cancer of the gallbladder associated with anomalous junction of the pancreatobiliary duct system...
TRANSCRIPT

Br. J. Surg. 1993, Vol. 80, May, 622-624
K. Tanaka, A. Nishimura, K. Yamada, R . Ishibe, N. Ishizaki, M. Yoshimine, N. Hamada and A. Taira
Second Department of Surgery, Faculty of Medicine, Kagoshima University, 35- 7 Sakuragaoka 8-chomeP Kagoshirna 890, Japan Correspondence to: Dr K . Tanaka
Cancer of the gallbladder associated with anomalous junction of the pancreatobiliary duct system without bile duct dilatation
The aim of this study was to delineate clinical features and prognosis of cancer of the gallbladder associated with anomalous junction of the pancreatobiliary duct system without bile duct dilatation, and to determine methods for managing the disease. A retrospective study of seven patients is presented. A further 27 cases f rom the Japanese literature were reviewed retrospectively with regard to method of treatment and prognosis. In I1 of 18 patients in whom staging was known the tumour was stage V, representing advanced disease. In seven of 34 cases curative operation was performed; only two patients survived for > 3 years. This poor outcome was due largely to delayed diagnosis of cancer of the gallbladder. Prophylactic cholecystectomy is recommended in patients with this anomalous junction without bile duct dilatation or a malignant lesion in the gallbladder, because of the high incidence of cancer of the biliary tract.
Anomalous junction of the pancreatobiliary duct system is a congenital defect defined as the union of the pancreatic and biliary ducts located outside the duodenal wall. Pancreatic juice refluxes into the common bile duct (CBD), or bile juice regurgitates into the pancreatic duct, because the action of the sphincter muscle does not affect the union functionally. Accordingly, there may be various complications such as cholangitis, gallstones, biliary cancer, pancreatitis and pancreatolithiasis' .
Attention has recently focused on the high incidence of cancer of the biliary tract in this The incidence of malignant change has been reported as 15-40 per There is an especially high incidence of cancer of the gallbladder in anomalous junction without bile duct dilatation.
The purpose of this study was to delineate clinical features and prognosis of cancer of the gallbladder accompanying this anomaly, and to determine a management strategy for the disease.
Patients and methods During the 15 years between January 1977 and December 1991, 32 adults with anomalous junction of the pancreatobiliary duct system have been treated in this department. Of these patients, 24 had cystic, fusiform or cylindrical dilatation of the CBD and the other eight no dilatation. Three of the 24 patients and seven of the eight had biliary tract cancer (eight gallbladder, two bile duct). Seven patients with gallbladder cancer without bile duct dilatation are reviewed retrospectively.
The diagnosis of anomalous junction was based on the presence of a long common channel and the anomalous form ofjunction, according to published criteria'. The mean age was 60.7 (range 43-77) years; there were two men and five women. The tumour was staged according to the criteria of Nevin et ~ 1 . ~ : stage I, intramucosal only; 11, involvement of mucosa and muscularis; 111, involvement of all three layers; IV, involvement of all three layers and the cystic lymph nodes; and V, involvement of the liver by direct extension or metastasis, or metastasis to any other organ.
Results Clinicopathological features are summarized in Tables 1 and 2. The majority of patients were first seen with abdominal pain.
Cervical lymph node swelling was noted in one. One patient (no. 5) was free from symptoms related to the disease; a mass in the gallbladder was discovered at ultrasonography for abdominal aneurysm. Serum carcinoembryonic antigen levels were abnormally high in two cases. The diagnosis of cancer of the gallbladder was made before operation in all patients. Maljunction was detected by preoperative endoscopic retro- grade cholangiopancreatography in four patients and by intraoperative cholangiography in three.
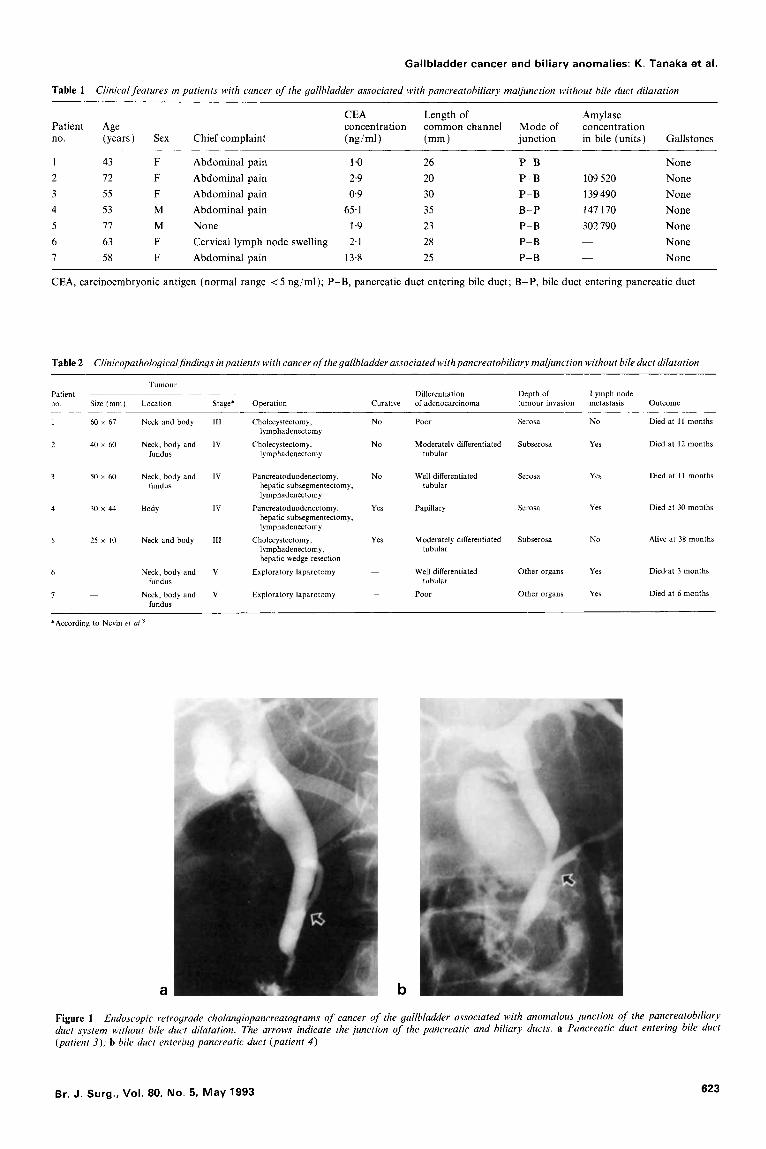
The mean length of the common channel was 26.7 (range 20-35) mm. The mode of junction in six cases was with the pancreatic duct entering the bile duct; in one case the bile duct entered the pancreatic duct. Two cholangiopancreatograms representative of the anomaly are shown in Figure 1 . The amylase level in the bile, determined in four patients, was very high. There were no gallstones in any case. In only two patients was the tumour limited to the gallbladder wall (stage 111).
Surgical resection was possible in the two patients with stage 111 disease, and in the three with stage IV tumours (Table 2). In the two patients with stage V disease, only laparotomy and tumour biopsy were performed because of massive invasion of the liver and distant metastasis.
In three patients (nos 1, 2 and 3) the resection performed was considered non-curative because of tumour involvement at the resection margin. Curative resection was performed in only two cases. Lymph node involvement was present in five patients; histological diagnosis is shown in Table 2. There was no operative death. One patient who underwent curative operation is still alive after 38 months. The other six patients died from progression of the tumour within 3-30 months.
Reuiew of the Japanese literature A total of 34 cases were reviewed: the present seven and a further 27 from the Japanese l i t e r a t ~ r e ' . ~ - ~ ~ , of cancer of the gallbladder accompanied by the anomaly without bile duct dilatation, for which the method of treatment and prognosis had been described adequately. In 18 cases tumour stage had been determined using the criteria of Nevin er aL8. Only two patients had stage I11 disease; the other 16 had stage IV or V tumours.
622 0007-1323/93/050622-03 0 1993 Butterworth-Heinernann Ltd
Gallbladder cancer and biliary anomalies: K. Tanaka et al.
Table 1 Clinical features in patients with cancer of the gallbladder associated with pancreatobiliary maljunction without bile duct dilatation
CEA Length of Amylase Patient Age concentration common channel Mode of concentration no. (years) Sex Chief complaint (nglml) (mm 1 junction in bile (units) Gallstones
1 43 F Abdominal pain 1 .o 26
3 55 F Abdominal pain 0.9 30
5 17 M None 1.9 23 6 63 F Cervical lymph node swelling 2.1 28 7 58 F Abdominal pain 13.8 25
2 12 F Abdominal pain 2.9 20
4 53 M Abdominal pain 65.1 35
~ P-B None P-B 109 520 None P-B 139 490 None B-P 147 170 None P-B 302 790 None P-B None P-B - None
~
CEA, carcinoembryonic antigen (normal range < 5 ng/ml); P-B, pancreatic duct entering bile duct; B-P, bile duct entering pancreatic duct
Table 2 Clinicopathological~ndings inpatients with cancer ofthe gallbladder associated with pancreatobiliary maljunction without bile duct dilatation
Tumour patient no Size (mm) Location
__ Stage* Operation
Differentiation Depth of Lymph node Curative of adenocarcinoma tumour invasion metastasis Outcome
1 60 x 67 Neck and body 111
2 40 Y 60 Neck, body and 1V fundus
3 50 x 60 Neck, body and IV fundus
4 30 x 44 Body IV
5 25 x I0 Neck and body Ill
6 ~ Neck, body and V
~ Neck, body and V fundus
fundus 7
Cholecystectomy,
Cholecystectomy,
lymphadenectomy
lymphadenectomy
Pancreatoduodenectomy, hepatic subsegmentectomy, lymphadenectomy
hepatic subsegmentectomy, lymphadenectomy
lymphadenectomy, hepatic wedge resection
Exploratory laparotomy
Exploratory laparotomy
Pancreatoduodenectomy,
Cholecystectomy,
No Poor Serosa No Died at I 1 months
No Moderately differentiated Subserosa Yes Died at I2 months tubular
No Well differentiated Serosa Yes Died at 11 months tubular
Yes Papillary Serosa Yes Died at 30 months
Yes Moderately differentiated Subserosa No Alive at 38 months tubular
Other organs Yes Diedcat 3 months - Well differentiated
~~ Poor Other organs Yes Died at 6 months tubular
'According to Nevin et ul."
a b
Figure 1 Endoscopic retrograde cholangiopancreatograms of cancer of the gallbladder associated with anomalous junction of the pancreatobiliary duct system without bile duct dilatation. The arrows indicate the junction of the pancreatic and biliary ducts. a Pancreatic duct entering bile duct (patient 3); b bile duct entering pancreatic duct (patient 4 )
Br. J . Surg., Vol. 80, No. 5. May 1993 623

Gallbladder cancer and biliary anomalies: K. Tanaka et al.
The following operations had been performed: curative cholecystectomy with or without hepatic resection (six cases); palliative cholecystectomy (nine ); pancreatoduodenectomy (three); right hepatic lobectomy (one); external biliary drainage (seven); bilioenteric anastomosis (two); exploratory laparotomy (four); and no operation (two).
Curative operation was performed in seven cases. Only two patients survived for > 3 years after surgery; 24 died within 1 year.
Discussion Aoki et aL4 analysed 569 patients in Japan with anomalous junction of the pancreatobiliary duct system. Dilatation of the extrahepatic bile duct was found in most of the patients (cystic 44 per cent, spindle 23 per cent, cylindrical 17 per cent); no dilatation was present in only 80 cases (14 per cent). A total of 131 patients (23 per cent) had associated cancer of the biliary tract; 93 had carcinoma of the gallbladder, 31 cancer of the bile duct, and seven cancer of unknown location.
There were some characteristic clinical features. In patients <30 years of age, a bile duct of normal calibre was found in only 2-5 per cent, but the incidence increased gradually in those aged 2 30 years, reaching 31 per cent4 for patients aged 60-69 years. Of 253 patients with cystic dilatation only 30 (12 per cent) had associated cancer of the biliary tract (gallbladder, nine; bile duct, 21), but of 80 patients with no dilatation, 49 (61 per cent) had this cancer (gallbladder, 44; bile duct, four; and unknown location, one). This high incidence of malignancy might be explained by reflux of pancreatic juice into the gallbladder with consequent chronic cholecystitis with intestinal metaplasia, a precancerous condition leading to differentiated carcinoma*. The mechanism of concentration of bile in the gallbladder may also promote cancerous change4.12.
A total of 34 patients with cancer of the gallbladder associated with anomalous junction without bile duct dilatation, including 27 previously reported and the present seven, are reviewed in this paper. In the majority of patients in whom staging was known (11 of 18), the tumour was stage V, representing advanced disease. In seven of 34 patients curative operation was performed, but only two survived for > 3 years after operation. This dismal outcome is due largely to delayed diagnosis of cancer of the gallbladder. The incidence of gallstones in patients with this cancer associated with anomalous junction is very compared with that in those with cancer of the gallbladder not accompanied by anomalous junctionL3-' '. The low incidence of gallstones may make the early diagnosis of cancer of the gallbladder difficult, because the tumour will have become widespread by the time symptoms associated with the cancer occur. Cure following cholecyst- ectomy is possible when the malignant lesion is limited to the mucosa or muscularis propria'!' '3' '. Early diagnosis is therefore essential for the successful treatment of cancer of the gallbladder.
For patients with anomalous junction without bile duct
dilatation in whom there is no malignant lesion in the gallbladder, prophylactic cholecystectomy is recommended because of the high incidence of cancer of the biliary tract.
References 1 .
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
The Committee of Diagnostic Criteria of the Japanese Study Group on Pancreaticobiliary Maljunction. Diagnostic criteria of pancreaticobiliary maljunction. Gastroenterological Surgery
Nagata E, Sakai K, Kinoshita H et al. The relation between carcinoma of the gallbladder and anomalous connection between the choledochus and the pancreatic duct. Ann Surg 1985; 202:
Kimura K, Ohto M, Saisho H et al. Association of gallbladder carcinoma and anomalous pancreaticobiliary ductal union. Gastroenterology 1985; 89: 1258-65. Aoki H, Sugaya H, Shimazu M . A clinical study on cancer of the bile duct associated with anomalous arrangements of the pancreaticobiliary ductal system. Analysis of 569 cases collected in Japan. JournaEofBiliary Tract andpancreas 1987; 8: 1539-51. Yamauchi S, Koga A, Matsumoto S et al. Anomalous junction of the pancreaticobiliary duct without congenital choledochal cyst: a possible risk factor for gallbladder cancer. Am J Gastroenterol 1987; 82: 20-4. Todani T, Watanabe Y, Fujii T et a/. Carcinoma arising from the bile duct in choledochal cyst and anomalous arrangement of the pancreatico-biliary ductal union. Journal of Biliary Tract and Pancreas 1985; 6 : 525-35. Nagakawa T, Ohta T, Takeshita Y et al. Clinical study on anomalous union of the pancreatico-biliary duct system - with special reference to biliary diseases. Stomach and Zntestine 1985;
Nevin JE, Moran TJ, Kay S et al. Carcinoma of the gallbladder. Staging, treatment and prognosis. Cancer 1976; 37: 141-8. Uchimura M, Mutoh Y, Waki S et al. Association of carcinoma with congenital dilatation of the bile duct. Journal of Biliary Tract and Pancreas 1982; 3 : 333-42. Kuroda S, Nagai H, Morioka Y. Anomalous union of the pancreaticobiliary ductal system and biliary carcinoma. Journal ofBiliary Tract and Pancreas 1988; 9: 1191-203. Ohta T, Nagakawa T, Ueno K et al. Clinical experience of biliary tract carcinoma associated with anomalous union of the pancreaticobiliary ductal system. Jpn J Surg 1990; 20: 36-43. Komi N, Tamura T. Intestinal metaplasia and malignant change of the biliary tract caused by the anomalous arrangement of the pancreaticobiliary duct. Jpn J Pediatr Surg 1982; 14: 43-51. Mutoh Y, Sho Y, Kurihara K at al. Morphological study of carcinoma of the gallbladder: differences between calculous and acalculous carcinoma. Nippon Geka Gakkai Zasshi 1985; 86:
Rassek D, Straub D, Sons HU et al. Ergehnisse nach chirurgischer Behandlung des Gallenblasencarcinoms. Chirurg
Tashiro S , Konno T, Mochinaga M et al. Treatment of carcinoma of the gallbladder in Japan. Jpn J Surg 1982; 12: 98-104. Mizumoto R, Ogura Y, Matsuda S et ul. Cooperative survey of surgical treatment for carcinoma of the biliary tract in Japan. Journal of Biliary Tract and Pancreas 1990; 11: 869-82.
1991; 14: 654-5.
182-90.
20: 361-8.
846-52.
1985; 56: 440-4.
Paper accepted 30 September 1992
624 Br. J. Surg., Vol. 80, No. 5, M a y 1993