cardiovascular system biomedicine review felix hernandez, m.d
TRANSCRIPT

Cardiovascular System
Biomedicine Review
Felix Hernandez, M.D.
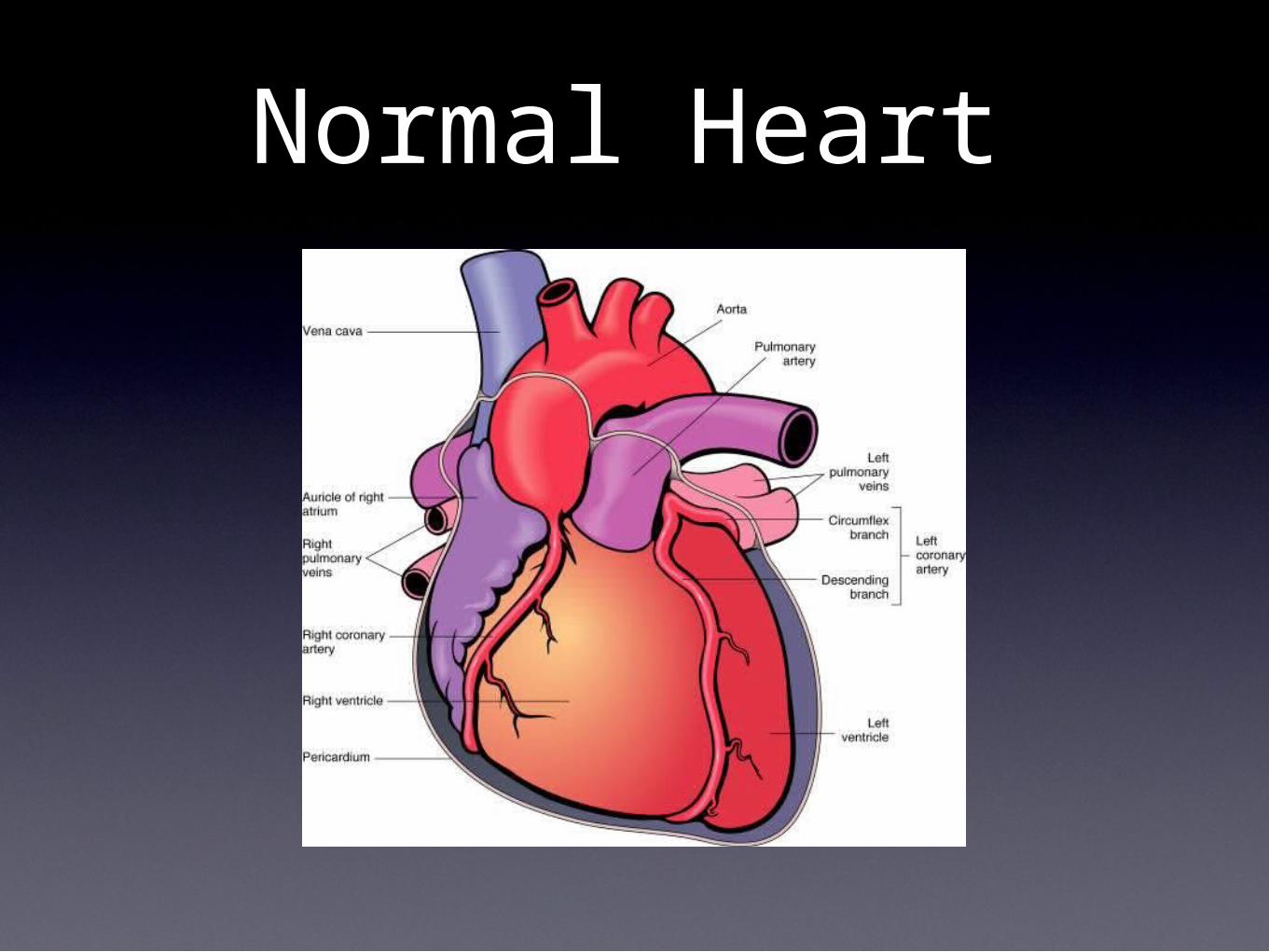
Normal Heart
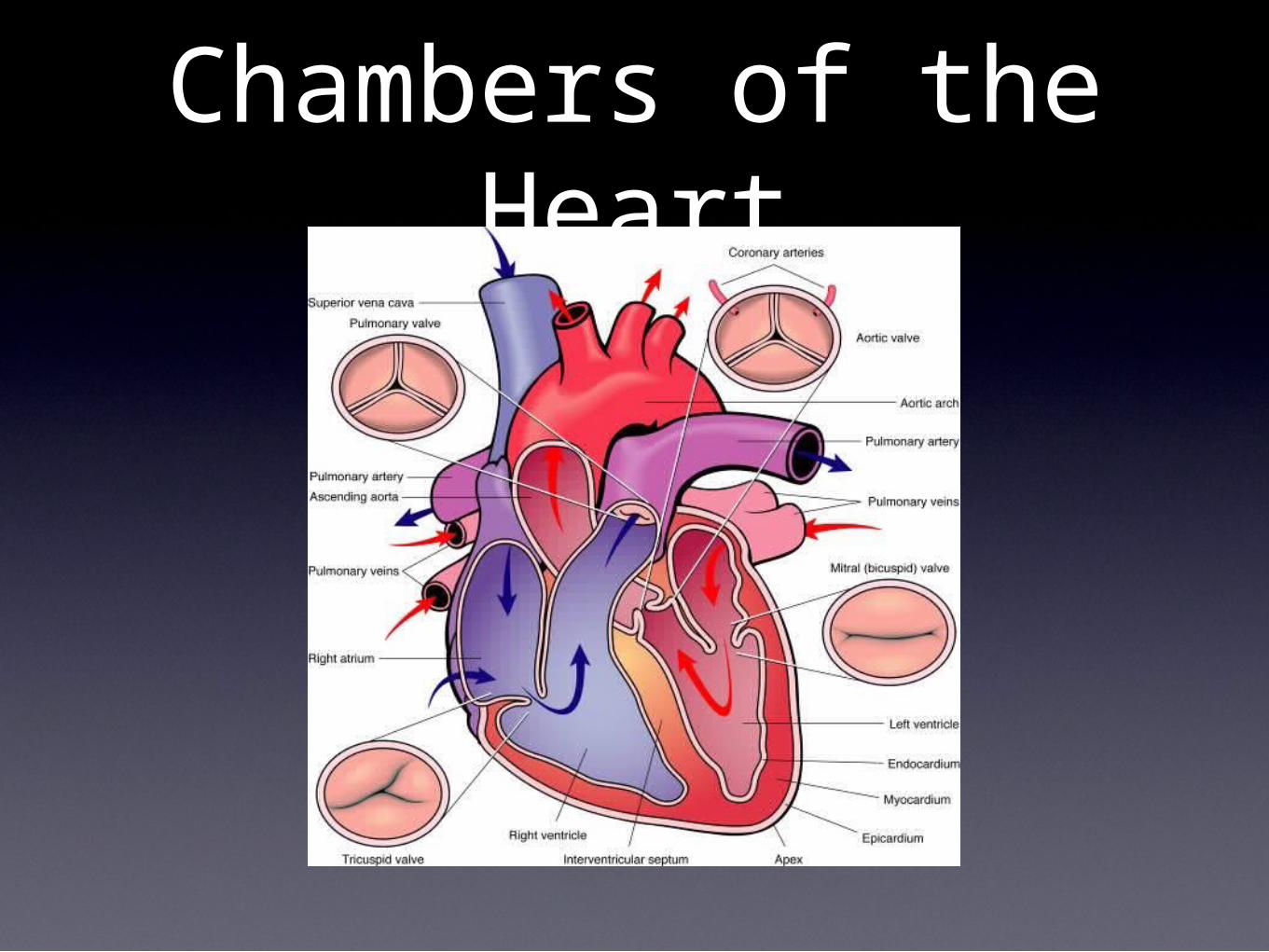
Chambers of the Heart
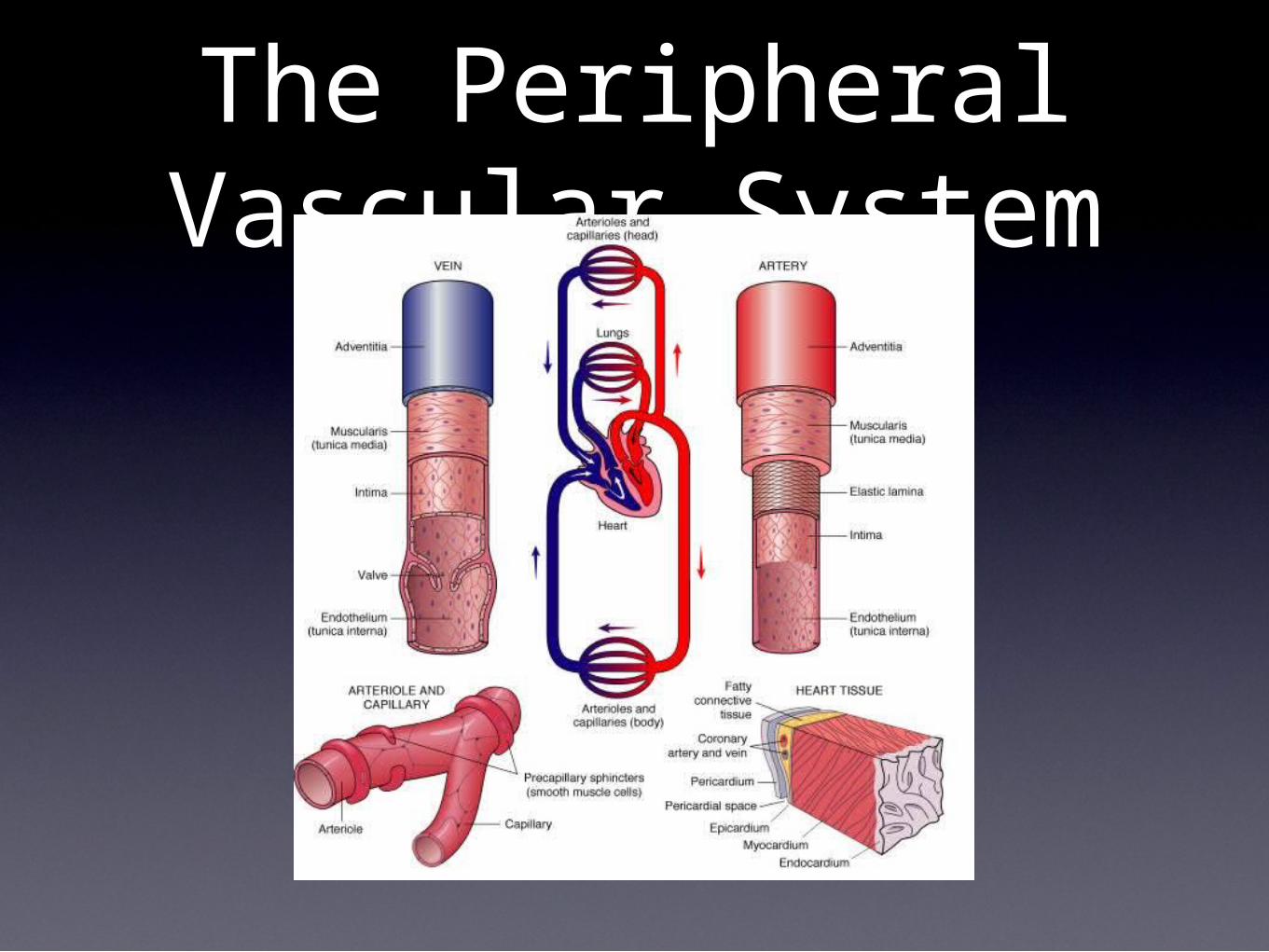
The Peripheral Vascular System

Blood Pressure•Blood pressure is regulated by cardiac
output and peripheral vascular resistance
•Systolic Blood Pressure
•the blood pressure measured during the period of ventricular contraction
•In a blood pressure reading, it is the higher of the two measurements.
•Diastolic Blood Pressure
•the minimum level of blood pressure measured between contractions of the heart.
•Can vary with age, gender, weight and emotional state.
Hypertension•Primary Hypertension
•elevated blood pressure without a known causative factor
•this is the most common type
•causes:
•genetic predisposition and obesity
•stress, increased alcohol intake
•diabetes, sodium and water retention
•Secondary Hypertension
•elevated blood pressure with an identifiable cause
•Causes:
•renal artery stenosis, congenital heart defects, cushing’s syndrome, sleep apnea, pregnancy, stimulants
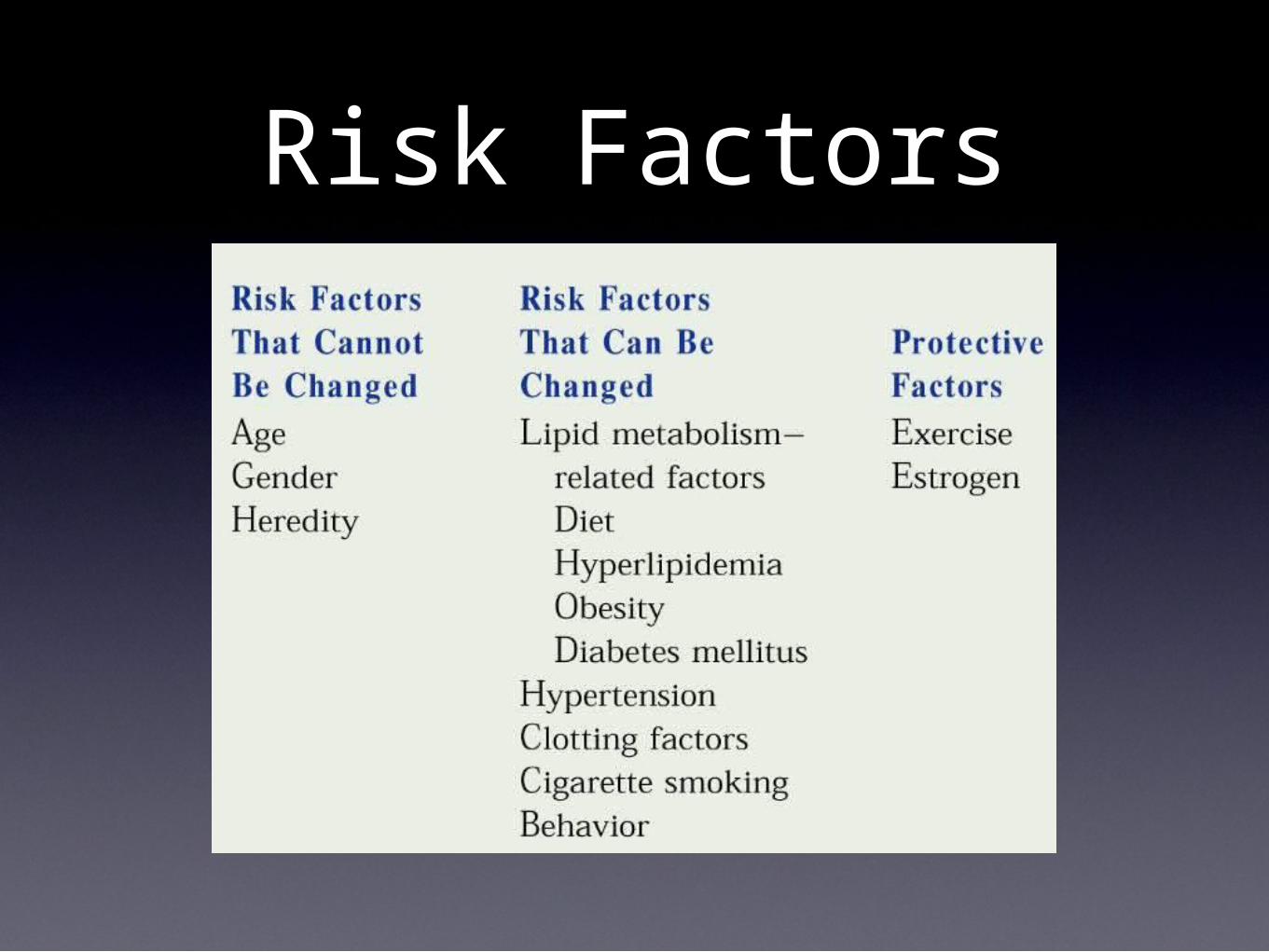
Risk Factors

Hypertension
•Signs and Symptoms
•no initial symptoms usually occur
•chronic fatigue
•headache
•dizziness
•dyspnea
•chest pain and palpitations

Treatment• ABC
• A: ACE Inhibitor
• Enalapril (Vasotec), Lisinopril (Zestril)
• block the conversion of angiotensin I to angiotensin II which would normaly act as a vasoconstrictor
• this blocking causes vasodilation which will cause a decrease in resistance and a decrease in BP
• B: Beta Blocker
• Action: blocks the beta adrenergic receptors of the sympathetic nervous system which results in vasodilation and a decrease in the release of renin
• Contraindications: Pregnancy and Lactation
• Cautions: asthma, diabetes
• Side Effects: Hypotension, bradycardia, wheezing, dyspnea
• C: Calcium Chanel Blocker
• Amlodipine (Norvasc), Diltiazem (Cardizem), Nifedipine (Procardia)
• block calcium influx into the beta receptors which causes a decrease in the force of contraction and reduces the heart rate

Specific Side Effects of Beta Blockers
•Propranolol (Inderal)
•bradycardia, CHF, impotence
•Atenolol (Tenormin)
•dizziness, fatigue, cold extremities, depression, impotence
•Timolol (Blocarden)
•fatigue, bradycardia, extremity pain, impotence
•Metoprolol (Lopressor)
•fatigue, dizziness, depression, confusion, short term memory loss, headache, impotence
Treatment•Diuretics
•Loop Diuretics
•Furosemide (Lasix)
•inhibit the reabsorption of sodium and chloride in the ascending loop of Henle
•Thiazide Diuretics
•Hydrochlorothiazide
•inhibit sodium and chloride reabsorption in the the distal tubules
•Used to treat hypertension and edema
•Contraindications: hypersensitivity to sulfonamides, anuria, oliguria, fluid and electrolyte depletion
•Side Effects: tiredness, weakness, dizziness, orthostatic hypotension, tinnitus
Treatment
•Potassium Sparring Diuretic
•Spironolactone (Aldactone)
•MOA: Antagonist of Aldosterone
•Side Effects: Hyperkalemia, glucose intolerance in DM patients
Unstable Angina
•an anginal attack occurring at rest or increasing in frequency
•caused by blockage of the coronary arteries
•has a high risk of subsequent myocardial infarction
•Labs: is evaluated with EKG. First you do a resting EKG, if that comes back normal then you perform an exercise stress test.
Treatment•Nitroglycerin
•Uses: Relief of anginal pain and to suppress tachycardia
•MOA: relaxes vasculature (both arteries and veins but mostly veins) causing a decreased in preload and afterload
•Contraindications: hypersensitivity, severe anemia, head trauma or cerebral hemorrhage
•Side Effects: orthostatic hypotension, dry mouth, blurred vision, tachycardia, headache
Myocardial Infarction
•Is the leading cause of death
•caused by an obstruction of a coronary artery
•S/S: chest pain that lasts for more than 30 minutes and radiates to the left arm. The pain is not relieved by nitroglycerin
•Labs: Increased Troponin and CK-MB
•EKG Changes: T-wave inversion, ST elevation, Q-wave formation
•Treatment: Oxygen, aspirin, morphine, beta-blocker, ARB
Ventricular Fibrillation
•Dangerous electrical dysfunction
•Commonly associated with MI, CHF and shock
•EKG: rapid, chaotic, and distorted
•S/S: cheat pain, SOB, sudden death
•Tx: Direct Current Cardioversion
Ventricular Flutter
•Heart rate of 150-350 BPM
•Associated with hypoxia or ischemic insults
•S/S: hypotension and sudden death
•EKG: loss of normal QRS morphology
•Tx: defibrillation
Atrial Fibrillation•Uncoordinated rapid contractions
of the atria
•S/S: dizziness, papitations, irregularly irregular pulse
•associated with the development of thrombi that can embolize
•Tx: Warfarin (Coumadin), anti-arrhythmics
Renal Artery Stenosis
•Caused by fibromuscular dysplasia in young women and atherosclerosis in older men
•S/S: HTN, audible abdominal bruit, high renin levels
•Tx: ACE, angioplasty
Hypothermia
•A decrease in body temperature
•S/S: decreased peripheral perfusion, decreased respiratory rate, decreased bowel sounds, decreased DTR
•Can also cause arrhythmia, bradycardia and hypotension
Deep Vein Thrombosis
•Development of a blood clot in the deep veins of the lower extremity
•Associated with cancer, estrogen therapy, and prolonged immobility
•Virchow’s Triad: hypercoagulability, venostasis, endothelial injury
•S/S: Homan’s Sign --> pain on foot dorsiflexion
•Tx: Heparin (works faster so it is used initially) and Warfarin (Coumadin)
•Prothrombin Time (PT) is used to measure the effects of Warfarin
Cholesterol• Total Cholesterol
• desired levels is <200
• >240 is considered high risk
• HDL
• desired level is >60
• considered protective against heart disease
• levels are increase by: vigorous exercise, insulin, estrogens
• levels are decreased by starvation, obesity, hypothyroidism, smoking, DM and liver disease
• LDL
• desired level <100
• >190 gives you the highest increased risk of heart disease
• Levels are increased by atherosclerosis, CHD
• Levels are decreased by depression, anxiety

Cholesterol Lowering Drugs
•Cholestyramine
•MOA: forms insoluble complexes with bile salts allowing them to be excreted in feces. The body compensates by increasing the number of LDL receptors and oxidizing cholesterol to bile acids
•Indications: LDL>190 or 160 with 2 risk factors
•Lipid Profile Effects:
•decreases TC, and LDL
•Increases Triglycerides, VLDL and HDL
Cholesterol Lowering Drugs•MOA: inhibit HMG-CoA reductase in the
liver which is the enzyme that catalyzes the rate limiting step in cholesterol synthesis.
•Profile Changes:
•Decreases TC, LDL, VLDL and Triglycerides
•Increases HDL
•Side Effects: Myalgia
•Drugs:
•Simvastatin (Zocor)
•Atorvastatin (Lipitor)
•Rosuvastatin (Crestor)
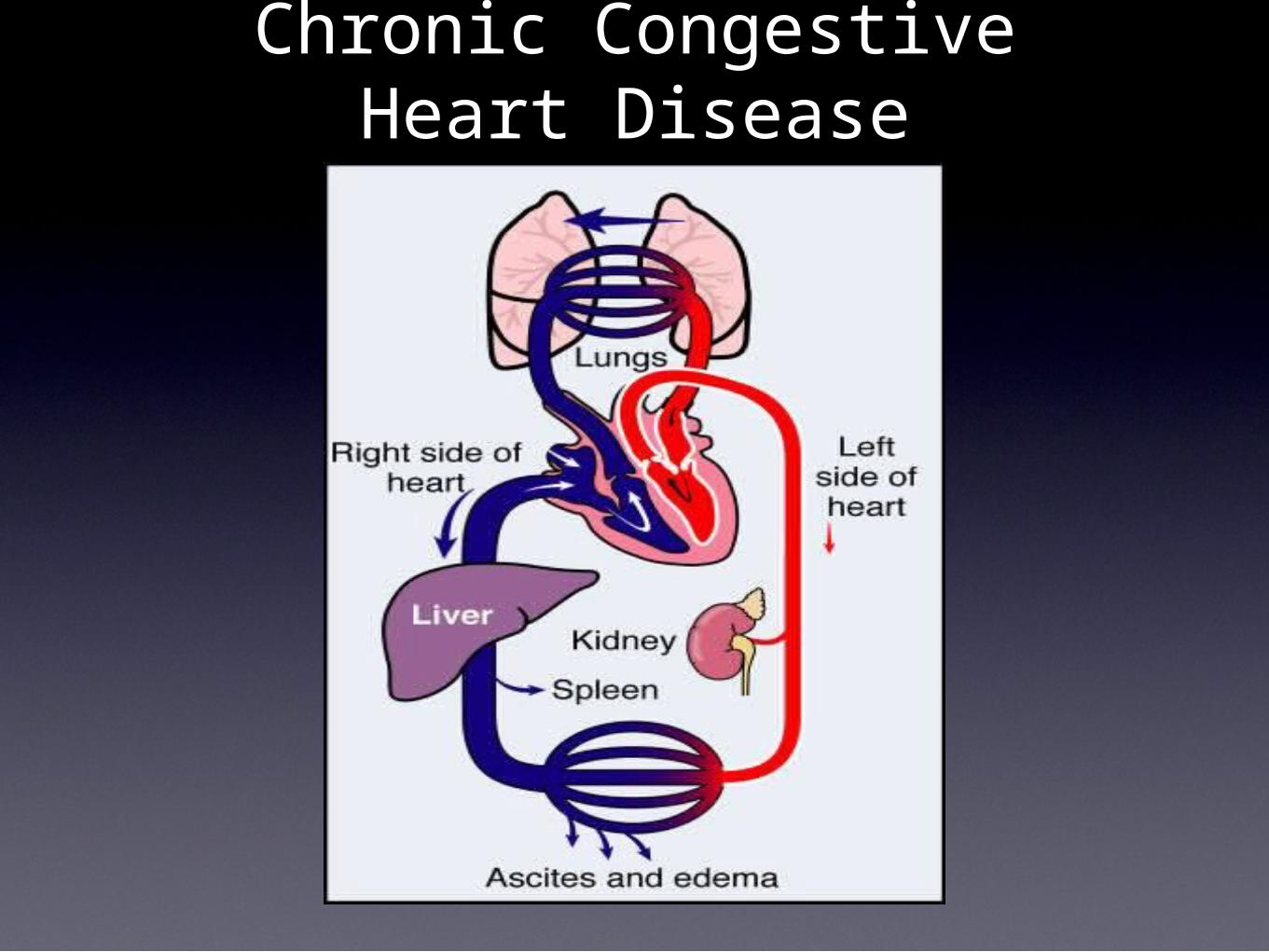
Chronic Congestive Heart Disease
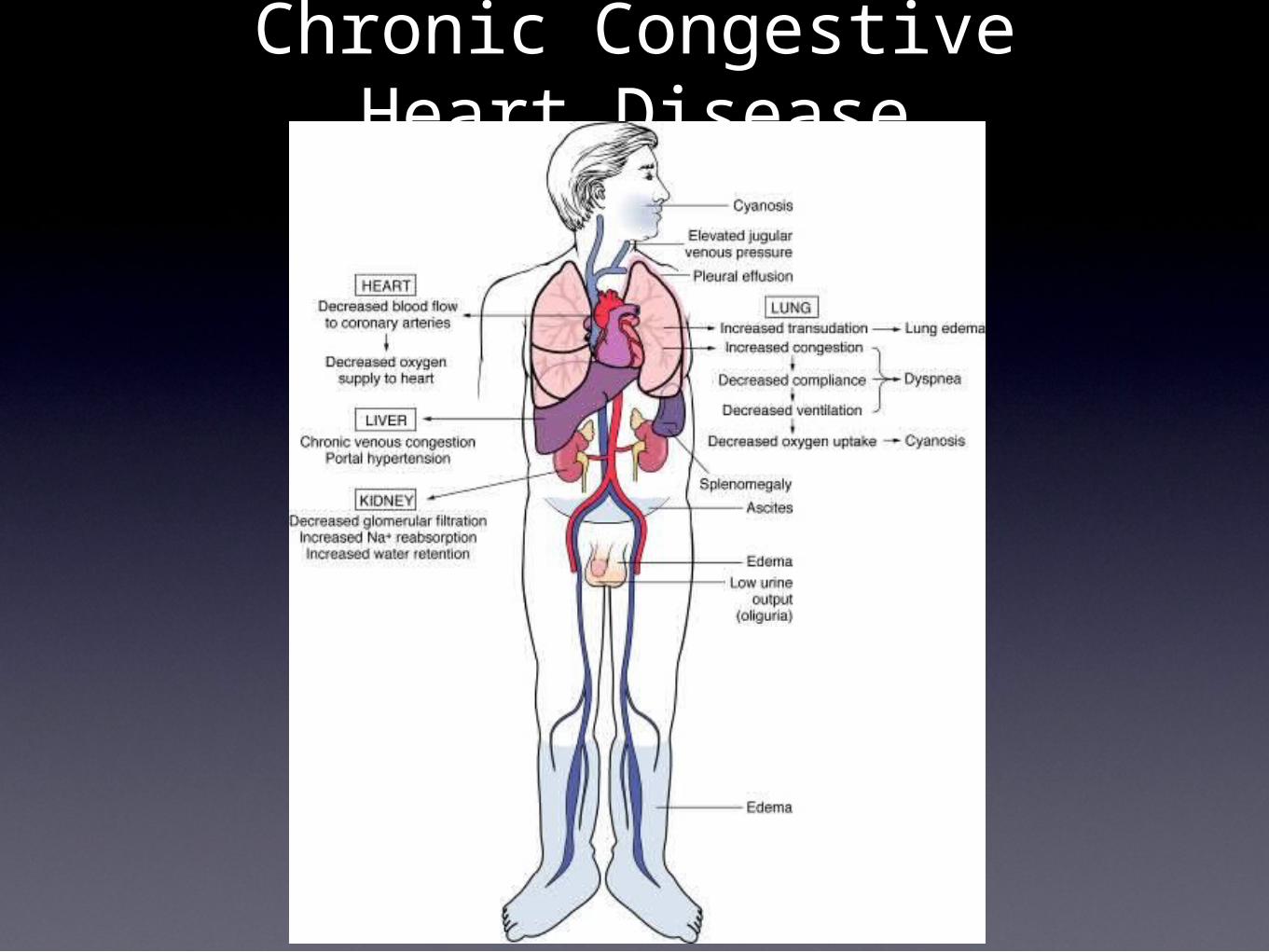
Chronic Congestive Heart Disease
Digitalis
•MOA: inhibits the Na-K ATPase which alters the mechanical and electrical actions of the heart and causes an increase in myocardial contractility
•Uses: Heart Failure (improves CO) and atrial fibrillation
•Contraindications: hypersensitivity, ventricular tachycardia
•Side Effects: dizziness, muscle weakness, visual disturbances, hypokalemia, bradycardia, arrhythmia

Cardiomyopathy•Dilated—viral infection, alcohol,
cardiotoxic drugs
•Ventricles are dilated and the myocardium is flabby and thinned
•Hypertrophic—genetic
•Thickening of LV myocardium
•Mutation in the genes that code for myocardium constrictive proteins
•Restrictive—amyloidosis, endomyocardial fibrosis
•Heart cant expand to receive inflowing blood
•Heart transplant is the only treatment
Leukocytes•Granulocytes
•Basophil: allergic and histamine reactions
•Eosinophil: parasitic infection, fungal infection
•Neutrophil: bacterial infection, inflammation, stress (Not Viral)
•Agranulocytes
•Lymphocyte: viral infection, chronic infection
•Monocyte: chronic infection
White Blood Cell Count
•Increased by:
•acute infection, neoplasm, leukemia
•Decreased by:
•bone marrow malfunction, immune deficiency, iron deficiency, AIDS, chemotherapy
Immunoglobulins
•IgG: most predominant, can cross the placenta and pass immunity to the fetus
•IgM: is the first to appear
•IgA: secretory antibody, is found in colostrum, secretions, saliva, tears
•IgE: least predominant, promotes histamine allergic reactions
•IgD: serves as a receptor on B-cells

Anemia• General Causes:
• chemo, GI bleed, rheumatoid arthritis, Lupus, AIDS, Cancer
• S/S: decreased hemoglobin, decreased hematocrit, changes in fingernail beds, pale skin, fatigue
• Specific Types:
• Aplastic anemia: caused by damage to the bone marrow from toxic chemicals or radiation
• Hemolytic Anemia: destruction of red blood cells by toxic chemicals or antibodies
• Iron Deficiency Anemia: caused by a dietary lack of iron which leads to deficient hemoglobin synthesis
• Pernicious Anemia: caused by an inability to absorb B12 which leads to immature RBCs
• Sickle Cell Disease: caused by a defective gene leading to sickle shaped RBCs
• Thalassemia: caused by a defective gene which causes the formation of abnormal hemoglobin and a shortened lifespan of RBCs

Blood Labs• Red Blood Cell Count (RBC)
• increased in: polycythemia, renal disease, pulmonary disease
• decreased in: anemia, Hodgkin’s leukemia, sickle cell disease
•Hemoglobin and Hematocrit
• Increased by: dehydration, shock, COPD, CHF, polycythemia
•Decreased by: anemia, leukemia, hyperthyroidism, cirrhosis, massive trauma
• Iron
• Increased by: acute hepatitis, nephrosis
•Decreased by: anemia, lupus, RA, hypothyroidism, 3rd trimester of pregnancy
Aspirin• MOA: inhibits cyclooxygenase which is required for
prostaglandin synthesis.
• Decreases inflammation and pyrogen-induced fever
• Decreases pain caused by injury or inflammation
• Prevents platelet aggregation
• Indications: symptomatic relief of minor main, inflammation, fever or RA. Reduction of stroke risk.
• Side Effects: GI upset and bleeding, allergic reaction.
• Increased risk of Reye’s Syndrome in children
• Occurs when giving aspirin after an infection. Can cause brain, liver and kidney damage with possible death
• Overdose is called salicylism and involves tinnitus, dizziness, HA, fever, mental status changes, hyperventilation, and respiratory alkalosis which can lead to a metabolic acidosis
• Contraindications: bleeding disorders and peptic ulcer disease
Quiz Next Week
•25 questions
•20 Cardiovascular
•5 Musculoskeletal
•2 bone diagrams
•3 multiple choice on muscles (action, innervation, special notes)