cap and pneumococcol pneumonia - atuder
TRANSCRIPT
Associated Prof Dr İsa KILICcedilASLAN
Gazi University School of Medicine
Emergency Medicine Department
18May2014
COMMUNITY ACQUIRED PNEUMONIA and
PNEUMOCOCCAL PNEUMONIA
Community Acquired Pneumonia (CAP)
bull Definition
bull CASES
bull Epidemiology
bull Pathogenesis
bull Microbiology
bull Treatment recommendations
bull The evidence for efficacy of different antibiotic mediations
2
Community Acquired Pneumonia
bull Definition
ndash hellip an acute infection of the pulmonary parenchyma
ndash associated with at least some symptoms of acute infection
ndash accompanied by the presence of an acute infiltrate on a chest radiograph or
ndash auscultatory findings consistent with pneumonia in a patient not hospitalized or residing in a long term care facility for gt 14 days before onset of symptoms
Bartlett Clin Infect Dis 200031347-82 3
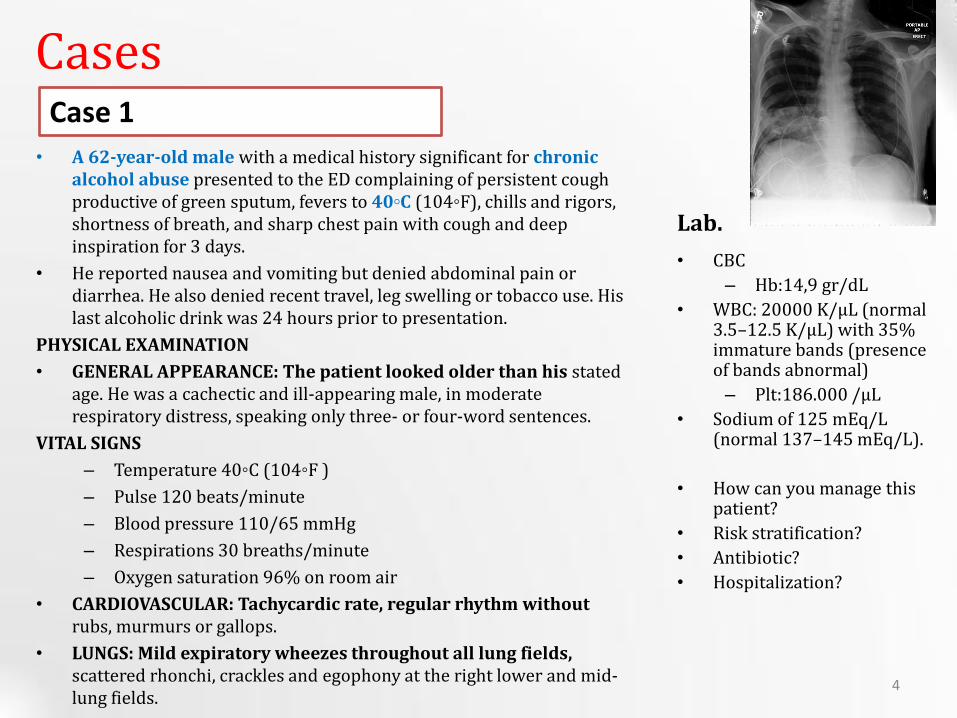
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
4
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
5
Case 3
Lab
bull 34 year old male
bull Complaint Fever chest pain cough severe myaljia
bull Hx
ndash Chest pain for 2 days cough for 1 week Hx for upper respiratory infection for 2 weeks ago
ndash Fevermdash4 days
ndash Sputum production
ndash He had complaints of severe myaljia
bull Past medical hx-Non
bull MedicationmdashParacetamol for fever and myalgia
bull Vital Sign
ndash BP 13070 mmHg
ndash Pulse 110min
ndash RR 24min
ndash Fever 380 ˚C
ndash Pulse 97
bull Physical exam
ndash Decreased breath sounds and crackles on left basal lobe
bull CBC
ndash Hb149 grdL
ndash WBC 18000
ndash Plt246000 microL
bull RFT and LFTmdashNormal
bull Arterial Blood Gases
ndash pH 738
ndash HCO3 26 mEqlt
ndash pCO2 38 mmH20
ndash pO2 65 mm H2O
bull How can you manage this patient
6
Community Acquired Pneumonia
bull Epidemiology
ndash Overall rate in adultsmdash5-61000 cases
ndash increases with aging
ndash Seasonal variationmdashoccurs more during the winter months
ndash Higher in men
ndash Mortality 2-30
bull lt1 for those not requiring hospitalization
bull Up to 23 mortality during 30-day follow-up among patients who require hospitalization
ndash Streptococcus pneumonia is the most common cause of pneumonia worldwide
7
Community Acquired Pneumonia
0
200
400
600
800
1000
1200
1400
lt5 5 to 17 18-24 25-44 45-64 gt65
898
1071
83
1171 1207
684
of cases
0
10
20
30
40
50
60
70
80
lt4 5 to 14 15-24 25-44 45-64 gt65
0 0 0 2
57
749
of deaths in 1000s
Mortality
Community Acquired Pneumonia
9
Age-specific Rates of Hospital Admission by Pathogen
Marston BJ Plouffe JF File TM Jr Hackman BA Salstrom SJ Lipman HB Kolczak MS Breiman RF Incidence of community-acquired pneumonia requiring hospitalization Results of a population-based active surveillance Study in Ohio The Community-Based Pneumonia Incidence Study Group Arch Intern Med 1997157(15)1709-18
10
CAP ndash Pathogenesis
bull Inhalation aspiration and hematogenous spread are the 3 main mechanisms by which bacteria reaches the lungs
Inhalation
Aspiration
Hematogenous
11
Pathogenesis
bull Primary inhalation when organisms bypass normal respiratory defense mechanisms or when the Pt inhales aerobic GN organisms that colonize the upper respiratory tract or respiratory support equipment
bull Aspiration occurs when the patient aspirates colonized upper respiratory tract secretions
ndash Stomach reservoir of GNR that can ascend colonizing the respiratory tract
bull Hematogenous originate from a distant source and reach the lungs via the blood stream
12
bull Risk Factors for pneumonia ndash age ndash smoking ndash asthma ndash immunosuppression ndash institutionalization ndash COPD ndash PVD ndash Dementia ndash HIVAIDS
Community Acquired Pneumonia
13
bull Risk Factors in Patients Requiring Hospitalization ndash older unemployed
ndash common cold in the previous year
ndash asthma COPD steroid or bronchodilator use
ndash Chronic disease
ndash amount of smoking
Farr BM Respir Med 200094954-63
Community Acquired Pneumonia
14
bull Risk Factors for Mortality
ndash age
ndash bacteremia (for S pneumoniae)
ndash extent of radiographic changes
ndash degree of immunosuppression
ndash amount of alcohol
Community Acquired Pneumonia
15
ndash S pneumoniae 20-60
ndash H influenzae 3-10
ndash Chlamydia pneumoniae 4-6
ndash Mycoplasma pneumonaie 1-6
Community Acquired Pneumonia
ndash Legionella spp 2-8
ndash S aureus 3-5
ndash Gram negative bacilli 3-5
ndash Viruses 2-13
40-60 - NO CAUSE IDENTIFIED
2-5 - TWO OR MORE CAUSES
Microbiology
Bartlett NEJM 19953331618-24
16
Microbial etiology of community-acquired pneumonia in patients who
underwent comprehensive testing
17
Streptococcus pneumonia (Pneumococcus)
Most common cause of CAP About 23 of CAP are due to
Spneumoniae These are gram positive diplococci Typical symptoms (eg malaise
shaking chills fever rusty sputum pleuritic chest pain cough)
Lobar infiltrate on CXR May be immunosuppressed host 25 will have bacteremia ndash serious
effects
18
Risk Factors for Pneumococcal Pneumonia
bull Influenza infection
bull Alcohol abuse
bull Smoking--(x4 fold )
bull COPD and asthma
bull Hyposplenism or splenectomy
bull Immunocompromise---HIV (x50-100 fold ) MM SLE Transplant
bull Others---homeless pregnancy crack cocaine use incarceration
19
64 year old male with insulin dependent diabetes mellitus
He was admitted with bacteremic pneumococcal pneumonia Note the left lower lobe opacity
Pneumococcal pneumonia is the paradigm of classic lobar bacterial pneumonia
20
Complications of pneumococcal pneumonia
21
OTHER BACTERIAL PNEUMONIA
22
Atypical Pneumonia
bull 2 cause (especially in younger population)
bull Commonly associated with milder Sxrsquos subacute onset non-productive cough no focal infiltrate on CXR
bull Mycoplasma younger Pts extra-pulm Sxrsquos (anemia rashes) headache sore throat
bull Chlamydia year round URI Sx sore throat
bull Legionella higher mortality rate water-borne outbreaks hyponatremia diarrhea
23
Mycoplasma pneumonia
24
Mycoplasma pneumonia
25
Pneumocystis jirovecii pneumonia in patient with AIDS
26
Viruses and Pneumonia Pneumonia in the normal host
bull Adults or Children
bull Influenza A and B RSV Adenovirus Para Influenza
Pneumonia in the immuno-compromised
bull Measles HSV CMV HHV-6 Influenza viruses
bull Can cause a primary viral pneumonia Cause partial paralysis of
ldquomucociliary escalatorrdquo - increased risk of secondary bacterial
LRTI Saureus pneumonia is a known complication following
influenza infection
27
Other bacteria bull Anaerobes
ndash Aspiration-prone Pt putrid sputum dental disease
bull Gram negative ndash Klebsiella - alcoholics
ndash Branhamella catarrhalis - sinus disease otitis COPD
ndash H influenza
28
Diagnosis and Management
29
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
Community Acquired Pneumonia (CAP)
bull Definition
bull CASES
bull Epidemiology
bull Pathogenesis
bull Microbiology
bull Treatment recommendations
bull The evidence for efficacy of different antibiotic mediations
2
Community Acquired Pneumonia
bull Definition
ndash hellip an acute infection of the pulmonary parenchyma
ndash associated with at least some symptoms of acute infection
ndash accompanied by the presence of an acute infiltrate on a chest radiograph or
ndash auscultatory findings consistent with pneumonia in a patient not hospitalized or residing in a long term care facility for gt 14 days before onset of symptoms
Bartlett Clin Infect Dis 200031347-82 3
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
4
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
5
Case 3
Lab
bull 34 year old male
bull Complaint Fever chest pain cough severe myaljia
bull Hx
ndash Chest pain for 2 days cough for 1 week Hx for upper respiratory infection for 2 weeks ago
ndash Fevermdash4 days
ndash Sputum production
ndash He had complaints of severe myaljia
bull Past medical hx-Non
bull MedicationmdashParacetamol for fever and myalgia
bull Vital Sign
ndash BP 13070 mmHg
ndash Pulse 110min
ndash RR 24min
ndash Fever 380 ˚C
ndash Pulse 97
bull Physical exam
ndash Decreased breath sounds and crackles on left basal lobe
bull CBC
ndash Hb149 grdL
ndash WBC 18000
ndash Plt246000 microL
bull RFT and LFTmdashNormal
bull Arterial Blood Gases
ndash pH 738
ndash HCO3 26 mEqlt
ndash pCO2 38 mmH20
ndash pO2 65 mm H2O
bull How can you manage this patient
6
Community Acquired Pneumonia
bull Epidemiology
ndash Overall rate in adultsmdash5-61000 cases
ndash increases with aging
ndash Seasonal variationmdashoccurs more during the winter months
ndash Higher in men
ndash Mortality 2-30
bull lt1 for those not requiring hospitalization
bull Up to 23 mortality during 30-day follow-up among patients who require hospitalization
ndash Streptococcus pneumonia is the most common cause of pneumonia worldwide
7
Community Acquired Pneumonia
0
200
400
600
800
1000
1200
1400
lt5 5 to 17 18-24 25-44 45-64 gt65
898
1071
83
1171 1207
684
of cases
0
10
20
30
40
50
60
70
80
lt4 5 to 14 15-24 25-44 45-64 gt65
0 0 0 2
57
749
of deaths in 1000s
Mortality
Community Acquired Pneumonia
9
Age-specific Rates of Hospital Admission by Pathogen
Marston BJ Plouffe JF File TM Jr Hackman BA Salstrom SJ Lipman HB Kolczak MS Breiman RF Incidence of community-acquired pneumonia requiring hospitalization Results of a population-based active surveillance Study in Ohio The Community-Based Pneumonia Incidence Study Group Arch Intern Med 1997157(15)1709-18
10
CAP ndash Pathogenesis
bull Inhalation aspiration and hematogenous spread are the 3 main mechanisms by which bacteria reaches the lungs
Inhalation
Aspiration
Hematogenous
11
Pathogenesis
bull Primary inhalation when organisms bypass normal respiratory defense mechanisms or when the Pt inhales aerobic GN organisms that colonize the upper respiratory tract or respiratory support equipment
bull Aspiration occurs when the patient aspirates colonized upper respiratory tract secretions
ndash Stomach reservoir of GNR that can ascend colonizing the respiratory tract
bull Hematogenous originate from a distant source and reach the lungs via the blood stream
12
bull Risk Factors for pneumonia ndash age ndash smoking ndash asthma ndash immunosuppression ndash institutionalization ndash COPD ndash PVD ndash Dementia ndash HIVAIDS
Community Acquired Pneumonia
13
bull Risk Factors in Patients Requiring Hospitalization ndash older unemployed
ndash common cold in the previous year
ndash asthma COPD steroid or bronchodilator use
ndash Chronic disease
ndash amount of smoking
Farr BM Respir Med 200094954-63
Community Acquired Pneumonia
14
bull Risk Factors for Mortality
ndash age
ndash bacteremia (for S pneumoniae)
ndash extent of radiographic changes
ndash degree of immunosuppression
ndash amount of alcohol
Community Acquired Pneumonia
15
ndash S pneumoniae 20-60
ndash H influenzae 3-10
ndash Chlamydia pneumoniae 4-6
ndash Mycoplasma pneumonaie 1-6
Community Acquired Pneumonia
ndash Legionella spp 2-8
ndash S aureus 3-5
ndash Gram negative bacilli 3-5
ndash Viruses 2-13
40-60 - NO CAUSE IDENTIFIED
2-5 - TWO OR MORE CAUSES
Microbiology
Bartlett NEJM 19953331618-24
16
Microbial etiology of community-acquired pneumonia in patients who
underwent comprehensive testing
17
Streptococcus pneumonia (Pneumococcus)
Most common cause of CAP About 23 of CAP are due to
Spneumoniae These are gram positive diplococci Typical symptoms (eg malaise
shaking chills fever rusty sputum pleuritic chest pain cough)
Lobar infiltrate on CXR May be immunosuppressed host 25 will have bacteremia ndash serious
effects
18
Risk Factors for Pneumococcal Pneumonia
bull Influenza infection
bull Alcohol abuse
bull Smoking--(x4 fold )
bull COPD and asthma
bull Hyposplenism or splenectomy
bull Immunocompromise---HIV (x50-100 fold ) MM SLE Transplant
bull Others---homeless pregnancy crack cocaine use incarceration
19
64 year old male with insulin dependent diabetes mellitus
He was admitted with bacteremic pneumococcal pneumonia Note the left lower lobe opacity
Pneumococcal pneumonia is the paradigm of classic lobar bacterial pneumonia
20
Complications of pneumococcal pneumonia
21
OTHER BACTERIAL PNEUMONIA
22
Atypical Pneumonia
bull 2 cause (especially in younger population)
bull Commonly associated with milder Sxrsquos subacute onset non-productive cough no focal infiltrate on CXR
bull Mycoplasma younger Pts extra-pulm Sxrsquos (anemia rashes) headache sore throat
bull Chlamydia year round URI Sx sore throat
bull Legionella higher mortality rate water-borne outbreaks hyponatremia diarrhea
23
Mycoplasma pneumonia
24
Mycoplasma pneumonia
25
Pneumocystis jirovecii pneumonia in patient with AIDS
26
Viruses and Pneumonia Pneumonia in the normal host
bull Adults or Children
bull Influenza A and B RSV Adenovirus Para Influenza
Pneumonia in the immuno-compromised
bull Measles HSV CMV HHV-6 Influenza viruses
bull Can cause a primary viral pneumonia Cause partial paralysis of
ldquomucociliary escalatorrdquo - increased risk of secondary bacterial
LRTI Saureus pneumonia is a known complication following
influenza infection
27
Other bacteria bull Anaerobes
ndash Aspiration-prone Pt putrid sputum dental disease
bull Gram negative ndash Klebsiella - alcoholics
ndash Branhamella catarrhalis - sinus disease otitis COPD
ndash H influenza
28
Diagnosis and Management
29
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
Community Acquired Pneumonia
bull Definition
ndash hellip an acute infection of the pulmonary parenchyma
ndash associated with at least some symptoms of acute infection
ndash accompanied by the presence of an acute infiltrate on a chest radiograph or
ndash auscultatory findings consistent with pneumonia in a patient not hospitalized or residing in a long term care facility for gt 14 days before onset of symptoms
Bartlett Clin Infect Dis 200031347-82 3
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
4
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
5
Case 3
Lab
bull 34 year old male
bull Complaint Fever chest pain cough severe myaljia
bull Hx
ndash Chest pain for 2 days cough for 1 week Hx for upper respiratory infection for 2 weeks ago
ndash Fevermdash4 days
ndash Sputum production
ndash He had complaints of severe myaljia
bull Past medical hx-Non
bull MedicationmdashParacetamol for fever and myalgia
bull Vital Sign
ndash BP 13070 mmHg
ndash Pulse 110min
ndash RR 24min
ndash Fever 380 ˚C
ndash Pulse 97
bull Physical exam
ndash Decreased breath sounds and crackles on left basal lobe
bull CBC
ndash Hb149 grdL
ndash WBC 18000
ndash Plt246000 microL
bull RFT and LFTmdashNormal
bull Arterial Blood Gases
ndash pH 738
ndash HCO3 26 mEqlt
ndash pCO2 38 mmH20
ndash pO2 65 mm H2O
bull How can you manage this patient
6
Community Acquired Pneumonia
bull Epidemiology
ndash Overall rate in adultsmdash5-61000 cases
ndash increases with aging
ndash Seasonal variationmdashoccurs more during the winter months
ndash Higher in men
ndash Mortality 2-30
bull lt1 for those not requiring hospitalization
bull Up to 23 mortality during 30-day follow-up among patients who require hospitalization
ndash Streptococcus pneumonia is the most common cause of pneumonia worldwide
7
Community Acquired Pneumonia
0
200
400
600
800
1000
1200
1400
lt5 5 to 17 18-24 25-44 45-64 gt65
898
1071
83
1171 1207
684
of cases
0
10
20
30
40
50
60
70
80
lt4 5 to 14 15-24 25-44 45-64 gt65
0 0 0 2
57
749
of deaths in 1000s
Mortality
Community Acquired Pneumonia
9
Age-specific Rates of Hospital Admission by Pathogen
Marston BJ Plouffe JF File TM Jr Hackman BA Salstrom SJ Lipman HB Kolczak MS Breiman RF Incidence of community-acquired pneumonia requiring hospitalization Results of a population-based active surveillance Study in Ohio The Community-Based Pneumonia Incidence Study Group Arch Intern Med 1997157(15)1709-18
10
CAP ndash Pathogenesis
bull Inhalation aspiration and hematogenous spread are the 3 main mechanisms by which bacteria reaches the lungs
Inhalation
Aspiration
Hematogenous
11
Pathogenesis
bull Primary inhalation when organisms bypass normal respiratory defense mechanisms or when the Pt inhales aerobic GN organisms that colonize the upper respiratory tract or respiratory support equipment
bull Aspiration occurs when the patient aspirates colonized upper respiratory tract secretions
ndash Stomach reservoir of GNR that can ascend colonizing the respiratory tract
bull Hematogenous originate from a distant source and reach the lungs via the blood stream
12
bull Risk Factors for pneumonia ndash age ndash smoking ndash asthma ndash immunosuppression ndash institutionalization ndash COPD ndash PVD ndash Dementia ndash HIVAIDS
Community Acquired Pneumonia
13
bull Risk Factors in Patients Requiring Hospitalization ndash older unemployed
ndash common cold in the previous year
ndash asthma COPD steroid or bronchodilator use
ndash Chronic disease
ndash amount of smoking
Farr BM Respir Med 200094954-63
Community Acquired Pneumonia
14
bull Risk Factors for Mortality
ndash age
ndash bacteremia (for S pneumoniae)
ndash extent of radiographic changes
ndash degree of immunosuppression
ndash amount of alcohol
Community Acquired Pneumonia
15
ndash S pneumoniae 20-60
ndash H influenzae 3-10
ndash Chlamydia pneumoniae 4-6
ndash Mycoplasma pneumonaie 1-6
Community Acquired Pneumonia
ndash Legionella spp 2-8
ndash S aureus 3-5
ndash Gram negative bacilli 3-5
ndash Viruses 2-13
40-60 - NO CAUSE IDENTIFIED
2-5 - TWO OR MORE CAUSES
Microbiology
Bartlett NEJM 19953331618-24
16
Microbial etiology of community-acquired pneumonia in patients who
underwent comprehensive testing
17
Streptococcus pneumonia (Pneumococcus)
Most common cause of CAP About 23 of CAP are due to
Spneumoniae These are gram positive diplococci Typical symptoms (eg malaise
shaking chills fever rusty sputum pleuritic chest pain cough)
Lobar infiltrate on CXR May be immunosuppressed host 25 will have bacteremia ndash serious
effects
18
Risk Factors for Pneumococcal Pneumonia
bull Influenza infection
bull Alcohol abuse
bull Smoking--(x4 fold )
bull COPD and asthma
bull Hyposplenism or splenectomy
bull Immunocompromise---HIV (x50-100 fold ) MM SLE Transplant
bull Others---homeless pregnancy crack cocaine use incarceration
19
64 year old male with insulin dependent diabetes mellitus
He was admitted with bacteremic pneumococcal pneumonia Note the left lower lobe opacity
Pneumococcal pneumonia is the paradigm of classic lobar bacterial pneumonia
20
Complications of pneumococcal pneumonia
21
OTHER BACTERIAL PNEUMONIA
22
Atypical Pneumonia
bull 2 cause (especially in younger population)
bull Commonly associated with milder Sxrsquos subacute onset non-productive cough no focal infiltrate on CXR
bull Mycoplasma younger Pts extra-pulm Sxrsquos (anemia rashes) headache sore throat
bull Chlamydia year round URI Sx sore throat
bull Legionella higher mortality rate water-borne outbreaks hyponatremia diarrhea
23
Mycoplasma pneumonia
24
Mycoplasma pneumonia
25
Pneumocystis jirovecii pneumonia in patient with AIDS
26
Viruses and Pneumonia Pneumonia in the normal host
bull Adults or Children
bull Influenza A and B RSV Adenovirus Para Influenza
Pneumonia in the immuno-compromised
bull Measles HSV CMV HHV-6 Influenza viruses
bull Can cause a primary viral pneumonia Cause partial paralysis of
ldquomucociliary escalatorrdquo - increased risk of secondary bacterial
LRTI Saureus pneumonia is a known complication following
influenza infection
27
Other bacteria bull Anaerobes
ndash Aspiration-prone Pt putrid sputum dental disease
bull Gram negative ndash Klebsiella - alcoholics
ndash Branhamella catarrhalis - sinus disease otitis COPD
ndash H influenza
28
Diagnosis and Management
29
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
4
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
5
Case 3
Lab
bull 34 year old male
bull Complaint Fever chest pain cough severe myaljia
bull Hx
ndash Chest pain for 2 days cough for 1 week Hx for upper respiratory infection for 2 weeks ago
ndash Fevermdash4 days
ndash Sputum production
ndash He had complaints of severe myaljia
bull Past medical hx-Non
bull MedicationmdashParacetamol for fever and myalgia
bull Vital Sign
ndash BP 13070 mmHg
ndash Pulse 110min
ndash RR 24min
ndash Fever 380 ˚C
ndash Pulse 97
bull Physical exam
ndash Decreased breath sounds and crackles on left basal lobe
bull CBC
ndash Hb149 grdL
ndash WBC 18000
ndash Plt246000 microL
bull RFT and LFTmdashNormal
bull Arterial Blood Gases
ndash pH 738
ndash HCO3 26 mEqlt
ndash pCO2 38 mmH20
ndash pO2 65 mm H2O
bull How can you manage this patient
6
Community Acquired Pneumonia
bull Epidemiology
ndash Overall rate in adultsmdash5-61000 cases
ndash increases with aging
ndash Seasonal variationmdashoccurs more during the winter months
ndash Higher in men
ndash Mortality 2-30
bull lt1 for those not requiring hospitalization
bull Up to 23 mortality during 30-day follow-up among patients who require hospitalization
ndash Streptococcus pneumonia is the most common cause of pneumonia worldwide
7
Community Acquired Pneumonia
0
200
400
600
800
1000
1200
1400
lt5 5 to 17 18-24 25-44 45-64 gt65
898
1071
83
1171 1207
684
of cases
0
10
20
30
40
50
60
70
80
lt4 5 to 14 15-24 25-44 45-64 gt65
0 0 0 2
57
749
of deaths in 1000s
Mortality
Community Acquired Pneumonia
9
Age-specific Rates of Hospital Admission by Pathogen
Marston BJ Plouffe JF File TM Jr Hackman BA Salstrom SJ Lipman HB Kolczak MS Breiman RF Incidence of community-acquired pneumonia requiring hospitalization Results of a population-based active surveillance Study in Ohio The Community-Based Pneumonia Incidence Study Group Arch Intern Med 1997157(15)1709-18
10
CAP ndash Pathogenesis
bull Inhalation aspiration and hematogenous spread are the 3 main mechanisms by which bacteria reaches the lungs
Inhalation
Aspiration
Hematogenous
11
Pathogenesis
bull Primary inhalation when organisms bypass normal respiratory defense mechanisms or when the Pt inhales aerobic GN organisms that colonize the upper respiratory tract or respiratory support equipment
bull Aspiration occurs when the patient aspirates colonized upper respiratory tract secretions
ndash Stomach reservoir of GNR that can ascend colonizing the respiratory tract
bull Hematogenous originate from a distant source and reach the lungs via the blood stream
12
bull Risk Factors for pneumonia ndash age ndash smoking ndash asthma ndash immunosuppression ndash institutionalization ndash COPD ndash PVD ndash Dementia ndash HIVAIDS
Community Acquired Pneumonia
13
bull Risk Factors in Patients Requiring Hospitalization ndash older unemployed
ndash common cold in the previous year
ndash asthma COPD steroid or bronchodilator use
ndash Chronic disease
ndash amount of smoking
Farr BM Respir Med 200094954-63
Community Acquired Pneumonia
14
bull Risk Factors for Mortality
ndash age
ndash bacteremia (for S pneumoniae)
ndash extent of radiographic changes
ndash degree of immunosuppression
ndash amount of alcohol
Community Acquired Pneumonia
15
ndash S pneumoniae 20-60
ndash H influenzae 3-10
ndash Chlamydia pneumoniae 4-6
ndash Mycoplasma pneumonaie 1-6
Community Acquired Pneumonia
ndash Legionella spp 2-8
ndash S aureus 3-5
ndash Gram negative bacilli 3-5
ndash Viruses 2-13
40-60 - NO CAUSE IDENTIFIED
2-5 - TWO OR MORE CAUSES
Microbiology
Bartlett NEJM 19953331618-24
16
Microbial etiology of community-acquired pneumonia in patients who
underwent comprehensive testing
17
Streptococcus pneumonia (Pneumococcus)
Most common cause of CAP About 23 of CAP are due to
Spneumoniae These are gram positive diplococci Typical symptoms (eg malaise
shaking chills fever rusty sputum pleuritic chest pain cough)
Lobar infiltrate on CXR May be immunosuppressed host 25 will have bacteremia ndash serious
effects
18
Risk Factors for Pneumococcal Pneumonia
bull Influenza infection
bull Alcohol abuse
bull Smoking--(x4 fold )
bull COPD and asthma
bull Hyposplenism or splenectomy
bull Immunocompromise---HIV (x50-100 fold ) MM SLE Transplant
bull Others---homeless pregnancy crack cocaine use incarceration
19
64 year old male with insulin dependent diabetes mellitus
He was admitted with bacteremic pneumococcal pneumonia Note the left lower lobe opacity
Pneumococcal pneumonia is the paradigm of classic lobar bacterial pneumonia
20
Complications of pneumococcal pneumonia
21
OTHER BACTERIAL PNEUMONIA
22
Atypical Pneumonia
bull 2 cause (especially in younger population)
bull Commonly associated with milder Sxrsquos subacute onset non-productive cough no focal infiltrate on CXR
bull Mycoplasma younger Pts extra-pulm Sxrsquos (anemia rashes) headache sore throat
bull Chlamydia year round URI Sx sore throat
bull Legionella higher mortality rate water-borne outbreaks hyponatremia diarrhea
23
Mycoplasma pneumonia
24
Mycoplasma pneumonia
25
Pneumocystis jirovecii pneumonia in patient with AIDS
26
Viruses and Pneumonia Pneumonia in the normal host
bull Adults or Children
bull Influenza A and B RSV Adenovirus Para Influenza
Pneumonia in the immuno-compromised
bull Measles HSV CMV HHV-6 Influenza viruses
bull Can cause a primary viral pneumonia Cause partial paralysis of
ldquomucociliary escalatorrdquo - increased risk of secondary bacterial
LRTI Saureus pneumonia is a known complication following
influenza infection
27
Other bacteria bull Anaerobes
ndash Aspiration-prone Pt putrid sputum dental disease
bull Gram negative ndash Klebsiella - alcoholics
ndash Branhamella catarrhalis - sinus disease otitis COPD
ndash H influenza
28
Diagnosis and Management
29
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
5
Case 3
Lab
bull 34 year old male
bull Complaint Fever chest pain cough severe myaljia
bull Hx
ndash Chest pain for 2 days cough for 1 week Hx for upper respiratory infection for 2 weeks ago
ndash Fevermdash4 days
ndash Sputum production
ndash He had complaints of severe myaljia
bull Past medical hx-Non
bull MedicationmdashParacetamol for fever and myalgia
bull Vital Sign
ndash BP 13070 mmHg
ndash Pulse 110min
ndash RR 24min
ndash Fever 380 ˚C
ndash Pulse 97
bull Physical exam
ndash Decreased breath sounds and crackles on left basal lobe
bull CBC
ndash Hb149 grdL
ndash WBC 18000
ndash Plt246000 microL
bull RFT and LFTmdashNormal
bull Arterial Blood Gases
ndash pH 738
ndash HCO3 26 mEqlt
ndash pCO2 38 mmH20
ndash pO2 65 mm H2O
bull How can you manage this patient
6
Community Acquired Pneumonia
bull Epidemiology
ndash Overall rate in adultsmdash5-61000 cases
ndash increases with aging
ndash Seasonal variationmdashoccurs more during the winter months
ndash Higher in men
ndash Mortality 2-30
bull lt1 for those not requiring hospitalization
bull Up to 23 mortality during 30-day follow-up among patients who require hospitalization
ndash Streptococcus pneumonia is the most common cause of pneumonia worldwide
7
Community Acquired Pneumonia
0
200
400
600
800
1000
1200
1400
lt5 5 to 17 18-24 25-44 45-64 gt65
898
1071
83
1171 1207
684
of cases
0
10
20
30
40
50
60
70
80
lt4 5 to 14 15-24 25-44 45-64 gt65
0 0 0 2
57
749
of deaths in 1000s
Mortality
Community Acquired Pneumonia
9
Age-specific Rates of Hospital Admission by Pathogen
Marston BJ Plouffe JF File TM Jr Hackman BA Salstrom SJ Lipman HB Kolczak MS Breiman RF Incidence of community-acquired pneumonia requiring hospitalization Results of a population-based active surveillance Study in Ohio The Community-Based Pneumonia Incidence Study Group Arch Intern Med 1997157(15)1709-18
10
CAP ndash Pathogenesis
bull Inhalation aspiration and hematogenous spread are the 3 main mechanisms by which bacteria reaches the lungs
Inhalation
Aspiration
Hematogenous
11
Pathogenesis
bull Primary inhalation when organisms bypass normal respiratory defense mechanisms or when the Pt inhales aerobic GN organisms that colonize the upper respiratory tract or respiratory support equipment
bull Aspiration occurs when the patient aspirates colonized upper respiratory tract secretions
ndash Stomach reservoir of GNR that can ascend colonizing the respiratory tract
bull Hematogenous originate from a distant source and reach the lungs via the blood stream
12
bull Risk Factors for pneumonia ndash age ndash smoking ndash asthma ndash immunosuppression ndash institutionalization ndash COPD ndash PVD ndash Dementia ndash HIVAIDS
Community Acquired Pneumonia
13
bull Risk Factors in Patients Requiring Hospitalization ndash older unemployed
ndash common cold in the previous year
ndash asthma COPD steroid or bronchodilator use
ndash Chronic disease
ndash amount of smoking
Farr BM Respir Med 200094954-63
Community Acquired Pneumonia
14
bull Risk Factors for Mortality
ndash age
ndash bacteremia (for S pneumoniae)
ndash extent of radiographic changes
ndash degree of immunosuppression
ndash amount of alcohol
Community Acquired Pneumonia
15
ndash S pneumoniae 20-60
ndash H influenzae 3-10
ndash Chlamydia pneumoniae 4-6
ndash Mycoplasma pneumonaie 1-6
Community Acquired Pneumonia
ndash Legionella spp 2-8
ndash S aureus 3-5
ndash Gram negative bacilli 3-5
ndash Viruses 2-13
40-60 - NO CAUSE IDENTIFIED
2-5 - TWO OR MORE CAUSES
Microbiology
Bartlett NEJM 19953331618-24
16
Microbial etiology of community-acquired pneumonia in patients who
underwent comprehensive testing
17
Streptococcus pneumonia (Pneumococcus)
Most common cause of CAP About 23 of CAP are due to
Spneumoniae These are gram positive diplococci Typical symptoms (eg malaise
shaking chills fever rusty sputum pleuritic chest pain cough)
Lobar infiltrate on CXR May be immunosuppressed host 25 will have bacteremia ndash serious
effects
18
Risk Factors for Pneumococcal Pneumonia
bull Influenza infection
bull Alcohol abuse
bull Smoking--(x4 fold )
bull COPD and asthma
bull Hyposplenism or splenectomy
bull Immunocompromise---HIV (x50-100 fold ) MM SLE Transplant
bull Others---homeless pregnancy crack cocaine use incarceration
19
64 year old male with insulin dependent diabetes mellitus
He was admitted with bacteremic pneumococcal pneumonia Note the left lower lobe opacity
Pneumococcal pneumonia is the paradigm of classic lobar bacterial pneumonia
20
Complications of pneumococcal pneumonia
21
OTHER BACTERIAL PNEUMONIA
22
Atypical Pneumonia
bull 2 cause (especially in younger population)
bull Commonly associated with milder Sxrsquos subacute onset non-productive cough no focal infiltrate on CXR
bull Mycoplasma younger Pts extra-pulm Sxrsquos (anemia rashes) headache sore throat
bull Chlamydia year round URI Sx sore throat
bull Legionella higher mortality rate water-borne outbreaks hyponatremia diarrhea
23
Mycoplasma pneumonia
24
Mycoplasma pneumonia
25
Pneumocystis jirovecii pneumonia in patient with AIDS
26
Viruses and Pneumonia Pneumonia in the normal host
bull Adults or Children
bull Influenza A and B RSV Adenovirus Para Influenza
Pneumonia in the immuno-compromised
bull Measles HSV CMV HHV-6 Influenza viruses
bull Can cause a primary viral pneumonia Cause partial paralysis of
ldquomucociliary escalatorrdquo - increased risk of secondary bacterial
LRTI Saureus pneumonia is a known complication following
influenza infection
27
Other bacteria bull Anaerobes
ndash Aspiration-prone Pt putrid sputum dental disease
bull Gram negative ndash Klebsiella - alcoholics
ndash Branhamella catarrhalis - sinus disease otitis COPD
ndash H influenza
28
Diagnosis and Management
29
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
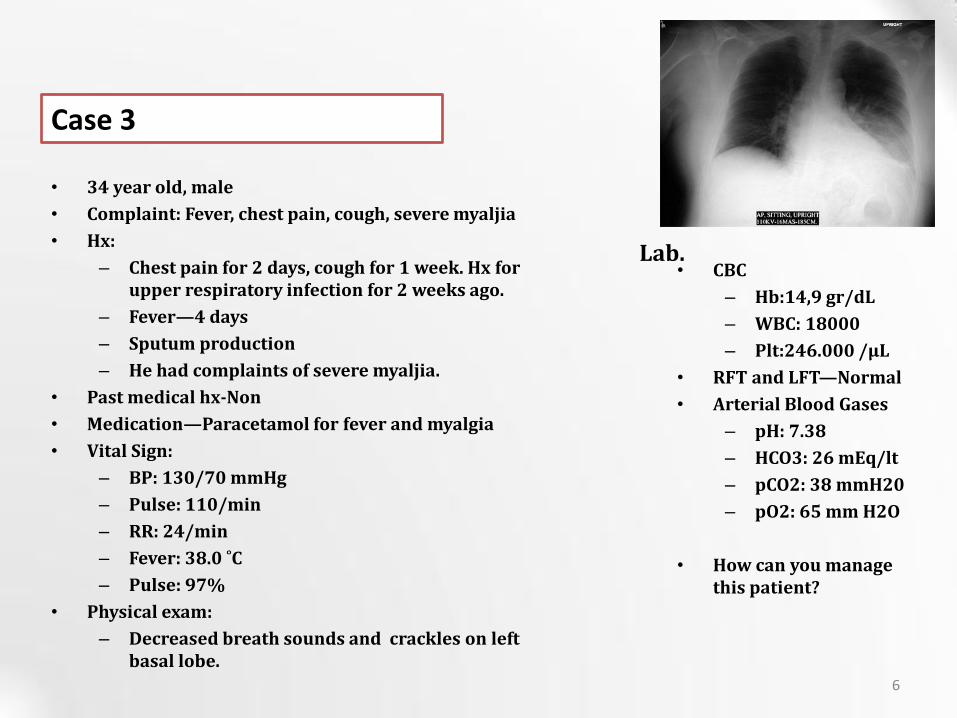
Case 3
Lab
bull 34 year old male
bull Complaint Fever chest pain cough severe myaljia
bull Hx
ndash Chest pain for 2 days cough for 1 week Hx for upper respiratory infection for 2 weeks ago
ndash Fevermdash4 days
ndash Sputum production
ndash He had complaints of severe myaljia
bull Past medical hx-Non
bull MedicationmdashParacetamol for fever and myalgia
bull Vital Sign
ndash BP 13070 mmHg
ndash Pulse 110min
ndash RR 24min
ndash Fever 380 ˚C
ndash Pulse 97
bull Physical exam
ndash Decreased breath sounds and crackles on left basal lobe
bull CBC
ndash Hb149 grdL
ndash WBC 18000
ndash Plt246000 microL
bull RFT and LFTmdashNormal
bull Arterial Blood Gases
ndash pH 738
ndash HCO3 26 mEqlt
ndash pCO2 38 mmH20
ndash pO2 65 mm H2O
bull How can you manage this patient
6
Community Acquired Pneumonia
bull Epidemiology
ndash Overall rate in adultsmdash5-61000 cases
ndash increases with aging
ndash Seasonal variationmdashoccurs more during the winter months
ndash Higher in men
ndash Mortality 2-30
bull lt1 for those not requiring hospitalization
bull Up to 23 mortality during 30-day follow-up among patients who require hospitalization
ndash Streptococcus pneumonia is the most common cause of pneumonia worldwide
7
Community Acquired Pneumonia
0
200
400
600
800
1000
1200
1400
lt5 5 to 17 18-24 25-44 45-64 gt65
898
1071
83
1171 1207
684
of cases
0
10
20
30
40
50
60
70
80
lt4 5 to 14 15-24 25-44 45-64 gt65
0 0 0 2
57
749
of deaths in 1000s
Mortality
Community Acquired Pneumonia
9
Age-specific Rates of Hospital Admission by Pathogen
Marston BJ Plouffe JF File TM Jr Hackman BA Salstrom SJ Lipman HB Kolczak MS Breiman RF Incidence of community-acquired pneumonia requiring hospitalization Results of a population-based active surveillance Study in Ohio The Community-Based Pneumonia Incidence Study Group Arch Intern Med 1997157(15)1709-18
10
CAP ndash Pathogenesis
bull Inhalation aspiration and hematogenous spread are the 3 main mechanisms by which bacteria reaches the lungs
Inhalation
Aspiration
Hematogenous
11
Pathogenesis
bull Primary inhalation when organisms bypass normal respiratory defense mechanisms or when the Pt inhales aerobic GN organisms that colonize the upper respiratory tract or respiratory support equipment
bull Aspiration occurs when the patient aspirates colonized upper respiratory tract secretions
ndash Stomach reservoir of GNR that can ascend colonizing the respiratory tract
bull Hematogenous originate from a distant source and reach the lungs via the blood stream
12
bull Risk Factors for pneumonia ndash age ndash smoking ndash asthma ndash immunosuppression ndash institutionalization ndash COPD ndash PVD ndash Dementia ndash HIVAIDS
Community Acquired Pneumonia
13
bull Risk Factors in Patients Requiring Hospitalization ndash older unemployed
ndash common cold in the previous year
ndash asthma COPD steroid or bronchodilator use
ndash Chronic disease
ndash amount of smoking
Farr BM Respir Med 200094954-63
Community Acquired Pneumonia
14
bull Risk Factors for Mortality
ndash age
ndash bacteremia (for S pneumoniae)
ndash extent of radiographic changes
ndash degree of immunosuppression
ndash amount of alcohol
Community Acquired Pneumonia
15
ndash S pneumoniae 20-60
ndash H influenzae 3-10
ndash Chlamydia pneumoniae 4-6
ndash Mycoplasma pneumonaie 1-6
Community Acquired Pneumonia
ndash Legionella spp 2-8
ndash S aureus 3-5
ndash Gram negative bacilli 3-5
ndash Viruses 2-13
40-60 - NO CAUSE IDENTIFIED
2-5 - TWO OR MORE CAUSES
Microbiology
Bartlett NEJM 19953331618-24
16
Microbial etiology of community-acquired pneumonia in patients who
underwent comprehensive testing
17
Streptococcus pneumonia (Pneumococcus)
Most common cause of CAP About 23 of CAP are due to
Spneumoniae These are gram positive diplococci Typical symptoms (eg malaise
shaking chills fever rusty sputum pleuritic chest pain cough)
Lobar infiltrate on CXR May be immunosuppressed host 25 will have bacteremia ndash serious
effects
18
Risk Factors for Pneumococcal Pneumonia
bull Influenza infection
bull Alcohol abuse
bull Smoking--(x4 fold )
bull COPD and asthma
bull Hyposplenism or splenectomy
bull Immunocompromise---HIV (x50-100 fold ) MM SLE Transplant
bull Others---homeless pregnancy crack cocaine use incarceration
19
64 year old male with insulin dependent diabetes mellitus
He was admitted with bacteremic pneumococcal pneumonia Note the left lower lobe opacity
Pneumococcal pneumonia is the paradigm of classic lobar bacterial pneumonia
20
Complications of pneumococcal pneumonia
21
OTHER BACTERIAL PNEUMONIA
22
Atypical Pneumonia
bull 2 cause (especially in younger population)
bull Commonly associated with milder Sxrsquos subacute onset non-productive cough no focal infiltrate on CXR
bull Mycoplasma younger Pts extra-pulm Sxrsquos (anemia rashes) headache sore throat
bull Chlamydia year round URI Sx sore throat
bull Legionella higher mortality rate water-borne outbreaks hyponatremia diarrhea
23
Mycoplasma pneumonia
24
Mycoplasma pneumonia
25
Pneumocystis jirovecii pneumonia in patient with AIDS
26
Viruses and Pneumonia Pneumonia in the normal host
bull Adults or Children
bull Influenza A and B RSV Adenovirus Para Influenza
Pneumonia in the immuno-compromised
bull Measles HSV CMV HHV-6 Influenza viruses
bull Can cause a primary viral pneumonia Cause partial paralysis of
ldquomucociliary escalatorrdquo - increased risk of secondary bacterial
LRTI Saureus pneumonia is a known complication following
influenza infection
27
Other bacteria bull Anaerobes
ndash Aspiration-prone Pt putrid sputum dental disease
bull Gram negative ndash Klebsiella - alcoholics
ndash Branhamella catarrhalis - sinus disease otitis COPD
ndash H influenza
28
Diagnosis and Management
29
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
Community Acquired Pneumonia
bull Epidemiology
ndash Overall rate in adultsmdash5-61000 cases
ndash increases with aging
ndash Seasonal variationmdashoccurs more during the winter months
ndash Higher in men
ndash Mortality 2-30
bull lt1 for those not requiring hospitalization
bull Up to 23 mortality during 30-day follow-up among patients who require hospitalization
ndash Streptococcus pneumonia is the most common cause of pneumonia worldwide
7
Community Acquired Pneumonia
0
200
400
600
800
1000
1200
1400
lt5 5 to 17 18-24 25-44 45-64 gt65
898
1071
83
1171 1207
684
of cases
0
10
20
30
40
50
60
70
80
lt4 5 to 14 15-24 25-44 45-64 gt65
0 0 0 2
57
749
of deaths in 1000s
Mortality
Community Acquired Pneumonia
9
Age-specific Rates of Hospital Admission by Pathogen
Marston BJ Plouffe JF File TM Jr Hackman BA Salstrom SJ Lipman HB Kolczak MS Breiman RF Incidence of community-acquired pneumonia requiring hospitalization Results of a population-based active surveillance Study in Ohio The Community-Based Pneumonia Incidence Study Group Arch Intern Med 1997157(15)1709-18
10
CAP ndash Pathogenesis
bull Inhalation aspiration and hematogenous spread are the 3 main mechanisms by which bacteria reaches the lungs
Inhalation
Aspiration
Hematogenous
11
Pathogenesis
bull Primary inhalation when organisms bypass normal respiratory defense mechanisms or when the Pt inhales aerobic GN organisms that colonize the upper respiratory tract or respiratory support equipment
bull Aspiration occurs when the patient aspirates colonized upper respiratory tract secretions
ndash Stomach reservoir of GNR that can ascend colonizing the respiratory tract
bull Hematogenous originate from a distant source and reach the lungs via the blood stream
12
bull Risk Factors for pneumonia ndash age ndash smoking ndash asthma ndash immunosuppression ndash institutionalization ndash COPD ndash PVD ndash Dementia ndash HIVAIDS
Community Acquired Pneumonia
13
bull Risk Factors in Patients Requiring Hospitalization ndash older unemployed
ndash common cold in the previous year
ndash asthma COPD steroid or bronchodilator use
ndash Chronic disease
ndash amount of smoking
Farr BM Respir Med 200094954-63
Community Acquired Pneumonia
14
bull Risk Factors for Mortality
ndash age
ndash bacteremia (for S pneumoniae)
ndash extent of radiographic changes
ndash degree of immunosuppression
ndash amount of alcohol
Community Acquired Pneumonia
15
ndash S pneumoniae 20-60
ndash H influenzae 3-10
ndash Chlamydia pneumoniae 4-6
ndash Mycoplasma pneumonaie 1-6
Community Acquired Pneumonia
ndash Legionella spp 2-8
ndash S aureus 3-5
ndash Gram negative bacilli 3-5
ndash Viruses 2-13
40-60 - NO CAUSE IDENTIFIED
2-5 - TWO OR MORE CAUSES
Microbiology
Bartlett NEJM 19953331618-24
16
Microbial etiology of community-acquired pneumonia in patients who
underwent comprehensive testing
17
Streptococcus pneumonia (Pneumococcus)
Most common cause of CAP About 23 of CAP are due to
Spneumoniae These are gram positive diplococci Typical symptoms (eg malaise
shaking chills fever rusty sputum pleuritic chest pain cough)
Lobar infiltrate on CXR May be immunosuppressed host 25 will have bacteremia ndash serious
effects
18
Risk Factors for Pneumococcal Pneumonia
bull Influenza infection
bull Alcohol abuse
bull Smoking--(x4 fold )
bull COPD and asthma
bull Hyposplenism or splenectomy
bull Immunocompromise---HIV (x50-100 fold ) MM SLE Transplant
bull Others---homeless pregnancy crack cocaine use incarceration
19
64 year old male with insulin dependent diabetes mellitus
He was admitted with bacteremic pneumococcal pneumonia Note the left lower lobe opacity
Pneumococcal pneumonia is the paradigm of classic lobar bacterial pneumonia
20
Complications of pneumococcal pneumonia
21
OTHER BACTERIAL PNEUMONIA
22
Atypical Pneumonia
bull 2 cause (especially in younger population)
bull Commonly associated with milder Sxrsquos subacute onset non-productive cough no focal infiltrate on CXR
bull Mycoplasma younger Pts extra-pulm Sxrsquos (anemia rashes) headache sore throat
bull Chlamydia year round URI Sx sore throat
bull Legionella higher mortality rate water-borne outbreaks hyponatremia diarrhea
23
Mycoplasma pneumonia
24
Mycoplasma pneumonia
25
Pneumocystis jirovecii pneumonia in patient with AIDS
26
Viruses and Pneumonia Pneumonia in the normal host
bull Adults or Children
bull Influenza A and B RSV Adenovirus Para Influenza
Pneumonia in the immuno-compromised
bull Measles HSV CMV HHV-6 Influenza viruses
bull Can cause a primary viral pneumonia Cause partial paralysis of
ldquomucociliary escalatorrdquo - increased risk of secondary bacterial
LRTI Saureus pneumonia is a known complication following
influenza infection
27
Other bacteria bull Anaerobes
ndash Aspiration-prone Pt putrid sputum dental disease
bull Gram negative ndash Klebsiella - alcoholics
ndash Branhamella catarrhalis - sinus disease otitis COPD
ndash H influenza
28
Diagnosis and Management
29
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
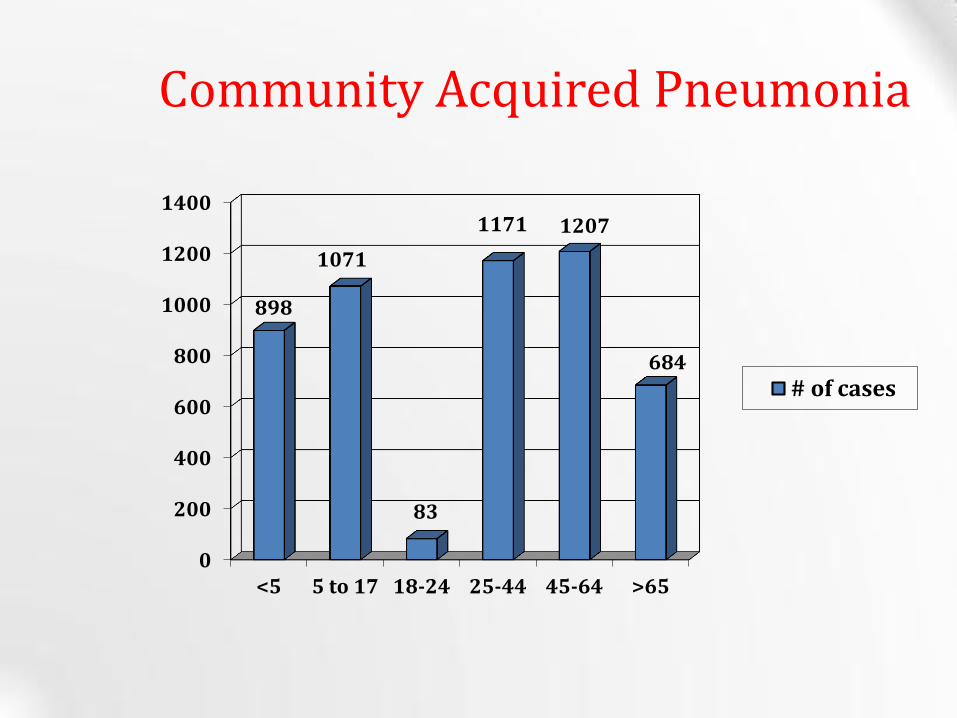
Community Acquired Pneumonia
0
200
400
600
800
1000
1200
1400
lt5 5 to 17 18-24 25-44 45-64 gt65
898
1071
83
1171 1207
684
of cases
0
10
20
30
40
50
60
70
80
lt4 5 to 14 15-24 25-44 45-64 gt65
0 0 0 2
57
749
of deaths in 1000s
Mortality
Community Acquired Pneumonia
9
Age-specific Rates of Hospital Admission by Pathogen
Marston BJ Plouffe JF File TM Jr Hackman BA Salstrom SJ Lipman HB Kolczak MS Breiman RF Incidence of community-acquired pneumonia requiring hospitalization Results of a population-based active surveillance Study in Ohio The Community-Based Pneumonia Incidence Study Group Arch Intern Med 1997157(15)1709-18
10
CAP ndash Pathogenesis
bull Inhalation aspiration and hematogenous spread are the 3 main mechanisms by which bacteria reaches the lungs
Inhalation
Aspiration
Hematogenous
11
Pathogenesis
bull Primary inhalation when organisms bypass normal respiratory defense mechanisms or when the Pt inhales aerobic GN organisms that colonize the upper respiratory tract or respiratory support equipment
bull Aspiration occurs when the patient aspirates colonized upper respiratory tract secretions
ndash Stomach reservoir of GNR that can ascend colonizing the respiratory tract
bull Hematogenous originate from a distant source and reach the lungs via the blood stream
12
bull Risk Factors for pneumonia ndash age ndash smoking ndash asthma ndash immunosuppression ndash institutionalization ndash COPD ndash PVD ndash Dementia ndash HIVAIDS
Community Acquired Pneumonia
13
bull Risk Factors in Patients Requiring Hospitalization ndash older unemployed
ndash common cold in the previous year
ndash asthma COPD steroid or bronchodilator use
ndash Chronic disease
ndash amount of smoking
Farr BM Respir Med 200094954-63
Community Acquired Pneumonia
14
bull Risk Factors for Mortality
ndash age
ndash bacteremia (for S pneumoniae)
ndash extent of radiographic changes
ndash degree of immunosuppression
ndash amount of alcohol
Community Acquired Pneumonia
15
ndash S pneumoniae 20-60
ndash H influenzae 3-10
ndash Chlamydia pneumoniae 4-6
ndash Mycoplasma pneumonaie 1-6
Community Acquired Pneumonia
ndash Legionella spp 2-8
ndash S aureus 3-5
ndash Gram negative bacilli 3-5
ndash Viruses 2-13
40-60 - NO CAUSE IDENTIFIED
2-5 - TWO OR MORE CAUSES
Microbiology
Bartlett NEJM 19953331618-24
16
Microbial etiology of community-acquired pneumonia in patients who
underwent comprehensive testing
17
Streptococcus pneumonia (Pneumococcus)
Most common cause of CAP About 23 of CAP are due to
Spneumoniae These are gram positive diplococci Typical symptoms (eg malaise
shaking chills fever rusty sputum pleuritic chest pain cough)
Lobar infiltrate on CXR May be immunosuppressed host 25 will have bacteremia ndash serious
effects
18
Risk Factors for Pneumococcal Pneumonia
bull Influenza infection
bull Alcohol abuse
bull Smoking--(x4 fold )
bull COPD and asthma
bull Hyposplenism or splenectomy
bull Immunocompromise---HIV (x50-100 fold ) MM SLE Transplant
bull Others---homeless pregnancy crack cocaine use incarceration
19
64 year old male with insulin dependent diabetes mellitus
He was admitted with bacteremic pneumococcal pneumonia Note the left lower lobe opacity
Pneumococcal pneumonia is the paradigm of classic lobar bacterial pneumonia
20
Complications of pneumococcal pneumonia
21
OTHER BACTERIAL PNEUMONIA
22
Atypical Pneumonia
bull 2 cause (especially in younger population)
bull Commonly associated with milder Sxrsquos subacute onset non-productive cough no focal infiltrate on CXR
bull Mycoplasma younger Pts extra-pulm Sxrsquos (anemia rashes) headache sore throat
bull Chlamydia year round URI Sx sore throat
bull Legionella higher mortality rate water-borne outbreaks hyponatremia diarrhea
23
Mycoplasma pneumonia
24
Mycoplasma pneumonia
25
Pneumocystis jirovecii pneumonia in patient with AIDS
26
Viruses and Pneumonia Pneumonia in the normal host
bull Adults or Children
bull Influenza A and B RSV Adenovirus Para Influenza
Pneumonia in the immuno-compromised
bull Measles HSV CMV HHV-6 Influenza viruses
bull Can cause a primary viral pneumonia Cause partial paralysis of
ldquomucociliary escalatorrdquo - increased risk of secondary bacterial
LRTI Saureus pneumonia is a known complication following
influenza infection
27
Other bacteria bull Anaerobes
ndash Aspiration-prone Pt putrid sputum dental disease
bull Gram negative ndash Klebsiella - alcoholics
ndash Branhamella catarrhalis - sinus disease otitis COPD
ndash H influenza
28
Diagnosis and Management
29
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
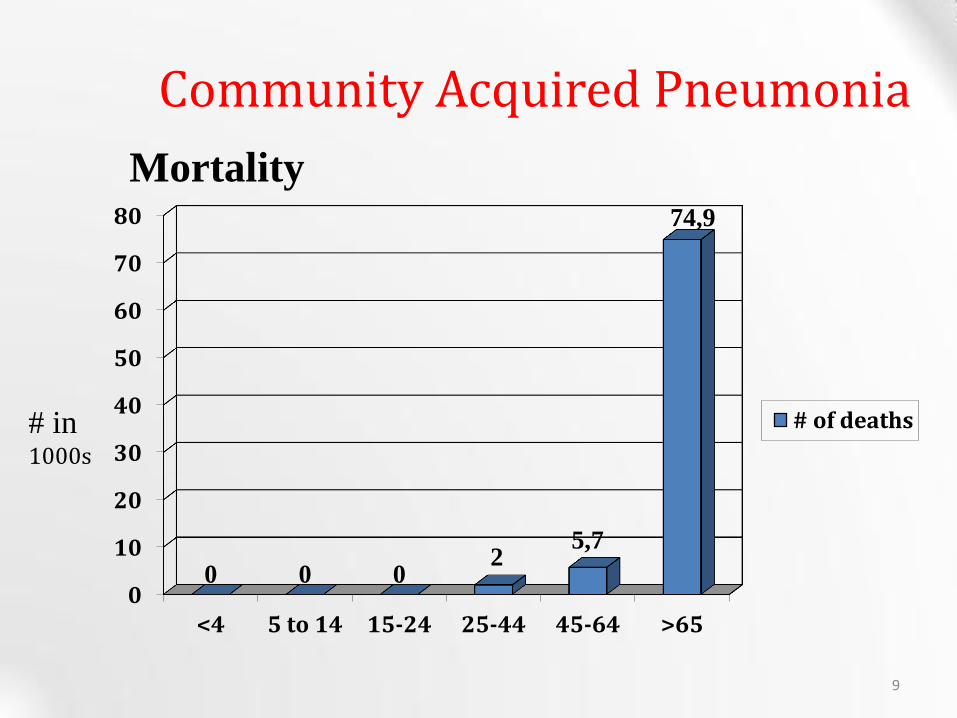
0
10
20
30
40
50
60
70
80
lt4 5 to 14 15-24 25-44 45-64 gt65
0 0 0 2
57
749
of deaths in 1000s
Mortality
Community Acquired Pneumonia
9
Age-specific Rates of Hospital Admission by Pathogen
Marston BJ Plouffe JF File TM Jr Hackman BA Salstrom SJ Lipman HB Kolczak MS Breiman RF Incidence of community-acquired pneumonia requiring hospitalization Results of a population-based active surveillance Study in Ohio The Community-Based Pneumonia Incidence Study Group Arch Intern Med 1997157(15)1709-18
10
CAP ndash Pathogenesis
bull Inhalation aspiration and hematogenous spread are the 3 main mechanisms by which bacteria reaches the lungs
Inhalation
Aspiration
Hematogenous
11
Pathogenesis
bull Primary inhalation when organisms bypass normal respiratory defense mechanisms or when the Pt inhales aerobic GN organisms that colonize the upper respiratory tract or respiratory support equipment
bull Aspiration occurs when the patient aspirates colonized upper respiratory tract secretions
ndash Stomach reservoir of GNR that can ascend colonizing the respiratory tract
bull Hematogenous originate from a distant source and reach the lungs via the blood stream
12
bull Risk Factors for pneumonia ndash age ndash smoking ndash asthma ndash immunosuppression ndash institutionalization ndash COPD ndash PVD ndash Dementia ndash HIVAIDS
Community Acquired Pneumonia
13
bull Risk Factors in Patients Requiring Hospitalization ndash older unemployed
ndash common cold in the previous year
ndash asthma COPD steroid or bronchodilator use
ndash Chronic disease
ndash amount of smoking
Farr BM Respir Med 200094954-63
Community Acquired Pneumonia
14
bull Risk Factors for Mortality
ndash age
ndash bacteremia (for S pneumoniae)
ndash extent of radiographic changes
ndash degree of immunosuppression
ndash amount of alcohol
Community Acquired Pneumonia
15
ndash S pneumoniae 20-60
ndash H influenzae 3-10
ndash Chlamydia pneumoniae 4-6
ndash Mycoplasma pneumonaie 1-6
Community Acquired Pneumonia
ndash Legionella spp 2-8
ndash S aureus 3-5
ndash Gram negative bacilli 3-5
ndash Viruses 2-13
40-60 - NO CAUSE IDENTIFIED
2-5 - TWO OR MORE CAUSES
Microbiology
Bartlett NEJM 19953331618-24
16
Microbial etiology of community-acquired pneumonia in patients who
underwent comprehensive testing
17
Streptococcus pneumonia (Pneumococcus)
Most common cause of CAP About 23 of CAP are due to
Spneumoniae These are gram positive diplococci Typical symptoms (eg malaise
shaking chills fever rusty sputum pleuritic chest pain cough)
Lobar infiltrate on CXR May be immunosuppressed host 25 will have bacteremia ndash serious
effects
18
Risk Factors for Pneumococcal Pneumonia
bull Influenza infection
bull Alcohol abuse
bull Smoking--(x4 fold )
bull COPD and asthma
bull Hyposplenism or splenectomy
bull Immunocompromise---HIV (x50-100 fold ) MM SLE Transplant
bull Others---homeless pregnancy crack cocaine use incarceration
19
64 year old male with insulin dependent diabetes mellitus
He was admitted with bacteremic pneumococcal pneumonia Note the left lower lobe opacity
Pneumococcal pneumonia is the paradigm of classic lobar bacterial pneumonia
20
Complications of pneumococcal pneumonia
21
OTHER BACTERIAL PNEUMONIA
22
Atypical Pneumonia
bull 2 cause (especially in younger population)
bull Commonly associated with milder Sxrsquos subacute onset non-productive cough no focal infiltrate on CXR
bull Mycoplasma younger Pts extra-pulm Sxrsquos (anemia rashes) headache sore throat
bull Chlamydia year round URI Sx sore throat
bull Legionella higher mortality rate water-borne outbreaks hyponatremia diarrhea
23
Mycoplasma pneumonia
24
Mycoplasma pneumonia
25
Pneumocystis jirovecii pneumonia in patient with AIDS
26
Viruses and Pneumonia Pneumonia in the normal host
bull Adults or Children
bull Influenza A and B RSV Adenovirus Para Influenza
Pneumonia in the immuno-compromised
bull Measles HSV CMV HHV-6 Influenza viruses
bull Can cause a primary viral pneumonia Cause partial paralysis of
ldquomucociliary escalatorrdquo - increased risk of secondary bacterial
LRTI Saureus pneumonia is a known complication following
influenza infection
27
Other bacteria bull Anaerobes
ndash Aspiration-prone Pt putrid sputum dental disease
bull Gram negative ndash Klebsiella - alcoholics
ndash Branhamella catarrhalis - sinus disease otitis COPD
ndash H influenza
28
Diagnosis and Management
29
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
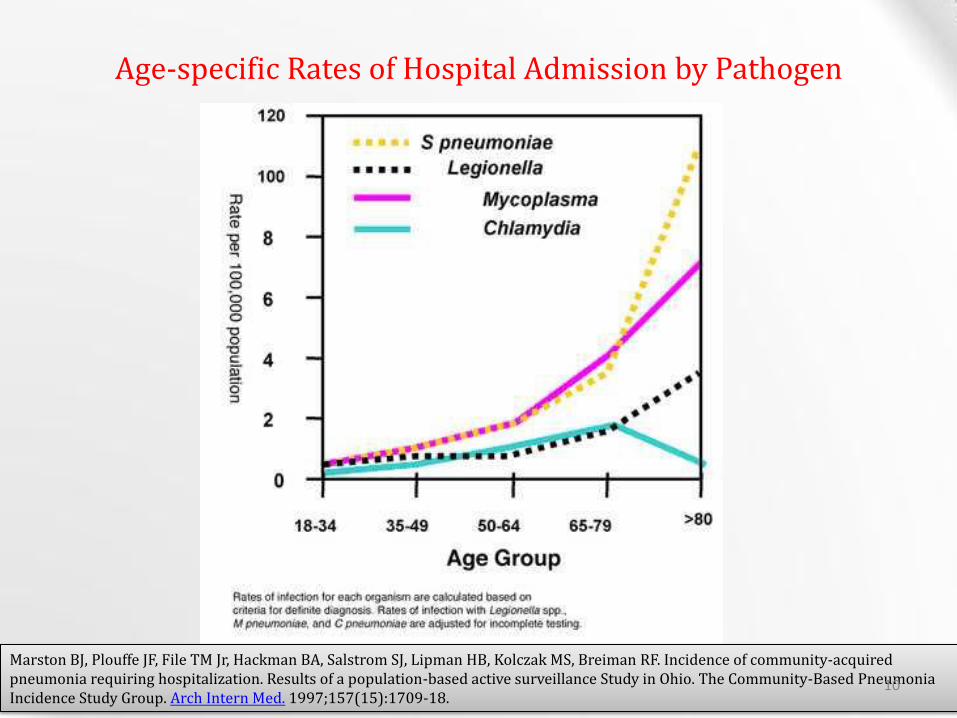
Age-specific Rates of Hospital Admission by Pathogen
Marston BJ Plouffe JF File TM Jr Hackman BA Salstrom SJ Lipman HB Kolczak MS Breiman RF Incidence of community-acquired pneumonia requiring hospitalization Results of a population-based active surveillance Study in Ohio The Community-Based Pneumonia Incidence Study Group Arch Intern Med 1997157(15)1709-18
10
CAP ndash Pathogenesis
bull Inhalation aspiration and hematogenous spread are the 3 main mechanisms by which bacteria reaches the lungs
Inhalation
Aspiration
Hematogenous
11
Pathogenesis
bull Primary inhalation when organisms bypass normal respiratory defense mechanisms or when the Pt inhales aerobic GN organisms that colonize the upper respiratory tract or respiratory support equipment
bull Aspiration occurs when the patient aspirates colonized upper respiratory tract secretions
ndash Stomach reservoir of GNR that can ascend colonizing the respiratory tract
bull Hematogenous originate from a distant source and reach the lungs via the blood stream
12
bull Risk Factors for pneumonia ndash age ndash smoking ndash asthma ndash immunosuppression ndash institutionalization ndash COPD ndash PVD ndash Dementia ndash HIVAIDS
Community Acquired Pneumonia
13
bull Risk Factors in Patients Requiring Hospitalization ndash older unemployed
ndash common cold in the previous year
ndash asthma COPD steroid or bronchodilator use
ndash Chronic disease
ndash amount of smoking
Farr BM Respir Med 200094954-63
Community Acquired Pneumonia
14
bull Risk Factors for Mortality
ndash age
ndash bacteremia (for S pneumoniae)
ndash extent of radiographic changes
ndash degree of immunosuppression
ndash amount of alcohol
Community Acquired Pneumonia
15
ndash S pneumoniae 20-60
ndash H influenzae 3-10
ndash Chlamydia pneumoniae 4-6
ndash Mycoplasma pneumonaie 1-6
Community Acquired Pneumonia
ndash Legionella spp 2-8
ndash S aureus 3-5
ndash Gram negative bacilli 3-5
ndash Viruses 2-13
40-60 - NO CAUSE IDENTIFIED
2-5 - TWO OR MORE CAUSES
Microbiology
Bartlett NEJM 19953331618-24
16
Microbial etiology of community-acquired pneumonia in patients who
underwent comprehensive testing
17
Streptococcus pneumonia (Pneumococcus)
Most common cause of CAP About 23 of CAP are due to
Spneumoniae These are gram positive diplococci Typical symptoms (eg malaise
shaking chills fever rusty sputum pleuritic chest pain cough)
Lobar infiltrate on CXR May be immunosuppressed host 25 will have bacteremia ndash serious
effects
18
Risk Factors for Pneumococcal Pneumonia
bull Influenza infection
bull Alcohol abuse
bull Smoking--(x4 fold )
bull COPD and asthma
bull Hyposplenism or splenectomy
bull Immunocompromise---HIV (x50-100 fold ) MM SLE Transplant
bull Others---homeless pregnancy crack cocaine use incarceration
19
64 year old male with insulin dependent diabetes mellitus
He was admitted with bacteremic pneumococcal pneumonia Note the left lower lobe opacity
Pneumococcal pneumonia is the paradigm of classic lobar bacterial pneumonia
20
Complications of pneumococcal pneumonia
21
OTHER BACTERIAL PNEUMONIA
22
Atypical Pneumonia
bull 2 cause (especially in younger population)
bull Commonly associated with milder Sxrsquos subacute onset non-productive cough no focal infiltrate on CXR
bull Mycoplasma younger Pts extra-pulm Sxrsquos (anemia rashes) headache sore throat
bull Chlamydia year round URI Sx sore throat
bull Legionella higher mortality rate water-borne outbreaks hyponatremia diarrhea
23
Mycoplasma pneumonia
24
Mycoplasma pneumonia
25
Pneumocystis jirovecii pneumonia in patient with AIDS
26
Viruses and Pneumonia Pneumonia in the normal host
bull Adults or Children
bull Influenza A and B RSV Adenovirus Para Influenza
Pneumonia in the immuno-compromised
bull Measles HSV CMV HHV-6 Influenza viruses
bull Can cause a primary viral pneumonia Cause partial paralysis of
ldquomucociliary escalatorrdquo - increased risk of secondary bacterial
LRTI Saureus pneumonia is a known complication following
influenza infection
27
Other bacteria bull Anaerobes
ndash Aspiration-prone Pt putrid sputum dental disease
bull Gram negative ndash Klebsiella - alcoholics
ndash Branhamella catarrhalis - sinus disease otitis COPD
ndash H influenza
28
Diagnosis and Management
29
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60

CAP ndash Pathogenesis
bull Inhalation aspiration and hematogenous spread are the 3 main mechanisms by which bacteria reaches the lungs
Inhalation
Aspiration
Hematogenous
11
Pathogenesis
bull Primary inhalation when organisms bypass normal respiratory defense mechanisms or when the Pt inhales aerobic GN organisms that colonize the upper respiratory tract or respiratory support equipment
bull Aspiration occurs when the patient aspirates colonized upper respiratory tract secretions
ndash Stomach reservoir of GNR that can ascend colonizing the respiratory tract
bull Hematogenous originate from a distant source and reach the lungs via the blood stream
12
bull Risk Factors for pneumonia ndash age ndash smoking ndash asthma ndash immunosuppression ndash institutionalization ndash COPD ndash PVD ndash Dementia ndash HIVAIDS
Community Acquired Pneumonia
13
bull Risk Factors in Patients Requiring Hospitalization ndash older unemployed
ndash common cold in the previous year
ndash asthma COPD steroid or bronchodilator use
ndash Chronic disease
ndash amount of smoking
Farr BM Respir Med 200094954-63
Community Acquired Pneumonia
14
bull Risk Factors for Mortality
ndash age
ndash bacteremia (for S pneumoniae)
ndash extent of radiographic changes
ndash degree of immunosuppression
ndash amount of alcohol
Community Acquired Pneumonia
15
ndash S pneumoniae 20-60
ndash H influenzae 3-10
ndash Chlamydia pneumoniae 4-6
ndash Mycoplasma pneumonaie 1-6
Community Acquired Pneumonia
ndash Legionella spp 2-8
ndash S aureus 3-5
ndash Gram negative bacilli 3-5
ndash Viruses 2-13
40-60 - NO CAUSE IDENTIFIED
2-5 - TWO OR MORE CAUSES
Microbiology
Bartlett NEJM 19953331618-24
16
Microbial etiology of community-acquired pneumonia in patients who
underwent comprehensive testing
17
Streptococcus pneumonia (Pneumococcus)
Most common cause of CAP About 23 of CAP are due to
Spneumoniae These are gram positive diplococci Typical symptoms (eg malaise
shaking chills fever rusty sputum pleuritic chest pain cough)
Lobar infiltrate on CXR May be immunosuppressed host 25 will have bacteremia ndash serious
effects
18
Risk Factors for Pneumococcal Pneumonia
bull Influenza infection
bull Alcohol abuse
bull Smoking--(x4 fold )
bull COPD and asthma
bull Hyposplenism or splenectomy
bull Immunocompromise---HIV (x50-100 fold ) MM SLE Transplant
bull Others---homeless pregnancy crack cocaine use incarceration
19
64 year old male with insulin dependent diabetes mellitus
He was admitted with bacteremic pneumococcal pneumonia Note the left lower lobe opacity
Pneumococcal pneumonia is the paradigm of classic lobar bacterial pneumonia
20
Complications of pneumococcal pneumonia
21
OTHER BACTERIAL PNEUMONIA
22
Atypical Pneumonia
bull 2 cause (especially in younger population)
bull Commonly associated with milder Sxrsquos subacute onset non-productive cough no focal infiltrate on CXR
bull Mycoplasma younger Pts extra-pulm Sxrsquos (anemia rashes) headache sore throat
bull Chlamydia year round URI Sx sore throat
bull Legionella higher mortality rate water-borne outbreaks hyponatremia diarrhea
23
Mycoplasma pneumonia
24
Mycoplasma pneumonia
25
Pneumocystis jirovecii pneumonia in patient with AIDS
26
Viruses and Pneumonia Pneumonia in the normal host
bull Adults or Children
bull Influenza A and B RSV Adenovirus Para Influenza
Pneumonia in the immuno-compromised
bull Measles HSV CMV HHV-6 Influenza viruses
bull Can cause a primary viral pneumonia Cause partial paralysis of
ldquomucociliary escalatorrdquo - increased risk of secondary bacterial
LRTI Saureus pneumonia is a known complication following
influenza infection
27
Other bacteria bull Anaerobes
ndash Aspiration-prone Pt putrid sputum dental disease
bull Gram negative ndash Klebsiella - alcoholics
ndash Branhamella catarrhalis - sinus disease otitis COPD
ndash H influenza
28
Diagnosis and Management
29
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
Pathogenesis
bull Primary inhalation when organisms bypass normal respiratory defense mechanisms or when the Pt inhales aerobic GN organisms that colonize the upper respiratory tract or respiratory support equipment
bull Aspiration occurs when the patient aspirates colonized upper respiratory tract secretions
ndash Stomach reservoir of GNR that can ascend colonizing the respiratory tract
bull Hematogenous originate from a distant source and reach the lungs via the blood stream
12
bull Risk Factors for pneumonia ndash age ndash smoking ndash asthma ndash immunosuppression ndash institutionalization ndash COPD ndash PVD ndash Dementia ndash HIVAIDS
Community Acquired Pneumonia
13
bull Risk Factors in Patients Requiring Hospitalization ndash older unemployed
ndash common cold in the previous year
ndash asthma COPD steroid or bronchodilator use
ndash Chronic disease
ndash amount of smoking
Farr BM Respir Med 200094954-63
Community Acquired Pneumonia
14
bull Risk Factors for Mortality
ndash age
ndash bacteremia (for S pneumoniae)
ndash extent of radiographic changes
ndash degree of immunosuppression
ndash amount of alcohol
Community Acquired Pneumonia
15
ndash S pneumoniae 20-60
ndash H influenzae 3-10
ndash Chlamydia pneumoniae 4-6
ndash Mycoplasma pneumonaie 1-6
Community Acquired Pneumonia
ndash Legionella spp 2-8
ndash S aureus 3-5
ndash Gram negative bacilli 3-5
ndash Viruses 2-13
40-60 - NO CAUSE IDENTIFIED
2-5 - TWO OR MORE CAUSES
Microbiology
Bartlett NEJM 19953331618-24
16
Microbial etiology of community-acquired pneumonia in patients who
underwent comprehensive testing
17
Streptococcus pneumonia (Pneumococcus)
Most common cause of CAP About 23 of CAP are due to
Spneumoniae These are gram positive diplococci Typical symptoms (eg malaise
shaking chills fever rusty sputum pleuritic chest pain cough)
Lobar infiltrate on CXR May be immunosuppressed host 25 will have bacteremia ndash serious
effects
18
Risk Factors for Pneumococcal Pneumonia
bull Influenza infection
bull Alcohol abuse
bull Smoking--(x4 fold )
bull COPD and asthma
bull Hyposplenism or splenectomy
bull Immunocompromise---HIV (x50-100 fold ) MM SLE Transplant
bull Others---homeless pregnancy crack cocaine use incarceration
19
64 year old male with insulin dependent diabetes mellitus
He was admitted with bacteremic pneumococcal pneumonia Note the left lower lobe opacity
Pneumococcal pneumonia is the paradigm of classic lobar bacterial pneumonia
20
Complications of pneumococcal pneumonia
21
OTHER BACTERIAL PNEUMONIA
22
Atypical Pneumonia
bull 2 cause (especially in younger population)
bull Commonly associated with milder Sxrsquos subacute onset non-productive cough no focal infiltrate on CXR
bull Mycoplasma younger Pts extra-pulm Sxrsquos (anemia rashes) headache sore throat
bull Chlamydia year round URI Sx sore throat
bull Legionella higher mortality rate water-borne outbreaks hyponatremia diarrhea
23
Mycoplasma pneumonia
24
Mycoplasma pneumonia
25
Pneumocystis jirovecii pneumonia in patient with AIDS
26
Viruses and Pneumonia Pneumonia in the normal host
bull Adults or Children
bull Influenza A and B RSV Adenovirus Para Influenza
Pneumonia in the immuno-compromised
bull Measles HSV CMV HHV-6 Influenza viruses
bull Can cause a primary viral pneumonia Cause partial paralysis of
ldquomucociliary escalatorrdquo - increased risk of secondary bacterial
LRTI Saureus pneumonia is a known complication following
influenza infection
27
Other bacteria bull Anaerobes
ndash Aspiration-prone Pt putrid sputum dental disease
bull Gram negative ndash Klebsiella - alcoholics
ndash Branhamella catarrhalis - sinus disease otitis COPD
ndash H influenza
28
Diagnosis and Management
29
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
bull Risk Factors for pneumonia ndash age ndash smoking ndash asthma ndash immunosuppression ndash institutionalization ndash COPD ndash PVD ndash Dementia ndash HIVAIDS
Community Acquired Pneumonia
13
bull Risk Factors in Patients Requiring Hospitalization ndash older unemployed
ndash common cold in the previous year
ndash asthma COPD steroid or bronchodilator use
ndash Chronic disease
ndash amount of smoking
Farr BM Respir Med 200094954-63
Community Acquired Pneumonia
14
bull Risk Factors for Mortality
ndash age
ndash bacteremia (for S pneumoniae)
ndash extent of radiographic changes
ndash degree of immunosuppression
ndash amount of alcohol
Community Acquired Pneumonia
15
ndash S pneumoniae 20-60
ndash H influenzae 3-10
ndash Chlamydia pneumoniae 4-6
ndash Mycoplasma pneumonaie 1-6
Community Acquired Pneumonia
ndash Legionella spp 2-8
ndash S aureus 3-5
ndash Gram negative bacilli 3-5
ndash Viruses 2-13
40-60 - NO CAUSE IDENTIFIED
2-5 - TWO OR MORE CAUSES
Microbiology
Bartlett NEJM 19953331618-24
16
Microbial etiology of community-acquired pneumonia in patients who
underwent comprehensive testing
17
Streptococcus pneumonia (Pneumococcus)
Most common cause of CAP About 23 of CAP are due to
Spneumoniae These are gram positive diplococci Typical symptoms (eg malaise
shaking chills fever rusty sputum pleuritic chest pain cough)
Lobar infiltrate on CXR May be immunosuppressed host 25 will have bacteremia ndash serious
effects
18
Risk Factors for Pneumococcal Pneumonia
bull Influenza infection
bull Alcohol abuse
bull Smoking--(x4 fold )
bull COPD and asthma
bull Hyposplenism or splenectomy
bull Immunocompromise---HIV (x50-100 fold ) MM SLE Transplant
bull Others---homeless pregnancy crack cocaine use incarceration
19
64 year old male with insulin dependent diabetes mellitus
He was admitted with bacteremic pneumococcal pneumonia Note the left lower lobe opacity
Pneumococcal pneumonia is the paradigm of classic lobar bacterial pneumonia
20
Complications of pneumococcal pneumonia
21
OTHER BACTERIAL PNEUMONIA
22
Atypical Pneumonia
bull 2 cause (especially in younger population)
bull Commonly associated with milder Sxrsquos subacute onset non-productive cough no focal infiltrate on CXR
bull Mycoplasma younger Pts extra-pulm Sxrsquos (anemia rashes) headache sore throat
bull Chlamydia year round URI Sx sore throat
bull Legionella higher mortality rate water-borne outbreaks hyponatremia diarrhea
23
Mycoplasma pneumonia
24
Mycoplasma pneumonia
25
Pneumocystis jirovecii pneumonia in patient with AIDS
26
Viruses and Pneumonia Pneumonia in the normal host
bull Adults or Children
bull Influenza A and B RSV Adenovirus Para Influenza
Pneumonia in the immuno-compromised
bull Measles HSV CMV HHV-6 Influenza viruses
bull Can cause a primary viral pneumonia Cause partial paralysis of
ldquomucociliary escalatorrdquo - increased risk of secondary bacterial
LRTI Saureus pneumonia is a known complication following
influenza infection
27
Other bacteria bull Anaerobes
ndash Aspiration-prone Pt putrid sputum dental disease
bull Gram negative ndash Klebsiella - alcoholics
ndash Branhamella catarrhalis - sinus disease otitis COPD
ndash H influenza
28
Diagnosis and Management
29
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
bull Risk Factors in Patients Requiring Hospitalization ndash older unemployed
ndash common cold in the previous year
ndash asthma COPD steroid or bronchodilator use
ndash Chronic disease
ndash amount of smoking
Farr BM Respir Med 200094954-63
Community Acquired Pneumonia
14
bull Risk Factors for Mortality
ndash age
ndash bacteremia (for S pneumoniae)
ndash extent of radiographic changes
ndash degree of immunosuppression
ndash amount of alcohol
Community Acquired Pneumonia
15
ndash S pneumoniae 20-60
ndash H influenzae 3-10
ndash Chlamydia pneumoniae 4-6
ndash Mycoplasma pneumonaie 1-6
Community Acquired Pneumonia
ndash Legionella spp 2-8
ndash S aureus 3-5
ndash Gram negative bacilli 3-5
ndash Viruses 2-13
40-60 - NO CAUSE IDENTIFIED
2-5 - TWO OR MORE CAUSES
Microbiology
Bartlett NEJM 19953331618-24
16
Microbial etiology of community-acquired pneumonia in patients who
underwent comprehensive testing
17
Streptococcus pneumonia (Pneumococcus)
Most common cause of CAP About 23 of CAP are due to
Spneumoniae These are gram positive diplococci Typical symptoms (eg malaise
shaking chills fever rusty sputum pleuritic chest pain cough)
Lobar infiltrate on CXR May be immunosuppressed host 25 will have bacteremia ndash serious
effects
18
Risk Factors for Pneumococcal Pneumonia
bull Influenza infection
bull Alcohol abuse
bull Smoking--(x4 fold )
bull COPD and asthma
bull Hyposplenism or splenectomy
bull Immunocompromise---HIV (x50-100 fold ) MM SLE Transplant
bull Others---homeless pregnancy crack cocaine use incarceration
19
64 year old male with insulin dependent diabetes mellitus
He was admitted with bacteremic pneumococcal pneumonia Note the left lower lobe opacity
Pneumococcal pneumonia is the paradigm of classic lobar bacterial pneumonia
20
Complications of pneumococcal pneumonia
21
OTHER BACTERIAL PNEUMONIA
22
Atypical Pneumonia
bull 2 cause (especially in younger population)
bull Commonly associated with milder Sxrsquos subacute onset non-productive cough no focal infiltrate on CXR
bull Mycoplasma younger Pts extra-pulm Sxrsquos (anemia rashes) headache sore throat
bull Chlamydia year round URI Sx sore throat
bull Legionella higher mortality rate water-borne outbreaks hyponatremia diarrhea
23
Mycoplasma pneumonia
24
Mycoplasma pneumonia
25
Pneumocystis jirovecii pneumonia in patient with AIDS
26
Viruses and Pneumonia Pneumonia in the normal host
bull Adults or Children
bull Influenza A and B RSV Adenovirus Para Influenza
Pneumonia in the immuno-compromised
bull Measles HSV CMV HHV-6 Influenza viruses
bull Can cause a primary viral pneumonia Cause partial paralysis of
ldquomucociliary escalatorrdquo - increased risk of secondary bacterial
LRTI Saureus pneumonia is a known complication following
influenza infection
27
Other bacteria bull Anaerobes
ndash Aspiration-prone Pt putrid sputum dental disease
bull Gram negative ndash Klebsiella - alcoholics
ndash Branhamella catarrhalis - sinus disease otitis COPD
ndash H influenza
28
Diagnosis and Management
29
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60

bull Risk Factors for Mortality
ndash age
ndash bacteremia (for S pneumoniae)
ndash extent of radiographic changes
ndash degree of immunosuppression
ndash amount of alcohol
Community Acquired Pneumonia
15
ndash S pneumoniae 20-60
ndash H influenzae 3-10
ndash Chlamydia pneumoniae 4-6
ndash Mycoplasma pneumonaie 1-6
Community Acquired Pneumonia
ndash Legionella spp 2-8
ndash S aureus 3-5
ndash Gram negative bacilli 3-5
ndash Viruses 2-13
40-60 - NO CAUSE IDENTIFIED
2-5 - TWO OR MORE CAUSES
Microbiology
Bartlett NEJM 19953331618-24
16
Microbial etiology of community-acquired pneumonia in patients who
underwent comprehensive testing
17
Streptococcus pneumonia (Pneumococcus)
Most common cause of CAP About 23 of CAP are due to
Spneumoniae These are gram positive diplococci Typical symptoms (eg malaise
shaking chills fever rusty sputum pleuritic chest pain cough)
Lobar infiltrate on CXR May be immunosuppressed host 25 will have bacteremia ndash serious
effects
18
Risk Factors for Pneumococcal Pneumonia
bull Influenza infection
bull Alcohol abuse
bull Smoking--(x4 fold )
bull COPD and asthma
bull Hyposplenism or splenectomy
bull Immunocompromise---HIV (x50-100 fold ) MM SLE Transplant
bull Others---homeless pregnancy crack cocaine use incarceration
19
64 year old male with insulin dependent diabetes mellitus
He was admitted with bacteremic pneumococcal pneumonia Note the left lower lobe opacity
Pneumococcal pneumonia is the paradigm of classic lobar bacterial pneumonia
20
Complications of pneumococcal pneumonia
21
OTHER BACTERIAL PNEUMONIA
22
Atypical Pneumonia
bull 2 cause (especially in younger population)
bull Commonly associated with milder Sxrsquos subacute onset non-productive cough no focal infiltrate on CXR
bull Mycoplasma younger Pts extra-pulm Sxrsquos (anemia rashes) headache sore throat
bull Chlamydia year round URI Sx sore throat
bull Legionella higher mortality rate water-borne outbreaks hyponatremia diarrhea
23
Mycoplasma pneumonia
24
Mycoplasma pneumonia
25
Pneumocystis jirovecii pneumonia in patient with AIDS
26
Viruses and Pneumonia Pneumonia in the normal host
bull Adults or Children
bull Influenza A and B RSV Adenovirus Para Influenza
Pneumonia in the immuno-compromised
bull Measles HSV CMV HHV-6 Influenza viruses
bull Can cause a primary viral pneumonia Cause partial paralysis of
ldquomucociliary escalatorrdquo - increased risk of secondary bacterial
LRTI Saureus pneumonia is a known complication following
influenza infection
27
Other bacteria bull Anaerobes
ndash Aspiration-prone Pt putrid sputum dental disease
bull Gram negative ndash Klebsiella - alcoholics
ndash Branhamella catarrhalis - sinus disease otitis COPD
ndash H influenza
28
Diagnosis and Management
29
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
ndash S pneumoniae 20-60
ndash H influenzae 3-10
ndash Chlamydia pneumoniae 4-6
ndash Mycoplasma pneumonaie 1-6
Community Acquired Pneumonia
ndash Legionella spp 2-8
ndash S aureus 3-5
ndash Gram negative bacilli 3-5
ndash Viruses 2-13
40-60 - NO CAUSE IDENTIFIED
2-5 - TWO OR MORE CAUSES
Microbiology
Bartlett NEJM 19953331618-24
16
Microbial etiology of community-acquired pneumonia in patients who
underwent comprehensive testing
17
Streptococcus pneumonia (Pneumococcus)
Most common cause of CAP About 23 of CAP are due to
Spneumoniae These are gram positive diplococci Typical symptoms (eg malaise
shaking chills fever rusty sputum pleuritic chest pain cough)
Lobar infiltrate on CXR May be immunosuppressed host 25 will have bacteremia ndash serious
effects
18
Risk Factors for Pneumococcal Pneumonia
bull Influenza infection
bull Alcohol abuse
bull Smoking--(x4 fold )
bull COPD and asthma
bull Hyposplenism or splenectomy
bull Immunocompromise---HIV (x50-100 fold ) MM SLE Transplant
bull Others---homeless pregnancy crack cocaine use incarceration
19
64 year old male with insulin dependent diabetes mellitus
He was admitted with bacteremic pneumococcal pneumonia Note the left lower lobe opacity
Pneumococcal pneumonia is the paradigm of classic lobar bacterial pneumonia
20
Complications of pneumococcal pneumonia
21
OTHER BACTERIAL PNEUMONIA
22
Atypical Pneumonia
bull 2 cause (especially in younger population)
bull Commonly associated with milder Sxrsquos subacute onset non-productive cough no focal infiltrate on CXR
bull Mycoplasma younger Pts extra-pulm Sxrsquos (anemia rashes) headache sore throat
bull Chlamydia year round URI Sx sore throat
bull Legionella higher mortality rate water-borne outbreaks hyponatremia diarrhea
23
Mycoplasma pneumonia
24
Mycoplasma pneumonia
25
Pneumocystis jirovecii pneumonia in patient with AIDS
26
Viruses and Pneumonia Pneumonia in the normal host
bull Adults or Children
bull Influenza A and B RSV Adenovirus Para Influenza
Pneumonia in the immuno-compromised
bull Measles HSV CMV HHV-6 Influenza viruses
bull Can cause a primary viral pneumonia Cause partial paralysis of
ldquomucociliary escalatorrdquo - increased risk of secondary bacterial
LRTI Saureus pneumonia is a known complication following
influenza infection
27
Other bacteria bull Anaerobes
ndash Aspiration-prone Pt putrid sputum dental disease
bull Gram negative ndash Klebsiella - alcoholics
ndash Branhamella catarrhalis - sinus disease otitis COPD
ndash H influenza
28
Diagnosis and Management
29
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
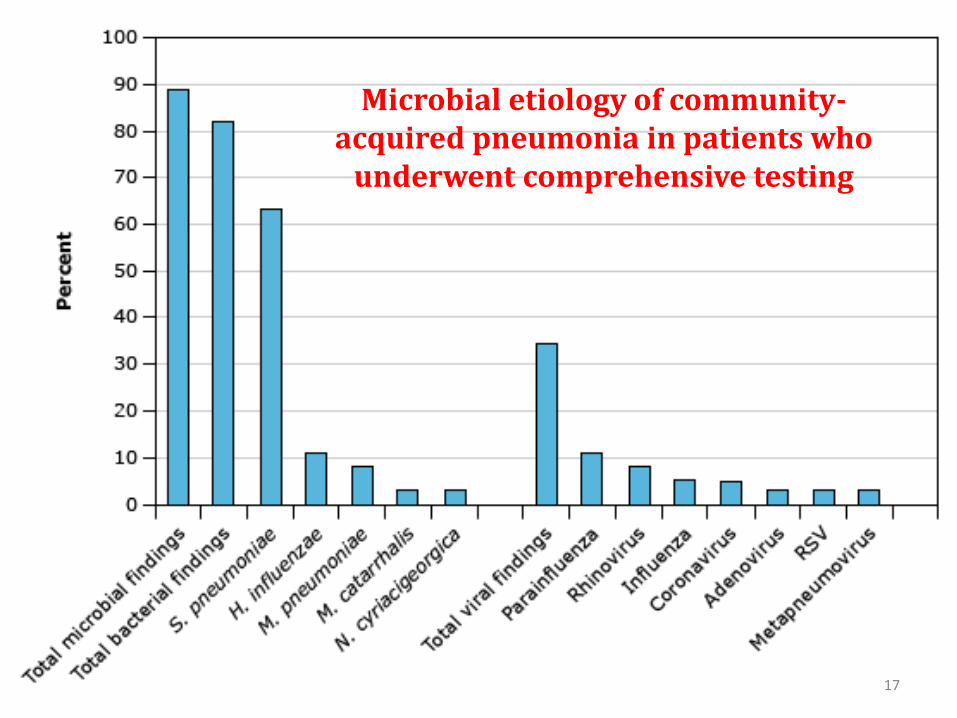
Microbial etiology of community-acquired pneumonia in patients who
underwent comprehensive testing
17
Streptococcus pneumonia (Pneumococcus)
Most common cause of CAP About 23 of CAP are due to
Spneumoniae These are gram positive diplococci Typical symptoms (eg malaise
shaking chills fever rusty sputum pleuritic chest pain cough)
Lobar infiltrate on CXR May be immunosuppressed host 25 will have bacteremia ndash serious
effects
18
Risk Factors for Pneumococcal Pneumonia
bull Influenza infection
bull Alcohol abuse
bull Smoking--(x4 fold )
bull COPD and asthma
bull Hyposplenism or splenectomy
bull Immunocompromise---HIV (x50-100 fold ) MM SLE Transplant
bull Others---homeless pregnancy crack cocaine use incarceration
19
64 year old male with insulin dependent diabetes mellitus
He was admitted with bacteremic pneumococcal pneumonia Note the left lower lobe opacity
Pneumococcal pneumonia is the paradigm of classic lobar bacterial pneumonia
20
Complications of pneumococcal pneumonia
21
OTHER BACTERIAL PNEUMONIA
22
Atypical Pneumonia
bull 2 cause (especially in younger population)
bull Commonly associated with milder Sxrsquos subacute onset non-productive cough no focal infiltrate on CXR
bull Mycoplasma younger Pts extra-pulm Sxrsquos (anemia rashes) headache sore throat
bull Chlamydia year round URI Sx sore throat
bull Legionella higher mortality rate water-borne outbreaks hyponatremia diarrhea
23
Mycoplasma pneumonia
24
Mycoplasma pneumonia
25
Pneumocystis jirovecii pneumonia in patient with AIDS
26
Viruses and Pneumonia Pneumonia in the normal host
bull Adults or Children
bull Influenza A and B RSV Adenovirus Para Influenza
Pneumonia in the immuno-compromised
bull Measles HSV CMV HHV-6 Influenza viruses
bull Can cause a primary viral pneumonia Cause partial paralysis of
ldquomucociliary escalatorrdquo - increased risk of secondary bacterial
LRTI Saureus pneumonia is a known complication following
influenza infection
27
Other bacteria bull Anaerobes
ndash Aspiration-prone Pt putrid sputum dental disease
bull Gram negative ndash Klebsiella - alcoholics
ndash Branhamella catarrhalis - sinus disease otitis COPD
ndash H influenza
28
Diagnosis and Management
29
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
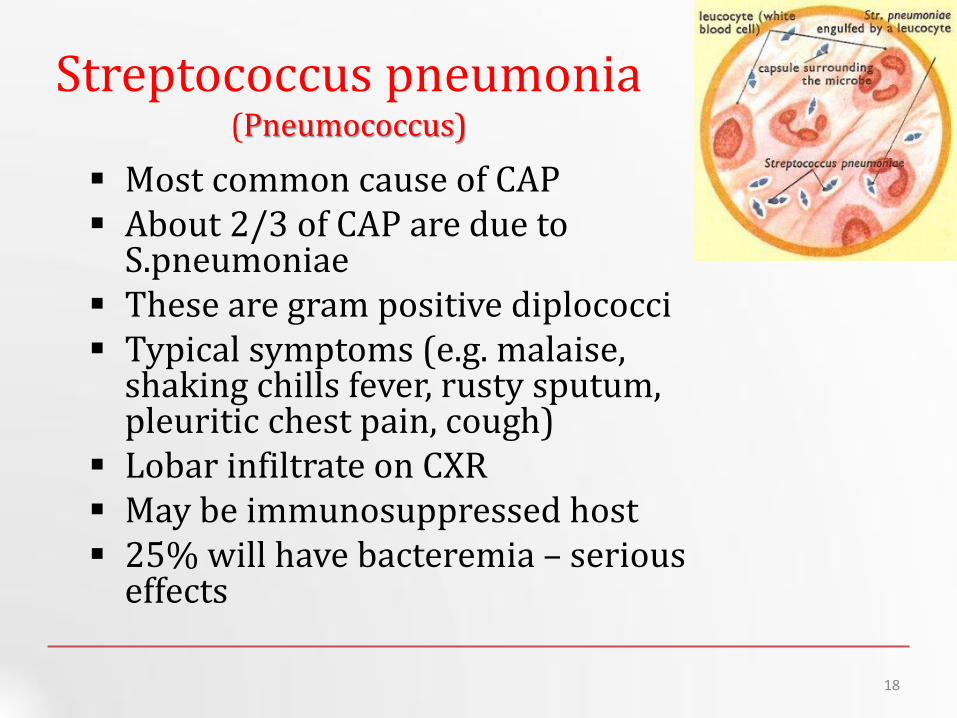
Streptococcus pneumonia (Pneumococcus)
Most common cause of CAP About 23 of CAP are due to
Spneumoniae These are gram positive diplococci Typical symptoms (eg malaise
shaking chills fever rusty sputum pleuritic chest pain cough)
Lobar infiltrate on CXR May be immunosuppressed host 25 will have bacteremia ndash serious
effects
18
Risk Factors for Pneumococcal Pneumonia
bull Influenza infection
bull Alcohol abuse
bull Smoking--(x4 fold )
bull COPD and asthma
bull Hyposplenism or splenectomy
bull Immunocompromise---HIV (x50-100 fold ) MM SLE Transplant
bull Others---homeless pregnancy crack cocaine use incarceration
19
64 year old male with insulin dependent diabetes mellitus
He was admitted with bacteremic pneumococcal pneumonia Note the left lower lobe opacity
Pneumococcal pneumonia is the paradigm of classic lobar bacterial pneumonia
20
Complications of pneumococcal pneumonia
21
OTHER BACTERIAL PNEUMONIA
22
Atypical Pneumonia
bull 2 cause (especially in younger population)
bull Commonly associated with milder Sxrsquos subacute onset non-productive cough no focal infiltrate on CXR
bull Mycoplasma younger Pts extra-pulm Sxrsquos (anemia rashes) headache sore throat
bull Chlamydia year round URI Sx sore throat
bull Legionella higher mortality rate water-borne outbreaks hyponatremia diarrhea
23
Mycoplasma pneumonia
24
Mycoplasma pneumonia
25
Pneumocystis jirovecii pneumonia in patient with AIDS
26
Viruses and Pneumonia Pneumonia in the normal host
bull Adults or Children
bull Influenza A and B RSV Adenovirus Para Influenza
Pneumonia in the immuno-compromised
bull Measles HSV CMV HHV-6 Influenza viruses
bull Can cause a primary viral pneumonia Cause partial paralysis of
ldquomucociliary escalatorrdquo - increased risk of secondary bacterial
LRTI Saureus pneumonia is a known complication following
influenza infection
27
Other bacteria bull Anaerobes
ndash Aspiration-prone Pt putrid sputum dental disease
bull Gram negative ndash Klebsiella - alcoholics
ndash Branhamella catarrhalis - sinus disease otitis COPD
ndash H influenza
28
Diagnosis and Management
29
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
Risk Factors for Pneumococcal Pneumonia
bull Influenza infection
bull Alcohol abuse
bull Smoking--(x4 fold )
bull COPD and asthma
bull Hyposplenism or splenectomy
bull Immunocompromise---HIV (x50-100 fold ) MM SLE Transplant
bull Others---homeless pregnancy crack cocaine use incarceration
19
64 year old male with insulin dependent diabetes mellitus
He was admitted with bacteremic pneumococcal pneumonia Note the left lower lobe opacity
Pneumococcal pneumonia is the paradigm of classic lobar bacterial pneumonia
20
Complications of pneumococcal pneumonia
21
OTHER BACTERIAL PNEUMONIA
22
Atypical Pneumonia
bull 2 cause (especially in younger population)
bull Commonly associated with milder Sxrsquos subacute onset non-productive cough no focal infiltrate on CXR
bull Mycoplasma younger Pts extra-pulm Sxrsquos (anemia rashes) headache sore throat
bull Chlamydia year round URI Sx sore throat
bull Legionella higher mortality rate water-borne outbreaks hyponatremia diarrhea
23
Mycoplasma pneumonia
24
Mycoplasma pneumonia
25
Pneumocystis jirovecii pneumonia in patient with AIDS
26
Viruses and Pneumonia Pneumonia in the normal host
bull Adults or Children
bull Influenza A and B RSV Adenovirus Para Influenza
Pneumonia in the immuno-compromised
bull Measles HSV CMV HHV-6 Influenza viruses
bull Can cause a primary viral pneumonia Cause partial paralysis of
ldquomucociliary escalatorrdquo - increased risk of secondary bacterial
LRTI Saureus pneumonia is a known complication following
influenza infection
27
Other bacteria bull Anaerobes
ndash Aspiration-prone Pt putrid sputum dental disease
bull Gram negative ndash Klebsiella - alcoholics
ndash Branhamella catarrhalis - sinus disease otitis COPD
ndash H influenza
28
Diagnosis and Management
29
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
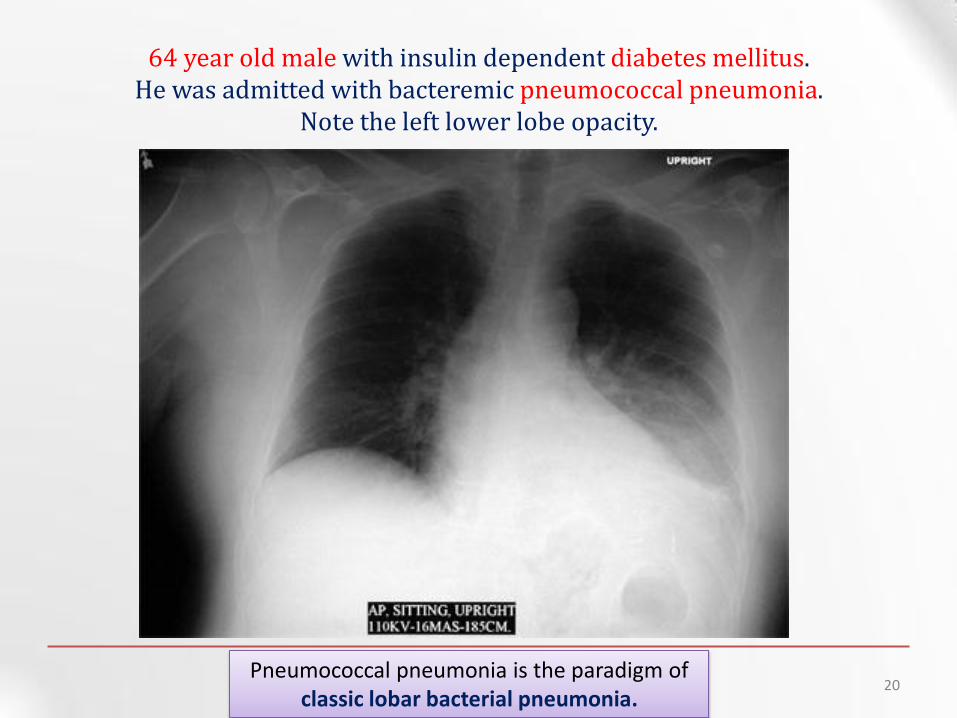
64 year old male with insulin dependent diabetes mellitus
He was admitted with bacteremic pneumococcal pneumonia Note the left lower lobe opacity
Pneumococcal pneumonia is the paradigm of classic lobar bacterial pneumonia
20
Complications of pneumococcal pneumonia
21
OTHER BACTERIAL PNEUMONIA
22
Atypical Pneumonia
bull 2 cause (especially in younger population)
bull Commonly associated with milder Sxrsquos subacute onset non-productive cough no focal infiltrate on CXR
bull Mycoplasma younger Pts extra-pulm Sxrsquos (anemia rashes) headache sore throat
bull Chlamydia year round URI Sx sore throat
bull Legionella higher mortality rate water-borne outbreaks hyponatremia diarrhea
23
Mycoplasma pneumonia
24
Mycoplasma pneumonia
25
Pneumocystis jirovecii pneumonia in patient with AIDS
26
Viruses and Pneumonia Pneumonia in the normal host
bull Adults or Children
bull Influenza A and B RSV Adenovirus Para Influenza
Pneumonia in the immuno-compromised
bull Measles HSV CMV HHV-6 Influenza viruses
bull Can cause a primary viral pneumonia Cause partial paralysis of
ldquomucociliary escalatorrdquo - increased risk of secondary bacterial
LRTI Saureus pneumonia is a known complication following
influenza infection
27
Other bacteria bull Anaerobes
ndash Aspiration-prone Pt putrid sputum dental disease
bull Gram negative ndash Klebsiella - alcoholics
ndash Branhamella catarrhalis - sinus disease otitis COPD
ndash H influenza
28
Diagnosis and Management
29
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
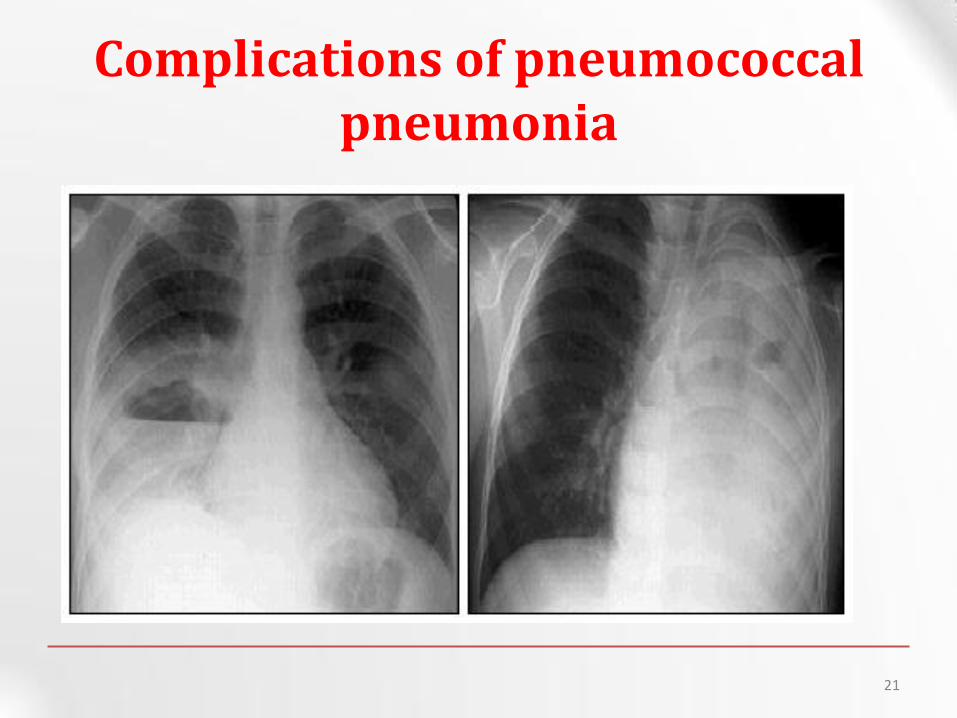
Complications of pneumococcal pneumonia
21
OTHER BACTERIAL PNEUMONIA
22
Atypical Pneumonia
bull 2 cause (especially in younger population)
bull Commonly associated with milder Sxrsquos subacute onset non-productive cough no focal infiltrate on CXR
bull Mycoplasma younger Pts extra-pulm Sxrsquos (anemia rashes) headache sore throat
bull Chlamydia year round URI Sx sore throat
bull Legionella higher mortality rate water-borne outbreaks hyponatremia diarrhea
23
Mycoplasma pneumonia
24
Mycoplasma pneumonia
25
Pneumocystis jirovecii pneumonia in patient with AIDS
26
Viruses and Pneumonia Pneumonia in the normal host
bull Adults or Children
bull Influenza A and B RSV Adenovirus Para Influenza
Pneumonia in the immuno-compromised
bull Measles HSV CMV HHV-6 Influenza viruses
bull Can cause a primary viral pneumonia Cause partial paralysis of
ldquomucociliary escalatorrdquo - increased risk of secondary bacterial
LRTI Saureus pneumonia is a known complication following
influenza infection
27
Other bacteria bull Anaerobes
ndash Aspiration-prone Pt putrid sputum dental disease
bull Gram negative ndash Klebsiella - alcoholics
ndash Branhamella catarrhalis - sinus disease otitis COPD
ndash H influenza
28
Diagnosis and Management
29
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60

OTHER BACTERIAL PNEUMONIA
22
Atypical Pneumonia
bull 2 cause (especially in younger population)
bull Commonly associated with milder Sxrsquos subacute onset non-productive cough no focal infiltrate on CXR
bull Mycoplasma younger Pts extra-pulm Sxrsquos (anemia rashes) headache sore throat
bull Chlamydia year round URI Sx sore throat
bull Legionella higher mortality rate water-borne outbreaks hyponatremia diarrhea
23
Mycoplasma pneumonia
24
Mycoplasma pneumonia
25
Pneumocystis jirovecii pneumonia in patient with AIDS
26
Viruses and Pneumonia Pneumonia in the normal host
bull Adults or Children
bull Influenza A and B RSV Adenovirus Para Influenza
Pneumonia in the immuno-compromised
bull Measles HSV CMV HHV-6 Influenza viruses
bull Can cause a primary viral pneumonia Cause partial paralysis of
ldquomucociliary escalatorrdquo - increased risk of secondary bacterial
LRTI Saureus pneumonia is a known complication following
influenza infection
27
Other bacteria bull Anaerobes
ndash Aspiration-prone Pt putrid sputum dental disease
bull Gram negative ndash Klebsiella - alcoholics
ndash Branhamella catarrhalis - sinus disease otitis COPD
ndash H influenza
28
Diagnosis and Management
29
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
Atypical Pneumonia
bull 2 cause (especially in younger population)
bull Commonly associated with milder Sxrsquos subacute onset non-productive cough no focal infiltrate on CXR
bull Mycoplasma younger Pts extra-pulm Sxrsquos (anemia rashes) headache sore throat
bull Chlamydia year round URI Sx sore throat
bull Legionella higher mortality rate water-borne outbreaks hyponatremia diarrhea
23
Mycoplasma pneumonia
24
Mycoplasma pneumonia
25
Pneumocystis jirovecii pneumonia in patient with AIDS
26
Viruses and Pneumonia Pneumonia in the normal host
bull Adults or Children
bull Influenza A and B RSV Adenovirus Para Influenza
Pneumonia in the immuno-compromised
bull Measles HSV CMV HHV-6 Influenza viruses
bull Can cause a primary viral pneumonia Cause partial paralysis of
ldquomucociliary escalatorrdquo - increased risk of secondary bacterial
LRTI Saureus pneumonia is a known complication following
influenza infection
27
Other bacteria bull Anaerobes
ndash Aspiration-prone Pt putrid sputum dental disease
bull Gram negative ndash Klebsiella - alcoholics
ndash Branhamella catarrhalis - sinus disease otitis COPD
ndash H influenza
28
Diagnosis and Management
29
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
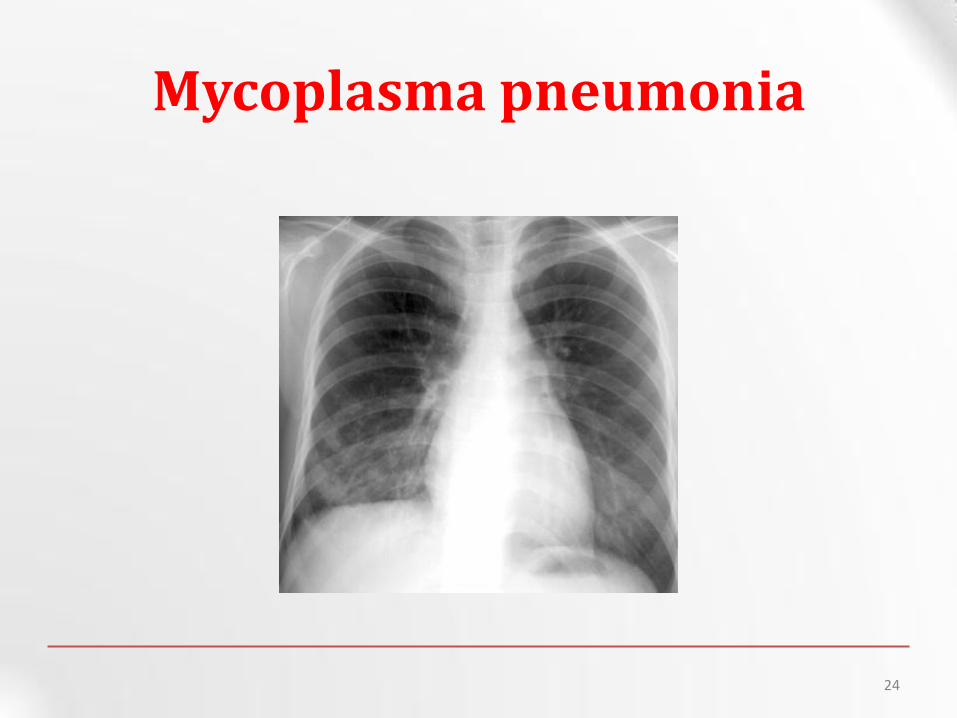
Mycoplasma pneumonia
24
Mycoplasma pneumonia
25
Pneumocystis jirovecii pneumonia in patient with AIDS
26
Viruses and Pneumonia Pneumonia in the normal host
bull Adults or Children
bull Influenza A and B RSV Adenovirus Para Influenza
Pneumonia in the immuno-compromised
bull Measles HSV CMV HHV-6 Influenza viruses
bull Can cause a primary viral pneumonia Cause partial paralysis of
ldquomucociliary escalatorrdquo - increased risk of secondary bacterial
LRTI Saureus pneumonia is a known complication following
influenza infection
27
Other bacteria bull Anaerobes
ndash Aspiration-prone Pt putrid sputum dental disease
bull Gram negative ndash Klebsiella - alcoholics
ndash Branhamella catarrhalis - sinus disease otitis COPD
ndash H influenza
28
Diagnosis and Management
29
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
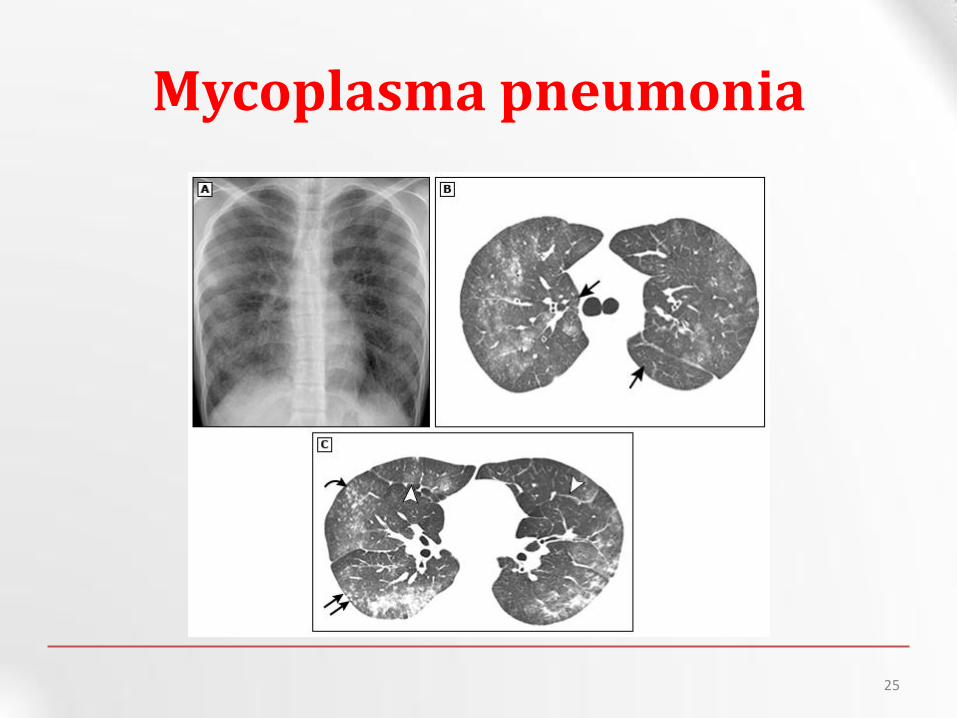
Mycoplasma pneumonia
25
Pneumocystis jirovecii pneumonia in patient with AIDS
26
Viruses and Pneumonia Pneumonia in the normal host
bull Adults or Children
bull Influenza A and B RSV Adenovirus Para Influenza
Pneumonia in the immuno-compromised
bull Measles HSV CMV HHV-6 Influenza viruses
bull Can cause a primary viral pneumonia Cause partial paralysis of
ldquomucociliary escalatorrdquo - increased risk of secondary bacterial
LRTI Saureus pneumonia is a known complication following
influenza infection
27
Other bacteria bull Anaerobes
ndash Aspiration-prone Pt putrid sputum dental disease
bull Gram negative ndash Klebsiella - alcoholics
ndash Branhamella catarrhalis - sinus disease otitis COPD
ndash H influenza
28
Diagnosis and Management
29
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
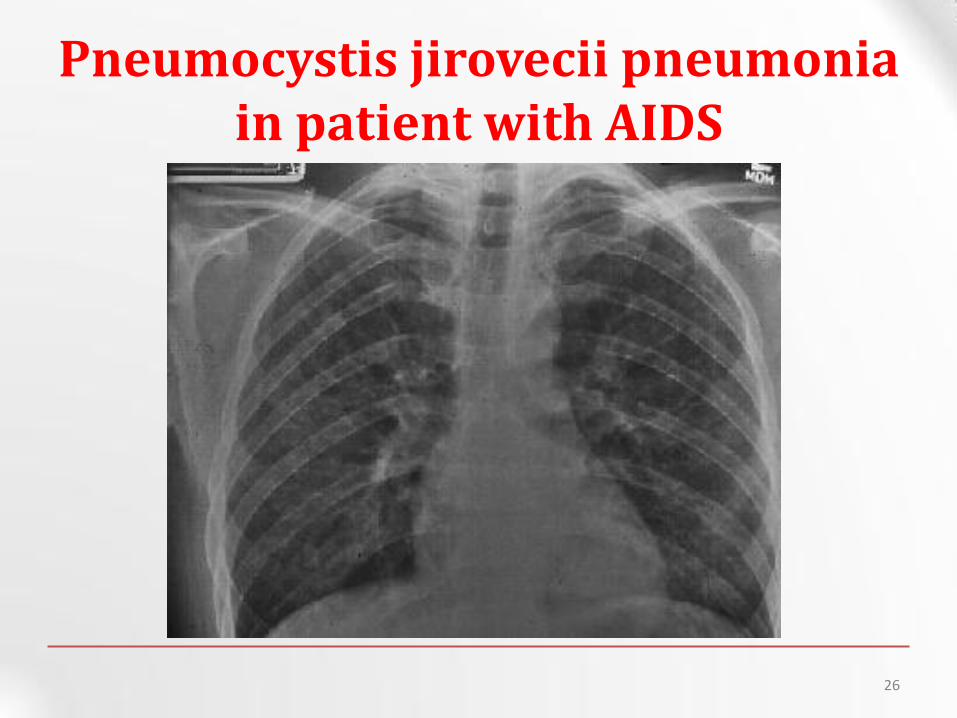
Pneumocystis jirovecii pneumonia in patient with AIDS
26
Viruses and Pneumonia Pneumonia in the normal host
bull Adults or Children
bull Influenza A and B RSV Adenovirus Para Influenza
Pneumonia in the immuno-compromised
bull Measles HSV CMV HHV-6 Influenza viruses
bull Can cause a primary viral pneumonia Cause partial paralysis of
ldquomucociliary escalatorrdquo - increased risk of secondary bacterial
LRTI Saureus pneumonia is a known complication following
influenza infection
27
Other bacteria bull Anaerobes
ndash Aspiration-prone Pt putrid sputum dental disease
bull Gram negative ndash Klebsiella - alcoholics
ndash Branhamella catarrhalis - sinus disease otitis COPD
ndash H influenza
28
Diagnosis and Management
29
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
Viruses and Pneumonia Pneumonia in the normal host
bull Adults or Children
bull Influenza A and B RSV Adenovirus Para Influenza
Pneumonia in the immuno-compromised
bull Measles HSV CMV HHV-6 Influenza viruses
bull Can cause a primary viral pneumonia Cause partial paralysis of
ldquomucociliary escalatorrdquo - increased risk of secondary bacterial
LRTI Saureus pneumonia is a known complication following
influenza infection
27
Other bacteria bull Anaerobes
ndash Aspiration-prone Pt putrid sputum dental disease
bull Gram negative ndash Klebsiella - alcoholics
ndash Branhamella catarrhalis - sinus disease otitis COPD
ndash H influenza
28
Diagnosis and Management
29
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
Other bacteria bull Anaerobes
ndash Aspiration-prone Pt putrid sputum dental disease
bull Gram negative ndash Klebsiella - alcoholics
ndash Branhamella catarrhalis - sinus disease otitis COPD
ndash H influenza
28
Diagnosis and Management
29
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
Diagnosis and Management
29
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
The approach to the patient with CAP
bull begins with
Clinical evaluation Followed by chest radiograph
Microbiological testing
30
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
Clinical Diagnosis
bull Suggestive signs and symptoms
bull CXR or other imaging technique
bull Microbiologic testing
31
Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60

Signs and Symptoms
bull Fever or hypothermia
bull Cough with or without sputum hemoptysis
bull Pleuritic chest pain
bull Myalgia malaise fatigue
bull GI symptoms
bull Dyspnea
bull Rales rhonchi wheezing
bull Egophony bronchial breath sounds
bull Dullness to percussion
bull Atypical Sxrsquos in older patients
32
Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60

Clinical Diagnosis CXR
bull Demonstrable infiltrate by CXR or other imaging technique
ndash Establish Dx and presence of complications (pleural effusion multilobar disease)
ndash May not be possible in some outpatient settings
ndash CXR classically thought of as the gold standard
33
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
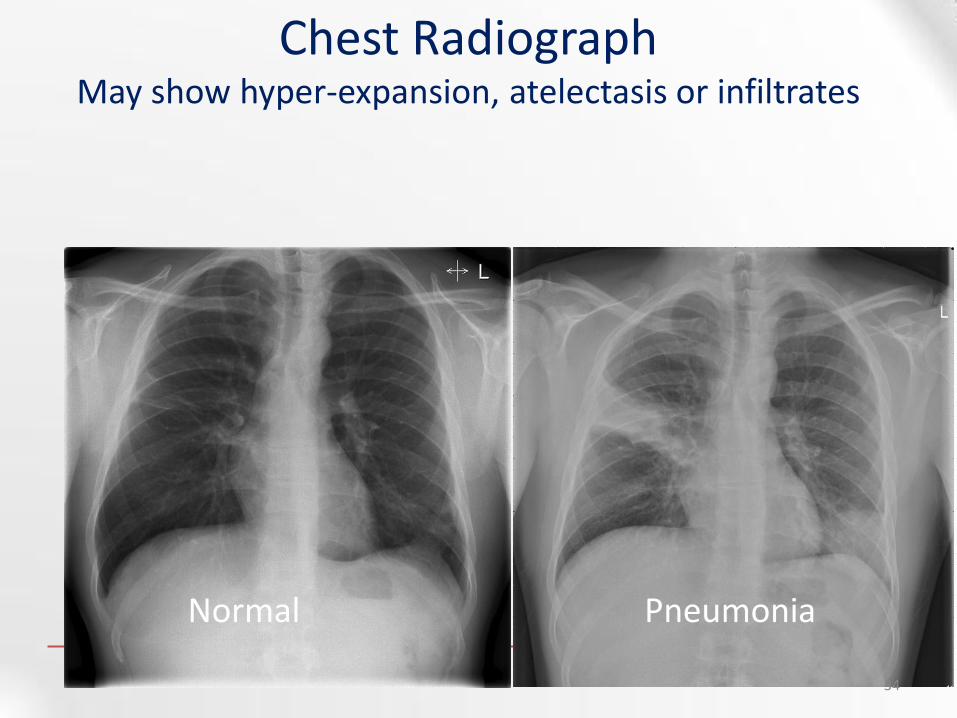
Normal Pneumonia
Chest Radiograph May show hyper-expansion atelectasis or infiltrates
34
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
Clinical Diagnosis Recommended testing
bull Outpatient CXR sputum Cx and Gram stain not required
bull Inpatient CXR Pox or ABG chemistry CBC two sets of blood Cxrsquos
ndash If suspect drug-resistant pathogen or organism not covered by usual empiric abx obtain sputum Cx and Gram stain
ndash Severe CAP Legionella urinary antigen consider bronchoscopy to identify pathogen
35
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
Community Acquired Pneumonia
Who should be hospitalized
36
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
To Admit or Not Pneumonia Severity amp Deciding Site of Care
bull Using objective criteria to risk stratify amp assist in decision outpatient vs inpatient management
bull Pneumonia Severity Index (PSI)
bull CURB-65
bull Caveats ndash Other reasons to admit apart from risk of death
ndash Not validated for ward vs ICU
ndash Labsvitals dynamic
37
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
Pneumonia Severity Index (PSI)
Fine MJ Auble TE Yealy DM Hanusa BH Weissfeld LA Singer DE Coley CM Marrie TJ Kapoor WN A prediction rule to identify low-risk patients with community-acquired pneumonia N Engl J Med 1997336(4)243-50
Patient outcome Research Team
(PORT) system
38
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
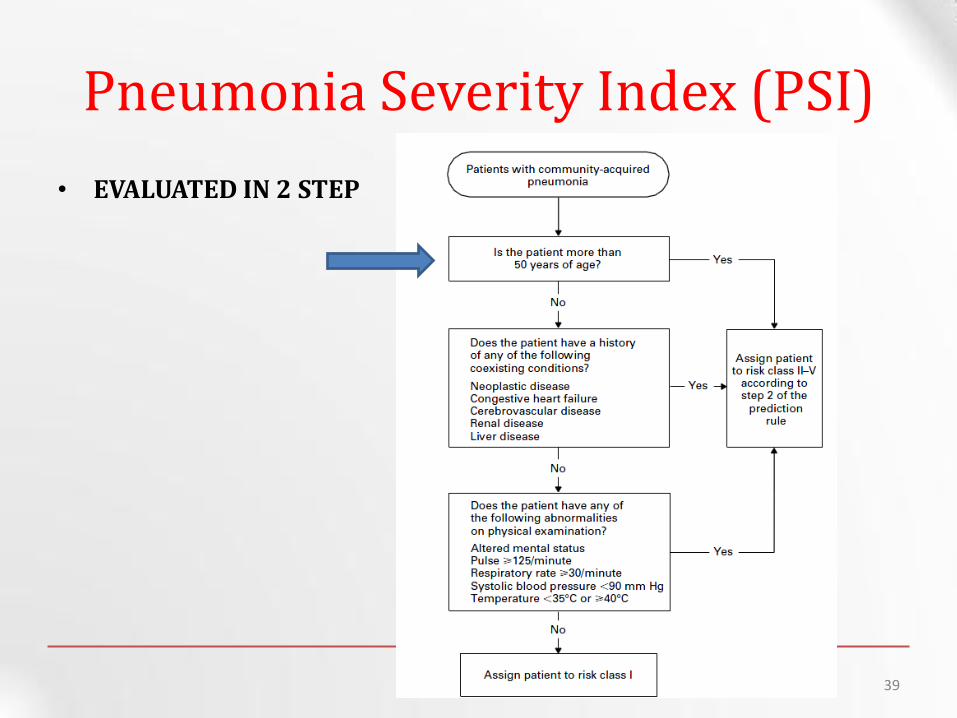
bull EVALUATED IN 2 STEP
Pneumonia Severity Index (PSI)
39
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
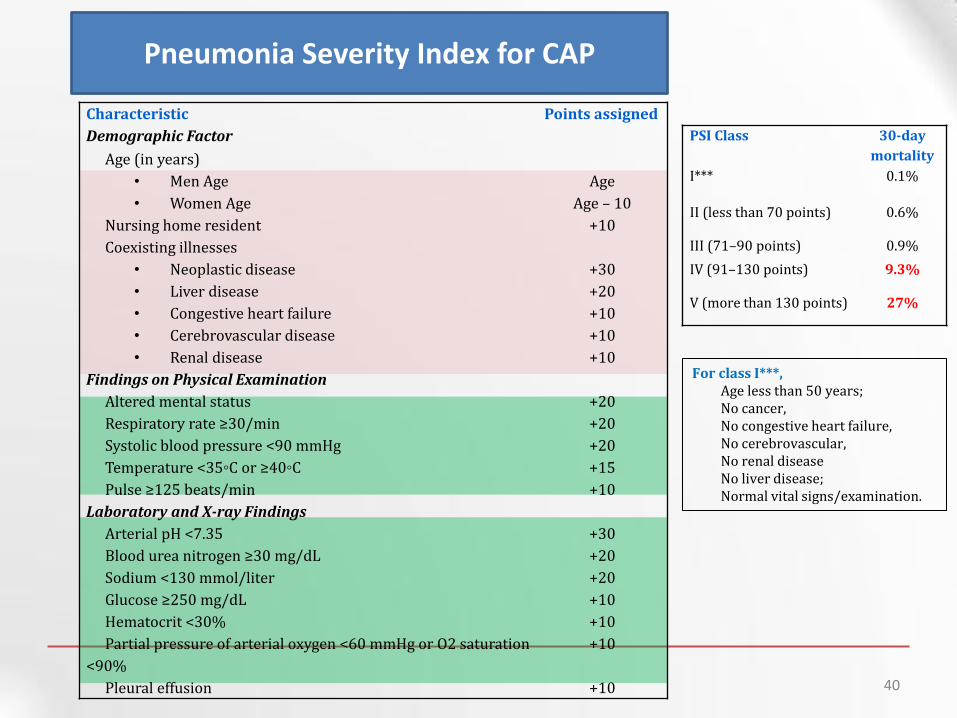
Characteristic Points assigned
Demographic Factor
Age (in years)
bull Men Age Age
bull Women Age Age ndash 10
Nursing home resident +10
Coexisting illnesses
bull Neoplastic disease +30
bull Liver disease +20
bull Congestive heart failure +10
bull Cerebrovascular disease +10
bull Renal disease +10
Findings on Physical Examination
Altered mental status +20
Respiratory rate ge30min +20
Systolic blood pressure lt90 mmHg +20
Temperature lt35C or ge40C +15
Pulse ge125 beatsmin +10
Laboratory and X-ray Findings
Arterial pH lt735 +30
Blood urea nitrogen ge30 mgdL +20
Sodium lt130 mmolliter +20
Glucose ge250 mgdL +10
Hematocrit lt30 +10
Partial pressure of arterial oxygen lt60 mmHg or O2 saturation
lt90
+10
Pleural effusion +10
Pneumonia Severity Index for CAP
PSI Class 30-day
mortality
I 01
II (less than 70 points) 06
III (71ndash90 points) 09
IV (91ndash130 points) 93
V (more than 130 points) 27
For class I Age less than 50 years No cancer No congestive heart failure No cerebrovascular No renal disease No liver disease Normal vital signsexamination
40
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
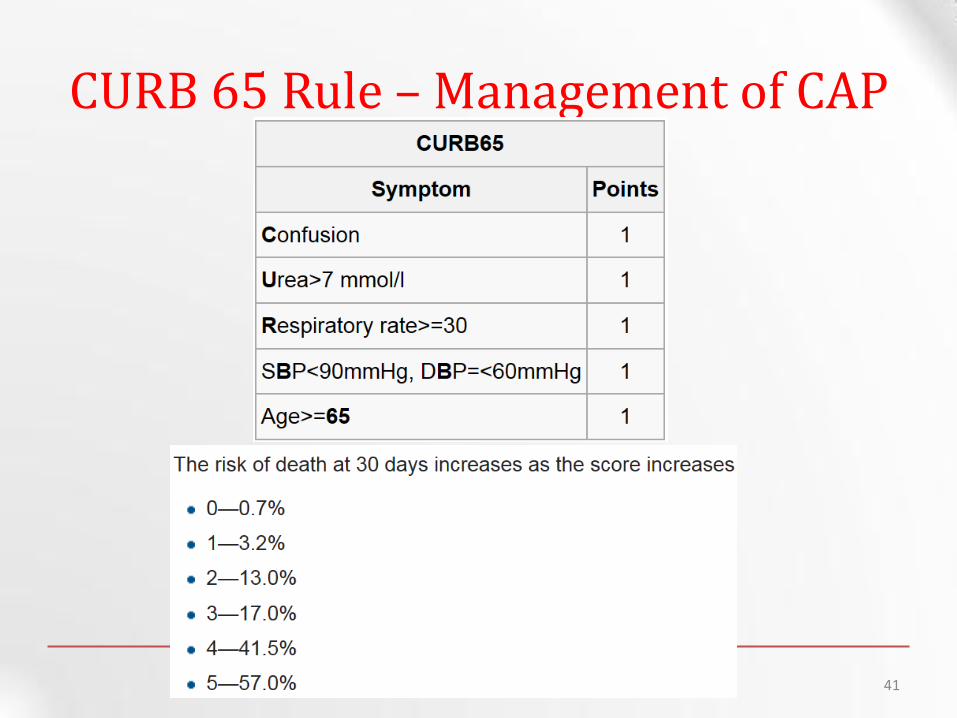
CURB 65 Rule ndash Management of CAP
41
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
Who Should be Hospitalized
Class I and II Usually do not require hospitalization
Class III May require brief hospitalization
Class IV and V Usually do require hospitalization
Severity of CAP with poor prognosis
RR gt 30 PaO2FiO2 lt 250 or PO2 lt 60 on room air
Need for mechanical ventilation Multi lobar involvement
Hypotension Need for vasopressors
Oliguria Altered mental status 42
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
CAP ndash Criteria for ICU Admission Major criteria
Invasive mechanical ventilation required
Septic shock with the need of vasopressors
Minor criteria (least 3)
Confusiondisorientation
Blood urea nitrogen ge 20 mg
Respiratory rate ge 30 min Core temperature lt 36ordmC
Severe hypotension PaO2FiO2 ratio le 250
Multi-lobar infiltrates
WBC lt 4000 cells Platelets lt100000
43
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
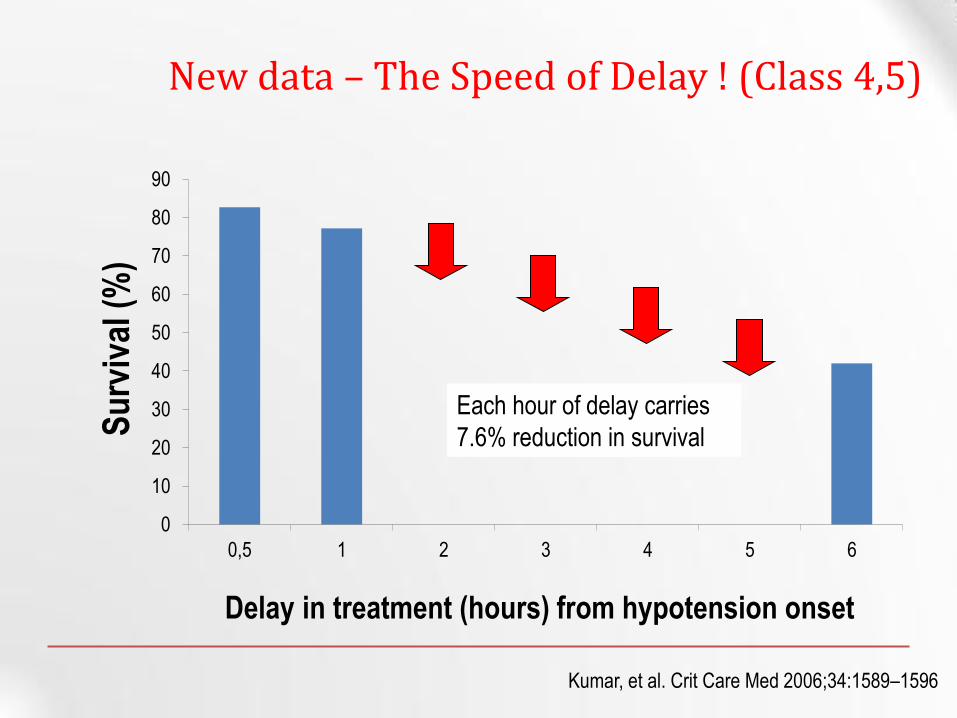
New data ndash The Speed of Delay (Class 45)
0
10
20
30
40
50
60
70
80
90
05 1 2 3 4 5 6
Delay in treatment (hours) from hypotension onset
Su
rviv
al (
)
Each hour of delay carries
76 reduction in survival
Kumar et al Crit Care Med 2006341589ndash1596
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
CAP ndash Complications
Hypotension and septic shock
3-5 Pleural effusion Clear fluid + pus cells
1 Empyema thoracis pus in the pleural space
Lung abscess ndash destruction of lung
Single (aspiration) anaerobes Pseudomonas
Multiple (metastatic) Staphylococcus aureus
Septicemia ndash Brain abscess Liver Abscess
Multiple Pyemic Abscesses
45
WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60

WHAT ABOUT THE ANTIBIOTIC CHOICE
46
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines (2007)
Mandell LA Wunderink RG Anzueto A et al Infectious Diseases Society of AmericaAmerican Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults Clin Infect Dis 200744Suppl 2S27-S72
47
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
Vanderkooi OG Low DE Green K Powis JE McGeer A Predicting antimicrobial resistance in invasive pneumococcal infections Clin Infect Dis 2005401288-97 48
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
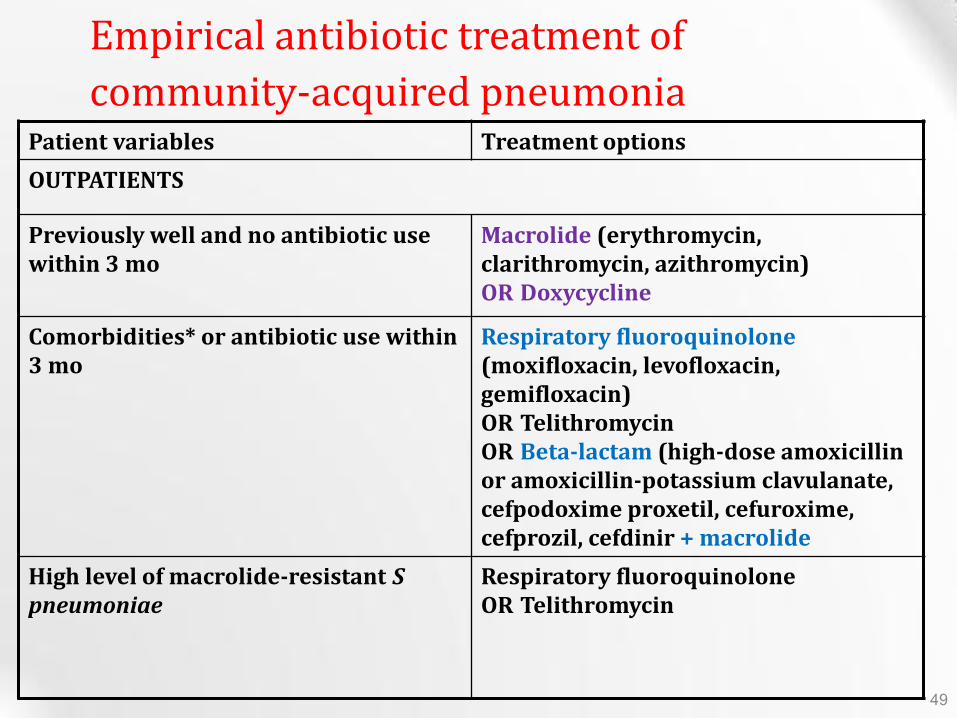
Treatment options Patient variables
OUTPATIENTS
Macrolide (erythromycin clarithromycin azithromycin)
OR Doxycycline
Previously well and no antibiotic use within 3 mo
Respiratory fluoroquinolone (moxifloxacin levofloxacin gemifloxacin) OR Telithromycin
OR Beta-lactam (high-dose amoxicillin or amoxicillin-potassium clavulanate cefpodoxime proxetil cefuroxime cefprozil cefdinir + macrolide
Comorbidities or antibiotic use within 3 mo
Respiratory fluoroquinolone
OR Telithromycin High level of macrolide-resistant S pneumoniae
Empirical antibiotic treatment of
community-acquired pneumonia
49
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
Outpatient treatment
bull The key to appropriate therapy is adequate coverage of
ndash Streptococcus pneumoniae and
ndash atypical bacterial pathogens (mycoplasma chlamydia and legionella)
bull For outpatients the coverage of atypical bacterial pathogens is most important especially for young adults
bull Macrolides doxycycline and fluoroquinolones are the most appropriate agents for the atypical bacterial pathogens
Wunderink RG Waterer GW Community-acquired pneumoniaN Engl J Med 2014370(19)1863 50
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
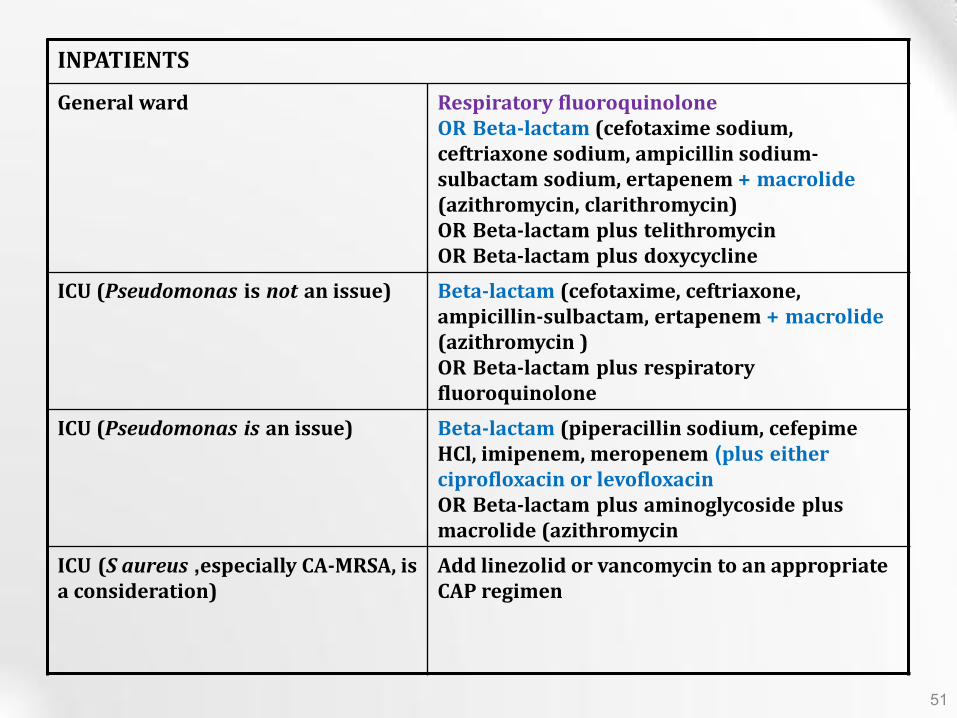
INPATIENTS
Respiratory fluoroquinolone
OR Beta-lactam (cefotaxime sodium ceftriaxone sodium ampicillin sodium-sulbactam sodium ertapenem + macrolide (azithromycin clarithromycin)
OR Beta-lactam plus telithromycin
OR Beta-lactam plus doxycycline
General ward
Beta-lactam (cefotaxime ceftriaxone ampicillin-sulbactam ertapenem + macrolide (azithromycin )
OR Beta-lactam plus respiratory fluoroquinolone
ICU (Pseudomonas is not an issue)
Beta-lactam (piperacillin sodium cefepime HCl imipenem meropenem )plus either ciprofloxacin or levofloxacin
OR Beta-lactam plus aminoglycoside plus
macrolide (azithromycin
ICU (Pseudomonas is an issue)
Add linezolid or vancomycin to an appropriate CAP regimen
ICU (S aureus especially CA-MRSA is a consideration)
51
IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60

IDSA Inpt Management-SevereICU
bull One of two major criteria
ndash Mechanical ventilation
ndash Septic shock OR
bull Two of three minor criteria
ndash SBPle90mmHg
ndash Multilobar disease
ndash PaO2FIO2 ratio lt 250
bull Organisms S pneumo Legionella GN Mycoplasma viral Pseudomonas
52
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
Switch to Oral Therapy
bull Four criteria
ndash Improvement in cough and dyspnea
ndash Afebrile on two occasions 8 h apart
ndash WBC decreasing
ndash Functioning GI tract with adequate oral intake
bull If overall clinical picture is otherwise favorable can can switch to oral therapy while still febrile
53
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
Duration of Therapy
bull Minimum of 5 days
bull Afebrile for at least 48 to 72 h
bull No gt 1 CAP-associated sign of clinical instability
bull Longer duration of therapy
If initial therapy was not active against the identified pathogen or
complicated by extra pulmonary infection
54
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
Prevention
bull Smoking cessation
bull Vaccination per ACIP recommendations
ndash Influenza
bull Inactivated vaccine for people gt50 yo those at risk for influenza compolications household contacts of high-risk persons and healthcare workers
bull Intranasal live attenuated vaccine 5-49yo without chronic underlying dz
ndash Pneumococcal
bull Immunocompetent ge 65 yo chronic illness and immunocompromised le 64 yo
55
OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60

OUR CASES
56
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
Case 1
Lab
bull A 62-year-old male with a medical history significant for chronic alcohol abuse presented to the ED complaining of persistent cough productive of green sputum fevers to 40C (104F) chills and rigors shortness of breath and sharp chest pain with cough and deep inspiration for 3 days
bull He reported nausea and vomiting but denied abdominal pain or diarrhea He also denied recent travel leg swelling or tobacco use His last alcoholic drink was 24 hours prior to presentation
PHYSICAL EXAMINATION
bull GENERAL APPEARANCE The patient looked older than his stated age He was a cachectic and ill-appearing male in moderate respiratory distress speaking only three- or four-word sentences
VITAL SIGNS
ndash Temperature 40C (104F )
ndash Pulse 120 beatsminute
ndash Blood pressure 11065 mmHg
ndash Respirations 30 breathsminute
ndash Oxygen saturation 96 on room air
bull CARDIOVASCULAR Tachycardic rate regular rhythm without rubs murmurs or gallops
bull LUNGS Mild expiratory wheezes throughout all lung fields scattered rhonchi crackles and egophony at the right lower and mid-lung fields
bull CBC
ndash Hb149 grdL
bull WBC 20000 KμL (normal 35ndash125 KμL) with 35 immature bands (presence of bands abnormal)
ndash Plt186000 microL
bull Sodium of 125 mEqL (normal 137ndash145 mEqL)
bull How can you manage this patient
bull Risk stratification
bull Antibiotic
bull Hospitalization
Cases
The patientrsquos calculated Pneumonia Severity Index (PSI) score was 117 (62 points for male age 10 points for respiratory rate greater than 29 15 points for temperature greater than or equal to 40C and 20 points for sodium less than 130 mEqL) which placed him in Risk Class IV
This estimated his 30-day mortality risk at 93
The patient received moxifloxacin 400 mg IV albuterol nebulized treatments and was admitted to the medicine service
Intravenous antibiotics were continued and the patientrsquos symptoms improved by hospital day 3 at which time he was afebrile with a room air oxygen saturation of 98
He was discharged on hospital day 4 to complete a ten-day course of oral moxifloxacin with close follow up arranged with his primary care provider
He was encouraged to stop drinking and was given resources to assist him
57
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
Case 2
Lab
bull A 67-year-old woman with mild Alzheimerrsquos disease who has a 2-day history of productive cough fever and increased confusion is transferred from a nursing home to the emergency department
bull According to the transfer records she has had no recent hospitalizations or recent use of antibiotic agents
PHYSICAL EXAMINATION
bull She is oriented to person only
bull Vital Signs
ndash Temperature is 384degC (101degF)
ndash Heart rate is 120 beats per minute
ndash The blood pressure is 14585 mm Hg
ndash The respiratory rate is 30 breaths per minute
bull The oxygen saturation is 91 while she is breathing ambient air
bull Crackles are heard in both lower lung fields
bull CBC
ndash The white-cell count is 4000mm3
bull The serum sodium level is 130 mEqL
bull BUN 25 mg dL (90 mmolL)
bull A radiograph of the chest shows infiltrates in both lower lobes
bull How and where should this patient be treated
The woman has a CURB-65 score of 4 suggesting that she would benefit from inpatient therapy
She has at least four minor criteria for severe community-acquired pneumonia (confusion respiratory rate ge30 breaths per minute multilobar infiltrates and uremia)
Although ICU admission may be prudent she would clearly benefit from further evaluation
We would measure the arterial blood gas and lactate levels given the high respiratory rate and low saturationand hydrate aggressively
As a nursing home resident the patient meets the current criteria for health carendashassociated pneumonia
However since she has no pneumonia-specific MDR risk factors but does have risk factors for severe community-acquired pneumonia we would initiate treatment with ceftriaxone and azithromycin
Influenza testing should be requested if she has presented during the appropriate season and empirical oseltamivir started if the local influenza rate is high
We would not obtain blood cultures or attempt to obtain sputum cultures because of the low likelihood of the presence of pathogens resistant to usual treatment for community-acquired pneumonia
58
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
Summary
bull Patients with CAP appropriate for the outpatient setting have a low mortality ndash (less than 1) compared to hospitalized patients who have a
mortality rate of approximately 15 bull Streptococcus pneumoniae is the most commonly diagnosed etiology of CAP
among hospitalized patients bull Laboratory tests have little use in outpatient management of patients with
CAP whereas tests obtained on admitted patients should include electrolytes blood urea nitrogen serum glucose and complete blood count (CBC)
bull Blood cultures should be obtained in seriously ill and admitted patients with CAP preferably before the initiation of antibiotics
bull Disease-specific prediction rules (eg Pneumonia Severity Index and CURB-65) can be used to assess the initial severity of pneumonia predict the risk of death and aid in deciding which patients diagnosed with CAP require hospital admission
59
THANK YOU
Questions Comments
60
THANK YOU
Questions Comments
60