case orthopaedic journal - university hospitals/media/uh/documents/for-clinicians/ortho...case...
TRANSCRIPT

Case Orthopaedic JournalVolume 4 Issue 1 | 2007
University Hospitals Case Medical Center
MetroHealth Medical Center
Louis Stokes VA Medical Center
University HospitalsAhuja Medical Center
Volume 9 | Issue 1 | 2012
ISSN 2324-8874Print

Department of Orthopaedics – Celebrating 106 Years of Innovation and Quality
© 2012 University Hospitals ORT 00067
This 106th year for the Department of Orthopaedics at University Hospitals Case Medical Center is proving to be another productive one, in terms of patient care, basic and clinical research and education. Through first-rate medical care, personalized attention and innovative scientific research with an unwavering sense of purpose, we continue to provide the best possible treatment for patients. This is reflected in our leadership in NIH funding to our primary affiliate relationship with Case Western Reserve University School of Medicine and our consistent ranking among the nation’s leading centers for orthopaedic care according to U.S.News & World Report.
Among the nation’s leading academic medical centers, University Hospitals Case Medical Center is the primary affiliate of Case Western Reserve University School of Medicine, a nationally recognized leader in medical research and education.
UH Case Medical Center is the 2012 recipient of the American Hospital Association–McKesson Quest for Quality Prize.
For more information, visit UHhospitals.org/ortho
University Hospitals Seidman
Cancer Center
UH Rainbow Babies &
Children’s Hospital
Center for Emergency Medicine and Marcy R. Horvitz Pediatric
Emergency Center
Case Western Reserve University School of Medicine
University Hospitals Samuel Mather
Pavilion
University Hospitals Alfred and Norma
Lerner Tower
Iris S. and Bert L. Wolstein Research Building –
Case Western Reserve University School of Medicine
University Hospitals Lakeside Hospital

Department of Orthopaedics – Celebrating 106 Years of Innovation and Quality
© 2012 University Hospitals ORT 00067
This 106th year for the Department of Orthopaedics at University Hospitals Case Medical Center is proving to be another productive one, in terms of patient care, basic and clinical research and education. Through first-rate medical care, personalized attention and innovative scientific research with an unwavering sense of purpose, we continue to provide the best possible treatment for patients. This is reflected in our leadership in NIH funding to our primary affiliate relationship with Case Western Reserve University School of Medicine and our consistent ranking among the nation’s leading centers for orthopaedic care according to U.S.News & World Report.
Among the nation’s leading academic medical centers, University Hospitals Case Medical Center is the primary affiliate of Case Western Reserve University School of Medicine, a nationally recognized leader in medical research and education.
UH Case Medical Center is the 2012 recipient of the American Hospital Association–McKesson Quest for Quality Prize.
For more information, visit UHhospitals.org/ortho
University Hospitals Seidman
Cancer Center
UH Rainbow Babies &
Children’s Hospital
Center for Emergency Medicine and Marcy R. Horvitz Pediatric
Emergency Center
Case Western Reserve University School of Medicine
University Hospitals Samuel Mather
Pavilion
University Hospitals Alfred and Norma
Lerner Tower
Iris S. and Bert L. Wolstein Research Building –
Case Western Reserve University School of Medicine
University Hospitals Lakeside Hospital

TSRH® 3Dx™
Spinal Instrumentation
Open MASTTLIF/PLIF
Degen ScoliosisSpondylolisthesis Scheuermann’s
What’s new in Spinal Fixation?
IRN
1012
2-1.
0-03
/109
To learn more about TSRH®3Dx™ Spinal Instrumentation call (800) 933-2635 or visit us online at www.medtronic.com.
CAPSTONE® PEEK Spinal System incorporates technology developed by Gary K. Michelson, MD.
26280 TSRH 3Dx Ad - 7x4_875.indd 1 9/26/11 1:14 PM

ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 5
Editorial Staff
Editors-in-ChiefErik Schnaser, MD Troy Mounts, MD
Senior EditorsLorraine Stern, MD- AdvertisingJonathan Macknin, MD-Copy Editing
Junior EditorsJonathan Streit , MDAshraf youssef, MDChristopher Bechtel, MDMichael Reich, MDChristina Cheng, MDAndrew Chen, MD
Faculty Editors
Randall Marcus, MDJ. Robert Anderson, MDEdward Greenfield, PhDShana Miskovsky, MD
Ellen GreenbergerSecretary
Phyllis LieAccounting
CONTENTS
Dedication to Barbara Peterson Ruhlman- Erik Schnaser, MD ........................................................ 6Letter from the Editor-in-Chief ............................................................................................................ 7year in Review Chairman’s Report- Randall Marcus, MD .................................................................................... 8 MetroHealth Medical Center Annual Report- Daniel Cooperman, MD .................................. 12 Louis Stokes Cleveland Department of veteran Affairs Orthopaedic Surgery Service Annual Report- Glenn Wera, MD ........................................................................................ 14 Research Section of the Department of Orthopaedic Surgery at Case Western Reserve
University School of Medicine- Edward Greenfield, PhD ................................................. 15 The Education Committee Update- James Learned, MD and Scott Kling, MD ...................... 16 The Harry E. Figgie III, MD Professorship .................................................................................. 17 The New Center for Joint Replacement & Preservation .......................................................... 18 ABC Traveling Fellowship ............................................................................................................ 19 Physician-in-training Fitness Center ........................................................................................ 20 Retirements Bob Boscarelli ....................................................................................................................... 21 Daniel Cooperman, MD ....................................................................................................... 22 Tommy Washington ............................................................................................................ 23 Photos from Throughout the year ............................................................................................. 24 University Hospitals Attendings ................................................................................................ 31 MetroHealth Attendings ............................................................................................................. 32 Basic Science Faculty ................................................................................................................... 33 vAMC Attendings ......................................................................................................................... 34 Ahuja Attendings ......................................................................................................................... 35 Current Residents ........................................................................................................................ 36 Incoming Intern Class of 2017 ............................................................................................................ 38 Awards and Recognitions ........................................................................................................... 39Manuscripts Culturing Stem Cells to Achieve Physiological Contexts and to Maximize Clinical Relevance ......................................................................................................................... 40 Iatrogenic Subtrochanteric Femoral Fracture ................................................................................43 Emergent Surgical Management for Spinal Metastases and Neurologic Deterioration ...... 49 Fibroblast Growth Factor Receptor 3 Signaling in Skeletal Dysplasia ........................................55 Mesenchymal Stromal Cells and their Orthopaedic Applications........................................... 60 Is Aseptic Loosening Mediated by Tirap/Mal? Future Research Goals ......................................66visiting Professors ............................................................................................................................... 69Obituaries ............................................................................................................................................. 74Exiting Residents Future Plans .......................................................................................................... 752012 Fellowship Match Results ......................................................................................................... 76Instructions for Authors ...................................................................................................................... 77

6
We are proud to introduce the ninth edition of the Case Orthopaedic
Journal. Every year, in our preproduction editorial meeting, the first topic of conversation is about the Journal’s dedication. We try to select an individual who inspires unrivaled patient care, has had a positive impact on the resident experience, and is a role model for the Department. This year, the editorial staff—comprised of past and present Allen Fellows—had a very easy decision. Because of her profound impact on University Hospitals and the University Hospitals Department of Orthopaedics for decades, we have chosen to dedicate this year’s Journal to Mrs. Barbara Peterson Ruhlman. Mrs. Ruhlman has tirelessly dedicated her time and energy to University Hospitals’ mission - To Heal, To Teach, and To Discover. She implements these values in her everyday life and inspires others to do the same.
Mrs. Ruhlman began volunteering in high school delivering gifts to the mothers and new babies in the original Lakeside
Labor & Delivery ward. She continued her volunteer work by later tending to the reception desk in MacDonald House. Her commitment to University Hospitals has continued to evolve and grow. She now serves on the Orthopaedic Leadership Council and the Development Committee of the University Hospitals Board of Directors.
In her early thirties, Mrs. Ruhlman was diagnosed with osteoarthritis and she has been a patient of Dr. Goldberg, Dr. Marcus, and Dr. Kraay. She owes her mobility to the “excellent” orthopaedic care that she has received. “I owe so much to the Orthopaedic team for all of the work they have done to keep me moving,” says Mrs. Ruhlman. “They keep me on my feet!”
This year, Mrs. Ruhlman generously supported the inaugural Barbara Peterson Ruhlman Chair in Orthopaedics. This chair is now held by Dr. Patrick Getty, the Director of Musculoskeletal Oncology Division in our Department. Dr. Getty’s
excellent care of patients and dedication to teaching has been and will continue to be an inspiration to us all. He is truly a selfless and deserving clinician. We thank Mrs. Ruhlman for her time, dedication, and generosity, and present this Journal in her honor.
Thank you,
Erik A. Schnaser, MD
DEDICATION TO BARBARA PETERSON RUHLMAN
Mrs Ruhlman with Drs Getty & Schnaser in the Ruhlman Conference Center. She was very surprised and delighted when we informed her of the Journal’s dedication.
Mrs. Barbara Peterson Ruhlman
Mrs Ruhlman volunteering at University Hospitals
ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 7
We have revamped many rotations in the residency to accommodate the evolving landscape of the Case Orthopaedics program. With the leadership of James Learned MD and Scott Kling MD, we have significantly improved upon the residency recruitment process in order to continue attracting top candidates from around the country. I would like to thank James and Scott for their hard work and dedication in this process.
Lastly, I would like to thank the past and present editorial board—comprised of past and present Allen Fellows—for their help in putting this year’s Journal together. The publication of this periodical is never a small undertaking and your help is greatly appreciated.
Thank you,
Erik A. Schnaser, MD Editor-in-Chief
Troy I. Mounts, MDEditor-in-Chief
It is with great pleasure that we introduce the 2012 Case Orthopaedic Journal. This will be the ninth publication of the Journal. With the encouragement of Dr. Richard A. Brand, we have elected to apply for MEDLINE® indexing. The National Library of Medicine uses an NIH-chartered committee, the Literature Selection Technical Review Committee (LSTRC), to review all new biomedical and health journal titles and recommend those to be indexed for MEDLINE®. About 5,000 titles are indexed and included in the MEDLINE® database. The LSTRC meets three times a year and considers approximately 140 titles at each meeting. As an important first step in the process, we have applied for and received an ISSN number from the U.S. Library of Congress (ISSN 2324-8874 (Print) & ISSN 2324-8882 (Online)). We are hopeful that the Journal will be selected and should hear back from the LSTRC later this year.
There have been several exciting developments in the Department of Orthopaedics this year. Notably, the Department has added new clinical faculty, opened the Center for Joint Replacement & Preservation, continued to be highly ranked by U.S. News and World Report in both adult and pediatric orthopaedics, and maintained the tradition of recruiting highly talented new residents to the program.
LETTER FROM THE EDITORS-IN-CHIEF
Erik A. Schnaser, MD
Troy I. Mounts, MD

8
I am delighted to introduce the 2012 volume of the Case Orthopaedic Journal, which highlights the outstanding achievements of the Department of Orthopaedics at Case Western Reserve University School of Medicine. The Department continues its ranking as one of the top orthopaedic departments in the United States, and we take great pride in the outstanding achievements and excellent work carried out during the past year by our clinicians, scientists, residents and staff.
The Department of Orthopaedics at Case Western Reserve University consists of four medical centers, our research laboratories and, most importantly, the outstanding people who have earned our reputation for excellence. Our medical centers include:
• University Hospitals Case Medical Center, which includes Rainbow Babies and Children’s Hospital,
• MetroHealth Medical Center, our Level I trauma hospital,
• Louis Stokes Veterans Administration Medical Center here on our Case Western campus, and
• University Hospitals Ahuja Medical Center and attached orthopaedic musculoskeletal center.
Our basic science laboratories are located:
• in the School of Medicine, with our Molecular Biology division in the Biomedical Research Building,
• in the Case Western Reserve School of Engineering, in the Musculoskeletal Mechanics and Materials Laboratory, and
• at MetroHealth Medical Center and the veterans Administration Medical Center, where our Functional Electrical Stimulation Laboratories are located.
• Additionally, our Anatomic Research Laboratory resides in the Cleveland Museum of Natural History, the home of the Hamann-Todd bone collection.
Medical Center and Medical School Achievements
This year marked the opening of our new Center for Joint Replacement & Preservation floor at University Hospitals Case Medical Center. The floor was designed in consultation with our orthopaedic surgeons and our patients. Uniquely, the entire $3 million renovation was funded by generous donations from our faculty, from the Orthopaedic Leadership Council and from grateful patients and foundations. The Center includes a unique insulation and sound-
abatement design that offers patients more of a hotel rather than a hospital experience. This experience includes an individualized nurse silent-electronic-call system and the use of special materials chosen for both their beauty and sound-absorbing properties. There is a specialized orthopaedic physical therapy satellite center built into the patient floor, which provides for state-of-the-art physical therapy and rehabilitation as well as privacy for the patients. The floor also incorporates a unique, specialized air-filtration system to reduce infection risk, as well as a specialized floor design
CHAIRMAN’S REPORT AND HIGHLIGHTSRandall E. Marcus, MDCharles H. Herndon Professor and Chairman, Department of OrthopaedicsCase Western Reserve University School of Medicine and University Hospitals Case Medical Center
Randall E. Marcus, MD
yEAR IN REvIEW

ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 9
with no steps, ledges or other possible impediments that might impair the safety of our patients. Dr. Matthew Kraay, Director of our Joint Replacement Division, did an outstanding job leading this effort which has provided our patients with a state-of-the-art facility.
U.S. News & World Report once again ranked Case Western Reserve University School of Medicine in the “Best Medical Schools” in America, and University Hospitals Case Medical Center is ranked among America’s 50 Best Hospitals in all 12 methodology-ranked specialties, including Orthopaedics (#20). Our medical center is now in the prestigious group of only 13 hospitals in the United States to rank among the nation’s best in all 12 of the methodology-ranked specialties. This stands out from a field of nearly 5,000 that U.S. News included in its ranking. Furthermore, University Hospitals Case Medical Center received the 2012 American Hospital Association-McKesson Quest for Quality Prize as the nation’s top hospital for leadership innovation in quality improvement and patient safety. Our medical center is the first large urban academic medical center to receive this prestigious national award, which represents the highest honor for hospital quality. UH Case Medical Center’s medical intensive care unit again achieved a Silver Beacon Award for Excellence from the American Association of Critical Care Nurses. University Hospitals Rainbow Babies & Children’s Hospital was rated as one of the “Best Children’s Hospitals in America,” and was ranked in all pediatric specialties, including Pediatric Orthopaedics (#10). University Hospitals Rainbow Babies & Children’s Hospital has been re-certified as a Level I pediatric trauma center, the highest distinction granted by the American College of Surgeons. The only Level I pediatric trauma center in Northern Ohio, our dedicated full-service children’s hospital
has provided exceptional trauma care for the critically ill and injured children for over a century.
UH Ahuja Medical Center placed 12th in Soliant Health’s annual national poll naming the top 20 most beautiful hospitals in the United States for 2012. Soliant described the new Ahuja Medical Center as “a true showpiece of modern architecture, blended with masterfully landscaped surrounding grounds.” Becker’s Hospital Review named University Hospitals Case Medical Center as one of the “100 hospitals with great orthopaedic programs.” Their citation noted:
“The surgeons focus on adult and pediatric extremities care, joint preservation, cartilage restoration, spine care, sports medicine, total joint replacement and orthopaedic oncology. The physicians also have a focus on research and have been supported by the National Institutes of Health. Past research projects include working on cartilage and bone cell biology, tissue engineering, biomechanics and functional electrical stimulation. Spine surgeons are able to perform minimally invasive surgical techniques and care for patients with traumatic and degenerative disorders. US News & World Report ranked the hospital among the top 20 in the country for orthopaedics in 2011-12.”
Departmental Achievements
The Department’s excellence in clinical activities was once again recognized by U.S. News & World Report, which ranked us as one of the top orthopaedic departments in the country (#20), and Pediatric Orthopaedics placed #10. Our national leadership in musculoskeletal research was again confirmed by our continued ranking in the top-funded orthopaedic departments in the United States by the National Institutes of Health (NIH, #14).
Our residency program received over 600 applications this year for our 6 residency positions, and the Department matched 6 of our top selections. We welcome to the program Dr. Andrew Chen from the University of North Carolina; Dr. Ronak Desai from Rush Medical Center; Dr. Sheeba Joseph from Case Western Reserve University School of Medicine; Dr. Adrienne Moraff from the University of Maryland School of Medicine; Dr. William Morris from the University of Texas Southwestern School of Medicine and Dr. Sunny Patel from Case Western Reserve University School of Medicine. The Trauma Fellow, based at MetroHealth Medical Center, is Dr. Jeffrey S. Earhart from Northwestern University Medical Center in Chicago, and our Joint Replacement Fellow is Dr. Warakorn Jingjit from Ching Mai, Thailand. The two Allen Research Fellowships for this year were awarded to Dr. Christina Cheng, working in the Biomedical Engineering Lab under the mentorship of Dr. Eben Alsberg, and Dr. Andrew Tsai, working in the Musculoskeletal Materials and Mechanics Lab under Dr. Ozan Akkus.
YEAR IN REVIEW

10
We also welcomed a new faculty member this year, Dr. Blaine T. Bafus, who joined the faculty as a hand surgeon at MetroHealth Medical Center. He completed his orthopaedic residency at the University of Michigan and his hand fellowship at the Combined Cleveland Clinic MetroHealth Medical Center Program.
The Department was once again selected by the American Orthopaedic Association to host the American-British-Canadian (ABC) Traveling Fellows. The Department played host to Drs. Piers J. Yates, MBBS, BSc, MRCS, FRCS, FRACS, from Perth, Australia; James S. Huntley, MA, DPhil, MB, from the Royal Hospital for Sick Children, Glasgow, Scotland; Michael R. Reid, MD, FRCS, Northumberland, United Kingdom; Catherine F. Kellett, FRCS, BM BCh, BSc, Perthshire, United Kingdom, Duncan Whitwell, BMedSci, BMBS, FRCS, Nuffield Orthopaedic Center, Oxford, England; Gordon Beadle, MB ChB, FRACS, Christchurch, New Zealand; and Christian H. Snyckers, MBChB, MMed, Pretoria, South Africa. During their 3-day visit, there were excellent educational and entertaining academic programs, which included presentations by the ABC Traveling Fellows and the CWRU faculty, as well as a visit to the Hamann-Todd Skeletal Collection hosted by Dr. Daniel Cooperman and Dr. Raymond Liu. Once again, this excellent traveling fellowship provided an outstanding opportunity to exchange ideas and develop new friendships.
Congratulations to Faculty Members and Residents
On June 21, 2012, Edward M. Greenfield, PhD, was installed as the inaugural holder of the Harry E. Figgie III, MD, Professorship in Orthopaedics at Case Western Reserve University. Dr. Greenfield, who is the Director of Research in the Department of Orthopaedics at Case Western Reserve University, is also the Director of our NIH Training Program in Musculoskeletal Research. Dr. Greenfield received his PhD at the University of North Carolina at Chapel Hill and his postdoctoral fellowship at Washington University in St. Louis before joining the CWRU faculty. His research interests focus on orthopaedic implants, orthopaedic infections, osteosarcoma and skeletal response to hormones and have resulted in more than 60 scientific publications. Professor Greenfield has received both the William Harris Award and the Kappa Delta Award for his research on orthopaedic implants. The Harry E. Figgie III, MD, Professorship in Orthopaedics was established by the Figgie Foundation to honor the academic excellence and dedication exemplified by their son’s career in medicine. Dr. Figgie, who died in 1999, received his medical degree and completed his orthopaedic residency here at Case Western Reserve University. Following a fellowship at the Hospital for Special Surgery in New york, Dr. Figgie served on the faculty here at University Hospitals Case Medical Center from 1985 to 1993.
Also in June, Patrick J. Getty, MD, was installed as the inaugural holder of the Barbara Peterson Ruhlman Professorship in Orthopaedics. Dr. Getty is the Director of the Musculoskeletal Oncology Service at University Hospitals Case Medical Center, and also serves as the Program Director of the Case Western Reserve University Orthopaedic Residency. He received his medical degree at the University of Chicago, where he also completed both his orthopaedic residency and musculoskeletal tumor fellowship. Dr. Getty is an Associate Professor of Orthopaedic Surgery at Case Western Reserve University and has been recognized for his clinical, educational and research accomplishments. These two new endowed professorships join the Herndon Professorship, the Heiple-Lennon Professorship, the Bohlman Professorship, the Clyde “Les” Nash Professorship and the Hansjoerg Wyss Professorship, for a grand total of 7 in our Department at Case Western Reserve University School of Medicine.
Dr. Glenn Wera, Assistant Professor of Orthopaedic Surgery and the Director of the Orthopaedic Service of the Cleveland v.A. Medical Center, received an OREF OMeGA Grant to fund our Joint Replacement Fellowship, and Dr. Patrick Getty received an OREF Research Residency Grant through the Clinician Development Program in support of our residency research component. Kingsbury G. Heiple, MD, Emeritus Professor and former Chairman of the Department of Orthopaedic Surgery at Case Western Reserve University, was recognized for his contributions to the Orange High School Adult Education Program, where he oversees adult woodworking classes. Dr. Michael Reich received the Baxter young Investigator Award for his research as an Allen Fellow under the mentorship of Dr. Ozan Akkus in the Musculoskeletal Materials
CHAIRMAN’S REPORT

ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 11
YEAR IN REVIEW
and Mechanics Laboratory. Dr. Reich’s research also received recognition by a Resident Research Grant from AO North America for his project “Sterilization of Bone Allografts by Chemical Crosslinking with Genipin.” This research resulted in a patent application by Drs. Akkus and Reich. Dr. Jonathan Streit received second place in the Cleveland Orthopaedic Research Society’s Barry Friedman Resident Research Award for his project “Acetabular Wear Patterns in Individuals with Different Types of Cam Deformity of the Proximal Femur.” Dr. Erik Schnaser received the American Orthopaedic Association/Orthopaedic Research and Education Foundation Resident Leadership Award. Ms. Ellen Greenberger, Resident Coordinator for the Case Western Reserve University Orthopaedic Residency Program, received an award from University Hospitals Case Medical Center for her 35 years of excellent service.
This year’s chief residents who graduated in June were another outstanding class. They are advancing on to Fellowships in their subspecialty areas of choice, and we welcome them into the Case Western / Charles Herndon Alumni Association and wish them all the best in their future careers:
• Michael Abdulian, MD – Sports Medicine, University of Southern California Medical Center, Los Angeles, California
• Kasra Ahmadinia, MD – Spine Surgery, Rush Medical Center, Chicago, Illinois
• Zachary Gordon, MD – Spine Surgery, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania
• Ari Levine, MD – Trauma, Carolinas Medical Center, Charlotte, North Carolina
• Daniel Master, MD – Hand Surgery, Stanford University Medical Center, Palo Alto, California
• James Murphy, MD – Reconstruction and Joint Replacement, University of Pennsylvania Medical Center, Philadelphia, Pennsylvania
Once again, it has been a privilege to lead this fabulous Orthopaedic Department in its 105th year. This year’s report highlights the high-quality work that typifies the faculty, residents and staff of this outstanding Department.
12
The orthopaedic faculty and staff at the MetroHealth Medical Center
provide Northeast Ohio with terrific surgical and medical care. Medical students, residents and fellows come to Metro from the Case Western Reserve University School of Medicine and the Cleveland Clinic’s Lerner College of Medicine. They enjoy an amazing opportunity to improve the health of patients, while they learn the art and science of orthopaedic surgery from experts.
Our primary research focus is acute trauma care and rehabilitation. Dr. Heather vallier was recently awarded a grant from the NIH to study early appropriate trauma surgery. This prospective study of the multiply injured patient monitors a host of physiologic markers in an attempt to delineate the best way to manage the first few days in the life of the trauma victim. The study is being done in concert with General Surgery as well as our new department of Neurosciences.
Our rehabilitation efforts continue to focus on the benefits of functional electrical stimulation. Basic science teams lead by Drs. Hunter Peckham and Ron Triolo interface with Orthopaedic, Neurosurgical and vascular physicians to search for ideal approaches to leveraging “high tech” for the benefit of our patients with spinal cord injuries.
UPDATE FROM METROHEALTH Daniel R. Cooperman, MDvice Chairman of Orthopedic Surgery, MetroHealth Medical Center
Dr. Jack Wilber, the Hansjoerg Wyss Professor of Orthopaedic Traumatology, still leads our traumatology group, which includes himself, Drs. Brady, Patterson, Sontich, vallier and Roger Wilber. Jack just completed his term as President of AO North America. He was recently elected to the AOvA, which is the Board of Directors of the AO Foundation. Dr. Roger Wilber is active in teaching through the AO institute and is especially active in the care of patients with complex pelvis and acetabular pathology.
Dr. John Sontich, the President elect of the Ohio Orthopaedic Society, is the “go-to-guy” for infections, non-unions and malunions because of his mastery of both internal and external fixation techniques. Additionally, through his work with the Limb Lengthening and Reconstruction Society, he is directing education and research in circular frames at a national level.
Dr. Heather vallier, the Clyde L. Nash Professor of Orthopaedic Education, continues her active efforts in teaching, clinical care and research. The Orthopaedic Learning Center, which she and Dr. Nash created, provides learners with 24/7/365 access to extensive information concerning trauma care.
Dr. Megan Brady is developing a general orthopaedic trauma practice. Additionally, she has developed a separate clinic to manage fractures that occur in the elderly.
Daniel R. Cooperman, MD
Dr. Daniel Cooperman continues in his role as Interim Chairman of the Department of Orthopaedic Surgery at MetroHealth. At this time, an active search for a new Department Chairman is unfolding. We anticipate that a new chairman will be seated by the beginning of 2013.

ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 13
YEAR IN REVIEW
Dr. Patterson continues teaching the residents about fractures, total joint arthroplasty, and life. Also, he is the director of surgical care at Metro. As director, he identifies and facilitates synergies between General Surgery, Orthopaedic Surgery, the Department of Neurosciences and Oral Surgery that allow Metro surgical patients to flourish.
This year, the Hand and Upper Extremity Service added Dr. Todd Bafus to the faculty. Originally from the Pacific Northwest, he graduated from the University of Michigan orthopaedic surgery program. Residency was followed by 3 years as an orthopaedic surgeon for the United States Air Force which involved deployment to the Air Force Theater Hospital in Iraq where he cared for both US and Coalition forces in a combat setting. After that, he completed the Cleveland Combined Hand Fellowship. His wife is a local plastic surgeon and they are both looking forward to long and productive careers in Cleveland. Dr. Bafus will develop a Hand and Upper Extremity practice in concert with our Metro faculty and will also serve as the Chief of Upper Extremity Surgery at the Louis Stokes vA Hospital. Drs. Michael Keith, Harry Hoyen, Kevin Malone and Stephen Lacey continue to provide the highest level of care to their patients and provide terrific resident education. Additionally, under the leadership of Dr. Michael Keith and Dr. Harry Hoyen, and with the indispensable help of the basic science aces, this group is creating motion and function for patients with spinal cord
injury.
Our Spine Team is headed by Dr. Tim Moore and supported by Dr. Clyde Nash. Dr. Moore is an integral part of our Orthopaedic program and is an essential member of MetroHealth’s newly formed Department of Neurosciences. Also, he teaches at the OTA basic fracture course for residents.
This year, Dr. Christina K. Hardesty joined the Rainbow Babies and Childrens Hospital faculty. She comes to Metro part-time. She did her orthopaedic residency at the University of Arkansas and then completed the Rainbow Pediatric Orthopaedic fellowship. Following that, she did a mini-fellowship at the Dupont Institute focusing on the care of children with neuromuscular diseases. Drs. Dan Cooperman and George Thompson continue to provide Pediatric Orthopaedic care at Metro, as they have for 25 and 33 years, respectively. Dr. Raymond Liu has an active part-time practice at Metro. He has a general practice in Peds Ortho as well as a special focus on complex bony
deformity and limb length inequality.
Dr. John Feighan is the Chief of the Foot and Ankle Service. The service manages a wide variety of post-traumatic, degenerative and sports-related injuries. Residents learn modern techniques, both closed and surgical, for managing foot and ankle pathology.
Working at Metro continues to be a pleasure. We have a wonderfully complementary group of physicians and staff, with a remarkably simple mission, help people get healthy. Under Dr. Patterson’s direction, we do that. At times, we face challenges in our effort to provide the best possible care to everyone who presents to our hospital. Overcoming the challenges is worth the effort.
14
The orthopaedic surgery section at the Cleveland veterans Affairs Medical
Center (vAMC) has continued to flourish in response to unprecedented clinical demand and institutional support.
This year I am happy to welcome new faculty members to the staff: Mike vento MD (general orthopaedic surgery consultant) and Todd Bafus MD (hand surgery staff). Dr. vento is a graduate of the Case Western Reserve University Orthopaedic Surgery residency. Dr. Bafus is a graduate of the University of Michigan orthopaedic surgery residency. After having practiced with the US Air Force in Balad, Iraq and Travis Air Force Base in California, Dr. Bafus completed the Cleveland Clinic Combined Hand fellowship in 2012. These new additions allow us to address ongoing demand in upper extremity surgery and general orthopaedic clinic.
I am proud of the contribution provided by our established faculty including Thomas McLaughlin MD (sports medicine, arthroscopy), Patrick Getty MD (orthopaedic oncology), J “Rob” Anderson MD (Hand & Upper Extremity), Randall Marcus (adult reconstruction, foot & ankle), victor Goldberg MD (adult reconstruction, total joints), and John Makley MD (orthopaedic oncology). I am especially appreciative of Robert Gillespie MD (shoulder & elbow) and Steven Fitzgerald MD (adult reconstruction, total joints) who have increased our arthroplasty capacity in
2011-2012 LOUIS STOKES CLEvELAND DEPARTMENT OF vETERANS AFFAIRS MEDICAL CENTER ORTHOPAEDIC SURGERy SERvICE ANNUAL REPORTGlenn Wera, MDChief, Orthopaedic Service Louis Stokes Cleveland vAMC
the last academic year. We are grateful for ongoing clinical support from our two physician assistants: Greg Field PA-C and Terry Bauer PA-C. In addition, the administrative support provided by Barbara Dennstedt RN-BSN and Carliss Towns RN-MSN has improved our efficiency and patient relations. I am happy to welcome Carliss Towns back from a recent Military Deployment to Al Asad, Iraq where she served as Lt. Colonel Officer in Charge (OIC). On the basic science level, Ron Triolo PhD has had a strong presence in FES, Spinal Cord Injury and the Advanced Platform Technology Center. Likewise, Kath Bogie DPhil has been a leading researcher in wound prevention and treatment in paralyzed individuals.
This year the section bid farewell to Richard Grant MD (adult reconstruction) who performed a great deal of arthroplasty cases, especially total knee replacements. We wish him well in his new leadership position in Philadelphia. We also wanted to acknowledge the hard work of Stephanie Stiner RN-BSN who is now in the section of general surgery. We also wanted to thank Fred Cason MD for his strong support of veterans orthopaedic care during his tenure as Chief of Surgery. We wish him well in his home town of Kansas City.
The current Residency Training Program
Glenn Wera, MD
is divided into two rotations each with a PGy-5 chief resident and PGy-3 resident. Their time is split roughly 50/50 between outpatient clinics and surgical services. In the 2011-2012 academic year we performed over 6900 outpatient clinic visits, 571 extremity, and 2 spinal operative cases. This productivity represents a 1.5% increase in office volume and 15% increase in extremity surgery due to more focused and efficient practice patterns.
ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 15
YEAR IN REVIEW
I am delighted that this issue of the COJ is dedicated to Barbara Ruhlman.
Mrs. Ruhlman has always been a huge advocate for our department. It was particularly gratifying for me when Patrick Getty was named the inaugural holder of the Barbara P. Ruhlman Chair in Orthopaedics as Patrick has been incredibly valuable during the last few years as we established a research program focusing on osteosarcoma.
Each year, two of our residents are selected as Allen Fellows, who join a research lab for a full-time, year-long, experience. The 2012-2013 Allen Fellows are Christina Cheng, MD and Andrew Tsai, MD. Christina is working with Eben Alsberg in the Biomedical Engineering Department on cartilage tissue engineering and Andrew is working with Ozan Akkus in the Department of Mechanical and Aerospace Engineering on a subtrochanteric fracture project that is a collaboration with Dr. Marcus. We are proud to be one of the four institutions that received a Research Residency Grant from the OREF to support Christina’s and Andrew’s research. Next year’s Allen Fellows will be Adrienne Moraff, MD and William Morris, MD, who are currently deciding on their mentors and projects.
RESEARCH SECTION OF THE DEPARTMENT OF ORTHOPAEDICS AT CASE WESTERN RESERvE UNIvERSITy SCHOOL OF MEDICINE Edward Greenfield, PhD, Director of ResearchHarry E. Figgie III MD Professor of OrthopaedicsDepartment of Orthopaedics, Case Western Reserve University
The 2012 Allen Fellows Society visiting Professor was Gary Friedlander, MD, who is the Chairman of Orthopaedic Surgery at yale University. Gary’s talks were on the use of growth factors to increase fracture healing.
Since last year’s COJ, three new trainees have joined the CWRU/NIH Musculoskeletal Training Grant. Lindsay Bashur, PhD is a post-doctoral trainee working on novel pathways that regulate mesenchymal differentiation with Guang Zhou, PhD, in our department. Francesca Scrimieri, PhD is also a post-doctoral trainee. She’s working on the role of vCAM in osteosarcoma with Alex Huang, MD, PhD in the Pediatric Hematology/Oncology Division. Daniel Alt is a MD, PhD student, who is also working with Eben Alsberg in the Biomedical Engineering Department on cartilage tissue engineering. The training grant is planning on hosting a Northeast Ohio Musculoskeletal Research Retreat in April 2013. We are looking forward to excellent oral and poster presentations from all of the institutions in the area with the long-term goal of increasing interactions and fostering new collaborations.
Finally, I’d like to express my deepest gratitude to the Figgie Family for their continued support of our department and, in particular, for establishing the Harry E. Figgie III, MD Professorship that I am honored to hold. We had a wonderful celebration of the professorship this summer where our faculty reminisced about Harry with his family, Dean Davis, and President Snyder.
Edward Greenfield, PhD
16
The Education Committee is made up of two fourth-year and two fifth-year
residents, as well as faculty members from all three of our teaching hospitals. With a mission to ensure that residents receive the best education possible, we meet monthly to help our training evolve as fast as the ever-changing field of Orthopaedic Surgery.
This year, we have made some big changes to the resident rotations. With feedback from faculty, recent graduates and current residents, we determined that residents needed more education in the still-growing field of Sports Medicine. With Dr. Cooperman’s retirement from practice at Rainbow Babies and Childrens Hospital, there was a fourth-year resident available for the new-and-improved Sports Service. We think that the new rotations will be a huge success.
Thank you,
James Learned, MDScott Kling, MDSenior Education Committee Representatives
Lorraine Stern, MD Jonathan Belding, MD Junior Education Committee Representatives
THE EDUCATION COMMITTEE UPDATEJames Learned, MD Scott Kling, MD
New RotationsJoints: PGy-4, PGy-3, PGy-1Spine: PGy-4, PGy-2Pediatrics: PGy-4, PGy-2, PGy-1Tumor/Basic Science: PGy-4Metro Hand: PGy-4Sports: PGy-4, PGy-2Foot/Ankle: PGy-3UH Hand: PGy-3vA: PGy-5, PGy-5, PGy-3, PGy-3MHMC: PGy-3, PGy-2, PGy-2, PGy-1Fracture: PGy-2
Previous RotationsJoints: PGy-4, PGy-3, PGy-1Spine: PGy-4, PGy-2Pediatrics: PGy-4, PGy-4, PGy-2Tumor/Basic Science: PGy-4Metro Hand: PGy-4Sports: PGy-3Foot/Ankle: PGy-3UH Hand: PGy-3vA: PGy-5, PGy-5, PGy-3, PGy-3MHMC: PGy-3, PGy-2, PGy-2, PGy-2Fracture: PGy-2
Resident Education Committee Representatives Scott Kling, Lorraine Stern, and James Learned.
Resident Education Committee Representative Jonathan Belding
ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 17
YEAR IN REVIEW
THE HARRy E. FIGGIE III, MD PROFESSORSHIP IN ORTHOPAEDICS
We would like to congratulate Edward M. Greenfield, PhD for
being appointed the inaugural Harry E. Figgie Professorship in Orthopaedics. The celebration for Dr. Greenfield and Harry E. Figgie took place on June 21, 2012.
The Harry E. Figgie III, MD Professorship in Orthopaedics was established by The Figgie Foundation to honor the academic excellence and dedication exemplified by their son’s career in medicine. The endowed Figgie Professorship supports in perpetuity the legacy of the late Dr. Harry E. Figgie, III by advancing the valuable clinical achievement, medical education, and research in arthritis and joint replacement that were central to his professional medical life and interests.
Dr. Figgie, who passed in 1999, was an alumnus of Hawken School and obtained his undergraduate degree in biomedical engineering and industrial engineering at Rensselaer Polytechnic Institute. He went on to Case Western Reserve University
School of Medicine, earning a medical degree in 1979. He was then accepted into the orthopaedic residency program at Case Western Reserve , following which he was invited to join the UH staff and School of Medicine faculty as an orthopaedic surgeon with a specialty in joint replacement. After a very successful medical career, Dr. Figgie turned to his other lifetime passion, industrial entrepreneur, joining his father, the late Harry E. Figgie Jr. as vice-Chairman of Technology and Strategic Planning for Figgie International, Inc.
In addition to his commitment to the medical and corporate worlds, Dr. Figgie was an avid sportsman. He excelled in a range of athletics; including football, baseball, and tennis. He is survived by his daughters Susan and Katie, and his son, Harry Iv.
Edward M. Greenfield PhD is a Professor of Orthopaedics and Pathology at Case Western Reserve University. He is also Director of Research in the Department of Orthopaedics at Case Western Reserve and is Director of the CWRU/NIH Training program in Musculoskeletal Research.
Dr. Greenfield is a graduate of New College in Sarasota, Florida. He completed his PhD at the University of North
Carolina at Chapel Hill and a post-doctoral fellowship at Washington University in St. Louis before joining the CWRU faculty.
His research interests focus on orthopaedic implants, orthopaedic infections, osteosarcoma, and skeletal responses to hormones. He has published more than 60 scientific publications. Professor Greenfield has received both the William Harris Award and the Kappa Delta Award for his research on orthopaedic implants. His research wisdom as well as his life and career advice has had a profound impact on undergraduate students, graduate students, and fellows.
Case Western Reserve University School of Medicine gratefully acknowledges the generous decision of the Figgie Family to make a gift through the Figgie Foundation that will significantly enhance the development of medical knowledge in orthopaedics that will lead to improved patient care.
Dr Edward M. Greenfield PhD
Drs Marcus & Greenfield with the Dean of the Medical School, Pamela Davis, MD, PhD.
Dr Figgie (front row) with past and present Case Western Orthopaedics Faculty
Harry E. Figgie III, MD

18
In June 2012, the Department of Orthopaedic Surgery opened the Center for Joint Replacement & Preservation at
University Hospitals Case Medical Center, bringing together a 105-year-legacy of surgical expertise and a patient care unit especially designed to meet the unique needs of patients undergoing total joint replacement (TJR) and joint preservation surgery. Although joint replacement has been the long-term focus of our program, this new venture has created a comprehensive program, that in addition to TJR, offers our patients access to innovative biologic and joint preserving techniques for joint related problems including hip arthroscopy, FAI surgery, pelvic and knee osteotomy, and cartilage transplantation. The nine high-volume orthopaedic surgeons who make up the joint replacement and joint preservation team have completed fellowships at some of the world’ s top medical centers and can provide our patients – regardless of age - with the full spectrum of joint replacement and joint preserving procedures.
An important aspect of the new UHCMC Center for Joint Replacement & Preservation was the redesign of the patient care environment and refinement of the process of how patient care is delivered, based on input from our patients, surgeons and other caregivers. The new Center – which can accommodate 30 patients at a time – was designed to be a quiet, peaceful, and bright environment that promotes a feeling of wellness and looks and feels more like a boutique hotel than an acute care hospital. To help patients better understand the importance of their role in the healing process, a comprehensive educational program is offered prior to
surgery. Throughout their entire episode of care, patients are cared for by a dedicated staff that is specially trained in treatment of patients undergoing major joint reconstructive surgery.
Research has shown that hospitals with high-volume joint replacement programs and high volume surgeons have better outcomes with fewer complications than lower volume hospitals. Under the leadership of Dr. Matthew J. Kraay , the Center for Joint Replacement & Preservation perform nearly 4,000 joint replacement and preservation procedures each year, one of the highest volumes in Ohio and the U.S. UH Case Medical Center has previously been recognized as a HealthGrades® Specialty Center of Excellence for joint replacement and has one of the lowest complication rates in the country.
Continually improving patient safety, surgical outcomes and patient satisfaction are the key goals of the center. The Centers Multidisciplinary Performance Improvement Committee is dedicated to the process of continuous quality improvement and continually tracks and analyzes complications, quality metrics and
outcomes, and establishes targets for improvement. The committee is comprised of surgeons, nurses, administrators, physical therapists, anesthesiologists, infectious diseases specialists and members of the hospital’s Quality Committee. Since its opening in June 2012, The UHCMC Center for Joint Replacement
& Preservation has received JCAHO subspecialty certification for both hip and knee replacement.
When joints replacements fail or wear out, and must be revised, the UHCMC Joint Replacement faculty is helping to advance the science of joint replacement by determining why these implants failed. The “UHCMC/CWRU Center for Evaluation of Implant Performance” is one of the largest implant retrieval programs in the U.S., and has received more than 10 million dollars in NIH funding over the last decade. This program is an internationally recognized collaboration between the Division of Joint Reconstruction and Arthritis Surgery at UHCMC, and the Department of Mechanical and Aerospace Engineering(MAE) at CWRU. Our program, which is co-directed by Clare M. Rimnac, PhD, Chair of MAE at CWRU and Dr. Kraay, has expanded over the last several years to include nearly a dozen other leading academic medical centers and universities in the U.S.
The information on all joint replacement implants retrieved at UHCMC is linked to a computerized clinical “registry” of all patients undergoing hip or knee replacement surgery at UHCMC since 1985. This extensive clinical research database is an important part of our Center for Evaluation of Implant Performance and provides us with clinical data on both failed, and perhaps more importantly, successful implants and procedures.
Joint ReplacementMatthew Kraay, MS, MD Director, Division of Joint Reconstruction and Arthritis Surgery, UH Case Medical Center Kingsbury G. Heiple and Fred A. Lennon Professor of Orthopaedics, Case Western Reserve UniversityRandall E. Marcus, MD Charles H. Herndon Professor and Chairman, Department of Orthopaedics, UH Case Medical Center/Case Western Reserve University School of MedicineWilliam Petersilge, MDGlenn Wera, MD Roger G. Wilber, MD Steven Fitzgerald, MD
Joint PreservationDonald Goodfellow, MD Michael J. Salata, MDBrian victoroff, MD
THE NEW CENTER FOR JOINT REPLACEMENT & PRESERvATION
The nine surgeons that make up the Joint Replacement and Preservation Center. Left to Right:Brian victoroff, Michael Salata, Donald Goodfellow, Matthew Kraay, William Petersilge, Steven Fitzgerald, Glenn Wera, Roger Wilber, & Randall Marcus
ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 19
YEAR IN REVIEW
Case Western University’s Department of Orthopedics was selected to be
one of the hosts to the 2012 American Orthopaedic Association’s (AOA) American-Bristish-Canadian (ABC) Traveling Fellowship. Lectures were given by the ABC Fellows and CWRU Faculty.
Case Western Reserve University Medical Center Program Date: June 21-22, 2012.
2012 American-British-Canadian Traveling Fellows
Gordon Beadel, MB ChB, FRACS-Christchurch, New Zealand (musculoskeletal oncology, hand & upper limb surgery, general trauma)
James S. Huntley, MA Jons MCh, DPhil, MB BChir- Royal Hospital for Sick Children Glasgow, Scotland (pediatric orthopaedics)
Catherine F. Kellett, FRCS, BM BCh, BSc-Perthshire, Unitied Kingdom (primary and revision hip & knee arthroplasty)
Michael R. Reed, MD, FRCS-Northumberland, United Kindom (hip & knee arthroplasty)
Christian H. Snyckers, MBChB, MMed
Duncan Whitwell, BMedSci, BMBS, FRCS- Nuffield Orthopaedic Center, Oxford, England (orthopaedic oncology)
Piers J. yates, MBBS, BSc, MRCS, FRCS, FRACS-Perth Australia (hip & knee surgery, trauma surgery)
AOA-ABC TRAvELING FELLOWSHIPCase Western Reserve University Medical Center Program
Piers J. yates, MBBS, BSc, MRCS, FRCS, FRACS-“Resurfacing Indications from the Australian Registry”
James S. Huntley, MA Jons MCh, DPhil, MB BChir- “ Mosaicplasty- Living and Dying on the Edge (Cartilage Repair)”
Michael R. Reed, MD, FRCS- “Infection Prevention in Joint Replacement”
Raymond Liu, MD- “An Anatomic Study of the Epiphyseal Tubercle and its Significance in the Pathogenesis of Slipped Capital Femoral Epiphysis”
Michael Salata, MD- “Hip Arthroscopy: Current Concepts”
Duncan Whitwell, BMedSci, BMBS, FRCS- “ A Girdlestone in Oxford?- Options to Reconstruct Severe Bone Loss Around the Hip/Pelvis”
Steven Fitzgerald, MD- “ Identification of Oral Bacterial DNA in Synovial Fluid of Patients with Arthritis with Native and Failed Prosthetic Joints”
Catherine F. Kellett, FRCS, BM BCh, BSc- “Cadaveric Surgery versus Anatomical Dissection: Trial of a Novel Approach to Clinical Anatomy for Medical Undergraduates”
Glenn Wera, MD-“ Predictors of Range of Motion in Patients Undergoing Manipulation Under Anesthesia Following TKA”
Edward Greenfield, PhD- “Novel Concepts of Aseptic Loosening of Prosthetic Joints”
Gordon Beadel, MB ChB, FRACS- “Early Outcome Results in Treatment of GCT of Bone from Two New Zealand Bone Tumour Centers”
Robert Gillespie, MD- “ Open Revision Surgery for Recurrent Should Instability”
Christian H. Snyckers, MBChB, MMed- “Conversion of External Fixation to Internal Fixation in a Non-acute Reconstructive Setting”
The 2012 AOA-ABC HostsUniversity of Western OntarioMayo ClinicUniversity of MinnesotaUniversity of ChicagoNorthwestern UniversityLoyola UniversityUniversity of Iowavanderbilt UniversityCampbell ClinicWashington UniversityCleveland ClinicCase Western ReserveUniversity of Pittsburgh
Further information on the program can be obtained @ http://www.aoassn.org/programs/traveling-fellowships/american-british-canadian-(abc).aspx
Dr Cooperman discussing orthopaedics and life with the Fellows.
Doctors Kraay, Marcus, and Cooperman enjoying dinner with the Fellows.

20
The “PIT”“When you realize the value of life, you dwell less on what is past and concentrate more on the preservation of the future.” Dian Fossey
In the act of providing excellent patient care it is my strong conviction that we physicians set the example for our patients by not losing sight of “self-care.” Approximately three years ago, I had a vision for University Hospitals; I wanted to improve the achievability of wellness not only for my patients but also among my colleagues by providing an in-house fitness center. With funds provided by the Association of Residents and Fellows (ARF) and the unanimous backing of the Graduate Medical Education Committee (GMEC), the “Physician-in-training Fitness Center” opened last spring. It is an easily accessible 24-hour access gym within the confines of University Hospital walls. Affectionately nicknamed the “PIT” and located in the space once occupied by our Emergency Department, University Hospitals now boasts six-hundred square feet of rubber, mirrors and steel. The gym provides a cardio room, 24 hour card swipe access, 10,000 pounds of free weights, an in-network computer, flat screen Tv and much more.
Preventive medicine is dependent upon a conscious informed respect of self-care, the strength of will to pursue it, and the availability of the necessary tools to achieve it. University
Hospitals is currently taking active strides in the pursuance of preventive medicine among both its patients and employees rewarding active participation in one’s own healthcare in the form of “Wellness Credits”. By providing easy and affordable access to the necessary tools for realizing one’s wellness goals this effort not only encourages but enables true active reform. This wonderful new addition to University Hospitals, allows its house staff to take the first steps towards achieving a new self.
I would like to thank Dr. Fred Rothstein President of University Hospitals, and GMEC for their support, the ARF for providing the funds and Dr. Randall E. Marcus, Chairman of the Department of Orthopaedics, for his encouragement and support. “Only one who devotes himself to a cause with his whole strength and soul can be a true master. For this reason mastery demands all of a person.” – Albert Einstein
– Troy Isaac Mounts MD
PHySICIAN-IN-TRAINING FITNESS CENTER

ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 21
On February 15, 2013 Bob Boscarelli will retire after 24 years at University
Hospitals. After receiving his training at Cleveland Community College and spending a few years at Lutheran Hospital and MetroHealth, Bob joined the operating rooms at UH as a surgical technologist in 1989. At this time, technology was changing rapidly and the department of Orthopaedic Surgery was growing.
Bob soon found himself working predominantly on the Orthopaedic cases and in particular with Drs Goldberg and Bohlman. Under these great surgeons, Bob thrived and soon became not only an integral part of the team but also a major factor in the growth and success of the surgical service. His quiet competence, professionalism and dedication particularly suited him for this position. He could always be depended upon to be completely ready to take on even the most challenging of surgery and surgeon.
He often stayed on well past his shift to help complete a surgery for the benefit of the patient. He remained calm and in control even under the most stressful conditions and was capable of quickly adapting to the needs of the surgeon and the patient. He has been a willing and capable teacher to everyone in the surgical suite including the techs , nurses, residents and the surgeons.
After Bob’s retirement he will be able to spend more time with the other passions in his life including his family, cooking and baseball. His wife Carol has recently retired from MetroHealth so they will be able to spend more time together with their grandchildren. Though Bob will be missed, he will certainly not be forgotten since he has left such a lasting memory with all who have worked with him.
We all wish him the very best in his retirement and sincerely thank him for his years of service and friendship.
– Jack Wilber, MD
RETIREMENTS
Bob Boscarelli
Bob Boscarelli
YEAR IN REVIEW
22
It is an honor and a pleasure to write this article on Daniel R. Cooperman,
MD, who retired from the Department of Orthopaedic Surgery on December 31, 2012 after 25 years of service. He received his undergraduate degree from Dartmouth in 1969 and his Doctor of Medicine from the University of Chicago in 1974. His orthopaedic residency was also at the University of Chicago, which he completed in 1980. During his residency he spent one year as a fellow at the Karolinska Institute in Stockholm, Sweden. Following residency, Dr. Cooperman did a Pediatric Orthopaedic fellowship at Newington Children’s Hospital (1981-1982) in Newington, CT. He returned to the faculty at the University of Chicago from 1982 to 1987 before being recruited to Case Western Reserve University, University Hospitals of Cleveland, and Rainbow Babies and Children’s Hospital in 1987.
During Dr. Cooperman’s 25 years of service he rose to the rank of Professor of Orthopaedic Surgery. He was the Director of the Pediatric Neuromuscular Rehabilitation Program in the Division of Pediatric Orthopaedic Surgery at Rainbow Babies and Children’s Hospital and finished his career as the Interim Chair at MetroHealth Medical Center (2011-2012). Next year will join the clinical faculty at yale University. His wife, Dr. Mariel Harris, has accepted a position as the Chief of Palliative Care at Bridgeport Hospital, a major affiliate of yale University. Dr. Harris is an internist, lawyer and a geriatrician. Her interest in palliative care made her a highly sought after individual. Naturally, he will accompany her in this new adventure.
Dr. Cooperman’s career interests have been in pediatric orthopaedics, particularly trauma, neuromuscular disorders, as well as in the natural history of untreated musculoskeletal disorders. The Hamann-Todd Osteological Museum at the Cleveland Museum of Natural History has been his major focus for the past 10 years. He has encouraged and directed many of our residents and faculty in performing research projects on the specimens. He has published numerous peer-reviewed studies and chapters while on our faculty and delivered many local, state, national and international lectures. Dr. Cooperman has had a lifelong interest in resident education. He particularly relished his role in assisting residents with low Orthopaedic In-Training Examination (OITE) scores prepare for and ultimately, pass their American Board of Orthopaedic Surgery (ABOS) examination. He has been a lifetime member of the Department’s Education Committee. Twice the residents voted him the Outstanding Teacher in our Department (1996 and 1999).
Dr. Cooperman will truly be missed. He is an outstanding Pediatric Orthopaedic Surgeon, educator, leader and my personal friend. He is one of the most intelligent individuals I have ever known. The Department and the Division of Pediatric Orthopaedics wish him well in his new career at yale University.
– George H. Thompson, MD Director, Pediatric Orthopaedics
Daniel R. Cooperman, MD
Daniel R. Cooperman, MD
RETIREMENTS

ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 23
Tommy Washington
Tom Washington retired on December 31, 2012, from the Department of
Orthopaedics. When I thought about words that could best describe him during the almost forty years that I worked with him, these came to mind: dependable, loyal, patient, thoughtful, educator and team player. Tom came to work at University Hospitals in 1966 in the supply department. Shortly thereafter, he was drafted into service and served a year in vietnam. After his military service, he returned to University Hospitals, initially in the supply department, but in 1971, when an opening in the Department of Orthopaedics was available as a technician, he applied and was appointed by the Department Chair, Dr. Herndon, as a member of Mary Daunt’s team. Tom was a quick learner and absorbed Mary’s extensive knowledge of orthopaedics. He truly appreciated the patience and education he received from Dr. Herndon and Mary. As part of the team he was always there to help and support the attendings and residents in their mission of outstanding patient care. Most importantly, his thoughtfulness, loyalty, patience and team building was evident in his teaching of many generations of residents in the “ins and outs” of traction and cast application. He was always a dependable steady hand in the operating room even under the most trying circumstances.
When Mary retired, he became the leader of the orthopaedic technician team. His quiet management was evident in the day to day activities of the group. He truly enjoyed teaching the younger technicians and watching them grow and become independent. His knowledge and patience created an outstanding team and
workplace to care for orthopaedic patients. Daryl Clinkscales, one of his colleages, describes him as a “good guy”. He will be missed, but we all can take solace in knowing that his legacy of orthopaedic education and service will be carried on by the scores of residents and present and future orthopaedic technicians.
We wish him well in his retirement, and his new activities focused on giving back to his community.
- victor Goldberg, MD
Dr Marcus and Mr Tommy Washington
Mr Tommy Washington
Residents and Ortho Techs celebrate Mr Washington’s tenure with the Department.
YEAR IN REVIEW
24
2012 Graduation Dinner/ Dance
1st Row: Christina Cheng, Andrew Tsai, Cynthia Nguyen, Kingsbury Heiple, James Murphy, Zachary Gordon, Kasra Ahmadinia, Randall Marcus, Michael Abdulian, Ari Levine, Daniel Master, Brendan Patterson, Brian victoroff, Steven Fitzgerald, John Wilber, Lorraine Stern
2nd Row: Claire Shannon, Megan Brady, Jason Eubanks, Christina Hardesty, Raymond Liu, Troy Mounts, Edward Greenfield, Sheeba Joseph, Abishek Ray, Christopher Bechtel, Michael Reich, Ashraf youssef, Stephen Lacey, Stephen Reichard, Shana Miskovsky
3rd Row: Kath Bogie, Adrienne Moraff, Anna Wallace, Guang Zhou, Patrick Getty, Ozan Akkus, John Shaffer, Dwight Davy, Thomas McLaughlin, James Learned, William Petersilge, Jason Solomon, Jonathan Belding, Harry Hoyen, Jonathan Macknin, Kelvin Lim
4th Row: Nicholas Ahn, Roger Wilber, Ke Xie, Robert Anderson, Andrew Chen, Sunny Patel, Ronak Desai, Donald Goodfellow, Daniel Cooperman, Scott Kling, Chad Fortun, Aaron Pemberton, Christopher Furey, Glenn Wera, William Morris
PHOTOS FROM THROUGHOUT THE yEAR
Case Western Reserve UniversityDepartment of Orthopaedics

ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 25
YEAR IN REVIEW
Herndon Dinner 2012- The Grand Café, San Francisco, California
Dr Learned, Mrs. Katy Marcus, Dr Marcus, Dr Schnaser, Dr Kling, Dr Gordon, & Dr Cooperman with his wife, Dr Harris.
Dr Skalak with his wife, Jen, and Dr Paczas.
Dr Furey and his wife, Meg, and Dr Goodman with his wife, Paula.Dr Walsh and his wife, Anne, with Dr Wertheim and with his wife, Melinda.
Dr Maheshwer, Dr Parr, Dr Haque, & Dr Elyaderani.Drs Archdeacon, Blakemore, Wilber, & Emery.
Drs Islam, Chen, Feighan, & Gillespie.
26
Drs McLaughlin, Frederick, Junglas, & friend.
Medical student Ernie young with Dr Mounts and his brother also Dr Mounts.
Medical Student Harpreet Bawa, Dr Nelson and Dr yoo.
Dr Farrow and his wife, Tenisha with Dr Goldman and his wife, Deb.
Drs Duffett, McLaughlin, Frederick, Junglas.
Drs Patterson, Getty, and Fitzgerald.
Dr Petersilge with Dr Grabow with his wife, Heidi.
PHOTOS FROM THROUGHOUT THE YEAR
ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 27
2012 Intern Picnic
Ellen Greenberger
Dr Tsai manning the grill.
Some of our new interns, Drs. Sheeba Joseph, Andrew Chen, Ronak Desai, William Morris and Sunny Patel.
Drs Tsai, Nguyen, & Cheng.
Drs Morris, Tsai, & Anderson waiting patiently to grill out.
YEAR IN REVIEW
28
2012 Trout Club
Drs Goodfellow, Makley, Wilber, Greenfield, & Petersilge. Dr Learned teaching Mike Karns the ropes.
Dr victoroff relaxing after a busy year.
Mike Abdulian and Ari Levine enjoying their last Trout Club with Jon Macknin and Ashraf youssef.
PHOTOS FROM THROUGHOUT THE YEAR
ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 29
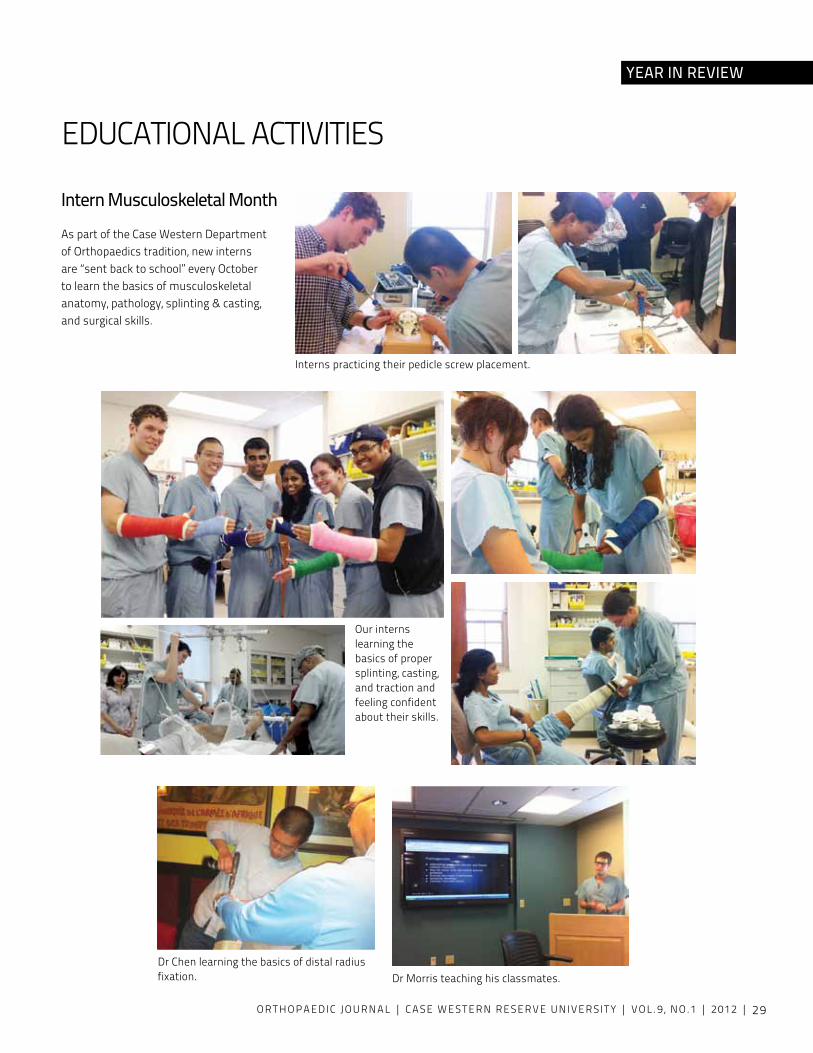
EDUCATIONAL ACTIvITIES
Intern Musculoskeletal MonthAs part of the Case Western Department of Orthopaedics tradition, new interns are “sent back to school” every October to learn the basics of musculoskeletal anatomy, pathology, splinting & casting, and surgical skills.
Dr Chen learning the basics of distal radius fixation.
Interns practicing their pedicle screw placement.
Dr Morris teaching his classmates.
Our interns learning the basics of proper splinting, casting, and traction and feeling confident about their skills.
YEAR IN REVIEW
30
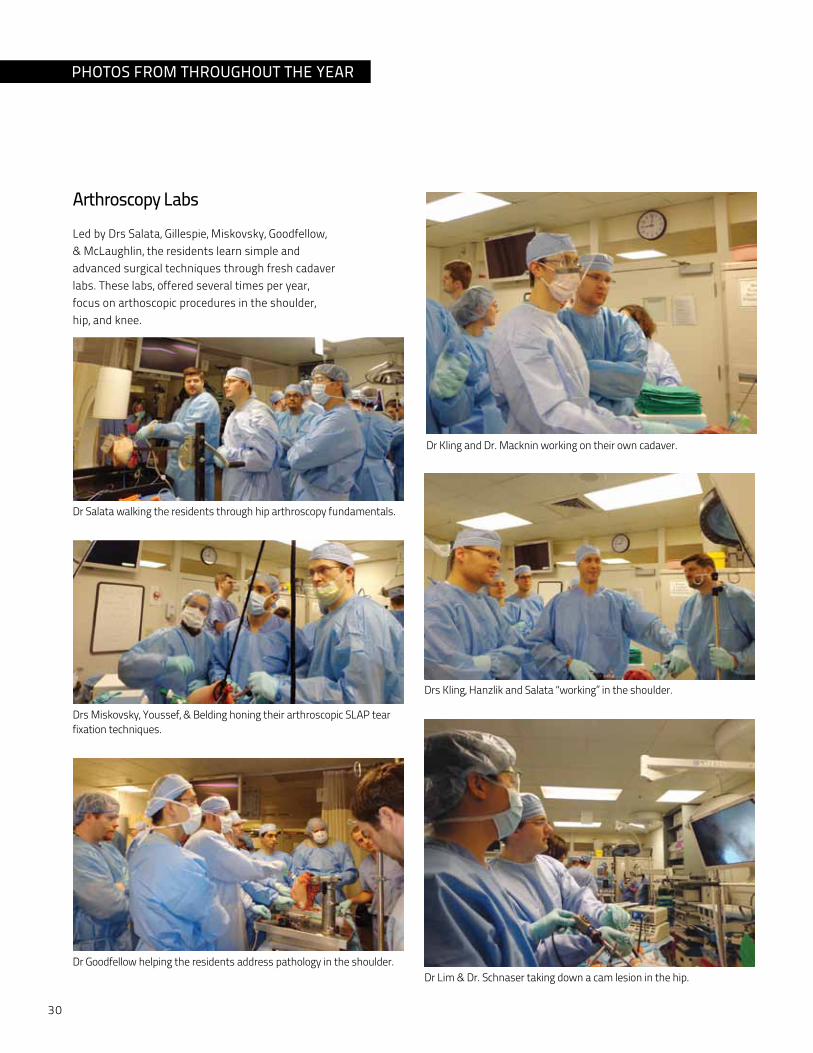
Arthroscopy LabsLed by Drs Salata, Gillespie, Miskovsky, Goodfellow, & McLaughlin, the residents learn simple and advanced surgical techniques through fresh cadaver labs. These labs, offered several times per year, focus on arthoscopic procedures in the shoulder, hip, and knee.
Dr Salata walking the residents through hip arthroscopy fundamentals.
Drs Miskovsky, youssef, & Belding honing their arthroscopic SLAP tear fixation techniques.
Dr Goodfellow helping the residents address pathology in the shoulder.
Dr Kling and Dr. Macknin working on their own cadaver.
Drs Kling, Hanzlik and Salata “working” in the shoulder.
Dr Lim & Dr. Schnaser taking down a cam lesion in the hip.
PHOTOS FROM THROUGHOUT THE YEAR

ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 31
Daniel Cooperman Steven Fitzgerald
Patrick Getty Allison Gilmore victor Goldberg Donald Goodfellow
Christina Hardesty Matthew Kraay Stephen Lacey Randall Marcus
William Petersilge John Shaffer George Thompson
Brian victoroff Glenn Wera Roger Wilber
Robert AndersonNicholas Ahn
Shana Miskovsky Joe Son-Hing
Susannah Briskin
UH ATTENDINGS
Jason Eubanks
John Wilber
Raymond Liu
Michael Salata
Christopher Furey Robert Gillespie
Amanda Weiss Kelly
YEAR IN REVIEW

32
METROHEALTH ATTENDINGS
Daniel Cooperman
Harry Hoyen Michael Keith Stephen Lacey
Brendan PattersonClyde Nash John Sontich Heather vallier
John Wilber
Tim Moore
Kevin Malone
John FeighanMegan Brady Christina Hardesty
Raymond Liu
Roger Wilber
Todd Bafus
Charlotte Wagamon
ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 33
Ronald Triolo
Kath Bogie
Edward Greenfield Shunichi Murakami P Hunter Peckham
Clare Rimnac Guang Zhou
Eben Alsberg
Joseph Mansour*
* Modified copy of image [Source] property of Case Western Reserve University Archives.
Ozan Akkus Dwight Davy
UH ATTENDINGS
BASIC SCIENCE FACULTy
YEAR IN REVIEW
34
vAMC ATTENDINGS
Robert Anderson
victor Goldberg Randall Marcus Thomas McLaughlin
Todd Bafus
Robert Gillespie
Glenn Wera
Steven Fitzgerald Patrick Getty

ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 35
Patrick Getty Jason Eubanks
Donald Goodfellow Stephen Lacey
John Shaffer Michael Salata
John Wilber
William PetersilgeShana Miskovsky
Christopher FureyRobert Anderson
Randall Marcus
AHUJA ATTENDINGS
Brian victoroff
YEAR IN REVIEW
Steven Fitzgerald
Raymond LiuAllison GilmoreRobert Gillespie
36
CURRENT RESIDENTS
Shane Hanzlik, MDMD, University of Nevada BS, University of Nevada
Scott Kling, MDMD, University of Pennsylvania BS, College of William and Mary
PGY-5 ResidentsEthan Lea, MDMD, Case Western Reserve UniversityBS, Kent State University
PGY-4 Residents
James Learned, MDMD, University of Southern CaliforniaBA, University of California, Berkeley
Troy Mounts, MDMD, University of Tennesse BS, Trevecca Nazarene UniversityMS, Fisk University
Erik Schnaser, MDMD, University of Nevada BS, University of Southern California
Jonathan Belding, MDMD, Case Western Reserve UniversityBA, Colgate University
Chad Fortun, MDMD, Case Western Reserve University BS, University of Wisconsin - La Crosse
Jonathan Macknin, MDMD, University of PennsylvaniaBA, University of Pennsylvania
Jason Solomon, MDMD, University of Medicine and Dentistry of New Jersey BS, The College of New Jersey
Lorraine Stern, MDMD, George Washington University BS, George Washington University
Anna Wallace, MDMD, University of Tennessee BA, University of Tennessee

ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 37
CURRENT RESIDENTS
Kelvin Lim, MDMD, Loma Linda University School of Medicine BS, Walla Walla University
Stephen Reichard, MDMD, Wake Forest University School of Medicine BA, University of North Carolina
PGY-3 ResidentsJonathan Streit, MDMD, University of Michigan BS, University of Notre Dame
PGY-2 Residents
Eugene Tsai, MDMD, Columbia University College of Physicians and SurgeonsBS, Northwestern University
Ke Xie, MDMD, University of Cincinnati College of MedicineBA, Northwestern University
Ashraf youssef, MDMD, University of virginiaBS, University of Michigan
Christopher Bechtel, MDMD, New york University School of Medicine BS, University of Notre Dame
Michael Karns, MDMD, University of Cincinnati BS, University of Dayton
Sean Mazloom, MDMD, Chicago Medical School BS, University of California San Diego
Cynthia Nguyen, MDMD, Baylor University BS, UCLA
Michael Reich, MDMD, vanderbilt University School of MedicineBA, Washington University
Claire Shannon, MDMD, University of RochesterBS, University of Western Ontario
Christina Cheng, MDMD, SUNy Buffalo BS, Cornell University
Andrew Tsai, MDMD, University of Minnesota MSc, Carnegie Mellon University BS, Carnegie Mellon University
Allen Fellows
YEAR IN REVIEW
38
Andrew Chen, MDMD, University of North Carolina MPH, Johns Hopkins University BS, University of North Carolina
Ronak Desai, MDMD, Rush University BS, Illinois Institute of Technology
Sheeba Joseph, MDMD, Case Western Reserve University BS, Case Western Reserve University
Adrienne Moraff, MDMD, University of MarylandBA, University of Maryland
William Morris, MDMD, University of Texas BA, University of Southern California
Sunny Patel, MDMD, Case Western Reserve University BA, University of Pennsylvania
CURRENT INTERNS – CLASS OF 2017

ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 39
Congratulations to all 2012 graduating residents for passing their 2012 ABOS Step 1 Examinations!
Please congratulate Shane Hanzlik, MD who won the trainee award for the best basic science paper at the Annual Meeting of the International Society of Hip Arthroscopy (ISHA).
Chad Fotun, MD was a finalist for the best basic science paper at the ISHA.
Michael Reich, MD, 2012 Baxter young Investigator Award.
Jonathan Streit, MD, won second place in the annual Mount Sinai Barry Freedman Award for residency programs in Northeast Ohio for his research project on acetabular wear patterns in individuals with different types of cam deformity of the proximal femur.
AWARDS/RECOGNITIONS
Lindsay Bonsignore, PhD, won the “Best Poster Award” during the CWRU Musculoskeletal Research day.
Erik Schnaser, MD, American OrthopaedicAssociation/Orthopaedic Research and Education Foundation Resident Leadership Award
Ellen Greenberger, our Orthopaedic Residency Coordinator, receiving an award for 35 years of service to University Hospitals Case Medical Center. l-to-r: Ms. Diane De Rubertis, Administrator for Department of Orthopaedics, Ellen, and Dr Randall E. Marcus, Department Chairman.
Congratulations to Valerie Schmedlen, the Department of Orthopaedic Surgery’s Research Editor, for joining University Hospitals Quarter Century Club for her 25 years of service. l-to-r: Dr Marcus, valerie Schmedlen, Dr Greenfield, and Phyllis Lie.
YEAR IN REVIEW
40
MANUSCRIPTS
CULTURING STEM CELLS TO ACHIEvE PHySIOLOGICAL CONTEXTS AND TO MAXIMIZE CLINICAL RELEvANCEHana Chang, M.S.1, Melissa L. Knothe Tate, Ph.D. 1,2
Case Western Reserve University, 1Department of Biomedical Engineering, 2Department of Mechanical and Aerospace Engineering
AbstractIn vitro studies using various types of stem cells have become fundamental tools in better understanding natural processes (differentiation, healing, disease etc.) that occur in living organisms. While basic cell or tissue culture techniques have been standardized to maximize cell viability and longevity, as well as laboratory functionality and convenience, it is important to carefully consider the physiological relevance of all aspects of cell culture when designing or interpreting the results of any particular experiment. These considerations can be especially significant in translational studies, where these non-physiological culture conditions may explain discrepancies between in vitro and in vivo results. This concise review briefly visits the major aspects of stem cell culture and how they do or do not mimic physiological contexts within the human body.
ArticleThe in vitro culture of pluripotent cells for research is practiced commonly and widely throughout the research community. However, with the progression and expansion of knowledge in the biological field it is important to continuously reevaluate the protocols and conditions involved in cell culture. For most researchers, particularly those
related to clinical application, it is critical to relate or optimize in vitro conditions to mimic if not to replicate normal or diseased physiological conditions. While in vitro culture can successfully propagate and differentiate stem cells, it is important to reevaluate which aspects adequately simulate in vivo conditions.
Mesenchymal stem cell (MSC) cultures are maintained at 37°C, the same temperature as a normal human body. Interestingly, thermal stress (similar to changes that occur during fever or inflammation) upregulates transcription of heat shock and other stress induced proteins, which can induce cellular change, such as enhancing osteogenic differentiation1,2. Even media conditioned by heat-shocked osteoblasts enhances differentiation of MSCs, indicating not only intracellular changes due to thermal stress but also the production of extracellular signals/factors3. This suggests that a stressful state of a biological system, in this case caused by excessive heat, can induce changes within and around the cell to affect its commitment. Since body temperature is regulated on a systemic level, subtle fluctuations that occur during abnormal conditions (injury, inflammation, healing) can be difficult to mimic in an in vitro setting.
Oxygenation is another controlled
component of cell culture. Typical O2
concentrations in human body tissues can range from about 1-7% 4. These oxygenation levels are spatially regulated by tissue permeability, vascularization, and oxygen metabolism rates, and different cellular niches reside in differently oxygenated compartments. In contrast, most tissue culture occurs at atmospheric O2 concentrations around 20%. This disparity affects the capacity for stem cells to differentiate. For instance, cell expansion at physiological O2 concentrations promotes osteogenic differentiation more greatly than differentiation at physiological O2 concentrations (compared to atmospheric), and differentiation at physiological O2 concentrations promotes chondrogenic differentiation more than expansion at physiological O2. However, the best results for both chondrogenic and osteogenic differentiation occur when both expansion and differentiation are conducted at physiological O2 conditions . Moreover, due to the differences in metabolic pathways and function between MSCs compared to fully differentiated cells, oxygenation levels strongly affect the metabolic state of these cells. MSCs differentiated into osteoblasts exhibit a fourfold increase in respiration rate, a threefold increase in ATP production, and a fivefold increase in ATP content compared to

ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 41
undifferentiated cells . This is consistent with pluripotent stem cells producing ATP mainly by the process of glycolysis, while most differentiated cells rely more heavily on oxidative phosphorylation for energy production7,8. The changes that occur during cell maturation are still poorly understood, but ultimately allow for the energy demands of the mature cell’s function to be met. Since glycolysis is an anaerobic process, stem cells do not have a high oxygen demand during cellular respiration. In fact, low oxygen environments assist in the maintenance of undifferentiated stem cells, which may explain their in vivo longevity in aging animals compared to in vitro culture conditions9. MSCs cultured at physiological O2 concentrations do not exhibit markers for cell death or hypoxia, while their lifespan (time until senescence) is prolonged10,11.
Growth media are another important component to cell culture. Different basal growth media (α-MEM, DMEM, BME, Ham’s F12, etc.) are not only comprised of different inorganic salts and amino acids, but also vary greatly in vitamins and supplements, which in turn vary greatly in comparison to physiological concentrations. It is important to consider that these media were initially developed to promote cell viability, not necessarily to mimic physiological conditions. MSCs not only vary their proliferation rate depending on the basal medium, but also differ in their surface marker expression and differentiation capacity in vitro12,13. Once these cultured cells are implanted in vivo, the basal medium also affects grafting and immunosuppressive properties13. Furthermore, serum is typically added as 10-20% of cell culture medium, and contains factors to promote cell growth, metabolism, and proliferation. These factors include proteins essential for cellular transport and cell attachment and spreading, as well as hormones,
growth factors, cytokines, fatty acids, lipids, etc. that cells typically encounter in a physiological setting. Serum also increases the viscosity of culture medium. yet, due to the nature of serum collection, even commercially available serum can vary and cannot be standardized. While commercially available standardized serum substitutes are shown to be comparable or superior to biological serum , its physiological comparability is still poorly understood. All these nutritive factors can directly contribute to the state of the cell and need to be carefully considered for the potential roles they can play in different cellular processes.
Another controlled aspect of cell culture is glucose concentration. The American Diabetes Association recommends preprandial blood glucose levels range from 3.9-7.2 mM and postprandial glucose levels up to 10mM. Consequently, the glucose levels are slightly lower in body tissues. While most basal mediums fall within this range at 5.5mM glucose, others contain as high as 25mM glucose, well beyond a hyperglycemic concentration. Most MSC cultures are maintained at a physiological glucose concentration, but many inductive or differentiation medias involved the use of high glucose formulations. While these formulations can successfully induce differentiation in vitro, these processes are drastically different from in vivo processes, and the resulting differences are poorly understood. MSC culture in high glucose can impair cellular functions, increase apoptosis, reduce multipotency and induce replicative senescence15,16. Since the ATP production by glycolysis is a fraction of that by oxidative phosphorylation, pluripotent cells possess several different mechanisms to maintain high glycolytic rates to supply their energy demands7. This high dependence on glucose suggests that exposure to such drastically larger
concentrations could potentially produce large quantities of lactate byproduct, which decreases cell proliferation and metabolic rates of MSCs17. This is consistent with results demonstrating the initiation of stress responses, inflammatory pathways, and autophagy during hyperglycemic conditions18. Similar to temperature, glucose levels constantly fluctuate and are regulated systemically, making them difficult to mimic in vitro.
The best efforts to control physiological aspects of cell culture have been in determining the physical environment of the cells, including culture substrate and topography, cellular construct and density and mechanical stress. Great efforts have been made to both measure and mimic both the structures and stresses experienced in native tissues. Substrates of similar physiological elasticities to brain, muscle, and bone tissue induce neuro-, myo-, and osteo-genic differentiation of pluripotent cells, respectively19. Similarly, softer substrates, rather than stiffer substrates, promote adipo- and chondro-genic differentiation20. Substrates have also been modified to control cell spreading or alignment to mimic native tissue organization21,22. Structural and mechanical changes within the cell are closely linked with cell fate, and are a great example of how the state of the cell can drive changes to its inner functions. While most in vitro cell culture is performed in a low density, two-dimensional platform, great strides have been made to create functional high density, three-dimensional matrix environments for in vivo implantation by increasing porosity and oxygenation23. Additionally, cell seeding and density contexts can influence the size and shape of cells and play a role in determining their fate24,25. Furthermore, many researchers have used compression or shear stress to mimic physiological conditions while simultaneously

42
increasing the differentiation and functionality of the stem cells26,27,28.
In summary, these listed aspects of controlled cell culture, in addition to many other unmentioned factors, are capable of maintaining cells in a biologically relevant or irrelevant context. While it is unrealistic to attempt to recreate the intricately vascularized and organized native environment of stem cells, it is still important to consider these disparities regarding specific research questions when translating in vivo results to an in vitro scenario. Only then can experimental results be accurately interpreted and appropriately translated for other applications.
References1. Mauney J, volloch v. Collagen I matrix
contributes to determination of adult human stem cell lineage via differential, structural conformation-specific elicitation of cellular stress response. Matrix Biol. 2009;28:251-262.
2. ye CP, Heng BC, Liu H, Toh WS, Cao T. Culture media conditioned by heat-shocked osteoblasts enhances the osteogenesis of bone marrow-derived mesenchymal stromal cells. Cell Biochem Funct. 2007;25(3):267-276.
3. Nørgaard R, Kassem M, Rattan SI. Heat shock-induced enhancement of osteoblastic differentiation of hTERT-immortalized mesenchymal stem cells. Ann N Y Acad Sci. 2006;1067:443-447.
4. Chow DC, Wenning LA, Miller WM, Papoutsakis ET.Modeling pO(2) distributions in the bone marrow hematopoietic compartment. I. Krogh’s model. Biophys J. 2001;81(2):675-684.
5. Fehrer C, Brunauer R, Laschober G, Unterluggauer H, Reitinger S, Kloss F, Gülly C, Gassner R, Lepperdinger G. Reduced oxygen tension attenuates differentiation capacity of human mesenchymal stem cells and prolongs their lifespan. Aging Cell. 2007;6(6):745-757.
6. Komarova Sv, Ataullakhanov FI, Globus RK.Bioenergetics and mitochondrial transmembrane potential during differentiation of cultured osteoblasts. Am J Physiol Cell Physiol. 2000;279(4):C1220-1229.
7. varum S, Rodrigues AS, Moura MB, Momcilovic O, Easley CA 4th, Ramalho-
Santos J, van Houten B, Schatten G. Energy metabolism in human pluripotent stem cells and their differentiated counterparts. PLoS One. 2011;6(6):e20914.
8. Shyh-Chang N, Zheng y, Locasale JW, Cantley LC. Human pluripotent stem cells decouple respiration from energy production. EMBO J. 2011;30(24):4851-2.
9. Mohyeldin A, Garzón-Muvdi T, Quiñones-Hinojosa A. Oxygen in stem cell biology: a critical component of the stem cell niche. Cell Stem Cell. 2010 Aug 6;7(2):150-61.
10. Sheehy EJ, Buckley CT, Kelly DJ. Oxygen tension regulates the osteogenic, chondrogenic and endochondral phenotype of bone marrow derived mesenchymal stem cells. Biochem Biophys Res Commun. 2012;417(1):305-310.
11. Ishikawa y, Ito T (1988) Kinetics of hemopoietic stem cells in a hypoxic culture. Eur. J. Haematol. 40, 126–129.
12. Jaiswal N, Haynesworth SE, Caplan a I, Bruder SP. Osteogenic differentiation of purified, culture-expanded human mesenchymal stem cells in vitro. J cell biochem. 1997;64(2):295-312.
13. Sotiropoulou PA, Perez SA, Salagianni M, Baxevanis CN, Papamichail M. Characterization of the Optimal Culture Conditions for Clinical Scale Production of Human Mesenchymal Stem Cells. Stem Cells. 2006;24(2):462-471.
14. Meuleman N, et al. Human marrow mesenchymal stem cell culture: serum-free medium allows better expansion than classical alpha-MEM medium. Eur J Haematol. 2006;76(4):309-16.
15. Li yM, Schilling T, Benisch P, Zeck S, Meissner-Weigl J, Schneider D, Limbert C, Seufert J, Kassem M, Schütze N, Jakob F, Ebert R. Effects of high glucose on mesenchymal stem cell proliferation and differentiation. Biochem Biophys Res Commun. 2007;363(1):209-215.
16. Stolzing A, Coleman N, Scutt A. Glucose-induced replicative senescence in mesenchymal stem cells. Rejuvenation Res. 2006;9(1):31-35.
17. Chen T, Zhou y, Tan WS. Influence of lactic acid on the proliferation, metabolism, and differentiation of rabbit mesenchymal stem cells. Cell Biol Toxicol. 2009;25(6):573-586.
18. Wang A, Hascall vC. Hyperglycemia, intracellular hyaluronan synthesis, cyclin D3 and autophagy. Autophagy. 2009 Aug;5(6):864-5. Epub 2009 Aug 13.
19. Engler AJ, Sen S, Sweeney HL, Discher DE. Matrix elasticity directs stem cell lineage specification. Cell. 2006;126(4):677-89.
20. Par JS et al. The effect of matrix stiffness on the differentiation of mesenchymal stem cells in response to TGF-b. Biomaterials, 2011;32(16):3921-3930.
21. Kurpinski K , Chu J , Hashi C , Li S. Anisotropic mechanosensing by mesenchymal stem cells . Proc Natl Acad Sci. 2006;103:16095–100 .
22. Dalby MJ, Gadegaard N, Tare R, Andar A, Riehle MO, Herzyk P, et al. The control of human mesenchymal cell differentiation using nanoscale symmetry and disorder. Nature Materials. 2007;6(12):997-1003.
23. Fedorovich NE, Kuipers E, Gawlitta D, Dhert WJ, Alblas J. Scaffold porosity and oxygenation of printed hydrogel constructs affect functionality of embedded osteogenic progenitors. Tissue Eng Part A. 2011 Oct;17(19-20):2473-86. Epub 2011 Jul 8.
24. McBride SH, Knothe Tate ML. Modulation of stem cell shape and fate A: the role of density and seeding protocol on nucleus shape and gene expression. Tissue Eng Part A. 2008 Sep;14(9):1561-72.
25. Zimmermann JA, Knothe Tate ML. Structure-function relationships in the stem cell’s mechanical world A: seeding protocols as a means to control shape and fate of live stem cells. Mol Cell Biomech. 2011 Dec;8(4):275-96.
26. Kishore v, Bullock W, Sun X, van Dyke WS, Akkus O. Tenogenic differentiation of human MSCs induced by the topography of electrochemically aligned collagen threads. Biomaterials. 2012 Mar;33(7):2137-44. Epub 2011 Dec 15.
27. Kim DH, Heo SJ, Kim SH, Shin JW, Park SH, Shin JW. Shear stress magnitude is critical in regulating the differentiation of mesenchymal stem cells even with endothelial growth medium. Biotechnol Lett. 2011 Dec;33(12):2351-9. Epub 2011 Jul 31.
28. Schätti O, Grad S, Goldhahn J, Salzmann G, Li Z, Alini M, Stoddart MJ. A combination of shear and dynamic compression leads to mechanically induced chondrogenesis of human mesenchymal stem cells. Eur Cell Mater. 2011 Oct 11;22:214-25.

ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 43
MANUSCRIPTS
IATROGENIC SUBTROCHANTERIC FEMORAL FRACTUREAndrew G. Tsai1, Timothy Ashworth2, Michael S. Reich1, Christopher Bechtel1, Randall E. Marcus1, Ozan Akkus1,3
Case Western Reserve University, 1School of Medicine, Department of Orthopaedics2School of Medicine, 3Department of Mechanical and Aerospace Engineering, Musculoskeletal Materials and Mechanics Laboratory
AbstractSurgical interventions that require drilling or reaming the proximal portion of the lateral femoral cortex may cause subsequent iatrogenic subtrochanteric fractures and are a significant concern for orthopaedic surgeons. Though the problem is known to exist, there remains a paucity of data explaining the biomechanics of this fracture pattern, and controversy remains regarding prevention of such fractures. Current literature on iatrogenic subtrochanteric fractures consists largely of retrospective analyses of small numbers of patients. Biomechanical analysis surrounding iatrogenic subtrochanteric fractures has not consistently and effectively proven surgical techniques for prevention of those fractures. A better understanding of the problem of iatrogenic subtrochanteric fractures will allow for the development of techniques to prevent this complication from occurring.
IntroductionOperative management of a number of conditions may require drilling or reaming of the proximal portion of the lateral femoral cortex for placement of metal implants through the cortex. Unfortunately, a subset of such interventions may be complicated by fractures in the area of the cortical disruption (Figure 1). Though more commonly associated with screw or pin placement for femoral neck fractures1, an iatrogenic subtrochanteric fracture (ISF)
can also complicate core decompression for avascular necrosis (AvN)2,3 or fixation of slipped capital femoral epiphysis (SCFE)4,5. These fractures remain incompletely understood from a biomechanical standpoint, with most of the information regarding such fractures coming from case reports. These fractures are thought to be related to the surgical fixation technique, as most of these fractures appear to initiate at, or at least propagate through, the cortical defect created during the operation. The defect on the lateral femoral cortex is hypothesized to contribute to creation of ISFs3,6.
Case reports of ISFs after internal fixation of femoral neck fractures with pins or cannulated screws are more common than after other operations. Approximately 3% of patients who undergo internal fixation for femoral neck fractures with screws and pins may experience ISFs7. Though a fairly small percentage, it represents a large number of patients when one considers that there are upwards of 340,000 hip fractures in the United States annually according to recent data from the CDC, of which approximately half may occur at the femoral neck8,9. Though the rate of hip fracture in the elderly population has declined in recent years, the incidence has been predicted to increase in the future, particularly because of the increase in the elderly population10-13. Two isolated cases of subtrochanteric fracture after core decompression for
AvN have been reported2-3, and at least seven patients are noted in the literature to have also sustained fracture related to surgical intervention for SCFE4, 5, 14, 15. The incidence may be low now, but because of the rising childhood obesity rate and incidence of SCFE, ISFs may become a more prominent complication in the future in the pediatric population16, 17. The rate of subtrochanteric fracture after core decompression for AvN or internal fixation for SCFE appears to be lower than screw fixation of hip fracture, but ISFs remain a serious and debilitating risk associated with these procedures as well.
The biomechanics of ISFs has not been investigated to a level of detail to support currently-accepted theories and practices. The proximal femoral cortex is one of the most highly stressed regions in the body18, and studies analyzing the proximal femur show the medial side to be in compression and the lateral side in tension19-21. Bone adaptation accommodates such stresses in the normal femur; however, creation of screw holes for fracture fixation results in stress concentration and may pave the way for fatigue failure.
Brooks et al. experimentally showed in our laboratory that lateral to medial drill holes in the cortex of canine femurs at the mid-shaft decreased the amount of energy the bone could absorb during torsion before fracturing6. During healing, bone has been reported to adapt to the

44
stress concentration effect by eight weeks, but during the post-operative period, the bone may be weakened significantly22. These effects may significantly contribute to subtrochanteric fracture occurrence after surgery.
The reported ISFs occurred between one week and two years from the day of surgery23-25. Previous literature show that iatrogenic fractures may occur in both the presence and absence of trauma, though only about half of the patients reported direct trauma as a possible cause of the fracture2, 4, 5, 23-28. An ISF in the absence of a clear precipitating event indicates that fatigue failure with crack initiation and propagation may be the likely mechanism of fracture. Unfortunately, most studies that have tested femoral neck fracture fixation constructs biomechanically have done so under monotonic loading conditions29-32.
This report serves to review relevant information pertaining to iatrogenic subtrochanteric fractures to increase the understanding of this devastating complication.
Case ReviewsInternal Fixation of Femoral Neck FracturesIatrogenic subtrochanteric fractures after internal fixation with many different implant types have been reported in literature. In the English literature, at least forty-seven cases of subtrochanteric fracture after internal fixation for femoral neck fractures have been reported1, 7, 23-28,
33-35. Cases are listed in Table 1. Jansen et al. reviewed forty-one reported cases as well as two of their own cases7. Garden screws were the predominantly reported fixation type in the patients with ISFs. Several other articles have described ISF after fixation of femoral neck fractures. Blyme et al. reported four cases (18.2% in their series) of ISFs within six weeks after femoral neck fracture fixation with placement of three variable-length
cannulated (vLC) screws26. The final step in fixation with vLC-screws was hammering the screw until flanges underneath the screw head were seated in the lateral cortex. One of their patients who did not sustain an iatrogenic fracture was actually noted to have had the screw head driven through the lateral cortex. All of the patients’ fracture line traveled through the vLC-screw holes, suggesting the involvement of screw hole in the incidence of fracture. Parker et al. reported two cases of ISF in their series of 185 patients who underwent internal fixation with parallel Garden screws, whereas previous Garden screw-related fractures involved obliquely-oriented Garden screws34.
When the cases in the literature are combined, thirty-eight out of 1281 patients, a 2.96% incidence rate, undergoing screw fixation for a femoral neck fracture were observed to have developed an ISF1, 7, 23-28, 33-35. When data were provided, the patients with an ISF were 78.4 years old on average1, 7, 23-28, 33,
34. Females represented 88% of the cases when sex of the patient was reported. For all patients, an average of 5.3 weeks (range 1-12 weeks, standard deviation 3.5 weeks) had elapsed since the initial operation. Two patients whose fracture occurred more than two years post-operatively —24 and 120 weeks— were excluded as outliers when calculating average time to fracture. Four more patients’ iatrogenic fractures were reported to have occurred less than six weeks from the time of operation, but a specific length of time was not reported26. For patients whom direct trauma was not involved, the ISF occurred approximately 4.9 weeks after the initial operation (range 1-12 weeks, standard deviation 3.5 weeks). If there was direct trauma to the patient, 7.1 weeks elapsed on average between the operation and the ISF (range 2-12 weeks, standard deviation 3.4 weeks). Direct trauma was
reported in 44.7% of the cases (21 of 47), 48.9% reported no trauma or indirect trauma (e.g. stumbling), and 3 cases did not report whether there was trauma. Placement of the most inferior screw or pin was at or below the distal border of the lesser trochanter in 70.2% of the cases (33 of 47), 6.4% had placement at or above the midpoint of the lesser trochanter, and in eleven of the cases, height of device placement was not reported or shown. In 20% (2 of 10) of patients reported by Andrew et al., the fracture occurred through an un-used drill hole23. A variety of screws and pins were used, including Gouffon, Moore, or Knowles pins25; crossed garden screws23, 24, 27, 33, 34; and parallel cannulated screws of different sizes1, 7, 35. Though crossed Garden screws were the most heavily represented type of screw used in association with subtrochanteric fractures, the orientation of the screws with a lower insertion point was thought to be the main contributing factor23. A recent Cochrane review of screws used for fixation of femoral neck fractures was unable to make any specific recommendation for one screw type over another based on available information36.
Internal fixation of Slipped Capital Femoral EpiphysisSlipped capital femoral epiphysis is seen in about 10.8/100,000 in the pediatric population17. Fixation with threaded screws or pins has been used to treat SCFE and prevent progression of the disease; and placement of one or two femoral screws is the mainstay of treatment for SCFE 37, 38. The screw or pin may be placed through the lateral femoral cortex in a manner similar to internal fixation for hip fractures. An uncommon complication is an ISF, some of which occur through either used or un-used holes created during the fixation procedure. There are multiple reports in the literature (Table 1) of subtrochanteric fractures occurring subsequent to pinning for SCFE4, 14, 15. Complications from
IATROGENIC SUbTROCHANTERIC FEMORAL FRACTURE
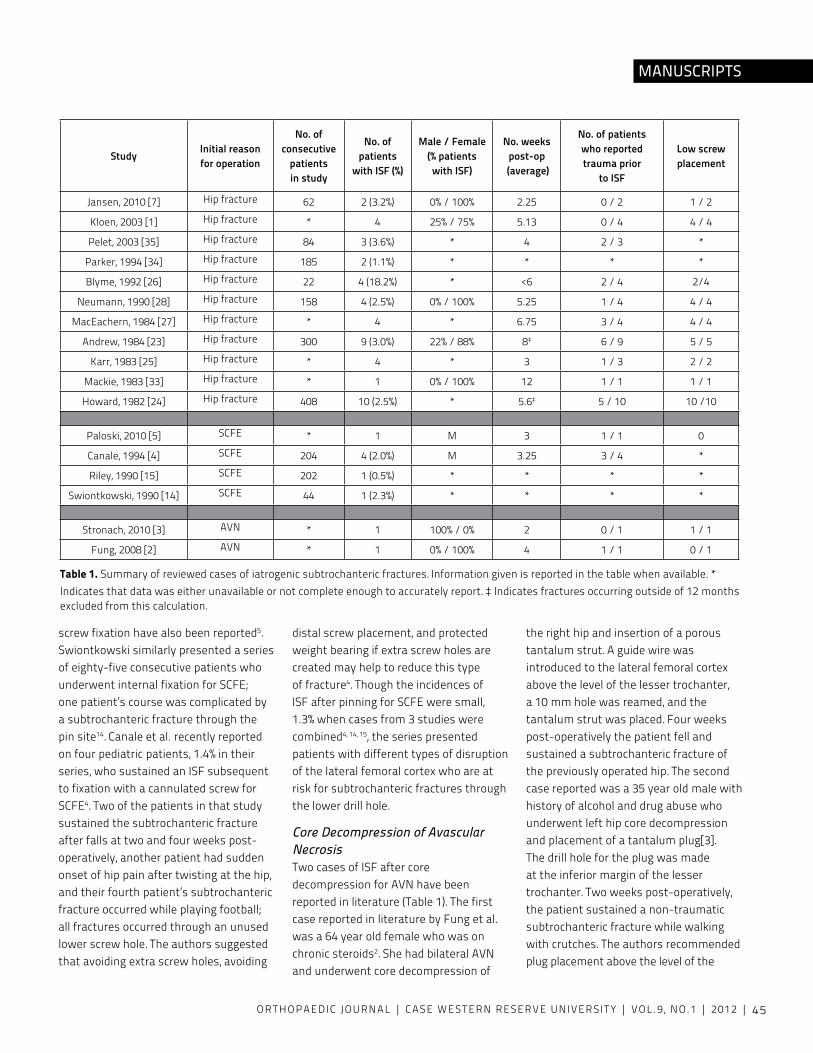
ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 45
MANUSCRIPTS
screw fixation have also been reported5. Swiontkowski similarly presented a series of eighty-five consecutive patients who underwent internal fixation for SCFE; one patient’s course was complicated by a subtrochanteric fracture through the pin site14. Canale et al. recently reported on four pediatric patients, 1.4% in their series, who sustained an ISF subsequent to fixation with a cannulated screw for SCFE4. Two of the patients in that study sustained the subtrochanteric fracture after falls at two and four weeks post-operatively, another patient had sudden onset of hip pain after twisting at the hip, and their fourth patient’s subtrochanteric fracture occurred while playing football; all fractures occurred through an unused lower screw hole. The authors suggested that avoiding extra screw holes, avoiding
distal screw placement, and protected weight bearing if extra screw holes are created may help to reduce this type of fracture4. Though the incidences of ISF after pinning for SCFE were small, 1.3% when cases from 3 studies were combined4, 14, 15, the series presented patients with different types of disruption of the lateral femoral cortex who are at risk for subtrochanteric fractures through the lower drill hole.
Core Decompression of Avascular NecrosisTwo cases of ISF after core decompression for AvN have been reported in literature (Table 1). The first case reported in literature by Fung et al. was a 64 year old female who was on chronic steroids2. She had bilateral AvN and underwent core decompression of
the right hip and insertion of a porous tantalum strut. A guide wire was introduced to the lateral femoral cortex above the level of the lesser trochanter, a 10 mm hole was reamed, and the tantalum strut was placed. Four weeks post-operatively the patient fell and sustained a subtrochanteric fracture of the previously operated hip. The second case reported was a 35 year old male with history of alcohol and drug abuse who underwent left hip core decompression and placement of a tantalum plug[3]. The drill hole for the plug was made at the inferior margin of the lesser trochanter. Two weeks post-operatively, the patient sustained a non-traumatic subtrochanteric fracture while walking with crutches. The authors recommended plug placement above the level of the
Table 1. Summary of reviewed cases of iatrogenic subtrochanteric fractures. Information given is reported in the table when available. * Indicates that data was either unavailable or not complete enough to accurately report. ‡ Indicates fractures occurring outside of 12 months excluded from this calculation.
Study Initial reason for operation
No. of consecutive
patients in study
No. of patients
with ISF (%)
Male / Female(% patients with ISF)
No. weeks post-op
(average)
No. of patients who reported trauma prior
to ISF
Low screw placement
Jansen, 2010 [7] Hip fracture 62 2 (3.2%) 0% / 100% 2.25 0 / 2 1 / 2
Kloen, 2003 [1] Hip fracture * 4 25% / 75% 5.13 0 / 4 4 / 4
Pelet, 2003 [35] Hip fracture 84 3 (3.6%) * 4 2 / 3 *
Parker, 1994 [34] Hip fracture 185 2 (1.1%) * * * *
Blyme, 1992 [26] Hip fracture 22 4 (18.2%) * <6 2 / 4 2/4
Neumann, 1990 [28] Hip fracture 158 4 (2.5%) 0% / 100% 5.25 1 / 4 4 / 4
MacEachern, 1984 [27] Hip fracture * 4 * 6.75 3 / 4 4 / 4
Andrew, 1984 [23] Hip fracture 300 9 (3.0%) 22% / 88% 8‡ 6 / 9 5 / 5
Karr, 1983 [25] Hip fracture * 4 * 3 1 / 3 2 / 2
Mackie, 1983 [33] Hip fracture * 1 0% / 100% 12 1 / 1 1 / 1
Howard, 1982 [24] Hip fracture 408 10 (2.5%) * 5.6‡ 5 / 10 10 /10
Paloski, 2010 [5] SCFE * 1 M 3 1 / 1 0
Canale, 1994 [4] SCFE 204 4 (2.0%) M 3.25 3 / 4 *
Riley, 1990 [15] SCFE 202 1 (0.5%) * * * *
Swiontkowski, 1990 [14] SCFE 44 1 (2.3%) * * * *
Stronach, 2010 [3] AvN * 1 100% / 0% 2 0 / 1 1 / 1
Fung, 2008 [2] AvN * 1 0% / 100% 4 1 / 1 0 / 1
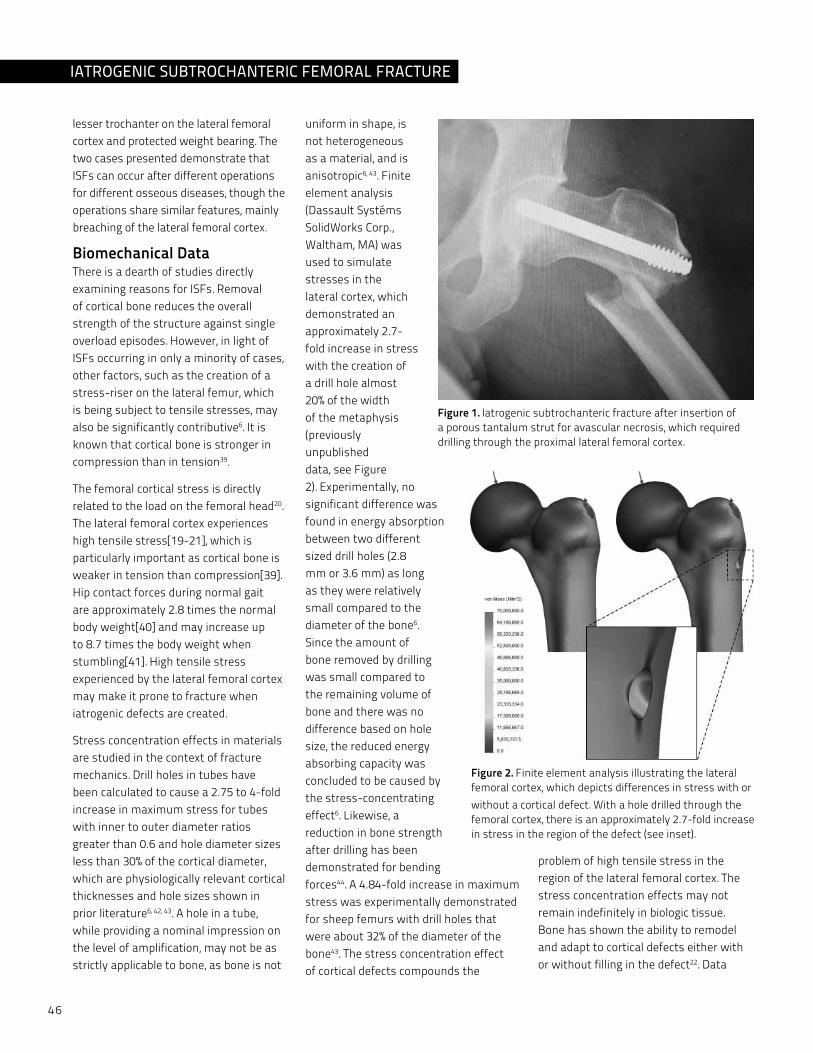
46
lesser trochanter on the lateral femoral cortex and protected weight bearing. The two cases presented demonstrate that ISFs can occur after different operations for different osseous diseases, though the operations share similar features, mainly breaching of the lateral femoral cortex.
Biomechanical DataThere is a dearth of studies directly examining reasons for ISFs. Removal of cortical bone reduces the overall strength of the structure against single overload episodes. However, in light of ISFs occurring in only a minority of cases, other factors, such as the creation of a stress-riser on the lateral femur, which is being subject to tensile stresses, may also be significantly contributive6. It is known that cortical bone is stronger in compression than in tension39.
The femoral cortical stress is directly related to the load on the femoral head20. The lateral femoral cortex experiences high tensile stress[19-21], which is particularly important as cortical bone is weaker in tension than compression[39]. Hip contact forces during normal gait are approximately 2.8 times the normal body weight[40] and may increase up to 8.7 times the body weight when stumbling[41]. High tensile stress experienced by the lateral femoral cortex may make it prone to fracture when iatrogenic defects are created.
Stress concentration effects in materials are studied in the context of fracture mechanics. Drill holes in tubes have been calculated to cause a 2.75 to 4-fold increase in maximum stress for tubes with inner to outer diameter ratios greater than 0.6 and hole diameter sizes less than 30% of the cortical diameter, which are physiologically relevant cortical thicknesses and hole sizes shown in prior literature6, 42, 43. A hole in a tube, while providing a nominal impression on the level of amplification, may not be as strictly applicable to bone, as bone is not
uniform in shape, is not heterogeneous as a material, and is anisotropic6, 43. Finite element analysis (Dassault Systéms SolidWorks Corp., Waltham, MA) was used to simulate stresses in the lateral cortex, which demonstrated an approximately 2.7-fold increase in stress with the creation of a drill hole almost 20% of the width of the metaphysis (previously unpublished data, see Figure 2). Experimentally, no significant difference was found in energy absorption between two different sized drill holes (2.8 mm or 3.6 mm) as long as they were relatively small compared to the diameter of the bone6. Since the amount of bone removed by drilling was small compared to the remaining volume of bone and there was no difference based on hole size, the reduced energy absorbing capacity was concluded to be caused by the stress-concentrating effect6. Likewise, a reduction in bone strength after drilling has been demonstrated for bending forces44. A 4.84-fold increase in maximum stress was experimentally demonstrated for sheep femurs with drill holes that were about 32% of the diameter of the bone43. The stress concentration effect of cortical defects compounds the
problem of high tensile stress in the region of the lateral femoral cortex. The stress concentration effects may not remain indefinitely in biologic tissue. Bone has shown the ability to remodel and adapt to cortical defects either with or without filling in the defect22. Data
Figure 1. Iatrogenic subtrochanteric fracture after insertion of a porous tantalum strut for avascular necrosis, which required drilling through the proximal lateral femoral cortex.
Figure 2. Finite element analysis illustrating the lateral femoral cortex, which depicts differences in stress with or without a cortical defect. With a hole drilled through the femoral cortex, there is an approximately 2.7-fold increase in stress in the region of the defect (see inset).
IATROGENIC SUbTROCHANTERIC FEMORAL FRACTURE

ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 47
MANUSCRIPTS
from our laboratory by Burstein et al. demonstrated in a rabbit model that torsional strength of the femur that had been penetrated by a screw was not different than a control after eight weeks22. It may be possible that some ISFs may be associated with a reduced ability of bone adaptation in the vicinity of the hole.
ISFs are more commonly observed after internal fixation for femoral neck fractures, and various studies evaluated surgical technique to improve stability of the fixation. Jansen, et al., has pointed out that there is no consensus for such techniques as data are conflicting regarding screw type, number of screws, or screw insertion patterns7. A handful of retrospective studies have suggested techniques to reduce ISFs without strong evidence. Reducing the number of holes formed by drilling or pinning has been suggested as a way to reduce the occurrence of iatrogenic fractures1,
23-25, 27, 28. Karr recommended protected or non-weight bearing after surgery as a possible means of reducing ISFs25. Based on retrospective analysis, others have recommended the placement of screws no lower than the lesser trochanter as many of their ISFs demonstrated low insertion of screws1, 23, 25, 28. If inserting three screws, orienting the screws in an upside-down triangle configuration was suggested by Kloen, Neumann, and more recently by Pelet1, 28, 35. Comparatively, only a limited number of experimental studies have addressed surgical technique with regard to reducing subtrochanteric fractures. Oakey et al. showed that screws inserted in an upside-down (apex distal) triangle pattern was capable of withstanding greater loads than screws in a right-side-up triangle pattern in monotonic load to failure30. Lichtblau et al. attempted a similar experiment comparing a right-side-up triangle pattern (the horizontal group) to a triangle pattern where no two screws
were on the same transverse plane (the vertical group) 45. While the vertical group in that study did not demonstrate greater stiffness or failure loads compared to the horizontal group, there were a statistically greater number of subtrochanteric fractures during monotonic loading to failure for the horizontal group (6 of 11) compared to the vertical group (0 of 11).
The recommendations to reduce ISFs call for more proximal placement of screws in lateral femoral cortex, but only one experimental study tests this hypothesis46. Stafford et al. found that extra screw or pin holes did not affect failure mode and had no affect on stability of the construct. On the other hand, unused holes are reported to have been associated with fractures in clinical case reports4. Additionally, Stafford et al. found that while lower screw placement was correlated with a less stiff construct, placement even 20 mm below the lesser trochanter did not cause subtrochanteric fractures in their biomechanical model.
ConclusionsThe current literature demonstrates that a small subset of patients experience ISFs, a serious complication after operations that disrupt the lateral femoral cortex. The conflicting data as well as lack of clear evidence for reducing ISFs represents a deficiency in the body of knowledge in this subject area. Computer simulations have demonstrated the tension on the lateral femoral cortex during normal gait as well as the stress riser effect of the cortical defect created during surgery. However, there is little evidence for surgical techniques to prevent this catastrophic complication based on biomechanical data. The vast majority of recommendations are still level v data based on retrospective case reports. Most instances of ISFs reported in literature are in patients who underwent internal fixation for femoral neck fractures. Since only two reports of ISFs have been reported in the setting
of core decompression for AvN and only scant reports of patients sustaining an ISF after fixation of SCFE are available, the incidence is likely very low, which could be explained by the younger average age of patients who experience AvN and SCFE. Surgical intervention for AvN and SCFE both violate the lateral femoral cortex, similar to interventions for hip fractures, thus further demonstrating the need for a better understanding about the effects of cortical defects and placement of surgical fixation in the lateral femoral cortex.
Future studies should determine the biomechanical relationships between surgical technique and ISFs. Current recommendations for insertion of surgical implants in hip fractures and SCFE are that the most distal screw not be insert below the lesser trochanter1, 4, though the only experimental study that evaluates lateral screw height failed to produce any subtrochanteric fractures46. A few studies have shown improvement with upside-down triangle screw pattern for internal fixation of hip fractures, but those studies were performed in monotonic loading, even though crack initiation and propagation appears to be a significant contributing factor. Further study needs to be undertaken to better understand ISF complications and reduce their occurrence after surgery.
References1. Kloen, P., et al., Subtrochanteric fracture
after cannulated screw fixation of femoral neck fractures: a report of four cases. J Orthop Trauma, 2003. 17(3): p. 225-9.
2. Fung, D.A., et al., Subtrochanteric fracture in a patient with trabecular metal osteonecrosis intervention implant. Orthopedics, 2008. 31(6): p. 614.
3. Stronach, B.M., et al., Subtrochanteric femur fracture after core decompression and placement of a tantalum strut for osteonecrosis of the femoral head. J Arthroplasty, 2010. 25(7): p. 1168 e5-7.
4. Canale, S.T., et al., Subtrochanteric fracture after fixation of slipped capital femoral epiphysis: a complication of unused drill holes. J Pediatr Orthop, 1994. 14(5): p. 623-6.
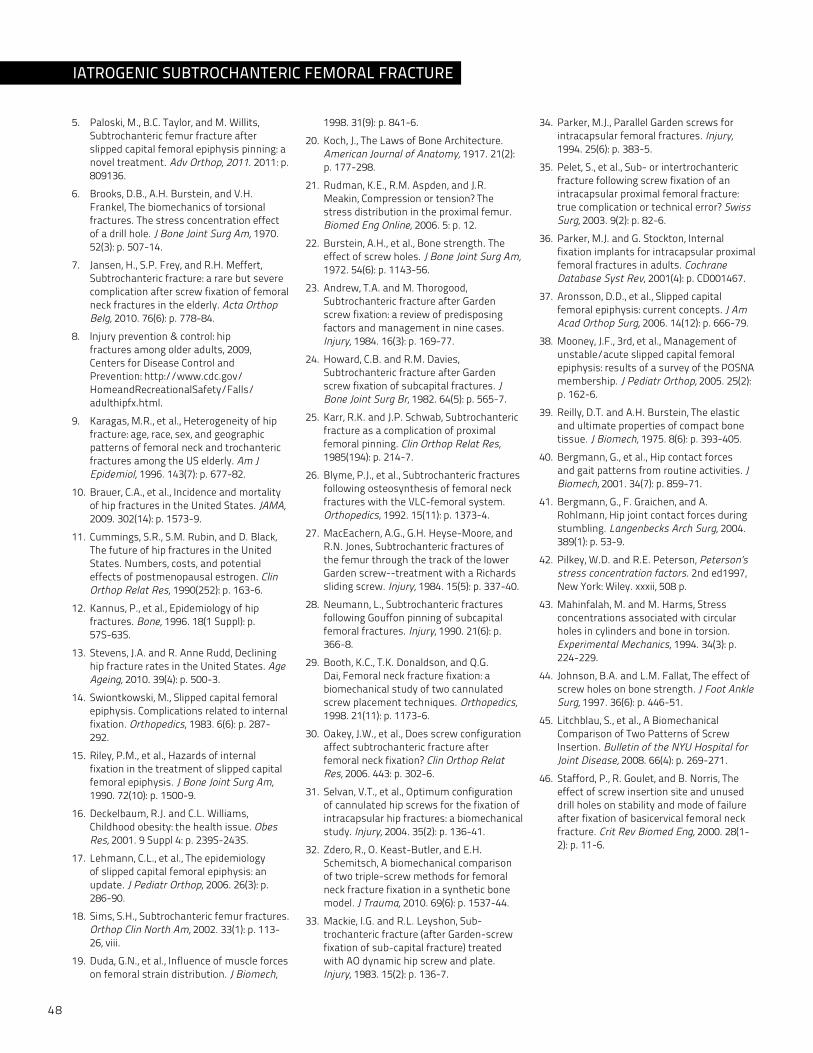
48
5. Paloski, M., B.C. Taylor, and M. Willits, Subtrochanteric femur fracture after slipped capital femoral epiphysis pinning: a novel treatment. Adv Orthop, 2011. 2011: p. 809136.
6. Brooks, D.B., A.H. Burstein, and v.H. Frankel, The biomechanics of torsional fractures. The stress concentration effect of a drill hole. J Bone Joint Surg Am, 1970. 52(3): p. 507-14.
7. Jansen, H., S.P. Frey, and R.H. Meffert, Subtrochanteric fracture: a rare but severe complication after screw fixation of femoral neck fractures in the elderly. Acta Orthop Belg, 2010. 76(6): p. 778-84.
8. Injury prevention & control: hip fractures among older adults, 2009, Centers for Disease Control and Prevention: http://www.cdc.gov/HomeandRecreationalSafety/Falls/adulthipfx.html.
9. Karagas, M.R., et al., Heterogeneity of hip fracture: age, race, sex, and geographic patterns of femoral neck and trochanteric fractures among the US elderly. Am J Epidemiol, 1996. 143(7): p. 677-82.
10. Brauer, C.A., et al., Incidence and mortality of hip fractures in the United States. JAMA, 2009. 302(14): p. 1573-9.
11. Cummings, S.R., S.M. Rubin, and D. Black, The future of hip fractures in the United States. Numbers, costs, and potential effects of postmenopausal estrogen. Clin Orthop Relat Res, 1990(252): p. 163-6.
12. Kannus, P., et al., Epidemiology of hip fractures. Bone, 1996. 18(1 Suppl): p. 57S-63S.
13. Stevens, J.A. and R. Anne Rudd, Declining hip fracture rates in the United States. Age Ageing, 2010. 39(4): p. 500-3.
14. Swiontkowski, M., Slipped capital femoral epiphysis. Complications related to internal fixation. Orthopedics, 1983. 6(6): p. 287-292.
15. Riley, P.M., et al., Hazards of internal fixation in the treatment of slipped capital femoral epiphysis. J Bone Joint Surg Am, 1990. 72(10): p. 1500-9.
16. Deckelbaum, R.J. and C.L. Williams, Childhood obesity: the health issue. Obes Res, 2001. 9 Suppl 4: p. 239S-243S.
17. Lehmann, C.L., et al., The epidemiology of slipped capital femoral epiphysis: an update. J Pediatr Orthop, 2006. 26(3): p. 286-90.
18. Sims, S.H., Subtrochanteric femur fractures. Orthop Clin North Am, 2002. 33(1): p. 113-26, viii.
19. Duda, G.N., et al., Influence of muscle forces on femoral strain distribution. J Biomech,
1998. 31(9): p. 841-6.
20. Koch, J., The Laws of Bone Architecture. American Journal of Anatomy, 1917. 21(2): p. 177-298.
21. Rudman, K.E., R.M. Aspden, and J.R. Meakin, Compression or tension? The stress distribution in the proximal femur. Biomed Eng Online, 2006. 5: p. 12.
22. Burstein, A.H., et al., Bone strength. The effect of screw holes. J Bone Joint Surg Am, 1972. 54(6): p. 1143-56.
23. Andrew, T.A. and M. Thorogood, Subtrochanteric fracture after Garden screw fixation: a review of predisposing factors and management in nine cases. Injury, 1984. 16(3): p. 169-77.
24. Howard, C.B. and R.M. Davies, Subtrochanteric fracture after Garden screw fixation of subcapital fractures. J Bone Joint Surg Br, 1982. 64(5): p. 565-7.
25. Karr, R.K. and J.P. Schwab, Subtrochanteric fracture as a complication of proximal femoral pinning. Clin Orthop Relat Res, 1985(194): p. 214-7.
26. Blyme, P.J., et al., Subtrochanteric fractures following osteosynthesis of femoral neck fractures with the vLC-femoral system. Orthopedics, 1992. 15(11): p. 1373-4.
27. MacEachern, A.G., G.H. Heyse-Moore, and R.N. Jones, Subtrochanteric fractures of the femur through the track of the lower Garden screw--treatment with a Richards sliding screw. Injury, 1984. 15(5): p. 337-40.
28. Neumann, L., Subtrochanteric fractures following Gouffon pinning of subcapital femoral fractures. Injury, 1990. 21(6): p. 366-8.
29. Booth, K.C., T.K. Donaldson, and Q.G. Dai, Femoral neck fracture fixation: a biomechanical study of two cannulated screw placement techniques. Orthopedics, 1998. 21(11): p. 1173-6.
30. Oakey, J.W., et al., Does screw configuration affect subtrochanteric fracture after femoral neck fixation? Clin Orthop Relat Res, 2006. 443: p. 302-6.
31. Selvan, v.T., et al., Optimum configuration of cannulated hip screws for the fixation of intracapsular hip fractures: a biomechanical study. Injury, 2004. 35(2): p. 136-41.
32. Zdero, R., O. Keast-Butler, and E.H. Schemitsch, A biomechanical comparison of two triple-screw methods for femoral neck fracture fixation in a synthetic bone model. J Trauma, 2010. 69(6): p. 1537-44.
33. Mackie, I.G. and R.L. Leyshon, Sub-trochanteric fracture (after Garden-screw fixation of sub-capital fracture) treated with AO dynamic hip screw and plate. Injury, 1983. 15(2): p. 136-7.
34. Parker, M.J., Parallel Garden screws for intracapsular femoral fractures. Injury, 1994. 25(6): p. 383-5.
35. Pelet, S., et al., Sub- or intertrochanteric fracture following screw fixation of an intracapsular proximal femoral fracture: true complication or technical error? Swiss Surg, 2003. 9(2): p. 82-6.
36. Parker, M.J. and G. Stockton, Internal fixation implants for intracapsular proximal femoral fractures in adults. Cochrane Database Syst Rev, 2001(4): p. CD001467.
37. Aronsson, D.D., et al., Slipped capital femoral epiphysis: current concepts. J Am Acad Orthop Surg, 2006. 14(12): p. 666-79.
38. Mooney, J.F., 3rd, et al., Management of unstable/acute slipped capital femoral epiphysis: results of a survey of the POSNA membership. J Pediatr Orthop, 2005. 25(2): p. 162-6.
39. Reilly, D.T. and A.H. Burstein, The elastic and ultimate properties of compact bone tissue. J Biomech, 1975. 8(6): p. 393-405.
40. Bergmann, G., et al., Hip contact forces and gait patterns from routine activities. J Biomech, 2001. 34(7): p. 859-71.
41. Bergmann, G., F. Graichen, and A. Rohlmann, Hip joint contact forces during stumbling. Langenbecks Arch Surg, 2004. 389(1): p. 53-9.
42. Pilkey, W.D. and R.E. Peterson, Peterson’s stress concentration factors. 2nd ed1997, New york: Wiley. xxxii, 508 p.
43. Mahinfalah, M. and M. Harms, Stress concentrations associated with circular holes in cylinders and bone in torsion. Experimental Mechanics, 1994. 34(3): p. 224-229.
44. Johnson, B.A. and L.M. Fallat, The effect of screw holes on bone strength. J Foot Ankle Surg, 1997. 36(6): p. 446-51.
45. Litchblau, S., et al., A Biomechanical Comparison of Two Patterns of Screw Insertion. Bulletin of the NYU Hospital for Joint Disease, 2008. 66(4): p. 269-271.
46. Stafford, P., R. Goulet, and B. Norris, The effect of screw insertion site and unused drill holes on stability and mode of failure after fixation of basicervical femoral neck fracture. Crit Rev Biomed Eng, 2000. 28(1-2): p. 11-6.
IATROGENIC SUbTROCHANTERIC FEMORAL FRACTURE

ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 49
MANUSCRIPTS
Introduction Metastatic disease of the spine is a cause for great morbidity in patients with cancer. The spine is the third most common site for metastases (following the liver and lung) and the most common within the skeleton. At autopsy, 50% of cancer patients will have evidence of spinal metastases. One-third of all patients with cancer will develop symptomatic spinal metastases, numbering nearly 20,000 new cases annually1. Twenty percent of those with symptomatic spine metastases will present with epidural compression and some degree of neurologic dysfunction, ranging from weakness to paralysis2.
Radiation therapy is effective for many symptomatic spinal metastases in patients with radiosensitive primary tumors and whose spinal stability has not been compromised. Surgery is reserved for patients with radio-resistant tumors, those who have reached a maximum dose of radiation, and when metastatic disease has rendered the spinal column unstable. The goals of surgery are to debulk the tumor burden from the neural elements and to provide mechanical stability. Surgery is palliative in nature and involves procedures of considerable magnitude with the potential for significant morbidity. Patients who undergo surgery have limited life expectancy and have numerous medical co-morbidities and
may be severely deconditioned. However, over the past two decades, surgical techniques have evolved significantly, especially with improvement in anterior and posterior instrumentation. Surgery has become the standard treatment for most patients with advanced metastatic disease of the spine, with proven efficacy in preserving and restoring neurologic function.3-8 A patient with progressive neurologic deterioration due to metastatic epidural compression poses unique challenges. In this circumstance, no other valid options exist and the decision to proceed with surgery must be made quickly. Many factors must be considered when proceeding with surgery, foremost are the likelihood of neurologic improvement and the potential for prolonged survival.
The goal of this study was to evaluate clinical outcomes of patients with progressive neurologic deterioration who underwent emergent surgery to treat to epidural compression and spinal instability resulting from metastatic disease. A particular effort was made to identify prognostic factors associated with improvement in neurologic function following surgery. Further clarification of these factors can shape future surgical strategies and may assist with education of patients and provide a more clear understanding of the expectations of surgery.
MethodsThe study evaluated 46 consecutive patients who presented to Case Medical Center over a 6 year period (2002-2007) with spinal metastases and epidural compression which caused progressive deterioration in neurologic function. Progressive neurologic deterioration was defined as worsening function documented to have occurred over a 72 hour period. All patients were hospitalized at Case Medical Center at the time of their initial evaluation by the Orthopedic Spine Service. Each patient was either an in-patient on the Oncology Service or had been transferred to the Spine Service directly from an outside institution. In each case, radiation therapy was not a viable option because the primary tumor was radio-resistant, maximum radiation had previously been delivered, there was evidence of spinal instability, or a combination of these factors existed.
There were 34 women and 12 men. The mean age of the patients was 56.6 years (range: 42 – 82 years). The primary tumor was renal cell in 12 patients (26%), lung in 11 patients (24%), breast in 9 patients (20%), prostate in 8 (17%), gastrointestinal in 4 (9%), and 2 patients had an unknown primary tumor (4%). Patients with myeloma or lymphoma were excluded, as they had a systemic hematologic disease, rather than true metastatic disease. The mean time for appearance of spinal
EMERGENT SURGICAL MANAGEMENT FOR SPINAL METASTASES AND NEUROLOGIC DETERIORATIONChristopher G. Furey, MD1, Katherine H. Sadowski, BS1, Nicholas U. Ahn, MD1, Jung U. yoo, MD2, Sanford E. Emery, MD3
1 Department of Orthopedic Surgery, Case Western Reserve University, Case Medical Center2 Department of Orthopedic Surgery, Oregon Health and Science University3 Department of Orthopedic Surgery, West virginia University

50
metastases from the time of the original diagnosis of malignancy was 12.4 months (range: 0-28 months). The pre-operative neurologic status, employing the ASIA criteria (Table 1) was ASIA B in 29 patients (63%), ASIA C in 12 (26%), and ASIA D in 5 (10%). The location of the metastatic lesion was the thoracic spine in 40 patients (87%) and the lumbar spine in 6 (13%). The location of maximum neural compression to the spinal cord or cauda equine was anterior in 26 patients (56%), posterior in 7 (15%), and circumferential in 13 (28%). A pathologic fracture or spinal instability was present in 32 patients (70%). Thirty patients (65%) had undergone prior fractionated, external beam radiation therapy (XRT) to the region of epidural compression. Further radiation was not deemed an option in each of these patients because either a maximal therapeutic dose had been reached (18 patients) or because the initial XRT had not been effective in arresting the patient’s neurologic decline (12 patients). The patient’s general condition was defined with the Tomita criteria.9 In this system, a numeric score is generated based on the aggressiveness of the
primary tumor, the presence of other skeletal metastases, and the presence of visceral metastases; a score of 2 to 10 is generated, with higher scores carrying worse prognosis. The mean Tomita score of the patients in this cohort was 6 (range: 4-10).
The surgical approach was made at the discretion of the
primary surgeon. The location of the tumor and resulting direction of neural compression, the degree of kyphosis, the presence of a pathologic fracture and the patient’s overall medical condition were the main considerations in choosing the surgical approach. A laminectomy alone was employed when the majority of tumor burden was posterior and there was no existing or impending pathologic fracture or instability. Posterior fusion with instrumentation was performed in the presence of fractures or instability. An anterior decompression and structural grafting was added when severe kyphosis was present. Three patients (7%) underwent laminectomy alone, 33 (79%) underwent a posterior decompression and instrumented fusion, and 6 (14%) underwent a circumferential procedure with an anterior decompression and strut grafting followed by a posterior instrumented fusion.
Multiple prognostic factors were considered, including gender, age (younger than 55 years or older than 56 based on the mean age of 56), type of primary tumor, pre-operative ASIA Grade, the
use of pre-operative radiation therapy, time from diagnosis of malignancy to the development of spine metastases (longer than 12 months or shorter than 11 months based on mean of 12.4 months), and the Tomita score (greater than 6 or less than 5 based on the mean of 6). As well, the five most common medical co-morbidities of the cohort were evaluated, diabetes, coronary disease, hypertension, COPD, and smoking. The length of pre-operative hospitalization, the type of surgical procedure, the occurrence of a post-operative complication, and the use of post-operative radiation therapy were also assessed.
Results The mean post-operative survival was 8.9 months (range: 2 weeks - 60 months). Four patients (10%) died within 6 weeks of surgery. Thirty-three patients (72%) regained the ability to ambulate following surgery. Survival was significantly longer in patients who regained the ability to ambulate (mean survival: 12.2 months) compared with those who did not ambulate post-operatively (mean survival: 2.3 months) (p=0.03). Thirty-six patients (78%) had neurologic improvement of at least one ASIA grade, 7 (15%) did not improve, and 3 (7%) regressed a single ASIA grade. According to the multivariate analysis, the ability to regain ambulation was associated with age < 65 years, less severe neurologic deficit (ASIA C or D), pre-surgical hospitalization less than 48 hours, a pre-operative Tomita score of less than 6 and patients who did not suffer a post-operative complication (Table 2). Pertinent factors not significantly affecting survival or the ability to ambulate included gender, type of primary malignancy, any of the medical co-morbidities, tumor location, and the type of surgical procedure.
Peri-operative medical complications occurred in 6 patients (14%), including 2 with pulmonary emboli, 2 with respiratory failure requiring mechanical
Grade A : “complete” spinal cord injury where no motor or sensory function is preserved in the sacral segments S4-S5
Grade B : “incomplete” spinal cord injury where sensory but not motor function is preserved below the neurological level and includes the sacral segments S4-S5
Grade C : “incomplete” spinal cord injury where motor function is preserved below the neurological level and more than half of key muscles below the neurological level have a muscle grade of less than 3, which indicates active movement with full range of motion against gravity
Grade D : “incomplete” spinal cord injury where motor function is preserved below the neurological level and at least half of the key muscles below the neurological level have a muscle grade of 3 or more
Grade E : motor and sensory function are normal
Table 1. The ASIA criteria.
EMERGENT SURGICAL MANAGEMENT
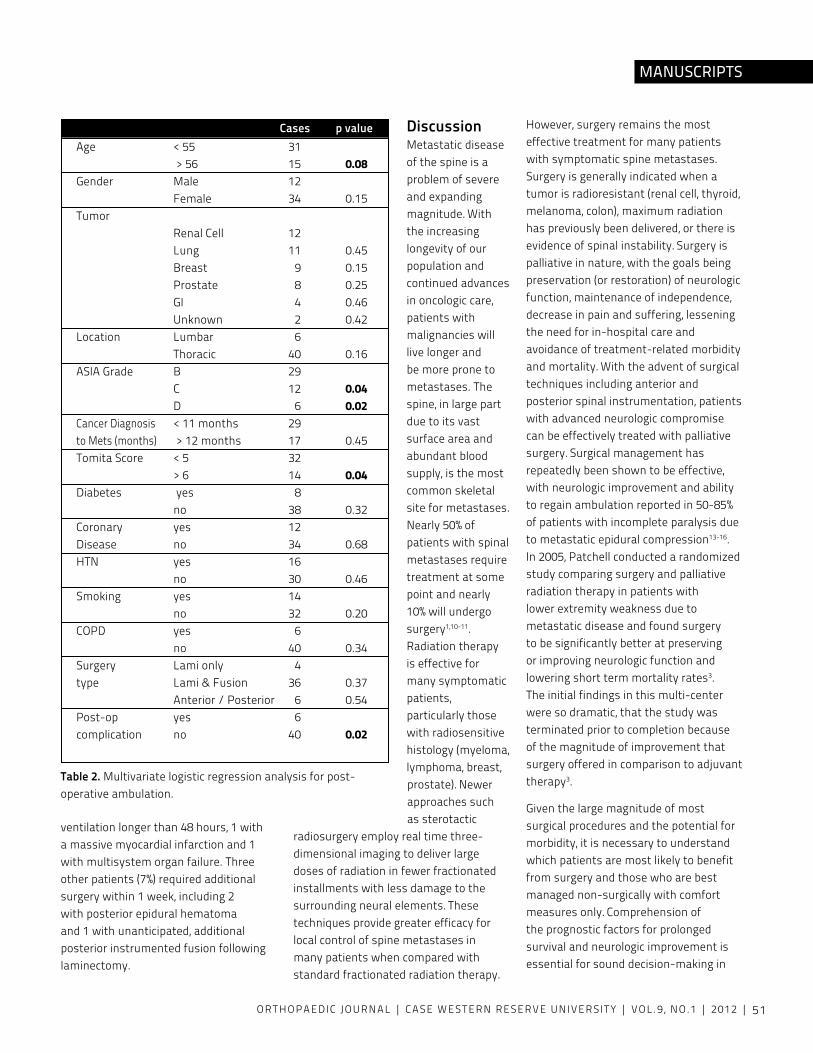
ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 51
MANUSCRIPTS
ventilation longer than 48 hours, 1 with a massive myocardial infarction and 1 with multisystem organ failure. Three other patients (7%) required additional surgery within 1 week, including 2 with posterior epidural hematoma and 1 with unanticipated, additional posterior instrumented fusion following laminectomy.
Discussion Metastatic disease of the spine is a problem of severe and expanding magnitude. With the increasing longevity of our population and continued advances in oncologic care, patients with malignancies will live longer and be more prone to metastases. The spine, in large part due to its vast surface area and abundant blood supply, is the most common skeletal site for metastases.
Nearly 50% of patients with spinal metastases require treatment at some point and nearly 10% will undergo surgery1,10-11. Radiation therapy is effective for many symptomatic patients, particularly those with radiosensitive histology (myeloma, lymphoma, breast, prostate). Newer approaches such as sterotactic
radiosurgery employ real time three-dimensional imaging to deliver large doses of radiation in fewer fractionated installments with less damage to the surrounding neural elements. These techniques provide greater efficacy for local control of spine metastases in many patients when compared with standard fractionated radiation therapy.
However, surgery remains the most effective treatment for many patients with symptomatic spine metastases. Surgery is generally indicated when a tumor is radioresistant (renal cell, thyroid, melanoma, colon), maximum radiation has previously been delivered, or there is evidence of spinal instability. Surgery is palliative in nature, with the goals being preservation (or restoration) of neurologic function, maintenance of independence, decrease in pain and suffering, lessening the need for in-hospital care and avoidance of treatment-related morbidity and mortality. With the advent of surgical techniques including anterior and posterior spinal instrumentation, patients with advanced neurologic compromise can be effectively treated with palliative surgery. Surgical management has repeatedly been shown to be effective, with neurologic improvement and ability to regain ambulation reported in 50-85% of patients with incomplete paralysis due to metastatic epidural compression13-16. In 2005, Patchell conducted a randomized study comparing surgery and palliative radiation therapy in patients with lower extremity weakness due to metastatic disease and found surgery to be significantly better at preserving or improving neurologic function and lowering short term mortality rates3.The initial findings in this multi-center were so dramatic, that the study was terminated prior to completion because of the magnitude of improvement that surgery offered in comparison to adjuvant therapy3.
Given the large magnitude of most surgical procedures and the potential for morbidity, it is necessary to understand which patients are most likely to benefit from surgery and those who are best managed non-surgically with comfort measures only. Comprehension of the prognostic factors for prolonged survival and neurologic improvement is essential for sound decision-making in
Cases p value Age < 55 31 > 56 15 0.08 Gender Male 12 Female 34 0.15 Tumor Renal Cell 12 Lung 11 0.45 Breast 9 0.15 Prostate 8 0.25 GI 4 0.46 Unknown 2 0.42 Location Lumbar 6 Thoracic 40 0.16 ASIA Grade B 29 C 12 0.04 D 6 0.02 Cancer Diagnosis < 11 months 29 to Mets (months) > 12 months 17 0.45 Tomita Score < 5 32 > 6 14 0.04 Diabetes yes 8 no 38 0.32 Coronary yes 12 Disease no 34 0.68 HTN yes 16 no 30 0.46 Smoking yes 14 no 32 0.20 COPD yes 6 no 40 0.34 Surgery Lami only 4 type Lami & Fusion 36 0.37 Anterior / Posterior 6 0.54 Post-op yes 6 complication no 40 0.02
Table 2. Multivariate logistic regression analysis for post-operative ambulation.
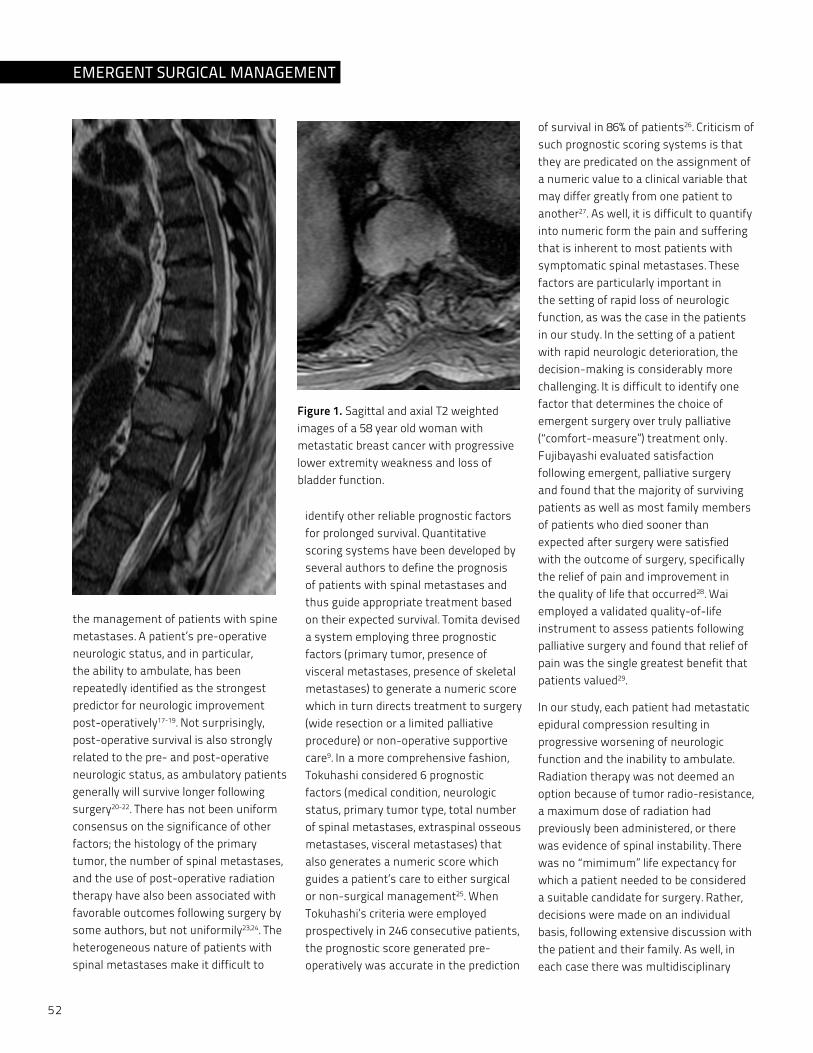
52
the management of patients with spine metastases. A patient’s pre-operative neurologic status, and in particular, the ability to ambulate, has been repeatedly identified as the strongest predictor for neurologic improvement post-operatively17-19. Not surprisingly, post-operative survival is also strongly related to the pre- and post-operative neurologic status, as ambulatory patients generally will survive longer following surgery20-22. There has not been uniform consensus on the significance of other factors; the histology of the primary tumor, the number of spinal metastases, and the use of post-operative radiation therapy have also been associated with favorable outcomes following surgery by some authors, but not uniformily23,24. The heterogeneous nature of patients with spinal metastases make it difficult to
identify other reliable prognostic factors for prolonged survival. Quantitative scoring systems have been developed by several authors to define the prognosis of patients with spinal metastases and thus guide appropriate treatment based on their expected survival. Tomita devised a system employing three prognostic factors (primary tumor, presence of visceral metastases, presence of skeletal metastases) to generate a numeric score which in turn directs treatment to surgery (wide resection or a limited palliative procedure) or non-operative supportive care9. In a more comprehensive fashion, Tokuhashi considered 6 prognostic factors (medical condition, neurologic status, primary tumor type, total number of spinal metastases, extraspinal osseous metastases, visceral metastases) that also generates a numeric score which guides a patient’s care to either surgical or non-surgical management25. When Tokuhashi’s criteria were employed prospectively in 246 consecutive patients, the prognostic score generated pre-operatively was accurate in the prediction
of survival in 86% of patients26. Criticism of such prognostic scoring systems is that they are predicated on the assignment of a numeric value to a clinical variable that may differ greatly from one patient to another27. As well, it is difficult to quantify into numeric form the pain and suffering that is inherent to most patients with symptomatic spinal metastases. These factors are particularly important in the setting of rapid loss of neurologic function, as was the case in the patients in our study. In the setting of a patient with rapid neurologic deterioration, the decision-making is considerably more challenging. It is difficult to identify one factor that determines the choice of emergent surgery over truly palliative (“comfort-measure”) treatment only. Fujibayashi evaluated satisfaction following emergent, palliative surgery and found that the majority of surviving patients as well as most family members of patients who died sooner than expected after surgery were satisfied with the outcome of surgery, specifically the relief of pain and improvement in the quality of life that occurred28. Wai employed a validated quality-of-life instrument to assess patients following palliative surgery and found that relief of pain was the single greatest benefit that patients valued29.
In our study, each patient had metastatic epidural compression resulting in progressive worsening of neurologic function and the inability to ambulate. Radiation therapy was not deemed an option because of tumor radio-resistance, a maximum dose of radiation had previously been administered, or there was evidence of spinal instability. There was no “mimimum” life expectancy for which a patient needed to be considered a suitable candidate for surgery. Rather, decisions were made on an individual basis, following extensive discussion with the patient and their family. As well, in each case there was multidisciplinary
Figure 1. Sagittal and axial T2 weighted images of a 58 year old woman with metastatic breast cancer with progressive lower extremity weakness and loss of bladder function.
EMERGENT SURGICAL MANAGEMENT
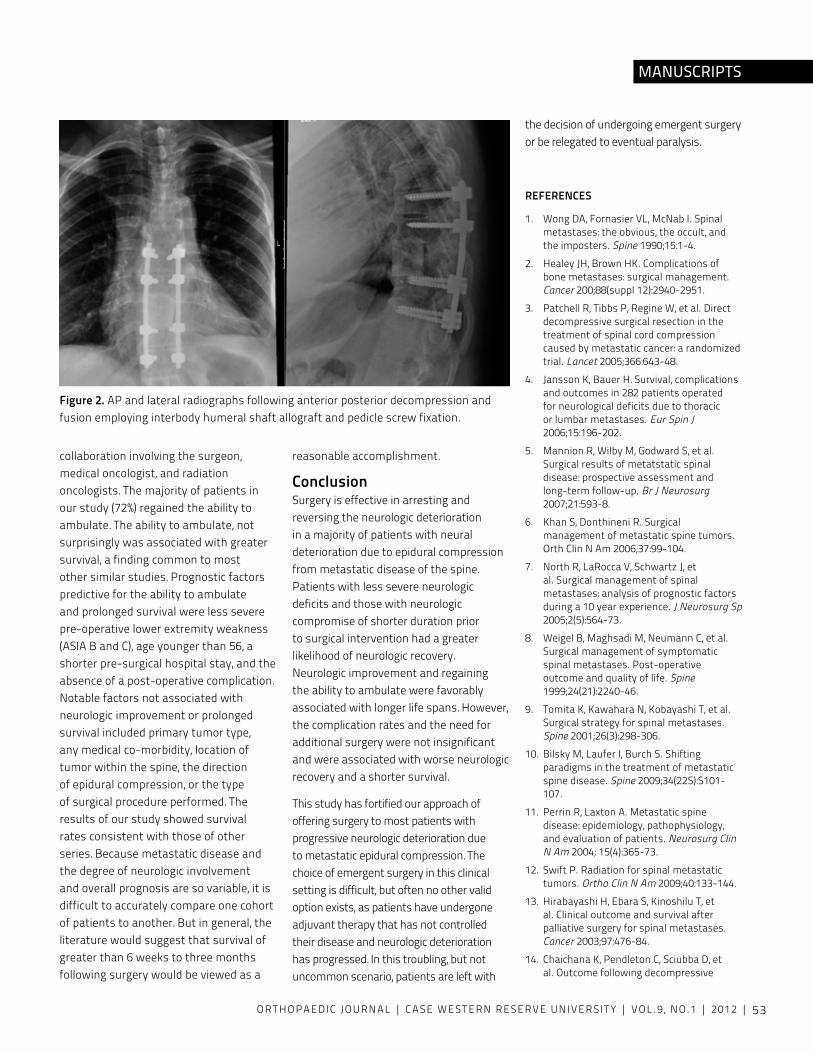
ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 53
MANUSCRIPTS
collaboration involving the surgeon, medical oncologist, and radiation oncologists. The majority of patients in our study (72%) regained the ability to ambulate. The ability to ambulate, not surprisingly was associated with greater survival, a finding common to most other similar studies. Prognostic factors predictive for the ability to ambulate and prolonged survival were less severe pre-operative lower extremity weakness (ASIA B and C), age younger than 56, a shorter pre-surgical hospital stay, and the absence of a post-operative complication. Notable factors not associated with neurologic improvement or prolonged survival included primary tumor type, any medical co-morbidity, location of tumor within the spine, the direction of epidural compression, or the type of surgical procedure performed. The results of our study showed survival rates consistent with those of other series. Because metastatic disease and the degree of neurologic involvement and overall prognosis are so variable, it is difficult to accurately compare one cohort of patients to another. But in general, the literature would suggest that survival of greater than 6 weeks to three months following surgery would be viewed as a
reasonable accomplishment.
ConclusionSurgery is effective in arresting and reversing the neurologic deterioration in a majority of patients with neural deterioration due to epidural compression from metastatic disease of the spine. Patients with less severe neurologic deficits and those with neurologic compromise of shorter duration prior to surgical intervention had a greater likelihood of neurologic recovery. Neurologic improvement and regaining the ability to ambulate were favorably associated with longer life spans. However, the complication rates and the need for additional surgery were not insignificant and were associated with worse neurologic recovery and a shorter survival.
This study has fortified our approach of offering surgery to most patients with progressive neurologic deterioration due to metastatic epidural compression. The choice of emergent surgery in this clinical setting is difficult, but often no other valid option exists, as patients have undergone adjuvant therapy that has not controlled their disease and neurologic deterioration has progressed. In this troubling, but not uncommon scenario, patients are left with
the decision of undergoing emergent surgery or be relegated to eventual paralysis.
REFERENCES
1. Wong DA, Fornasier vL, McNab I. Spinal metastases: the obvious, the occult, and
the imposters. Spine 1990;15:1-4.
2. Healey JH, Brown HK. Complications of bone metastases: surgical management. Cancer 200;88(suppl 12):2940-2951.
3. Patchell R, Tibbs P, Regine W, et al. Direct decompressive surgical resection in the treatment of spinal cord compression caused by metastatic cancer: a randomized trial. Lancet 2005;366:643-48.
4. Jansson K, Bauer H. Survival, complications and outcomes in 282 patients operated for neurological deficits due to thoracic or lumbar metastases. Eur Spin J 2006;15:196-202.
5. Mannion R, Wilby M, Godward S, et al. Surgical results of metatstatic spinal disease: prospective assessment and long-term follow-up. Br J Neurosurg 2007;21:593-8.
6. Khan S, Donthineni R. Surgical management of metastatic spine tumors. Orth Clin N Am 2006;37:99-104.
7. North R, LaRocca v, Schwartz J, et al. Surgical management of spinal metastases: analysis of prognostic factors during a 10 year experience. J Neurosurg Sp 2005;2(5):564-73.
8. Weigel B, Maghsadi M, Neumann C, et al. Surgical management of symptomatic spinal metastases. Post-operative outcome and quality of life. Spine 1999;24(21):2240-46.
9. Tomita K, Kawahara N, Kobayashi T, et al. Surgical strategy for spinal metastases. Spine 2001;26(3):298-306.
10. Bilsky M, Laufer I, Burch S. Shifting paradigms in the treatment of metastatic spine disease. Spine 2009;34(22S):S101-107.
11. Perrin R, Laxton A. Metastatic spine disease: epidemiology, pathophysiology, and evaluation of patients. Neurosurg Clin N Am 2004; 15(4):365-73.
12. Swift P. Radiation for spinal metastatic tumors. Ortho Clin N Am 2009;40:133-144.
13. Hirabayashi H, Ebara S, Kinoshilu T, et al. Clinical outcome and survival after palliative surgery for spinal metastases. Cancer 2003;97:476-84.
14. Chaichana K, Pendleton C, Sciubba D, et al. Outcome following decompressive
Figure 2. AP and lateral radiographs following anterior posterior decompression and fusion employing interbody humeral shaft allograft and pedicle screw fixation.
54
surgery for different histological types of metastatic tumors causing epidural spinal cord compression. J Neurosurg Sp 2009;11:56-63.
15. Klimo P, Thompson C, Kestle, Schmidt M. A meta-analysis of surgery versus conventional radiotherapy for the treatment of metastatic spinal epidural disease. Neuro Oncol 2005;7:64-76.
16. Li H, Gasbarrini A Cappuccio M, et al. Outcome of excisional surgeries for patients with spinal metastases. Eur Spine J 2009;18:1423-30.
17. Putz C, Wiedehofer B, Geran H, et al. Tokuhashi prognosis score: an important tool in prediction of the neurologic outcome in mestastatic spinal cord compression. Spine 2008;33:2669-74.
18. Chaichan B, Woodworth G, Sciubba D, et al. Predictors of ambulatory function after decompressive surgery for metastatic epidural spinal cord compression. Neurosurg 2008;62(3):683-92.
19. Wise J, Fischgrund J, Herkowitz H, et al. Complications, survival rates and risk factors of surgery for metatstatic disease of the spine. Spine 1999;24:1943-51.
20. Douglas S, Huttenlocher S, Bajrovic A, et al. Prognostic factors for different outcomes in patients with metastatic spinal cord compression from cancer of unknown primary. Cancer 2012; published online.
21. Sundareson N, Galicich J, Lane J, et al. Treatment of neoplastic epidural cord compression by vertebral body resection and stabilization. J Neurosurg 1985;63:676-84.
22. Holman P, Suki D, McCutcheon I, et al. Surgical management of metastatic disease of the lumbar spine: experience with 139 patients. J Neurosurg Spine 2005;2:550-63.
23. Wibmer C, Leithner A, Hofmann G, et al. Survival analysis of 254 patients after manifestation of spinal metastases. Spine 2011;36(23):1977-86.
24. Sioutos P, Arbit E, Meshulam C, et al. Spinal metastases from solid tumors. Analysis of factors affecting survival. Cancer 1995;76:1453-59.
25. Tokuhashi y, Matsuzaki H, Toriyama S, et al. Scoring system for the preoperative evaluation of metastatic spine tumor prognosis. Spine 1990;15:1110-13.
26. Tokuhashi y, Matsuzaki H, Oda H, et al. A revised scoring system for preoperative evaluation of metastatic spine tumor prognosis. Spine 2005;30:2186-91.
27. Bauer H. Letter to the editor. Spine 2002;27(10):1124-25.
28. Fujibayahi S, Neo M, Miyaki K, et al. The value of palliative surgery for metastatic spinal disease: satisfaction of patients and their families. Spine J 2010;10(1):42-9.
29. Wai E, Finkelstein J, Tangente R, et al. Quality of life in surgical treatment of metastatic spine disease. Spine 2003;28(5):508-12.
EMERGENT SURGICAL MANAGEMENT
ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 55
MANUSCRIPTS
AbstractActivating mutations in Fibroblast Growth Factor Receptor 3 (FGFR3) cause a number of skeletal dysplasias, such as achondroplasia, hypochondroplasia, and thanatophoric dysplasias. During the last decade, major advances have improved our understanding of the molecular mechanisms by which FGFR3 signaling controls cartilage development. These recent, novel insights offer a basis for developing new therapeutic strategies for FGFR3-related skeletal dysplasias.
IntroductionFibroblast growth factor (FGF) and FGF receptor (FGFR) signaling plays an important role in skeletal development. Activating mutations in FGFRs cause multiple skeletal disorders including chondrodysplasia and craniosynostosis 1-4. The most frequent FGF-related skeletal dysplasia is achondroplasia (ACH), caused by point mutations in the fibroblast growth factor receptor 3 (FGFR3) gene. Mutations in FGFR3 also cause a series of skeletal dysplasias, including hypochondroplasia (HCH); thanatophoric dysplasia type I (TDI) and type II (TDII); severe achondroplasia with developmental delay and acanthosis nigricans (SADDAN); and platyspondylic lethal skeletal dysplasias, San Diego type 5. In this review, we will summarize the recent progress in our understanding of the molecular mechanisms by which mutated FGFR3 causes skeletal dysplasias.
1. FGFR3 and its mutationsFGFR3 is one of four transmembrane FGF receptors that contain an extracellular ligand-binding domain, a transmembrane domain (TM), and an intracellular tyrosine kinase domain (Fig.1) 2,3,6. The extracellular region comprises three immunoglobulin-like domains (IgI, IgII, and IgIII). There are two tyrosine kinase (TK1, TK2) domains in the intracellular region (Fig. 1). Specific ligand FGFs bind to the IgII domain, together with heparin or heparan sulfate proteoglycans, and promote dimerization of two FGFR3 molecules. The TK1 domain phosphorylates the TK2 domain of the other receptor molecule, triggering intracellular signaling 7.
ACH is the most common short-limb dwarfism, characterized by short stature with disproportionately short arms and legs, genu varum, trident hands, exaggerated lumbar lordosis, congenital spinal canal and foramen magnum stenosis, megalencephaly, and characteristic facial features with frontal bossing and mid-facial hypoplasia3,8-11. The majority of ACH is caused by the G380R substitution in the TM domain, but G375C also causes the same skeletal phenotype 12. HCH presents with skeletal abnormalities similar to those of ACH, but the phenotype is milder. HCH is caused in about 70% of cases by the N540K substitution11,12. It is also caused by I538v substitution in the TK1 domain and K650N substitution in the TK2 domain8,11,13. In contrast to HCH, SADDAN dysplasia shows skeletal manifestations
that are more severe than those of ACH. SADDAN is accompanied by a profound developmental delay, structural abnormalities of the brain, hearing loss, and acanthosis nigricans5,9,13,14. SADDAN is caused by the K650M substitution in FGFR311,12,15.
TD is a neonatally lethal skeletal dysplasia characterized by micromelia, macrocrania, and thoracic hypoplasia16-19. TD has been classified into two distinct subtypes. While TDI is the most common subtype, characterized by curved femora and occasionally a cloverleaf skull18, TDII is characterized by short but straight femora and a cloverleaf skull20. Multiple mutations have been identified for TDI. These include cysteine substitutions in the extracellular domain (R240C, R248C, S249C, G370C, S371C, y373C) and stop codon mutations (X807C, X807R, X807G)21-24. In contrast to TDI, only one mutation (K650E in the TK2 domain) has been identified for TDII25.
While all of the above FGFR3-related skeletal disorders manifest as short-limb dwarfisms, the phenotypic severity ranges from relatively mild HCH to the neonatally lethal TD. This range has been shown to correlate with the varying degrees of receptor activation caused by a given mutation7,26. Biochemical studies have indicated that the receptor activity increases in the following order: wild-type < N540K (HCH) < G380R (ACH) << R248C (TDI) = y373C (TDI) < K650M (TDI) ≤ K650E (TDII)7.
FIBROBLAST GROWTH FACTOR RECEPTOR 3 SIGNALING IN SKELETAL DySPLASIA Zhijun Chen, MD, PhD1, and Shunichi Murakami, MD, PhD1,2
1Department of Orthopaedics, Case Western Reserve University2Division of General Medical Sciences, National Center for Regenerative Medicine, Case Western Reserve University
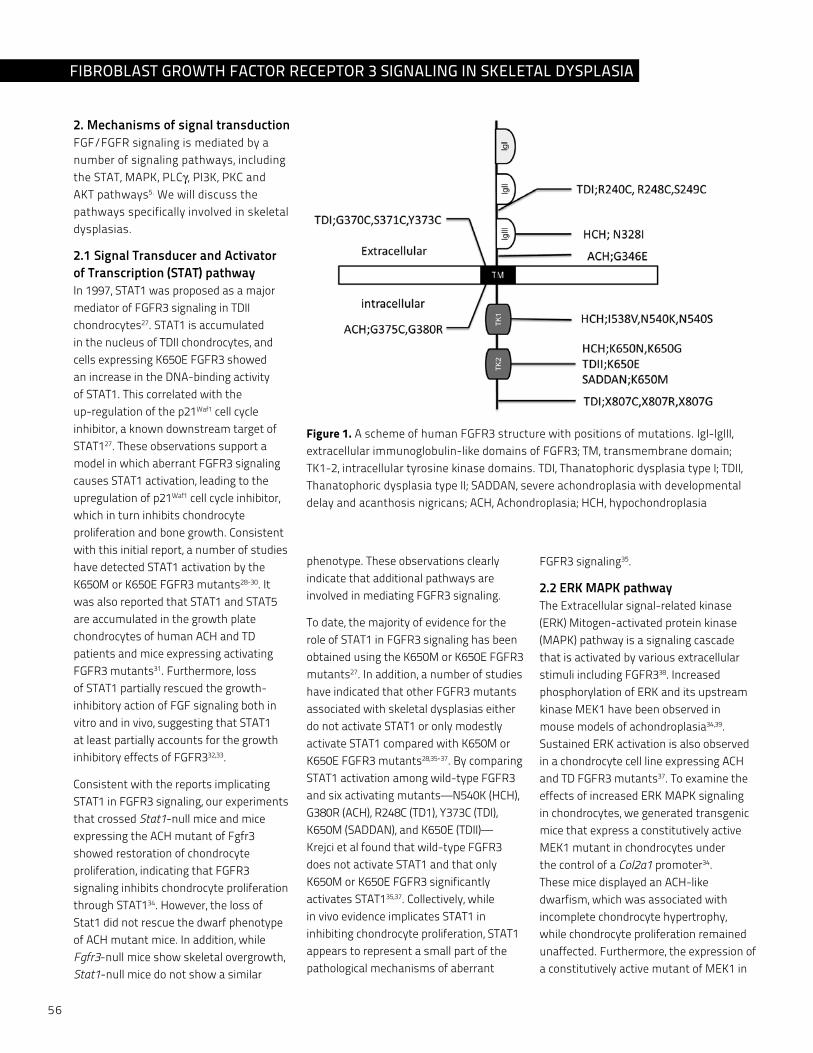
56
2. Mechanisms of signal transductionFGF/FGFR signaling is mediated by a number of signaling pathways, including the STAT, MAPK, PLCγ, PI3K, PKC and AKT pathways5. We will discuss the pathways specifically involved in skeletal dysplasias.
2.1 Signal Transducer and Activator of Transcription (STAT) pathway In 1997, STAT1 was proposed as a major mediator of FGFR3 signaling in TDII chondrocytes27. STAT1 is accumulated in the nucleus of TDII chondrocytes, and cells expressing K650E FGFR3 showed an increase in the DNA-binding activity of STAT1. This correlated with the up-regulation of the p21Waf1 cell cycle inhibitor, a known downstream target of STAT127. These observations support a model in which aberrant FGFR3 signaling causes STAT1 activation, leading to the upregulation of p21Waf1 cell cycle inhibitor, which in turn inhibits chondrocyte proliferation and bone growth. Consistent with this initial report, a number of studies have detected STAT1 activation by the K650M or K650E FGFR3 mutants28-30. It was also reported that STAT1 and STAT5 are accumulated in the growth plate chondrocytes of human ACH and TD patients and mice expressing activating FGFR3 mutants31. Furthermore, loss of STAT1 partially rescued the growth-inhibitory action of FGF signaling both in vitro and in vivo, suggesting that STAT1 at least partially accounts for the growth inhibitory effects of FGFR332,33.
Consistent with the reports implicating STAT1 in FGFR3 signaling, our experiments that crossed Stat1-null mice and mice expressing the ACH mutant of Fgfr3 showed restoration of chondrocyte proliferation, indicating that FGFR3 signaling inhibits chondrocyte proliferation through STAT134. However, the loss of Stat1 did not rescue the dwarf phenotype of ACH mutant mice. In addition, while Fgfr3-null mice show skeletal overgrowth, Stat1-null mice do not show a similar
phenotype. These observations clearly indicate that additional pathways are involved in mediating FGFR3 signaling.
To date, the majority of evidence for the role of STAT1 in FGFR3 signaling has been obtained using the K650M or K650E FGFR3 mutants27. In addition, a number of studies have indicated that other FGFR3 mutants associated with skeletal dysplasias either do not activate STAT1 or only modestly activate STAT1 compared with K650M or K650E FGFR3 mutants28,35-37. By comparing STAT1 activation among wild-type FGFR3 and six activating mutants—N540K (HCH), G380R (ACH), R248C (TD1), y373C (TDI), K650M (SADDAN), and K650E (TDII)—Krejci et al found that wild-type FGFR3 does not activate STAT1 and that only K650M or K650E FGFR3 significantly activates STAT135,37. Collectively, while in vivo evidence implicates STAT1 in inhibiting chondrocyte proliferation, STAT1 appears to represent a small part of the pathological mechanisms of aberrant
FGFR3 signaling35.
2.2 ERK MAPK pathwayThe Extracellular signal-related kinase (ERK) Mitogen-activated protein kinase (MAPK) pathway is a signaling cascade that is activated by various extracellular stimuli including FGFR338. Increased phosphorylation of ERK and its upstream kinase MEK1 have been observed in mouse models of achondroplasia34,39. Sustained ERK activation is also observed in a chondrocyte cell line expressing ACH and TD FGFR3 mutants37. To examine the effects of increased ERK MAPK signaling in chondrocytes, we generated transgenic mice that express a constitutively active MEK1 mutant in chondrocytes under the control of a Col2a1 promoter34. These mice displayed an ACH-like dwarfism, which was associated with incomplete chondrocyte hypertrophy, while chondrocyte proliferation remained unaffected. Furthermore, the expression of a constitutively active mutant of MEK1 in
Figure 1. A scheme of human FGFR3 structure with positions of mutations. IgI-IgIII, extracellular immunoglobulin-like domains of FGFR3; TM, transmembrane domain; TK1-2, intracellular tyrosine kinase domains. TDI, Thanatophoric dysplasia type I; TDII, Thanatophoric dysplasia type II; SADDAN, severe achondroplasia with developmental delay and acanthosis nigricans; ACH, Achondroplasia; HCH, hypochondroplasia
FIbRObLAST GROWTH FACTOR RECEPTOR 3 SIGNALING IN SkELETAL DYSPLASIA

ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 57
MANUSCRIPTS
the chondrocytes of Fgfr3-deficient mice rescued the skeletal overgrowth caused by the Fgfr3 deficiency, suggesting that the skeletal overgrowth of Fgfr3-deficient mice is due to the reduced activity of the ERK MAPK pathway. We further created a loss-of-function mouse model of ERK1 and ERK2, in which both genes for ERK1 and ERK2 were disrupted in chondrocytes40. Histological analysis of these ERK1 and ERK2-null embryos showed a widening of the zone of hypertrophic chondrocytes in the long bones, similar to Fgfr3-null mice. In addition, the inactivation of ERK1 and ERK2 in chondrocytes promoted the growth of cartilaginous skeletal elements in embryos, further supporting the notion that FGFR3 signaling inhibits endochondral bone growth through the ERK MAPK pathway41.
Our genetic experiments in mice and the histopathological analyses of human homozygous ACH and TD specimens have also implicated FGFR3 and ERK MAPK signaling a synchondrosis closure42. A synchondrosis is a growth plate-like cartilaginous structure connecting ossification centers such as in the spine and cranial base. We found premature synchondrosis closure in the spine and cranial base in human homozygous ACH and TD specimens and in mice heterozygous for the ACH mutation in Fgfr3. Therefore, premature synchondrosis closure may account for the foramen magnum and spinal canal stenosis and the cranial base and mid-facial hypoplasia in heterozygous ACH patients. Our experiments also indicated that transgenic mice that express a constitutively active mutant of MEK1 in chondrocytes show premature synchondrosis closure, while ERK1 and ERK2 inactivation in chondrocytes delays synchondrosis closure and enlarges the spinal canal41,42. These observations strongly suggest that aberrant FGFR3 signaling accelerates synchondrosis closure through the ERK MAPK pathway.
Consistent with the notion that the ERK MAPK pathway plays a central role in FGFR3 signaling, the genetic overexpression of C-type natriuretic peptide (CNP)—a peptide capable of inhibiting the ERK MAPK pathway in chondrocytes—at least partially rescues the dwarf phenotype of transgenic mice expressing human achondroplasia G380R FGFR3 in chondrocytes 39. We also found that the overexpression of CNP in chondrocytes partially rescues the accelerated synchondrosis closure in mice harboring an ACH mutation in Fgfr3 42. Although CNP is not totally specific for the ERK MAPK pathway, these observations also support the role of the ERK MAPK pathway in FGFR3 signaling.
3. Therapeutic perspectives of FGFR3-related skeletal dysplasiasThe recent advancements in our understanding of FGFR3 signaling have offered clues to the development of therapeutic approaches for FGFR3-related skeletal dysplasias. We found that increased FGFR3 and ERK MAPK signaling promotes synchondrosis closure and fusion of ossification centers, while the inactivation of ERK1 and ERK2 in chondrocytes promotes bone growth and enlarges the spinal canal41,42. These observations indicate that ERK1 and ERK2 would be an appropriate target for treating the skeletal phenotypes of FGFR3-related skeletal dysplasias. Pharmacological inhibition of the ERK MAPK pathway would be a straightforward and promising approach for counteracting aberrant FGFR3 signaling.
C-type natriuretic peptide (CNP) and signaling from its receptor, natriuretic peptide receptor-B (NPR-B), have been shown to inhibit the ERK MAPK pathway39,43. Biochemical studies in a chondrocyte cell line have shown that CNP interferes with the ERK MAPK pathway at the level of Raf1, an upstream kinase of MEK143,44. CNP is physiologically expressed in proliferating chondrocytes
in the growth plate, and the genetic overexpression of CNP as well as the continuous infusion of the peptide at least partially rescues the dwarf phenotype of transgenic mice expressing human achondroplasia G380R FGFR3 in chondrocytes39,45,46. Since other natriuretic peptides have already been used clinically for their hemodynamic effects, CNP or its stable analogue could be an effective medicine in the future47.
Other future therapeutic strategies would include: inhibitors for the kinase activity of FGFR3, monoclonal antibodies that block FGFR3 activation, specific RNA interference (RNAi) that inhibits FGFR3 expression, and Hsp90 inhibition that will block proper folding and maturation of the protein48-50. All of these approaches have been shown to block FGFR3 signaling in vitro. It will be a major challenge to determine their feasibility and efficacy for in vivo applications5.
Conclusion Inorganic phosphate is an essential element for bone mineralization. In addition to its role in mineralization, recent studies have shown its significant ability to regulate gene expression and cellular phenotype. Inorganic phosphate regulates various matrix molecules that are closely associated with matrix mineralization. Inorganic phosphate also regulates cell proliferation and apoptosis. At least some of these regulations are mediated by the ERK1/2 MAPK pathway. FGF signaling may be also involved in the phosphate-induced activation of ERK1/2 MAPK. Further analysis of phosphate signaling will uncover novel regulatory mechanisms of bone metabolism and lead to the development of new treatments for various bone disorders.
58
Acknowledgements
We thank Ms. valerie Schmedlen for editorial assistance. Work in the laboratory of the authors was supported by Arthritis Investigator Award of the Arthritis Foundation, March of Dimes Birth Defects Foundation, National Center for Regenerative Medicine, and NIH grants R21DE017406, R01AR055556, R03DE019814 to S.M.
References1. Degnin CR, Laederich MB, and Horton
WA. FGFs in endochondral skeletal development. J Cell Biochem. 2010; (110)1046-57.
2. Horton WA and Degnin CR. FGFs in endochondral skeletal development. Trends Endocrinol Metab. 2009; (20)341-8.
3. Harada D, yamanaka y, Ueda K, Tanaka H, and Seino y. FGFR3-related dwarfism and cell signaling. J Bone Miner Metab. 2009; (27)9-15.
4. Marie PJ, Coffin JD, and Hurley MM. FGF and FGFR signaling in chondrodysplasias and craniosynostosis. J Cell Biochem. 2005; (96)888-96.
5. Laederich MB and Horton WA. FGFR3 targeting strategies for achondroplasia. Expert Rev Mol Med. 2012; (14)e11.
6. Naski MC and Ornitz DM. FGF signaling in skeletal development. Front Biosci. 1998; (3)781-94.
7. Foldynova-Trantirkova S, Wilcox WR, and Krejci P. Sixteen years and counting: the current understanding of fibroblast growth factor receptor 3 (FGFR3) signaling in skeletal dysplasias. Hum Mutat. 2012; (33)29-41.
8. Shirley ED and Ain MC. Achondroplasia: manifestations and treatment. J Am Acad Orthop Surg. 2009; (17)231-41.
9. Laederich MB and Horton WA. Achondroplasia: pathogenesis and implications for future treatment. Curr Opin Pediatr. 2010; (22)516-23.
10. Wright MJ and Irving MD. Clinical management of achondroplasia. Arch Dis Child. 2012; (97)129-34.
11. Richette P, Bardin T, and Stheneur C. Achondroplasia: from genotype to phenotype. Joint Bone Spine. 2008; (75)125-30.
12. Horton WA and Lunstrum GP. Fibroblast
growth factor receptor 3 mutations in achondroplasia and related forms of dwarfism. Rev Endocr Metab Disord. 2002; (3)381-5.
13. Horton WA, Hall JG, and Hecht JT. Achondroplasia. Lancet. 2007; (370)162-72.
14. Carter EM, Davis JG, and Raggio CL. Advances in understanding etiology of achondroplasia and review of management. Curr Opin Pediatr. 2007; (19)32-7.
15. Aviezer D, Golembo M, and yayon A. Fibroblast growth factor receptor-3 as a therapeutic target for Achondroplasia--genetic short limbed dwarfism. Curr Drug Targets. 2003; (4)353-65.
16. Hall JG. The natural history of achondroplasia. Basic Life Sci. 1988; (48)3-9.
17. Rimoin DL. Clinical variability in achondroplasia. Basic Life Sci. 1988; (48)123-7.
18. Isaacson G, Blakemore KJ, and Chervenak FA. Thanatophoric dysplasia with cloverleaf skull. Am J Dis Child. 1983; (137)896-8.
19. Martinez-Frias ML, De Frutos CA, Bermejo E, Nieto MA, and Group EW. Review of the recently defined molecular mechanisms underlying thanatophoric dysplasia and their potential therapeutic implications for achondroplasia. Am J Med Genet A. 2010; (152A)245-55.
20. Kulkarni ML, Sureshkumar C, venkataramana v, Koshy S, Bhagyavathi M, and Reddy GS. Thanatophoric dysplasia. Indian Pediatr. 1994; (31)1405-10.
21. Brodie SG, Kitoh H, Lachman RS, Nolasco LM, Mekikian PB, and Wilcox WR. Platyspondylic lethal skeletal dysplasia, San Diego type, is caused by FGFR3 mutations. Am J Med Genet. 1999; (84)476-80.
22. Tavormina PL, Shiang R, Thompson LM, Zhu yZ, Wilkin DJ, Lachman RS, Wilcox WR, Rimoin DL, Cohn DH, and Wasmuth JJ. Thanatophoric dysplasia (types I and II) caused by distinct mutations in fibroblast growth factor receptor 3. Nat Genet. 1995; (9)321-8.
23. Tavormina PL, Rimoin DL, Cohn DH, Zhu yZ, Shiang R, and Wasmuth JJ. Another mutation that results in the substitution of an unpaired cysteine residue in the extracellular domain of FGFR3 in thanatophoric dysplasia type I. Hum Mol
Genet. 1995; (4)2175-7.
24. 24. Rousseau F, Saugier P, Le Merrer M, Munnich A, Delezoide AL, Maroteaux P, Bonaventure J, Narcy F, and Sanak M. Stop codon FGFR3 mutations in thanatophoric dwarfism type 1. Nat Genet. 1995; (10)11-2.
25. Webster MK, D’avis Py, Robertson SC, and Donoghue DJ. Profound ligand-independent kinase activation of fibroblast growth factor receptor 3 by the activation loop mutation responsible for a lethal skeletal dysplasia, thanatophoric dysplasia type II. Mol Cell Biol. 1996; (16)4081-7.
26. Naski MC, Wang Q, Xu J, and Ornitz DM. Graded activation of fibroblast growth factor receptor 3 by mutations causing achondroplasia and thanatophoric dysplasia. Nat Genet. 1996; (13)233-7.
27. Su WC, Kitagawa M, Xue N, Xie B, Garofalo S, Cho J, Deng C, Horton WA, and Fu Xy. Activation of Stat1 by mutant fibroblast growth-factor receptor in thanatophoric dysplasia type II dwarfism. Nature. 1997; (386)288-92.
28. Harada D, yamanaka y, Ueda K, Nishimura R, Morishima T, Seino y, and Tanaka H. Sustained phosphorylation of mutated FGFR3 is a crucial feature of genetic dwarfism and induces apoptosis in the ATDC5 chondrogenic cell line via PLCgamma-activated STAT1. Bone. 2007; (41)273-81.
29. Hart KC, Robertson SC, and Donoghue DJ. Identification of tyrosine residues in constitutively activated fibroblast growth factor receptor 3 involved in mitogenesis, Stat activation, and phosphatidylinositol 3-kinase activation. Mol Biol Cell. 2001; (12)931-42.
30. Lievens PM and Liboi E. The thanatophoric dysplasia type II mutation hampers complete maturation of fibroblast growth factor receptor 3 (FGFR3), which activates signal transducer and activator of transcription 1 (STAT1) from the endoplasmic reticulum. J Biol Chem. 2003; (278)17344-9.
31. Legeai-Mallet L, Benoist-Lasselin C, Munnich A, and Bonaventure J. Overexpression of FGFR3, Stat1, Stat5 and p21Cip1 correlates with phenotypic severity and defective chondrocyte differentiation in FGFR3-related chondrodysplasias. Bone. 2004; (34)26-36.
32. Sahni M, Ambrosetti DC, Mansukhani A, Gertner R, Levy D, and Basilico C.
FIbRObLAST GROWTH FACTOR RECEPTOR 3 SIGNALING IN SkELETAL DYSPLASIA

ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 59
MANUSCRIPTS
FGF signaling inhibits chondrocyte proliferation and regulates bone development through the STAT-1 pathway. Genes Dev. 1999; (13)1361-6.
33. Sahni M, Raz R, Coffin JD, Levy D, and Basilico C. STAT1 mediates the increased apoptosis and reduced chondrocyte proliferation in mice overexpressing FGF2. Development. 2001; (128)2119-29.
34. Murakami S, Balmes G, Mckinney S, Zhang Z, Givol D, and De Crombrugghe B. Constitutive activation of MEK1 in chondrocytes causes Stat1-independent achondroplasia-like dwarfism and rescues the Fgfr3-deficient mouse phenotype. Genes Dev. 2004; (18)290-305.
35. Krejci P, Salazar L, Goodridge HS, Kashiwada TA, Schibler MJ, Jelinkova P, Thompson LM, and Wilcox WR. STAT1 and STAT3 do not participate in FGF-mediated growth arrest in chondrocytes. J Cell Sci. 2008; (121)272-81.
36. Nowroozi N, Raffioni S, Wang T, Apostol BL, Bradshaw RA, and Thompson LM. Sustained ERK1/2 but not STAT1 or 3 activation is required for thanatophoric dysplasia phenotypes in PC12 cells. Hum Mol Genet. 2005; (14)1529-38.
37. Krejci P, Salazar L, Kashiwada TA, Chlebova K, Salasova A, Thompson LM, Bryja v, Kozubik A, and Wilcox WR. Analysis of STAT1 activation by six FGFR3 mutants associated with skeletal dysplasia undermines dominant role of STAT1 in FGFR3 signaling in cartilage. PLoS One. 2008; (3)e3961.
38. Sturgill TW. MAP kinase: it’s been longer than fifteen minutes. Biochem Biophys Res Commun. 2008; (371)1-4.
39. yasoda A, Komatsu y, Chusho H, Miyazawa T, Ozasa A, Miura M, Kurihara T, Rogi T, Tanaka S, Suda M, Tamura N, Ogawa y, and Nakao K. Overexpression of CNP in chondrocytes rescues achondroplasia through a MAPK-dependent pathway. Nat Med. 2004; (10)80-6.
40. Matsushita T, Chan y, Kawanami A, Balmes G, Landreth GE, and Murakami S. Extracellular Signal-Regulated Kinase 1 (ERK1) and ERK2 play essential roles in osteoblast differentiation and in supporting osteoclastogenesis. Mol Cell Biol. 2009; (29)5843-57.
41. Sebastian A, Matsushita T, Kawanami A, Mackem S, Landreth GE, and Murakami S. Genetic inactivation of ERK1 and ERK2 in chondrocytes promotes bone growth and enlarges the spinal canal. J Orthop Res.
2011; (29)375-9.
42. Matsushita T, Wilcox WR, Chan yy, Kawanami A, Bukulmez H, Balmes G, Krejci P, Mekikian PB, Otani K, yamaura I, Warman ML, Givol D, and Murakami S. FGFR3 promotes synchondrosis closure and fusion of ossification centers through the MAPK pathway. Hum Mol Genet. 2009; (18)227-40.
43. Krejci P, Masri B, Fontaine v, Mekikian PB, Weis M, Prats H, and Wilcox WR. Interaction of fibroblast growth factor and C-natriuretic peptide signaling in regulation of chondrocyte proliferation and extracellular matrix homeostasis. J Cell Sci. 2005; (118)5089-100.
44. Pejchalova K, Krejci P, and Wilcox WR. C-natriuretic peptide: an important regulator of cartilage. Mol Genet Metab. 2007; (92)210-5.
45. Chusho H, Tamura N, Ogawa y, yasoda A, Suda M, Miyazawa T, Nakamura K, Nakao K, Kurihara T, Komatsu y, Itoh H, Tanaka K, Saito y, Katsuki M, and Nakao K. Dwarfism and early death in mice lacking C-type natriuretic peptide. Proc Natl Acad Sci USA. 2001; (98)4016-21.
46. yasoda A, Kitamura H, Fujii T, Kondo E, Murao N, Miura M, Kanamoto N, Komatsu y, Arai H, and Nakao K. Systemic administration of C-type natriuretic peptide as a novel therapeutic strategy for skeletal dysplasias. Endocrinology. 2009; (150)3138-44.
47. Potter LR, yoder AR, Flora DR, Antos LK, and Dickey DM. Natriuretic peptides: their structures, receptors, physiologic functions and therapeutic applications. Handb Exp Pharmacol. 2009; (191)341-66.
48. Hartmann JT, Haap M, Kopp HG, and Lipp HP. Tyrosine kinase inhibitors - a review on pharmacology, metabolism and side effects. Curr Drug Metab. 2009; (10)470-81.
49. Qing J, Du X, Chen y, Chan P, Li H, Wu P, Marsters S, Stawicki S, Tien J, Totpal K, Ross S, Stinson S, Dornan D, French D, Wang QR, Stephan JP, Wu y, Wiesmann C, and Ashkenazi A. Antibody-based targeting of FGFR3 in bladder carcinoma and t(4;14)-positive multiple myeloma in mice. J Clin Invest. 2009; (119)1216-29.
50. Laederich MB, Degnin CR, Lunstrum GP, Holden P, and Horton WA. Fibroblast growth factor receptor 3 (FGFR3) is a strong heat shock protein 90 (Hsp90) client: implications for therapeutic manipulation. J Biol Chem. 2011; (286)19597-604.
60
Introduction Stem cells have emerged as a promising alternative to traditional surgical procedures for the regeneration and repair of skeletal tissues resulting from common and rare skeletal diseases and trauma. Skeletal tissues undergo continuous remodeling and regeneration during skeletal development and normal adult life, and in response to injury or disease. Therefore, in the field of orthopaedic regenerative medicine, which seeks to repair, replace, or regenerate tissues and organs damaged by injury or disease, many clues can be drawn from skeletal development. Similar to skeletal development, skeletal healing requires mesenchymal stromal (or stem) cells (MSCs). In this review, we aim to provide a glimpse of the recent progress made in this rapidly developing field and the great promise MSCs hold for future orthopaedic applications. We summarize the application of MSCs in regenerative medicine for the treatment of skeletal diseases, including osteogenesis imperfecta, fibrous dysplasia, osteoarthritis, and fracture healing. We also discuss the recent discovery of induced pluripotent stem (iPS) cells and their potential orthopaedic applications as a renewable source of skeletal cells.
Embryonic Skeletal Development During embryonic development, the mesodermal layer contains multipotent mesenchymal progenitor cells that give rise to bone, cartilage, fat, muscle, and other tissues1, 2. Skeletal formation then occurs through either intramembranous
ossification or endochondral ossification. During intramembranous ossification, which mostly occurs in flat bones, mesenchymal cells directly differentiate into osteoblasts and produce bone matrix. For endochondral ossification, which occurs in the majority of the skeleton, the undifferentiated mesenchymal cells migrate from the lateral plate mesoderm and paraxial mesoderm and form mesenchymal condensations at the locations of future skeletal elements. The mesenchymal cell condensations form a cartilage template, which grows as the chondrocytes proliferate and becomes surrounded by capillaries. The mesenchymal cells around the cartilage template differentiate into osteoblasts and produce a collar of bone around the middle of the cartilage, and the chondrocytes in the center of the cartilage undergo hypertrophy. Eventually, the capillaries invade the bone collar, and the hypertrophic cartilage is replaced by bone.
Transcription factors play an essential role in skeletal development by regulating all aspects of the differentiation of chondrocytes and osteoblasts. Chondrocytes and osteoblasts, as well as many other cell types, originate from the same mesenchymal progenitor cells3. A mouse genetic cell-lineage tracing study demonstrated that the progenitor cells expressing the transcription factor Sox9 are committed to the skeletal lineage and can differentiate into both chondrocytes and osteoblasts4. Thus, those early Sox9-expressing cells in future skeletal locations are called skeletal precursor
cells or osteochondro progenitor cells 4,
5. Subsequently, chondrocyte lineage is determined by Sox9 together with Sox5 and Sox62. Chondrocyte hypertrophy is activated by Runx2 and repressed by Sox9, whereas osteoblast differentiation is promoted by Runx2 and its downstream effector Osterix.
Sox9 and Runx2 are master transcription factors of skeletogenesis because they regulate many other genes involved in the development of the skeleton, and are required for proper skeletal formation. More tellingly, mutations in SOX9 and RUNX2 both cause human skeletal diseases. Heterozygous mutations in the human SOX9 gene cause campomelic dysplasia, a very severe form of generalized chondrodysplasia2. Campomelic dysplasia is characterized by bowing of the long bones and malformations in all cartilage, and can result in infant death at or soon after birth due to respiratory distress. Heterozygous mutations in the RUNX2 gene are associated with human cleidocranial dysplasia2. Individuals with cleidocranial dysplasia have underdeveloped or absent collarbones, causing their shoulders to be close together in front of the body. The other features of cleidocranial dysplasia include the delayed closing of fontanels, short stature, and dental abnormalities6.
Stem Cells Stem cells are unspecialized cells that are defined by their self-renewal and differentiation capacity7-10. Stem cells can be broadly categorized into two major classes: embryonic and adult stem
MESENCHyMAL STROMAL CELLS AND THEIR ORTHOPAEDIC APPLICATIONS Lindsay A. Bashur, PhD, and Guang Zhou, PhD
Department of Orthopaedics, Case Western Reserve University

ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 61
MANUSCRIPTS
cells. Embryonic stem cells (ESCs) are isolated from the inner cell mass of the blastocyst, can self-renew indefinitely, and are pluripotent cells with the potential of differentiating into cell types from all three germ layers: endoderm, ectoderm, and mesoderm8. However, many factors have limited their use in clinical applications, including ethical concerns, immunological incompatibilities, potential for malignant tumor growth, heterogeneous differentiation, and an insufficient understanding of and control over ESC differentiation.
Adult mesenchymal stem cells (MSCs) are multipotent undifferentiated cells that are capable of self-renewal and responsible for adult tissue regeneration7-10. Bone marrow stromal cells were initially described by Alexander Friedenstein in 196811. Friedenstein and colleagues isolated bone marrow-derived fibroblast-like cells based on their ability to adhere to plastic substrates and form colony units12. They also showed that these cells had osteogenic and adipogenic potential13. Marshall Urist showed that demineralized bone or its extracts induced the differentiation of mesenchymal cells into cartilage and bone when implanted into subcutaneous or intramuscular sites in human and animal models14. Similar work was performed independently by others15 and confirmed the existence of multipotent progenitor cells in adult tissues. In the 1970s, Caplan and colleagues reported the dissociation of embryonic stage 24 chick limb bud mesenchymal progenitor cells and their subsequent differentiation into bone, cartilage, muscle, and other mesenchymal tissues16, 17. During the early 1980s, they showed that exposing embryonic chick limb bud cultures to extracts of demineralized bone can induce BMP-mediated chondrogenic differentiation18-20.
MSCs are identified in vitro largely based on three specific characteristics 8-10. The first is the ability to adhere
to plastic culture dishes and to form fibroblast-like colonies. The second characteristic is the ability to differentiate into various specialized cell lineages, such as osteoblasts, adipocytes, and chondrocytes, and some other cell types under certain culture conditions. The third is the expression of defined cell surface markers. The molecular characterization of MSCs is challenging because they do not uniquely express any specific molecule. In addition, cell surface marker expression can vary with different isolation techniques, tissue origins and species, and culture conditions. Thus, the International Society of Cellular Therapy (ISCT) proposed that MSCs must be positive for cell surface markers CD73, CD90, and CD105 and lack expression of typical hematopoietic lineage markers, including CD34, CD45, CD14, CD11b, CD19, CD79a, and HLA-DR [21]. MSCs predominantly reside in the bone marrow compartment, but they have also been described in other tissues such as fat and muscle. They represent a highly heterogeneous population of immature cells of still poorly defined physical, phenotypic, and functional properties, especially in vivo. Nonetheless, at least in mouse models, a subpopulation of bone marrow MSCs are dynamic and critical participants in bone maintenance and regeneration22. MSCs have begun to be utilized in clinical trials for tissue repair and regeneration worldwide, albeit sometimes under very poor or no regulations.
MSCs in Skeletal Disease Models and TreatmentOsteogenesis ImperfectaOsteogenesis imperfecta (OI) is a heterogeneous group of inherited disorders in which a genetic defect in type I collagen of osteoblasts causes osteopenia, multiple fractures, severe bony deformities, and shortened stature 10, 23. The clinical phenotype of OI ranges from normal life expectancy with mild
bone fragility to osteopenia to death. The treatment options are limited for OI as a genetic disease. Many studies have shown that bisphosphate therapy in OI increased bone density and strength, and reduced incidence of fractures10,
23. However, bisphosphates can have potential adverse skeletal effects in children, which is a concern for long-term treatment.
Stem cells are a promising alternative treatment for OI. A study by Pereira et al. showed that when MSCs from wild-type mice were infused into transgenic mice that exhibited an OI phenotype, the wild-type MSCs contributed to the continual renewal of cells in a number of nonhematopoietic tissues in the mutant mice24. Horwitz et al. performed clinical trials to transplant allogeneic bone marrow into children with severe OI25. The results showed an increase in total body mineral content, increase in bone growth, and reduction in fracture rates after three months. In their next study, Horwitz et al. transplanted MSCs into children that had previously undergone bone marrow transplantation for OI26. The results demonstrated the engraftment of donor MSCs in the recipient bone and an increase in bone velocity. Panaroni et al. evaluated the intrauterine transplantation of adult bone marrow into a knockin murine model for OI27. They showed that the adult bone marrow donor cells can engraft into hematopoietic and nonhematopoietic tissues and further differentiate to trabecular and cortical bone cells, synthesizing up to 20% of all type I collagen in the host bone, and also rescuing the perinatal lethality of mice with dominant OI.
Gene therapy in combination with stem cells also offers a promising approach to treating OI. Chamberlain et al. used adeno-associated virus (AAv) vectors to target and inactivate mutant COL1A1 genes28 and mutant COL1A2 genes29 in the MSCs from OI individuals. Their

62
results, largely from ex vivo cultures, showed that the targeted-MSCs produced normal type I procollagen and formed bone, thus demonstrating their therapeutic potential. The future goal is to return the corrected stem cells to the OI patients from whom the MSCs were harvested to improve their bone quality.
Fibrous DysplasiaFibrous dysplasia (FD) is a skeletal disease caused by activating missense mutations in the GNAS gene, which encodes the α subunit of the stimulatory G protein (Gs)30, 31. FD is a crippling, occasionally lethal disease, where normal bone and bone marrow is replaced by abnormal, fibrous bone tissue. There is currently no cure for FD. Surgery is used to treat fractures and deformities, but is often unsuccessful.
Piersanti et al. have explored two roles of MSCs in FD32. First, they were able to stably transfer the FD genotype and phenotype to normal human skeletal progenitor cells to model the mutation effects32. Second, they used MSCs as a tool for the treatment of FD through cell replacement or gene correction in MSCs33. Here, they silenced the mutated allele only in skeletal progenitors. For both goals, they used lentiviral transduction technology to effectively and efficiently target a dominant gain-of-function mutation in GNAS32, 33. Therefore, Piersanti et al. have demonstrated the feasibility of a gene therapy approach for treating FD, through the reversal of the disease phenotype at the cellular level, based on the selective knockdown of the dominant gain-of-function Gsα mutations in skeletal stem cells.
OsteoarthritisOsteoarthritis (OA), the most common type of arthritis, is a chronic degenerative joint disease characterized by progressive cartilage deterioration34,
35. The symptoms of OA include joint pain, impairment of movement, and
local inflammation. Current treatments relieve pain temporarily with nonsteroidal anti-inflammatory drugs, steroids, hyaluronic acid, or surgery, but eventually fail over time. OA is associated with progressive inflammation; thus, MSCs are a promising candidate for cell therapy because they have anti-inflammatory and immunosuppressive properties36. In addition, MSCs have shown the ability to migrate and engraft onto multiple musculoskeletal tissues, especially at sites of injury, and undergo site-specific differentiation, then influence the microenvironment to aid in the regeneration of cartilage.
Recent efforts have focused on the use of direct intra-articular injection of MSCs as a therapy for OA. Lee et al. intra-articularly injected MSCs suspended in HA for the treatment of cartilage defects in the medial femoral condyle of adult minipigs37. At 6 and 12 weeks postoperatively, the MSC-treated groups showed improved cartilage healing compared with the controls. Horie et al. investigated the efficiency of meniscal regeneration in rat massive meniscal defects using intra-articular MSCs38. Their results showed that the MSCs adhered to the lesion, differentiated into meniscal cells directly, and promoted meniscal regeneration. MSCs have also been genetically modified for OA cell therapy to release therapeutic proteins that can interact with the injured cartilage. In one study by Matsumoto et al., when the MSCs expressing bone morphogenetic protein (BMP)-4, in combination with MSCs expressing the vascular endothelial growth factor antagonist soluble Flt-1, were intra-articularly injected into an immunodeficient rat model for OA, the quality and the persistence of regenerated articular cartilage were significantly improved39. Recently, controlled growth factor release from microspheres incorporated in MSC sheets has been shown to enhance cartilage
tissue formation40. Furthermore, the over-expression of SOX9, the master regulator of chondrogenesis, can also increase MSC-mediated cartilage repair in an animal model41.
Wakitani et al. reported the clinical use of transplanted bone marrow-derived MSCs seeded onto type I collagen-containing hydrogels to repair cartilage defects in the medial femoral condyle of human knees with OA42. Forty-two weeks after transplantation, the arthroscopic and histological grading scores were better in the MSC-transplanted group than in the cell-free control group. In another clinical study, by Davatchi et al., four patients ages 54-65 years old with moderate to severe knee OA received intra-articular injections of autologous bone marrow-derived MSCs43. After 6 months, three patients showed improvement in walking time and pain scores. All patients showed improvement in the number of stairs they could climb and pain relief. A recent study reported the discovery of a small molecule, kartogenin, which can promote the differentiation of MSCs into chondrocytes44. Johnson et al. showed that kartogenin can upregulate chondrocyte-specific gene expression in vitro, and significantly increase cartilage thickness in an OA mouse model.
Bone Fractures Normal bone fracture healing involves a complex network of signaling events in response to injury. Undifferentiated MSCs are recruited to the injury site where, with the aid of regulatory cytokines, e.g. BMPs, they proliferate, differentiate into chondrocytes and osteoblasts, and form bone, thus repairing the defect. Failure to heal properly results in either delayed union, or nonunion if fractures fail to heal after 8-9 months10, 23. While fractures are a common clinical occurrence, the treatment of nonunions remains a challenge. MSCs are promising candidates for bone regeneration due to their ability to migrate to injured tissues and
MESENCHYMAL STROMAL CELLS

ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 63
MANUSCRIPTS
undergo osteogenic and chondrogenic differentiation.
Numerous studies have successfully used MSCs for fracture repair and bone regeneration in animal models. Granero-Molto et al. demonstrated that MSCs migrated towards the fracture site in a mouse model, and contributed to fracture healing by expressing BMP-2 and modulating the injury-related inflammatory response45. Bone repair often requires a scaffold for structural and mechanical support. Kadiyala et al. expanded bone marrow-derived MSCs in culture, seeded them onto ceramic cylinders, and implanted the constructs into 8 mm segmental defects in rat femurs46. The results showed new bone formation after 8 weeks. Several other studies have also been performed using different scaffold materials in combination with MSCs to achieve bone regeneration7, 47.
Gene therapy has also been explored for the use in fracture healing and bone regeneration. Musgrave et al. showed that MSCs can be used to deliver BMP-2 ex vivo48. The delivery of BMP-2 stimulates the MSCs at the injury site to differentiate and form bone. Burastero et al. found that the combination of MSCs with BMP-7 on a scaffold resulted in a better osteoinductive graft than either MSCs or BMP-7 alone49.
Human studies have been reported in which autologous bone marrow-derived MSCs were expanded in vitro, then loaded onto 100% hydroxyapatite macroporous ceramic scaffolds50. The constructs were then implanted into four patients with diaphyseal segmental defects that ranged from 3 to 28.3 cm3 in one tibia, one humerus, and two ulna fractures, respectively. Good integration of the implanted constructs with the preexisting bone was maintained, and no major adverse reactions were observed. All patients experienced recovery of
limb function, and good integration was maintained at the last follow-up (6-7 years after surgery). Hernigou et al. treated 60 cases of atrophic non-union of the tibia with the percutaneous injection of concentrated bone marrow51. They reported a high union rate of 43/60, and a correlation between the number and concentration of colony-forming units in the graft and the volume of mineralized callus at 4 months. Quarto et al. treated critical-sized segmental defects in the long bones of three patients with size-matching hydroxyapatite scaffolds loaded with expanded autologous MSC cultures52. They reported that graft integration was detected as early as 2 months after surgery and all three patients regained function of their limbs with no adverse effects.
iPS Cells: An Alternative Stem Cell Source Induced pluripotent stem (iPS) cells have recently been discovered as an alternative to ESCs. Takahashi et al. generated iPS cells by transfecting mouse somatic cells with pluripotent transcription factors Oct3/4, c-Myc, Sox2, and K1f453. They reported that these iPS cells were highly similar to ESCs in their morphology, proliferation, gene expression, and in vitro differentiation53. This landmark study has been cited more than 3700 times, reflecting the growing interest and wide application of its findings. Different groups subsequently replicated their findings in human cells. To date, iPS cells have been derived at increased efficiency from easily accessible human cell types such as dermal fibroblasts, blood cells, and keratinocytes54. To eliminate the potential risk of virally induced tumor formation associated with the early iPS cell derivation procedure, intense efforts are underway to develop virus-free and/or vector-free iPS cell protocols. More importantly, various patient-specific iPS cells have been generated to serve as novel models to study disease pathogenesis and to screen for new
drugs55. However, in order for iPS cells to be used in clinical settings, many remaining obstacles must be overcome, such as low reprogramming efficiency and tumorigenicity with iPS cells.
Efforts have also been underway to convert somatic cells directly into differentiated cell types, including chondrocytes. Indeed, the combination of c-Myc, Klf4, and Sox9 can reprogram adult dermal fibroblasts directly into chondrocytes and form hyaline cartilage in mice56. Although SOX9 is required for converting iPS cells and other progenitor cells to chondrocytes, it should be borne in mind that SOX9 expression has to be tightly controlled to avoid unintended effects. Our group has recently showed that ectopic Sox9 expression in differentiated osteoblasts can lead to severe osteopenia, altered bone mechanical properties, and impaired MSC functions in mice57. Furthermore, in addition to cartilage development, SOX9 is also critical for the development of other organs such as the central nervous system, pancreas, prostate, intestine, skin, pituitary, heart, kidney, and liver. Over-expression of SOX9 has been associated with the tumorigenesis of colorectal cancer, breast cancer, and prostate cancer. Thus, a more comprehensive understanding of the regulation of SOX9 itself is critical to generate abundant chondrocytes with minimal side effects for orthopaedic applications.
Conclusions MSCs and iPS cells can both develop into multiple tissues including bone and cartilage. They hold great promise for orthopaedic applications such as generating specific disease models and developing novel therapies. There have been great advances in MSC technology to treat skeletal diseases since the discovery of MSCs several decades ago. Our knowledge about the role of progenitor cells in

64
skeletal development has enabled us to better understand the role of MSCs in adult skeletal disease and injury. However, MSC transplantation has its risks that cannot be overlooked when developing MSC therapy. For example, ex vivo amplifications of MSCs via extensive passages may lead to malignant transformation with cytogenetic aberrations and sarcoma formation. Thus more research, such as understanding the signaling pathways involved in musculoskeletal tissue regeneration, is critical for developing MSC therapy. The recent development of iPS cell technology is a versatile alternative to MSCs. The first human clinical trial using iPS cells to repair diseased retinas is scheduled to start in 2013 at the RIKEN Center for Developmental Biology in Kobe, Japan. However, for iPS cells, additional research and animal trials are also necessary to establish their safety and efficacy before clinical application. In summary, a better understanding of the molecular basis of pluripotency, cellular reprogramming, and lineage-specific differentiation of MSCs and iPS cells is essential to realize their clinical potential in regenerative medicine in the future.
Acknowledgements
We thank valerie Schmedlen for editorial assistance.
References1. Mackie, E.J., L. Tatarczuch, and M. Mirams,
The skeleton: a multi-functional complex organ: the growth plate chondrocyte and endochondral ossification. J Endocrinol, 2011. 211(2): p. 109-21.
2. Zelzer, E. and B.R. Olsen, The genetic basis for skeletal diseases. Nature, 2003. 423(6937): p. 343-8.
3. Karsenty, G., The complexities of skeletal biology. Nature, 2003. 423(6937): p. 316-8.
4. Akiyama, H., et al., Osteo-chondroprogenitor cells are derived from Sox9 expressing precursors. Proc Natl Acad
Sci USA, 2005. 102(41): p. 14665-70.
5. Hartmann, C., Transcriptional networks controlling skeletal development. Curr Opin Genet Dev, 2009. 19(5): p. 437-43.
6. Zhou, G., et al., CBFA1 mutation analysis and functional correlation with phenotypic variability in cleidocranial dysplasia. Hum Mol Genet, 1999. 8(12): p. 2311-6.
7. Caplan, A.I., Review: mesenchymal stem cells: cell-based reconstructive therapy in orthopedics. Tissue Eng, 2005. 11(7-8): p. 1198-211.
8. Shenaq, D.S., et al., Mesenchymal Progenitor Cells and Their Orthopedic Applications: Forging a Path towards Clinical Trials. Stem Cells Int, 2010. 2010: p. 519028.
9. Spencer, N.D., J.M. Gimble, and M.J. Lopez, Mesenchymal stromal cells: past, present, and future. Vet Surg, 2011. 40(2): p. 129-39.
10. Undale, A.H., et al., Mesenchymal stem cells for bone repair and metabolic bone diseases. Mayo Clin Proc, 2009. 84(10): p. 893-902.
11. Friedenstein, A.J., et al., Heterotopic of bone marrow. Analysis of precursor cells for osteogenic and hematopoietic tissues. Transplantation, 1968. 6(2): p. 230-47.
12. Friedenstein, A.J., R.K. Chailakhjan, and K.S. Lalykina, The development of fibroblast colonies in monolayer cultures of guinea-pig bone marrow and spleen cells. Cell Tissue Kinet, 1970. 3(4): p. 393-403.
13. Owen, M. and A.J. Friedenstein, Stromal stem cells: marrow-derived osteogenic precursors. Ciba Found Symp, 1988. 136: p. 42-60.
14. Urist, M.R., Bone: formation by autoinduction. Science, 1965. 150(3698): p. 893-9.
15. Reddi, A.H. and C. Huggins, Biochemical sequences in the transformation of normal fibroblasts in adolescent rats. Proc Natl Acad Sci USA, 1972. 69(6): p. 1601-5.
16. Caplan, A.I., Effects of the nicotinamide-sensitive teratogen3-acetylpyridine on chick limb cells in culture. Exp Cell Res, 1970. 62(2): p. 341-55.
17. Caplan, A.I. and S. Koutroupas, The control of muscle and cartilage development in the chick limb: the role of differential vascularization. J Embryol Exp Morphol, 1973. 29(3): p. 571-83.
18. Lucas, P.A., G.T. Syftestad, and A.I. Caplan, Partial isolation and characterization of a chemotactic factor from adult bovine bone for mesenchymal cells. Bone, 1986. 7(5): p. 365-71.
19. Lucas, P.A., G.T. Syftestad, and A.I. Caplan,
A water-soluble fraction from adult bone stimulates the differentiation of cartilage in explants of embryonic muscle. Differentiation, 1988. 37(1): p. 47-52.
20. Syftestad, G.T. and A.I. Caplan, A fraction from extracts of demineralized adult bone stimulates the conversion of mesenchymal cells into chondrocytes. Dev Biol, 1984. 104(2): p. 348-56.
21. Dominici, M., et al., Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy, 2006. 8(4): p. 315-7.
22. Park, D., et al., Endogenous bone marrow MSCs are dynamic, fate-restricted participants in bone maintenance and regeneration. Cell Stem Cell, 2012. 10(3): p. 259-72.
23. Beyth, S., J. Schroeder, and M. Liebergall, Stem cells in bone diseases: current clinical practice. Br Med Bull, 2011. 99: p. 199-210.
24. Pereira, R.F., et al., Marrow stromal cells as a source of progenitor cells for nonhematopoietic tissues in transgenic mice with a phenotype of osteogenesis imperfecta. Proc Natl Acad Sci USA, 1998. 95(3): p. 1142-7.
25. Horwitz, E.M., et al., Transplantability and therapeutic effects of bone marrow-derived mesenchymal cells in children with osteogenesis imperfecta. Nat Med, 1999. 5(3): p. 309-13.
26. Horwitz, E.M., et al., Clinical responses to bone marrow transplantation in children with severe osteogenesis imperfecta. Blood, 2001. 97(5): p. 1227-31.
27. Panaroni, C., et al., In utero transplantation of adult bone marrow decreases perinatal lethality and rescues the bone phenotype in the knockin murine model for classical, dominant osteogenesis imperfecta. Blood, 2009. 114(2): p. 459-68.
28. Chamberlain, J.R., et al., Gene targeting in stem cells from individuals with osteogenesis imperfecta. Science, 2004. 303(5661): p. 1198-201.
29. Chamberlain, J.R., et al., Gene targeting of mutant COL1A2 alleles in mesenchymal stem cells from individuals with osteogenesis imperfecta. Mol Ther, 2008. 16(1): p. 187-93.
30. Bianco, P., et al., “Mesenchymal” stem cells in human bone marrow (skeletal stem cells): a critical discussion of their nature, identity, and significance in incurable skeletal disease. Hum Gene Ther, 2010. 21(9): p. 1057-66.
31. Riminucci, M., et al., Skeletal progenitors and the GNAS gene: fibrous dysplasia
MESENCHYMAL STROMAL CELLS
ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 65
MANUSCRIPTS
of bone read through stem cells. J Mol Endocrinol, 2010. 45(6): p. 355-64.
32. Piersanti, S., et al., Transfer, analysis, and reversion of the fibrous dysplasia cellular phenotype in human skeletal progenitors. J Bone Miner Res, 2010. 25(5): p. 1103-16.
33. Piersanti, S., et al., Lentiviral transduction of human postnatal skeletal (stromal, mesenchymal) stem cells: in vivo transplantation and gene silencing. Calcif Tissue Int, 2006. 78(6): p. 372-84.
34. Chen, F.H. and R.S. Tuan, Mesenchymal stem cells in arthritic diseases. Arthritis Res Ther, 2008. 10(5): p. 223.
35. Qi, y., G. Feng, and W. yan, Mesenchymal stem cell-based treatment for cartilage defects in osteoarthritis. Mol Biol Rep, 2012. 39(5): p. 5683-9.
36. Keating, A., Mesenchymal stromal cells: new directions. Cell Stem Cell, 2012. 10(6): p. 709-16.
37. Lee, K.B., et al., Injectable mesenchymal stem cell therapy for large cartilage defects--a porcine model. Stem Cells, 2007. 25(11): p. 2964-71.
38. Horie, M., et al., Intra-articular Injected synovial stem cells differentiate into meniscal cells directly and promote meniscal regeneration without mobilization to distant organs in rat massive meniscal defect. Stem Cells, 2009. 27(4): p. 878-87.
39. Matsumoto, T., et al., Cartilage repair in a rat model of osteoarthritis through intraarticular transplantation of muscle-derived stem cells expressing bone morphogenetic protein 4 and soluble Flt-1. Arthritis Rheum, 2009. 60(5): p. 1390-405.
40. Solorio, L.D., et al., Engineered cartilage via self-assembled hMSC sheets with incorporated biodegradable gelatin microspheres releasing transforming growth factor-beta1. J Control Release, 2012. 158(2): p. 224-32.
41. Cao, L., et al., The promotion of cartilage defect repair using adenovirus mediated Sox9 gene transfer of rabbit bone marrow mesenchymal stem cells. Biomaterials, 2011. 32(16): p. 3910-20.
42. Wakitani, S., et al., Human autologous culture expanded bone marrow mesenchymal cell transplantation for repair of cartilage defects in osteoarthritic knees. Osteoarthritis Cartilage, 2002. 10(3): p. 199-206.
43. Davatchi, F., et al., Mesenchymal stem cell therapy for knee osteoarthritis. Preliminary report of four patients. Int J Rheum Dis, 2011. 14(2): p. 211-5.
44. Johnson, K., et al., A stem cell-based
approach to cartilage repair. Science, 2012. 336(6082): p. 717-21.
45. Granero-Molto, F., et al., Regenerative effects of transplanted mesenchymal stem cells in fracture healing. Stem Cells, 2009. 27(8): p. 1887-98.
46. Kadiyala, S., et al., Culture expanded canine mesenchymal stem cells possess osteochondrogenic potential in vivo and in vitro. Cell Transplant, 1997. 6(2): p. 125-34.
47. Sundelacruz, S. and D.L. Kaplan, Stem cell- and scaffold-based tissue engineering approaches to osteochondral regenerative medicine. Semin Cell Dev Biol, 2009. 20(6): p. 646-55.
48. Musgrave, D.S., et al., Human skeletal muscle cells in ex vivo gene therapy to deliver bone morphogenetic protein-2. J Bone Joint Surg Br, 2002. 84(1): p. 120-7.
49. Burastero, G., et al., The association of human mesenchymal stem cells with BMP-7 improves bone regeneration of critical-size segmental bone defects in athymic rats. Bone, 2010. 47(1): p. 117-26.
50. Marcacci, M., et al., Stem cells associated with macroporous bioceramics for long bone repair: 6- to 7-year outcome of a pilot clinical study. Tissue Eng, 2007. 13(5): p. 947-55.
51. Hernigou, P., et al., Percutaneous autologous bone-marrow grafting for nonunions. Influence of the number and concentration of progenitor cells. J Bone Joint Surg Am, 2005. 87(7): p. 1430-7.
52. Quarto, R., et al., Repair of large bone defects with the use of autologous bone marrow stromal cells. N Engl J Med, 2001. 344(5): p. 385-6.
53. Takahashi, K., et al., Induction of pluripotent stem cells from adult human fibroblasts by defined factors. Cell, 2007. 131(5): p. 861-72.
54. yamanaka, S., Induced pluripotent stem cells: past, present, and future. Cell Stem Cell, 2012. 10(6): p. 678-84.
55. Sun, N., et al., Patient-specific induced pluripotent stem cells as a model for familial dilated cardiomyopathy. Sci Transl Med, 2012. 4(130): p. 130ra47.
56. Hiramatsu, K., et al., Generation of hyaline cartilaginous tissue from mouse adult dermal fibroblast culture by defined factors. J Clin Invest, 2011. 121(2): p. 640-57.
57. Liang, B., et al., Ectopic expression of SOX9 in osteoblasts alters bone mechanical properties. Calcif Tissue Int, 2012. 90(2): p. 76-89.

66
Total joint arthroplasty is an extremely successful orthopaedic surgery with approximately 600,000 total hip and knee replacements performed annually. Moreover, it is estimated that by the year 2030, there will be between 3.5 – 4 million total hip and knee replacements performed annually1,2. While these procedures routinely provide patients excellent outcomes, there are a number of complications that continue to plague the field of arthroplasty. The most common complication resulting in the need for revision arthroplasty is aseptic loosening, which by definition is implant loosening without clinical or microbiologic evidence of active infection3. Periprosthetic osteolysis is believed to be the largest contributing factor towards aseptic loosening4,5. The generation of periprosthetic wear particles into the effective joint space is thought to be the sentinel event responsible for inducing osteolysis5. Macrophages phagocytose these microscopic wear particles and then synthesize proinflammatory cytokines such as tumor necrosis factor alpha, interleukin 1, and interleukin 6, which ultimately leads to increased osteoclast differentiation and resorption of the periprosthetic bone3,6.
Pathogen-associated molecular patterns (PAMPs) are a group of small molecular motifs that are recognized by and activate the innate immune system. Lipopolysaccharide (LPS) and lipoteichoic acid (LTA), the classic Gram negative and Gram positive endotoxins, respectively,
are examples of bacterial PAMPs. Our lab has been at the forefront of investigating the possibility that bacterial PAMPs contribute to aseptic loosening. Metallic and polymeric wear particles with adherent LPS and LTA induce higher cytokine production in macrophage cell cultures and cause higher rates of osteolysis in mice compared to endotoxin-free wear particles7-13. LPS has also been found in periprosthetic tissue surrounding aseptically loose joints which further confirms the likelihood that PAMPs have an integral role in both osteolysis and aseptic loosening14. Three potential sources of bacterial PAMPs include implant manufacturing15, systemically-derived sources from gut flora, minor infections and dental procedures16,17 and bacterial biofilms18,19.
Toll-like receptors (TLRs) are a group of thirteen evolutionarily conserved transmembrane receptors located on macrophages that bind PAMPs associated with microbial pathogens and subsequently activate the innate immune system20,21. PAMPs activate specific cognate TLRs, whereby LPS and LTA bind to TLR4 and TLR2, respectively20,21. Previous work from our lab demonstrated that TLR4 and TLR2 are required for the increase in osteolysis and macrophage cytokine production induced by PAMPs adherent to wear particles7,11; thereby illustrating the important link between PAMP-TLR interaction, activation of the innate immune system and particle-induced
osteolysis.
The cytoplasmic portion of TLRs has a conserved Toll/IL-1 receptor (TIR) domain that binds various adaptor proteins19. In 2001, an adaptor protein unique to TLR2 and TLR4 was discovered by two different labs. Horng et al.22, named the molecule TIR domain-containing adaptor protein (TIRAP), while Fitzgerald et al.23, named it MyD88 adaptor-like protein (Mal). TIRAP/Mal is a 235 amino acid adaptor protein whose C-terminus possesses a TIR domain which exclusively binds to TLR2 and TLR422,23. TIRAP/Mal activation promotes Nuclear Factor-KappaB (NF-κB) signal transduction, which ultimately leads to inflammatory cytokine production and secretion (Figure 1). Recent work by Del vescovo et al identified several single nucleotide polymorphisms within genes regulating inflammatory cytokine signaling that may increase the risk of aseptic loosening and osteolysis24. There is also preliminary evidence linking three single nucleotide polymorphisms within the TIRAP/Mal gene to increased risk of aseptic loosening. However, no studies to date have investigated the role of TIRAP/Mal in response to orthopaedic wear particles either in vitro or in vivo.
Given the potential predisposition to osteolysis and the lack of orthopaedic basic science research on TIRAP/Mal, our lab found it imperative to further investigate whether TIRAP/Mal impacts the proinflammatory cytokine production and osteolysis in response to orthopaedic wear particles. Our primary
IS ASEPTIC LOOSENING MEDIATED By TIRAP/MAL? FUTURE RESEARCH GOALS Christopher P. Bechtel, MD1, Jeremy J. Gebhart, BS1, Joscelyn M. Tatro, MS1, Edward M. Greenfield, PhD1,2,3
Departments of 1Orthopaedics, 2Physiology and Biophysics and 3Pathology, Case Western Reserve University, University Hospitals of Cleveland
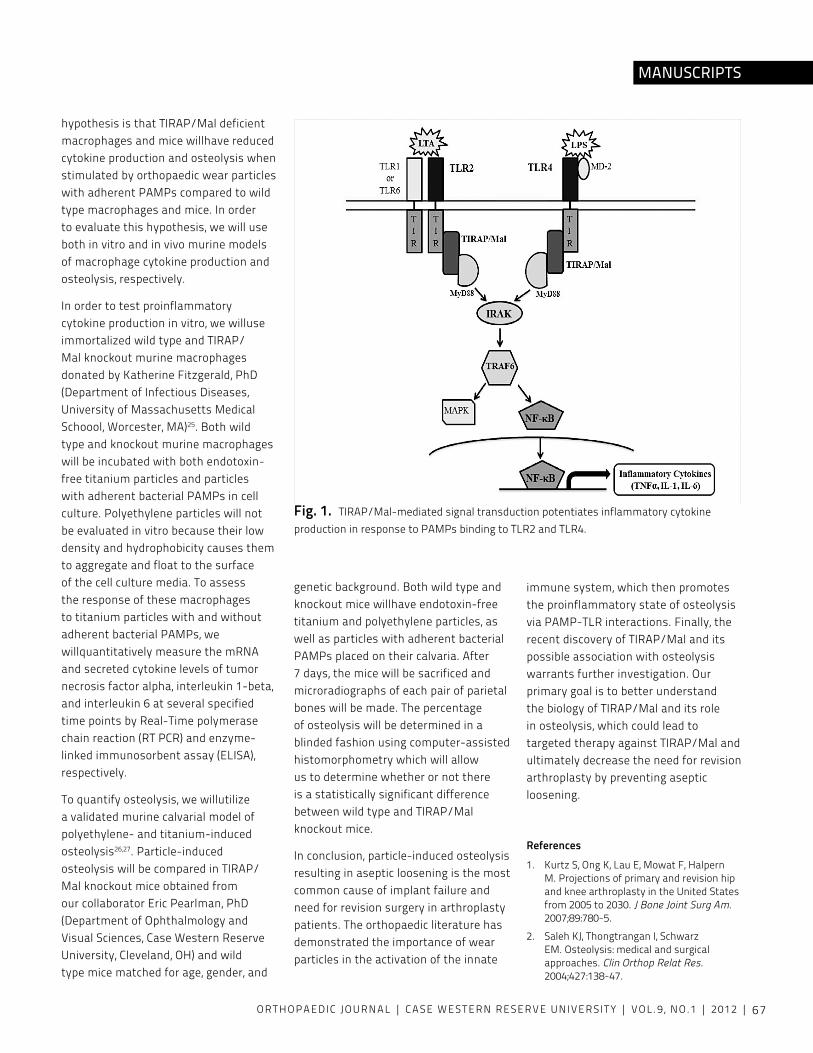
ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 67
hypothesis is that TIRAP/Mal deficient macrophages and mice willhave reduced cytokine production and osteolysis when stimulated by orthopaedic wear particles with adherent PAMPs compared to wild type macrophages and mice. In order to evaluate this hypothesis, we will use both in vitro and in vivo murine models of macrophage cytokine production and osteolysis, respectively.
In order to test proinflammatory cytokine production in vitro, we willuse immortalized wild type and TIRAP/Mal knockout murine macrophages donated by Katherine Fitzgerald, PhD (Department of Infectious Diseases, University of Massachusetts Medical Schoool, Worcester, MA)25. Both wild type and knockout murine macrophages will be incubated with both endotoxin-free titanium particles and particles with adherent bacterial PAMPs in cell culture. Polyethylene particles will not be evaluated in vitro because their low density and hydrophobicity causes them to aggregate and float to the surface of the cell culture media. To assess the response of these macrophages to titanium particles with and without adherent bacterial PAMPs, we willquantitatively measure the mRNA and secreted cytokine levels of tumor necrosis factor alpha, interleukin 1-beta, and interleukin 6 at several specified time points by Real-Time polymerase chain reaction (RT PCR) and enzyme-linked immunosorbent assay (ELISA), respectively.
To quantify osteolysis, we willutilize a validated murine calvarial model of polyethylene- and titanium-induced osteolysis26,27. Particle-induced osteolysis will be compared in TIRAP/Mal knockout mice obtained from our collaborator Eric Pearlman, PhD (Department of Ophthalmology and visual Sciences, Case Western Reserve University, Cleveland, OH) and wild type mice matched for age, gender, and
genetic background. Both wild type and knockout mice willhave endotoxin-free titanium and polyethylene particles, as well as particles with adherent bacterial PAMPs placed on their calvaria. After 7 days, the mice will be sacrificed and microradiographs of each pair of parietal bones will be made. The percentage of osteolysis will be determined in a blinded fashion using computer-assisted histomorphometry which will allow us to determine whether or not there is a statistically significant difference between wild type and TIRAP/Mal knockout mice.
In conclusion, particle-induced osteolysis resulting in aseptic loosening is the most common cause of implant failure and need for revision surgery in arthroplasty patients. The orthopaedic literature has demonstrated the importance of wear particles in the activation of the innate
immune system, which then promotes the proinflammatory state of osteolysis via PAMP-TLR interactions. Finally, the recent discovery of TIRAP/Mal and its possible association with osteolysis warrants further investigation. Our primary goal is to better understand the biology of TIRAP/Mal and its role in osteolysis, which could lead to targeted therapy against TIRAP/Mal and ultimately decrease the need for revision arthroplasty by preventing aseptic loosening.
References1. Kurtz S, Ong K, Lau E, Mowat F, Halpern
M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89:780-5.
2. Saleh KJ, Thongtrangan I, Schwarz EM. Osteolysis: medical and surgical approaches. Clin Orthop Relat Res. 2004;427:138-47.
Fig. 1. TIRAP/Mal-mediated signal transduction potentiates inflammatory cytokine production in response to PAMPs binding to TLR2 and TLR4.
MANUSCRIPTS
68
3. Wooley PH, Schwarz EM. Aseptic loosening. Gene Ther. 2004;11:402-7.
4. Jacobs JJ, Roebuck KA, Archibeck M, Hallab NJ, Glant TT. Osteolysis: basic science. Clin Orthop Relat Res. 2001;393:71-7.
5. Harris WH. Wear and periprosthetic osteolysis: the problem. Clin Orthop Relat Res. 2001;393:66–70.
6. Ingham E, Fisher J. The role of macrophages in osteolysis of total joint replacement. Biomaterials. 2005;26:1271-86.
7. Bi y, Collier TO, Goldberg vM, et al. Adherent endotoxin mediates biological responses of Ti particles without stimulating their phagocytosis. J Orthop Res. 2002;20:696–703.
8. Bi y, Seabold JM, Kaar SG, et al. Adherent endotoxin on orthopedic wear particles stimulates cytokine production and osteoclast differentiation. J Bone Miner Res. 2001;16:2082–91.
9. Brooks RA, Wimhurst JA, Rushton N. Endotoxin contamination of particles produces misleading inflammatory cytokine responses from macrophages in vitro. J Bone Joint Surg Br. 2002;84:295–9.
10. Charlebois SJ, Daniels AU, Smith RA. Metabolic heat production as a measure of macrophage response to particles from orthopedicimplant materials. J Biomed Mater Res. 2002;59:166–75.
11. Greenfield EM, Beidelschies MA, Tatro JM, et al. Bacterial pathogen-associated molecular patterns stimulate biological activity of orthopaedic wear particles by activating cognate Toll-like receptors. J Biol Chem. 2010;285;32378-84.
12. Cho DR, Shanbhag AS, Hong Cy, et al. The role of adsorbed endotoxin in particle-induced stimulation of cytokine release. J Orthop Res. 2002;20:704–13.
13. Skoglund B, Larsson L, Aspenberg PA. Bone-resorptive effects of endotoxin-contaminated high-density polyethylene particles spontaneously eliminated in vivo. J Bone Joint Surg Br. 2002;84:767–73.
14. Nalepka JL, Lee MJ, Kraay MJ, et al. Lipopolysaccharide found in aseptic loosening of patients with inflammatory arthritis. Clin Orthop Relat Res. 2006;451:229-35.
15. Ragab AA, van De Motter R, Lavish SA, et al. Measurement and removal of adherentendotoxin from Ti particles and implant surfaces. J Orthop Res. 1999;17:803–9.
16. Cooperstock MS, Tucker RP, Baublis Jv. Possible pathogenic role of endotoxin in Reye’s Syndrome. Lancet. 1975;1:1272–4.
17. Inada K, Endo S, Takahashi K, et al. Establishment of a new perchloric acid treatment method to allow determination of the total endotoxin content in human plasma by the limulus test and clinical application. Microbiol Immunol. 1991;35:303–14.
18. Greenfield EM, Bi y, Ragab AA, et al. Does endotoxin contribute to aseptic loosening of orthopedic implants? J Biomed Mater Res B Appl Biomater. 2005;72:179–85.
19. Tunney MM, Patrick S, Curran MD, et al. Detection of prosthetic hip infection at revision arthroplasty by immunofluorescence microscopy and PCR amplification of the bacterial 16S rRNA gene. J Clin Microbiol. 1999;37:3281–90.
20. Takeda K, Akira S. Toll-like receptors in innate immunity. Int Immunol. 2005;17:1-14.
21. vogel SN, Fitzgerald KA, Fenton MJ. TLRs: differential adapter utilization by Toll-like receptors mediates TLR-specific patterns of gene expression. Mol Interv. 2003;3:466-77.
22. Horng T, Barton GM, Medzhitov R. TIRAP: An adapter molecule in the Toll signaling pathway. Nat Immunol. 2001;2:825-41.
23. Fitzgerald KA, Palsson-McDermott EM, Bowie AG, et al. Mal (MyD88 adapter-like) is required for Toll-like receptor-4 signal transduction. Nature. 2001;413:78-83.
24. Del vescovo E, MacInnes SJ, Ollier WER, et al. Genetic variation in inflammasome signaling and bone turnover pathways and risk of osteolysis after total hip arthroplasty. Trans Orthop Res Soc, 2012.
25. Nagpal K, Plantinga TS, Wong J, et al. A TIR domain variant of MyD88 adapter-like (Mal)/TIRAP results in loss of MyD88 binding and reduced TLR2/TLR4 signaling. J Biol Chem. 2009;284:25742-8.
26. Karr SG, Ragab AA, Kaye SJ, et al. Rapid repair of Ti particle-induced osteolysis is dramatically reduced in aged mice. J Orthop Res. 2001;19:171-8.
27. Taki N, Tatro JM, Nalepka JK, et al. Polyethylene and Ti particles induce osteolysis by similar, lymphocyte-independent, mechanisms. J Orthop Res. 2005;23:376-83.
IS ASEPTIC LOSSENING MEDIATED bY TIRAP/MAL?

ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 69
CARTER-MAkLEY VISITING PROFESSOR LECTURESHIP FOR MUSCULOSkELETAL ONCOLOGY 2011
November 1-2, 2011
visiting Professor
Michael J. Klein, MDProfessor, Pathology and Laboratory MedicineDirector of Pathology and Laboratory MedicineHospital for Special SurgeryWeill Medical College of Cornell University New york, New york
Drs Makley, Klein, and Getty
vISITING PROFESSORS
November 13-14, 2012
visiting Professor
Dempsey Springfield, MDAssociate Orthopaedic SurgeonMassachusetts General HospitalHarvard Medical SchoolBoston, Massachusetts
Musculoskeletal Orthopaedic Oncology: My Lifetime Perspective
Limb Salvage is not a new desire. Major resections were done even as anesthesia was just being used. Jan Mikulicz-Radecki, a surgeon in vienna, who was an early advocate of surgical gloves and mask in the late 19th century advocated curative surgery for sarcomas.
A number of limb salvage operations were described but only done in a limited number of centers.
Although there are those who believe Damien and Cosmos transplanted a limb, Erich Lexer at the University of Wurzburg, transplanted an entire knee–still warm– in 1907. Despite some clinical successes, bone transplants were not considered useful until the late 1970’s.
There was little follow-up and no registries until E.A. Codman from Boston established the first tumor registry. From his ideas came the current tumor registries that every hospital now must
have. This was the beginning of a better understanding of outcomes.
Bone biology was being explored in the early 1900’s. In Chicago, Dallas Phemister studied how bone grafts heal and his studies explained much of what we know about bone healing. He used large autogenous bone grafts to reconstruct the skeleton after tumor resection. His protégé at the University of Chicago was Howard Hatcher. Hatcher is considered the father and grandfather to many of us in the world of musculoskeletal (MSK) tumors. He trained many of the orthopaedic educators of the generation just prior to my generation and we all have benefited from their dedication and education.
Other advances were being made that would benefit the MSK oncologist. Austin Moore implanted this vitallium prosthesis into a patient with a giant cell tumor of bone in the early 1940’s This is thought to be the first prosthetic replacement of a bone after a tumor resection. Interestingly, Henry Bohlman’s father
CARTER-MAkLEY VISITING PROFESSOR LECTURESHIP FOR MUSCULOSkELETAL ONCOLOGY 2012

70
CARTER-MAkLEY VISITING PROFESSOR LECTURESHIP FOR MUSCULOSkELETAL ONCOLOGY
was involved and reportedly he buried vitallium implants in his backyard to prove they were resistant to corrosion. I heard this story from Dr. Marcus.
That was the state of the specialty when I started my career. In May of 1977, the first meeting of a group of surgeons interested in MSK tumor was in Boston and was organized by Crawford Campbell, Henry Mankin, Hugh Watts, and Norman Jaffe.
We did amputations for most malignant tumors. Limb salvage surgery was mainly for Giant Cell Tumor of Bone. We had some tumor prostheses but they were crude by today’s standards.
MSK pathology was just beginning to be explored. Henry Jaffe and Louis Lichtenstein were together in New york City and described many of the MSK bone tumors assigning histologic criteria used for their diagnosis. After these two are a number of pathologists interested in MSK bone tumors including Lauren Ackerman, Howard Dorfman, Harlan Spjut, Jack Carter, Andy Huvos, Lent Johnson, Fritz Schajowicz, and Dave Dahlin just to name a few. Other pathologists were interested in the MSK soft tissue tumors. Stout and Lattes wrote the AFIP fascicle on soft tissue tumors. After which Enzinger and Weiss published their book devoted to soft tissue tumors and continues to be the major reference for all interested in this topic. Dr. Weiss continues as a faculty member at Emery University.
Before my professional career began, chemotherapy for MSK tumor was rarely used. There was Coley’s toxin and some chemotherapists were experimenting with new drugs. James Holland, Norman Jaffe, and Gerald Rosen had just published improved survival for patients with osteosarcoma. In Gainesville, William Enneking and Jim Neff were using immunotherapy to treat osteosarcoma.
We did not have three dimensional imaging when I started. We used angiography and bone scans. Sir Godrey Hounsfield and Allan Cormack, working in different countries, came up with the idea for computed tomography. This dramatically and almost immediately changed the practice of MSK surgery. Then the MRI became clinically useful. Raymond Damadian invented the MRI but Sir Peter Mansfield and Paul Lauterbur received the Nobel Prize.
The surgeons involved in MSK tumors were ready for all of these advances. William Enneking at the University of Florida, Jack Ivins at the Mayo Clinic, Mario Campanacci at the Rizzoli Institute in Bologna, Bertil Stener in Goteborg Sweeden were the major players.
There were changes in the management of benign bone tumors also. Injections for unicameral bone cysts and Langerhans histiocytosis was advanced by Scaglietti
from Florence, Italy. Cementation
for Giant Cell Tumor of Bone was done by Persson in Holland. Radiofrequency ablation was done for osteoid osteomas by Dan Rosenthal in Boston. Ian Taylor, in Australia, demonstrated how the fibula could be transferred with its vascular supply.
Ralph Marcove and Hugh Watts were early advocates for limb salvage for patients with osteosarcoma. Fred Eibler advocated multimodal treatments. Frank Parrish, Carlos Ottolenghi, and Henry Mankin reintroduced bone transplants. John Scales in England and Ed Chao at the Mayo Clinic improved the metal
prosthesis. Mike Lewis introduced the first “growing” prosthesis. Marin Salzer and Rainer Kotz showed that the rotationplasty, that was originally used to treat proximal femoral focal deficiency (PFFD), could be used for the young patient with an osteosarcoma of the distal femur. Herman Suit and Henry Mankin showed that adjuvant irradiation could reduce the need for amputations in patients with soft tissue sarcomas.
Now the care of the patient with a MSK tumor is a team sport. The radiologist, pathologist, medical oncologist, pediatric oncologist, and surgeon must confer and decide together the optimal method of treatment. There are many new tools and toys and I expect many advances to come.
Dr Patrick Getty
Drs Makley, Getty, Springfield, and Marcus
Dr Marcus & Dr Springfield concluding the 2012 Carter-Makley visiting Professor Lectureship.

ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 71
ALLEN FELLOWSHIP VISITING PROFESSOR 2011
October 11-12, 2011
visiting Professor
Sanford E. Emery, MDProfessor and Chairman, Department of Orthopaedic SurgeryWest virginia UniversityMorgantown, West virginia
ALLEN FELLOWSHIP VISITING PROFESSOR 2012
October 16-17, 2012
visiting Professor
Gary E. Friedlaender, MDWayne O. Southwick Professor of Orthopaedics and Rehabilitation and Professor of PathologyChair, Department of Orthopaedics and Rehabilitationyale School of MedicineNew Haven, Connecticut Dr Bechtel, left, and Dr Reich, 2011-2012 Allen Fellows presenting
their research.
The 2012-13 & 2011-2012 Allen Fellows with Dr. Friedlaender. Drs Friedlaender and Marcus.
VISITING PROFESSORS

72
April 24-25, 2012
visiting Professor
Michael B. Millis, MDProfessor, Department of Orthopaedic SurgeryBoston Children’s Hospital Harvard Medical School Boston, Massachusetts
Grand Rounds Title: “Hipology 2012, A User Friendly Guide to Hip Function and Hip-Preserving Surgery in the Adolescent and young Adult Hip”
RAINbOW VISITING PROFESSOR 2012
Front row: Allison Gilmore, MD, Suzanne Fortuna, Michael Millis, MD, Connie Poe-Kochert. Back row: Raymond Liu, MD, Daniel Cooperman, MD, George Thompson, MD, Joe Son-Hing, MD, and Randall Marcus, MD.
June 12-13, 2012
visiting Professor
Terry R. Light, MDProfessor and Chairman, Department of Orthopaedic SurgeryLoyola University Stritch School of MedicineMaywood, Illinois
RESIDENT RESEARCH VISITING PROFESSOR 2012
Dr Light and Marcus after Dr Light’s Grand Rounds.

ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 73
VISITING PROFESSORS
Timothy Wright, PhD
MUSCULOSkELETAL RESEARCH DAY VISITING PROFESSOR 2012
April 3-4, 2012
visiting Professor
Timothy Wright, PhDSenior Scientist, Hospital for Special SurgeryProfessor of Applied Biomechanics, Department of Orthopaedic SurgeryWeill Medical College of Cornell University New york, New york
Drs Greenfield, Rimnac, Wright, and Akkus Members of the Greenfield lab with Dr Wright. Dr Bonsignore won the “Best Poster Award” during the CWRU Musculoskeletal Research day.
May 8-9, 2012
visiting Professor
Alexander J. Ghanayem, MDChief, Spine SurgeryDepartment of Orthopaedic SurgeryLoyola University Stritch School of MedicineMaywood, Illinois
Grand Rounds Title: “Interbody Cage Complications: Evolution, Technical & Biological”
bOHLMAN VISITING PROFESSOR 2012
Drs Goodfellow, Furey, Ghanayem, Ahn, & Marcus at the conclusion of the Bohlman visiting Professor Program.
74
DR LEROy KLEIN OBITUARy
It is with great sadness that I inform you of the recent death of LeRoy Klein, MD,
PhD, Professor Emeritus of Orthopaedics, Case Western Reserve University School of Medicine.
Dr Klein passed away on September 5, 2012, from complications of Alzheimer’s Disease. He was 85 years old and is survived by his wife Elizabeth and 3 children.
Dr Klein was a Professor and scientist in the Department of Orthopaedics at Case Western Reserve University, with secondary appointments in Biochemistry and Macromolecular Science for over 4 decades. He was widely published and made significant contributions to our understanding of the biology of the musculoskeletal system.
Kenneth “van” Jackman MD, Professor Emeritus of Pediatric Orthopaedics at
the University of Rochester, 69, passed away peacefully at his home on Upper Saranac Lake surrounded by family on Wednesday, Aug. 18, 2010 after a six-month battle with ALS.
He received a BA at Pomona College in 1963, his MD at the University of Rochester in 1967 and served at the U.S. Naval Hospital in Guam from 1969-1971.
In Saranac Lake, he was a member of SARANAK (Search and Rescue Association of the Northern Adirondacks), AARA (Adirondack Amateur Radio Association) and a naturalist volunteer at The Wild Center (Natural History Museum of the Adirondacks). Dr Jackman was an alumni of the Case Western Reserve Orthopaedic training program 1972 - 1975.
DR KENNETH JACKMAN OBITUARy

ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 75
EXITING RESIDENTS’ FUTURE PLANS
From left: Dr James Murphy, Dr Michael Abdulian, Dr Zachary Gordon, Dr Marcus, Dr Kasra Ahmadinia, Dr Ari Levine, Dr Daniel Master.
Congratulations to the six graduating chiefs of 2012. All six will be doing a
fellowship in the 2012/2013 academic year. Listed below are their subspecialty of choice and the fellowship program they will be attending.
James Murphy, MDAdult ReconstructionUniversity of PennsylvaniaPhiladelpha, PA
Michael Abdulian, MDSports Medicine University of Southern California Los Angeles, CA
Zachary Gordon, MDSpineUniversity of Pittsburgh Medical CenterPittsburgh, PA
Kasra Ahmadinia, MDSpineRush University Medical CenterChicago, IL
Ari Levine, MDTraumaOrthopaedic TraumaCarolinas Medical CenterCharlotte, NC
Daniel Master, MDHandStanford UniversityPalo Alto, CA
76
2012 FELLOWSHIP MATCH RESULTS
Ethan Lea, MDTraumaUC Davis Medical CenterUniversity of California-Davis Sacramento, CA
James Learned, MD Trauma Harborview Medical CenterUniversity of Washington Seattle, WA
Scott Kling, MD Sports MedicineUniversity of Pittsburgh Medical CenterUniversity of PittsburghPittsburgh, PA
Troy Mounts, MDSpineThe Rothman Institute at JeffersonThomas Jefferson Medical CollegePhiladelphia, PA
Erik Schnaser, MDAdult Reconstruction Hospital for Special Surgery Weill College of Medicine of Cornell UniversityNew york, Ny
1. Manuscript submissions are accepted in electronic format only. ALL SUBMISSIONS SHOULD BE SENT TO [email protected] and have COJ submission as the subject heading. Alternatively, the submission can be submitted via CD. ALL submissions should be in Word format. Photos, figures and tables should be submitted in seperate jpeg, tiff or PDf files, not embedded in the Word document.
2. Title should include author’s name, degree achieved, institutional affiliation, and the order of authors in which they should appear.
3. Manuscipta. Abstract – Limit to 325 wordsb. Body –
i. Introduction - State the problem that led to the study, including a concise review of only the relevant literature. State your hypothesis and the purpose of the study.
ii. Methods - Describe the study design in detail using standard methodologic terms. All study designs should include information how the sample was identified (inclusions and exclusions). The statistical section should be described in detail, with particular emphasis on the statistical strategy

ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 77
INSTRUCTIONS FOR AUTHORS
1. Manuscript submissions are accepted in electronic format only. ALL SUBMISSIONS SHOULD BE SENT TO [email protected] and have COJ submission as the subject heading. Alternatively, the submission can be submitted via CD. ALL submissions should be in Word format. Photos, figures and tables should be submitted in seperate jpeg, tiff or PDf files, not embedded in the Word document.
2. Title should include author’s name, degree achieved, institutional affiliation, and the order of authors in which they should appear.
3. Manuscipta. Abstract – Limit to 325 wordsb. Body –
i. Introduction - State the problem that led to the study, including a concise review of only the relevant literature. State your hypothesis and the purpose of the study.
ii. Methods - Describe the study design in detail using standard methodologic terms. All study designs should include information how the sample was identified (inclusions and exclusions). The statistical section should be described in detail, with particular emphasis on the statistical strategy
used to analyze the data. iii. Results – Provide a detailed report on
the data obtained during the study. iv. Conclusion - Be succinct in this section.
Describe what your study shows. Discuss the importance of this article with regard to the relevant literature. Analyze your data and discuss their strengths, their weaknesses, and the limitations of the study.
4. References a. The references should be numbered according
to the order of citation in the text (not alphabetically) and should be in PubMed/Index Medicus format (go to the NCBI web site for examples (www.ncbi.nlm.nih.gov/entrez/query.fcgi).
b. All references must be cited in the text.5. Figures and Tables should be submitted separate
from the manuscript text.6. Submit all Figures in TIFF format.
a. No more than 8 Figures per article.7. Scientific Manuscripts – Limit total word count to
4000.8. Case Reports – Limit total word count to 1500.
CALL FOR ABSTRACTS 2013Dear faculty, fellows, residents, and students,
We are now taking scholarly submissions for the 2013 Case Orthopaedic Journal.
The manuscripts should be on research that has been completed, should answer a scientific question, should be of high scientific quality, and should be original.
The submission deadline for the journal will be Sept 1, 2013.
Previously published articles are welcome for submission as long as there is a copyright release from the publisher. All submissions will go through a peer review process.
Submissions should be emailed to Lorraine Stern at [email protected].
78
Our knee revision system manages
metaphyseal defects…Does yours?
www.DePuy.com
©DePuy Orthopaedics, Inc. 2012. All rights reserved.
Join the revolution. Talk to your DePuy Orthopaedics sales rep today about Knee Revision Solutions.
Metaphyseal Sleeves
3
7
DePuy Revision Knee Solutions
Competition
Featuring:
Proprietary Rotating Platform Technology
• Diffuse loosening forces, especially important with additional constraint
• Universal tray, used with PS, constrained, and hinge
Proprietary Metaphyseal Sleeve Technology
• Compressively load the bone
• Provide strong foundation for implant stability
• Fill bone defects
• Universal sleeves can be used with PS, constrained, and hinge
Join the RevolutionThe Fastest Growing Knee Revision Portfolio
ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 79
T H E B E N E F I T S O F P A R T N E R I N G W I T H N R I N C L U D E : n Our extensively trained and certified clinical staff can measure, fit and
educate patients about the bracing we offer.
4 Appointments with our clinicians are available in a variety of healthcare settings conveniently located in Ohio, Western Pennsylvania and West Virginia, including Cleveland, Pittsburgh, Erie, Wheeling and Morgantown.
4 Our knowledgeable product and insurance specialists can assist healthcare professionals and their patients with product selection and insurance guideline education.
4 We take the hassle of working with insurance companies off of patients so they can focus on regaining their health. NR is a participating provider with Medicare and hundreds of commercial insurances, as well as select Medicaid and Managed Care plans.
1-800-451-6510T www.nationalrehab.comW
For more information about National Rehab (NR):
A trusted pArtner in pAtient cAre.
National Rehab (NR) is a leading provider of custom and off-the-shelf orthopedic products, as well as wound care, urological, ostomy and incontinence supplies.
NR has earned the reputation among patients, healthcare providers and insurers alike as being patient-centric. With fast, efficient and empathetic, patients and healthcare professionals have peace of mind knowing they truly have a partner that puts their needs first.
© 2012 National Rehab Equipment, Inc. All Rights Reserved. NR_AD_OP_CaseJournal_092112
NR_AD_OP_CaseJournal_092012.indd 1 9/27/12 9:59 AM

80
The Future of Minimally Invasive SurgeryCALIBER™ Expandable Lumbar Fusion Device
Caliber™ is an innovative expandable lumbar fusion
device that represents the future of minimally invasive
surgery by assisting the surgeon in achieving proper
endplate-to-endplate fit, while helping to reduce
insertion impaction and nerve root retraction.
life moves us is a registered trademark of Globus Medical.
www.globusmedical.com 866.456.2871
ORTHOPAEDIC JOURNAL | CASE WESTERN RESERvE UNIvERSITy | vOL.9 , NO.1 | 2012 | 81
The Future of Minimally Invasive SurgeryCALIBER™ Expandable Lumbar Fusion Device
Caliber™ is an innovative expandable lumbar fusion
device that represents the future of minimally invasive
surgery by assisting the surgeon in achieving proper
endplate-to-endplate fit, while helping to reduce
insertion impaction and nerve root retraction.
life moves us is a registered trademark of Globus Medical.
www.globusmedical.com 866.456.2871
Could more efficiencybe achieved in your OR?
Let Zimmer® Patient Specific Instruments guide you.
Cutting edge pre-op planning
Customizedinstruments
Streamlinedsurgical technique
OR efficiency Reduced instrumentation
For more information, contact your Zimmer representative.
A collaborative partnership with Materialise™.©2012 Zimmer, Inc. Materialise™ is a trademark of Materialise N.V.
www.zimmer.com
PSI Efficiency Ad_8.5625x11.125_9-11-12.indd 1 9/11/2012 8:54:34 AM

82
Track Malone
Three Rivers Orthopaedic & Spine Products, Inc. www.3riv.com Representing Stryker Reconstructive, Trauma & Spine Products
Craig Liberatore
Terry Koziara
Brian Inkrott
Pat Bryan Jack Frampton
Mike Lynch Jorge Rodriguez
Bill Lynch
Roger Herrmann Ben Bair Chris Adler
The Three Rivers team wishes you success wherever your training takes you.
Amber Hruska