case report gliosarcoma with primitive neuroectodermal ... · gliosarcoma with primitive...
TRANSCRIPT
Int J Clin Exp Pathol 2015;8(2):2079-2084www.ijcep.com /ISSN:1936-2625/IJCEP0004809
Case ReportGliosarcoma with primitive neuroectodermal, osseous, cartilage and adipocyte differentiation: a case report
Kun Yao1, Xue-Ling Qi2, Xi Mei3, Tao Jiang4
1Department of Neurosurgery, Beijing Tiantan Hospital, Capital Medical University, Beijing, China; 2Department of Pathology, Beijing San Bo Brain Hospital, Capital Medical University, Haidian District, Beijng, P. R. China; 3Beijing Key Laboratory of Epilepsy, Beijing San Bo Brain Hospital, Capital Medical University, Haidian District, Beijng, P. R. China; 4Department of Neurosurgery, Beijing Tiantan Hospital, Capital Medical University, Beijing, China
Received December 14, 2014; Accepted February 6, 2015; Epub February 1, 2015; Published February 15, 2015
Abstract: We describe a rare case of gliosarcoma with primitive neuroectodermal, osseous, cartilage and adipo-cyte differentiation. A 57-year-old man experienced a month history of headache, nausea and vomiting. Worse yet, the headache has become more severe for the past 6 days. Magnetic resonance (MR) images disclosed a lesion with operative indications located in the right frontal lobe. Then the tumor was macroscopically totally removed. Histologically, the tumor showed two kinds of components. One kind of the tumor cells appeared typical astrocytic tumor cells with anaplastic appearance. The other kind of the tumor cells appeared sheets of small round hyper-chromatic cells, which presented a kind of pancreatic neuroendocrine tumor (PNET) -like structure. These sheets of small round cells were surrounded by a large number of relative-sparse-spindle cells. Multiple separate distinct areas of adipose tissue, osteoid matrix laid down and cartilage tissue were also identified. Immunohistochemically, a portion of typical astrocytic tumor cells and some small round hyperchromatic cells showed GFAP positivity. Small round hyperchromatic cells were positive for S-100, Fli-1, Nestin, MAP-2 and Syn. A large amount of relative sparse spindle cells (sarcomatous areas) were positive for vimentin. In addition, reticulin staining demonstrated expres-sion of reticular fibers in relative-sparse-spindle cells areas but not in the astrocytic tumor cells and small round hyperchromatic cells areas. Molecular cytogenetic analyses demonstrated PTEN allele loss and no evidence of amplification of EGFR in both the astrocytic tumor cells, PNET-like structure and sparse spindle cells areas. These data suggest that this tumor was a gliosarcoma with primitive neuroectodermal, osseous, cartilage and adipocyte differentiation. To our knowledge, this is a rare gliosarcoma , reporting our additional new case would add to the better understanding of this tumor.
Keywords: Gliosarcom, osseous, cartilage, adipocyte, FISH, PNET
Introduction
Gliosarcoma (GS) is a primary central nervous system neoplasm composed of both malignant glial and sarcomatous components. While GS belongs to World Health Organization (WHO) grade IV neoplasm the occurrence of osseous, cartilage and adipocyte elements is an exceed-ingly rare case. The histogenesis and histology of GS was highly controversial. Recent studies have supported the contention that both ele-ments of this biphasic neoplasm may arise from a single progenitor clone rather than from separate clones. Both glial and mesenchymal elements may be derived from a common neo-plastic neuroectodermal progenitor cell [1-3]. We therefore present the clinical, light micro-
scopic, immunohistochemical and molecular findings of this rare gliosarcoma with primitive neuroectodermal, osseous, cartilage and adi-pocyte differentiation.
Case report
A 57-year-old man presented with a month his-tory of headache, nausea and vomiting and the headache has worsened for the past 6 days. Magnetic resonance (MR) images disclosed a lesion in the right frontal lobe. T2 weighted axial MR imaging of the brain revealed a large het-erogeneous mass lesion in the right frontal lobe with wide peri-tumoral oedema. The tumor had complex solid areas with associated mass effect and midline shift (Figure 1B). MR images

GS with PNET, osseous, cartilage and adipocyte differentiation
2080 Int J Clin Exp Pathol 2015;8(2):2079-2084
showed hypointense on T1-weighted MR imag-es and enhancement on T1 gadolinium (Gd) image (Figure 1A, 1C). No attachment to the overlying skull bones or meninges was appa- rent.
The tumor was microscopically totally removed and subjected to histopathological examina-tion. Afterwards the patient received radiother-apy and chemotherapy during the next follow-ing months. Up to now, he has not showed any symptom or sign of recurrence, with a survival time of more than 11 months.
Microscopically, the tumor was texture medi-um, dark- red mass, rubbery tissue with associ-ated chondro-osseous portions, measured 6.5 cm × 5 cm × 4.5 cm in size. After formalin fixa-tion, 4-μ-thick paraffin sections were stained routinely with HE and reticulin. Immunohisto- chemical (IHC) staining was performed with monoclonal antibodies against GFAP (1:500), Fli-1 (1:400), vimentin (1:50), MAP-2 (1:500), nestin (1:300), synaptophysin (Syn, 1:300), EMA (1:250) S-100 (1:300), pan-cytokeratin (1:250), desmin (1:300), TP53 (1:300) and MIB-1 respectively. All antibodies were pur-chased from DAKO, Denmark. In addition, posi-tive and negative controls were also included and evaluated appropriately for each proce-dure. In addition, reticular fiber staining were also performed.
Histologically, there was significant heterogene-ity among the sections of formalin fixed paraffin embedded tumor tissue. One kind of the tumor appeared typical astrocytic tumor cells with
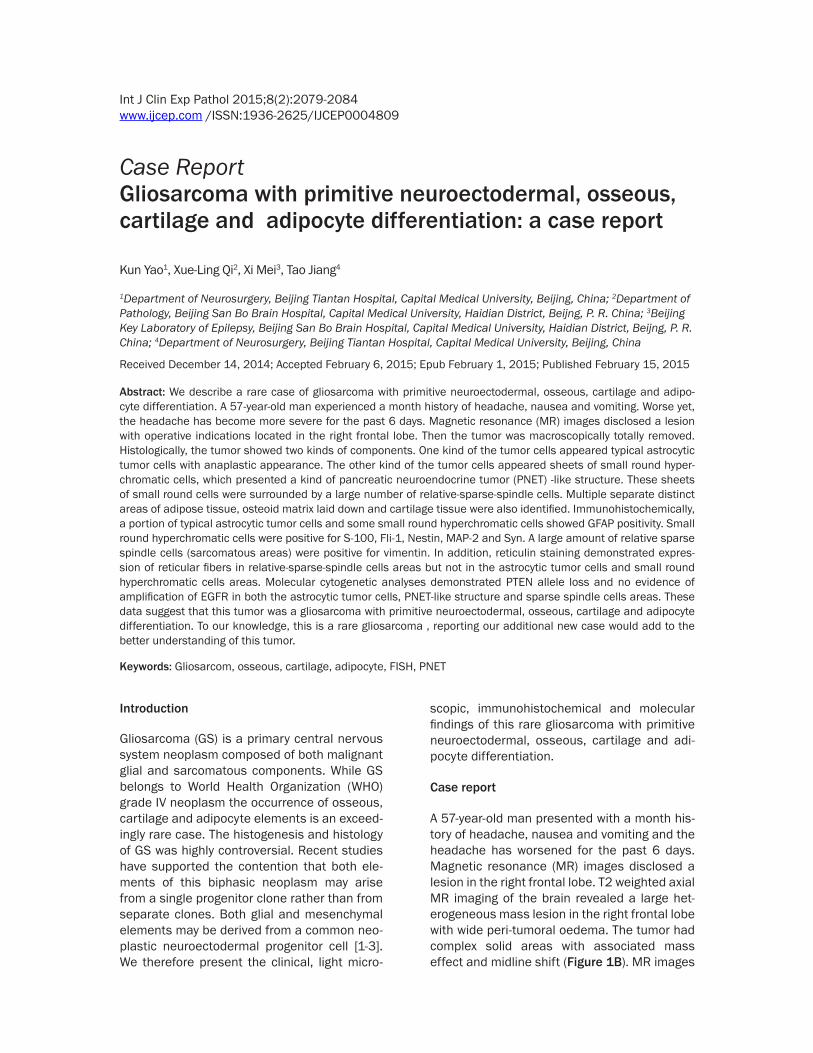
anaplastic appearance, high mitotic index, focal complex microvascular proliferation and geographic foci of necrosis (Figure 2A, 2B). Occasional prominent nucleoli and multinucle-ated giant cells were present (Figure 2C). The other kind appeared sheets of small round hyperchromatic cells with minimal cytoplasm and numerous mitoses oval (Figure 2D, 2E), which presents sort of PNET-like structure (2F), but was devoid of reticulin fibers. These cells were predominately arranged in sheets and nests, surrounded by relative sparse spindle cells. The spindle cells areas (sarcomatous) were with a large amount of thin reticulin fibers. Multiple separate distinct areas of adipose tis-sue (Figure 2G) osteoid matrix laid down (Figure 2H) and cartilage (Figure 2I) tissue were also identified. Their overall portion in the tumor tis-sue was less than 5%. These areas were sur-rounded by spindle cells (sarcomatous areas).
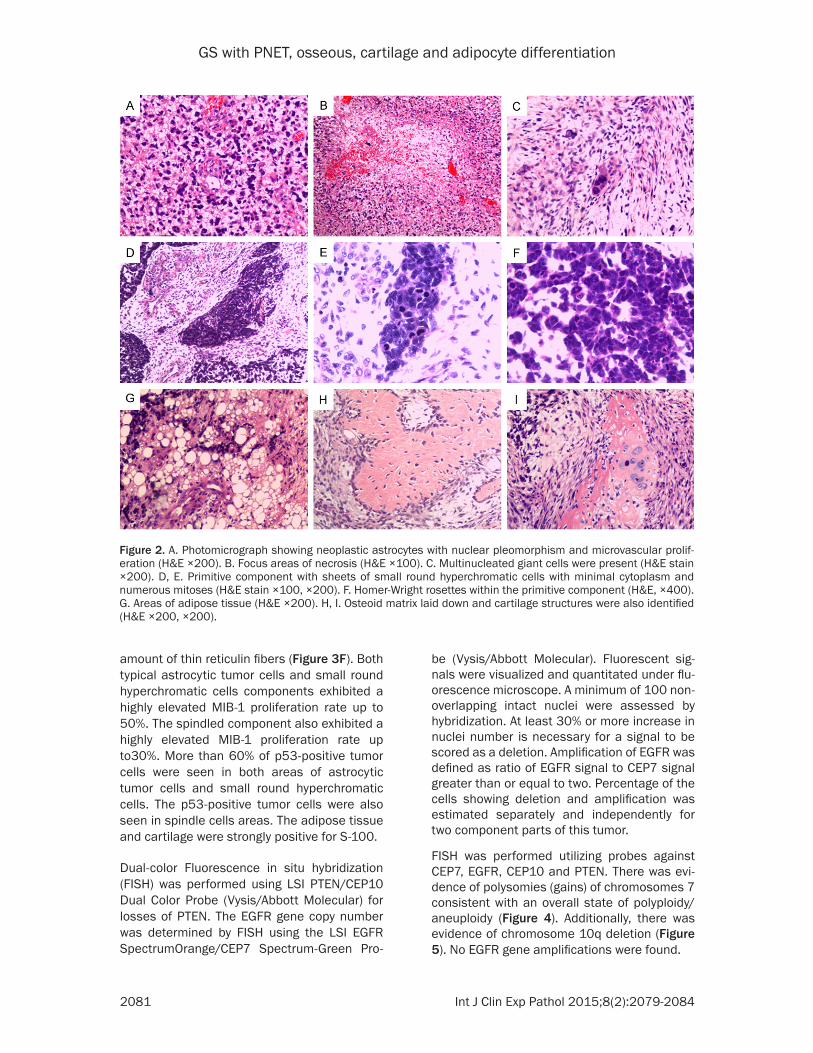
IHC staining demonstrated cytoplasmic expres-sion of GFAP in the typical astrocytic tumor cells portion and some small round hyperchro-matic cells portion (Figure 3A), but not in the relative-sparse-spindle cells areas. The astro-cytic tumor cells portion and small round hyper-chromatic cells portion were devoid of reticulin fibers (Figure 3B). The small round hyperchro-matic cells portion was immune-positive for S-100 (Figure 3C), Fli-1 (Figure 3D), MAP-2, Syn and Nestin. In addition, focal expression of EMA and pan-cytokeratin was also observed. No expression of pan-cytokeratin, desmin or glial markers was seen in spindle cells area. The spindled cells area (sarcomatous) was pos-itive for vimentin (Figure 3E), with a large
Figure 1. MR images disclosed a lesion in the right frontal lobe. A. MR images showed hypointense signal on T1-weighted MR images. B. T2 revealed a large heterogeneous mass lesion in the right frontal lobe with wide peri-tumoral oedema. C. The central part of lesion was observed on Gadolinium-enhanced T1 weighed MRI (axial).
GS with PNET, osseous, cartilage and adipocyte differentiation
2081 Int J Clin Exp Pathol 2015;8(2):2079-2084
amount of thin reticulin fibers (Figure 3F). Both typical astrocytic tumor cells and small round hyperchromatic cells components exhibited a highly elevated MIB-1 proliferation rate up to 50%. The spindled component also exhibited a highly elevated MIB-1 proliferation rate up to30%. More than 60% of p53-positive tumor cells were seen in both areas of astrocytic tumor cells and small round hyperchromatic cells. The p53-positive tumor cells were also seen in spindle cells areas. The adipose tissue and cartilage were strongly positive for S-100.
Dual-color Fluorescence in situ hybridization (FISH) was performed using LSI PTEN/CEP10 Dual Color Probe (Vysis/Abbott Molecular) for losses of PTEN. The EGFR gene copy number was determined by FISH using the LSI EGFR SpectrumOrange/CEP7 Spectrum-Green Pro-
be (Vysis/Abbott Molecular). Fluorescent sig-nals were visualized and quantitated under flu-orescence microscope. A minimum of 100 non-overlapping intact nuclei were assessed by hybridization. At least 30% or more increase in nuclei number is necessary for a signal to be scored as a deletion. Amplification of EGFR was defined as ratio of EGFR signal to CEP7 signal greater than or equal to two. Percentage of the cells showing deletion and amplification was estimated separately and independently for two component parts of this tumor.
FISH was performed utilizing probes against CEP7, EGFR, CEP10 and PTEN. There was evi-dence of polysomies (gains) of chromosomes 7 consistent with an overall state of polyploidy/aneuploidy (Figure 4). Additionally, there was evidence of chromosome 10q deletion (Figure 5). No EGFR gene amplifications were found.
Figure 2. A. Photomicrograph showing neoplastic astrocytes with nuclear pleomorphism and microvascular prolif-eration (H&E ×200). B. Focus areas of necrosis (H&E ×100). C. Multinucleated giant cells were present (H&E stain ×200). D, E. Primitive component with sheets of small round hyperchromatic cells with minimal cytoplasm and numerous mitoses (H&E stain ×100, ×200). F. Homer-Wright rosettes within the primitive component (H&E, ×400). G. Areas of adipose tissue (H&E ×200). H, I. Osteoid matrix laid down and cartilage structures were also identified (H&E ×200, ×200).
GS with PNET, osseous, cartilage and adipocyte differentiation
2082 Int J Clin Exp Pathol 2015;8(2):2079-2084
The morphological and immunohistochemical features are consistent with a GS with primitive neuroectodermal, cartilage and adipocyte diffe- rentiation.
Discussion
GSs are primary central nervous system neo-plasms composed of both malignant glial and sarcomatous components. Their histogenesis and histology have been highly controversial. It was first proposed by Feigin and Gross that the sarcomatous component arises from proliferat-ing tumor cells [4]. However, it has been shown that the EGFR gene, which is involved in cell proliferation control and amplification, occurs in approximately 40% of all glioblastomas with predominance for primary glioblastomas. Its expression seems to be mutually exclusive
from mutations in the TP53 tumor suppressor gene [5]. In contrast EGFR expression is not common in gliosarcomas, whereas mutations in the TP53 and PTEN genes are pre-dominantly observed [2]. Bier- nat et al. first proposed the monoclonal theory in GS, and his study demonstrated identi-cal p53 mutations in both tumor areas (gliomatous and sarcomatous areas) [6]. Sub- sequently, many studies found both components in GS sh- ared the similar genetic char-acteristics by comparative ge- nomic hybridization, FISH, cy- togenetic analysis and micro-satellite analysis [7]. Recent comparative genomic hybrid-ization studies have also sh- own similar genetic alterati- ons in both components, wh- ich strongly support the inter-pretation that both elements are derived from a common neuroectodermal progenitor [1-3]. The molecular genetic analyses displaying identical mutations in the PTEN and p53 genes favored a monoclo-nal origin [2, 6]. In our case, the mutations in PTEN and p53 genes were used to help diagnostic requirements. In
Figure 3. A. Immunohistochemistry for GFAP highlighting the neoplastic glial component (×100). B. Devoid of reticulin fibers in the astrocytic tumor portions and small round hyperchromatic portions (×100). C. The primitive component expressed S-100 (×200). D. The primitive component strongly expressed Fli-1 (×100), whereas the spindle cells areas (sarcomatous) and astrocytic elements were negative. E, F. GFAP negative spindle cells area (sar-comatous) expressed vimentin (×200) and showing reticulin fibres (×100).
this case the mutations in PTEN and p53 genes were found, but No EGFR gene amplifications were found. Immunohistochemical stains also help to delineate the biphasic nature of GS bet-ter. GFAP stains the glial component, whereas vimentin positivity is diagnostic for the spindled cells component (sarcomatous component).
In this case, the tumor presented the primitive neuroectodermal, osseous, cartilage and adi-pocyte elements primitive neuroectodermal all in one case of GS. Only few cases of gliosarco-ma with cartilage or chondroid differentiation have been reported in literature so far [8-10]. Cases of GS with PNET reported were even much less [11]. Some reports found that the presence of a PNET-like component in GS may reflect the capability of neuroectodermal pro-genitor cells to differentiate along multiple lines

GS with PNET, osseous, cartilage and adipocyte differentiation
2083 Int J Clin Exp Pathol 2015;8(2):2079-2084
[11] or may reflect a clonal proliferation of the stem/progenitor cell itself. Recent data showed that a cancer stem cell can be isolated even from conventional glioblastomas [1], which would be consistent with the latter hypothesis.
Some reports suggested the osseous compo-nent in GS may be unequivocally malignant [8-10]. It was demonstrated that neoplastic astrocytes are capable of differentiating into cartilage through mucopolysaccharide deposi-tion, which can evolve to form a chondroid matrix [12, 13]. In our case there was dominant morphological evidence of glioblastoma with PNET differentiation, with relatively sparse spindle cell (sarcomatous component) transfor-mation. There were also focal area of adipocyte tissues, area with osteoid matrix laid down and chondroid metaplasia areas. And the focal car-tilaginous components were completely sur-rounded by sarcomatous neoplastic tissue. The chondroid metaplasia areas and adipocyte tis-sues present had focal S-100 positivity.
It was considered the malignant potential of the tumor, the patient underwent radiotherapy and chemotherapy with temozolomide as adju-vant treatment. He has remained free of recur-rence for 11 months. We believe that this com-bination therapy is presently reasonable and appropriate.
In conclusion, we experienced a very rare GS case associated with a primitive neuroepitheli-al component, osseous, cartilage and adipo-cyte differentiation. It is possible that the primi-
tive neuroectodermal component seen in this tumor either reflects the capacity of the neo-plastic neuroectodermal progenitor cell or may represent a clonal proliferation of the progeni-tor cell itself. Generally speaking, it is possible that patients with PNET-like component may require altered, more aggressive treatment regimens. However, follow-up of additional cases is needed to definitely determine wheth-er the presence of this component significantly alters the already aggressive biology of GS in general. Reporting additional cases would be of great help in better understanding of the patho-genesis, clinical course and outcome of GS.
Acknowledgements
This work was supported by Beijing Postdoctoral Research Foundation (Grant No. 2013ZZ-22) and Capital Health Research and Development of special (Grant No. 2011-1020-01).
Disclosure of conflict of interest
None.
Address correspondence to: Dr. Tao Jiang, Depart- ment of Neurosurgery, Beijing Tiantan Hospital, Capital Medical University, Beijing, China. Tel: +861062856911; Fax: +86-10-62856901; E-mail: [email protected]
References
[1] Actor B, Cobbers JM, Buschges R, Wolter M, Knobbe CB, Lichter P, Reifenberger G, Weber RG. Comprehensive analysis of genomic alter-
Figure 4. FISH utilizing probes against the chromo-some 7 centromere (green) and the EGFR gene (red) yielded more than two signals for each in most tumor nuclei. No EGFR gene amplifications were found.
Figure 5. FISH utilizing probes against the PTEN (10q23; red) and CEP10 (green) genes yielded only one signal for each in most tumor nuclei. This is con-sistent with either a chromosome 10q deletion.
GS with PNET, osseous, cartilage and adipocyte differentiation
2084 Int J Clin Exp Pathol 2015;8(2):2079-2084
ations in gliosarcoma and its two tissue com-ponents. Genes Chromosomes Cancer 2002; 34: 416-427.
[2] Reis RM, Konu-Lebleblicioglu D, Lopes JM, Kleihues P, Ohgaki H. Genetic profile of gliosar-coma. J Neurosurg 2000; 156: 425-432.
[3] Boerman RH, Anderl K, Herath J, Borell T, John-son N, Schaeffer-Klein J, Kirchhof A, Raap AK, Scheithauer BW, Jenkins RB. The glial and mesenchymal elements of gliosarcomas share similar genetic alterations. J Neuropathol Exp Neurol 1996; 55: 973-981.
[4] Feigin IH, Gross SW. Sarcoma arising in glio-blastoma of the brain. Am J Pathol 1955; 31: 633-653.
[5] Watanabe K, Tachibana O, Sata K, Yonekawa Y, Kleihues P, Ohgaki H. Overexpression of the EGF receptor and p53 mutations are mutually exclusive in the evolution of primary and sec-ondary glioblastomas. Brain Pathol 1996; 6: 217-223.
[6] Biernat W, Aguzzi A, Sure U, Grant JW, Kleihues P, Hegi ME. Identical mutations of the p53 tu-mor supressor gene in the gliomatous and the sarcomatous components suggests a common origin from glial cells. J Neuropathol Exp Neurol 1995; 54: 651-656.
[7] Actor B, Cobbers JMJL, Buschges R, Wolter M,Knobbe CB, Reifenberger G, Weber RG. Comprehensive analysis of genomic altera-tions in gliosarcoma and its two tissue compo-nents. Genes Chromosomes Cancer 2002; 34: 416-427.
[8] Barresi V, Cerasoli S, Morigi F, Cremonini AM, Volpini M, Tuccari G. Gliosarcoma with features of osteoblastic osteosarcoma: a review. Arch Pathol Lab Med 2006; 130: 1208-1211.
[9] Charfi S, Ayadi L, Khabir A, Daoud E, Kallel R, Kharrat O, Mnif Z, Boudawara Z, Makni S, Bou-dawara T. Gliosarcoma with osteosarcomatous features: a short illustrated review. Acta Neuro-chir 2009; 151: 809-813.
[10] Alatakis S, Stuckey S, Siu K, McLean C. Gliosar-coma with osteosarcomatous differentiation: review of radiological and pathological fea-tures. J Clin Neurosci 2004; 11: 650-656.
[11] Dulai MS, Bosanko CM, Wang AM, Horoupian DS, Boodin S, Chen PY, Wilson JD. Mixed cystic gliosarcoma and primitive neuroectodermal tumor: a case report. Clin Neuropatho 2004; 23: 218-222.
[12] Kepes JJ, Rubinstein LJ, Chiang H. The role of astrocytes in the formation of cartilage in glio-mas. An immunohistochemical study of four cases. Am J Pathol 1984; 117: 471-483.
[13] Kishikawa M, Tsuda N, Fujii H, Nishimori I, Yo-koyama H, Kihara M. Glioblastoma with sarco-matous component associated with myxoid change. A histochemical, immunohistochemi-cal and electron microscopic study. Acta Neu-ropathol 1986; 70: 44-52.