cataract
TRANSCRIPT

CataractBy: Ola S. Eldardiry
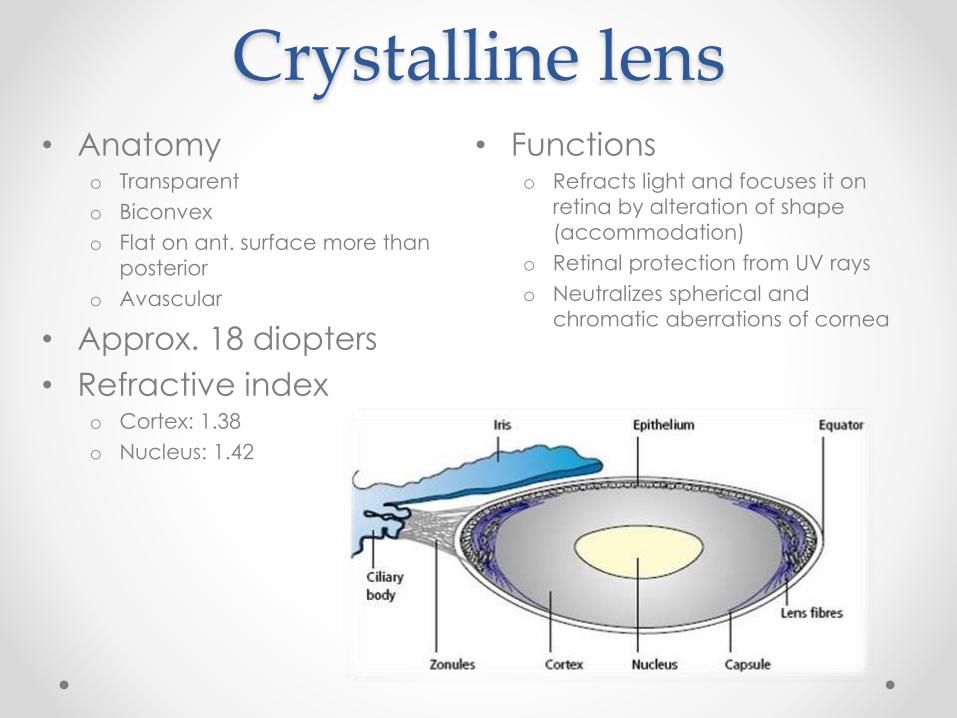
Crystalline lens• Anatomy
o Transparent
o Biconvex
o Flat on ant. surface more than
posterior
o Avascular
• Approx. 18 diopters
• Refractive indexo Cortex: 1.38
o Nucleus: 1.42
• Functionso Refracts light and focuses it on
retina by alteration of shape
(accommodation)
o Retinal protection from UV rays
o Neutralizes spherical and
chromatic aberrations of cornea

Structure and zones
• Made up ofo Capsule
o Lens epithelium (anterior only)
o Lens fibers
• Zoneso Cortex
• Anterior cortex
• Equatorial cortex
• Posterior cortex
o Nucleus
• Embryonic
• Foetal
• Infantile
• Adult
• Metabolism: facilitated diffusion of glucose from across capsule
Cataract
(opacity of crystalline lens)
Congenital/developmental Acquired
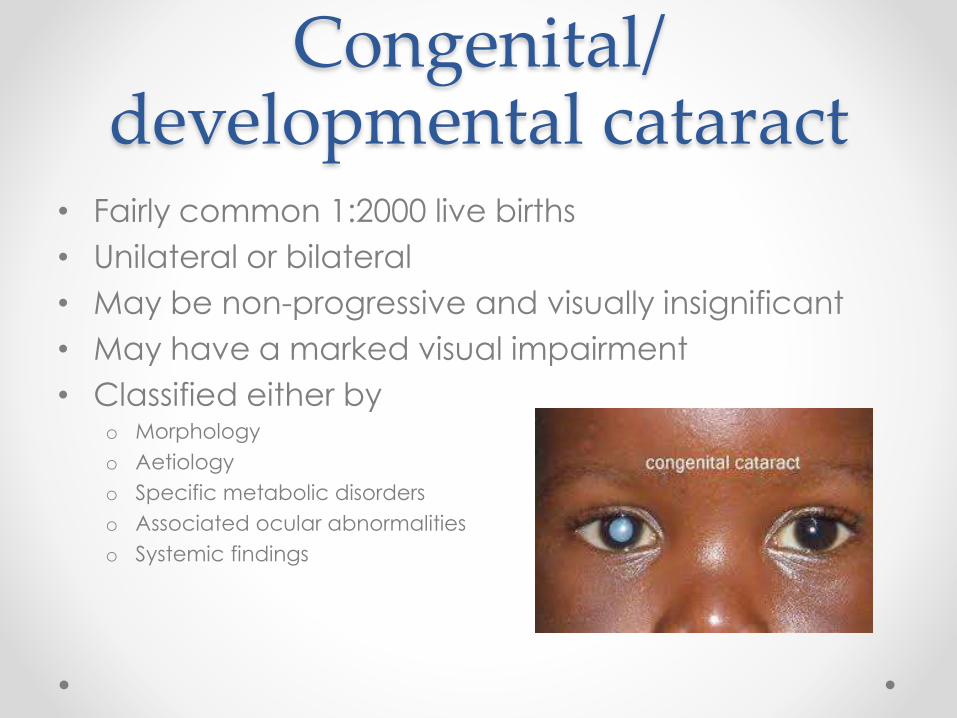
Congenital/ developmental cataract
• Fairly common 1:2000 live births
• Unilateral or bilateral
• May be non-progressive and visually insignificant
• May have a marked visual impairment
• Classified either byo Morphology
o Aetiology
o Specific metabolic disorders
o Associated ocular abnormalities
o Systemic findings

Aetiology• Gestational disturbance
o Intrauterine infections
o Maternal drug intake
o Irradiation
o Nutritional
• Metabolic disorderso DM
o Galactosemia
o Hypoglycaemia
o Hypoparathyroidism
• Traumao Mechanical
o Electric shock
• Ocular anomalieso Aniridia
o Ectopia lentis
o Persistent hyperplastic primary
vitreous
o Remnants of tunica vasculosa
lentis
o Congenital anomalies of lens
• Idiopathic
• Inheritance (recessive)
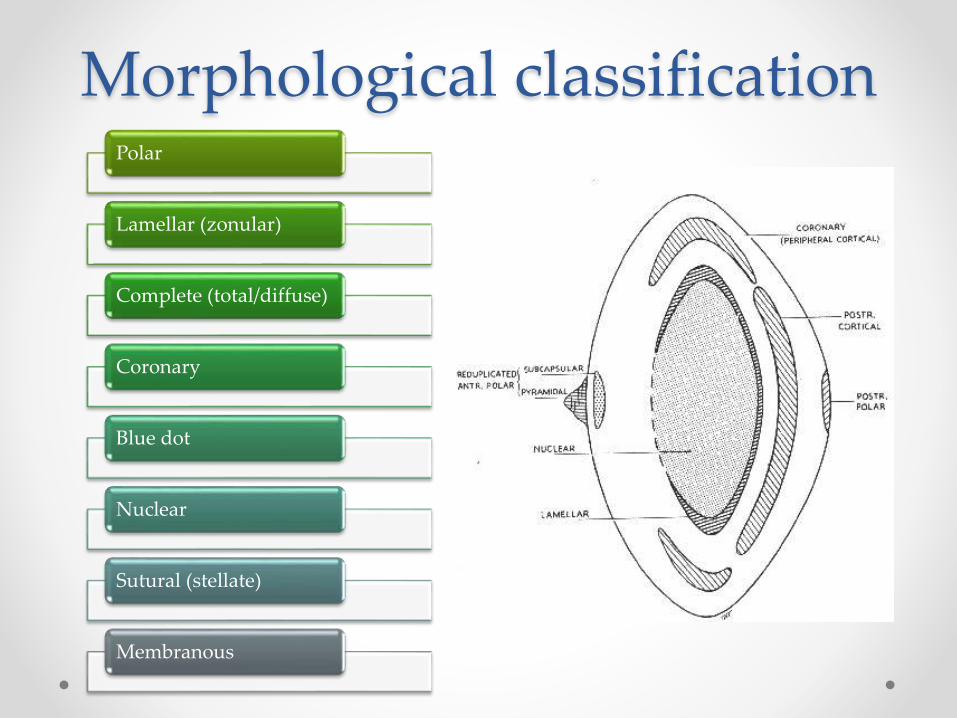
Morphological classificationPolar
Lamellar (zonular)
Complete (total/diffuse)
Coronary
Blue dot
Nuclear
Sutural (stellate)
Membranous

Polar cataract• Opacities involve Lens capsule and subcapsular
cortex
• Subtypes o Anterior polar
• Small
• Symmetric
• Non progressive
• Doesn’t impair vision
• May project into AC – pyramidal cataract
o Posterior polar
• Larger
• Closer to NP
• More visual
impairment

Lamellar (zonular)
• Most common type
• Bilateral
• Opacification of specific
layers/zones
• Slit lamp examinationo Layer of opacification involving foetal
nucleus surrounding clearer center and
surrounded in turn by layer of clear cortex
o Front view: disc shaped configuration
o Arcuate opacities straddle equator (riders)
• Aetiologyo transient toxic influence during
embryogenesis
o Calcium and vit D deficiency during
pregnancy

Complete (total/diffuse)
• May start as subtotal at birth then progress
• Profound visual impairment
• Requires urgent surgery

Coronary cataract
• Developmenta
• Manifested usually at puberty
• Club shaped opacities near periphery of lens with
broad ends towards center

Blue dot cataract• Multiple small bluish dots
• Scattered all over lens
• Cause no visual disturbance
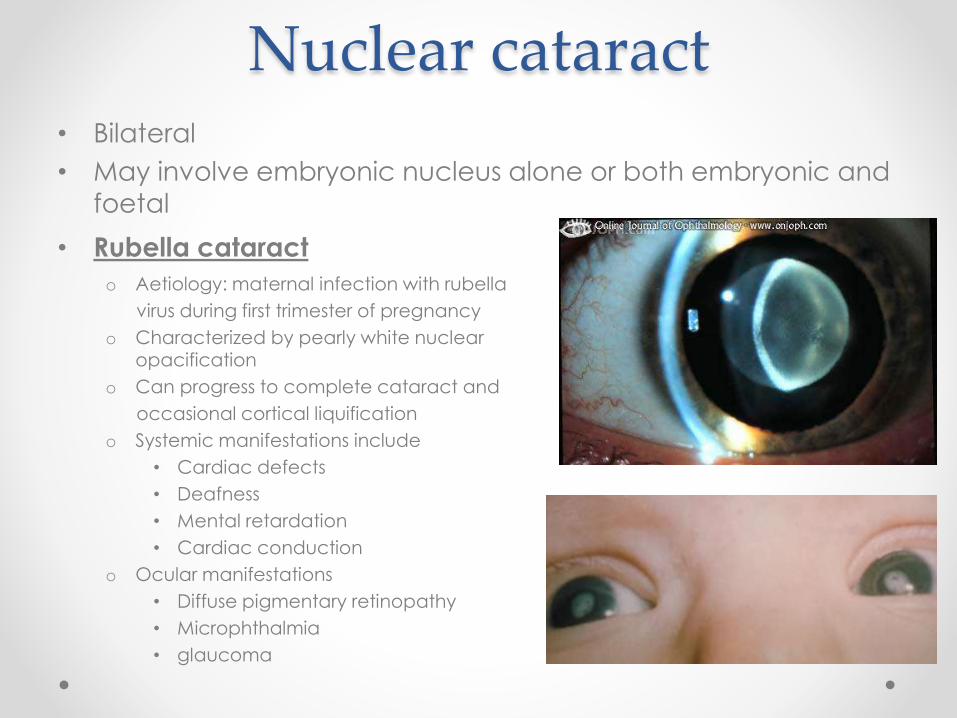
Nuclear cataract
• Rubella cataract
o Aetiology: maternal infection with rubella
virus during first trimester of pregnancy
o Characterized by pearly white nuclear opacification
o Can progress to complete cataract and
occasional cortical liquification
o Systemic manifestations include
• Cardiac defects
• Deafness
• Mental retardation
• Cardiac conduction
o Ocular manifestations
• Diffuse pigmentary retinopathy
• Microphthalmia
• glaucoma
• Bilateral
• May involve embryonic nucleus alone or both embryonic and
foetal

Membranous cataract
• Lens proteins resorbed
• Only anterior and posterior lens capsules remain
and fuse into dense white membrane
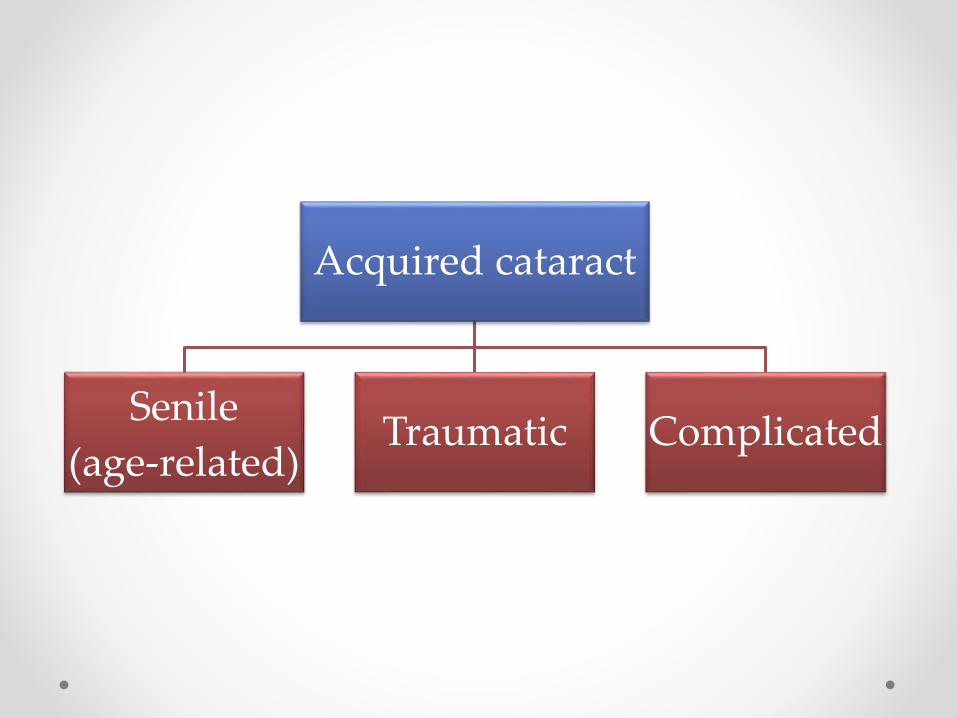
Acquired cataract
Senile
(age-related)Traumatic Complicated
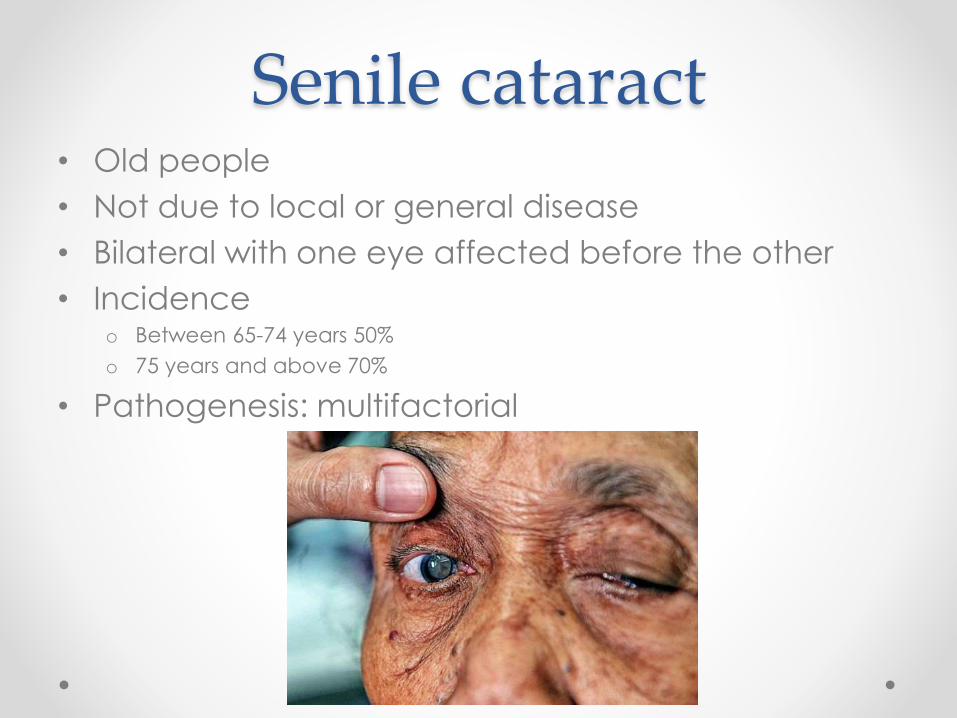
Senile cataract• Old people
• Not due to local or general disease
• Bilateral with one eye affected before the other
• Incidenceo Between 65-74 years 50%
o 75 years and above 70%
• Pathogenesis: multifactorial
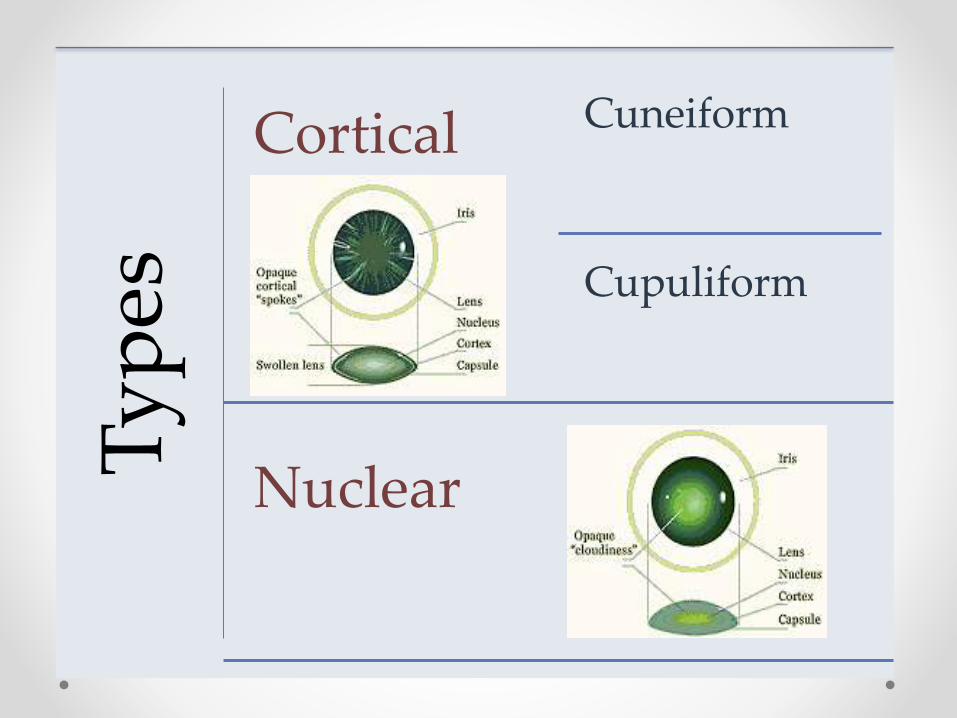
Ty
pes
Cortical Cuneiform
Cupuliform
Nuclear
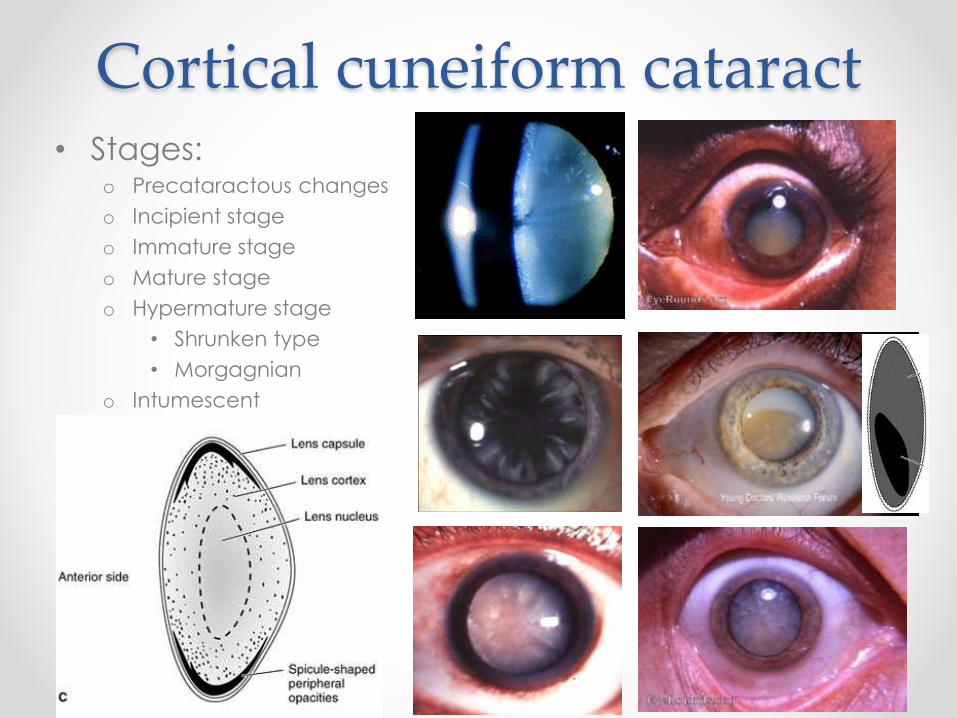
Cortical cuneiform cataract• Stages:
o Precataractous changes
o Incipient stage
o Immature stage
o Mature stage
o Hypermature stage
• Shrunken type
• Morgagnian
o Intumescent

Cortical cupuliformcataract
• Posterior subcapsular
• Central
• Causes glare and poor vision under bright lightening
conditions
• Near vision reduced more than distant
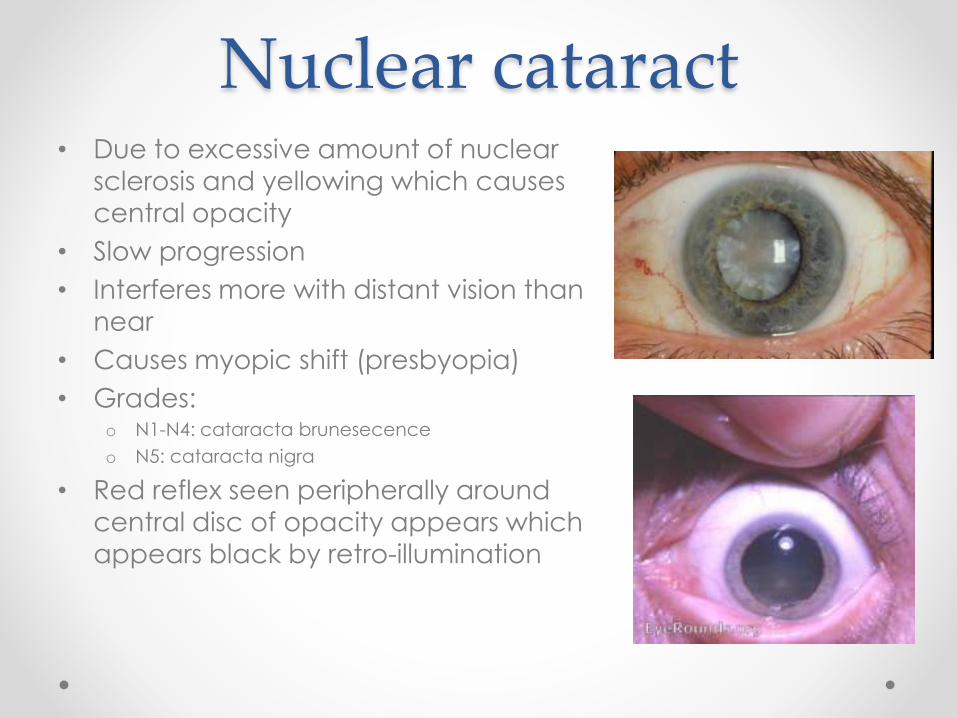
Nuclear cataract• Due to excessive amount of nuclear
sclerosis and yellowing which causes
central opacity
• Slow progression
• Interferes more with distant vision than
near
• Causes myopic shift (presbyopia)
• Grades:o N1-N4: cataracta brunesecence
o N5: cataracta nigra
• Red reflex seen peripherally around
central disc of opacity appears which
appears black by retro-illumination

Traumatic cataract• Perforating injury
• Concussion (contusion) injuryo Vossius ring
o Rosette-Shaped opacity
o Subluxation and dislocation
• Radiation injuryo Ionizing radiation (X-ray)
o Infra-red radiation (glass blower’s cataract)
o UV radiation
• Chemical injuryo Alkali (caustic) burn
o Chalcosis (sunflower cataract)
o Siderosis
• Electrical injury

Complicated cataract• Due to local eye disease or general (systematic)
disease
• Local eye diseaseo Perforated corneal ulcer
o Iridocyclitis
o Chronic glaucoma
o Retina and choroid disease
• General diseaseo Metabolic
• DM
• Galactosemia
o Endocrinal
• Hyperparathyroidism
• Hypothyroidism
o Severe anaemia
o Hypertension
o Idiopathic: systemic steroids in genetically prone patients

Diabetes mellitus and the lens
Increased blood sugar
Increased aqueous
content of lens
Increased glucose
content of lenssorbitol
Water influx into lens
Lens swelling +
myopic change
Ch
ang
e in
ref
ract
ive
ind
ex
• Reverse to hypermetropic change if there is hypoglycemia
• Decreased amplitude
of accommodation
o With early presbyopia
• Cataract (two types)
o True-diabetic (snow-flake
cataract)
o Senile and pre-senile
cataract
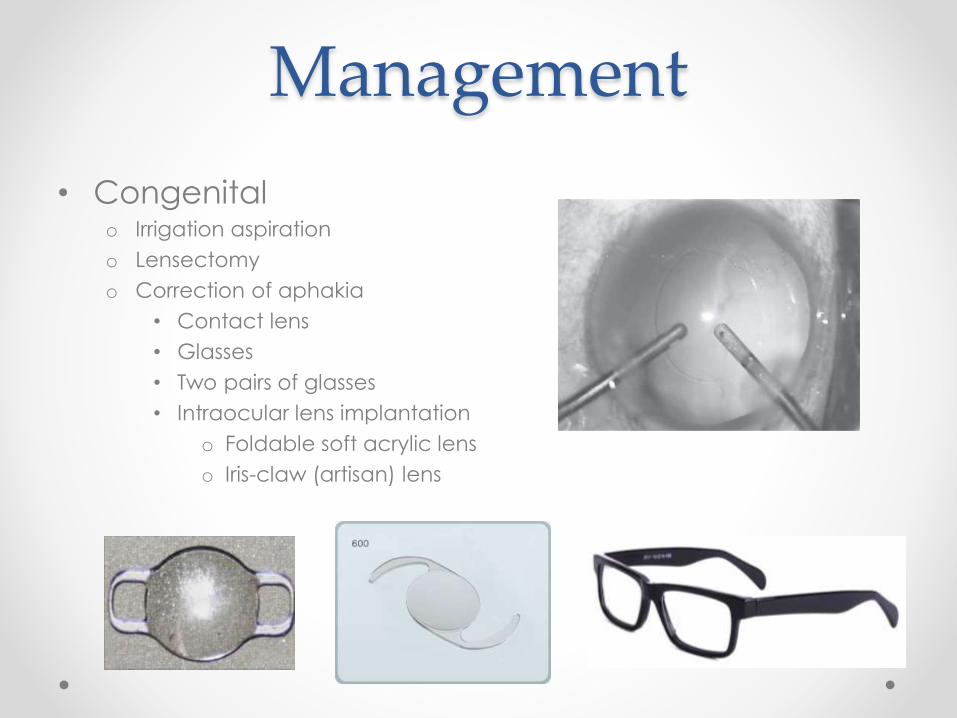
Management
• Congenitalo Irrigation aspiration
o Lensectomy
o Correction of aphakia
• Contact lens
• Glasses
• Two pairs of glasses
• Intraocular lens implantation
o Foldable soft acrylic lens
o Iris-claw (artisan) lens
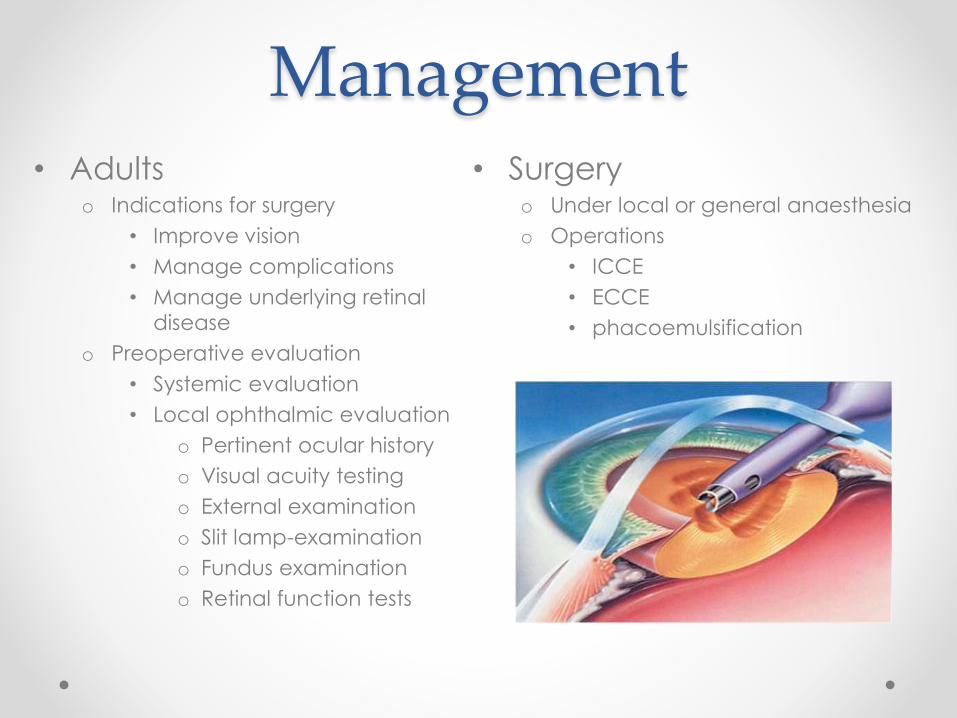
Management • Adults
o Indications for surgery
• Improve vision
• Manage complications
• Manage underlying retinal
disease
o Preoperative evaluation
• Systemic evaluation
• Local ophthalmic evaluation
o Pertinent ocular history
o Visual acuity testing
o External examination
o Slit lamp-examination
o Fundus examination
o Retinal function tests
• Surgeryo Under local or general anaesthesia
o Operations
• ICCE
• ECCE
• phacoemulsification
