c hapter 6 gingival diseases copyright © 2014, 2007, 2001, 1996 by saunders, an imprint of elsevier...
TRANSCRIPT

CHAPTER 6Gingival Diseases
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
INTRODUCTION
Diseases of the gingival tissues range from common forms, such as dental plaque biofilm–induced gingivitis, to rare but potentially life-threatening forms, such as squamous cell carcinoma or acute leukemia.
2
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

INTRODUCTION (CONT.)
The following figure demonstrates the normal appearance of healthy gingiva.
3
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

GINGIVITIS
Gingivitis is an inflammation of the gingival tissues.
It occurs in a periodontium with no attachment loss or in a periodontium with attachment loss that is not progressing.
4
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.
GINGIVITIS (CONT.)
Gingivitis manifestations include: Color change (redness) Edema (swelling of the tissues) Exudate (drainage of gingival fluid from the
sulcus) Spontaneous bleeding (hemorrhage in response
to gentle periodontal probing or toothbrushing)
5
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

GINGIVITIS (CONT.)
Changes may also be observed in the gingival contour, loss of tissue adaptation to the teeth, and an increased flow of gingival crevicular fluid.
Gingivitis is one of the most common human diseases and among the easiest to treat and control.
However, patients often fail to recognize gingivitis because it is painless and the symptoms are thought to be normal.
6
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

PATHOGENESIS OF GINGIVAL DISEASE
Pathogenesis refers to the events in the development and progression of a disease.
Describing the histologic events as they relate to clinical signs is the best way to explain the pathogenesis of gingivitis.
7
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

PATHOGENESIS OF GINGIVAL DISEASE (CONT.)
The development of gingival inflammation can be separated into four stages:1. Initial2. Early3. Established4. Advanced
The extension of inflammation into the alveolar bone, at which point the gingival disease has progressed to periodontal disease, characterizes the fourth (or advanced) stage.
8
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

STAGE I GINGIVITIS—INITIAL OR SUBCLINICAL STAGE
Stage I gingivitis occurs in the first few days of contact between microbial plaque and the gingival tissues.
The dilation of the blood vessels and increased blood flow characterize the acute inflammatory response that occurs at this initial stage.
Polymorphonuclear neutrophils (PMNs) attach to the vessel walls and begin to migrate into the surrounding connective tissues. PMNs are the principal defense in acute
inflammation.
9
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

STAGE I GINGIVITIS—INITIAL OR SUBCLINICAL STAGE (CONT.)
PMNs phagocytize bacteria, their products, and other products of destroyed tissue.
Small amounts of plasma also leak into the surrounding tissues, causing edema in the tissues.
PMNs amass in the connective tissue and migrate through the sulcular epithelium into the plaque, forming exudate.
Exudate from early gingival inflammation, made up of mostly serum, is referred to as gingival fluid flow. The gingival fluid is clear. 10
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.
STAGE I GINGIVITIS—INITIAL OR SUBCLINICAL STAGE (CONT.)
Lymphocytes appear in the gingival connective tissues. Mostly T lymphocytes
In addition, activation of the host immune system causes epithelial cell changes and collagen degradation.
These first tissue reactions are not visible; therefore they do not cause obvious clinical changes.
This initial inflammatory response is a subclinical infection.
11
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

STAGE II GINGIVITIS—EARLY STAGE
Stage II gingivitis is referred to as early gingivitis.
Clinical evidence of gingivitis occurs at this stage.
Lesions begin to form 4 to 7 days after plaque has accumulated in the gingival sulcus.
The T lymphocytes increase in number and are localized in the connective tissue under the epithelium of the gingival sulcus.
The inflammatory exudate increases and may appear white or yellow.
12
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

STAGE II GINGIVITIS—EARLY STAGE (CONT.)
Clinically, the tissues appear slightly red and swollen.
Inflammation destroys the perivascular collagen fibers in the connective tissues, and blood plasma and inflammatory cell infiltrate replace the perivascular collagen fibers.
Collagen fibers that attach the underlying connective tissue to the gingival epithelium are also destroyed, and gingival stippling begins to disappear, causing the gingiva to appear shiny.
13
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

STAGE II GINGIVITIS—EARLY STAGE (CONT.)
The junctional epithelium begins to lengthen against the root surface.
Gingival tissues tend to bleed when gently probed.
Cellular changes occur in the connective tissue fibroblasts, leading to their destruction.
This early stage of gingivitis may continue for 21 days or longer.
14
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

STAGE III GINGIVITIS—ESTABLISHED STAGE
After 15 to 21 days, the gingival inflammation reaches the stage III gingivitis, which is referred to as the established stage.
Plasma cells, usually associated with an intense antigen-antibody response, are present.
T and B lymphocytes are found in equal amounts, indicating that tissue destruction by the inflammatory reaction is taking place. B lymphocytes are related to cell surface
immunity and release lymphokines, which accelerate the tissue destruction in inflammation.
15
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

STAGE III GINGIVITIS—ESTABLISHED STAGE (CONT.)
More connective tissue collagen is destroyed.
The junctional epithelium thickens and extends apically into the underlying connective tissues.
The clinical probing depth increases for two reasons:
1. The periodontal probe penetrates more deeply through the junctional epithelium into the connective tissue by approximately 1 mm as a result of the loss of collagen.
2. Edema in the tissues moves the gingival margin coronally, increasing the probe readings.
16
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

STAGE III GINGIVITIS—ESTABLISHED STAGE (CONT.)
The blood vessels proliferate, permitting more seepage of serum into the tissues and through the sulcular epithelium. This change, along with the increased presence
and activity of inflammatory cells, causes visible pus formation.
17
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

STAGE III GINGIVITIS—ESTABLISHED STAGE (CONT.)
Capillary proliferation also causes the gingiva to appear red. In extreme cases, the tissue appears blue, or
cyanotic, because of the presence of many oxygen-depleted red blood cells.
In combination, these changes result in red, swollen, and shiny gingiva that may also exhibit noticeable pus formation and gingival exudate.
18
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

STAGE III GINGIVITIS—ESTABLISHED STAGE (CONT.)
The established gingivitis stage may persist unchanged for months or years.
The condition is reversible when plaque is regularly removed, permitting the tissues to return to normal.
When healing occurs, no residual tissue destruction remains.
19
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

STAGE IV GINGIVITIS—ADVANCED STAGE
Stage IV gingivitis is referred to as the advanced stage of gingivitis.
The inflammatory processes have extended beyond the gingiva and into the other periodontal tissues.
The extension of disease into the bone is referred to as periodontitis.
20
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

HEALING OF THE GINGIVAAFTER TREATMENT
Healing of gingivitis begins in the connective tissues.
Fibroblasts, which lay down a firm extracellular matrix of collagen, replace the inflammatory cells. These fibers produce a dense subgingival
connective tissue. This connective tissue does not permit
penetration of the periodontal probe, reducing the probing depth.
The gingival color returns to pink, and stippling reappears. 21
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

HEALING OF THE GINGIVAAFTER TREATMENT (CONT.)
Gingivitis has been classified into a number of categories on the basis of: Clinical manifestations of the disease Cause Association with systemic diseases Association with medications Other causes
22
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

RECESSION OF THE GINGIVA
Recession of the gingiva refers to the location of the margin of the tissue.
Recession can occur in gingivitis, or it can be associated with clinically healthy tissue.
Recession can be localized to one tooth or extend to any number of teeth.
23
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

RECESSION OF THE GINGIVA (CONT.)
Etiologic factors associated with recession include: Gingival abrasion Tooth malposition (rotated, tilted, or displaced
tooth) Gingival ablation (friction from other soft tissues) Gingival inflammation Abnormal frenum attachment
24
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.
RECESSION OF THE GINGIVA (CONT.)
Recession is of significance in dental hygiene care because: Root surfaces can decay. Cemental surfaces can wear away, creating
sensitivity. Recessed areas can be more difficult for the
patient to clean.
25
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

DENTAL PLAQUE–INDUCEDGINGIVAL DISEASE
The most obvious symptom of gingivitis is bleeding gums.
Many people live with this condition and are often unaware that bleeding is a symptom of a disease.
26
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

GINGIVITIS ASSOCIATED WITH DENTAL PLAQUE BIOFILM ONLY
The most common form of gingivitis found in the general population is gingivitis associated with dental plaque only; it is also called plaque-associated gingivitis or gingivitis.
This disease is directly related to the presence of bacterial plaque on the tooth surface.
27
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

GINGIVITIS ASSOCIATED WITH DENTAL PLAQUE BIOFILM ONLY (CONT.)
Clinically, gingivitis causes: Reddened gingival margin Pocket formation as a result of:
Gingival swelling and edema Hypertrophy Deepened penetration of periodontal
probes on clinical evaluation
28
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.
GINGIVITIS ASSOCIATED WITH DENTAL PLAQUE BIOFILM ONLY (CONT.)
The surface of the gingiva appears glazed or smooth, and stippling usually disappears.
Microscopically, capillaries increase along the gingival margin.
Epithelium lining the gingival sulcus is ulcerated. Ulceration causes a tendency to bleed on
probing. Clear gingival fluid flow, or exudate, appears
to increase with the severity of the gingivitis.
29
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

GINGIVITIS ASSOCIATED WITH DENTAL PLAQUE BIOFILM ONLY (CONT.)
The following figure demonstrates the typical appearance of dental plaque–induced gingivitis.
30
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.
GINGIVITIS ASSOCIATED WITH DENTAL PLAQUE BIOFILM ONLY (CONT.)
Gingivitis is directly related to the amount of plaque biofilm on the teeth and the amount of time the plaque is allowed to remain undisturbed.
Plaque biofilm is considered nonspecific because it is not associated with any specific type of microorganism.
Mature plaque biofilm has a large percentage of gram-negative bacteria.
This change from gram-positive plaque to predominantly gram-negative plaque is characteristic of gingivitis.
31
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

DISTRIBUTION OF GINGIVITIS
The location of the disease and the degree of involvement in the dentition may further classify plaque-associated gingivitis.
The disease may be localized to a few teeth or generalized throughout the mouth.
It may be limited to the interdental papilla, spread along the entire gingival margin, or involve all of the attached gingival tissues.
32
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

DESCRIBING THE GINGIVAL CONDITION
The terms commonly used to describe the tissues in relation to gingivitis include: Extent of involvement: localized, generalized Tissues affected: marginal, papillary Degree of inflammation: slight, moderate, severe
33
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

DESCRIBING THE GINGIVAL CONDITION (CONT.)
The description of the gingival condition should also include the color, shape, and shininess of the tissues.
Examples: Localized inflammation, redness, and swelling on
the buccal and lingual posterior sextants Generalized severe inflammation; tissues
intensely red, with rounded, shiny marginal and papillary gingiva; easily bleeds on probing
These descriptors permit the dental hygienist to evaluate changes in the clinical appearance at subsequent appointments. 34
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

DESCRIBING THE GINGIVAL CONDITION (CONT.)
Gingivitis is reversible.
Evidence of complete resolution of gingival inflammation is presented in the following figure.
35
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

PLAQUE BIOFILM–INDUCED GINGIVITIS MODIFIED BY LOCAL CONTRIBUTING FACTORS
Tooth-related factors that modify or predispose localized gingivitis often include: Malposed or crowded teeth Dental restorations Orthodontic appliances
These factors act to retain plaque and make oral hygiene practices more difficult and less effective.
Although these factors do not cause gingivitis, ordinary cleaning practices are not sufficient to remove plaque biofilm.
36
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.
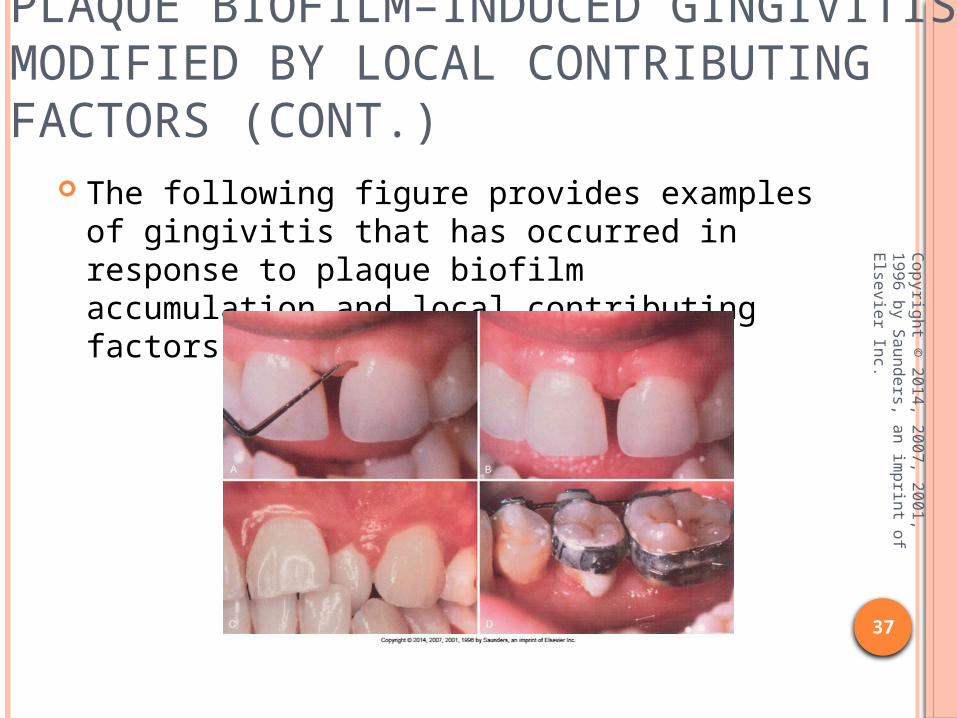
PLAQUE BIOFILM–INDUCED GINGIVITIS MODIFIED BY LOCAL CONTRIBUTING FACTORS (CONT.)
The following figure provides examples of gingivitis that has occurred in response to plaque biofilm accumulation and local contributing factors.
37
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

GINGIVAL DISEASES MODIFIEDBY SYSTEMIC FACTORS
Many systemic factors act to modify the manner in which an individual’s immune system responds to dental plaque biofilm.
These systemic factors do not cause gingivitis but act to intensify it, resulting in gingival diseases modified by systemic factors.
38
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

ENDOCRINE-INFLUENCED GINGIVAL DISEASE
Steroid-type hormones produced by the endocrine glands influence gingivitis.
Hormones associated with puberty and pregnancy also affect gingival disease. The use of birth control medications is also
associated with gingival changes. When female hormone levels are increased,
some subgingival bacteria increase, such as Bacteroides species, possibly causing the increased gingival inflammation.
39
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

ENDOCRINE-INFLUENCED GINGIVAL DISEASE (CONT.)
Estrogen receptors in the gingival tissues and serum concentrations of female sex hormones during pregnancy both influence the gingival tissues.
Estrogen may also regulate cellular proliferation, keratinization, and vascular proliferation and fragility in the gingival tissues.
The extent of hormone-related changes also depends on the level of plaque biofilm control.
40
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

ENDOCRINE-INFLUENCED GINGIVAL DISEASE (CONT.)
As hormone levels increase during the second trimester of pregnancy, gingival inflammation may increase.
The gingiva may become dark red and hyperplasic and may bleed excessively.
The following figure demonstrates an example of pregnancy gingivitis.
41
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

ENDOCRINE-INFLUENCED GINGIVAL DISEASE (CONT.)
Changes may increase as the pregnancy progresses.
Most pregnancy-related gingivitis improves or resolves with good homecare and the removal of local irritants.
42
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

ENDOCRINE-INFLUENCED GINGIVAL DISEASE (CONT.)
Some pregnant women develop a specific type of gingival lesion called a pregnancy tumor.
This gingival lesion is not a tumor but a localized area of pyogenic granulation tissue.
The tissues are highly inflamed, easily bleed, and may cause the teeth to be mobile and possibly migrate out of the way.
Poor plaque biofilm control is related to the severity of the inflammation.
43
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

ENDOCRINE-INFLUENCED GINGIVAL DISEASE (CONT.)
The following figure demonstrates an example of a pregnancy tumor.
44
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

ENDOCRINE-INFLUENCED GINGIVAL DISEASE (CONT.)
Gingival changes associated with pregnancy may occur in women who are taking oral contraceptives or in women who are taking hormone replacement therapy.
Two mechanisms may cause this gingival response:
1. An increase in some pathogenic bacteria, such as Porphyromonas gingivalis and Actinobacillus actinomycetemcomitans
2. Possible increase in prostaglandin E, a mediator of inflammation
45
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

GINGIVAL DISEASES MODIFIEDBY MEDICATIONS
Medications can cause changes in gingival tissues, resulting in gingival diseases modified by medications.
Phenytoin, an antiseizure medication, is associated with gingival hyperplasia (overgrowth). Tissues become fibrotic and enlarged.
Fibroblasts that create a denser connective tissue cause the enlargement.
An increase in bacterial plaque is related to an increase in gingival overgrowth. 46
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

GINGIVAL DISEASES MODIFIEDBY MEDICATIONS (CONT.)
Medication-induced gingival enlargement results in gingival contours that enhance plaque accumulation and make plaque biofilm removal more difficult.
Treatment of this type of gingival enlargement requires good homecare, regular scaling and root planing, and, often, surgical reduction of the enlargements with surgical gingivectomy procedures.
47
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

GINGIVAL DISEASES MODIFIEDBY MEDICATIONS (CONT.)
Some cardiac medications, including nifedipine and verapamil, also cause an overgrowth of gingival tissues. Both agents are classified as calcium channel
blockers. Some evidence suggests that excellent
plaque control helps control the symptoms of hyperplasia and gingivitis.
48
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

GINGIVAL DISEASES MODIFIEDBY MEDICATIONS (CONT.)
The following figure demonstrates examples of drug-induced gingival enlargement.
49
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

GINGIVAL DISEASES MODIFIEDBY MEDICATIONS (CONT.)
Cyclosporine, the major drug used for immunosuppression in patients who have undergone organ transplantation, may also cause gingival overgrowth. This medication may also be used to treat
multiple sclerosis. Unlike phenytoin- or nifedipine-induced
hyperplasia, which is usually limited to the gingiva, cyclosporine can cause excessive accumulation of connective tissue in many other tissues of the body.
50
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.
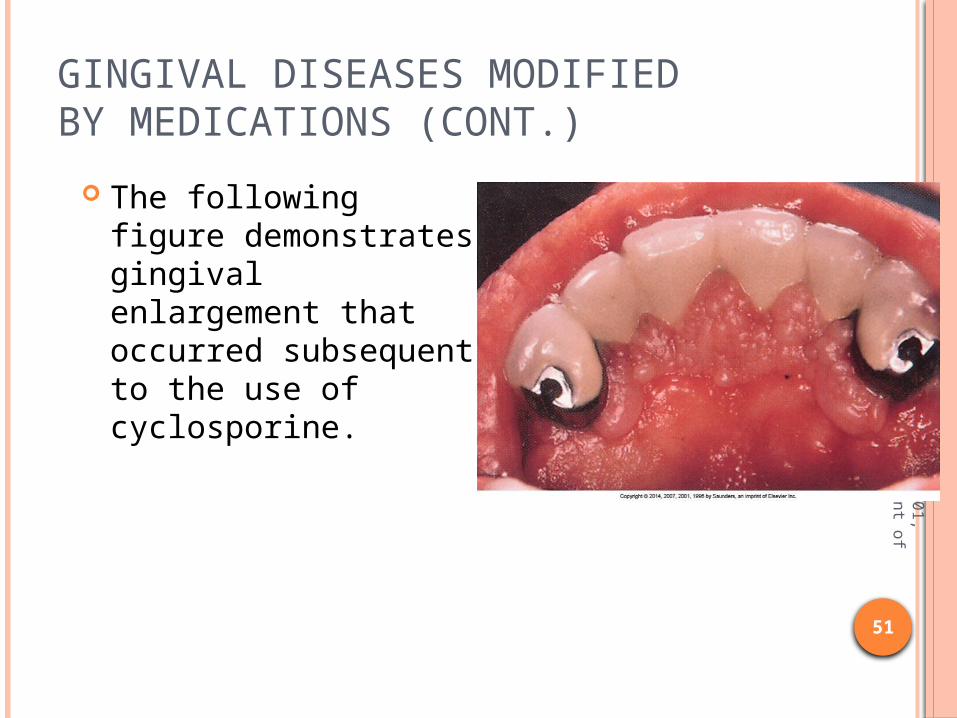
GINGIVAL DISEASES MODIFIEDBY MEDICATIONS (CONT.)
The following figure demonstrates gingival enlargement that occurred subsequent to the use of cyclosporine.
51
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

GINGIVAL DISEASES MODIFIEDBY MALNUTRITION
Deficiencies in many vitamins can produce changes in the oral tissues and is referred to as gingival diseases modified by malnutrition. These vitamins include A, B1, B2, B6, and C.
Although rare, vitamin C deficiency can cause scurvy, a condition resulting in defective collagen formation and maintenance. The gingiva becomes hemorrhagic and swollen,
and the condition rapidly progresses to advanced periodontitis. 52
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

GINGIVAL DISEASES MODIFIEDBY MALNUTRITION (CONT.)
The following figure demonstrates an example of gingival disease associated with severe malnutrition.
53
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

NONPLAQUE-BIOFILM–INDUCED GINGIVAL LESIONS
Many systemic infections caused by specific bacteria may have gingival signs and symptoms.
Fungal infections may also be exhibited in the gingival tissues.
These infections are referred to as nonplaque-biofilm–induced gingival lesions.
Some of these conditions require antimicrobial or antiviral interventions or, in the case of many viruses, usually run their course. 54
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.
GINGIVAL DISEASES OF SPECIFIC BACTERIAL ORIGIN
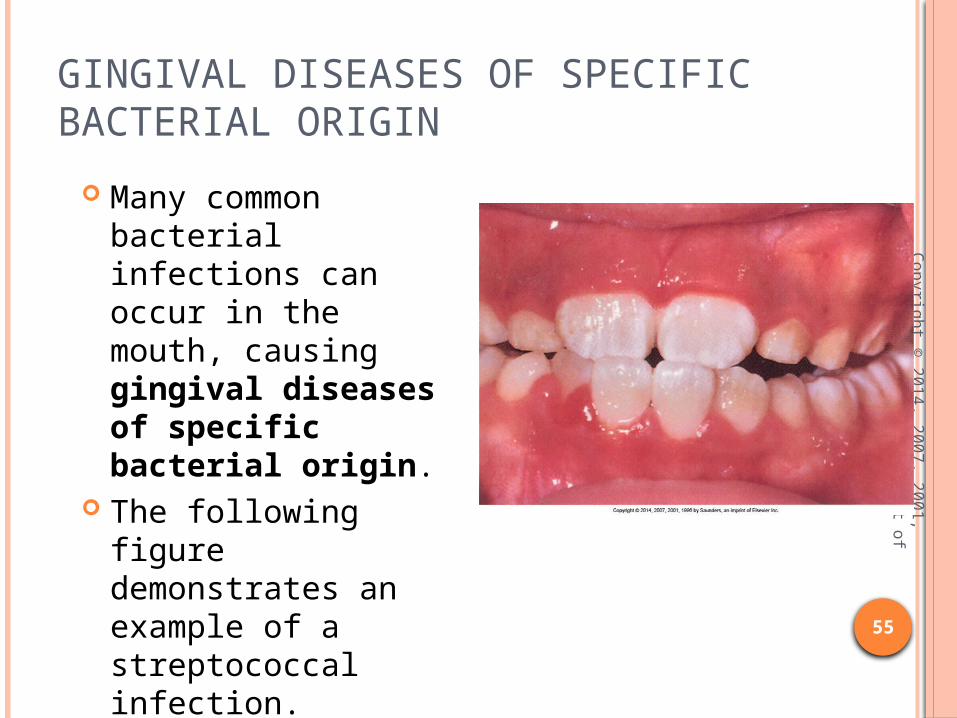
Many common bacterial infections can occur in the mouth, causing gingival diseases of specific bacterial origin.
The following figure demonstrates an example of a streptococcal infection. 55
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

GINGIVAL DISEASES OF SPECIFIC BACTERIAL ORIGIN (CONT.)
Sexually transmitted diseases such as meningococcal gonorrhea or syphilis have oral manifestations. These examples are less commonly observed in
dental offices today.
56
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

NECROTIZING ULCERATIVE GINGIVITIS
The rapid onset of pain and the development of necrotic ulcerative lesions of the gingiva characterize necrotizing ulcerative gingivitis (NUG).
NUG is a condition that can occur with no bone loss but with a specific identifiable bacterial component.
NUG has been related to excessive stress.
57
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

NECROTIZING ULCERATIVE GINGIVITIS (CONT.)
NUG begins in the interdental papillae. After a few days, the tips of the papillae
appear punched out and covered by a white necrotic pseudomembrane.
This pseudomembrane is a collection of PMNs trapped in the fibrin clot.
Attached gingival tissues are also usually inflamed.
A distinctive breath odor that has been termed fetor oris is evident.
58
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

NECROTIZING ULCERATIVE GINGIVITIS (CONT.)
The following figure demonstrates an example of NUG.
59
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

NECROTIZING ULCERATIVE GINGIVITIS (CONT.)
A significant feature of NUG infection is the presence of two microorganisms—a fusiform bacillus and a spirochete.
These so-called Vincent’s organisms appear to be present in all patients with NUG.
Occasionally, patients develop a fever. Antibiotics are useful in the treatment of NUG
but are recommended only if the patient has systemic symptoms of fever and severe malaise.
60
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

NECROTIZING ULCERATIVE GINGIVITIS (CONT.)
The treatment for NUG is to débride the plaque from the tissues completely and begin a home regimen of excellent plaque control.
Postoperatively, patients can rinse with a dilute solution of hydrogen peroxide and warm water.
Untreated, this disease may lead to bone loss and become necrotizing ulcerative periodontitis (NUP).
61
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

GINGIVAL DISEASES OF VIRAL ORIGIN
Gingival disease of viral origin may resemble plaque-induced gingivitis.
One viral infection in particular, herpesvirus infection, is highly contagious and common.
Primary and secondary forms of the infection exist.
62
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.
GINGIVAL DISEASES OF VIRAL ORIGIN (CONT.)
Primary herpetic gingivostomatitis exhibits the following symptoms: Elevated temperature Malaise Vesicle formation
The vesicles associated with herpesvirus coalesce to form ulcerative lesions on the gingiva or oral mucosa.
63
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

GINGIVAL DISEASES OF VIRAL ORIGIN (CONT.)
The following figure demonstrates an example of primary herpetic infection.
64
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

GINGIVAL DISEASES OF FUNGAL ORIGIN
Fungal infections may occur on the gingiva or other oral tissues.
Although several fungi species can infect the oral tissues, the most common is Candida albicans.
Gingival diseases of fungal origin are treated with antifungal or antiseptic therapies or both.
65
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

CANDIDIASIS OF THE GINGIVA
Candida infections are often observed in patients with pronounced immunosuppression such as individuals who have undergone organ transplantation and those with human immunodeficiency virus (HIV).
66
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

CANDIDIASIS OF THE GINGIVA (CONT.)
The following figure demonstrates an example of a Candida infection associated with HIV.
67
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

CANDIDIASIS OF THE GINGIVA (CONT.)
The gingival conditions caused by Candida range from initial signs of redness at the gingival margin, called linear gingival erythema, to severe redness with white patches on the gingiva. The white patches easily rub off the gingiva,
exposing ulcerated tissue.
68
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

GINGIVAL LESIONS OF GENETIC ORIGIN
Some individuals seem to be genetically predisposed to gingival changes.
Research into genetic diseases is growing, and more information will be available as human genome research continues.
Gingival enlargement is one condition that may be observed.
69
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.
GINGIVAL ENLARGEMENT
Gingival enlargement, termed hyperplasia or hypertrophy, is a pathologic overgrowth of the gingiva.
It has a variety of causes including: Excessive reactions to bacterial plaque biofilm Certain medications Certain infections Side effect of systemic diseases
70
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

GINGIVAL ENLARGEMENT (CONT.)
Gingival hypertrophy related to these conditions does not respond well to good plaque biofilm control.
However, plaque biofilm control is important because poor patient plaque biofilm control worsens most conditions.
71
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

GINGIVAL ENLARGEMENT (CONT.)
The following figure presents a case of gingival enlargement.
72
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

GINGIVAL MANIFESTATIONSOF SYSTEMIC CONDITIONS
Certain systemic conditions can result in changes to the gingival tissues.
The more common gingival manifestations of systemic conditions are related to mucocutaneous disorders, dermatologic diseases, or blood dyscrasias.
73
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

BLOOD DYSCRASIA–ASSOCIATED GINGIVITIS
Gingival conditions related to blood dyscrasias are not often observed in the dental office.
One condition, acute leukemia, is sometimes first seen in the dental office because of the quick onset of gingival changes.
74
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

ACUTE LEUKEMIA
Acute leukemia may initially be observed in the gingival tissues.
It causes hemorrhagic and swollen gingival tissues, far more pronounced than would be expected from the amount of plaque and calculus present.
The patient often reports that the tissues were normal until recently.
The gums easily bleed and are swollen and tender.
75
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.
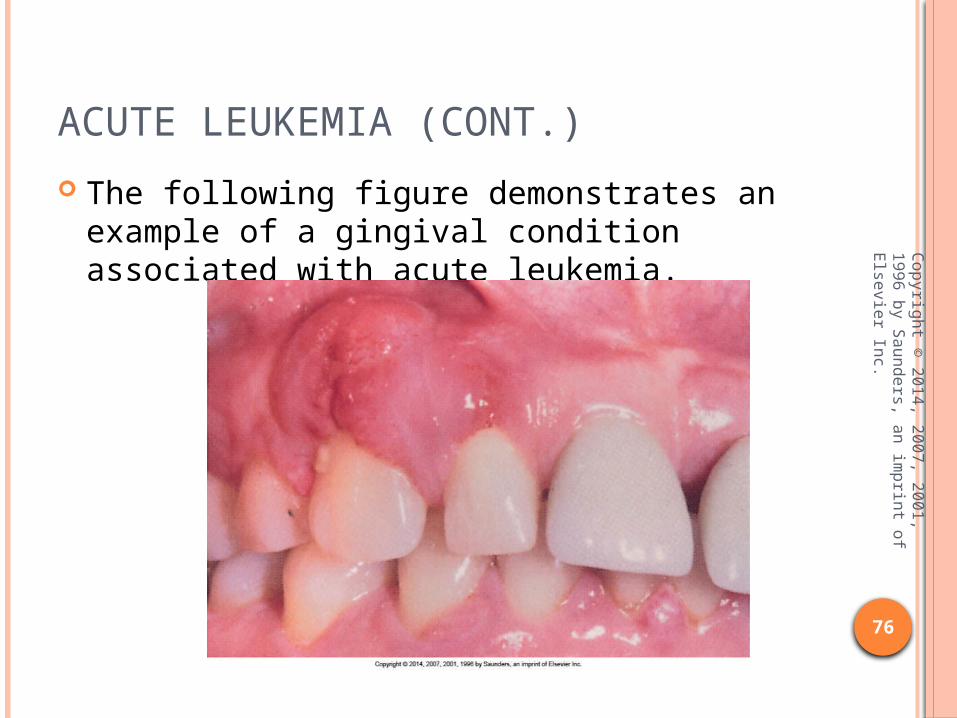
ACUTE LEUKEMIA (CONT.)
The following figure demonstrates an example of a gingival condition associated with acute leukemia.
76
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

GINGIVAL MANIFESTATIONSOF DERMATOLOGIC DISEASE
The more common systemic diseases revealed as dermatologic conditions are: Lichen planus Benign mucous membrane pemphigoid
77
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

LICHEN PLANUS
Lichen planus is a chronic disease thought to be related to the immune system.
It affects the skin and mucous membranes of
middle-aged patients. Men and women are equally affected.
Forms of lichen planus include: Reticular Erosive and bullous
78
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.
LICHEN PLANUS (CONT.)
The reticular form usually identified as lacy white lines (Wickham’s striae) with a bumpy appearance.
The erosive form of lichen planus exhibits areas of white lesions alternating with raw, reddened areas.
The severity of lichen planus appears to be related to the stress level of the patient.
79
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.
LICHEN PLANUS (CONT.)
Most studies suggest a cell-mediated immune reaction causes lichen planus, although the mechanism is not known.
A concern exists that the erosive form of lichen planus has the potential to transform into squamous cell carcinoma.
Topical steroids have been used to control lichen planus during flare-ups, but no known cure has been developed.
80
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.
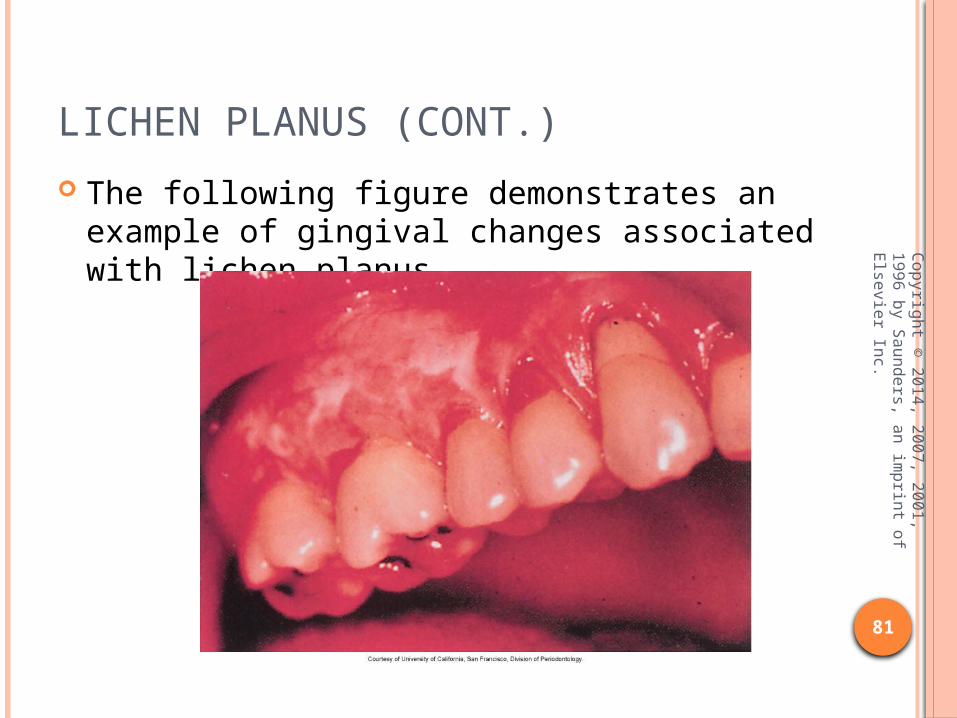
LICHEN PLANUS (CONT.)
The following figure demonstrates an example of gingival changes associated with lichen planus.
81
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

MUCOUS MEMBRANE PEMPHIGOID
Benign mucous membrane pemphigoid, or cicatricial pemphigoid, is a chronic vesiculobullous disease seen as blistering and sloughing of the surface of gingival epithelium.
Although the cause is not known, benign mucous membrane pemphigoid is considered an autoimmune reaction.
This disease is more common in older individuals and significantly more common in women than in men.
82
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

MUCOUS MEMBRANE PEMPHIGOID (CONT.)
Lesions may appear on oral tissues other than the gingiva including the buccal mucosa and inner surface of the lips.
Symptoms range from mild discomfort to painful raw, bleeding areas, because the epithelium strips away from the underlying connective tissue. This peeling when rubbed is known as Nikolsky
sign.
83
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

MUCOUS MEMBRANE PEMPHIGOID (CONT.)
The following figure demonstrates an example of mucous membrane pemphigoid.
84
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

MUCOUS MEMBRANE PEMPHIGOID (CONT.)
Treatment is palliative and may include: Steroid therapy Topical corticosteroids Chlorhexidine mouth rinses
85
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.
DESQUAMATIVE GINGIVITIS
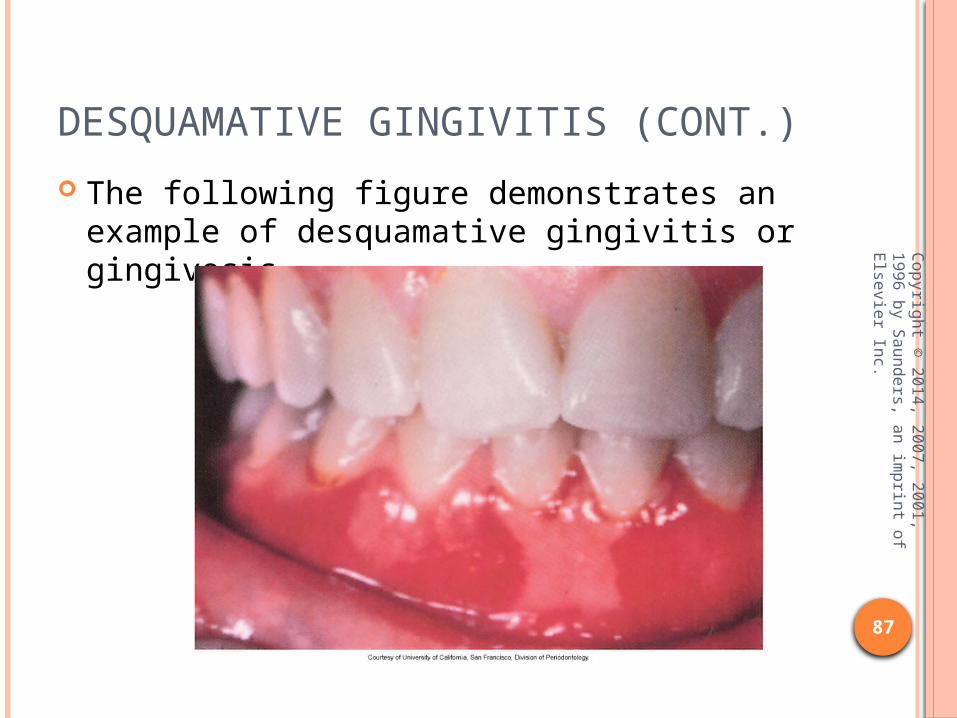
When cicatricial pemphigoid lesions are limited to the gingival tissues, the disease may be termed desquamative gingivitis or gingivosis.
This condition is most often described as sloughing of the gingival epithelium, leaving a painfully raw, red surface.
86
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.
DESQUAMATIVE GINGIVITIS (CONT.)
The following figure demonstrates an example of desquamative gingivitis or gingivosis.
87
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

DESQUAMATIVE GINGIVITIS (CONT.)
The cause is suspected to be autoimmune related, but an allergic reaction to drugs, food, or other substances may also be the cause.
Meticulous plaque control may help, but control is often difficult for the patient to perform because of the painful erosive lesions.
The disease may continue for many years or, particularly in children, may spontaneously disappear.
Topical and systemic steroid therapy may help control the disease process.
88
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

TRAUMATIC LESIONS
Often the gingival tissues are damaged by trauma.
Common traumatic lesions observed in dental hygiene practice are burns from foods, chemical burns from aspirin placed on the gingiva, or cuts.
89
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

TRAUMATIC LESIONS (CONT.)
Some interesting cases of advanced recession caused by trauma are illustrated in the following figure.
90
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.
FOREIGN BODY REACTIONS
Foreign body reactions in or near the tissues, similar to traumatic lesions, can damage the gingival tissue.
A commonly observed lesion is an acute gingival reaction to food impaction from food particles such as popcorn husks or apple skins.
These localized painful lesions have a sudden onset.
91
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.

FOREIGN BODY REACTIONS (CONT.)
The following figure demonstrates an example of such an acute gingival reaction.
92
Copyright ©
2014, 2007, 2001, 1996 by S
aunders, an imprint of E
lsevier Inc.