ccr5 antagonists and tropism testing in clinical practice this activity is supported by educational...
TRANSCRIPT
CCR5 Antagonists and Tropism Testing inClinical Practice
This activity is supported by educational grants from
Faculty: W. David Hardy, M.D.Director, Division of Infectious Diseases Cedars-Sinai Medical Center; Los Angeles, California
W. David Hardy, M.D.
Copyright © 2008 Body Health Resources Corporation. All rights reserved.
The Body PRO Presents:
This activity is jointly sponsored by Postgraduate Institute for Medicine and The Body PRO.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
2
Faculty for This ActivityFaculty for This Activity
W. David Hardy, M.D.
W. David Hardy, M.D., is an associate professor of medicine-in-residence at the David Geffen School of Medicine, University of California, Los Angeles (UCLA). He gained his medical degree from the Baylor College of Medicine in Houston, Texas, in 1981, completed a residency in internal medicine at Harbor-UCLA Medical Center in Torrance, California in 1984 and a clinical fellowship in infectious diseases and immunology in 1986 at UCLA School of Medicine. Later in his career he also completed a postdoctoral fellowship in basic retrovirology in 2002, also at the UCLA School of Medicine.
Dr. Hardy has conducted clinical trials with several antiretroviral agents beginning in 1986. He is a member of numerous professional societies including the American Academy of HIV Medicine, for whom he serves as a member of the National Board of Directors and Chairman of the California/Hawaii Chapter.
Disclosures
Dr. Hardy has received grants or research support from Boehringer Ingelheim, Gilead Sciences, GlaxoSmithKline, Pfizer and Tibotec. He has served as a consultant for Boehringer Ingelheim, Bristol-Myers Squibb, GlaxoSmithKline, Merck, Monogram, Pfizer and Tibotec. He has received fees for non-CME services from Gilead Sciences, Pfizer and Tibotec. He owns stock in Merck.
The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
3
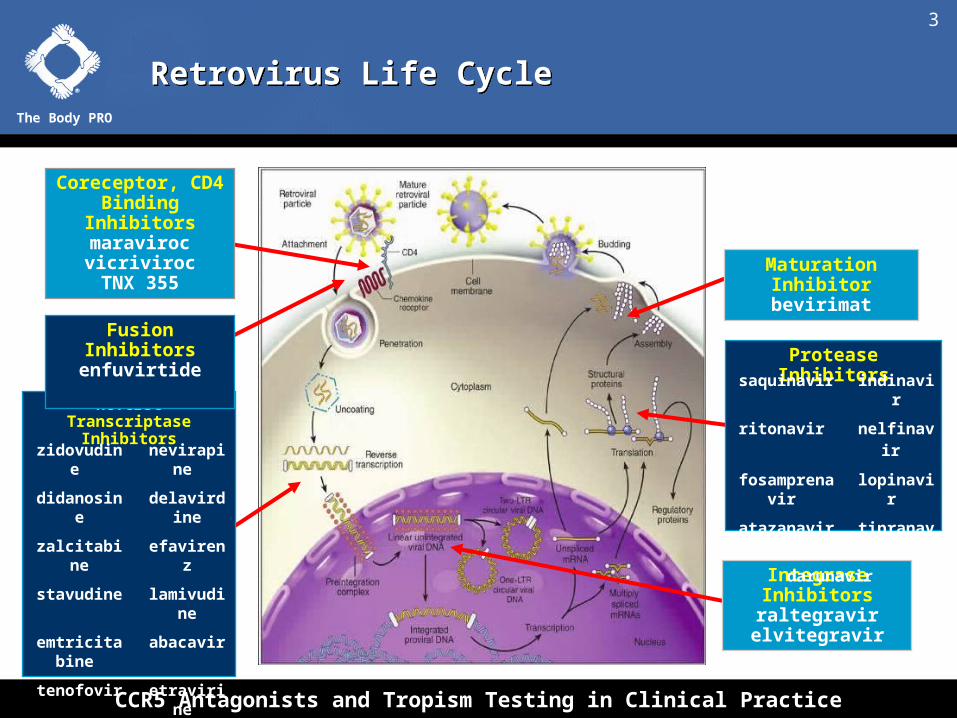
Retrovirus Life CycleRetrovirus Life Cycle
Coreceptor, CD4 Binding Inhibitors
maravirocvicrivirocTNX 355
Reverse Transcriptase Inhibitors
Protease Inhibitors
Maturation Inhibitorbevirimat
Integrase Inhibitorsraltegravirelvitegravir
Fusion Inhibitorsenfuvirtide
zidovudine nevirapine
didanosine delavirdine
zalcitabine efavirenz
stavudine lamivudine
emtricitabine abacavir
tenofovir etravirine
rilpivirine
saquinavir indinavir
ritonavir nelfinavir
fosamprenavir lopinavir
atazanavir tipranavir
darunavir

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
4
HIV Entry InhibitorsHIV Entry Inhibitors
Adapted from Moore JP, PNAS 2003;100:10598-10602.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
5
Targets Involved in HIV EntryTargets Involved in HIV Entry
Copyright © 2002-2008 Pfizer Inc. All rights reserved. Reprinted with permission.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
6
Structure of the HIV-1 Envelope GlycoproteinStructure of the HIV-1 Envelope Glycoprotein
Copyright © 2002-2008 Pfizer Inc. All rights reserved. Reprinted with permission.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
7
Binding of the gp120 Subunit to CD4Binding of the gp120 Subunit to CD4
Copyright © 2002-2008 Pfizer Inc. All rights reserved. Reprinted with permission.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
8
Conformational ChangeConformational Change
Copyright © 2002-2008 Pfizer Inc. All rights reserved. Reprinted with permission.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
9
gp120 Binds to the Coreceptor, CCR5gp120 Binds to the Coreceptor, CCR5
Copyright © 2002-2008 Pfizer Inc. All rights reserved. Reprinted with permission.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
10
Conformational Changes in the gp41 SubunitConformational Changes in the gp41 Subunit
Copyright © 2002-2008 Pfizer Inc. All rights reserved. Reprinted with permission.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
11
Fusion of the Viral and Cell MembranesFusion of the Viral and Cell Membranes
Copyright © 2002-2008 Pfizer Inc. All rights reserved. Reprinted with permission.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
12
HIV Natural History and Tropism Expression

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
13
CCR5 Function and GeneticsCCR5 Function and Genetics
• CCR5 is a receptor for C-C chemokines (chemo-attractive cytokines)
– Expressed on immune effector cells and antigen presenting cells
– Molecules that bind to CCR5 include MIP-1, MIP-1, and RANTES
• Activation of CCR5 on T cells by chemokines leads to:
– T-cell migration to the site of inflammation
– Immune response to various antigens
• CCR5, together with CD4, are the primary receptors utilized by HIV for viral entry
Galvani AP et al. Proc Natl Acad Sci U S A. 2003;100:15276-15279. McNicholl JM et al. Emerg Infect Dis. 1997;3:261-271.Stephens JC et al. Am J Hum Genet. 1998;62:1507-1515.
The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
14
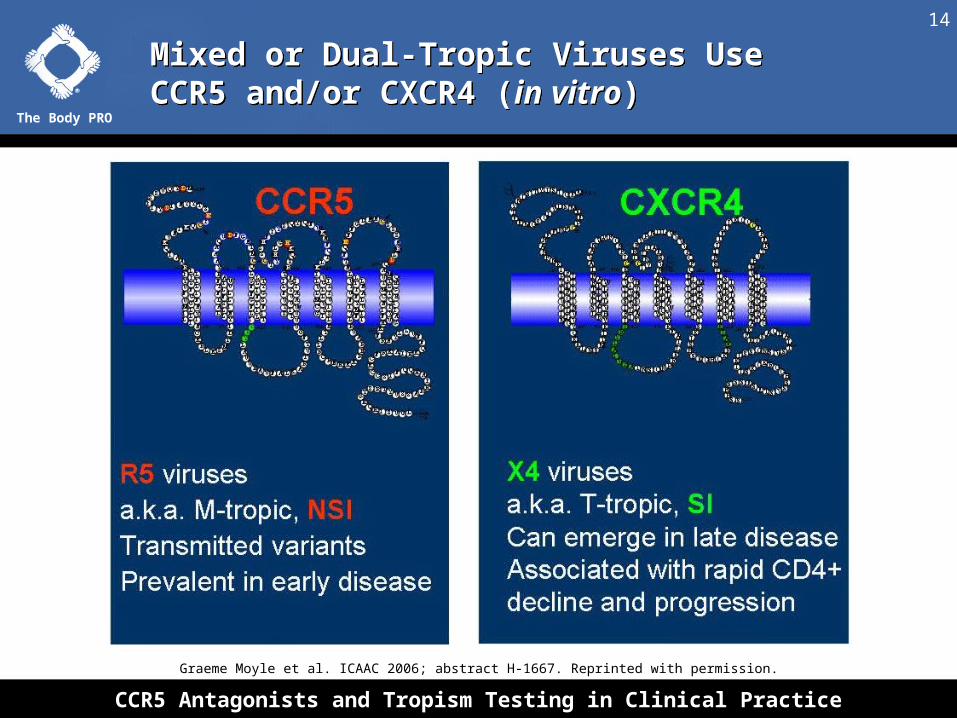
Mixed or Dual-Tropic Viruses Use CCR5 and/or CXCR4 (in vitro)Mixed or Dual-Tropic Viruses Use CCR5 and/or CXCR4 (in vitro)
Graeme Moyle et al. ICAAC 2006; abstract H-1667. Reprinted with permission.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
15
Coreceptor Usage of HIV-1 VariantsCoreceptor Usage of HIV-1 Variants
X4 R5
CXCR4 CCR5
CD4
T-cell lines Primary lymphocytes Monocyte/macrophages
CD4 Naive CD4 memory
CD4
Copyright © 2002-2008 Pfizer Inc. All rights reserved.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
16
Global Prevalence of CCR5 32 AlleleGlobal Prevalence of CCR5 32 Allele
Galvani AP et al. PNAS. 2003;100:15276-15279. McNicholl JM et al. Emerg Infect Dis. 1997;3:261-271.Stephens JC et al. Am J Hum Genet. 1998;62:1507-1515.
~14%
~6%Rare
10%-15%
Rare
Rare
~10%
~10%
Rare
• 5%-14% of Caucasians of European descent carry CCR5 32 (1% are CCR5 32 homozygous)
• The origin of the CCR5 D32 allele has been traced to European geography ~1,000 years ago
Possible selection by pandemic pathogen, likely smallpox or bubonic plague
The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
17
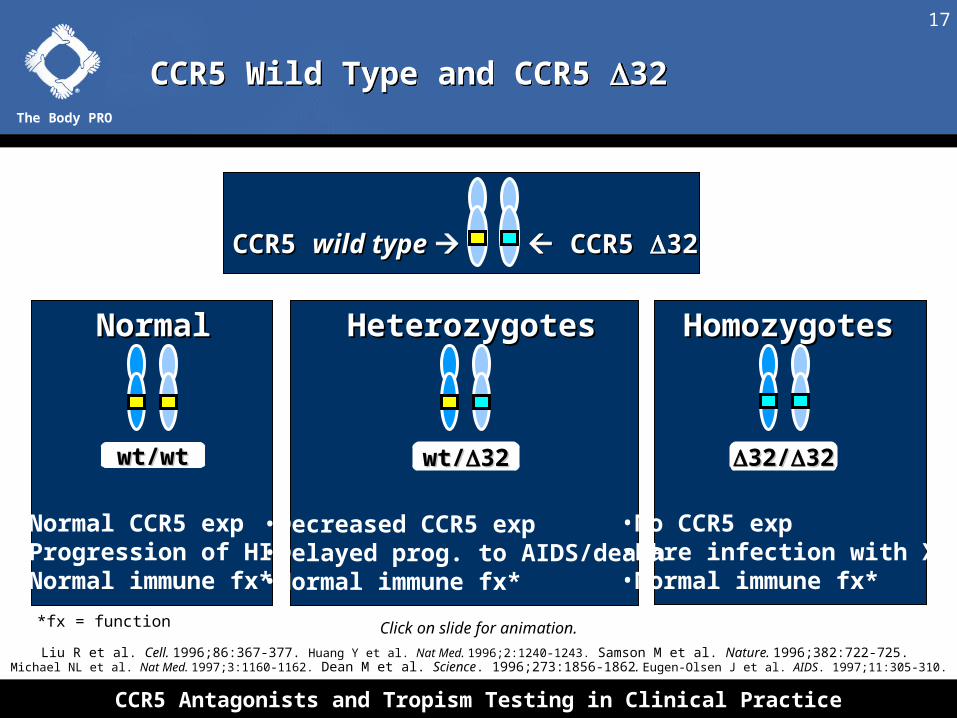
CCR5 Wild Type and CCR5 32CCR5 Wild Type and CCR5 32
CCR5 CCR5 wild type wild type CCR5 CCR5 32 32
wt/wtwt/wt wt/wt/3232 3232//3232
NormalNormal HeterozygotesHeterozygotes HomozygotesHomozygotes
Click on slide for animation.
Liu R et al. Cell. 1996;86:367-377. Huang Y et al. Nat Med. 1996;2:1240-1243. Samson M et al. Nature. 1996;382:722-725. Michael NL et al. Nat Med. 1997;3:1160-1162. Dean M et al. Science. 1996;273:1856-1862. Eugen-Olsen J et al. AIDS. 1997;11:305-310.
• Normal CCR5 exp• Progression of HIV• Normal immune fx*
• Decreased CCR5 exp• Delayed prog. to AIDS/death• Normal immune fx*
• No CCR5 exp• Rare infection with X4 • Normal immune fx*
*fx = function

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
18
Patients Heterozygous for CCR5 32 Have Slower Progression to AIDS and DeathPatients Heterozygous for CCR5 32 Have Slower Progression to AIDS and Death
Adapted from de Roda Husman A-M, et al. Ann Intern Med. 1997;127:882-890.
The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
19
The Tropism Assay

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
20
Why is a Tropism Test Required?Why is a Tropism Test Required?
• CCR5 antagonists block entry of HIV that uses CCR5 only, no effect on HIV that uses CXCR4
• Presence of X4 HIV has been associated with more rapid CD4 decline and disease progression
• The effect a CCR5 antagonist will have in patients with R5/X4 HIV is unknown
• Regulatory agencies likely to require tropism assay prior to use of a CCR5 antagonist
Copyright © 2002-2008 Pfizer Inc. All rights reserved. Reprinted with permission.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
21
The Monogram Tropism AssayThe Monogram Tropism Assay
HIV-1 Expression Vector (pHIVlucU3)
Envelope Expression Vector (pHIVenv)
P A+
HIV envelope
a/b c/d
Indicator Gene
U5
gag
pol
Luciferase
P R env
P
R A+
gp120 gp41
Copyright © Monogram Biosciences. Reprinted with permission.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
22
HIV Entry Cell AssayHIV Entry Cell Assay
Adapted from Petropoulos CJ et al. Antimicrob Agents Chemother. 2000;44:920-928.
The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
23
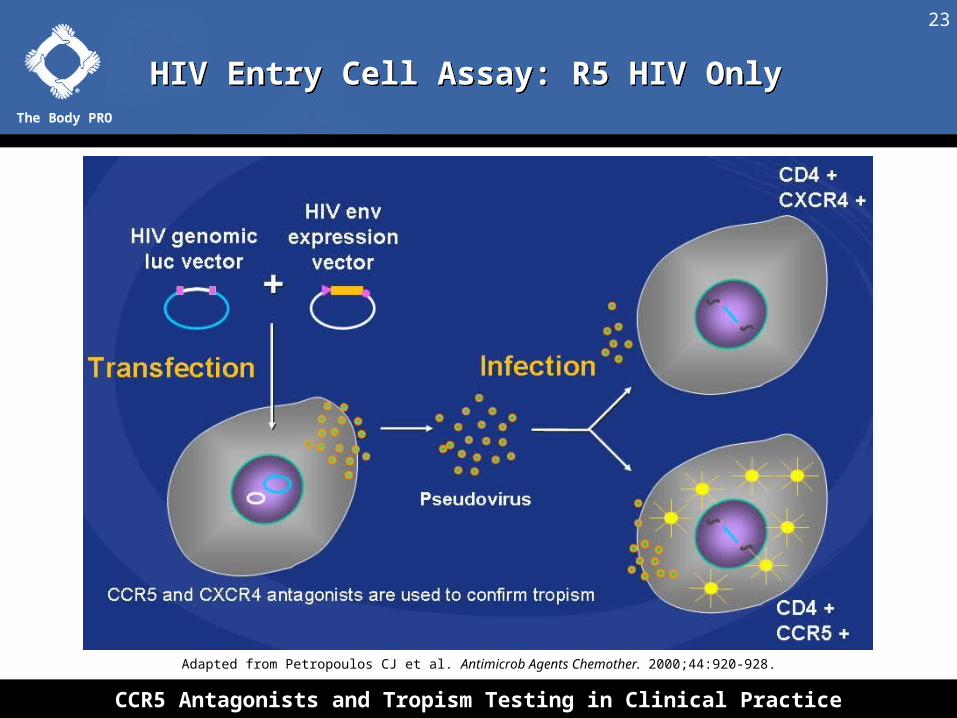
HIV Entry Cell Assay: R5 HIV OnlyHIV Entry Cell Assay: R5 HIV Only
Adapted from Petropoulos CJ et al. Antimicrob Agents Chemother. 2000;44:920-928.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
24
HIV Entry Cell Assay: X4 HIV OnlyHIV Entry Cell Assay: X4 HIV Only
Adapted from Petropoulos CJ et al. Antimicrob Agents Chemother. 2000;44:920-928.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
25
HIV Entry Cell Assay: R5/X4 Tropic HIVHIV Entry Cell Assay: R5/X4 Tropic HIV
Adapted from Petropoulos CJ et al. Antimicrob Agents Chemother. 2000;44:920-928.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
26
Demonstration of R5 VirusDemonstration of R5 Virus
Light Generated CCR5 UseR5 Virus
No Light GeneratedNo CXCR4 UseNot an X4 VirusVirus
Virus
Virus
Click on slide for animation.
Copyright © Monogram Biosciences. Reprinted with permission.
CCR5 CXCR4

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
27
Demonstration of Dual VirusDemonstration of Dual Virus
Light is generated on both CCR5 and CXCR4 cell lines.
This is a DUAL virus.
Virus
Virus Virus
Virus
CCR5 CXCR4
Click on slide for animation.
Copyright © Monogram Biosciences. Reprinted with permission.
The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
28
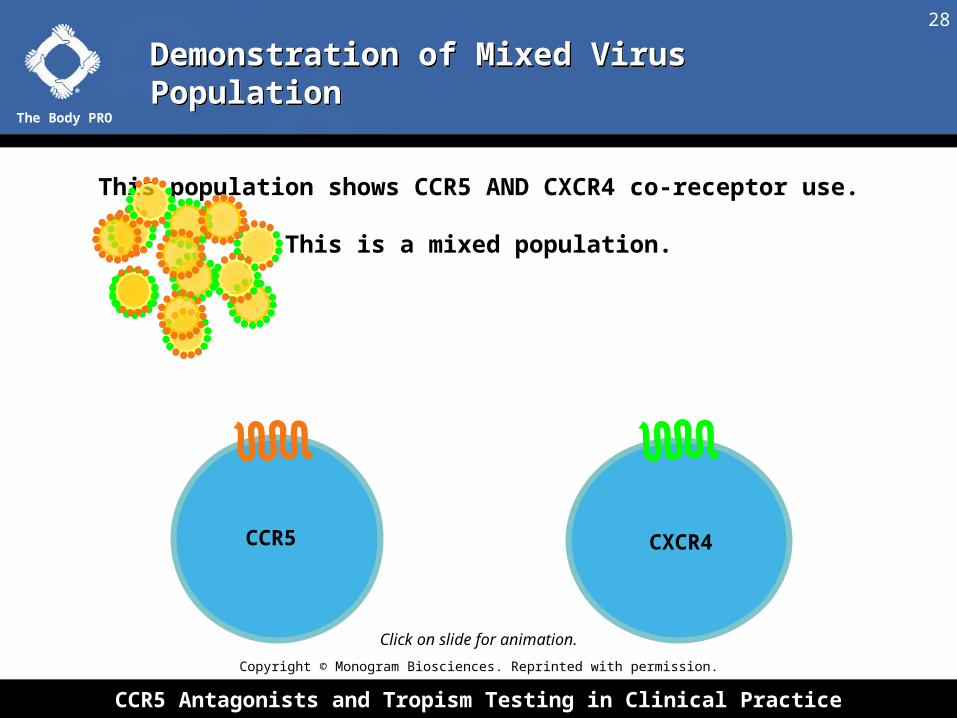
This population shows CCR5 AND CXCR4 co-receptor use.
This is a mixed population.
Demonstration of Mixed Virus PopulationDemonstration of Mixed Virus Population
CCR5 CXCR4
Click on slide for animation.
Copyright © Monogram Biosciences. Reprinted with permission.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
29
What Is This Population?What Is This Population?
Most of these viruses are R5: Strong luciferase activity
Some are X4: Lower level luciferase activity
CXCR4CCR5
Click on slide for animation.
Copyright © Monogram Biosciences. Reprinted with permission.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
30
Comparison of Original Tropism to Enhanced Sensitivity Tropism TestComparison of Original Tropism to Enhanced Sensitivity Tropism Test
Standard Tropism Assay
(August 2007 – June 2008)
Enhanced Tropism Assay(June 2008 – Present)
Sensitivity
• 100% if X4-using HIV > 10% of viral population
• 83% if X4-using HIV > 5% of viral population
• 100% if X4-using HIV > 0.3% of viral population
Plasma Volume Required 3 mL 3 mL
Shipping Requirement Dry ice Dry ice
Viral Load Requirement > 1,000 copies/mL > 1,000 copies/mL
Turnaround Time ~ 2 weeks ~ 2 weeks
Copyright © Monogram Biosciences. Reprinted with permission.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
31
Coreceptor Tropism: Epidemiological Data

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
32
Percentage of HIV Coreceptor UsagePercentage of HIV Coreceptor Usage
Study/Source Population N R5 X4 R5/X4
Homer cohort1 Naive 979 82% < 1% 18%
C & W cohort2 Naive 402 81% < 1% 19%
Demarest3 Naive 299 88% 0% 12%
Study 10264 Naïve 1428 85% < 1% 15%
TORO 1/26 Experienced 612 62% 4% 34%
ViroLogic5 Experienced > 2000 48% 2% 50%
ACTG 52117 Experienced 391 49% 4% 47%
MOTIVATE 1/28 Experienced 2560 56% 3% 41%
1Brumme ZL et al. J Infect Dis. 2005;192:466-474. 2Moyle GJ et al. J Infect Dis. 2005;191:866-872. 3Demarest J et al. ICAAC 2004; abstract H-1136. 4Waters L et al. ICAAC 2006; abstract H-1667.
5Whitcomb JM et al. CROI 2003; abstract 557. 6Paxinos EE et al. ICAAC 2002; abstract 2040.7Wilkin T et al. CROI 2006; abstract 655. 8Coakley E et al. International Workshop on Targeting HIV Entry 2006; abstract 8.
This table may not include all available reported data; majority of data are generated in the developed world (subtype B)
The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
33
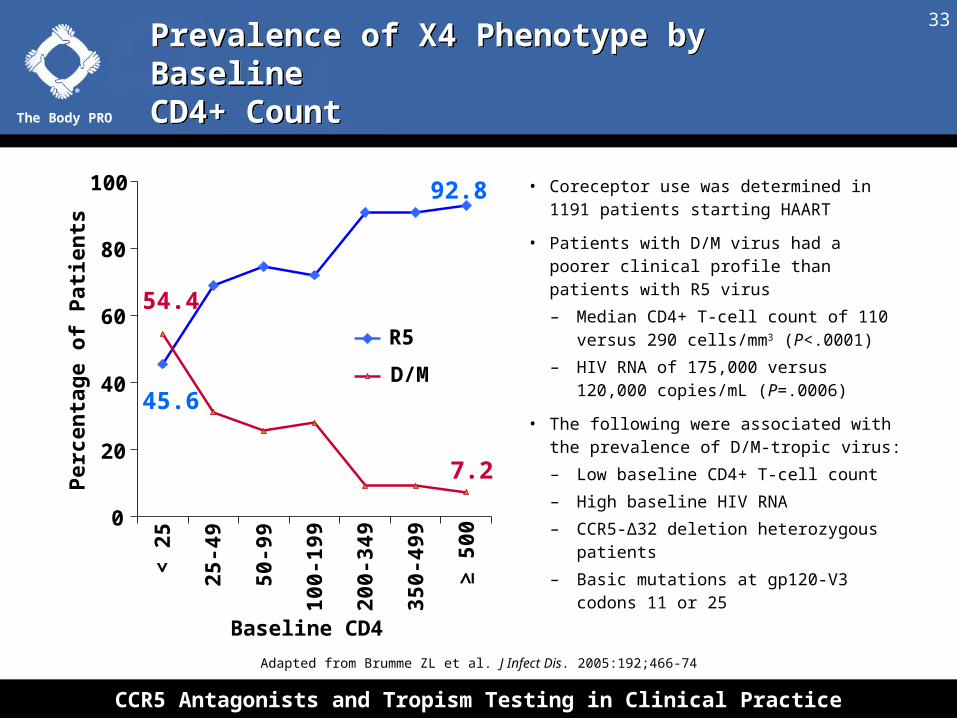
Prevalence of X4 Phenotype by Baseline CD4+ CountPrevalence of X4 Phenotype by Baseline CD4+ Count
Adapted from Brumme ZL et al. J Infect Dis. 2005:192;466-74
Baseline CD4
• Coreceptor use was determined in 1191 patients starting HAART
• Patients with D/M virus had a poorer clinical profile than patients with R5 virus
– Median CD4+ T-cell count of 110 versus 290 cells/mm3 (P<.0001)
– HIV RNA of 175,000 versus 120,000 copies/mL (P=.0006)
• The following were associated with the prevalence of D/M-tropic virus:
– Low baseline CD4+ T-cell count
– High baseline HIV RNA
– CCR5-Δ32 deletion heterozygous patients
– Basic mutations at gp120-V3 codons 11 or 25
92.8
45.6
7.2
54.4
0
20
40
60
80
100<
25
25-4
9
50-9
9
100-
199
200-
349
350-
499
≥ 50
0
Per
cen
tag
e o
f P
atie
nts
R5
D/M

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
34
Tropism in Naive Patients: Impact on CD4+ Decline and Response to TreatmentTropism in Naive Patients: Impact on CD4+ Decline and Response to Treatment
Graeme Moyle et al. ICAAC 2006; abstract H-1667. Reprinted with permission.
• 402 treatment-naive subjects had tropism tested
– 326 R5
– 73 D/M
– 3 X4
• 340 started HAART by August 2006
– 229 R5
– 60 D/M
– 51 excluded from analysis

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
35
CD4+ Decline Before HAARTCD4+ Decline Before HAART
Graeme Moyle et al. ICAAC 2006; abstract H-1667. Reprinted with permission.
DAVG analysis (time weighted differences in average. Censored at HAART; Error bars are 95% CI
The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
36
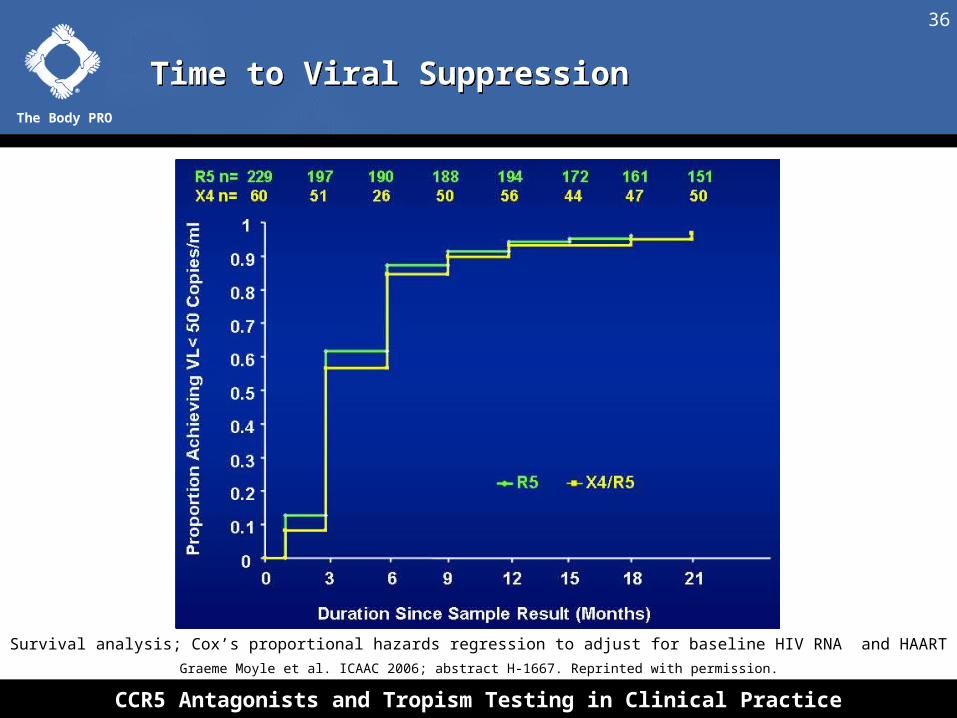
Time to Viral SuppressionTime to Viral Suppression
Graeme Moyle et al. ICAAC 2006; abstract H-1667. Reprinted with permission.
Survival analysis; Cox’s proportional hazards regression to adjust for baseline HIV RNA and HAART

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
37
Tropism Does Not Affect Response to HAARTTropism Does Not Affect Response to HAART
Graeme Moyle et al. ICAAC 2006; abstract H-1667. Reprinted with permission.
R5 TropicR5/X4 Tropic
P Value
CD4+ T-Cell Count Rise at 12 Months, Cells/mm3 (95% CI)
185 (166-204)
182 (145-219)
.812
CD4+ T-Cell Count Rise at 24 Months, Cells/mm3 (95% CI)
247 (227-267)
292 (254-330)
.482
Patients With VL < 50 Copies/mL at 12 Months, n (%)
168 (73.4) 47 (78.3) .509
Patients With VL < 50 Copies/mL at 24 Months, n (%)
166 (72.4) 41 (68.3) .67
CI = confidence interval

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
38
Clinical Trials

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
39
MOTIVATE 1&2: Trial DesignMOTIVATE 1&2: Trial Design
David Hardy et al. CROI 2008; abstract 792. Reprinted with permission.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
40
MOTIVATE 1&2: Demographics and Baseline CharacteristicsMOTIVATE 1&2: Demographics and Baseline Characteristics
David Hardy et al. CROI 2008; abstract 792. Reprinted with permission.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
41
MOTIVATE 1&2: Mean Change in HIV-1 RNA* From Baseline to Week 48MOTIVATE 1&2: Mean Change in HIV-1 RNA* From Baseline to Week 48
David Hardy et al. CROI 2008; abstract 792. Reprinted with permission.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
42
MOTIVATE 1&2: Percentage of Patients With Undetectable HIV-1 RNA
MOTIVATE 1&2: Percentage of Patients With Undetectable HIV-1 RNA
David Hardy et al. CROI 2008; abstract 792. Reprinted with permission.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
43
MOTIVATE 1&2: Mean Change in CD4+ Cell Count From Baseline to Week 48MOTIVATE 1&2: Mean Change in CD4+ Cell Count From Baseline to Week 48
David Hardy et al. CROI 2008; abstract 792. Reprinted with permission.
• CD4+ cell count increases up to 48 weeks were more
favorable in both the maraviroc groups than the placebo group
• The mean change from baseline in CD4+ cell count* was:
• +61 cells/mm3 in the placebo + OBT
• +116 cells/mm3 in maraviroc QD + OBT
• +124 cells/mm3 in the maraviroc BID + OBT group
* Last observation carried forward approach used to impute missing values

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
44MOTIVATE 1&2: Patients With HIV-1 RNA < 50 Copies/mL by Screening Viral Loads and Baseline CD4+ Cell Count (Week 48)
MOTIVATE 1&2: Patients With HIV-1 RNA < 50 Copies/mL by Screening Viral Loads and Baseline CD4+ Cell Count (Week 48)
David Hardy et al. CROI 2008; abstract 792. Reprinted with permission.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
45
MOTIVATE 1&2: Safety Analyses Unadjusted For Duration of ExposureMOTIVATE 1&2: Safety Analyses Unadjusted For Duration of Exposure
David Hardy et al. CROI 2008; abstract 792. Reprinted with permission.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
46MOTIVATE 1&2: Maximum Liver Function Test Values Over 48 Weeks Without Regard To Baseline
MOTIVATE 1&2: Maximum Liver Function Test Values Over 48 Weeks Without Regard To Baseline
David Hardy et al. CROI 2008; abstract 792. Reprinted with permission.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
47MOTIVATE 1&2: Percentage of Adverse Events Occurring in ≥ 5% of Patients in Any Group, Unadjusted for Treatment Exposure
MOTIVATE 1&2: Percentage of Adverse Events Occurring in ≥ 5% of Patients in Any Group, Unadjusted for Treatment Exposure
David Hardy et al. CROI 2008; abstract 792. Reprinted with permission.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
48
VICTOR-E1: Phase IIb Trial of Vicriviroc in Treatment-Experienced PatientsVICTOR-E1: Phase IIb Trial of Vicriviroc in Treatment-Experienced Patients
Barry Zingman et al. CROI 2008; abstract 39LB. Reprinted with permission.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
49
VICTOR-E1: Virologic Efficacy of Vicriviroc vs. Placebo at Week 48VICTOR-E1: Virologic Efficacy of Vicriviroc vs. Placebo at Week 48
No clinically significant differences in adverse events between VCV arms and placebo
Mea
n C
ha
ng
e in
HIV
-1 R
NA
Fro
m
BL
(lo
g1
0 co
pie
s/m
L)
-1.77
-0.79
-2.0
-1.8
-1.0
-0.8
VCV 30 mgn = 39
0
VCV 20 mgn = 40
Placebon = 35
-1.75Difference:
-0.96P = .0028
Difference:-0.98
P = .0017
-1.6
-1.4
-1.2
-0.6
-0.4
-0.2
20
30
70
10
40
50
60
80
90
100
5653
14Pat
ien
ts W
ith
HIV
-RN
A-1
<
50
cop
ies/
mL
(%
)
VCV 30 mgn = 22
0 VCV 20 mg
n = 21 Placebo
n = 5
Barry Zingman et al. CROI 2008; abstract 39LB. Reprinted with permission.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
50
MERIT: Maraviroc vs. Efavirenz in Treatment-Naive PatientsMERIT: Maraviroc vs. Efavirenz in Treatment-Naive Patients
Michael Saag et al. IAS 2007; abstract WESS104. Reprinted with permission.
Antiretroviral-naive patients infected with
CCR5-tropic HIV-1 and HIV-1 RNA
2000 copies/mL
(N = 740)
MVC 300 mg twice daily + ZDV/3TC(n = 360)
EFV 600 mg once daily + ZDV/3TC(n = 361)
Week 48 primary endpoint
Stratified by HIV-1 RNA < or 100,000 copies/mL and by Northern or Southern
Hemisphere
MVC 300-mg once-daily arm discontinued early due to failure to demonstrate noninferiority to efavirenz at end of phase IIB (Week 16)
Week 96
Stringent noninferiority margin: -10% for lower bound of 1-sided 97.5% CI
The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
51
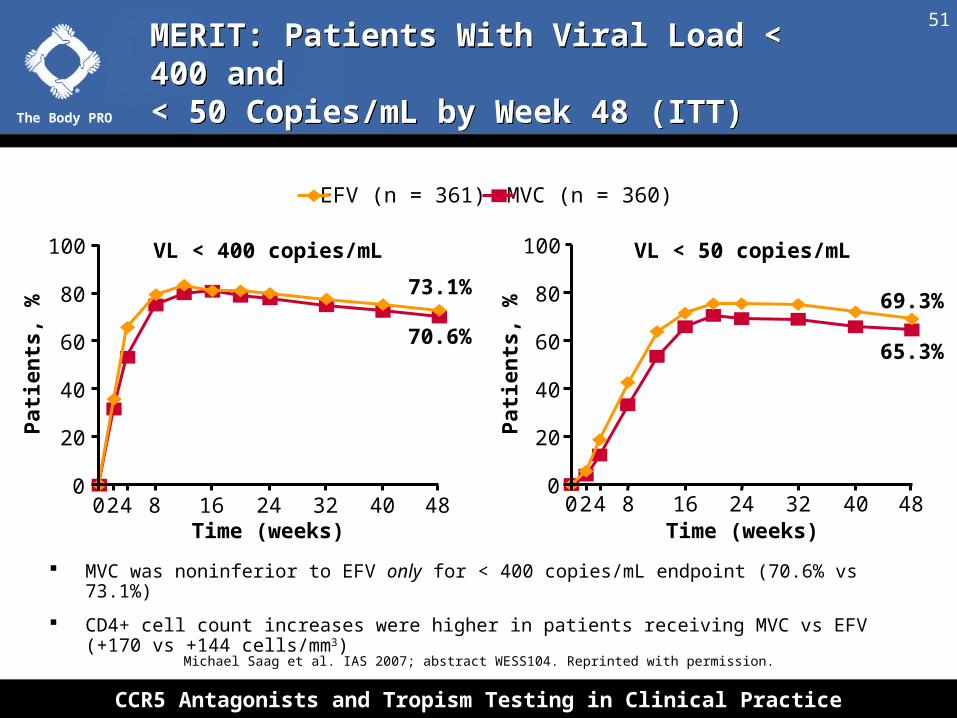
MERIT: Patients With Viral Load < 400 and < 50 Copies/mL by Week 48 (ITT)MERIT: Patients With Viral Load < 400 and < 50 Copies/mL by Week 48 (ITT)
Michael Saag et al. IAS 2007; abstract WESS104. Reprinted with permission.
VL < 400 copies/mL VL < 50 copies/mL
Pat
ien
ts, %
Pat
ien
ts, %
Time (weeks) Time (weeks)
0
20
40
60
80
100
70.6%
73.1%69.3%
65.3%
0
20
40
60
80
100
EFV (n = 361) MVC (n = 360)
24 8 16 24 32 40 480 24 8 16 24 32 40 480
MVC was noninferior to EFV only for < 400 copies/mL endpoint (70.6% vs 73.1%)
CD4+ cell count increases were higher in patients receiving MVC vs EFV (+170 vs +144 cells/mm3)

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
52
MERIT: Patients With Viral Load < 50 Copies/mL by Baseline Viral LoadMERIT: Patients With Viral Load < 50 Copies/mL by Baseline Viral Load
Michael Saag et al. IAS 2007; abstract WESS104. Reprinted with permission.
71.6 69.6 66.659.6
Pat
ien
ts,
%
BL VL < 100,000 Copies/mL
BL VL ≥ 100,000 Copies/mL
0
10
20
30
40
50
60
70
80
90
100
n =
211 204
150 156
MVCEFV EFV patients more likely
to discontinue due to AE
– Overall : 25.2%
– AE: 13.6%
– Efficacy: 4.2%
MVC patients more likely to discontinue due to lack of efficacy
– Overall: 26.9%
– AE: 4.2%
– Efficacy: 11.9%

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
53
MERIT: Week 48 Safety AnalysesMERIT: Week 48 Safety Analyses
All Causalities and Severities EFV + CBVN=361
MVC + CBVN=360
Patients With Adverse Events 340 (94.2) 331 (91.9)
Patients With Grade 3 AEs, n (%) 66 (18.3) 51 (14.2)
Patients With Grade 4 AEs, n (%) 24 (6.6) 22 (6.1)
Patients With SAEs, n (%)† 46 (12.7) 41 (11.3)
Patients With Category C events, n (%) 12 (3.3) 6 (1.7)
Malignancies 16 (4.4) 10 (2.8)
Deaths†*, n (%) 1 1
AEs = adverse events; SAEs = serious adverse events †Based on all data through 21 June 2007*Deaths reported up to 28 days after stopping study drug; one additional death on EFV
within 28 days, date of death not captured in database
Michael Saag et al. IAS 2007; abstract WESS104. Reprinted with permission.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
54
MERIT: Viral Suppression at Week 48 by Baseline TropismMERIT: Viral Suppression at Week 48 by Baseline Tropism
20
30
70
0
10
40
50
60
80
90
100
69.3
54.6
7.1
n = 11 14
68.0
339 331
Pa
tie
nts
Wit
h V
L <
50
c/m
L a
t W
ee
k 4
8 (
%)
EFV
MVC
69.365.3
Tropism at Screening (Overall)
361 360
Tropism at Baseline
(R5)
Tropism at Baseline
(D/M)
• Change in detected HIV-1 tropism from R5 at screening to D/M at BL and potentially adherence may explain some treatment failures on MVC
– 3.5% of patients experienced change in detected tropism between screening and BL
– 50.0% of patients with R5 virus at BL and without confirmed X4 at failure had plasma MVC concentrations below limit of detection
• Tropism changes more common in patients with lower mean CD4+ cell count at screening as well as with clade B or other/undetermined HIV-1 subtype vs clade C
Jayvany Heera et al. CROI 2008; abstract 40LB. Reprinted with permission.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
55
MERIT: Fewer Lipid Effects With Maraviroc vs. Efavirenz at Week 48MERIT: Fewer Lipid Effects With Maraviroc vs. Efavirenz at Week 48
Edwin DeJesus et al. CROI 2008; abstract 929. Reprinted with permission.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
56
Questions
The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
57
Main Discussion QuestionsMain Discussion Questions
• Does the use of CCR5 antagonists prevent the immune system from mounting an effective defense against West Nile virus infection and its complications?
• Is the new enhanced tropism test sensitive enough to more accurately identify patients who may have some X4-tropic virus?
• Is there going to be a second clinical trial of maraviroc in treatment-naive patients that uses the more sensitive assay?
• Who is the best patient to use a CCR5 antagonist?

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
58
Case Studies

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
59
Case 1

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
60
• 37-year-old male with extensive ART history dating back to 1995
• Past ARVs included all NRTIs except ddC, all NNRTIs except DLV, and all PIs except FPV and full-dose RTV
• History of “buffalo hump” while taking IDV; removed with liposuction
• Former participant in the RESIST 1 trial (2003-2005); ART regimen—TPV/r, TDF-FTC, EFV, ddI and ENV
– HIV-1 RNA decreased from 510,000 to 5,200 copies/mL
– CD4+ increased from 75 to 120 cells/mm3
– Failed to achieve HIV-1 RNA < 50 copies/mL
• Discontinued ENF after 2.5 years due to lack of any available injection sites
Experienced low-level viremia prior to discontinuing ENF
Case 1: Patient HistoryCase 1: Patient History

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
61
• Patient also a participant in the MOTIVATE 1 trial
• Randomized to placebo with OBR* of: SQV/RTV, TDF/FTC, ddI, EFV
– IDV/RTV predicted to have full activity by resistance testing, but refused by patient due to prior history of lipodystrophy (buffalo hump)
• After eight weeks, VL 734,000 copies/mL (from 1,162,500 copies/mL), CD4+ 75 cells/mm3 (7.8%)
– < 0.5 log10 decrease, thus considered a virologic failure
• Switched to open-label MVC 150 mg BID, IDV/RTV, TDF/FTC, ddI
– Patient achieved HIV-1 RNA < 50 c/mL by week 24 and CD4+ cells increase to 155/mm3 (22%); maintained for the next six months
– At this time, patient develops bilateral hip pain, is diagnosed with advanced aseptic necrosis of the right hip joint and undergoes right total hip replacement surgery
* Optimized Background Regimen
Case 1: Patient History ContinuedCase 1: Patient History Continued

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
62
A. No
B. Not Sure
C. Yes
Case 1: Would You Consider Changing the Patient’s Regimen at This Time?Case 1: Would You Consider Changing the Patient’s Regimen at This Time?

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
63
Case 1: Case ProgressionCase 1: Case Progression
• You convince the patient to remain on his current regimen to
maintain his HIV RNA < 50 copies/mL
• HIV-1 RNA increases to 580 copies/mL (repeat 1,280 copies/mL)
(You suspect that patient’s confidence in his ART regimen has
waned due to his hip surgery.)
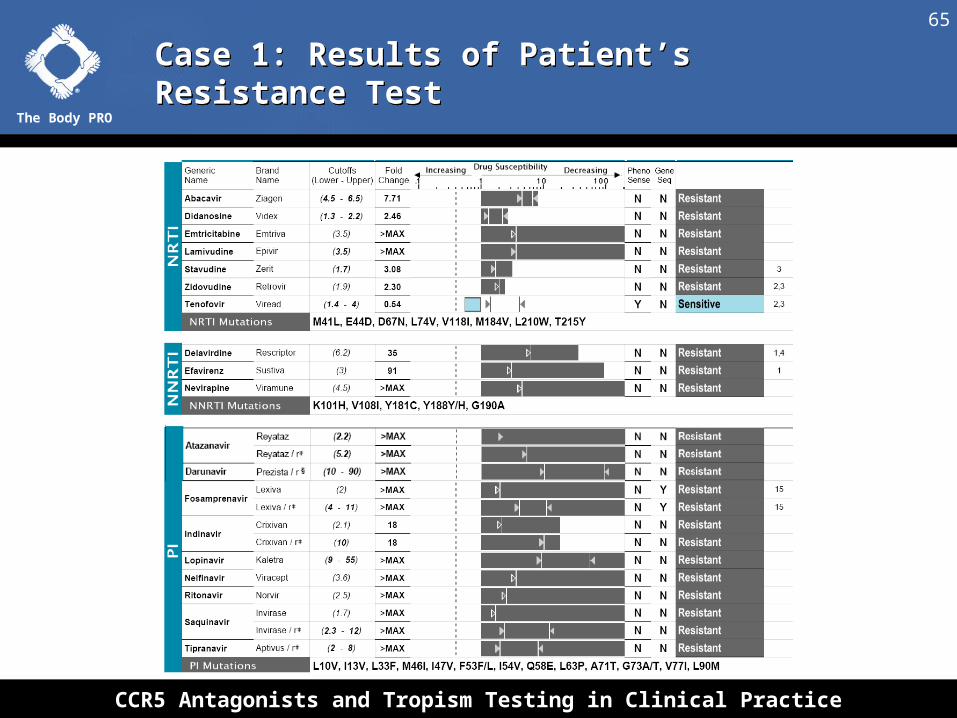
• You determine that a change in regimen is indicated and order a
phenotype and tropism assay
The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
64
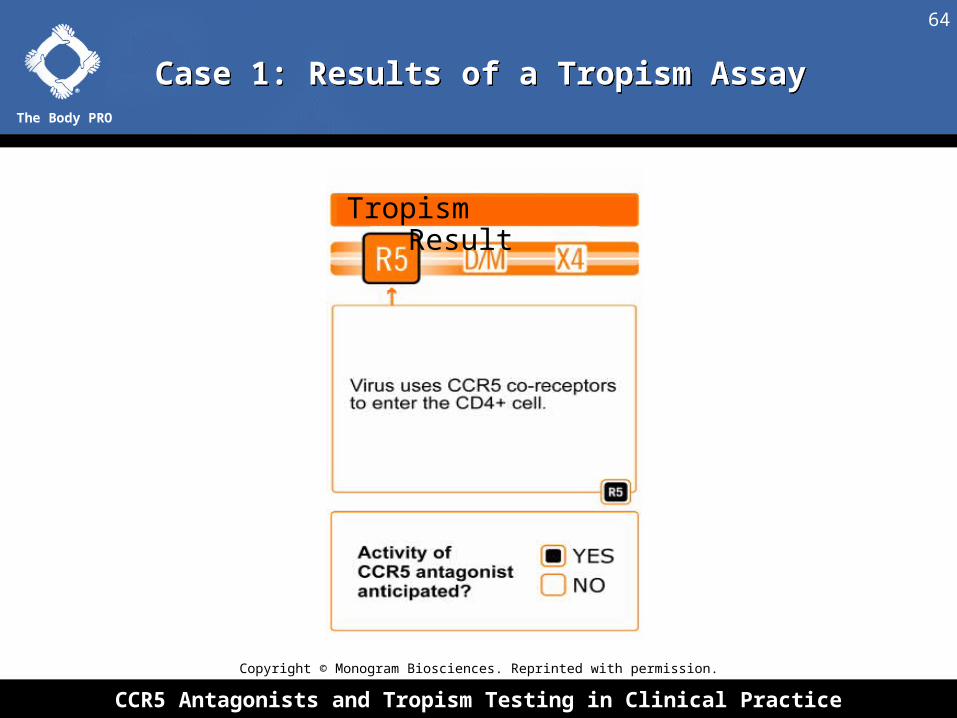
Case 1: Results of a Tropism AssayCase 1: Results of a Tropism Assay
Tropism Result
Copyright © Monogram Biosciences. Reprinted with permission.
The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
65
Case 1: Results of Patient’s Resistance TestCase 1: Results of Patient’s Resistance Test

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
66
Case 1: Should a Boosted PI Be Included in the Patient’s New Regimen?Case 1: Should a Boosted PI Be Included in the Patient’s New Regimen?
A. Yes
B. No
C. Not sure
The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
67
Case 1: If You Included a PI, Which Would You Use?Case 1: If You Included a PI, Which Would You Use?
A. Atazanavir + ritonavir
B. Darunavir + ritonavir
C. Fosamprenavir + ritonavir
D. Lopinavir/ritonavir
E. Saquinavir + ritonavir
F. Tipranavir + ritonavir
G. No PIs

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
68
Case 1: Would You Switch the NRTI Component of the Patient’s Regimen?Case 1: Would You Switch the NRTI Component of the Patient’s Regimen?
A. No
B. Yes, I would drop ddI
C. Yes, I would drop tenofovir/FTC
D. Yes, I would not use NRTIs in his new regimen

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
69
Case 1: Would You Include Raltegravir in the Patient’s New Regimen?Case 1: Would You Include Raltegravir in the Patient’s New Regimen?
A. Yes
B. No
C. Not sure

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
70
Case 1: Would You Include Etravirine in the Patient’s New Regimen?Case 1: Would You Include Etravirine in the Patient’s New Regimen?
A. Yes
B. No
C. Not sure

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
71
Case 1: Etravirine Resistance InformationCase 1: Etravirine Resistance Information
2008 Update
• Clinical cut offs (CCOs) determined for
phenotypic sensitivity
• Four additional etravirine RAMS identified
(17 total)
• Weighted scoring system developed

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
72
Case 1: Response According to Phenotypic Etravirine CCOsCase 1: Response According to Phenotypic Etravirine CCOs
Etravirine
CCO
Proportion of Patients With Viral Load < 50 Copies/mL (DUET Week 24),
% (n)
Decrease in log10 Viral Load From Baseline (DUET Week 24),
Mean (SE)
< 3 71 (190/269) –2.67 (1.03)
3–13 50 (37/74) –2.39 (1.21)
> 13 37 (22/60) –1.79 (1.42)
Overall Placebo
36 (149/414) –1.51 (1.42)
The highest responses occurred in patients with a fold change < 3
Virological responses were greater than placebo in patients with a fold change < 13
The highest responses occurred in patients with a fold change < 3
Virological responses were greater than placebo in patients with a fold change < 13

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
73
00
1010
2020
3030
4040
5050
6060
7070
8080
no muta
tion*
no muta
tion*
L100I
L100I
G190A
G190A
V90I
V90I
E138A
E138A
Y181I
Y181I
M23
0L
M23
0L
A98G
A98G
Y181C
Y181C
K101E
K101E
K101P
K101P
K101H
K101H
V179D
V179D
V106I
V106I
V179T
V179T
Y181V
Y181V
G190S
G190S
V179F
V179F
34 115 4 59 110 26 5 24 8 6 14 7Pat
ien
ts w
ith
co
nfi
rmed
VL
P
atie
nts
wit
h c
on
firm
ed V
L
<50
HIV
-1 R
NA
co
pie
s/m
L (
%)
<50
HIV
-1 R
NA
co
pie
s/m
L (
%)
Pat
ien
ts w
ith
co
nfi
rmed
VL
P
atie
nts
wit
h c
on
firm
ed V
L
<50
HIV
-1 R
NA
co
pie
s/m
L (
%)
<50
HIV
-1 R
NA
co
pie
s/m
L (
%)
*no detectable baseline NNRTI RAM from the list of 44; Dashed line indicates 75% of response in patients without NNRTI RAMs
22 12 8 53 9 n=n=
NewNew NewNewNewNew
NewNew
52
Effect of the Etravirine RAMs 2008(17) on Virological ResponseEffect of the Etravirine RAMs 2008(17) on Virological Response

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
74

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
75
§§
Y181IY181IY181VY181VK101PK101PL100IL100IY181CY181CM230LM230LE138AE138AV106IV106IG190SG190SV179FV179FV90IV90I
V179DV179DK101EK101EK101HK101HA98GA98GV179TV179TG190AG190A
§V179F was never present as single Etravirine RAM (always with Y181C)
Weight for Individual Mutations
Weight for Individual Mutations
Add TogetherAdd TogetherAdd TogetherAdd Together
Total Weighted
Score
Total Weighted
Score
33
2.52.52.52.51.51.51.51.51111111
Case 1: Weighting of 2008 Etravirine RAMsCase 1: Weighting of 2008 Etravirine RAMs

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
76Case 1: Relation Between the 2008 Etravirine Genotypic Score and the Virological Response (< 50 Copies/mL At Week 24)
Case 1: Relation Between the 2008 Etravirine Genotypic Score and the Virological Response (< 50 Copies/mL At Week 24)

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
77
Case 1: Would You Continue Maraviroc in the Patient’s New Regimen?Case 1: Would You Continue Maraviroc in the Patient’s New Regimen?
A. Yes
B. No
C. Not sure

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
78
Case 1: Case ProgressionCase 1: Case Progression
• On his new regimen of MVC, DRV/r, ETV, RAL and
TDF/FTC his HIV-1 RNA remains < 50 copies/mL and
CD4+ cells slowly rise to 280 cells/mm3 (28%) over the
next eight months
• His left hip pain and MRI of it stabilize showing no further
progression
• He continues to tolerate his ART regimen well

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
79
Case 2

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
80
Case 2: Patient HistoryCase 2: Patient History
• 45-year-old man
• Diagnosed with HIV-1 in 1994 when he presented
with cutaneous Kaposi’s Sarcoma
– CD4+ cell count: 360 cells/mm³
– HIV-1 RNA test not available in 1994
• PMH: mild hypertension, controlled with diuretics
• FMH: diabetes, CVD
The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
81
Case 2: Patient ARV HistoryCase 2: Patient ARV History
• 1994: ZDV monotherapy
– Discontinued six months later due to anemia and
nausea
• ddI monotherapy
– Tolerated for nine months, then developed
pancreatitis
• Discontinued ARVs: KS quiescent, CD4+ cell count
stable at 360 cells/mm³

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
82
Case 2: Patient History on HAART RegimensCase 2: Patient History on HAART Regimens
• Starting in 1996, various regimens including
– d4T + 3TC + SQV
– d4T + 3TC + NFV
– ABC + 3TC + EFV
– d4T + 3TC + LPV/RTV
– TDF + 3TC + LPV/RTV + FPV
• Intolerant to ZDV (anemia), ddI (pancreatitis), d4T
(peripheral neuropathy), NFV (diarrhea), dual-
boosted PIs (GI symptoms)

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
83
Case 2: Patient History on HAART Regimens (Continued)Case 2: Patient History on HAART Regimens (Continued)
• Reached HIV-1 RNA < 400 copies/mL but never < 50 copies/mL
• First genotypic assay (after d4T + 3TC + SQV)
– RT gene: M41L, L74V, M184V, T215Y
PR gene: L10I, L63P, L90M
• Second genotypic assay (after ABC + 3TC + EFV)
– RT gene: M41L, L74V, K101P, K103N, Y181C, M184V, T215Y,
K219R
– PR gene: L10I, D30D/N, L63P, G73T, V77I, L90M
• CD4+ cell counts rose and fell, nadir: 240 cells/mm³

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
84
Case 2: Current History: 2008Case 2: Current History: 2008
• Regimen: TDF + 3TC + LPV/RTV
– HIV-1 RNA: 1,500-2,500 copies/mL
– CD4+ cell count: 300-350 cells/mm³
• Hypertension poorly controlled with ACE
inhibitor/diuretic + β-blocker
• Fasting glucose > 180 mg/dL
• Serum creatinine 1.9 mg/dL (baseline 1.0-1.4 mg/dL)
• Patient wants to consider a new regimen

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
85
Case 2: Drug Resistance Test ResultsCase 2: Drug Resistance Test Results

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
86
Case 2: Viral Tropism AssayCase 2: Viral Tropism Assay
Tropism Result
Copyright © Monogram Biosciences. Reprinted with permission.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
87
Darunavir Resistance Mutations
• 11I, 32I, 33F, 47V, 50V, 54L/M, 74P, 76V, 84V, 89V
Tipranavir Resistance Mutations
• 10V, 13V, 20M/R/V, 33F, 35G, 36I, 43T, 46L, 47V, 54A/M/V, 58E, 69K, 74P, 82L/T, 83D, 84V
Case 2: Would You Use Darunavir or Tipranavir in the New Regimen?Case 2: Would You Use Darunavir or Tipranavir in the New Regimen?
A. Yes, I would use darunavir + ritonavir
B. Yes, I would use tipranavir + ritonavir
C. Yes, I would use both
D. No, I would not use either

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
88
Case 2: Would You Use NRTIs inThis Regimen?Case 2: Would You Use NRTIs inThis Regimen?
Phenotype
• NRTIs: susceptible to TDF, ZDV, d4T
• NNRTIs: resistant to DLV, EFV, NVP
• PIs: partially susceptible to DRV
A. Yes
B. No

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
89Case 2: How Many Additional Active Agents Does This Patient Need to Achieve HIV-1 RNA < 50 Copies/mL?
Case 2: How Many Additional Active Agents Does This Patient Need to Achieve HIV-1 RNA < 50 Copies/mL?
A. 1
B. 2
C. 3
D. Individualized for patient’s viral resistance
The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
90
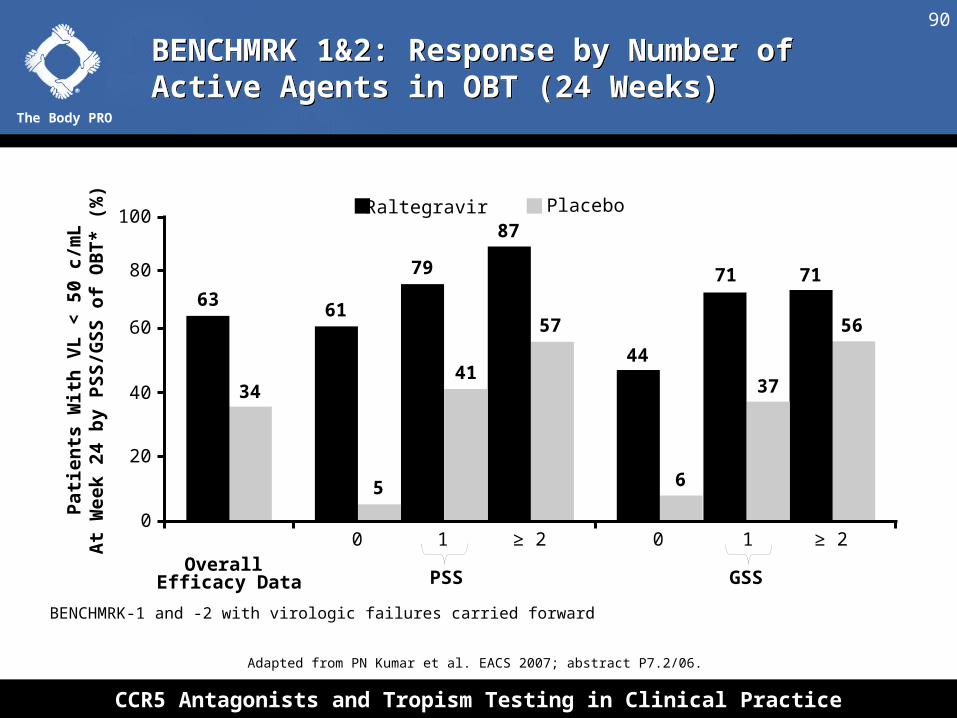
BENCHMRK-1 and -2 with virologic failures carried forward
5
PSS GSS
63
34
61
41
87
79
57
71
56
37
71
6
44
0 1 ≥ 2 0 1 ≥ 2Overall
Efficacy Data
Pat
ien
ts W
ith
VL
< 5
0 c/
mL
At
Wee
k 2
4 b
y P
SS
/GS
S o
f O
BT
* (%
)
0
20
40
60
80
100 Raltegravir Placebo
BENCHMRK 1&2: Response by Number of Active Agents in OBT (24 Weeks)BENCHMRK 1&2: Response by Number of Active Agents in OBT (24 Weeks)
Adapted from PN Kumar et al. EACS 2007; abstract P7.2/06.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
91
DUET 1&2: Response by Number of Active Agents in OBT (24 Weeks)DUET 1&2: Response by Number of Active Agents in OBT (24 Weeks)
Anthony Mills and Christine Katlama et al. IAS 2007, abstract WESS204. Reprinted with permission.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
92
MOTIVATE 1&2: Response by Number of Active Agents in OBT (24 Weeks)MOTIVATE 1&2: Response by Number of Active Agents in OBT (24 Weeks)
0
20
40
60
80P
atie
nts
(%
)
3 or More 2 1 0
MVC BID + OBT
MVC QD + OBT
Placebo + OBT
3
58 61
5355
19
52
43 43
9
29
18
N= 121 132 64 104 88 59 134 130 44 56 51 35
Number of Active Drugs in OBT
Adapted from Mark Nelson et al. CROI 2007; abstract 104aLB. Adapted from Jacob Lalezari et al. CROI 2007; abstract 104bLB.

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
93
Case 2: Which Regimen Would You Choose?Case 2: Which Regimen Would You Choose?
A. tenofovir/emtricitabine, darunavir + ritonavir,
etravirine, maraviroc
B. tenofovir/emtricitabine, darunavir + ritonavir,
maraviroc, raltegravir
C. tenofovir/emtricitabine, darunavir + ritonavir,
etravirine, raltegravir
D. tenofovir/emtricitabine, darunavir + ritonavir,
etravirine, maraviroc, raltegravir
E. Something else

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
94
Case 2: EvolutionCase 2: Evolution
• New regimen: TDF/FTC + DRV/RTV + ETR + MVC + RAL
• HIV-1 RNA at 6 weeks: < 50 copies/mL
• CD4+ cell count at 10 weeks: 420 cells/mm³
• Serum creatinine ↑ to 2.7 mg/dL (from 1.9 mg/dL);
24-hour ClCr: 48 mL/min

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
95
Case 2: What Would You Do Now With the NRTI Portion of the Regimen?
Case 2: What Would You Do Now With the NRTI Portion of the Regimen?
A. Continue TDF/FTC QD
B. Continue TDF/FTC but decrease the dose to QOD
C. Change TDF/FTC to ABC/3TC
D. Discontinue TDF/FTC

The Body PRO
CCR5 Antagonists and Tropism Testing in Clinical Practice
96
Case 2: EvolutionCase 2: Evolution
• Tenofovir discontinued due to concerns about
decreased renal function
• New regimen: DRV/RTV + ETR + MVC + RAL
• HIV-1 RNA < 50 copies/mL
• CD4+ count ↑ to 550 cells/mm³ (from 420 cells/mm³)
• Serum creatinine to 1.8 mg/dL (from 2.7 mg/dL);
24-hour ClCr: ↑ to 80 mL/min (from 24 mL/min)