[cancer research 36, 2958-2966, august 19761...
TRANSCRIPT

[CANCER RESEARCH 36, 2958-2966, August 19761
occurs most frequently after cumulative doses of 500 to 600mg/sq m. Characterization of the adniamycin and daunonubicin cardiomyopathy has been reported in humans byLefrak et a!. (18) and Buja et a!. (4); recently, Jaenke (15) hasdescribed a similar myocandial syndrome produced expemimentally in the rabbit. Myocandial lesions produced bychronic daunorubicin administration in rabbits were firstdescribed briefly by Mamabet a!. (20); since then it hasbecome obvious that the rabbit represents a convenientanimal model in which to study the pathogenesis of theadniamycmn-and daunonubicin-induced card iomyopathies.This investigation was conducted in order to study thecumulative and delayed nature of the adniamycin card iotoxicity in rabbits and to characterize progressive and nonrevemsible myocardial changes in the posttmeatment period.Recognition of these properties is important in minimizingthe cardiotoxic response in humans.
MATERIALS AND METHODS
A group of 75 male and female New Zealand White rabbitsweighing 2.7 to 3.4 kg received i.v. injections of 4%aqueous solutions of adniamycmnhydrochloride (FarmitaliaResearch Laboratories, Milan, Italy) supplied by the Laboratory of Toxicology, National Cancer Institute, Bethesda,Md., at a dose of 2.25 mg/kg/week given in 3 dividedinjections. Four treatment groups were utilized to examine4 total adniamycmndoses (Table 1). The 1st group (Group A)of 6 rabbits were scheduled to receive adriamycin for a totalof 77 days and were to be sacrificed at the end of thetreatment period. In 3 groups (Groups B, C, and D), replicates of 3 adniamycin-treated and 1 control rabbit receiving0.9% NaCI solution (0.2 mI/kg) (Group E) were included in
each treatment group ton sacrifice at predetermined intervals of the posttreatment period.
Evidence of bone marrow suppression was monitored byperiodic total leukocyte and hematocnit determinations. Semum enzymes were determined cobonimetnically (SigmaChemical Co. , St. Louis, Mo.) throughout the experiment toprovide indications of myocandial cellular damage. Creatinephosphokinase activity was expressed in Sigma units(nmoles of creatine phosphorybated per mm at 37°),andlactin dehydrogenase was expressed in Bengem-Broidaunits(@moles of pynuvate reduced per mm at 37°).
At necropsy, representative tissue samples of various ongan systems were fixed in buffered neutral fonmalin forhistopathobogical examination. The heart was divided intoatmialand ventricular portions and then the latter was sectioned in a routine manner, as shown in Chart 1. Myocardial
2958 CANCER RESEARCH VOL. 36
Delayed and Progressive Myocardial Lesions after AdriamycinAdministration in the Rabbft
Roger S. Jaenke2
Department of Pathology, Colorado State University, Fort Collins, Colorado 80523
SUMMARY
A candiomyopathy similar to that observed in cancer patients after prolonged chemotherapy with adniamycin canbe produced in the rabbit, characterized by mitochondnialand myofilamentous degeneration with noninflammatomymyolysis and connective tissue repair. The progressive anddelayed myocardial lesions produced in rabbits receivingincreasing total doses of adniamycin were studied after 23,35, 43, and 77 days of continuous treatment and in posttreatment periods up to 150 to 180 days after the last administration of adniamycin. Total adniamycin doses that produced increased serum enzyme, myocandial sodium, andcalcium levels but that failed to elicit serious myocandialmorphological lesions during the period of drug administration resulted in a delayed cardiomyopathy leaving focalareas of fibrosis and progressive lesions that became moresevere after discontinuation of drug administration. Thesefindings suggest that the myocardial effects of adniamycinare cumulative and potentially nonmeversible.
INTRODUCTION
Adniamycin and daunorubicin, 2 closely related anthracycline antibiotics isolated from cultures of Streptomycesspecies, are composed of an anthraquinone chromophoreand a 6-carbon amino sugar joined through a glycosidiclinkage. Both compounds are active against a variety ofexperimental animal tumors (2, 9) and recently have expenienced wide application as broad-spectrum antitumoragents in humans (2, 18, 21 , 22, 29). The anthracyclmneantitumom agents are reported to form complexes with DNAand thus to inhibit DNA replication and DNA-dependentRNA synthesis (10, 30), properties which apparently explaintheir cytotoxic and antimitotic activity.
In addition to their antitumor activity, adniamycin anddaunomubicin exhibit several undesirable toxic side effects,the most insidious of which is a cardiotoxicity that hasresulted in the establishment of maximal recommendedtotal drug doses (11, 18). The myocardial effects of thesecompounds in humans are of 2 types: (a) reversible altenations in the electrocardiogram which may occur at any totaldose bevel; and (b) irreversible congestive heart failure that
I This work was supported by Contract NIH-71-2i92 from the Division of
Cancer Treatment, National Cancer Institute, NIH, Department of Health,Education and Welfare.
2 To whom requests for reprints should be addressed.
Received December 8, 1975: accepted May 5, 1976.
Research. on August 22, 2018. © 1976 American Association for Cancercancerres.aacrjournals.org Downloaded from
Adriamycin treatmentgroupsTreat
mentgroupTotal
no. ofrabbitsTotal
dose(mg/sq m)Total
daystreatedPosttreatment
sacrifice time(days)A
B
CDE6
18
151521270
85
120160
Controls77
23
35430
0, 30, 60, 90, 120,180
0, 30, 60, 90, 1500, 30, 60, 90, 1800, 30, 60, 90, 120,
150, 180
Adriamycin Cardiotoxicity
Table rabbits; however, none of the treated group recovered fromthe early reduction in growth.
Serum creatine phosphokinase was elevated early in thetreatment period of all groups of rabbits receiving adniamycm and continued to rise as treatment continued (Chart 3).In the posttmeatment period of Groups B, C, and D, creatinephosphokinase values declined rapidly and by the end ofthe experiment had returned to control ranges (Chart 4).Serum lactate dehydrogenase levels also increased duringtreatment with adniamycin (Chart 3) and decreased in theposttneatment period in rabbits receiving the 85- and 120-mg/sq m total doses (Chart 4). However, in those rabbitsreceiving admiamycin at a total dose of 160 mg/sq m, lactatedehydnogenase values remained elevated throughout theperiod of observation.
Myocardial Lesions within Treatment Groups (Table 3).Two of 6 rabbits in Group A died in myocardial failure after72 days (260 mg/sq m) of continuous adniamycin treatment.All rabbits in this treatment group exhibited severe andextensive myocardial lesions at the time of death on at theend of the treatment period.
Chart 1. Method for sectioning ventricular myocardium for microscopicevaluation and electrolyte determination.
Microscopic criteria for scoring adriamycin-inducedcardiomyopathy
Qualitativescore°
1+ Early degeneration alterations, i.e. , vesiculation of myocardialcells
2+ Advanced degenerative alterations of myocardial cells, e.g.,altered cellular tintorial properties, intracellular inclusions,loss of myofilaments, and homogenization of the sarcoplasm
3+ Connective tissue proliferation and accompanying myofiberatrophy and degeneration
4+ Myofiber degeneration accompanied by myolysis and fibroplasia
Quantitative score―
1+ Involvement of single scattered myofibers at 1 or more bevels
2+ Involvementof focal groups of cells at 1 level
3+ Involvement of focal groups of cells at 2 or more levels
4+ Confluent areasof involvementat 1 or more levelsa The total score represents a composite of the qualitative and
quantitative evaluationof the lesion.
tissue fixed in buffered neutral formalin and embedded inparaffin was sectioned at 8 j.tm and stained with Masson'stnichrome on hematoxylin and eosin and examined histobogically at the plane of Sections 1, 2, and 3. Samples ofmyocandium taken between Sections 1 and 2 and the apexof the heart distal to Section Plane 4 were frozen ton totalelectrolyte determinations. Qualitative and quantitativescoring of the myocandial lesions was conducted on sections through Planes 1, 2, and 3, using the criteria of Table2. Tissues for electron microscopy were fixed in 3% glutaraldehyde, posttixed in 1.5% osmium tetroxide with 0.1 Mphosphate buffer, and embedded in Epon. Plastic sectionscut at 1 @mwere stained with methylene blue and Azure IIton light microscopy and orientation for thin sectioning.Silver-gray sections were cut on an LKB Ultramicrotome Ill,placed on 150 mesh copper grids, stained with unanyl acetate and lead citrate, and examined in an Hitachi HS 9electron microscope.
Myocardial tissue samples were dried in a vacuum oven(16 psi) at 80°ton 12 hr in porcelain cnucibles and ashed in amuffle furnace (Thermodyne Type 1400) at 550°for 12 hr.Ash was reconstituted with 5.0 ml of 20% hydrochloric acid,transferred to polyethylene bottles, and diluted to a totalvolume (actual weight) equal to 200 times the dry sampleweight. Total tissue calcium and magnesium levels werethen determined, and, after a 30-fold dilution with additionof ionization suppressant, sodium and potassium bevels,each expressed as mmoles/100 g of dry tissue, were determined by atomic absorption spectrophotometry.
RESULTS
Clinical Signs of Adriamycin Toxicity. Total leukocytecounts decreased (30%) after approximately 21 days in allrabbits receiving adniamycin and remained reducedthroughout the treatment period. The leukocyte counts meturned to normal ranges within 14 days after the last injection of drug. Hematocnits were decreased (11%) in rabbitstreated for periods greater than 42 days; these values alsoreturned to normal ranges within 14 days of the last adniamycin injection.
The weight of control rabbits continued to increase binearly for approximately 100 to 120 days, after which a plateau was reached at approximately 180% of the weight ofthe rabbit at the beginning of the experiment (Chart 2).While receiving admiamycin, rabbits had reduced weightgains as compared to controls. After receiving the last injection of drug, the rate of weight gains increased in surviving
‘SECTIONPLANE 2
SECTION PLANE 3
‘SECTIONPLANE 4
. MUSCLES
VENTRICLE
JMRIGHT
Table2
AUGUST 1976 2959
Research. on August 22, 2018. © 1976 American Association for Cancercancerres.aacrjournals.org Downloaded from

Scoring of myocardiallesions in adriamycin-treatedrabbitsMean
qualMeanNo.ofDays post itativequantita Meantotalrabbitstreatmentscoretive
scorescoreGroup
A (260-270mg/sq603.5+3.5+7.2+m;72-77days)GroupB(85mg/sqm;2330000days)3
333330
6090
1201800
01+000
00.7+000
01.7+0
0Group
C (120 mg/sqm;300.3+0.3+0.7+35days)3
33330
6090
1500.3+
1.0+0.3+3.0+0.3+
1.0+0.3+3.0+0.7+
2.0+0.7+
6.0+GroupD(l6Omg/sqm;43301.0+1.3+2.3+days)3
33330
6090
1801.3+
3.7+3.0+2.7+1.3+
2.7+2.7+3.7+2.7+
6.3+5.7+
6.3+Group
E (controls)33333330
306090
1201501800
0000000
0000000
000000
a
R. S. Jaenke
Myocandial lesions were absent in the initial 60 days posttreatment of rabbits receiving a total adniamycin dose of 85mg/sq m in 23 days. At 90 days posttneatment, 2 rabbitsexhibited degenerative changes in small numbers of myocardial cells located at the base of the left ventricle. Fur
wU)4z
0
0@
4I'J@z
wU
ITO a•050 a .MO a .@ •s•ss•
ISO a •a • • . o@oo@@oo
110 LPtOtO'o :@@-:a@ aa
‘Uz-J
za,
z
io 40 SO SO 100 ItO 140 @OMO toO ItO
DAYS
Chart 2. Weight gains of adriamycin-treated and control rabbits duringthe treatment and posttreatment periods. & Group A (260 to 270 mg/sq m):., GroupB(85mg/sqm):U,GroupC(120mg/sqm):0, GroupD(160mg/sq m): A, Group E (control): arrow, last day of treatment.
‘UU)4
b
hi
U
DAY OF TREATMENT DAY OF TREATMENT
Chart 3. Serum enzyme levels of adriamycin-treated and control rabbitsduring the treatment period. & Group A (260 to 270 mg/sq m): @,Group B(85 mg/sq m): S Group C (120 mg/sq m): 0, Group D (160 mg/sq m): A,Group E (control).
i:@!
w@
t;øi@:60
@°
400300
200100
40 60 80 100 @O i40 ISO ISODAY OF POSTTREATMENT
Chart 4. Serum enzyme levels of adriamycin-treated and control rabbitsduring the posttreatment period. & Group A (260 to 270 mg/sq m): •.GroupB (85 mg/sq m):@ , Group C (120 mg/sq m): 0, Group D (160 mg/sq m): A,Group E (control).
Table 3
2960 CANCERRESEARCHVOL. 36
Research. on August 22, 2018. © 1976 American Association for Cancercancerres.aacrjournals.org Downloaded from

Adriamycin Cardiotoxicity
then myocardial lesions were absent at subsequent sacrificetimes of 120 and 180 days.
Rabbits receiving a total admiamycin dose of 120 mg/sq min 35 days showed, in the initial 90 days posttreatment, onlyoccasional evidence of mild, focal myocardial cellular degeneration at the base of the left ventricle and septum.However, 150 days after the last injection of admiamycin,focal areas of intense myofiben degeneration and atrophyaccompanied by fibrosis were found in multiple locations ofthe left ventricle and septum (Fig. 1).
Rabbits receiving adniamycin (160 mg/sq m) during atreatment period of 43 days developed increasingly severemyocandial lesions in the posttneatment period. At 0 and 30days after the end of the treatment period, small numbers ofvesiculated cells characteristic of early myotiber degeneration were present in the left ventricle and septum of treatedrabbits. At 60 days, however, more severe myofiben degenenation and fibrosis with loss of myotibens were present atmultiple levels of the left ventricle and septum. In subsequent periods, i.e. , 90 and 180 days after the last adniamycininjection, large areas of severe degeneration and atrophy ofcardiac myocytes along with myolysis and diffuse fibrosiswere present (Fig. 2).
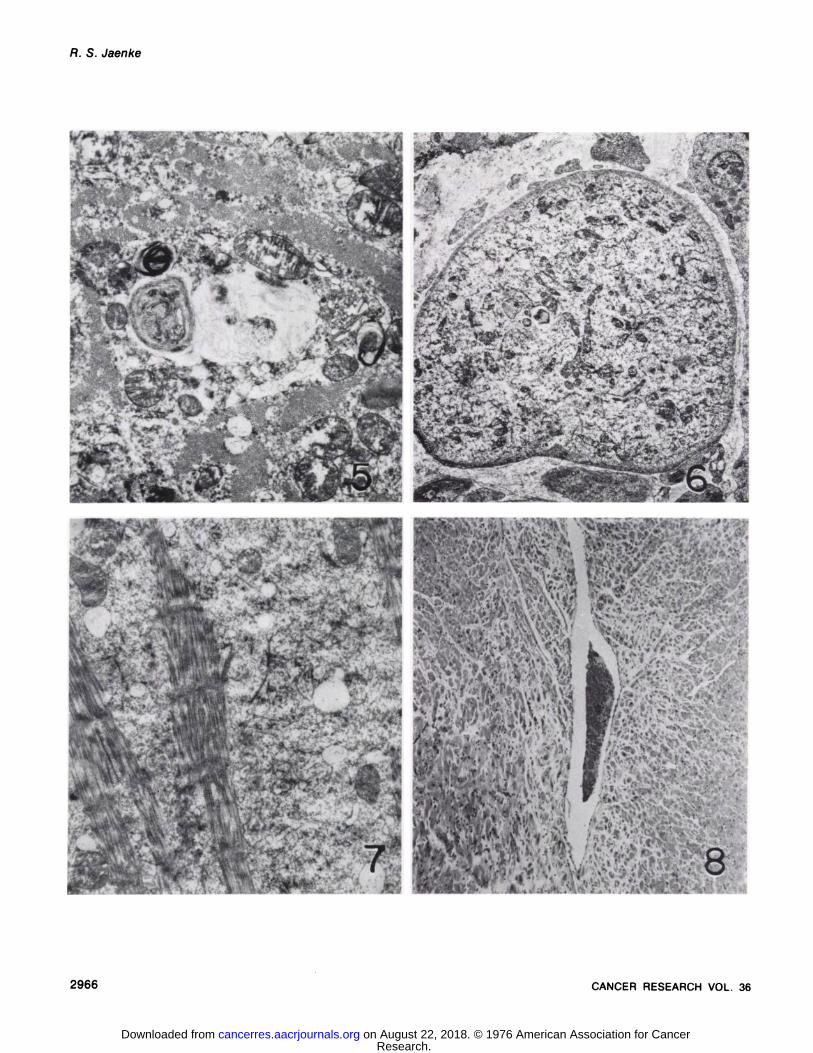
Character of the Myocardial Lesion. The microscopicfeatures of the myocardial cellular alterations in the GroupA, chronically treated rabbits were similar to those reportedin detail previously for the rabbit (15). The earliest cardiacalteration noted was a characteristic vesiculation of myocardial cells (Fig. 3). The sancoplasm of these myofibenshad a typical lace-like appearance formed by lange, cleftshaped, clean spaces bordered by myofilamentous bundles.Later, evidence of more severe myocardial cell injury wasnoted (Fig. 4). Focal to diffuse areas of cytoplasmic degnadation appeared, resulting in a loss of subcellulan structuralelements and a consequent homogenization of the sarcoplasm. Particularly evident in many fibers were severe mitochondmial degeneration and the formation of multilaminatedmyelin whorls (Fig. 5).
A prominent feature of the sancoplasmic degradation frequently included the loss of myofilaments and progressiveatrophy of myofibens (Figs. 4 and 6). Affected fibers, although still viable, were depleted of contractile elementsand contained only tangled remnants of filaments and inmegubanpleomorphic mitochondnia (Figs. 6 and 7).
Groups B, C, and D received total adniamycin doses thatin previous studies generally failed to produce microscopicevidence of severe myofiber degeneration or myolysis andresulted in no apparent myocandial deaths during the treatment period. All rabbits in these treatment groups remainedin good health throughout the posttneatment period. How
even, as shown above, a delayed and progressive card iomyopathy was observed in many rabbits after discontinuationof adniamycin administration . Although the subcellulan degnadative features in the posttreatment period were similar inthese animals and in those receiving continuous, chronicadniamycmntreatment, loss of myofilaments and progressivemyofibem atrophy accompanied by connective tissue pmobiferation became increasingly prominent in the posttneatmentperiod. In Group C, fibmoplasia accompanied by myofiberdegenerative alterations was focal in distribution (Fig. 1)
and was not observed until late in the posttreatment period(150 days). In Group D rabbits, chronic, active myofibendegeneration accompanied by connective tissue repair became progressively more severe and diffuse in the left yentnicle and septum after cessation of adniamycin administration (Fig. 2). In many areas of the myocardium, the connective tissue response appeared to be disproportionate to themyofibemchanges, resulting in secondary atrophy and add itionab bossof myocandial cells. Infiltrations of inflammatorycells in general were absent throughout the observationperiod except for occasional phagocytic cells seen in thevicinity of some severely degenerative myocardial cells.
Distribution of the Myocardial Lesions. The earliest myofibemchanges were seen in the left ventricle at the base ofthe heart in close association with the annulus fibrosis andat the tips of the anterior and posterior papillary muscles ofthe left ventricle. Later, myofiber degenerative changes became more generalized in the left ventricle and septum.Occasionally, interstitial fibrosis, accompanied by myofibemdegeneration and atrophy, was particularly intense at thebase of the papillary muscles, resulting in thinning of theventricular wall at this site. Involvement of the subendocandial regions of the left ventricle was also prominent in laterstages (Fig. 2). Frequently, intense degeneration and fibrosis were seen around coronary arteries and veins (Figs. 1and 8); however, lesions of the vessel wall were not apparent. Although the myocardium of the septum adjacent to theright ventricle was often involved, the night ventricular wallwas seldom affected at the total doses used in this investigation.
Myocardial Electrolytes. Total myocandial electrolyteswere determined at the end of each treatment period and ateach sacrifice time in the posttneatment period. Potassiumand magnesium levels of treated rabbits were not significantly different from controls. One of the most consistentchanges noted was an increase in myocardial sodium inadniamycin-treated rabbits at the end of their respectivetreatment periods (Table 4). In subsequent posttmeatmentsacrifice times, however, total myocardial sodium levelswere not observed to be significantly diffement from those ofcontrols. In addition to changes in myocardial sodium, anincrease in total myocardial calcium was also observed atthe end of each of the treatment periods but not at subsequent posttreatment sacrifice times. Although the rabbits inGroup A exhibited severe morphological changes at necropsy, the rabbits in Group B exhibited no myocandiablesions, and those in Groups C and D exhibited only earlydegenerative changes in the myocardium at the end of thetreatment periods. Apparently, then, myocamdial electrolytealterations precede the development of structural changes.
DISCUSSION
The myocardial effects of adniamycin and daunonubicin inhumans are manifest in 2 ways: (a) as transient ECG3changes that disappear with discontinuation of drug administration or even while drug administration continues; and
3 The abbreviation used is: ECG, electrocardiogram.
AUGUST1976 2961
Research. on August 22, 2018. © 1976 American Association for Cancercancerres.aacrjournals.org Downloaded from

Myocardial electrolytes at end of treatmentperiodmmoles
of ebectrobyte/100g ventricularmyocardium@'Sodi
urn Potassium CalciurnMagnesiumWet
Dry Wet Dry Wet DryWetDryGroupA (260—270mg/sq rn, 72-77
days)N = 34.7922.97b 6.06 28.90 0.17e 0.81d
±0.26 ±0.84 ±0.88 ±2.03 ±0.04 ±0.180.763.63
±0.04±0.12Group
B (85mg/sq rn,23days)N =3557d
2570― 7.14 32.90 0.15 0.69b±1.12 ±2.77 ±0.72 ±2.03 ±0.01 ±0.100.82
3.85±0.03±0.06Group
C (120mg/sq m, 35 days)N= 34.48
23.70― 5.79 28.00 0.15 O.71d±0.45 ±1.15 ±1.07 ±4.00 ±0.01 ±0.060.79
3.85±0.05±0.19Group
0 (160mg/sq m, 43 days)N= 35.00
23.50 6.26 28.47 0.15 0.69b±0.06 ±1.70 ±0.56 ±2.04 ±0.10 ±1.100.80
3.74±0.06±0.04Group
E (controls) N = 184.49 19.36 6.19 26.71 0.14 0.61±0.46 ±2.05 ±0.99 ±4.44 ±0.01 ±0.030.80
3.47±0.05 ±0.32
R. S. Jaenke
Table 4
a Mean ±SE.bp > 0.010.
(‘p> 0.005.dp < 0.001.
(b) as a fulminating syndrome of congestive myocandialfailure that is usually delayed and appears to result fromcumulative drug toxicity to the myocardium. ReversibleECG changes are usually not accompanied by other signs ofmyocardial damage (6, 16, 29) and are described by someauthors as nonspecific and a consequence of widespreadtumor metastasis or other debilitating disease (26). Undercertain circumstances, however, myocardial disease attnibuted directly to admiamycin or daunorubicin occurs (19).Fatal drug-induced cardiomyopathies occur primarily aftercumulative doses greaten than 500 to 600 mg/sq m with anincidence of less than 1% at lower doses and an incidenceas great as 30% at higher doses (11, 13, 18). In someinstances, myocandial failure reportedly occurs severalweeks after the last administration of drug (12, 18). Thus, itappears that adriamycin and daunorubicin cardiotoxicityare both cumulative and progressive on potentially nonmeversible .
The present study has demonstrated in an experimentalanimal model, the rabbit, an adniamycin-induced myocardial syndrome which was accompanied by bone marrowsuppression and was heralded by serum enzyme elevationsthat may remain elevated in the presence of continued,progressive degeneration. After chronic, continuous adniamycin administration to rabbits (Group A), some rabbitsdied in myocardial failure while all exhibited severe myocamdial left ventricular degeneration and loss of myofibers. Atlower total adriamycin doses, myofiber alterations at theend of the treatment period were generally absent on werelimited to early degenerative changes that morphologicallyare considered to represent reversible pathological cellularalterations (28). However, in the posttreatment period, afterdiscontinuation of drug administration, a delayed progressive cardiomyopathy developed in surviving animals. Theseobservations indicate that, in rabbits, total adniamycindoses that are not characterized by immediate fulminatingmyocardial disease may progress in the absence of continued drug administration to severe myocardiab damage.
Adniamycin and daunorubicin are administered to cancerpatients by a variety of dosage schedules; however, mostschedules permit periods of 14 to 21 days between drugadministrations. Admiamycin is taken up rapidly by the heartas well as by the lungs and liven, but levels in these tissuesdecrease rapidly within 8 hr postinjection as the drug isexcreted rapidly in the feces and urine (7, 8). After a rapiddecrease of initial blood and plasma levels, adniamycin 1evels remain constant for 7 to 10 days. Based on these findings it has been suggested that the appropriate dose schedule for adniamycin should be intermittent with intervals ofapproximately 21 days between courses to provide maximaltherapeutic response with the least toxicity. In studies ofexperimental admiamycin cardiotoxicity in the rabbit, drugwas administered at more frequent intervals of every threeto four days continuously for up to 11 weeks. Under theseconditions, adniamycmnlevels are likely to remain high continuously during the treatment period, which may explainthe higher incidence of myocardial lesions at lower totaldoses in chronically treated animals. These findings mdicate that more prolonged intervals between adniamycin injections may be useful in reducing the drug-associated myocardial toxicity. It appears, however, that continuous highserum and tissue admiamycin levels are not required formyocardial damage. In the present study, progressive myocardial lesions were observed during the posttmeatmentperiod of rabbits that received total admiamycin doses causing minimal myofibem morphological alterations at the endof the treatment period. This observation suggests a cumulative and persistent drug toxicity to the myocandium andthat, after some critical total admiamycin dose, irreversiblealterations in myofiber cellular metabolism are initiated thatmay result in delayed myocardial disease on may influencesubsequent administrations of drug.
A consistent, specific distribution of myocandial lesionsthat included the left ventricular free wall and septum wasobserved in the rabbit model. Although the night ventricularwall was not affected in this investigation, previous studies
2962 CANCER RESEARCH VOL. 36
Research. on August 22, 2018. © 1976 American Association for Cancercancerres.aacrjournals.org Downloaded from

Adriamycin Cardiotoxicity
with higher total doses did demonstrate that this portion ofthe myocardium was not completely resistent to the effectsof adniamycmnon daunonubicin (15). The presence of earlydegenerative and late fibrosing reactions at the base of theleft ventricle and septum in the rabbit would be expected toinvolve conducting pathways of the heart and might thenexplain the alterations in the EGG commonly observed duning all phases of drug administration (6, 16, 29). SimilarEGG changes have been observed in rabbits (C. Bier, man uscript in preparation). Lesions at the base of the left ventnicle near the attachment of the atnioventnicular valves, thedistal end of the papillary muscles which serve as the attachment of the condae tendineae, and the attachment ofthe papillary muscles at the apex of the left ventricle mayrepresent sites of predilection represented by areas of panticular stress in the ventricular musculature. The penivascuIanand subendocandial orientation of lesions also suggestsa possible vascular basis to the admiamycmn-mnducedlesions.Rona et a!. (27) have referred to the subendocardium as avascularly “handicapped―region.
The mechanism responsible for the adniamycin-inducedcandiomyopathy remains undefined. On the basis of thefindings of several laboratories, 3 possible modes of actionwarrant consideration: (a) interference with protein synthesis and subcellulam onganelbeturnover, (b) alteration of cononamyblood flow resulting in cellular hypoxia, and (c) directtoxic degradation of specific subcellular structural andfunctional components ofthe myocandial cell. Bujaeta!. (3,4) have described ultrastructunal alterations in the nuclei ofmyocardial cells of patients dying from daunorubicin-associated cardiomyopathies that were interpreted as unraveling and uncoiling of chromatin. Recognizing the DNA-intercalating ability of this class of compounds, it was suggestedthat such alterations are of importance in the pathogenesisof the anthracycline-induced candiotoxicity. Similar nuclearalterations have not been observed in the rabbit; however,progressive disappearance of myofibmils and cellular atmophy are prominent microscopic features of the candiomyopathy. The delayed nature of the myocandial lesion suggests primary damage to a cellular system capable of surviving initial toxic doses of drug. Although preexisting RNAmay be sufficient to meet the protein synthesis requirements of the myocardial cells and to prevent morphologicaldamage initially, further DNA-dependent RNA synthesiseventually is required to replace structural and functionalproteins such as myotibnils and mitochondnia lost duringprotein metabolism and turnover. Myocandial cells exposedchronically to admiamycin may be incapable of such synthesis.
Myocandial ischemia resulting from coronary arterial disease represents the most common cause of myofibem degeneration and necrosis. The pemivascular orientation ofmyofibem alterations noted in some myocardial sections ofadniamycin-treated rabbits suggests a possible vascularbasis for the lesion . It should be noted , however, that vascubar lesions were absent in the rabbit and, further, that themyofibem alterations were frequently associated with largeconducting branches of the coronary arteries rather thanwith end arterioles. The absence of vascular lesions doesnot necessarily preclude this mechanism, however, as studies by Herman and Vick (14) suggest that daunorubicin may
produce myocardial hypoxia due to increased coronary vasoactivity. However, a pemivascular distribution of lesions inthe heart has also been observed in nonvasculan card iomyopathies, which indicates that predilection for this site maycarry implications other than myofiber ischemia (1). Theperivenous distribution of lesions also suggests a nonhypoxic mechanism.
A variety of cardiotoxic agents have been investigated,some of which possess specific sites of action within themyocandial cell. Recognition of prominent mitochondniallesions in the admiamycin- and daunorubicin-induced cardiomyopathy of the rabbit (15) has prompted investigationof the effects of this group of antibiotics on mitochondniabmetabolism (5). However, initial studies have failed to demonstrate in vivo an effect on mitochondnial function thatsatisfactorily explains the morphological alterations inthese onganebbes. Although some antibiotics have beenshown to act as specific inhibitors of electron transport (17),others interfere indirectly with mitochondnial functionthrough alterations in electrolyte movements (23). Recently,considerable interest has been focused on the moleof electnolyte metabolism in the genesis of myocardial lesions (25).In the present study, increased myocardial sodium and calcium content was noted at the end of the adniamycmntreatment periods. Similar findings have been reported by Olsonet a!. (24) in chronic admiamycin-treated rabbits. Since structural lesions were absent at the end of the 23-day treatmentperiod (Group B), it would appear that electrolyte changesprecede the morphological manifestations of the card iomyopathy. Previous morphological studies of rabbits (15), aswell as the present study, have demonstrated early compartmental swelling in myocardial cells, which representsevidence of loss of cell volume control possibly related toalterations in electrolyte distribution. Studies by Trump eta!. (28) suggest that these cellular alterations may resultfrom increased permeability of the cell membrane or decreased activity of the energy-dependent ion pump locatedwithin the membrane. One must consider, therefore, thatthe mitochondnial and myofilamentous lesions observedmay be secondary to adniamycin-induced alterations in myocandial electrolyte metabolism and that these early ionicdisturbances may also be responsible for the electrocardiogmaphic changes commonly noted during adniamycin administration.
ACKNOWLEDGMENTS
The author wishes to thank Patricia McMurry and Christy Morris for theirtechnical assistance.
REFERENCES
1. Bajusz, E. The Terminal Electrolyte-Shift Mechanism in Heart Muscle: ItsSignificance in the Pathogenesis and Prevention of Necrotizing Cardiomyopathies. In: E. Bajusz (ed), Electrolytes and Cardiovascular Diseases, pp. 274-322. Basal: S. Karger AG, 1965.
2. Bonadonna, G., Monfardini, 5., deLena, M., Fossati-Bellani, F., andBeretta, G. Phase I and Preliminary Phase II Evaluation of Adriamycin(NSC-123127). Cancer Res., 30: 2572-2582, 1970.
3, Buja, L. M., Ferrans, V. J., Mayer, R. J., Roberts, W. C., and Henderson,E. S. Cardiac Ultrastructural Changes Induced by Daunorubicin Therapy.Cancer, 32: 771-788, 1973.
4. Buja, L. M. , Ferrans, V. J. , and Rabson, A. S. Unusual Nuclear Alterstions. Lancet, 1: 402-403, 1974.
AUGUST 1976 2963
Research. on August 22, 2018. © 1976 American Association for Cancercancerres.aacrjournals.org Downloaded from

R. S. Jaenke
5. Cargill, C., Bachmann, E., and zbinden, G. Effects of Daunomycin andAnthramycin on Electrocardiogram and Mitochondrial Metabolism of theRat Heart. J. NatI. Cancer Inst., 53: 481-486, 1974.
6. Cortes, E. P., Ellison, R. R., and Yates, J. W. Adriamycin (NSC-123127) inthe Treatment of Acute Myelocytic Leukemia. Cancer ChemotherapyRept., 56: 237-243, 1972.
7, DiFronzo, G. , Gambetta, R. A. , and Lenaz, L. Distribution and Metabolism of Adriamycin in Mice. Comparison with Daunomycin. Rev. Europeene D'etudes Clin. Biol., 16: 572-576, 1971.
8. DiFronzo, G. , Lenaz, L. , and Bonadonna, G. Distribution and Excretionof Adriamycin in Man. Biomedicine, 19: 169-171 , 1973.
9. DiMarco, A. , Gaetani, M., and Scarpinato, B. Adriamycin, A New Antibiotic with Antitumor Activity. Cancer Chemotherapy Rept., 53: 33-37,1969.
10. DiMarco, A., Silvestrini, R., DiMarco, S., and Dasdia, T. Inhibiting Effectof the New Cytotoxic Antibiotic Daunomycin on Nucleic Acids and Mitotic Activity of HeLa Cells. J. Cell Biol., 27: 545-550, 1965.
11. Gottlieb, J. A., Lefrak, E. A., O'Brien, P. M., and Burgess, M. A. FatalAdriamycin Cardiomyopathy: Prevention by Dose Limitation. Proc. Am.Assoc. Cancer Res., 14: 88, 1973.
12. Greene, W., Huffman, D., Wiernik, P. H., Schimpff, S., Benjamin, R., andBachur, N. High-dose Daunorubicin Therapy for Acute NonlymphocyticLeukemia: Correlation of Response and Toxicity with Pharmacokineticsand Intracellular Daunorubicin Reductase Activity. Cancer, 30: 1419-1427, 1972.
13. Halazun, J. F., Wagner, H. R., and Sinks, L. F. Daunorubicin CardiacToxicity in Children with Acute Leukemia. Proc. Am. Assoc. Cancer Res.,13: 61, 1972.
14. Herman, E. H., and Vick, J. A. The Acute Pharmacological Actions ofDaunomycin in the Dog and Monkey. Pharmacology, 3: 291-304, 1970.
15. Jaenke, R. S. An Anthracycline Antibiotic-Induced Cardiomyopathy inRabbits. Lab. Invest., 30: 292-304, 1974.
16. Klener, P., Donner, L. , and Kozena, J. Daunorubicin and Adriamycin inthe Treatment of Leukemia. Neoplasma, 20: 87-97, 1973.
17. Lardy, H. A., Johnson, D., and McMurry, W. C. Antibiotics as Tools forMetabolic Studies. I. A Survey of Toxic Antibiotics in Respiratory, Phosphorylative and Glycolytic Systems. Arch. Biochem. Biophys., 78: 587-597, 1958.
18. Lefrak, E. A., Pitha, J., Rosenheim, S., and Gottlieb, J. A. A Clinicopathologic Analysis ofAdriamycin Cardiotoxicity. Cancer, 32: 302-314, 1973.
19. Macrez, C., Marneffe-Lebrequier, H., Ripault, J., Clauvel, J. P., Jacquillat, C. , and Weil, M. Accidents Cardiaques Observes au Cours desTraitements par Ia Rubidomycine. Pathol. Biol. Semaine Hop. , 15: 949-953, 1967.
20. Maral, A., Bourat, C., Ducrot, R., Fournel,J., Ganter, P., Julow, L.,Koenig, F., Myon, J., Pascal, S. , Pasquet, J. . Populaire, P., deRatuld, Y.,and Werner, G. H. Etude Toxicologique et ActivitéAntitumorale Experimentale de Ia Rubidomycine (13-057RP). Pathol. Biol., Semaine Hop.,15: 903-918, 1967.
21. Middleman, E., Luce, J., and Frei, E. Clinical Trials with Adriamycin.Cancer, 28: 844-850, 1971.
22. O'Bryan, R. M., Luce, J. K., Talley, R. w., Gottleib, J. A. , Baker, L. H.,and Bonadonna, G. Phase II Evaluation of Adriamycin in Human Neoplasia. Cancer, 32: 1-8, 1973.
23. Ogata,E., andRasmussen,H.ValinomycinandMitochondrialIonTransport. Biochemistry, 5: 57-66, 1966.
24. Olson,H.M.,Young,D.M., Prieur,D.J., LeRoy,A.F.,and Reagan,R.L.Electrolyte and Morphologic Alterations of Myocardium in AdriamycinTreated Rabbits. Am. J. Pathol., 77: 455-466, 1974.
25. Raab, W. Myocardial Electrolyte Derangement: Crucial Feature of Pluricausal, So-called Coronary Heart Disease. Ann. N. V. Acad. Sci., 147:627-686, 1969.
26. Romano, C., Pongiglione. R., Raffaelli, E. , and Fossati, A. ECG Findingsin 34 Children Treated with Daunomycin. Minerva Pediatr., 22: 71-75,1970.
27. Rona, G., Kahn, D. S., and Chappel, C. J. The Effect of Electrolytes onExperimental Infarct-Like Myocardial Necrosis. In: E. Bajusz (ed), Electrolytes and Cardiovascular Disease, Vol. 1, pp. 181-191 . Basel: S.Karger AG, 1965.
28. Trump, B. G. , Croker, B. P., and Mergner, W. J. The Role of EnergyMetabolism, Ion and Water Shifts in the Pathogenesis of Cell Injury. In:G.W. Richterand0. G.Scarpelli(eds.),CellMembranes:BiologicalandPathological Aspects, pp. 84-128. Baltimore: The Williams & Wilkins Co.,1971.
29. Wang,J. J.,Cortes,E.,Sinks,L. F.,andHolland,J. E.TherapeuticEffectand Toxicity of Adriamycin in Patients with Neoplastic Disease. Cancer,28: 837-843,1971.
30. Ward, D. C., Reich, E., and Goldberg, I. H. Base Specificity in theInteraction of Polynucleotides with Antibiotic Drugs. Science, 149: 1259—1263, 1965.
Fig. 1 . Focal area of myofiber degeneration adjacent to large coronary artery. Accompanying the degeneration and loss of myocardial cells are proliferation of connective tissue and associated myofiber atrophy. Adriamycin-treated rabbit, 120 mg/sq m, 150 days posttreatment. Masson's trichrome, x 65.
Fig. 2. Severe and diffuse myocardial degeneration and loss of myofibers accompanied by intense fibroplasia in the subendocardium and midventricularwall. Arterial vessels included in lesion have widely patent lumina with no apparent intimal or medial lesions. Adriamycin-treated rabbit, 160 mg/sq m, 180days posttreatment. Masson's trichrome, x 40.
Fig. 3. Early vesiculation of myocardial cells. Adriamycin-treated rabbit. Methylene blue and Azure II, x 490.Fig. 4. Advanced myofiber lesions with extensive myofilamentous loss and homogenization of the sarcoplasm. Myofibers are irregular in size and shape
andoften appearatrophic. Adriamycin-treatedrabbit. Methyleneblue and AzureII, x 490.Fig. 5. Mitochondrial degeneration accompanied by the formation of myelin whorls. Adriamycin-treated rabbit. Uranyl acetate and lead citrate, x 13,000.Fig. 6. Low-power electron micrograph of cross-sectioned myocardial fiber showing complete loss of myofilamentous bundles. Irregular, small mitochon
dna are distributed among filamentous debris. Adriamycin-treated rabbit. Uranyl acetate and lead citrate, x 3,900.Fig. 7. Electron micrograph of longitudinally sectioned myocyte showing disorientation and disintegration of myofilamentous bundles. Sarcoplasm
contains tangled, disorganized filaments and small mitochondria. Adriamycin-treated rabbit. Uranyl acetate and lead citrate, x 13,000.Fig. 8. Perivenous distribution of myofiber degeneration and fibrosis. Adriamycin-treated rabbit, 160 mg/sq m, 180 days posttreatment. H & E, x 60..
2964 CANCER RESEARCH VOL. 36
Research. on August 22, 2018. © 1976 American Association for Cancercancerres.aacrjournals.org Downloaded from

Adriamycin Cardiotoxicity
‘ ‘-. ‘::‘@e ..‘@ ‘@‘@
,‘.@@ @%‘.4@Ø
.@ . , ..@ . .@@@
‘4..@.; . - @@‘-:@:@@ : . .. @‘@ ‘@@@ ‘@ ‘ @@‘-@@
-‘@:‘@‘@@
,..st@ @‘@ :: .@.@@ ‘@TA:.@@ ..;,@‘‘, .-.‘.@ :“ .:@ ..@ .:@
‘‘@..* ‘@ ‘S.@
@@ I
.$,t@'@@ ‘;@;,3@1@:.@ - .. #,‘, 4.@
@:-@@@ .@ @-@ ‘@ @@e',@@ ‘@@ . .
-‘.‘- @J,@@ L, :;
@ @‘
@ .@@ “).
.‘@.
@-,
@.
4
AUGUST 1976 2965
Research. on August 22, 2018. © 1976 American Association for Cancercancerres.aacrjournals.org Downloaded from
‘-@ - ... @@‘c @“
@ @:.r:@@‘1―:.., @,‘.. . .
@ .‘,.;@ ...‘
,.t 7 1.@ • ‘@.‘....I.'.@,.'.. ‘@ @‘
. ‘, 1• â€.̃ •• •
,‘@@ a'@,•:.,‘@,‘•@ i, ‘1
@i' . : ..@.‘ @•;@ .
. . .@I_@ •,. S @,.,.. I ‘@ @@@‘@:‘•‘@@@
L@
@. k'
@k' ,).@-@ .t': ..,.“..@ ,‘@@ •@•@., ,‘@‘.‘.@ †.̃ . . .. a ‘@ , ,@ . , . ‘
eV “, a
t :@@@@
‘.,@ .@ . :@ @‘
‘. 4@@ @‘ •‘@ @‘.
.@.@ :“ :/@:Y;.@;;
:.-@@
@ @‘@
..@.:1:i:@@@@:;@ :‘@
r@-. £
&@%a@@@ ‘@ @‘
@ y.
;“@‘-@. .,
.4 @•
. ‘
2966 CANCERRESEARCHVOL. 36
A. S. Jaenke
@ :; .@@@
@ :i@*@ ‘@@ l@[email protected];
@@ ‘@@@@@@@@
@ • -@.@
Research. on August 22, 2018. © 1976 American Association for Cancercancerres.aacrjournals.org Downloaded from

1976;36:2958-2966. Cancer Res Roger S. Jaenke Administration in the RabbitDelayed and Progressive Myocardial Lesions after Adriamycin
Updated version
http://cancerres.aacrjournals.org/content/36/8/2958
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/36/8/2958To request permission to re-use all or part of this article, use this link
Research. on August 22, 2018. © 1976 American Association for Cancercancerres.aacrjournals.org Downloaded from