cadth 2015 d7 regier recruitment
TRANSCRIPT

Advancing Health Economics, Services, Policy and Ethics
Regier DA, Bentley C, McTaggart-Cowan
H, Burgess M, Peacock S
2015 CADTH Symposium
Saskatoon, Saskatchewan
Identifying a “Representative Public”:
Recruiting for Demographic and Values
Diversity for a Public Engagement
Event on Priority Setting and Cancer
Drug Funding in Vancouver

• Public engagement event
• Recruitment (background)
• Diversity of experience
• Diversity of utility
• Recruitment Algorithm
Outline
2
Objective of event:
• Solicit the public’s values on setting priorities, cancer drug funding, and the need to make trade-offs using deliberative public engagement
Deliberative methods (Burgess et al, 2008; 2014)
• Collective solutions to challenging issues in the form of recommendations; not consensus oriented
• Mini public; include marginal groups; non experts
• Free, equal, and respectful exchange of views and reasons for them
• Presence of decision makers, end users (to observe event)
“Making Decisions about Funding for Cancer Drugs: A Deliberative Public Engagement”
3

Understanding different views
• Listen and consider all points of view
Respectful engagement
• Participants are equals, avoid reactive positions
Informed deliberation on trade-offs
• Present participants with a variety of information and information types
Include diverse experiences
• Wide range of views
Key aspects for deliberative event
4

Sampling for representativeness
• Stratified random sampling
• SRS + civic lottery (Bombard et al 2011/Dowlen 2008)
Do randomly sampled respondents encompass full range of interests and perspectives?
Recruit for diversity of interests
• Wide range of participants drawing from distinct life experiences, values, and styles of reasoning (Longstaff and
Burgess, 2010)
• Interests are situational and may not be stable
Background - recruitment
5

Recruitment strategies (Longstaff and Burgess, 2010)
1. Recruit participants from each of the geographic BC health regions
2. Random digit dial to recruit a small sample with only basic filters for gender, age. This allows all citizens to have an equal opportunity of being selected.
3. Recruit a sample that accurately represents the population of BC by allowing all citizens to have an equal opportunity of being selected
4. Recruit those who are typically absent from deliberative events (e.g., ethno-cultural groups, youth)
5. Recruit a demographically stratified sample of 25 from a registry and minority groups (e.g., voters list or health care system subscribers)
6. Recruit by advertising for interested participants and with identifiable groups (e.g., recruit for enclave representation)
7. Screen to avoid like-minded stakeholders or those with extreme views
8. Recruiting a mix of citizens, politicians, industry representatives
Guidance (Diversity of Interests)
6

Objective: to recruit members from the BC public who represent a diversity of interests
Diversity of interests = diversity of experiences and utility weightings
Recruitment objective
7

Proxy for diversity of experience
• Demographic characteristics of the BC population, incl. oversample of minority and younger age groups
Proxy for diversity of utility weightings
• Discrete choice experiment method to elicit utility
Proxy for experience and utility?
8

Online questionnaire:
• Pre-screens: tobacco, policy maker, availability, experience with chronic disease
• Stratified by age, sex, geography (urban/rural; health authority), parenthood, ethnicity, income, education,experience with chronic diseases)
Recruit 80 people (from 35,000)
– Representative of BC population
– Also completed a discrete choice experiment
9
Diversity of Experience

Snapshot of BC demographic data
Based on BC Ministry of Health data
9 demographic categories in total
– (not pictured, education, sex, children)
10
n=30 n=80
Urban 26 69
Rural 4 11
AGE
18-24 3 8
25-34 5 13
35-49 8 21
50-64 8 21
65+ 6 16
HEALTH AUTHORITY
Fraser Health 11 29
Interior Health 5 13
Island Health 5 13
Northern Health 2 5
Vancouver Coastal Health 7 19
ETHNICITY
Aboriginal 2 5
Caucasian 20 53
Chinese 3 8
South Asian 3 8
Other 2 5
CHRONIC DISEASE
Confirmed (65+) 11 29
INCOME
<$19,999 2 5
$20,000-$34,999 4 11
$35,000-$49,999
$50,000-$79,999
4
8
11
21
$80,000+ 12 32

Discrete choice experiment method
• Attribute-based survey measure of utility
– Any good can be described by its attributes
• Creates a market using experimental design
– In healthcare it is difficult to observe real-world choices people make between health technologies
• Individuals choose between alternative goods
– Opportunity cost and trade-offs (in-line with objective of event)
Diversity of Utility Weightings
11

12
Choice example
• 16 choice questions posed to 80 respondents
• Latent class analysis used to analyse limited dependent data
• Each individual N=80 was assigned a probability of belonging to a latent class

What did your choices tell us?Category Class A
(14 people)Class B(16 people)
Class C(50 people)
Perfect health Reference category Reference category Reference category
Some problems with usual activity,no pain
-0.32 -0.25 -2.21
Some problems with usual activity, moderate pain
-0.78 -0.69 -2.54
Some problems with usual activity, extreme pain
-3.78 -1.23 -7.59
Duration of life 0.14 0.480 0.64
Extra tax payment -0.0002 -0.0001 -0.00026
Utility of moderate pain to no pain
0.46 gain in QOL,willingness to pay
$2,271
0.44 gain in QOL,Willingness to pay
$4,400
0.32 gain in QOL, willingness to pay
$1,21513
Latent class analysis
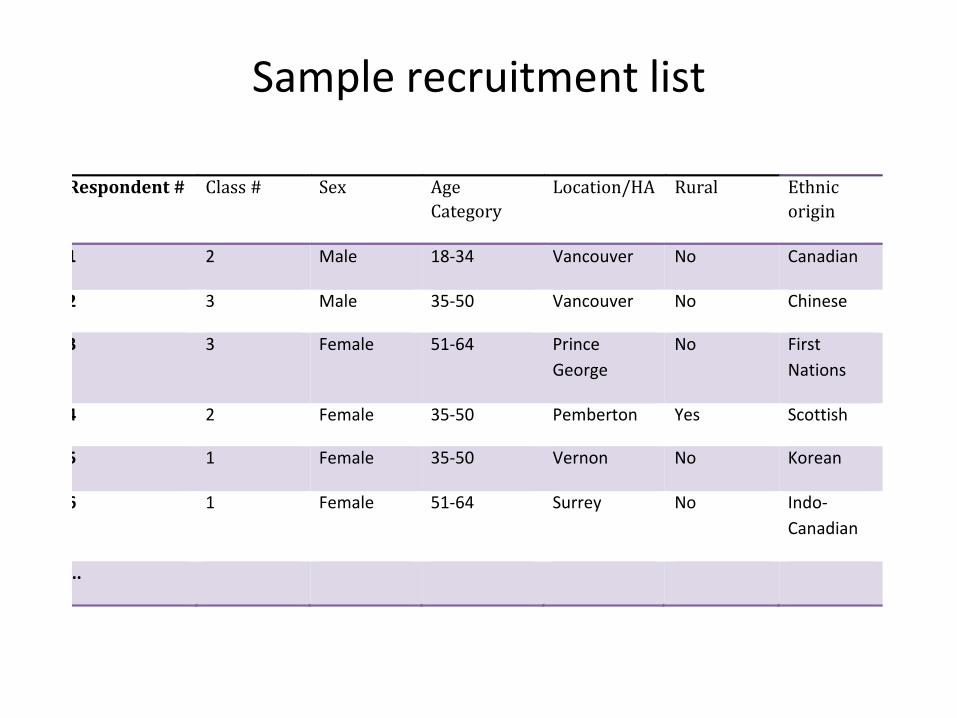
Sample recruitment list
Respondent# Class# Sex Age
Category
Location/HA Rural Ethnic
origin
1 2 Male 18-34 Vancouver No Canadian
2 3 Male 35-50 Vancouver No Chinese
3 3 Female 51-64 Prince
George
No First
Nations
4 2 Female 35-50 Pemberton Yes Scottish
5 1 Female 35-50 Vernon No Korean
6 1 Female 51-64 Surrey No Indo-
Canadian
...
14

The sample of 30 – Randomly select 30 from population of N=80 – record
their demographic and “latent class” characteristics
– Using I-statistic, determine how close the hypothetical sample of 30 is to the target demographics and latent classes
– Repeat many, many times to determine the sample of 30 closest to specified criteria
Determining the sample of 30
15

16
n=30 n=24 Actual
(24)
Sex (male) 15 12 11
Urban 26 21 26
Rural 4 3 4
AGE
18-24 3 3 3
25-34 5 4 5
35-49 8 6 8
50-64 8 6 8
65+ 6 5 6
HEALTH AUTHORITY
Fraser Health 11 9 9
Interior Health 5 4 4
Island Health 5 4 3
Northern Health 2 2 2
Vancouver Coastal
Health
7 5 6
ETHNICITY
Aboriginal 2 2 2
Caucasian 20 16 16
Chinese 3 2 3
South Asian 3 2 1
Other 2 2 2
Target of 30
(Random sample 99%
close to stratified sample)
Target number if 24
Actual characteristics of
24 participants attending
the event

17
n=30 n=24 Actual
(24)
Children (yes) 17 14 14
Education
High School 11 9 6
College 9 7 10
Some University 3 2 2
University or above 7 6 6
Latent Class
Class 1 5 4 3
Class 2 6 5 5
Class 3 19 14 13
INCOME
<$19,999 2 2 3
$20,000-$34,999 4 3 3
$35,000-$49,999
$50,000-$79,999
4
8
3
6
3
7
$80,000+ 12 10 8
CHRONIC DISEASE
Confirmed (65+) 11 9 8
Target of 30
(Random sample 99%
close to stratified sample)
Target number if 24
Actual characteristics of
24 subjects attending the
event

We recruited on life experience & utility weight
• Demographic proxy for life experience
• Discrete choice experiment – utility
Created a sample of 30 (from 80) using novel sampling strategy
Future work to incorporate ‘reasoning’
Overview
18

“Making Decision about Funding for Cancer Drugs: A Deliberative Public Engagement”
Research Team
Stuart Peacock, PI – BC Cancer Agency (BCCA), Canadian Centre for Applied Research in Cancer Control (ARCC), U of British Columbia (UBC)
Mike Burgess, Co-I – UBC
Dean Regier, Co-I – BCCA, ARCC, UBC – [email protected]
Colene Bentley – BCCA, ARCC
Helen McTaggart-Cowan – BCCA, ARCC
Event Team
Liz Wilcox , Sarah Costa, Reka Pataky, Sonya Cressman, Emily McPherson, Lisa Scott, Kim van der Hoek, Holly Longstaff
Funders
19

• Burgess, M., O'Doherty, K., & Secko, D. (2008). Biobanking in British Columbia: discussions of the future of personalized medicine through deliberative public engagement. Personalized Medicine, 5, 285-296
• Longstaff H, Burgess M. (2010) Recruitment for representation in public deliberation on the ethics of biobanks. Public Understanding of Science , 19(2), 212-224.
• Bombard Y, Abelson J, Simeonov D, Gauvin FP. (2011). Eliciting ethical and social values in health technology assessment: a participatory approach. Social Science & Medicine. 73 135-144.
• Burgess, M. (2014). From 'trust us' to participatory governance: Deliberative publics and science policy. Public Understanding of Science, 23, 48-52.
References
20