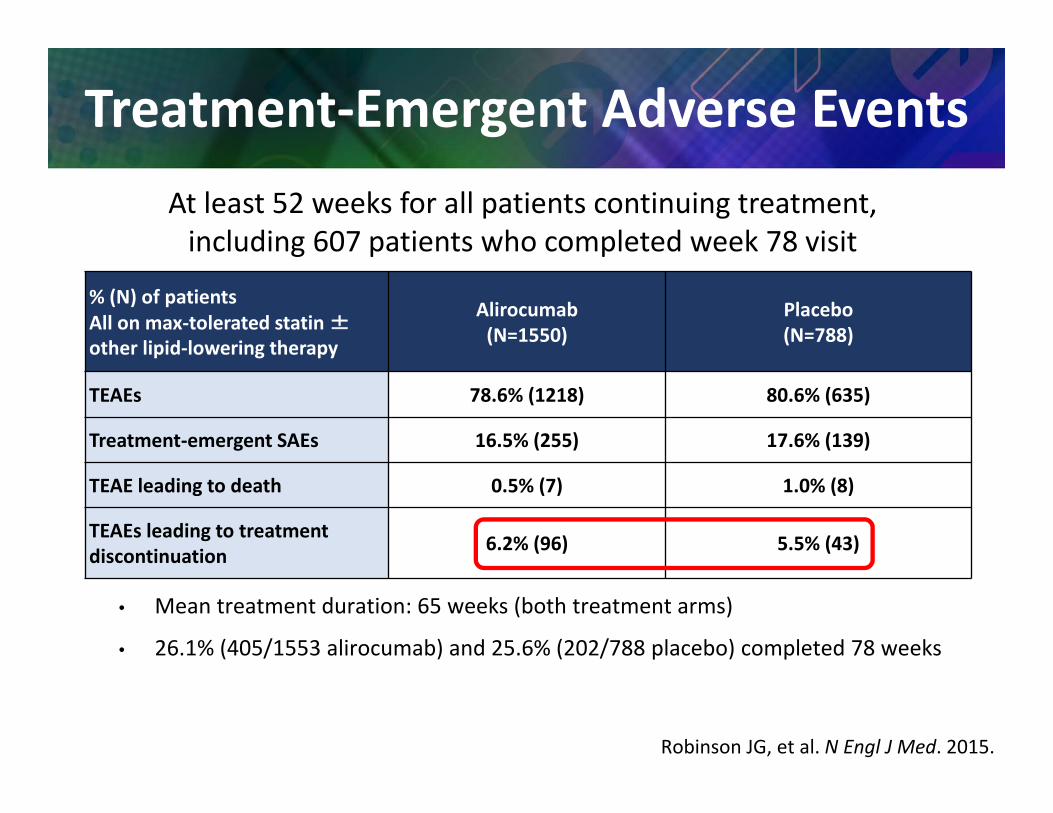
Treatment‐Emergent Adverse Events
% (N) of patientsAll on max‐tolerated statin ±other lipid‐lowering therapy
Alirocumab(N=1550)
Placebo(N=788)
TEAEs 78.6% (1218) 80.6% (635)
Treatment‐emergent SAEs 16.5% (255) 17.6% (139)
TEAE leading to death 0.5% (7) 1.0% (8)
TEAEs leading to treatment discontinuation 6.2% (96) 5.5% (43)
• Mean treatment duration: 65 weeks (both treatment arms)
• 26.1% (405/1553 alirocumab) and 25.6% (202/788 placebo) completed 78 weeks
Robinson JG, et al. N Engl J Med. 2015.
At least 52 weeks for all patients continuing treatment, including 607 patients who completed week 78 visit

Event Odds Ratio (95% CI)
All‐cause Mortality 0.45 (0.23‐0.86)
CVD Mortality 0.50 (0.23‐1.10)
MI 0.49 (0.26‐0.93)
Unstable Angina 0.61 (0.06‐6.14)
CK 0.72 (0.54‐0.96)
Serious AE 1.01 (0.87‐1.18)
Pooled PCSK9 Safety & Efficacy
Navarese EP, et al. Ann Intern Med. 2015.
(Alirocumab, Bococizumab, and Evolocumab; N=10,159)

Evolocumab Decreases Coronary Atheromas(IVUS data from GLAGOV)
Evolocumab 420 mg q 4 weeks x 76 weeks; LDL‐C 37 vs 93; 20% ↓ASCVD events; Nicholls SJ. JAMA 2016 epub 15 Nov.

Evolocumab Decreases Coronary Atheromas(IVUS data from GLAGOV)
Evolocumab 420 mg q 4 weeks x 76 weeks; LDL‐C 37 vs 93; 20% ↓ASCVD events; Nicholls SJ. JAMA 2016 epub 15 Nov.
Evolocumab
Placebo

Fewer Skeletal Muscle AEs with Alirocumab than with Atorvastatin or Ezetimibe
0.50
0.45
0.40
0.35
0.30
0.25
0.20
0.15
0.10
0.05
0.00Cum
ulat
ive
prob
abili
ty o
f eve
nt
Week
Atorvastatin
Alirocumab
0 4 8 12 16 20 24 28 32 36
Kaplan-Meier estimates for time to first skeletal muscle event
Cox model analysis:HR ALI vs ATV = 0.61 (95% CI: 0.38 to 0.99), nominal P=.042
Ezetimibe
HR ALI vs EZE = 0.71 (95% CI: 0.47 to 1.06), nominal P=.096
Moriarty PM, et al. J Clin Lipidol. 2015.

PCSK9: Roles Beyond LDL‐Receptor Degradation
PCSK9 promotes receptor degradation:• LDL receptor• VLDL receptor• Apo E receptor• CD81 receptor (binds hepatitis C virus)• CD36 (multi‐ligand scavenger receptor):
– FFA – Modified lipoproteins– Various pathogens– Amyloidogenic peptides
Moore KJ, Goldberg IJ. Arterioscler Thromb Vasc Biol. 2016.
Bottom line: PCSK9‐I may be anti‐athero beyond LDL‐C

Evolution of mAb Therapies
Catapano AL , Papadopoulos N. Atherosclerosis. 2013.
Immun
ogen
icity
Fully Mouse1st generation
Chimeric2nd generation
Humanized3rd generation
“Fully” Human4th generation
Highly Immunogenic
Still immunogenic
Less immunogenic
Least immunogenic
~30% mouse
5%–10% mouse
100% human
100% mouse Mouse variableMouse constantHuman variableHuman constant
AlirocumabEvolocumab
Bococuzumab

Advent of PCSK9‐I Requires Return to On‐Rx LDL‐C (albeit Thresholds > Goals)
• Question: WHO requires addi onal ↓LDL‐C?• NLA PCSK9‐I Rx thresholds = goal + 30; so 2oprev. threshold >100, HR 1o prev. thrsh. >130
• ACC statement reinstates thresholds• PCSK9‐I class allows us to overshoot LDL‐C goals in most cases– How low is too low? (likely no such thing)– LDL‐C <40 mg/dL provides lowest CVD risk– LDL‐C <25 mg/dL appears safe– Should we back‐titrate statins? (likely not)
Shrank WH, et al. JAMA. 2015.

2016 ACC Statement on Lipid Rx Thresholds for Non‐statins
Stable ASCVD
Comorbid‐ities1
Base LDL‐C
2First look for LDL‐C↓< 50%
2May consider if LDL‐C
2May consider if non‐HDL‐C
+ + NA + >70 >100
+ ‐ NA + >100 NA+ ‐ >190 + >70 NA‐ ‐ >190 + >100 NA
‐ ‐3 70‐189 + >100 >130
‐ ‐4 70‐189 + >100 >130
1. Comorbidities = DM1, DM2, acute ASCVD < 3mos ago, ASCVD event while on statin, baseline LDL‐C > 190, poorly controlled major ASCVD RF, ↑Lp(a), CKD.
2. 1st round: address statin non‐adherence, intensify lifestyle, consider phytosterols, ↑to high‐intensity statin, consider Lipidologist referral if statin intolerant or HoFH, control other RFs. 2nd round:consider non‐statin (ezet, BAS, PCSK9‐I)
3. DM1 or DM2 present: 1st & 2nd rounds as #2 above except no PCSK9‐I4. 10‐y ASCVD Risk >7.5% and age 40‐75; iterative adjustments, see #3.
Lloyd‐Jones DM, et al. J Am Coll Cardiol. 2016.

Stable ASCVD
Comorbid‐ities1
Base LDL‐C
2First look for LDL‐C↓< 50%
2May consider if LDL‐C
2May consider if non‐HDL‐C
+ + NA + >70 >100
+ ‐ NA + >100 NA+ ‐ >190 + >70 NA‐ ‐ >190 + >100 NA
‐ ‐3 70‐189 + >100 >130
‐ ‐4 70‐189 + >100 >1301. Comorbidities = DM1, DM2, acute ASCVD < 3mos ago, ASCVD event while on statin, baseline LDL‐C >
190, poorly controlled major ASCVD RF, ↑Lp(a), CKD.2. 1st round: address statin non‐adherence, intensify lifestyle, consider phytosterols, ↑to high‐intensity
statin, consider Lipidologist referral if statin intolerant or HoFH, control other RFs. 2nd round:consider non‐statin (ezet, BAS, PCSK9‐I)
3. DM1 or DM2 present: 1st & 2nd rounds as #2 above except no PCSK9‐I4. 10‐y ASCVD Risk >7.5% and age 40‐75; iterative adjustments, see #3.
2016 ACC Statement on Lipid Rx Thresholds for Non‐statins
Lloyd‐Jones DM, et al. J Am Coll Cardiol. 2016.

2016 ACC Statement on Lipid Rx Thresholds for Non‐statins
Stable ASCVD
Comorbid‐ities1
Base LDL‐C
2First look for LDL‐C↓< 50%
2May consider if LDL‐C
2May consider if non‐HDL‐C
+ + NA + >70 >100
+ ‐ NA + >100 NA+ ‐ >190 + >70 NA‐ ‐ >190 + >100 NA
‐ ‐3 70‐189 + >100 >130
‐ ‐4 70‐189 + >100 >130
1. Comorbidities = DM1, DM2, acute ASCVD < 3mos ago, ASCVD event while on statin, baseline LDL‐C > 190, poorly controlled major ASCVD RF, ↑Lp(a), CKD.
2. 1st round: address statin non‐adherence, intensify lifestyle, consider phytosterols, ↑to high‐intensity statin, consider Lipidologist referral if statin intolerant or HoFH, control other RFs. 2nd round: consider non‐statin (ezet, BAS, PCSK9‐I)
3. DM1 or DM2 present: 1st & 2nd rounds as #2 above except no PCSK9‐I4. 10‐y ASCVD Risk >7.5% and age 40‐75; iterative adjustments, see #3.
NB: ACC Thresholds ≈ consensus goals, but NLA thresholds (for PCSK9‐I) = goals + 30
Lloyd‐Jones DM, et al. J Am Coll Cardiol. 2016.

On‐Rx LDL‐C Predicts ↓CVD
N=312,175 (25% women) in 49 trials, 39,645 MVE, base LDL‐C 122 mg/dL. Silverman MG, et al. JAMA. 2016.

Can LDL‐C be Too Low?• Abetalipoproteinemia & homozygous hypobetalipoproteinemia (LDL‐C 0‐25 mg/dL)– Autosomal recessive LoF MTP or apo B gene mutations– V. Low/absent apo B‐cont. lipos (chylos, VLDL, LDL)– Neurological/ophthalm sequelae Rx w/ fat‐soluble vits/EFFA– Malabsorption Sx reduced by low fat diet + MCT oil– Hepa c steatosis and ↑AST/ALT (no hep. fibrosis)– ↓↓↓ASCVD
• Heterozygous PCSK9 LoF (LDL‐C ~60‐100)—N=100s– Low PCSK9– ↓↓ASCVD– Normal neurological and reproductive function
• Homozygous PCSK9 LoF (LDL‐C 10‐20)—N=3– Absent PCSK9– Normal neurological and reproductive function
Lee J, Hegele RA. J Inherit Metab Dis. 2014; Cohen JC, et al. N Engl J Med. 2006.

TEAEs of Interest in Patients with 2 Consecutive LDL‐C < 25mg/dL
Safety Analysis (at least 52 weeks for all patients continuing treatment, including 607 patients who completed W78 visit)
% of Patients (All on maximally tolerated statin ± other lipid‐lowering therapy)
Alirocumab Total
(N=1550)
Alirocumab with 2 consecutive
LDL‐C <25mg/dL(N=575)
Placebo(N=788)
Summary of AE – no. of patients (%)
Any adverse event 1255 (81.0) 435 (75.7) 650 (82.5)
Serious adverse event 290 (18.7) 98 (17.0) 154 (19.5)
Adverse event leading to death 8 (0.5) 4 (0.7) 10 (1.3)
Adverse event leading to study drug discontinuation 111 (7.2) 26 (4.5) 46 (5.8)
Adapted from Robinson JG, et al. N Engl J Med. 2015.

PCSK9 Safety w/ LDL‐C <25 mg/dL
• No increase in:– Total mortality– Cancer– Myopathy– Cognitive symptoms– Metabolic/reproductive disorders– Skin disorders
Most AEs↓(!) →↑compliance/healthy‐user?
Robinson JG, et al. N Engl J Med. 2015.
(N=575 of 1550)
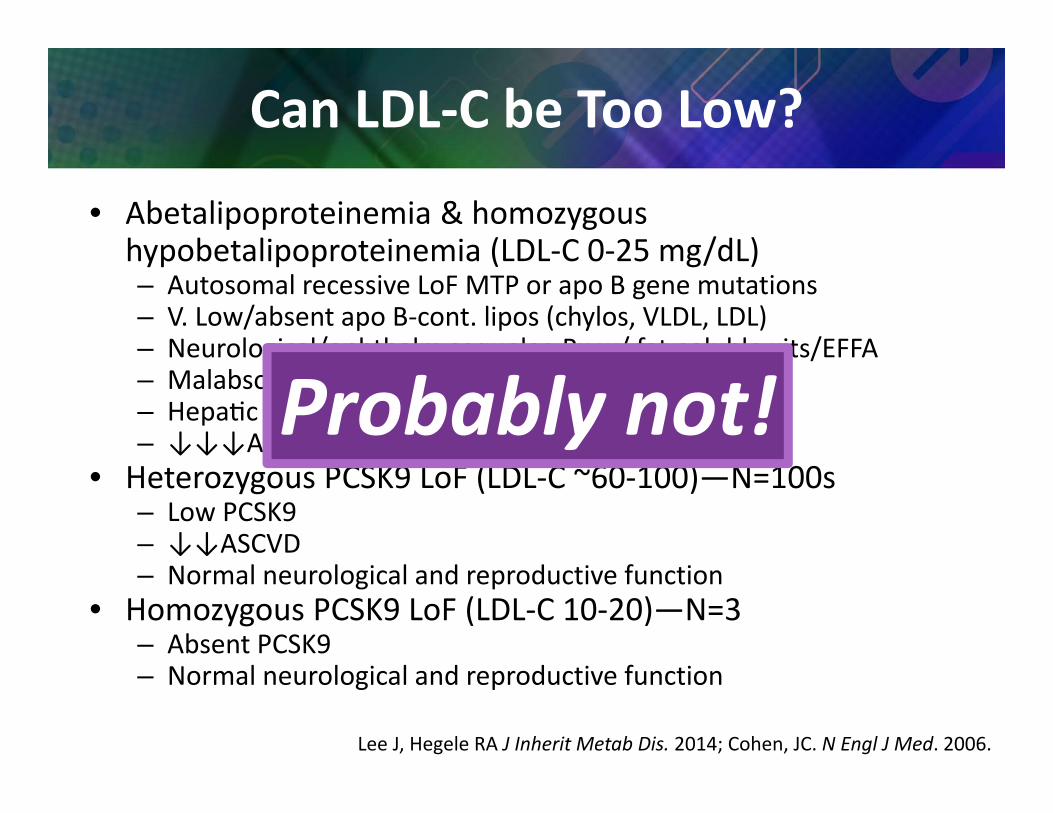
Can LDL‐C be Too Low?
• Abetalipoproteinemia & homozygous hypobetalipoproteinemia (LDL‐C 0‐25 mg/dL)– Autosomal recessive LoF MTP or apo B gene mutations– V. Low/absent apo B‐cont. lipos (chylos, VLDL, LDL)– Neurological/ophthalm sequelae Rx w/ fat‐soluble vits/EFFA– Malabsorption Sx reduced by low fat diet + MCT oil– Hepa c steatosis and ↑AST/ALT (no hep. fibrosis)– ↓↓↓ASCVD
• Heterozygous PCSK9 LoF (LDL‐C ~60‐100)—N=100s– Low PCSK9– ↓↓ASCVD– Normal neurological and reproductive function
• Homozygous PCSK9 LoF (LDL‐C 10‐20)—N=3– Absent PCSK9– Normal neurological and reproductive function
Lee J, Hegele RA J Inherit Metab Dis. 2014; Cohen, JC. N Engl J Med. 2006.
Probably not!

Gene Scores for PCSK9 & HMGCR, Similar ↓CHD & ↑DM2
Ference BA. NEJM 2016;375;2144‐53.

When?*• Rx beyond statin & ezet. (BAS, NA, PCSK9‐I, LDL apheresis,
lomitapide, mipomersen) – Severe hypercholesterolemia: LDL‐C >160‐200 depending on age, ASCVD risk, and Rx response
– ASCVD bad/progressive (adv. testing & Rx)– Statin intolerant/phobic
To Whom?• ABCL‐certified physician—see lipidboard.org• Other lipid experts—NLA members (lipid.org), FH foundation,
Lp(a) foundation, etc. • Become a lipidologist—(by choice, not by training, as noted
above)
Referral to a Lipidologist
*Also consider Lipidology referral for: • Severe HTG (> ~500, or if 200‐500 + ↑ ASCVD risk/history)• High Lp(a)

Summary: LDL Rx for Atheroprevention
• LDL and other Non‐HDL (atherogenic) lipoproteins drive atherogenesis• Chest CT for CAC is a good measure of athero in 1o prev. (best in ~45‐75
y/o), $70‐$300• 2013 ACC/AHA guidelines are good for
– Statin benefit groups and – High‐intensity statin use– Easy definition of HeFH (un‐Rx LDL‐C>190), but
• LDL‐C/Non‐HDL‐C goals/thresholds are needed• Statin adjuncts/alternatives are useful:
– Ezetimibe (to get LDL/Non‐HDL < goal)– Other for LDL/Non‐HDL (BAS, NA)– Other for HTG/↓HDL‐C– PCSK9‐I mAb (get LDL/Non‐HDL << goal)—game‐changer
• Refer severe/difficult pts to a lipidologist