case no. 12 sh, 25 years old with a history of asthma since childhood presented to the opd clinic...
TRANSCRIPT

Case No. 12Case No. 12SH, 25 years old with a history of asthma since childhood preSH, 25 years old with a history of asthma since childhood presented to the OPD clinic with complaints of worsening dyspnesented to the OPD clinic with complaints of worsening dyspnea and wheezing. He had similar intermittent symptoms over ta and wheezing. He had similar intermittent symptoms over the past 3 months, usually requiring E.R visits. Last E.R visit whe past 3 months, usually requiring E.R visits. Last E.R visit was 2 weeks earlier where he was discharged on inhaled broncas 2 weeks earlier where he was discharged on inhaled bronchodilators and a 10 days course on steroids. He has received hodilators and a 10 days course on steroids. He has received oral glucocorticoids patient still has multiple episodes of wheeoral glucocorticoids patient still has multiple episodes of wheezing and shortness of breath. His present medications include zing and shortness of breath. His present medications include time released theophylline 300 mg BID and salbutamol metertime released theophylline 300 mg BID and salbutamol metered dose inhaler 2 puffs every hour. Previous pulmonary functied dose inhaler 2 puffs every hour. Previous pulmonary function tests revealed normal lung volumes except for the residual on tests revealed normal lung volumes except for the residual volume which is increased. P.E showed a well developed malvolume which is increased. P.E showed a well developed male in respiratory distress: BP=130/80, PR=112/min, RR=40/min,e in respiratory distress: BP=130/80, PR=112/min, RR=40/min, T°=36.6°C. Lungs: diffuse inspiratory and expiratory wheezes. T°=36.6°C. Lungs: diffuse inspiratory and expiratory wheezes.
Diagnosis: AsthmaDiagnosis: Asthma
Asthma is a chronic disease of the respiratory sAsthma is a chronic disease of the respiratory system in which the airway occasionally constricystem in which the airway occasionally constricts, becomes inflamed, and is lined with excessits, becomes inflamed, and is lined with excessive amounts of mucus, often in response to one ve amounts of mucus, often in response to one or more triggers. or more triggers.
It’s divide into 2 phaseIt’s divide into 2 phase
1.1. Early phase which is IgE mediated, associated Early phase which is IgE mediated, associated with histamin release from mast cells.with histamin release from mast cells.
2.2. Late phase is associated with cytokine release.Late phase is associated with cytokine release.
Causes:Causes:
1. Inhalant allergens and oral ingestion.1. Inhalant allergens and oral ingestion.
2. Irritants and others.2. Irritants and others.
Sign and symptom:Sign and symptom:
1. Triad – dyspnea, cough, and wheezing.1. Triad – dyspnea, cough, and wheezing.
2. Bronchospasms.2. Bronchospasms.
3. Bronchiole edema.3. Bronchiole edema.
4. Hypersecretion.4. Hypersecretion.


Lab and Physical exam:Lab and Physical exam:
1.Spirometry:1.Spirometry: FEV1 is <80% of the predicted value.FEV1 is <80% of the predicted value. FEV1/FVC is <75% of the predicted value.FEV1/FVC is <75% of the predicted value. (FEV1: Forced expiratory volume in 1 second. FVC: Forced vital capa(FEV1: Forced expiratory volume in 1 second. FVC: Forced vital capa
city.)city.)
2.Oxygen saturation <95%.2.Oxygen saturation <95%.3.Wheezing on exhalation.3.Wheezing on exhalation.4.Retractions of sternocleidomastoids.4.Retractions of sternocleidomastoids.5.Blood cultures: ↑IgE and eosinophil.5.Blood cultures: ↑IgE and eosinophil.

Prescription for asthmaPrescription for asthma

Drugs used to treat asthmaDrugs used to treat asthma
<Bronchodilator><Bronchodilator> Sympathomimetic agentsSympathomimetic agentsββ2 – Adrenergic angonistsTheophylline<Anti-inflammatory agent>Cromolyn and NedocromilCorticosteroids <Luekotriene antagonists>Montelukast, Zafirlukast, Zileuton


BronchodilatorBronchodilator
MOA : MOA : Relax airway smooth muscle by stimulating adenyl
cyclase and increase the formation of cAMP in the airway tissues that results in bronchodilatation
Side effect:
Anorexia, N/V, abdominal discomfort, headache and anxiety. Seizures or arrhythmia.

Anti-inflammatory agentsAnti-inflammatory agents
MOA: MOA: - Inhibit production of inflammatory cytokine
s. - Reduce bronchial reactivity. - Increase airway caliber.
Side effect:
oral candidiasis, throat irritation, cough, mouth dryness, myositis, gastroenteritis.

Luekotriene antagonistsLuekotriene antagonists
MOA:MOA:
- - inhibition of 5-lipoxygenase and binding of leukotriene D4 to its receptor on target tissues, thereby preventing its action.
Side effect:
Less effect than others two.
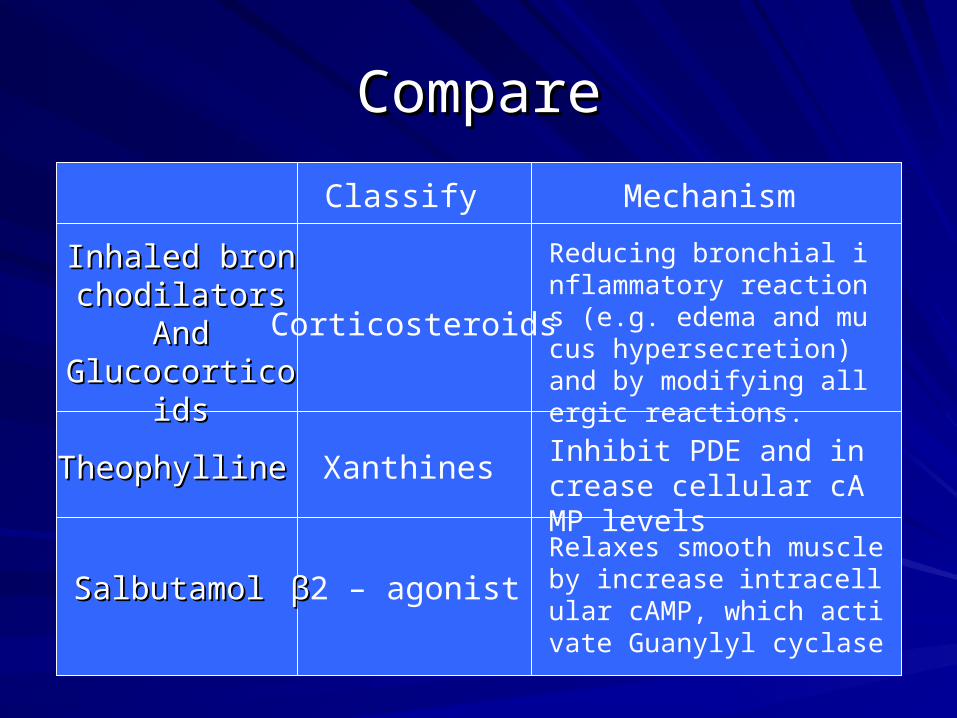
CompareCompare
Inhaled bronchoInhaled bronchodilatorsdilators
AndAndGlucocorticoidsGlucocorticoids
TheophyllineTheophylline
Mechanism
SalbutamolSalbutamol
Inhibit PDE and increase cellular cAMP levels
Classify
Xanthines
ββ2 – agonist
Corticosteroids
Reducing bronchial inflammatory reactions (e.g. edema and mucus hypersecretion) and by modifying allergic reactions.
Relaxes smooth muscle by increase intracellular cAMP, which activate Guanylyl cyclase
Complementary treatmentsComplementary treatments
Sometimes called “alternative” treatments thSometimes called “alternative” treatments that work with your traditional medical care tat work with your traditional medical care to aid in your health.o aid in your health.
Ex:Ex:
YogaYoga

完