case report congenital adrenal hyperplasia and … report congenital adrenal hyperplasia and enamel...
TRANSCRIPT
Case Report
Congenital adrenal hyperplasiaand enamel hypoplasia: case reportKerrod B. Hallett, MDSc, FRACDS Roger K. Hall, MDSc, FRACDS, FICD
Abstract
A female with congenitaladrenal hyperplasia and enameldefects involving the permanent maxillary incisors and allcanines and premolars received composite veneer splintoverlays under general anesthesia. Possible etiological fac-tors involved in the formation of the enamel defects andoverall case management is discussed. (P ediatr Dent 17:54-59, 1995)
C ongenital adrenal hyperplasia (CAH) andadrenogenital syndrome (AS) are terms usedto describe a group of rare autosomal recessive
medical conditions involving inborn errors of steroido-genesis.i, 2 Because of a lack of circulating cortisol,ACTH-mediated adrenal hypertrophy occurs, but theadrenal glands generally are incapable of secreting largequantities of steroids other than androgens. In the mostcommon form of CAH, the underlying abnormality inthe adrenal cortex is a deficiency of the enzyme 21-hydroxylase which results in a partial block of cortisol(glucocorticoid) and aldosterone (mineralocorticoid)biosynthesis. The diagnosis of CAH is readily con-firmed by elevated 17-hydroxyprogesterone in the se-rum and an excess of pregnanetriol in the urine. Theother adrenal enzyme defects, each with their owncharacteristic abnormalities, have been described pre-viously, i, 2 but comprise only 10% of remaining cases.
Females with the classic form of CAH are born withambiguous external genitalia and require reconstruc-tive surgical procedures for cosmetic reasons and tofacilitate normal reproductive function. The excess se-cretion of fetal androgens results in clitoral enlarge-ment and fusion of the labia causing genitalia that, inthe most extreme form, may be similar to those of themale with undescended testes. Both sexes undergoprecocious advance in somatic growth and progres-sive virilization in the female or incomplete masculin-ization in the male occurs. Gender confusion in af-fected females may develop from incorrect sexassignment and rearing. Pseudohermaphroditism maybe prevented by prenatal administration ofdexamethasone to the at-risk mother in the first trimes-ter of pregnancy to suppress the abnormal secretion of
androgens by the fetal adrenal gland.3 In addition, threeof four children are at risk for sudden death due to saltwasting and fluid loss, hypoglycemia, and systemicinfection unless hormone replacement therapy is com-menced early in infancy. Gluco- and mineralocorticoidreplacement therapy has been shown to correct the saltimbalance and ensure essential adrenal function dur-ing growth and maturation.4
The long-term use of replacement corticosteroidscan cause many side-effects,s often beginning soon af-ter therapy commences. In children, overall growthretardation, osteoporosis, impaired glucose tolerance,and increased susceptibility to infection are importantconsiderations. Of interest to the pediatric dentist is thepotential effect of corticosteroid therapy on calciumhomeostasis in general and permanent tooth develop-ment, particularly enamel protein matrix synthesis andmineralization.
Dental management of children with CAH requiresan individualized protocol for corticosteroid supple-mentation depending on their current replacement regi-men. Patients who have taken daily corticosteroid re-placement within the last year are at risk fromhypotensive crisis if they are not given supplementarycorticosteroids before and during periods of stress suchas dental procedures,s, 6
The purpose of this case report is to present a previ-ously unreported association of CAH and enamel hy-poplasia and an oral rehabilitation technique utilizingsectional arch splints to restore the affected dentition.
Case reportChief complaint and past history
AC, a 6-year 11-month-old female with salt-wastingCAH diagnosed at age 2 weeks, was referred by herendocrinologist to the Department of Dentistry, RoyalChildren’s Hospital, for initial assessment and man-agement of "terrible front teeth."
She was the only child of consanguineous parents ofLebanese background, born at term following a nor-mal pregnancy and vaginal delivery. Sex was indeter-minate until chromosome analysis confirmed 46 XXkaryotype. She was commenced on oral cortisone ac-etate at medical diagnosis and additional oral
54 American Academy of Pediatric Dentistry Pediatric Dentistry-17:1,1995

prednisolone at age 5 years 2 months. Her medicalhistory included multiple febrile episodes during earlyinfancy and childhood, recurrent otitis media, pooreating habits, vomiting, and diarrhea. Her develop-mental milestones were considered normal, but heightand weight were at or below the third centile through-out childhood.
Clinical examinationAC was timid and shy with extremely short stature
and a wasted appearance in general. Her weight was14.9 kg (3.5 kg below the third centile for her age) andher height was 109.0 cm (4 cm below the third centilefor her age). Vital signs were: pulse 127, blood pressure108/86, and temperature 36.7°C. She cooperated poorlyand her behavior further deteriorated during the initialconsultation and later investigations.
Facial proportionswere balanced and shehad a thin face with astraight profile and ageneral brachyce-phalic pattern (Fig 1).Periorbital and peri-oral pigmentation wasapparent with lowhairline, thick eye-brows, and upper lipfacial hair. Mandibularopening was withinnormal limits with nodeviation on openingor closure. She had amixed dentition thatwas advanced for herchronological age. Softtissues were withinnormal limits with nogingival pigmentationapparent. The gingivae
Fig 1. Frontal view of patient'sface at presentation showingperiorbital and perioralpigmentation, thick eyebrows,low hairline. were marginally in-
flamed due to poororal hygiene and erup-
tion of permanent incisors. All erupting permanentmaxillary incisor teeth were noted to have a general-ized thin, rough, hypoplastic enamel surface involvingthe entire crown (Fig 2). Both the permanent mandibu-lar incisors and first molars were unaffected, but themandibular incisal enamel appeared thin with accen-tuation of the mammelons. The remaining primary teethalso had a normal appearance and morphology exceptfor the canines, which may have been hypoplastic pre-viously as they were now heavily worn. Amalgam den-tal restorations were present on the interproximal sur-faces of maxillary primary molars and on the occlusalsurface of the mandibular right second primary molar.All remaining teeth appeared to be clinically sound.We assessed the occlusion as bilateral flush molar ter-minal plane with a normal anterior overjet and over-bite relationship. Both arches were mildly crowdedwith ectopic eruption of the incisors. A panoramic ra-diographic examination (Fig 3) revealed a chronologi-cally advanced, complete succedaneous dentition andperiapical pathology associated with pulpal necrosis
Fig 2. Frontal view of anterior teeth showing hypoplasticmaxillary incisors and thin mandibular incisors withaccentuated mammelons.
Fig 3. Panoramic radiograph showing dental development at age 7years 8 months, nonvital right mandibular second primary molar.
Fig 4. Steiner cephalometric analysis at age 7years 8 months showing Class II skeletalpattern. Cephalometric angles are SNA 89°,SNB 79°, ANB 10°, MP 25°, OP 14°,Maxillary incisor SN 100°, Mandibularincisor MP 96°, Interincisal angle 137°.
Pediatric Dentistry-17:1, 1995 American Academy of Pediatric Dentistry 55
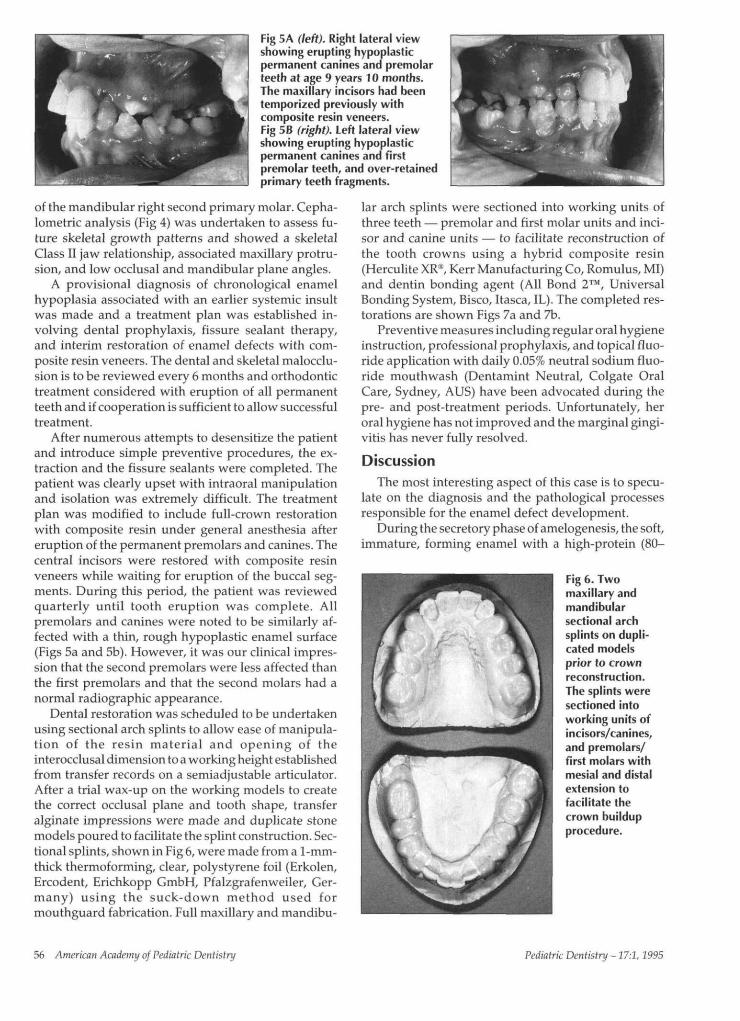
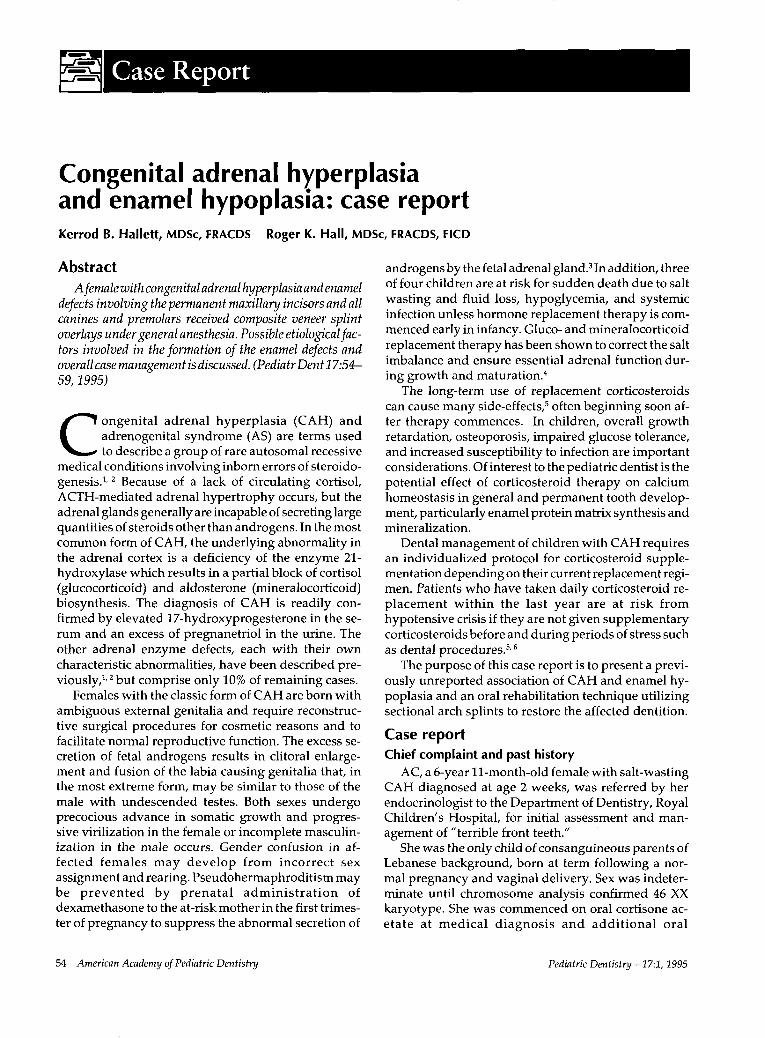
Fig 5A (left). Right lateral viewshowing erupting hypoplasticpermanent canines and premolarteeth at age 9 years 10 months.The maxillary incisors had beentemporized previously withcomposite resin veneers.Fig 5 B (right). Left lateral viewshowing erupting hypoplasticpermanent canines and firstpremolar teeth, and over-retainedprimary teeth fragments.
of the mandibular right second primary molar. Cepha-lometric analysis (Fig 4) was undertaken to assess fu-ture skeletal growth patterns and showed a skeletalClass II jaw relationship, associated maxillary protru-sion, and low occlusal and mandibular plane angles.
A provisional diagnosis of chronological enamelhypoplasia associated with an earlier systemic insultwas made and a treatment plan was established in-volving dental prophylaxis, fissure sealant therapy,and interim restoration of enamel defects with com-posite resin veneers. The dental and skeletal malocclu-sion is to be reviewed every 6 months and orthodontictreatment considered with eruption of all permanentteeth and if cooperation is sufficient to allow successfultreatment.
After numerous attempts to desensitize the patientand introduce simple preventive procedures, the ex-traction and the fissure sealants were completed. Thepatient was clearly upset with intraoral manipulationand isolation was extremely difficult. The treatmentplan was modified to include full-crown restorationwith composite resin under general anesthesia aftereruption of the permanent premolars and canines. Thecentral incisors were restored with composite resinveneers while waiting for eruption of the buccal seg-ments. During this period, the patient was reviewedquarterly until tooth eruption was complete. Allpremolars and canines were noted to be similarly af-fected with a thin, rough hypoplastic enamel surface(Figs 5a and 5b). However, it was our clinical impres-sion that the second premolars were less affected thanthe first premolars and that the second molars had anormal radiographic appearance.
Dental restoration was scheduled to be undertakenusing sectional arch splints to allow ease of manipula-tion of the resin material and opening of theinterocclusal dimension to a working height establishedfrom transfer records on a semiadjustable articulator.After a trial wax-up on the working models to createthe correct occlusal plane and tooth shape, transferalginate impressions were made and duplicate stonemodels poured to facilitate the splint construction. Sec-tional splints, shown in Fig 6, were made from a 1-mm-thick thermoforming, clear, polystyrene foil (Erkolen,Ercodent, Erichkopp GmbH, Pfalzgrafenweiler, Ger-many) using the suck-down method used formouthguard fabrication. Full maxillary and mandibu-
lar arch splints were sectioned into working units ofthree teeth — premolar and first molar units and inci-sor and canine units — to facilitate reconstruction ofthe tooth crowns using a hybrid composite resin(Herculite XR®, Kerr Manufacturing Co, Romulus, MI)and dentin bonding agent (All Bond 2™, UniversalBonding System, Bisco, Itasca, IL). The completed res-torations are shown Figs 7a and 7b.
Preventive measures including regular oral hygieneinstruction, professional prophylaxis, and topical fluo-ride application with daily 0.05% neutral sodium fluo-ride mouthwash (Dentamint Neutral, Colgate OralCare, Sydney, AUS) have been advocated during thepre- and post-treatment periods. Unfortunately, heroral hygiene has not improved and the marginal gingi-vitis has never fully resolved.
DiscussionThe most interesting aspect of this case is to specu-
late on the diagnosis and the pathological processesresponsible for the enamel defect development.
During the secretory phase of amelogenesis, the soft,immature, forming enamel with a high-protein (80-
Fig 6. Twomaxillary andmandibularsectional archsplints on dupli-cated modelsprior to crownreconstruction.The splints weresectioned intoworking units ofincisors/canines,and premolars/first molars withmesial and distalextension tofacilitate thecrown buildupprocedure.
56 American Academy of Pediatric Dentistry Pediatric Dentistry -17:1,1995

Figs 7 A (left), and 7B (right).Left and right lateral viewsof completed compositeresin splint restorationof incisor/canine andpremolar/molar teeth.
90% amelogenin, 10-20% enamelin), high water, andlow mineral content attains its full thickness, and thenthe protein framework is broken down by intrinsicprotease activity as secondary mineralization with hy-droxyapatite crystallites occurs. Initially, during pro-tein removal, considerable porosity occurs as matrix isreplaced by tissue fluid. Protein removal and mineral-ization may occur concurrently with matrix secretionand deposition as a continuum.7
A genetic factor responsible for the enamel defectwas difficult to investigate with no siblings and allimmediate family members in Lebanon. The unusualdistribution of the permanent enamel defects and theunaffected primary dentition make this etiologicalmodel unlikely, although the consanguinity of the par-ents must increase the potential for an autosomal re-cessive form of hypoplastic or hypocalcifiedamelogenesis imperfecta.
The possibility of factors operating within CAH it-self as the cause of the enamel defects in a mannersimilar to other inborn errors of metabolism such asgalactosemia, phenylketonuria, alkaptonuria, erythro-poietic porphyria, and hyperoxaluria was considered.Pindborg8 does not list CAH as a possible metaboliccondition in the development of enamel hypoplasia inhis review article of 140 causative factors, and to ourknowledge no other case reports have highlighted thisassociation. The unequal distribution of the defectsdoes not support a hypothetical metabolic influence,which would influence all permanent tooth formationequally. CAH is inherited as a monogenetic autosomalrecessive trait closely linked to the HLA major histo-compatibility complex on the short arm of chromo-some 6.2 Amelogenins comprise 80-90% of the imma-ture enamel protein matrix. Lau et al.9 have reportedthe mapping of the human amelogenin gene to thedistal short arm of the X chromosome and thepericentrometric region of the Y chromosome, whileSalido et al.10 have confirmed these genes to be tran-scriptionally active in developing human fetustoothbuds in the formation of enamel protein and crys-tallites during the secretory stage of tooth develop-ment. It is unlikely that CAH and amelogenin synthe-sis are genetically related.
Another differential diagnosis considered was chro-nological enamel hypoplasia due to a systemic insultaffecting the permanent maxillary incisor and all ca-
nine and premolar teeth during their critical period ofamelogenesis.11 Urinary infection, childhood viral ill-nesses, and poor nutritional intake have been postu-lated as possible etiological factors in the developmentof chronological enamel hypoplasia.8 This possibility issupported by: 1) the distribution of the defects in thiscase involving only those teeth in which enamel matrixsynthesis would normally have commenced from 5-6months in utero to 8 months after birth;7 2) a provenEscherichia coli urinary infection in the neonatal period;and 3) a postnatal history of recurrent febrile illness ofprobable viral etiology and poor nutrition intake.
Advanced tooth development and eruption in con-junction with advanced somatic bone maturation andmeasured cephalometric facial growth parameters asseen in this case have been studied in children withCAH.12 It is conceivable that the enamel matrix synthe-sis for the unaffected permanent mandibular incisorsand first molars — teeth that are known to commenceenamel protein synthesis at 3 1 /2 to 5 months in utero7
— was complete before birth and that these teeth wereunaffected by postnatal events. The pathogenesis isstill unclear, but it is presumed that an exanthematousfever or enteropathy may result in direct damage to theameloblasts, the supporting cells of the dental follicle,and their vascular supply, producing enamel defects.In addition, increased susceptibility to systemic infec-tion due to immunosuppression from long-term ste-roid replacement therapy5 would potentiate the likeli-hood of a medical insult producing chronologicalenamel hypoplasia.
An additional factor in the etiology of the enamelhypoplasia could be the direct effect of long-term cor-ticosteroids administration on tooth development.Microradiographic examination of the incisors of corti-sone-treated rats has shown deposition of intrapulpalcementum-like globules and frequent incremental lineswithin the dentin.13 These defects suggest that the min-eral content of dentin may be lower than normal, pos-sibly due to odontoblast disorganization or poor celldifferentiation during dentinogenesis. In a similar studyinvestigating cortisone-induced enamel hypoplasia,14
accentuated surface perikymata and closely apposedincremental lines were seen in enamel prismatic struc-ture. Other features included irregularly calcified,cementum-like globules within the dental follicle con-sisting of fine needle-like crystals smaller than those of
Pediatric Dentistry -17:1, 1995 American Academy of Pediatric Dentistry 57

normal enamel. This earlier work by Anneroth andBloom13 and Hall, 14 though limited, suggests a directinfluence of cortisone on odontogenesis and mineral-ization. The side effects of osteoporosis andhypocalcemia from long-term, high-dose corticoster-oid therapy described by several clinicians ~,ls and sug-gested by others, 16 and its subsequent effect on enameldevelopment require further laboratory investigationbefore a direct cause and effect relationship can bestated.
Current principles in the management of general-ized enamel defects such as amelogenesis imperfecta,stress the need for early interception and conservativerestoration of the affected teeth to prevent attrition.~7-21
The pediatric dentist must time intervention to thepatient’s current dental needs and maximize the futureprosthodontic options for definitive restoration. Here,this decision was further confounded by our patient’smedical, psychological, and behavior-managementproblems.
Interim restoration of affected permanent teeth withcomposite resin veneers for anterior teeth and stainlesssteel crowns for posterior teeth has been suggested byseveral authors. 17, 18 Early intervention is advised toprevent caries development, gingivitis, and occlusalattrition. 18 Of more importance to the patient is theimproved dental appearance and the reduced sensitiv-ity, which allows normal eating, drinking, and clean-ing. Strict dietary control of between-meal sugarysnacks and drinks, topical fluoride therapy with supple-mental fluoride tablets and fluoride toothpaste, andmeticulous oral hygiene has also been advocated toprevent further loss of already-compromised toothstructure. 18 In our case, the patient was anorexic andher diet mainly consisted of high-caloric supplementa-tion with carbohydrate-containing foods and drinks toencourage weight increase. She was poorly compliantwith oral hygiene measures but did use a fluoride tooth-paste and lived in an optimally fluoridated area. Un-fortunately, dental caries developed in the proximalsurfaces of the first molar and premolar teeth duringthe waiting period and the generalized marginal gingi-vitis did not resolve.
However, it was still considered appropriate to in-tervene when the permanent canines were fully eruptedto protect the dentition from dental caries and wear. Ahybrid composite resin was chosen for occlusal over-lay of the molar teeth and for crown buildup of theincisor, canine, and premolar teeth due to its estheticappearance and durability. Splinting the incisor andcanine teeth and both premolar and first molar teeth,should achieve sufficient strength and retention. Anesthetic and functional interim restoration will sufficeuntil definitive orthodontic, periodontic, andprosthodontic treatment~9-2~ can be undertaken at thecompletion of dental and facial development.
ConclusionThe etiology of the enamel defects must remain un-
certain. A coincidental autosomal recessive defect un-related to CAH may be present in this child with con-sanguineous parents. Chronological, systemicallymediated enamel defects also could have occurred dueto the multiple neonatal events and episodes of child-hood illness with associated hyperpyrexia and endo-crine and metabolic imbalance sustained in this child.The sparing of the permanent lower incisors and firstmolar teeth could be due to the accelerated dental de-velopment occuring in CAH patients.
Dr. Hallett was senior registrar, pediatric dentistry, and Dr. Halldirector and chief pediatric dental surgeon, Department of Den-tistry, Royal Children’s Hospital Melbourne, Australia, at thetime of this case report.
1. New MI, White PC, Pang S, Dupont B, Speiser PW: Thecongenital adrenal hyperplasias. In: The Metabolic Basis ofInherited Disease, 6th Ed. Scriver CR, Beaudet AL, Sly WS,Valle D, Eds. New York: McGraw Hill, 1989, pp 1881-1917.
2. White PC, New MI, Dupont B: Congenital adrenal hyper-plasia (1) and (2). N Engl J Med 316:1519-24,1580-86, 1987.
3. New MI: Prenatal diagnosis and treatment of adrenogenitalsyndrome (Steroid 21-hydroxylase deficiency). DevPharmacol Ther 15:200-10, 1990.
4. Klingensmith GJ, Garcia SC, Jones HW Jr, Migeon CJ, Bliz-zard RM: Glucocorticoid treatment of girls with congenitaladrenal hyperplasia: effects on height, sexual maturation,and fertility. J Pediatr 90:996-1004, 1977.
5. Scully C, Cawson RA: Complications of corticosteroidtherapy. In: Medical Problems in Dentistry, 2nd Ed. Bristol:Wright, 1987, pp 240-45.
6. Glick M: Glucocorticosteroid replacement therapy: a litera-ture review and suggested replacement therapy. Oral SurgOral Med Oral Pathol 67:614-20, 1989.
7. Hall RK: Developmental defects of tooth enamel. In: Pediat-ric Orofacial Medicine and Pathology, 1st Ed. London:Chapman and Hall, 1994, pp 10-11, pp 184-202, p 391.
8. Pindborg JJ: Aetiology of developmental enamel defectsnot related to fluorosis. Int Dent J 32:123-34, 1982.
9. Lau EC, Slavkin HC, Snead ML: Analysis of human enamelgenes: insights into genetic disorders of enamel. Cleft Pal-ate J 27:121-30, 1990.
10. Salido EC, Yen PH, Koprivnikar K, Loh-Chung Y, ShapiroL J: The human enamel protein gene amelogenin is expressedfrom both the X and the Y chromosome. Am J Hum Genet50:303-16, 1992.
11. Goodman AH, Armelagos GJ: The chronological distribu-tion of enamel hypoplasia in human permanent incisor andcanine teeth. Arch Oral Biol 30:503-7, 1985.
12. Speigel RN, Sather AH, Hayles AB: Cephalometric study ofchildren with various endocrine diseases. Am J Orthod59:362-75, 1971.
13. Anneroth G, Bloom G: Structural changes in the incisors ofcortisone-treated rats. J Dent Res 45:229-35, 1966.
14. Hall RK: Microradiographic study of induced enamel de-fects of rat molar enamel. J Dent Res (Abstr #2) 55:517, 1976.
15. Spiegel RJ, Vigersky RA, Oliff AI, Echelberger CK, Burton J,Poplack DG: Adrenal suppression after short term corticos-teroid therapy. Lancet 1:630-33, 1979.
16. Shusterman S, Fellers FX: The prevalence of enamel defectsin childhood nephrotic syndrome. ASDC J Dent Child36:435-40, 1969.
17. Rada RE, Hasiakos PS: Current treatment modalities in theconservative restoration of amelogenesis imperfecta: a casereport. Quintessence Int 21:937-42, 1990.
58 American Academy of Pediatric Dentistry Pediatric Dentistry- 17:1, 1995
18. Mackie IC, Blinkhorn AS: Amelogenesis imperfecta: earlyinterception to prevent attrition. Dent Update 18:79-80,1991.
19. Patel RA, Hovijitra S, Kafrawy AH, Bixler D: X-linked (re-cessive) hypomaturation amelogenesis imperfecta: prosthodontic, genetic, and histopathologic report. J ProsthetDent 66:398-402, 1991.
20.Wright JT, Waite P, Mueninghoff L, Sarver DM: Themultidisciplinary approach managing enamel defects. J AmDent Assoc 122:62-65, 1991.
21.Greenfield R, Iacono V, Zove S, Baer P: Periodontal andprosthodontic treatment of amelogenesis imperfecta: a clini-cal report. J Prosthet Dent 68:572-74, 1992.
Most childhood leukemia survivorsable to overcome school problemsDose of cranial radiotherapy andage of diagnosis big education-related risk factors
Most childhood survivors of acute lymph-oblastic leukemia overcome school problems eventhough they are more likely to enter a special educa-tion or learning disabled program, according toan article in a recent Journal of the AmericanMedical Association.
Riccardo Haupt, MD, Clinical EpidemiologyBranch, National Cancer Institute, Bethesda, Mary-land, Lonnie Zeltzer, MD, Department of Pediatrics,UCLA Medical Center, Los Angeles, California, andcolleagues analyzed data to determine the impact oftreatment on scholastic performance in the first co-hort of survivors of childhood acute lymphoblasticleukemia who are old enough to have completedtheir educational experience.
"This large study demonstrates that childhoodacute lymphoblastic leukemia survivors have a greaterlikelihood of being placed in special education orlearning disabled programs than their siblings, butthat most are able to overcome these problems. Doseof cranial radiotherapy and age at diagnosis are themost important education-related risk factors," theresearchers conclude.
The study consisted of 593 adult survivors ofchildhood acute lymphoblastic leukemia and 409sibling controls. Outcome measures included enroll-ment in special programs, grades during high school,
graduation from high school, college admission,and college graduation.
"Our findings confirm that survivors experi-ence some difficulties during the school years. Onaverage, leukemia survivors had lower grades,higher enrollment rates into special education orlearning disabled programs, and they spent a longertime in these programs. They were also at higherrisk of missing school for long periods and/or re-peating one year of school. On the other hand, ourdata show that most all survivors have rates of highschool graduation, college entry, and college gradu-ation that are similar to those of their brothers andsisters. Only survivors treated with 2,400 cGycranial radiotherapy (a relatively high amountof irradiation therapy treatment) and those diag-nosed at a preschool age were at a higher risk ofpoor educational performance and this groupshould be especially targeted for remediation," the
¯ authors write."Complications of treatment and the trauma of
having cancer itself may continue to exert an influ-ence well beyond the end of treatment. Time spentin the hospital or in an outpatient clinic reducesschool attendance, with a consequent potential re-duction in scholastic performance. Body changes,such as weight gain, hair loss, or growth deficits,have been reported to alter the patient’s self-es-teem, with diminished expectations and reducedschool performance."
Pediatric Dentistry - 17:1, 1995 American Academy of Pediatric Dentistry 59