caring october 3, 2002
TRANSCRIPT

Inside:Radiation Oncology .............. 11111
Jeanette Ives Erickson ......... 22222Magnet Hospitals
Fielding the Issues ............... 33333Hospital Emergency IncidentCommand System
Exemplars ............................. 66666Sheila Brown, RNKaren Reed, RTT
NERBNA 30th AnniversaryCelebration ........................ 88888
Patient Safety ........................ 99999Patient Observervation Program
AMMP RecognitionLuncheon ....................... 1010101010
Educational Offerings ........ 1111111111
Interpreter Services ........... 1212121212
Working together to shape the futureMGH Patient Care Services
CaringCaringOctober 3, 2002
H E A D L I N E S
adiation therapy is oneof the primary weaponsin the treatment of can-cer. Approximately
60% of all patientsdiagnosed with cancer receiveradiation treatment at somepoint during the course of theirdisease. And yet, there is still agreat deal of misunderstandingabout what radiation therapyactually is. Radiation therapyutilizes high-energy x-rays, elec-trons, protons, or other sources
of ionizing radiation to destroytumor cells or prevent them fromreproducing. The goal of radiationtherapy is to maximize the destruc-tion of cancerous cells while mini-mizing injury to the surroundingtissues and organs.
Radiation therapy is similar tosurgery in that it precisely targetsthe tumor and any surroundingtissue that may be at risk for tumorinvolvement. It is not systemic ther-
apy like chemotherapy. Radiationtherapy can be given alone as aprimary treatment, but it is fre-quently used in combination withother forms of cancer therapy,such as chemotherapy and sur-gery. Radiation therapy can begeared toward cure, tumor-con-trol, or palliation of symptomssuch as pain, obstruction, bleed-ing, or neurological deficit due toa compression of the spinal cordby the tumor.
An inside look atRadiation Oncology
—by Katie Mannix, RN, nurse manager,and Kathy Bruce RTT, technical director,
Radiation OncologyR
continued on page 4
At the Northeast Proton Therapy Center, (l-r) staff nurse,Pat McManus, RN; radiation therapist, Jim Matthews, RTT;pediatric anesthesiologist, Mei Sang, MD; and radiation
therapist, Ann Eliachar, RTT, prepare 4-year-old,Logan Shafer, for proton treatment.

Page 2
October 3, 2002October 3, 2002
Magnet Hospital Recognition:an important and coveted
certification
Jeanette Ives Erickson, RN, MS, senior vicepresident for Patient Care and chief nurse
Jeanette Ives EricksonJeanette Ives Erickson
would liketo take thisopportunityto tell you
about an excit-ing process we’re under-taking that involves eachand every one of us.
Many of you alreadyknow what a Magnethospital is, but for thoseof you who don’t, let megive you a brief explana-tion. In the early 1980s,in response to a seriousnursing shortage, researchwas conducted to deter-mine what factors char-acterized those hospitalsthat were best able toattract and retain nursesdespite the shortage.Hospitals that successful-ly attracted and retained
I nurses were termed ‘Mag-net’ hospitals.
In 1993, the Ameri-can Nurse CredentialingCenter, a subsidiary ofthe American NursesAssociation, introducedThe Magnet NursingServices RecognitionProgram, a certificationprocess that recognizesexcellence in patient carebased on excellencethroughout the organiza-tion in key areas such asprofessional practice,professional develop-ment, quality, inter-dis-ciplinary teamwork, ourability to provide cultur-ally competent care, lead-ership, and documen-tation.
Some characteristicsof Magnet hospitals in-clude:
Nurses identify thehospital as a goodplace to work andpracticeHospital has a reputa-tion for quality nursingas rated by patients.Increased retention ofqualified nurses.Lower turnoverLower burn-out rateUse of supplementalstaff virtually non-existentIncreased percentageof registered nursesStaff are more edu-catedFlexible staffingstrategiesHigh degree of team-workStaff work where theirwork has meaning andthey feel good aboutwhat they do.I’m happy to tell you
that MGH is in the pro-cess of preparing to applyfor Magnet hospital cer-tification. As many ofyou know, earning Mag-net hospital status is asformidable a task as earn-ing JCAHO accredi-tation; and the processesare similar in many ways.In both cases we are pro-vided with a list of stan-dards that must be met,and in both cases prepa-ration culminates withan intensive, multi-daysite visit by the certify-ing board.
To guide us in ourpreparation, I have con-
vened a Magnet NursingServices RecognitionSteering Committee, co-chaired by Lori ClarkCarson, RN, and Mari-anne Ditomassi, RN,with staff support pro-vided by Lauren Holm,RN, and Ed Coakley,RN. The Steering Com-mittee is responsible forthe oversight, implemen-tation, and evaluation ofthe entire process, in-cluding communication,marketing, and educa-tion.
Within the SteeringCommittee, four work-groups have been estab-lished to guide specificaspects of our work (see
MGH Guiding Principles
in preparing for the MagnetNursing Services
Recognition ProgramReflective leadership should be evidencedby reflective nursing practice
The process of the Magnet Nursing ServicesRecognition Program application is, in andof itself, an outcome; it is an iterative pro-cess
Every nurse is an active participant in thisjourney
Enrollment of all nurses and departments inthe process is key
Think conceptually—translate concepts intopractical and simple actions
Maximize use of existing groups
The Magnet Nursing Services RecognitionProgram application process dovetails theJCAHO process, although it uniquely high-lights the contributions of nursing to the pa-tient care team
Magnet Work Groups
Inter-Disciplinary Team Workgroup;chaired by Theresa Gallivan, RN, and JudyNewell, RN
Professional Practice Workgroup;chaired by Jackie Somerville, RN, andMarie LeBlanc, RN
Professional Development Workgroup;chaired by Trish Gibbons, RN, and KeithPerlberg, RN
Knowledge Management Workgroup;chaired by Dawn Tenney, RN, and SallyMillar, RN
shaded box below). Theapplication process iscomprised of two com-ponents: evidence collec-tion to document ouralignment with Magnetstandards, and a sitevisit, which will encom-pass several days of on-and off-shift visits topatient care units andother settings throughoutthe hospital.
More and more, Mag-net hospital certificationis being recognized bypatients and the publicas an important factorwhen choosing theirhealthcare providers. It isrecognized by clinicians,
continued on next page

Page 3
October 3, 2002October 3, 2002Fielding the IssuesFielding the IssuesHospital Emergency IncidentCommand System (HEICS)
The Fielding the Issues section of Caring Headlines is an adjunctto Jeanette Ives Erickson’s regular column. This section gives thesenior vice president for Patient Care a forum in which to address
current issues, questions or concerns presented by staffat meetings and venues throughout the hospital.
Question: What is HEICS?Jeanette:HEICS standsfor Hospital EmergencyIncident Command Sys-tem. It is an emergencyresponse system that usesa standardized manage-ment and communicationstructure to assist withthe operation of the hos-pital in the event of acrisis. For example, thereare generic roles andresponsibilities withinthe Incident CommandSystem that allow formaximum flexibility inresponding internally.Everyone knows whatthey’re responsible forand whom they report toduring an emergency.HEICS utilizes a clearchain of command and a
common language toallow hospitals and otheremergency responders tocommunicate effectivelywith one another.
Question:Why is it nec-essary?Jeanette:Given the cur-rent world situation, it isimperative that we areprepared to protect ourpatients and employeesin the event of a crisis.Adopting HEICS stand-ards and integrating thisapproach into our emer-gency preparedness planallows us to communi-cate effectively withother hospitals and agen-cies if necessary.
Question:Where did theHEICS originate?
Jeanette: In the 1980s, afire-protection initiativein the state of Californialed to the development ofa management systemthat has become standardoperating procedure forfire departments acrossthe country. This system,called FIRESCOPE,facilitates inter-stateassistance. Many firedepartments across theUnited States and Can-ada have implementedthis system. In 1987, theHospital Council ofNorthern California ad-apted the system to fithospital emergency re-sponse systems and be-came the original HEICSmodel. For consistency,HEICS is being integrat-
ed into other civil serviceareas and the privatesector as well.
Question:Where are wein planning for HEICS?Jeanette:Senior admini-strators and managersfrom throughout thePartners system haveattended training ses-sions to learn more aboutHEICS. An MGH Steer-ing Committee has beenworking to:
incorporate the inci-dent command system(HEICS) into ourcurrent emergencyresponse plan.integrate responseplans for internal andexternal emergenciesrevise/update policiesand proceduresadd specific responseplans for biological,chemical and nucleareventsIn October, there will
be a tabletop drill to testthe system. This drillwill involve members ofthe Steering Committee
and designated othersand is designed to testour new emergency re-sponse plan. Once theplan is approved, eachdepartment will need toupdate their emergencyplans and training for allstaff.
Question:Will this changemy role in responding toan emergency?Jeanette: When the emer-gency response plan iscompleted, you will needto review it to becomefamiliar with the newlanguage, roles, and com-munication strategies.Some staff may need tobe trained in more spe-cific tasks, as well. Ingeneral, you will need tobe ready to respond asyou do now—to followthe direction of yourmanager or supervisor.
Question:Are other Part-ners hospitals doing thesame?All acute-care hospitalsin the Partners Systemare adopting HEICS.
insurers, politicians andlegislators across thecountry as a symbol ofexcellence in patient caredelivery.
Of the more than5,000 hospitals in theUnited States, fewer than1% have received Mag-net certification, andnone in Massachusetts atthis time.
Because so many ofour values and guidingprinciples echo those ofthe Magnet Nursing Ser-vices Recognition Pro-
Jeanette Ives EricksonJeanette Ives EricksonJeanette Ives EricksonJeanette Ives EricksonJeanette Ives Ericksoncontinued from previous page
gram, I knew we wereready to seek this covet-ed certification. And theresults of our annualsurvey (Staff Perceptionsof the Professional Prac-tice Environment) rein-force my belief that thiscertification is within ourreach.
As we proceed withthe application process,I’ll keep you informed ofour progress, includingthe important work ofour MGH Magnet hos-pital champions, the four
Magnet workgroups, andthe many other groupsand individuals through-out the hospital who areworking hard to help usprepare.
Again, although Mag-net certification is be-stowed by the AmericanNurses Association, itreflects and recognizesthe contributions of allclinicians and all depart-ments throughout thehospital. Excellence inpatient care can only beachieved with the kindof day-to-day collabo-ration and teamwork thatis the hallmark of prac-tice at MGH.
The MGH ProTechProgram
For more than a decade, with support fromthe Boston Private Industry Council and the
Boston Public School System, the MGHProTech Program has helped prepare minority
students for careers in health care.
Open your doors for just one hour to a youngperson interested in learning about careers in
health care. The ProTech Program is looking forstaff to share their work experience by having
small groups of students visit their departmentson the morning of October 24, 2002.
If you are is interested in providing a tour,please e-mail Galia Kagan, program manager,
at [email protected] call 4-8326 by October 15, 2002.
OpporOpporOpporOpporOpportunity is a terrible thing to wastetunity is a terrible thing to wastetunity is a terrible thing to wastetunity is a terrible thing to wastetunity is a terrible thing to waste

Page 4
October 3, 2002October 3, 2002
Part of the MGHCancer Center, the de-partment of RadiationOncology is located onthe lower level of theCox Building. On a ty-pical day, we see num-erous new patients andconduct follow-up exams,perform a variety of spe-cialized procedures andsimulations, and provide200 or more radiationtreatments.
We offer a broadrange of treatment op-tions. External beamtreatment (EBRT) is themost common method ofdelivery. EBRT utilizeshigh-energy x-ray orelectron beams generatedby linear accelerators totreat a wide variety oftumor types and sites.Our five linear accelerat-
ors are fixed pieces ofexpensive and highlycomplex equipment,housed in heavily shield-ed ‘vaults’ that preventradiation exposure tovisitors and staff. Ourlinear accelerators gener-ate beams from 4 millionelectron volts (MeV) to18 MeV. To understandthe power of these ma-chines, compare thesevalues to those of x-raymachines used in diag-nostic radiology, wherehigh-quality images areobtained using between40 thousand electronvolts (KeV) and 120KeV. Through the sci-ence of Radiation Biol-ogy we know that nor-mal cells have a greaterability to recover fromradiation damage than
tumor cells, this allowsus to eradicate manytumors knowing that theside effects of radiationwill diminish over time.
Another area of treat-ment is called brachy-therapy, or implant ther-apy. The prefix, ‘brachy’is from the Greek wordfor short. In brachyther-apy, radioactive implantsdeliver a dose of radia-tion from a short dis-tance, thus the name. Inthis type of treatment,sealed radiation sourcesare placed directly intoor adjacent to the tumor.This is done in the oper-ating room under anes-thesia, or in a procedureroom. Implants are eitherpermanent, as in prostateseed implants, or temp-orary, like those used forcertain gynecologicalcancers.
Another techniqueavailable at MGH (and
in only a few other hos-pitals in the country) isintra-operative radiationtherapy. Room 43 of theBlake Operating Suitehouses a linear accelerat-or dedicated exclusivelyto this specialized tech-nique. Patients with cer-tain types of malignan-cies have benefited froma single high dose ofradiation that is deliver-ed ‘intra-operatively,’i.e., during the course ofa surgical procedure. Thesurgeon, pathologist, andradiation oncologist con-fer on the need for, andpotential benefit of, thiskind of treatment. If thedecision is to proceed, ahighly focused electronbeam is aimed at thetumor bed while literallymoving normal organsand tissues, such as thesmall bowel, out of theway of the beam. Thistreatment is most often
used in the treatment ofpancreatic cancer, rectalcancer, some gynecolog-ical cancers, and connec-tive-tissue tumors.
Our most publicizedtreatment is probably pro-ton therapy. The NortheastProton Therapy Center(NPTC) is located dir-ectly across from theClinics Building andwill become the lowerlevel of the new YawkeyCenter, currently underconstruction. There areonly two proton centersin the country at thistime. This is due to thehigh cost of building themachines themselves,called cyclotrons, andthe complex structuresneeded to contain them.Over the past 25 years,MGH clinicians havedemonstrated the effic-acy of proton therapy inthe treatment of rare tu-mors called, chordomasor chondro-sarcomas,that arise at the base ofthe skull or in the spine.
We have also beensuccessful in treatingmalignant melanomas ofthe eye, avoiding enucle-ation and in many casesalso preserving vision.This is possible due tothe physical properties ofprotons (positively charg-ed particles)—specific-ally that protons stop;and x-rays don’t. Whenconventional x-rays areused, part of the beam’senergy remains in thepatient, and part of itkeeps going. If thisweren’t the case, x-rayimages would not bepossible because no ra-diation would emerge tostrike the film. Protons,on the other hand, will
Radiation OncologyRadiation OncologyRadiation OncologyRadiation OncologyRadiation Oncologycontinued from front cover
continued on next page(Pho
to b
y Pau
l Bat
ista
) (L-r): Radiation therapist, Thomas Forbes, RTT;resident pediatric anesthesiologist, Dr. Kenneth
Toth; and pediatric anesthesiologist, Dr. Steve Korn,prepare young patient, Shoq Lari,
for radiation treatment.

Page 5
October 3, 2002October 3, 2002
travel a certain distanceinto tissue, then literallystop, depositing all theirenergy. This property isvaluable when treatingtumors situated close tosensitive normal tissue ororgans. As the protonprogram grows, we willbe able to expand treat-ment to include manynew anatomic sites. Thismodality is especiallyattractive for pediatricsolid tumors, where cur-rently used technologycan result in impairedgrowth or other undesir-able long-term effects.
One of the most chal-lenging and stimulatingaspects of our work isthe level of diversityamong the patients wetreat. We see patientsfrom throughout NewEngland and around theworld representing a richblend of cultures andethnicities. Our patientsrange in age from pedi-atric to geriatric withcorresponding age-speci-fic needs. Because of thisgreat diversity amongour patient population,close collaboration withour colleagues in SocialServices, Interpreter Ser-vices, and the Interna-tional Office is a must.
A typical course ofradiation therapy requirestreatment once or twice aday, Monday throughFriday, for up to eightweeks. The actual treat-ment can take from 15minutes to more than anhour, depending on thecomplexity of the treat-ment. Computers haveenhanced so many areas
of our lives, and that isespecially true in Radia-tion Oncology. Our abil-ity to obtain superblydetailed images of tu-mors utilizing CT, MRI,and PET (and then fusingthese images) enableshighly ‘conformal’ treat-ment (treatment dosesare shaped and aimed toconform to the shape ofthe tumor). Of course,the success of radiationtherapy relies upon pre-cise delivery to the tumorevery session. Thus, var-ious positioning andimmobilization devicesare used to ensure theaccuracy of patients’positioning and beamalignment. Patients withbrain tumors or othertumors of the head andneck are usually immo-bilized using a custom-made perforated maskaffixed to the treatmenttable. Some intra-craniallesions are treated usingremovable neuro headframes. Other mold andcasting techniques areemployed for other partsof the body.
Most patients receivesmall tattoos to mark keyreference points on theskin. These permanentmarks are needed to eli-minate repeated visits tothe treatment planningsuite and extensive re-working of their plan.One of the most challeng-ing situations arises inthe treatment of youngchildren who may requiregeneral anesthesia fordaily treatments to en-sure correct positioningis maintained.
As technology hasadvanced, the roles ofnurses and radiationtherapists have grown aswell. Collaboration be-tween the two is a keycomponent of care in ourdepartment. Both rolesrequire fundamentalknowledge of the diseaseprocess and radiobiology(the response of the tu-mor and normal tissuesto radiation).
The RadiationOncology Team
The Radiation OncologyTreatment Team consistsof nurses, physicians,radiation therapists, phy-sicists, dosimetrists, andmold room technicians,as well as front-desk andoffice-support staff. Ittakes a multi-disciplin-ary approach to delivertreatment in a safe, effec-tive and individualized
manner. Collaborationbetween all members ofthe team is vital to en-sure seamless, qualitypatient care.
The radiation oncol-ogy nurse practices in anoncology sub-specialtyand has a solid oncologyfoundation in order tounderstand the relation-ship and potential impactthat chemotherapy andsurgery have on a pa-tient’s course of treat-ment (e.g., skin reactions,tissue healing, and therisk for lowered bloodcounts). The scope ofnursing practice in Ra-diation Oncology in-cludes the assessment ofevery patient; providingeducation about the dis-ease, course of treatment,potential side-effects, andany procedures the pa-tient will undergo. Thenurse assists in proced-
Radiation OncologyRadiation OncologyRadiation OncologyRadiation OncologyRadiation Oncologycontinued from previous page
ures such as implants,trans-rectal ultrasounds,neuro frame placement,and post-anesthesia re-covery. The nurse eval-uates the patient on anongoing basis through-out the course of treat-ment to provide appropri-ate symptom-manage-ment for side-effectssuch as nausea, vomit-ing, and fatigue. Pain-assessment and manage-ment are essential aspectsof patient care as theyimpact patients’ abilityto lie on a treatment tableand affect their qualityof life. Many of our pa-tients present with medic-ally complex situationsthat combine physical,cultural, psycho-socialand age-specific needsand concerns that canimpact treatment. Thenurse must be knowledg-
continued on page 8
Radiation oncology staff nurse, Donna Stamatis, RN,assists neurosurgeon, Paul Chapman, MD, in placing
immobilization head frame on patient, Roger Ladurantaye.

Page 6
October 3, 2002October 3, 2002
Sheila Brown, RNRadiation Oncology
M
ExemplarExemplar
y name isSheila Brownand I am anurse in Radi-
ation Oncol-ogy. Before coming toRadiation Oncology, Iworked on adult andpediatric inpatient unitsand spent 12 years in thePediatric Hematology-Oncology OutpatientClinic.
It was in 1991, in thePedi Hem-Onc Clinic,that I first met Greg, a 7-year-old boy with a pin-eal germ cell tumor. Iwas drawn to this youngboy, who had a wonder-ful sense of humor andan incredibly supportive
family who were natural-ly devastated by thisdiagnosis.
Initially, Greg’s braintumor was treated surgic-ally with a sub-total re-section. Over time, Greg’sbeta HCG levels (a mark-er for his tumor) becameelevated. A subsequentMRI of his brain showedthat there was tumorrecurrence. Greg under-went a course of radia-tion treatment to hisbrain and spine. Onceagain, Greg was closelyfollowed with serialMRIs, and in 1997 heexperienced another re-lapse. This time, a moreintensive course of che-
motherapy combinedwith a peripheral bloodstem cell transplant wasneeded, followed byanother surgical resec-tion.
It was during Greg’smultiple hospitalizationsand subsequent visits tothe clinic that I came toreally know him and hisfamily, especially hismother Ann, an intelli-gent strong woman. Shewas by his side constant-ly, staying overnightduring admissions, ask-ing questions about histreatments, and alwaysadvocating for her son.At times, this advocacypresented challenges to
staff. I came to realizehow desperately Annwanted to maintain herson’s sense of indepen-dence despite the manyobstacles in his path. Ibecame a resource per-son for Ann, someoneshe was comfortablecalling with her ques-tions and concerns, some-one to confide in.
Last year, after I trans-ferred to Radiation On-cology, I received a callfrom a nurse in Pedi-atrics informing me thatGreg had experiencedanother relapse, whichrequired a right-sidedoccipital craniotomy. Hewas at Spaulding Rehab-ilitation Hospital forextensive rehabilitationand was scheduled for acourse of radiation. WhenGreg arrived on our unitfor treatment, he had nostrength or control of hislower extremities; hewas unable to communi-cate; and it was not clearwhether he comprehend-ed or recognized his en-vironment. Despite hissevere physical condi-tion, he was in a wheel-
chair with his mother byhis side.
Ann greeted me with,“I’m so glad you’re here.”She was upset and pro-ceeded to tell me she’dbeen informed that Gregwould have to come forhis treatments on a stret-cher. She had been toldit would make Greg’stransfer to the treatmenttable easier, and thatGreg’s safety was also aconcern.
I knew immediatelywhat this meant to Ann:a loss of normalcy andindependence, a rever-sal. She knew that Greghad a sense of aware-ness and she wanted topreserve his sense ofindependence and dig-nity. I needed to commu-nicate Greg’s history andAnn’s feelings and con-cerns to the therapistswho would be treatinghim.
A team meeting withall Greg’s caregiverswould be important inensuring continuity anda consistent plan of care.
story continues withexemplar on next page
Compassion, continuityand collaboration drive care for
radiation oncology patient
Radiation therapist, Gidget Manning, RTT, preparespatient, Alyssa Karakos, for stereotactic radiotherapy treatment
in the Radiation Oncology Unit on the Cox lower level.

Page 7
October 3, 2002October 3, 2002
y name isKaren Reedand I am a
senior radia-tion therapist in the de-partment of RadiationOncology. I have beenemployed at MGH forfour years and have work-ed in various radiationoncology departmentsthroughout the UnitedStates and New Zealandfor more than 12 years.
I am Gidget Man-ning, senior radiationtherapist and MGH em-ployee for more than 11years. Together, we arepart of the StereotacticRadiotherapy and Radio-surgery team in the de-partment of RadiationOncology.
Greg was scheduledto begin stereotactic ra-diotherapy for his pinealtumor recurrence. InGreg’s case, stereotacticradiotherapy was thetreatment of choice be-cause it would optimallyminimize the dose to theareas that had been pre-viously treated, whilegiving a high dose to the
area now involved.Stereotactic radio-
therapy is a 3-dimen-sional radiation therapyused to treat various be-nign and malignant braintumors using multiple,small, highly conformalbeams of high-energyx-rays. The goal of ra-diation therapy is to deli-ver therapeutic doses ofradiation to the target,while minimizing thedose to surrounding tis-sues. Stereotactic radio-therapy is ideal for smallintracranial lesions, be-nign auditory lesions,and orbital tumors inboth adult and pediatricpatients.
During the team meet-ing prior to Greg’s firsttreatment, we discussedthe emotional impactthat this type of recur-rence can have on thepatient and family, andthe issues related to achild who had been treat-ed many years ago andpresents with disease inlater life. Although Greg’sfamily, in particular hismother, Ann, were verysupportive and involved
in his care, we felt theneed to support them allthe more in this difficulttime. During the meet-ing, we, the radiationtherapists, expressed ourconcerns about Greg’scandidacy for stereo-tactic radiotherapy. Thetreatment involves theuse of a customized headframe, placed daily for4-6 weeks. Given Greg’spoor physical conditionafter surgery, and hislack of mobility and re-sponse, we didn’t feel hewas an ideal candidatefor this complex treat-ment regimen.
We also had concernsabout Greg’s safety andthe safety of those in-volved in his care. It wasimportant to Greg tocome to his daily treat-ments in a wheelchair;important for his inde-pendence and maintain-ing his sense of self.Could we safely transferhim to the treatmenttable each day when hehad very little use of hislegs? It was decided thatgiven Greg’s history oftreatment and recentdisease progression, thiswould be the best optionfor him at this time.
Transferring Gregfrom the wheelchair tothe treatment table re-quired the help of at least
five people. Nurses, ther-apists and residents allpitched in to ensure asafe transfer and properpositioning of his bodyon the table.
With the help of hismother, we began Greg’streatment and learned ina very short time what anamazing family this was.Their strong desire totake their son home andresume normalcy in theirlives was a driving forcein his recovery. Our res-ervations about thistreatment regimen forGreg diminished quicklyas his physical limita-tions and challengesdecreased.
The 18-year-oldyoung man who hadcome into our depart-ment in a near-lethargicstate was now walking,talking, even dancing!We grew to love him, hisremarkable family, andhis wonderful personal-ity, which was emergingmore and more each day.
Radiation Oncologysees more than 200 pa-tients each day. The paceis often hurried, if notsome days frantic, yetover a 4-6 week periodwe get to know our pa-tients on a personal level.In a department that wit-nesses so much grief andsadness, people often ask
Karen Reed, RTT, and Gidget Manning, RTT,senior radiation therapists
if we find our job de-pressing. With the ad-vances in technology andcancer care, Greg’s storyis just one of many hap-py endings we see. Weare thrilled with the out-come, and the team effortthat made it possible.
Comments byJeanette IvesErickson, RN, MS,senior vice presidentfor Patient Care andchief nurse
These narratives, whichso beautifully comple-ment each other, are anextension of the team-work and collaborationthat made this patient’sstory such a success. Itwasn’t just ‘knowing’Greg that led to this pos-itive outcome. It wascaring for and abouthim, understanding hisneeds even when he wasunable to voice them,and respecting this fam-ily’s desire to supporttheir son in a way thatpreserved his dignity andindependence. This storyis about risk-taking,strong patient advocacy,and a willingness tolearn and grow as clini-cians. This is a wonder-ful example of teamworkand commitment.
Thank-you, Sheila,Karen, and Gidget.
M
“Complementary andalternative medicine”
Program will look at acupuncture,meditation, and therapeutic touch.Case studies will help demonstrate
the impact of complementaryhealing modalities.
November 22, 20028:00am–4:00pm
O’Keeffe AuditoriumFor more information, call 6-3111
“Depression: What YouShould Know”
Presented by John B. Herman, MD
This seminar will provide information onthe signs, symptoms and treatment of
depression.
October 11, 200212:30–1:30pm
Wellman Conference RoomFor more information, call 726-6976.

Page 8
October 3, 2002October 3, 2002
eable about all of theseelements.
The radiation thera-pist’s role is truly anextension of the radia-tion oncologist. Radia-tion therapists operatethe linear accelerators toprecisely deliver the pre-scribed radiation doseaccording to the oncolo-gist’s treatment plan. Thetherapist also participatesin the ‘simulation’ orplanning procedure, gen-erating x-rays of the treat-ment ‘fields.’ Contemp-orary radiation therapy isendlessly challenging as
we add sophisticatednew treatment techniquesto our program whileparticipating in complexmulti-disciplinary pro-tocols. Working in teamsthat change semi-annual-ly, radiation therapistsdeliver most, if not all,treatments to any givenpatient. This continuityof care enables us tobuild trust and meaning-ful relationships with ourpatients.
No individual takeslightly the need for high-energy radiation to bedirected at his or herbody. It is critical thattherapists earn the con-fidence of their patientsand work to preserve thattrust for the duration of
the program. Radiationtherapists are licensedpractitioners, with eitheran associate’s or bacca-laureate degree. Specialareas of study includeradiation physics andbiology, radiation safety,computer-aided bio-physics, and medicalimaging. MGH is thesingle clinical educationsite for student therapistsenrolled in the BS degreeprogram in RadiationTherapy Technology atSuffolk University.
How nurses and ther-apists interact has directbearing on the care thatpatients receive. We usea primary-practice modelfor both nursing and
Cover StorCover StorCover StorCover StorCover Storyyyyycontinued from page 5
treatment delivery toensure consistency andcontinuity of care. Witha high level of collabor-ation and sharing of in-formation, nurses andtherapists coordinatetreatments and identifythe resources needed byeach patient. Therapistsproviding daily care areable to recognize physi-cal and emotional changesand communicate themto the nurse. Because acourse of radiation canbe lengthy, we get toknow patients and fam-ilies over a long periodof time. Providing phy-sical care as well as emo-tional support is an inte-gral part of our practice.Developing relationships
through the course oftreatment enables us tobetter evaluate and re-spond to individual needs.
In addition to thespecialized skills andservices provided bynurses and therapists inRadiation Oncology,there’s no way to ade-quately describe the hu-man factor that is pro-vided in the form of on-going support, compas-sion, understanding,communication, and justbeing present to our pa-tients. We are privilegedto share intimate andemotional moments withour patients and theirfamilies.
RecognitionRecognitionNERBNA celebrates 30th
anniversary; Ives Erickson receivesPresident’s Award
elebrating its30th anniver-sary as an organ-
ization and threedecades of service to thecommunity, The NewEngland Regional BlackNurses Association(NERBNA) held its an-nual meeting and lunch-eon at the Quincy Mar-riott, Sunday, September22, 2002. It was a day offestivities, good food,and friendship as blacknurses from all over NewEngland came togetherto celebrate this mile-stone occasion.
Keynote speaker andpast NERBNA presi-dent, Dr. Marcia I. Wells,spoke about the greatstrides made by nurses ofcolor in the past 30 years.
C She spoke of the impor-tance of having a vision,thinking outside the box,and in fact, getting to aplace where ‘there is nobox’ because boxes arelimiting. Advocacy, act-ivism and empowerment,said Wells, are the keysto continued advance-ment.
Ron Greene, RN,MGH case manager andpresident of NERBNA,recognized several in-dividuals with specialawards. Among them,Jeanette Ives Erickson,RN, senior vice presi-dent for Patient Care,was honored forher outstandingleadership andcommitment todiversity.
Said Greene, “Jean-ette has been recognizedas a nursing leader lo-cally and nationally; she
has worked hard to givenurses the professionalrespect they so rightlydeserve. When it comesto diversity, Jeanettedoes more than talk thetalk; she walks the walk.Due largely to her ef-forts, MGH is becominga more diverse hospital,
and under her leader-ship, the department ofNursing is leading theway for change.”
Ives Erickson wasunable to attend theevent. Associate chiefnurse, Theresa Gallivan,RN, accepted the awardon her behalf.
Associate chief nurse, Theresa Gallivan, RN,accepts award for Ives Erickson as NERBNA
president, Ron Greene, RN, looks on.
Page 9
October 3, 2002October 3, 2002
Published by:Caring Headlines is published twice eachmonth by the department of Patient Care
Services at Massachusetts General Hospital.
PublisherJeanette Ives Erickson RN, MS,
senior vice president for Patient Careand chief nurse
Managing Editor/WriterSusan Sabia
Editorial Advisory BoardChaplaincy
Mary Martha Thiel
Development & Public Affairs LiaisonGeorgia Peirce
Editorial SupportMarianne Ditomassi, RN, MSN, MBAMary Ellin Smith, RN, MS
Materials ManagementEdward Raeke
Nutrition & Food ServicesPatrick BaldassaroMartha Lynch, MS, RD, CNSD
Office of Patient AdvocacySally Millar, RN, MBA
Orthotics & ProstheticsEileen Mullen
Patient Care Services, DiversityDeborah Washington, RN, MSN
Physical TherapyOccupational Therapy
Michael G. Sullivan, PT, MBA
Police & SecurityJoe Crowley
Reading Language DisordersCarolyn Horn, MEd
Respiratory CareEd Burns, RRT
Social ServicesEllen Forman, LICSW
Speech-Language PathologyCarmen Vega-Barachowitz, MS, SLP
Volunteer, Medical Interpreter, Ambassadorand LVC Retail Services
Pat Rowell
DistributionPlease contact Ursula Hoehl at 726-9057 for
all issues related to distribution
Submission of ArticlesWritten contributions should be
submitted directly to Susan Sabiaas far in advance as possible.
Caring Headlines cannot guarantee theinclusion of any article.
Articles/ideas may be submittedby telephone: 617.724.1746
by fax: 617.726.8594or by e-mail: [email protected]
Please recycle
Next Publication Date:October 17, 2002
continued on next page
Patient SafetyPatient Safety
ur mission is to pro-vide the highest qualitypatient care in an envi-ronment that is safe
for all patients, families,visitors and employees. MGH iscommitted to maintaining therights, dignity and well-being ofall patients, which includes ahigh-quality Patient ObserverProgram.
This column, provided bythe Office of Quality & Safety,highlights some frequently ask-ed question about our PatientObserver Program.
Question: What is the MGHPatient Observation Program?Answer: When a patient is de-termined to be at risk for injury,appropriate nursing strategiesare implemented to ensure pa-tient safety. When these strate-
Patient observers:frequently asked questions
Ogies are ineffective and thepatient remains at risk, obser-vation of the patient may be anoption. Nurses, in consultationwith unit leadership, identifythe need for, and determine thelevel of, observation necessaryfor each individual patient.
Question: If an observer sees apatient getting out of bed, canhe or she physically help re-direct the patient to stay inbed?Answer: If a patient is gettingout of bed, a Bulfinch Tempo-rary observer should call forassistance. Patient care associ-ates acting in the role of patientobservers, are allowed to per-form these duties within thescope of their job responsibili-ties, and would be able to re-direct the patient back to bed.
Question: What do patient ob-servers document on the Patientat Risk for Injury flowsheets?Answer: Observers documentpatients’ actions every 15 min-utes. This documentation em-phasizes the dynamic nature ofthe observer role. It is used bystaff nurses along with theirown assessments to determinewhether or not there is a needfor ongoing observation.
Question: Is using the observerworksheet optional?Answer: In order to maintainconsistency and appropriatelysupport Bulfinch Temporaryobservers and patient care asso-ciates who have been trained inthese procedures, it is importantto use the observer worksheetsthe way they were designed tobe used. The observer work-sheets are used for all patientsfor whom observation is deem-ed necessary, and are maintain-ed with the nursing assignmentsheets on the unit.
The Employee AssistanceProgram
presents
National DepressionScreening Day
The Employee Assistance Program (EAP)is participating in a nationwide programto provide information about the signs,
symptoms, and treatment of depression.As part of the effort to heighten awareness
about depression in the workplace,the EAP will offer free, anonymous,
confidential screenings to all employees.Employees may walk in for a 15-minute,
self-administered test. Mental healthprofessionals will be on hand
to review and discuss the tests.Employees will have an opportunity
to speak confidentially about concerns theymay have about friends and family.
October 10, 2002MGH employees: 9:00am–4:00pm
VBK427
General public: 9:00am–1:00pm4th floor, 50 Staniford St.
For more information, call 726-6976.
MGH celebrates Case Management WeekOctober 7–11, 2002
Educational Booth in the Main CorridorTuesday, October 8th and Thursday, October 10th
1st Annual Case Management Change ShowOur very own Saturday Night Live!
Wednesday, October 9th2:00–3:30pm
O’Keeffe Auditorium
Nursing Grand Rounds: “Case Management”Thursday, October 10th
1:30-2:30pmO’Keeffe Auditorium
Case Management Presentation:“Dealing with the Changing Healthcare Times:
It’s Time to Break the Rules”presented by Louis Feuer, MA, MSW,
nationally rcognized lecturer, author, and healthcaremanagement consultant; leading customer service
expert in the healthcare industry.Tuesday, October 15th
10:00–11:00amO’Keeffe Auditorium.
(CEUs pending)
For more information, call Leah Wolf 4-8561or Ron Greene at 4-8252.
Page 10
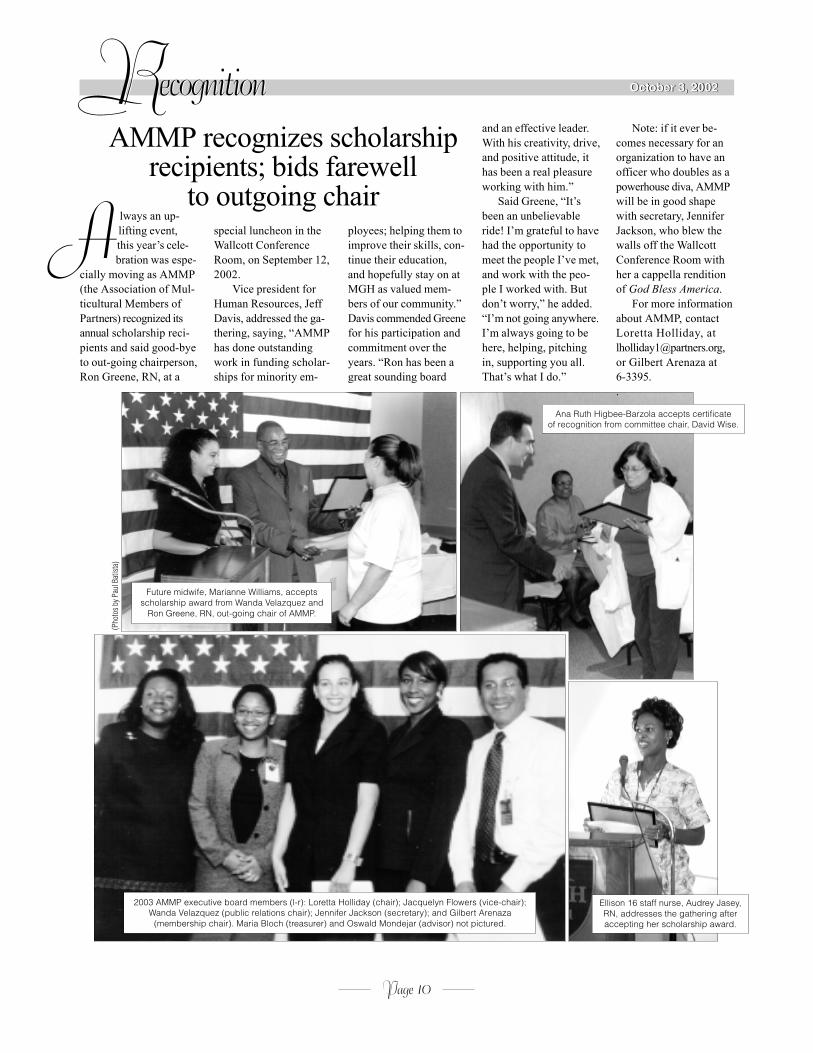
October 3, 2002October 3, 2002RecognitionRecognitionAMMP recognizes scholarship
recipients; bids farewellto outgoing chair
2003 AMMP executive board members (l-r): Loretta Holliday (chair); Jacquelyn Flowers (vice-chair);Wanda Velazquez (public relations chair); Jennifer Jackson (secretary); and Gilbert Arenaza
(membership chair). Maria Bloch (treasurer) and Oswald Mondejar (advisor) not pictured.
Future midwife, Marianne Williams, acceptsscholarship award from Wanda Velazquez and
Ron Greene, RN, out-going chair of AMMP.
Ana Ruth Higbee-Barzola accepts certificateof recognition from committee chair, David Wise.
Ellison 16 staff nurse, Audrey Jasey,RN, addresses the gathering afteraccepting her scholarship award.
(Pho
tos b
y Pau
l Bat
ista
)
lways an up-lifting event,this year’s cele-bration was espe-
cially moving as AMMP(the Association of Mul-ticultural Members ofPartners) recognized itsannual scholarship reci-pients and said good-byeto out-going chairperson,Ron Greene, RN, at a
A special luncheon in theWallcott ConferenceRoom, on September 12,2002.
Vice president forHuman Resources, JeffDavis, addressed the ga-thering, saying, “AMMPhas done outstandingwork in funding scholar-ships for minority em-
ployees; helping them toimprove their skills, con-tinue their education,and hopefully stay on atMGH as valued mem-bers of our community.”Davis commended Greenefor his participation andcommitment over theyears. “Ron has been agreat sounding board
and an effective leader.With his creativity, drive,and positive attitude, ithas been a real pleasureworking with him.”
Said Greene, “It’sbeen an unbelievableride! I’m grateful to havehad the opportunity tomeet the people I’ve met,and work with the peo-ple I worked with. Butdon’t worry,” he added.“I’m not going anywhere.I’m always going to behere, helping, pitchingin, supporting you all.That’s what I do.”
Note: if it ever be-comes necessary for anorganization to have anofficer who doubles as apowerhouse diva, AMMPwill be in good shapewith secretary, JenniferJackson, who blew thewalls off the WallcottConference Room withher a cappella renditionof God Bless America.
For more informationabout AMMP, contactLoretta Holliday, [email protected],or Gilbert Arenaza at6-3395..
2002
2002
October 3, 2002Educational OfferingsEducational Offerings
Page 11
October 3, 2002
For detailed information about educational offerings, visit our web calendar at http://pcs.mgh.harvard.edu. To register, call (617)726-3111.For information about Risk Management Foundation programs, check the Internet at http://www.hrm.harvard.edu.
DescriptionWhen/Where Contact Hours
Managing Patients with Psychiatric Illness in the General-Care SettingO’Keeffe Auditorium
TBAOctober 118:00am–4:00pm
CPR—Age-Specific Mannequin Demonstration of BLS SkillsVBK 401 (No BLS card given)
- - -October 158:00am–12:00pm (Adult)10:00am–2:00pm (Pediatric)
CPR—American Heart Association BLS Re-Certificationfor Healthcare ProvidersVBK 401
- - -October 167:30–11:30am,12:00–4:00pm
USA Educational SeriesBigelow 4 Amphitheater
- - -October 161:30–2:30pm
Social Services Grand Rounds“The Mind-Body Connection: Learning and Leading Relaxation Exercises.”O’Keeffe Auditorium. For more information, call 617-726-8673.
CEUsfor social workers only
October 1710:00–11:30am
Nursing Grand RoundsO’Keeffe Auditorium
1.2October 171:30–2:30pm
Pediatric Trauma–Part VIWellman Conference Room
---October 217:30–11:30am, and 12:30–4:30pm
CPR—American Heart Association BLS Re-Certificationfor Healthcare ProvidersVBK 401
- - -October 237:30–11:30am,12:00–4:00pm
New Graduate Nurse Development Seminar IITraining Department, Charles River Plaza
5.4 (contact hoursfor mentors only)
October 238:00am–2:30pm
Intra-Aortic Balloon Pump WorkshopDay 1: Wellman Conference Room. Day 2: VBK607
14.4for completing both days
Oct. 28: 7:30am–4:30pmOct. 29: 7:30am–4:30pm
Preceptor Development Program: Level IITraining Department, Charles River Plaza
7.8October 308:00am–4:30pm
Intermediate ArrhythmiasHaber Conference Room
3.9October 318:00–11:30am
Pacing : Advanced ConceptsHaber Conference Room
5.1October 3112:15–4:30pm
CPR—Age-Specific Mannequin Demonstration of BLS SkillsVBK 401 (No BLS card given)
- - -November 18:00am–12:00pm (Adult)10:00am–2:00pm (Pediatric)
November 18:00am–4:30pm
Care of the Person with Cancer: Back to BasicsO’Keeffe Auditorium
TBA
16.8for completing both days
Advanced Cardiac Life Support (ACLS)—Provider CourseDay 1: O’Keeffe Auditorium. Day 2: Wellman Conference Room
November 4 and November 158:00am–5:00pm
---Deb Wing Memorial LectureHaber Conference Room
November 64:00–6:00pm
CPR—American Heart Association BLS Re-Certificationfor Healthcare ProvidersVBK 401
- - -November 77:30–11:30am,12:00–4:00pm
Diversity Considerations in Responding to Domestic ViolenceWalcott Conference Room
---October 312:00–1:00pm
The African American Community Responds to Domestic ViolenceWellman Conference Room
---October 1012:00–1:00pm

Page 12
October 3, 2002October 3, 2002
CaringGRB015
MGH55 Fruit Street
Boston, MA 02114-2696
CaringH E A D L I N E S
First ClassUS Postage PaidPermit #57416
Boston MA
Interpreter ServicesInterpreter Services
Seated (l-r): Lulu Sanchez, manager,Interpreter Services; and staff interpreters,Dennis Trujillo, and Katia Canenguez, field
questions from visitors at the InterpeterServices educational booth.
MGH celebratesInterpreter Services Week
MGH interpreters were out in force, September 16–20,2002, staffing an educational booth in the Main Corridor,disseminating information and answering questions forstaff, patients and visitors. Medical interpreters provide animportant service at MGH, ensuring that patients from allbackgrounds and cultures can communicate effectivelywith their healthcare providers.
The Interpreter Services office is located in ClinicsRoom 141; they are open from 7:00am–12:00am Mondaythrough Friday, and 10:00am–10:00pm on weekends. Formore information, call 726-6966.