cardiac tumors - society of thoracic radiology · left atrial myxoma pericadial biopsy was normal...
TRANSCRIPT
516
TU
ESD
AY
CARDIACTUMORS
Sharon Sudarshan Brouha, MD, MPHAssistant Clinical Professor
Cardiothoracic Imaging SectionCardiothoracic Imaging SectionUniversity of California San Diego
Imaging techniquesImaging techniques
Cardiac and pericardial massesCardiac and pericardial masses
Cardiac tumor mimicsCardiac tumor mimics
OverviewOverview
Prevalence of 0.002-0.3% at autopsy
75% are benign
Cli i l i ifiClinical significance�Cardiac physiologyp y gy�Embolism�Arrhythmias
Radiology: Volume 268: Number 1�July 2013
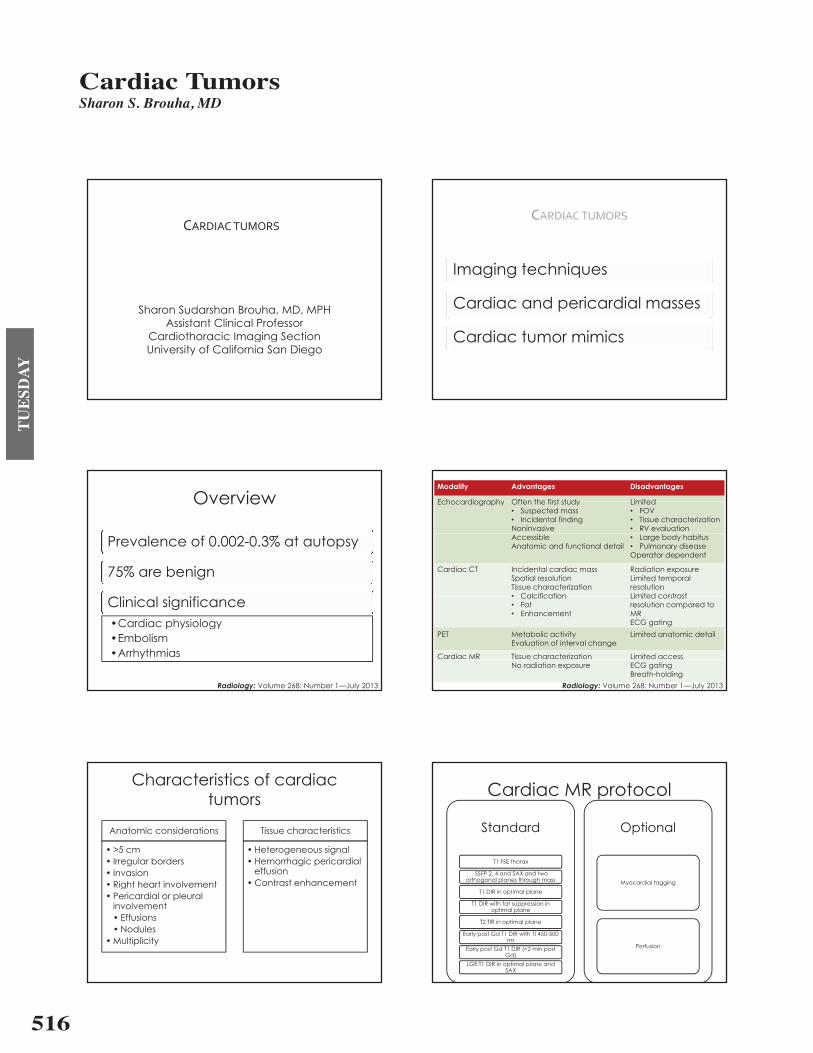
Modality Advantages Disadvantages
Echocardiography Often the first study LimitedEchocardiography Often the first study� Suspected mass� Incidental findingNoninvasive
Limited � FOV� Tissue characterization� RV evaluation
AccessibleAnatomic and functional detail
� Large body habitus� Pulmonary diseaseOperator dependent
Cardiac CT Incidental cardiac massSpatial resolutionTissue characterization� Calcification
Radiation exposureLimited temporal resolution Limited contrast� Calcification
� Fat� Enhancement
Limited contrast resolution compared to MRECG gating
PET Metabolic activityEvaluation of interval change
Limited anatomic detail
Cardiac MR Tissue characterization Limited access
Radiology: Volume 268: Number 1�July 2013
No radiation exposure ECG gatingBreath-holding
Characteristics of cardiac ttumors
Anatomic considerations
� >5 cm
Tissue characteristics
� Heterogeneous signal� Irregular borders� Invasion� Right heart involvement
� Hemorrhagic pericardial effusion
� Contrast enhancementg� Pericardial or pleural
involvement� EffusionsEffusions� Nodules
� Multiplicity
Cardiac MR protocolCardiac MR protocol
St d rd Opti lStandard Optional
T1 FSE thorax
SSFP 2, 4 and SAX and two orthogonal planes through mass Myocardial tagging
T1 DIR in optimal plane
T1 DIR with fat suppression in optimal plane
T2 TIR in optimal plane
Early post Gd T1 DIR with TI 450-500 ms
Early post Gd T1 DIR (<2 min post Perfusiony p ( pGd)
LGE T1 DIR in optimal plane and SAX
Cardiac Tumors Sharon S. Brouha, MD
517
TU
ESD
AY
Cardiac MR protocolCardiac MR protocol
T1 FSE thoraxT1 FSE thorax
Overview of the thoraxOverview of the thoraxIdentification of tumorBreath-hold or free breathing if necessaryg y
Cardiac MR protocolCardiac MR protocol
SSFP 2, 4 and SAXSSFP 2, 4 and SAX
Localization of massLocalization of massAnatomic detailMobility of massyFunctional significance
Cardiac MR protocolCardiac MR protocol
T1 weighted images pre and post contrastT1 weighted images pre and post contrast
Tissue characterizationTissue characterizationFat suppression for diagnosis of fatty elementsEarly Gd enhancementy� T1 of 450-500 ms post Gd renders thrombus low in signalLate Gd enhancement�Myocardial tumor infiltration with increased interstitial matrix or�Myocardial tumor infiltration with increased interstitial matrix or
scarring
Cardiac MR protocolCardiac MR protocol
T2 weighted imagesT2 weighted images
Tissue characterizationTissue characterizationEdema and liquefactive necrosis=high signalCoagulative necrosis=low signalg gHemorrhage or thrombus
Cardiac MR protocolCardiac MR protocol
Optional techniquesOptional techniques
TaggingTagging� Pericardial adherence/invasion� Pericardial inflammation
First pass perfusion� Tumor vascularity
Imaging techniquesImaging techniques
Cardiac and pericardial massesCardiac and pericardial masses
Cardiac tumor mimicsCardiac tumor mimics
518
TU
ESD
AY
Tumor and tumor-like conditions b l tiby location
AtriaAtria�Angiosarcoma (right)�Lymphoma (right)�Myxoma (left)�Other sarcomas (left)�Other sarcomas (left)�Thrombus (left)
VentriclesVentricles�FibromaFibroma �Rhabdomyoma
ValvesValves�Papillary fibroelastoma�Vegetations
PericardiumPericardium�Pericardial cyst
t t�Metastases
Cardiac tumorsCardiac tumors
Relative incidence of primary cardiac tumors in adults and children
Benign Malignant
� Myxoma (30%)� Lipoma (10%)� Fibroelastoma (10%)
� Angiosarcoma (9%)� Rhabdomyosarcoma
(6%)Fibroelastoma (10%)� Rhabdomyoma� Fibroma
H i
( )� Mesothelioma (4%)� Fibrosarcoma (3%)� Lymphoma (2%)� Hemangioma
� Teratoma� Lymphoma (2%)� Other sarcoma� Teratoma
M t t ti di t th h t i 20 40Metastatic disease to the heart is 20-40 x more common
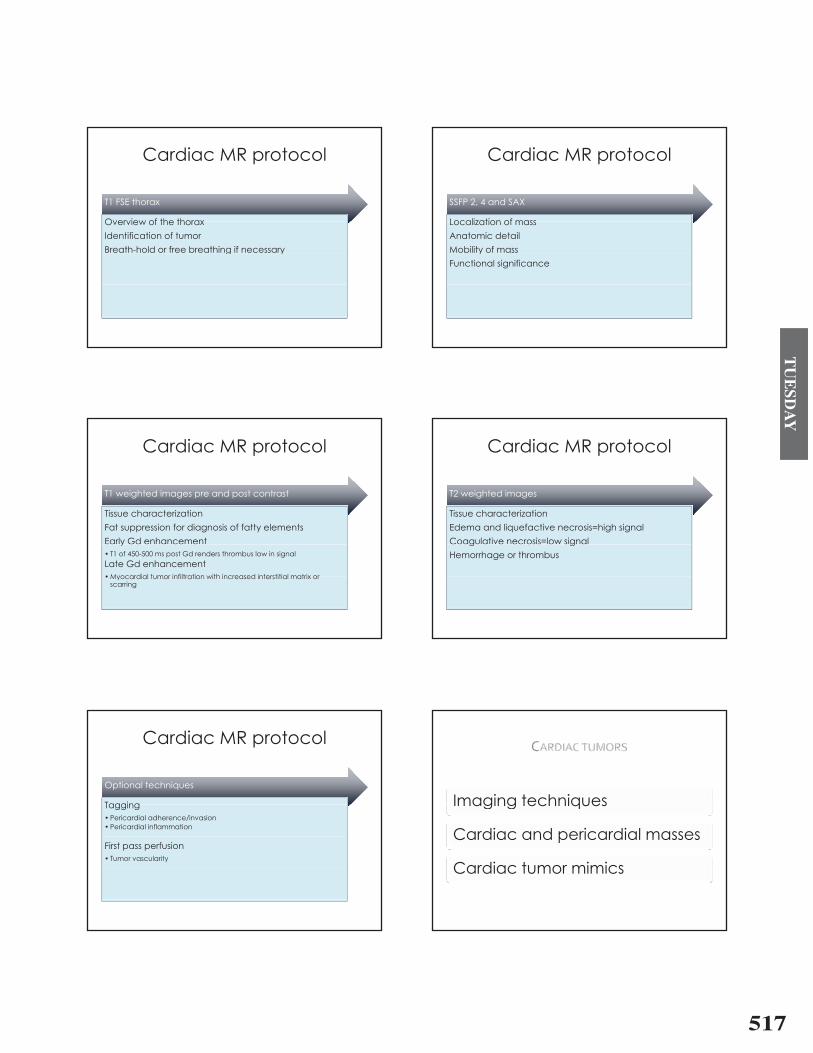
28FHx: Persistent progressive shortnessprogressive shortness of breath
Outside hospital CT pchest showed multiple pulmonary emboli
Returned to ED for SOB � Repeat CT chest
showed cardiac mass and thrombusmass and thrombus in right atrium and ventricle
UNDIFFERENTIATEDPatient died 1 month after tumor resection
UNDIFFERENTIATED PLEOMORPHIC SARCOMA
SarcomaSarcoma
Angiosarcoma is the most common malignant cardiac tumor in adultsAngiosarcoma is the most common malignant cardiac tumor in adults
Rhabdomyosarcoma is the most common malignant cardiac tumor in children
Rare but aggressive tumor with poor prognosis
Present between the 3rd and 5th decades of life
Clinical presentation
�Right heart failure�Hemorrhagic pericardial effusion�Metastatic disease
519
TU
ESD
AY
Sarcoma: Imaging manifestationsSarcoma: Imaging manifestations
Location varies depending on histology�Angiosarcoma�right atriumg g�Rhadomyosarcoma�multiple�Undifferentiated sarcoma�left atrium
MR�Heterogeneous signal on T1 and T2 weighted�Heterogeneous signal on T1 and T2 weighted
images�Avid inhomogeneous enhancement
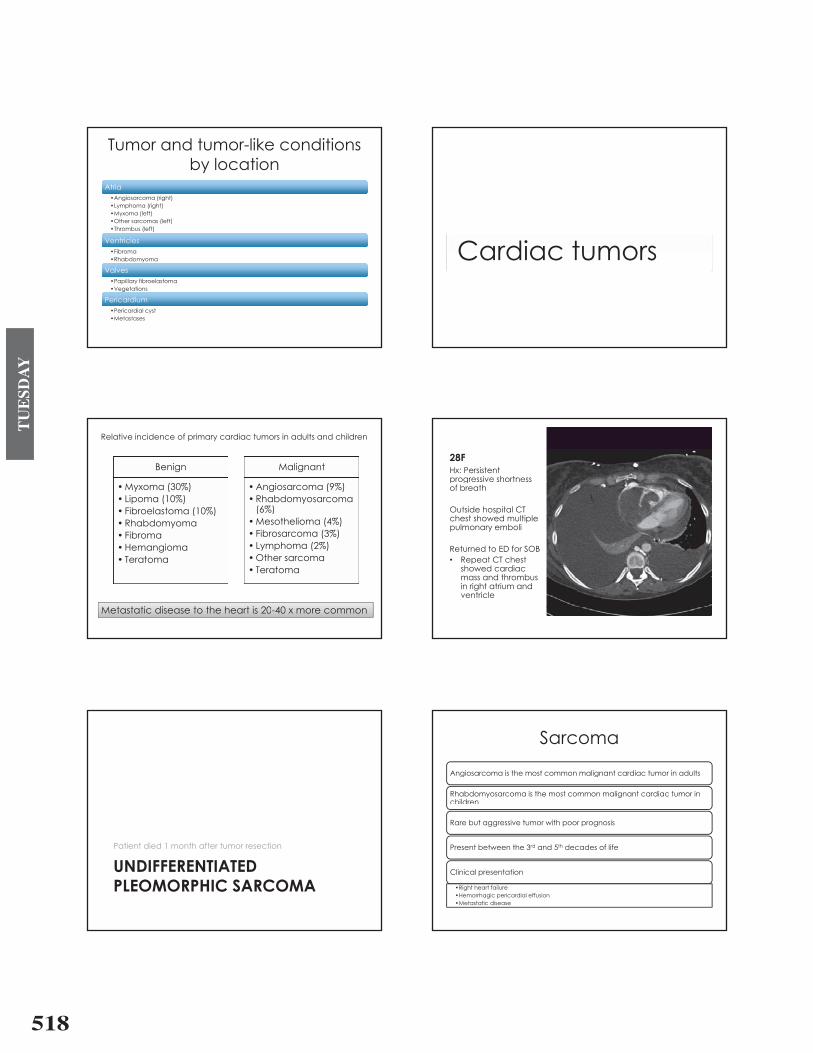
42MHx: HIV+, troponin bump and lactatebump and lactate elevation
CT abdomen demonstrated cardiac abnormality
CT chest and CMRCT chest and CMR subsequently ordered
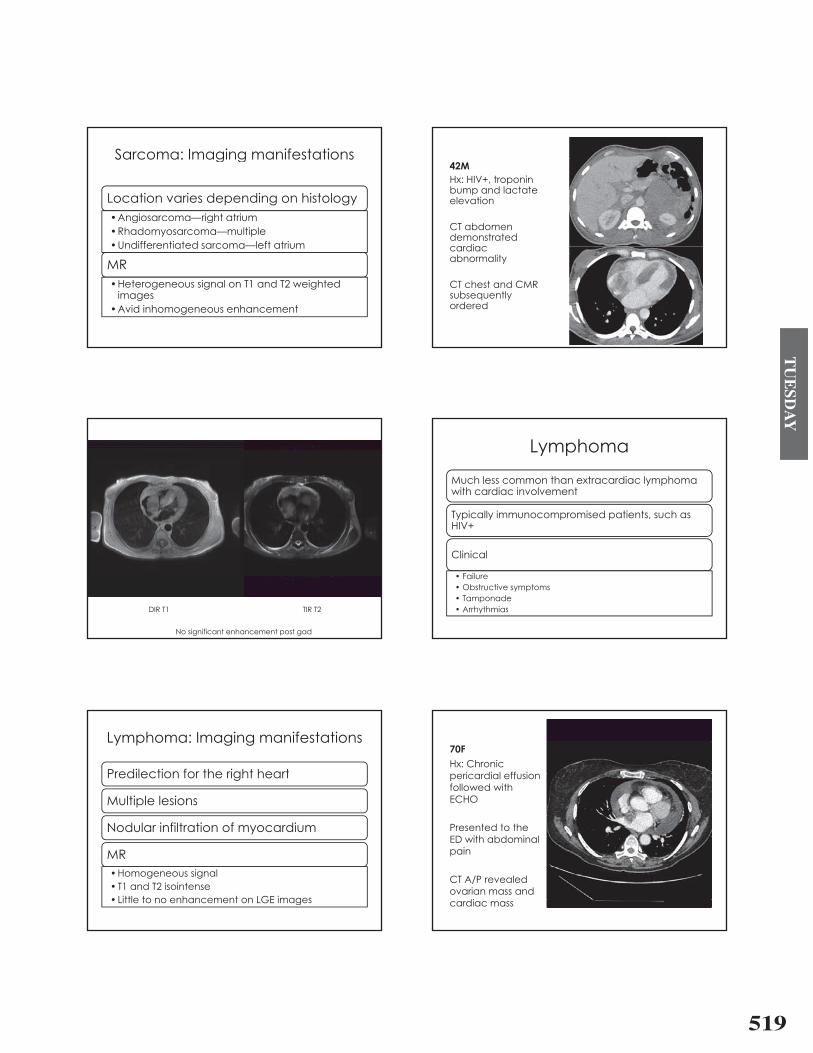
DIR T1 TIR T2DIR T1 TIR T2
No significant enhancement post gad
LymphomaLymphoma
Much less common than extracardiac lymphomaMuch less common than extracardiac lymphoma with cardiac involvement
Typically immunocompromised patients such asTypically immunocompromised patients, such as HIV+
Clinical
� Failure� Failure� Obstructive symptoms� Tamponade
Arrh thmias� Arrhythmias
Lymphoma: Imaging manifestationsLymphoma: Imaging manifestations
Predilection for the right heartPredilection for the right heart
Multiple lesionsMultiple lesions
Nodular infiltration of myocardium
MR�Homogeneous signal� T1 and T2 isointense� Little to no enhancement on LGE images� Little to no enhancement on LGE images
70FHx: Chronic
i di l ff ipericardial effusion followed with ECHO
Presented to the ED ith bd i lED with abdominal pain
CT A/P revealed ovarian mass and
dicardiac mass
520
TU
ESD
AY
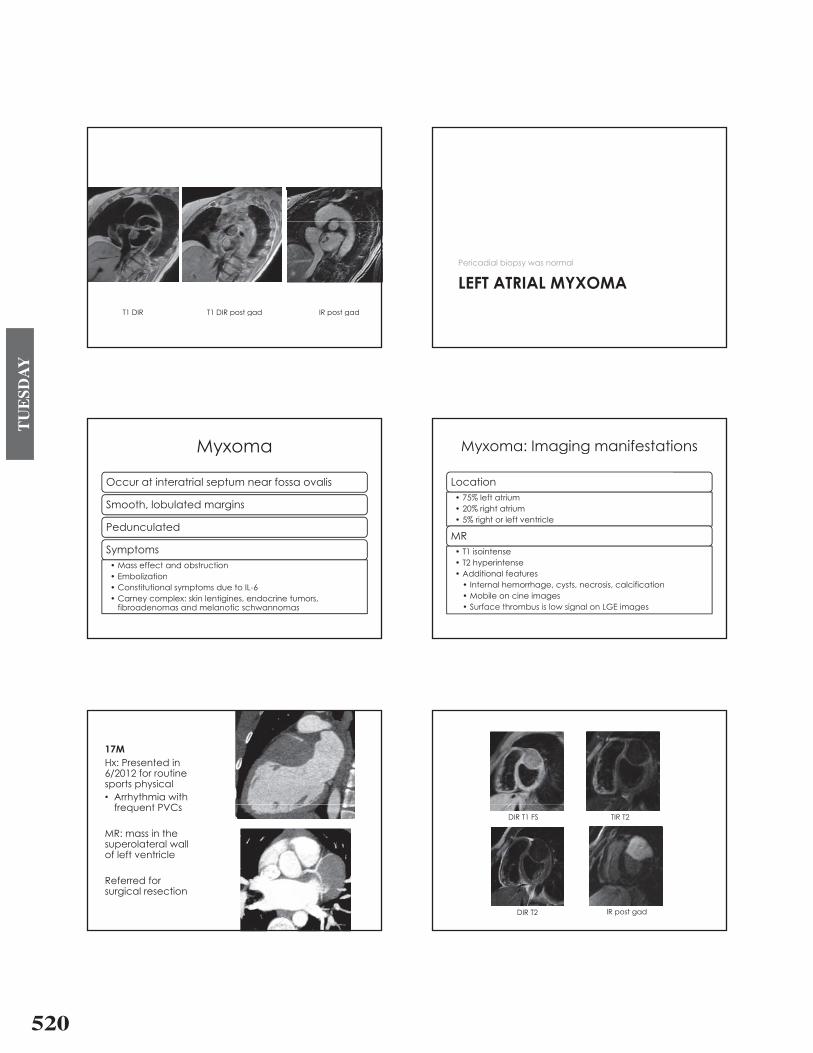
T1 DIR T1 DIR post gad IR post gad
LEFT ATRIAL MYXOMAPericadial biopsy was normal
LEFT ATRIAL MYXOMA
MyxomaMyxoma
Occur at interatrial septum near fossa ovalisOccur at interatrial septum near fossa ovalis
Smooth, lobulated margins
Pedunculated
Symptoms� Mass effect and obstruction� Embolization� Embolization� Constitutional symptoms due to IL-6� Carney complex: skin lentigines, endocrine tumors,
fibroadenomas and melanotic schwannomasfibroadenomas and melanotic schwannomas
Myxoma: Imaging manifestationsMyxoma: Imaging manifestations
LocationLocation� 75% left atrium� 20% right atrium� 5% right or left ventricle
MR� T1 isointense� T2 hyperintense� Additional featuresAdditional features� Internal hemorrhage, cysts, necrosis, calcification� Mobile on cine images� Surface thrombus is low signal on LGE imagesSurface thrombus is low signal on LGE images
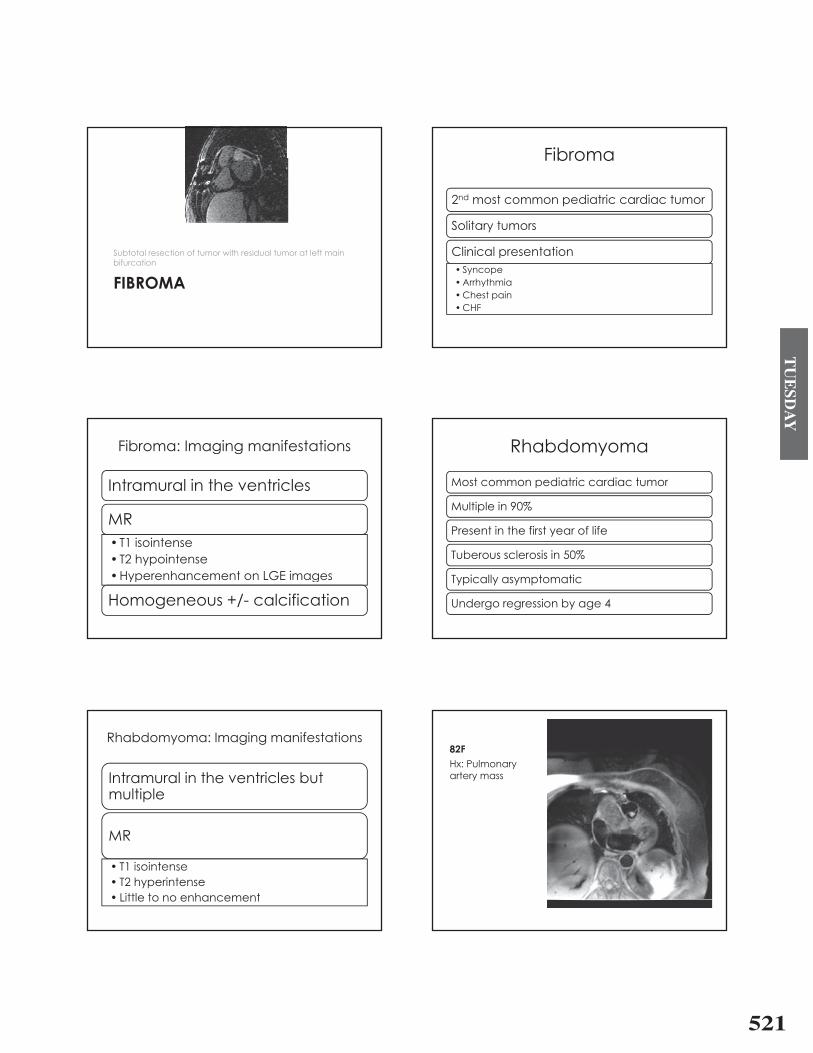
17MHx: Presented in 6/2012 for routine6/2012 for routine sports physical� Arrhythmia with
f t PVCfrequent PVCs
MR: mass in theMR: mass in the superolateral wall of left ventricle
Referred for surgical resection
DIR T1 FS TIR T2
DIR T2 IR post gad
521
TU
ESD
AY
Subtotal resection of tumor with residual tumor at left main
FIBROMA
Subtotal resection of tumor with residual tumor at left main bifurcation
FIBROMA
FibromaFibroma
2nd most common pediatric cardiac tumor
S lit tSolitary tumors
Clinical presentationClinical presentation� Syncope�ArrhythmiaArrhythmia�Chest pain�CHF
Fibroma: Imaging manifestationsFibroma: Imaging manifestations
I t l i th t i lIntramural in the ventricles
MR� T1 isointenseT1 isointense� T2 hypointense�Hyperenhancement on LGE images�Hyperenhancement on LGE images
Homogeneous +/- calcificationg
RhabdomyomaRhabdomyoma
Most common pediatric cardiac tumorMost common pediatric cardiac tumor
Multiple in 90%
Present in the first year of life
Tuberous sclerosis in 50%
T i ll t tiTypically asymptomatic
Undergo regression by age 4g g y g
Rhabdomyoma: Imaging manifestationsRhabdomyoma: Imaging manifestations
I t l i th t i l b tIntramural in the ventricles but multiple
MRMR
� T1 isointenseT1 isointense� T2 hyperintense� Little to no enhancementLittle to no enhancement
82FHx: Pulmonary
tartery mass
522
TU
ESD
AY
Papillary fibroelastoma: Imaging if t timanifestations
T i ll < 1 5Typically < 1.5 cm
Cli i l iClinical presentation�Often asymptomaticOften asymptomatic�Embolization of surface thrombus/tumor�No valvular abnormality�No valvular abnormality�Surgery if symptomatic or >1cm and
left-sidedleft sided
Papillary fibroelastoma: Imaging if t timanifestations
Pedicle adherent to downstream side of valvePedicle adherent to downstream side of valve unlike vegetation
Mobile
MR
� Isointense T1� Hyperintense T2� No enhancement� No enhancement
Pericardial tumorsPericardial tumors
Relative incidence of primary pericardial tumors
Benign
�Pericardial cyst�Pericardial lipoma
Malignant
�Mesothelioma�HemangiomaPericardial lipoma Hemangioma�Sarcoma�Lymphoma�Lipoblastomap�Paraganglioma�Germ cell tumors�Fibroma� Inflammatory
pseudotumor/IgG4-related disease
�PNET�PNET
Primary pericardial tumors much less common than primary cardiac tumorstumors
Direct invasion by neoplasm or metastatic disease is 100-1000x more common than primary pericardial tumor
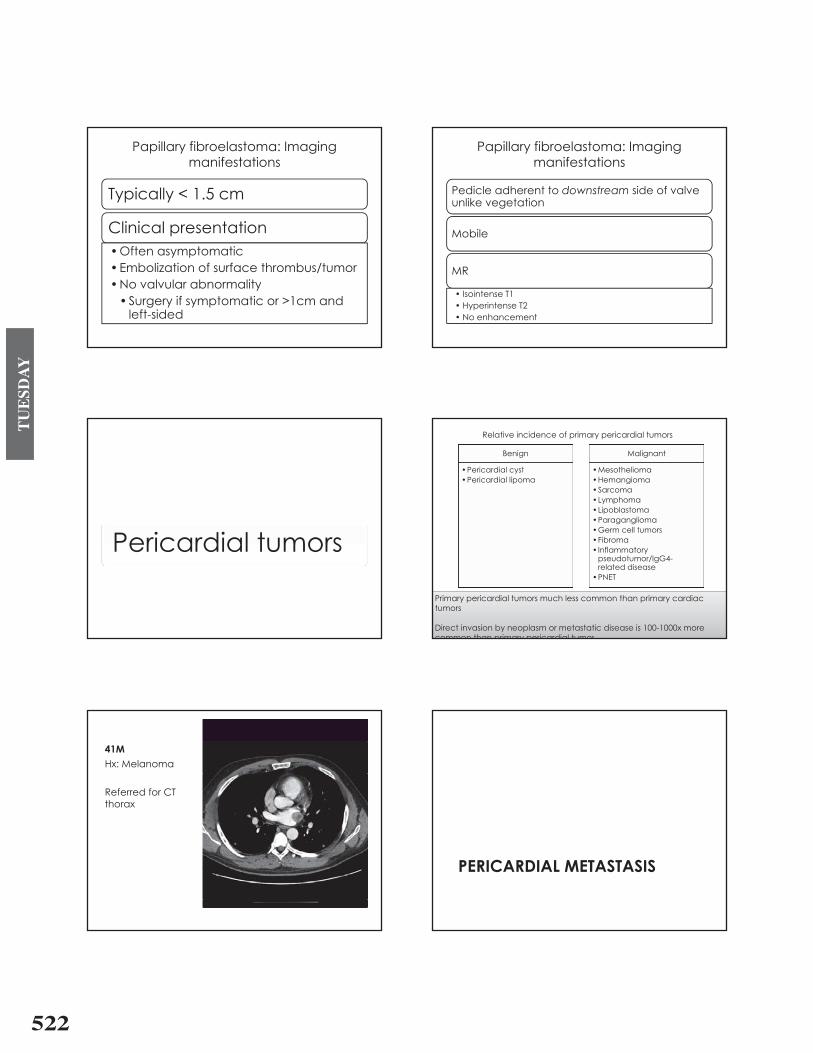
41MHx: Melanoma
Referred for CT thoraxthorax
PERICARDIAL METASTASISPERICARDIAL METASTASIS
523
TU
ESD
AY
Cardiac metastasesCardiac metastases
20 40x more common than primary cardiac tumors20-40x more common than primary cardiac tumors
10-12% of patients with known malignancy have cardiac metastases at autopsyautopsy
Pericardial involvement is most common (~95%)
Modes of spread (*most common)
�Hematogenous�lymphoma*, melanoma*, leukemia�Direct invasion�lung*, breast*, esophagus�Transvenous�RCC, HCC
Metastatic melanoma high T1/low T2
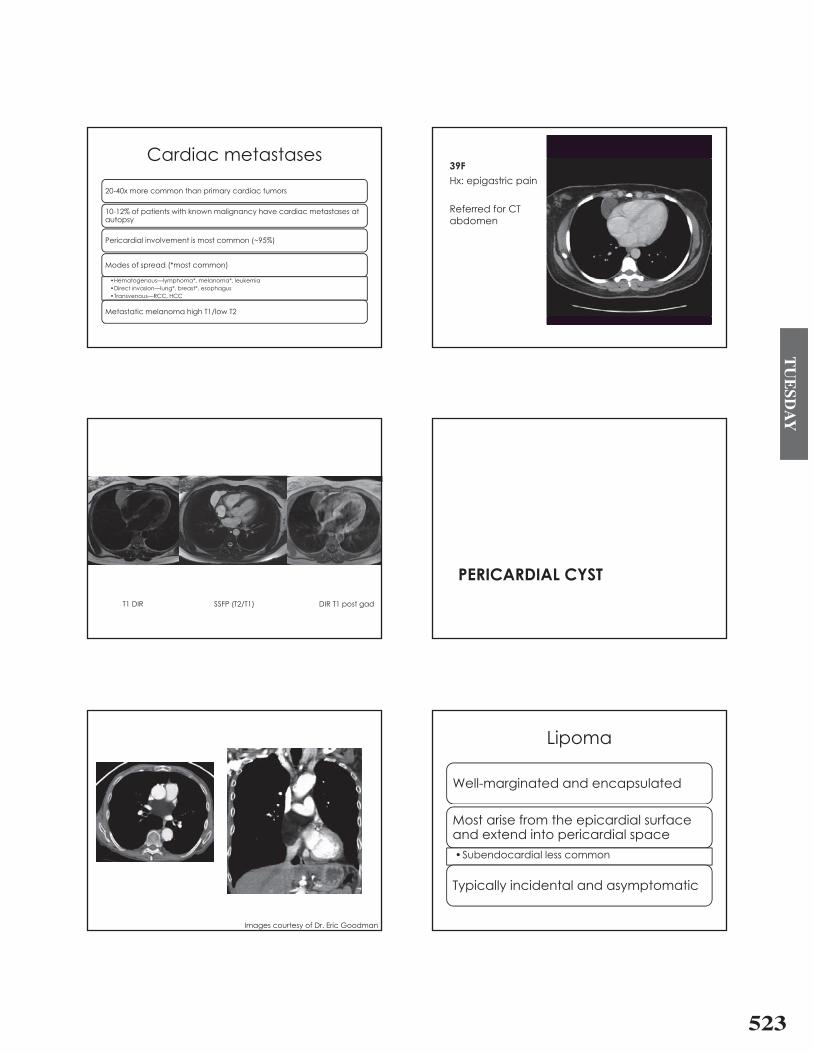
39F Hx: epigastric pain
Referred for CT abdomenabdomen
T1 DIR SSFP (T2/T1) DIR T1 post gad
PERICARDIAL CYSTPERICARDIAL CYST
Images courtesy of Dr. Eric Goodman
LipomaLipoma
Well-marginated and encapsulated
Most arise from the epicardial surface and extend into pericardial spaceand extend into pericardial space�Subendocardial less common
Typically incidental and asymptomatic
524
TU
ESD
AY
Lipoma: Imaging manifestationsLipoma: Imaging manifestations
CT f t tt tiCT: fat attenuation
MR�T1 hyperintense�T1 hyperintense�Low signal on fat suppressed
sequencessequences
No enhancement
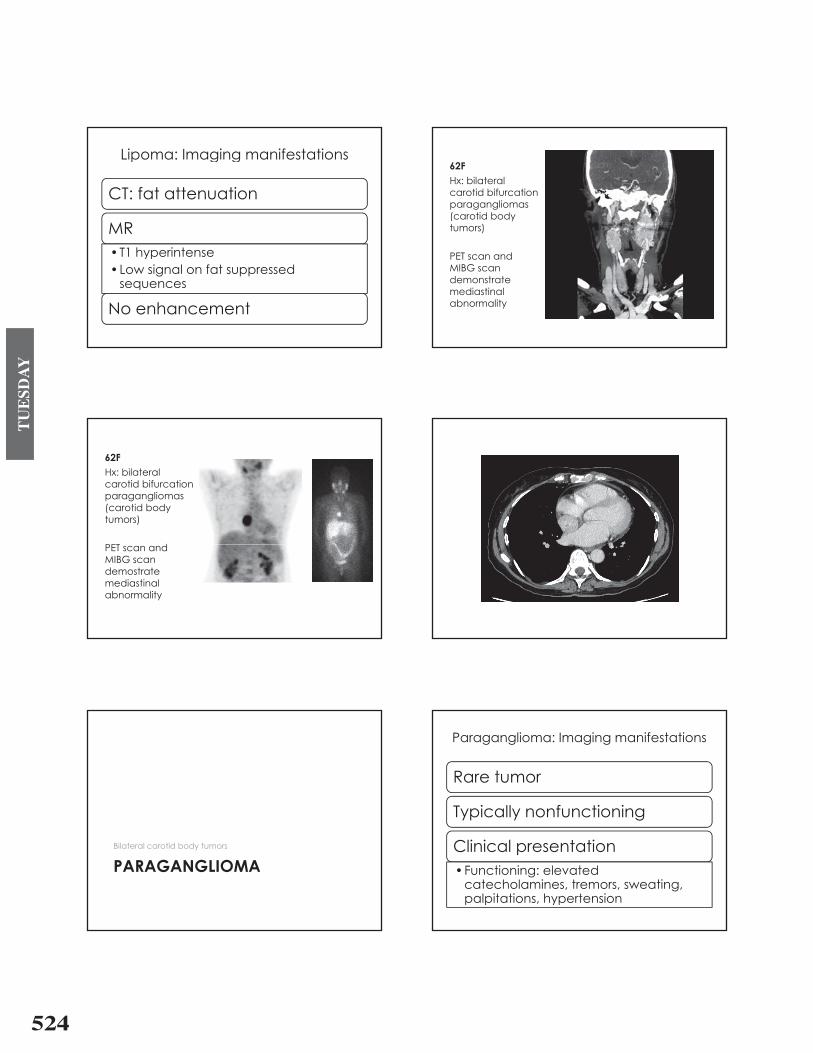
62FHx: bilateral
tid bif ticarotid bifurcation paragangliomas(carotid body tumors)
PET dPET scan and MIBG scan demonstrate mediastinalabnormality
62FHx: bilateral
tid bif ticarotid bifurcation paragangliomas(carotid body tumors)
PET dPET scan and MIBG scan demostratemediastinalabnormality
PARAGANGLIOMABilateral carotid body tumors
PARAGANGLIOMA
Paraganglioma: Imaging manifestationsParaganglioma: Imaging manifestations
R tRare tumor
Typically nonfunctioning
Clinical presentationF ti i l t d�Functioning: elevated catecholamines, tremors, sweating, palpitations hypertensionpalpitations, hypertension

525
TU
ESD
AY
Paraganglioma: Imaging manifestationsParaganglioma: Imaging manifestations
Adjacent to left atrium or anterior to aorticAdjacent to left atrium or anterior to aortic root
CT: hypervascular mass
� Feeding vessel may originate from coronary artery
MR: T2 hyperintense
� Enhancement post GdEnhancement post Gd
65M Hx: epicardialmass
T1 DIR T1 TIR
Post gad T1 3D FSPGR LGEPost gad T1 3D FSPGR LGE
Epicardial mass with extrinsic compression
HEMANGIOMA
Epicardial mass with extrinsic compressionNo invasion of cardiac structures
HEMANGIOMA
HemangiomaHemangioma
Usually solitaryUsually solitary
Predilection for the ventricles
526
TU
ESD
AY
Hemangioma: Imaging manifestationsHemangioma: Imaging manifestations
H tHeterogeneous
MR�T1 hyperintense�T1 hyperintense�T2 hyperintense
Avid enhancement although�Avid enhancement although calcification or fibrous septations may be presentbe present
Cardiac tumor mimics
Normal structures Pseudotumors
� Coumadin ridge� Between the LAA and
the left superior l i ( ti
� Thrombus� Caseous calcification
of the mitral annuluspulmonary vein (Q tip sign)
� Eustachian valveC i t t i li
� Lipomatous hypertrophy� > 2cm
� Crista terminalis � Nonencapsulated� Spares the fossa
ovalis giving it a d bb ll hdumbbell shape
� Vegetation� Typically on low
id f lpressure side of valve
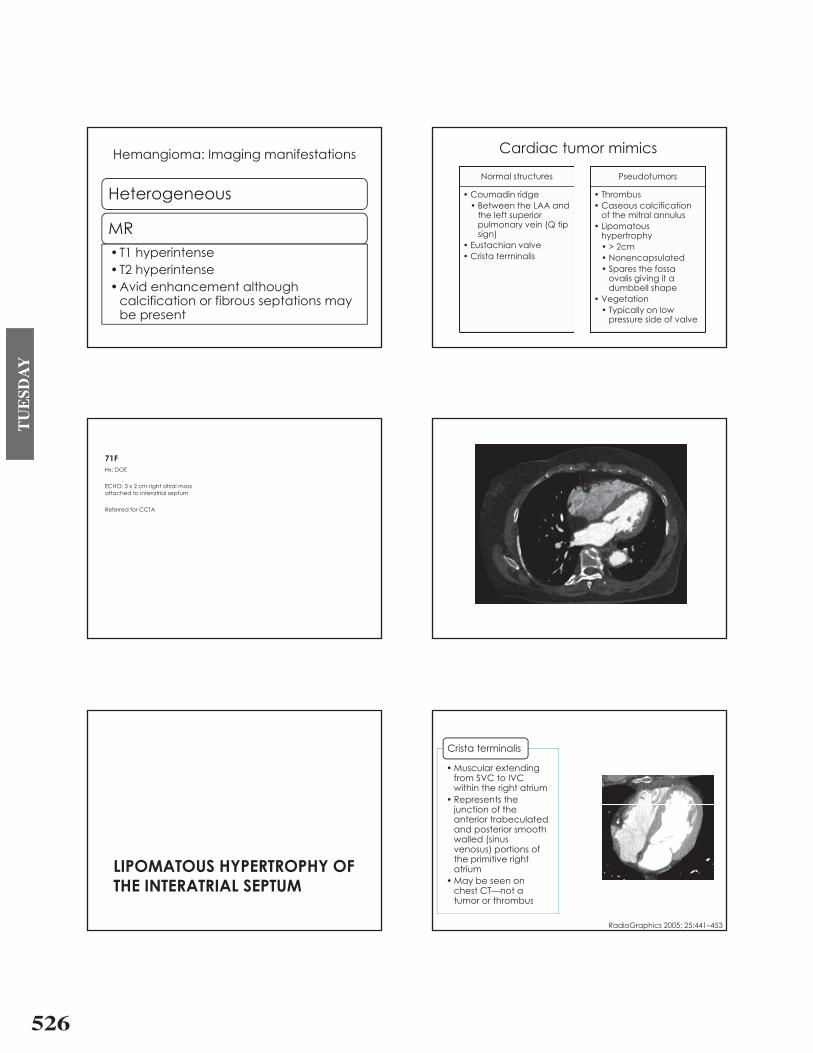
71FHx: DOE
ECHO: 3 x 2 cm right atrial mass attached to interatrial septum
Referred for CCTA
LIPOMATOUS HYPERTROPHY OFLIPOMATOUS HYPERTROPHY OF THE INTERATRIAL SEPTUM
� Muscular extending
Crista terminalis
from SVC to IVC within the right atrium
� Represents the junction of the anterior trabeculatedand posterior smooth
ll d ( iwalled (sinus venosus) portions of the primitive right atriumatrium
� May be seen on chest CT�not a tumor or thrombustumor or thrombus
RadioGraphics 2005; 25:441�453
527
TU
ESD
AY
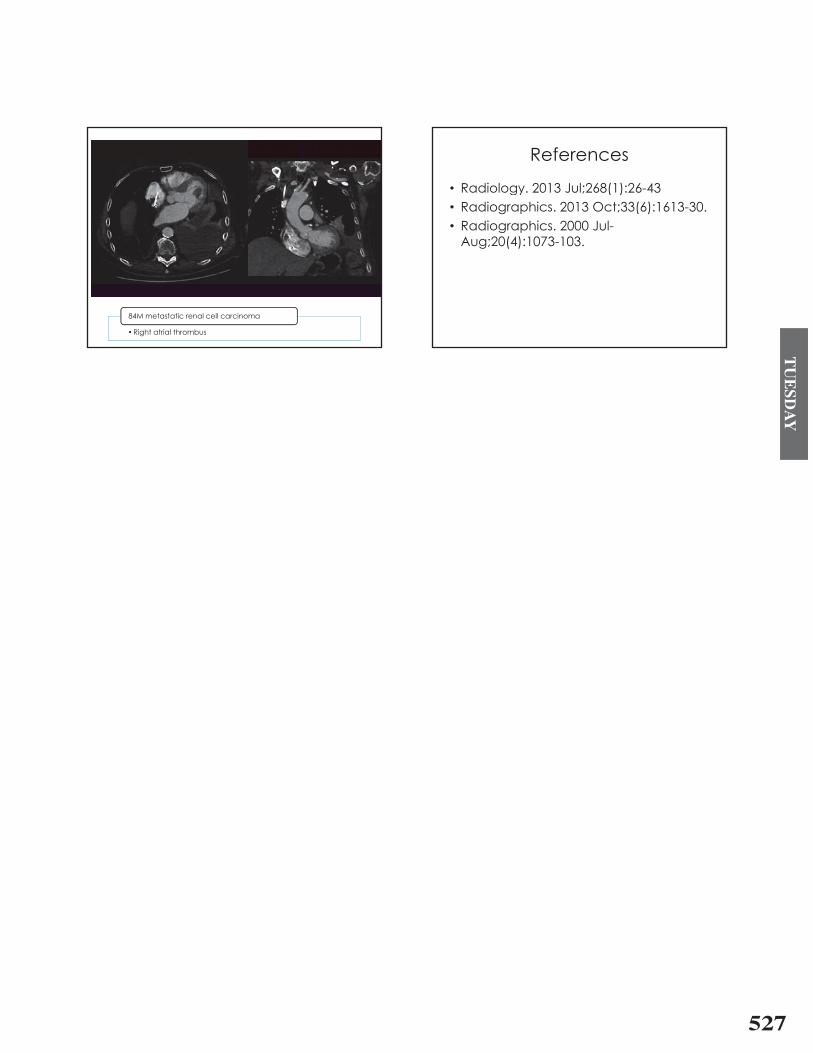
84M metastatic renal cell carcinoma
� Right atrial thrombus
84M metastatic renal cell carcinoma
ReferencesReferences
� Radiology 2013 Jul;268(1):26-43Radiology. 2013 Jul;268(1):26 43� Radiographics. 2013 Oct;33(6):1613-30.
R di hi 2000 J l� Radiographics. 2000 Jul-Aug;20(4):1073-103.