by - school of nursingnursing.hku.hk/dissert/uploads/cheng ka lai.pdf · wonderful master of...
TRANSCRIPT

“Evidence-based Guideline for
Antenatal Interpersonal Psychotherapy Education Program”
By
Cheng Ka lai
Bachelor of Nursing (CUHK)
Postgraduate Diploma in Occupational Health Practice (CUHK)
Master of Science in Health Care (HK PolyU)
A dissertation submitted in partial fulfillment of the requirements for
The Degree of Master of Nursing
at the University of Hong Kong
August 2013

i
DECLARATION
I declare that this dissertation represents my own works, except where due
acknowledgement is made, and that it has not been previously included in a thesis,
dissertation or report submitted to this University or to any other institution for a
degree, diploma or other qualifications.
Signed:____________________________
CHENG Ka-Lai

ii
ACKNOWLEDGEMENTS
I would like to thank Professor TIWARI and her team for their efforts in this
wonderful Master of Nursing course. I believe that evidence-based practice (EBP)
of translational nursing in Hong Kong is not just an academic issue. Viewing
Hong Kong contemporary nursing development, the emergence of EBP has
induced profound changes in clinical practice and brought modernity to nursing
science and art. EBP should emphasis on the modern evolution of nursing in Hong
Kong’s public health sector for better health outcomes. The University of Hong
Kong continues to be the icon for the best practice in nursing and enlightenment
of health care philosophy.
My heartfelt gratitude also goes to Dr. HUI-CHOI Wai-hing, Elizabeth. Dr.
HUI-CHOI shared with me her integrated experiences and wisdom throughout her
guidance of my dissertation, reacted ably to new models and new styles of nursing,
elevated my perceptions and refined my technique.
I wish to express my sincere gratitude to Dr. Marie TARRANT and Dr.
Daniel FONG, who have been abundantly helpful and offered me invaluable
assistance, support and guidance.
I would like to express my sincere thanks to Miss SING Chu, Miss WONG

iii
Shuk-ching, Ruth and Miss WONG Wai-fong, Susanna for their great supports in
my dissertation paper. I would also like to thanks my fellow classmates for
supporting each other to go through difficult times and to share happiness and
hardship during study.
Last but not least, my sincere gratitude goes to my family and MCHC
colleagues. They were patient with me and gave me encouragement and
understanding in the past 2 years.

iv
Abstract of Dissertation entitled
“Evidence-based Guideline for
Antenatal Interpersonal Psychotherapy Education Program”
Submitted by
CHENG Ka-lai
For the Degree of Master of Nursing
The University of Hong Kong
August, 2013
ABSTRACT
Background
Postnatal depression (PND) has become a world-wide public health problem.
Maternal Child Health Centers (MCHCs) provide maternal and child healthcare
with community-based Comprehensive Child Development Services (CCDS)
aimed for early identification for provision of appropriate referral for intervention.
There were 13.8% suspected PND cases in 2011(Department of Health PND
Report, 2011). Antenatal Interpersonal Psychotherapy (IPT) has found efficacious
for high depression risk (HDR) pregnant women. Evidence-based practice (EBP)

v
antenatal IPT guideline best suited for MCHCs implementation.
Purpose
This dissertation intends to develop an effective EBP antenatal IPT guideline
for HDR pregnant women, and to offer plans for implementation and evaluation.
Methods
Six electronic databases searched for updated relevant studies. Randomized
controlled trails (RCTs) with antenatal IPT intervention for HDR pregnant women
targeted. Evidence data related to EBP guideline development were extracted for
critical appraisal. Program implementation potentials assessed for transferability,
feasibility and cost-benefit ratio. Guideline with level of evidence and
recommendation grading developed. Communication plan for different
stakeholders and potential users were developed. Pilot test planned for process
evaluation. Impact evaluation, outcome evaluation and economic evaluation
planned to verify empirical evidences to initial changes in MCHCs.
Results
Eight RCTs studies, which compare group receiving antenatal IPT
intervention with routine antenatal education group, were reviewed. Target
population was HDR pregnant women. Antenatal IPT intervention found effective
for HDR pregnant women with PND. The studies suggest antenatal IPT

vi
intervention give 0.89 reductions in EPDS, improved psychological well-being,
0.77 reductions in GHQ and improved role competence 2.43 increases in PSOC-E.
After critical appraisal of reviewed studies, antenatal IPT guideline
developed. Pregnant women should be screened between 20 to 32 gestation weeks.
Those with EPDS≥13 scores should enrolled into two 2-hour antenatal IPT
program educated by trained nurse educators in class size ≤10. Those refusing to
join the program receive routine education. Three-point measurements of EPDS,
GHQ and PSOC-E at baseline, postnatal 6 to 8 weeks and 3 to 6 months of both
groups are conducted. Postnatal EPDS ≥13 participants referred for psychiatric
services upon their consent.
Program will propose implementation in MCHCs. Steering Committee is
established and communicates with various stakeholders. Pilot test implement in
one MCHC and reviewed for clinical applicability, feasibility and to obtain
process evaluation for quality improvement.
Program should have quasi-experimental non-equivalent pretest-posttest
control group and analyze data with ‘two-sample t-test’, ‘paired t-tests’ and
‘chi-square test’. Target achievement should be:
i. Primary outcomes: EPDS score reduced to 0.89, GHQ reduced to 0.77 and
PSOC-E score increased to 2.43;

vii
ii. Secondary outcomes: Reduction of PND incidence and PND management
caseloads by 20%.
Participants’ gestation ages, program attendance and satisfactory rates
recorded. Economic evaluation indicates for every $1 invested, the return is $8.45,
program is a sound investment suggested.
Conclusions
Eight RCT studies provide evidence that antenatal IPT program is effective
for HDR pregnant women in reducing PND, and in promoting higher maternal
role efficacy level and psychological well-being. Implementation of this EBP
program guideline can potentially help PND prevention and ease antenatal
depression management of HDR pregnant women in MCHCs.

viii
CONTENTS
DECLARATION……………………………………………………………. i
ACKNOWLEDGEMENTS………………………………………………… ii
ABSTRACT…………………………………………………………………. iv
TABLE OF CONTENTS…………………………………………………… viii
Chapter 1 INTRODUCTION
1.1 Background……………………………………………………..... 1
1.1.1 Postnatal Depression Definition...……………………… 1
1.1.2 Epidemiology…………………………………………… 1
1.1.3 PND Health Impacts………………….………………… 2
1.2 Hong Kong Affirming Needs ……………………………………. 4
1.2.1 Interpersonal Psychotherapy……………………………. 7
1.2.2 Study Significance……………………………………… 8
1.3 Study Objectives …….................................................................... 10
1.3.1 Short Term Objectives………………………………...... 10
1.3.2 Long Term Objectives………………………………….. 10
1.4 Outcome Measurement Tools………………..………………….. 11
1.4.1 Depressive Measurements……………………...………. 11
1.4.1.1 EPDS………………………………………… 11
1.4.1.2 BDI…………………………………………... 11
1.4.2 Psychological Well-being Measurement…………..…… 12
1.4.2.1 GHQ…………………………………………. 12
1.4.3 Maternal Role Competence Measurement……..……….. 12
1.4.3.1 PSOC………………………………………… 12
1.4.4 Appropriateness Application of Outcome Measurement
Tools…………………………………………………….
13
1.5 Research Hypothesis……..……………………………………… 14
1.6 Research Questions……………...……………….......................... 15
Chapter 2 CRITICAL APPRAISAL
2.1 Literature Search and Appraisal………………………….............. 16
2.2 Inclusion and Exclusion Criteria………………………………….. 16
2.2.1 Inclusion Criteria…………………...…………………… 16
2.2.2 Exclusion Criteria……………………………………….. 17
2.3 Systematic Search Results……………………………………....... 17
2.3.1 PsycINFO………………………………………………. 17

ix
2.3.2 British Nursing Index………………………………....... 18
2.3.3 Maternal and Infant Care………………………………... 18
2.3.4 Embase………………………………………………….. 19
2.3.5 PubMed…………………………………………………. 19
2.3.6 IsIPT…………………………………………………….. 20
2.4 Final Articles Selection……………..……………………………. 20
2.5 EBP Guideline Development…………..……………..………….. 21
2.6 Appraisal Strategies………………………………...…………...... 21
2.6.1 Assess Quality Method…………………..……………... 21
2.7 Data Summary…………………………………………………..... 22
2.7.1 Reviewed Studies Description…..…………………….... 22
2.7.2 Bibliographic Citation & Study Country………..…….... 23
2.7.3 Subject Number…………………………………………. 23
2.7.4 Subject Characteristics………………………………….. 23
2.7.4.1 High Depression Risk (HDR) Pregnancy
Women………………………………………...
23
2.7.4.2 Age……………………………………………. 24
2.7.4.3 Gestation Weeks…...…………………………. 24
2.7.4.4 Education……………………………………... 24
2.7.4.5 Marital Status…………………………………. 24
2.7.4.6 Occupational Status………………...……….... 25
2.7.4.7 Income………………………………………... 25
2.7.4.8 Dropout Rate & Reasons..………..…………... 25
2.7.5 Studies Result of Randomized Control Trials (RCTs)…. 25
2.7.6 Level of Evidence………………………………………. 27
2.7.7 Interventions…………………………………………….. 27
2.7.8 Comparison Group………………..…………………..... 28
2.7.9 Outcome Measurement Times……………………...….... 28
2.7.10 Outcome Measurements………………………………… 28
2.7.11 Effect Sizes……………………………………………… 29
2.8 Data Synthesis……………………………………………………. 29
2.9 Implications……………………………………………………..... 30
Chapter 3 IMPLEMENTATION POTENTIAL
3.1 Evidence-base Innovation………………………………………. 32
3.2 Assessing Implementation Potentials…………………………… 32
3.2.1 Transferability………………………………………….. 33
3.2.1.1 Target Setting……………………………….... 33

x
3.2.1.2 Target Audiences.……………………………. 33
3.2.1.3 Philosophy of Care………………………….... 34
3.2.1.4 Sufficient Patients Benefit……………………. 35
3.2.1.5 Innovation Implementation and Evaluation
Time…………………………………………..
36
3.2.2 Feasibility………………………………………………. 37
3.2.3 Cost and Benefit Ratio…………………………………. 39
3.2.3.1 Cost and Benefit Ratio of High Risk
Pregnancy Women……………………………
39
3.2.3.2 Cost and Benefit Ratio of Maternal and Child
Health Centers………………………………...
39
3.3 Implementation Potential Estimation…………………………… 40
Chapter 4 ANTENATAL INTERPERSONAL PSYCHOTHERAPY
EDUCATION PROGRAM GUIDELINE
4.1 Program Guideline Objectives…………………………………. 41
4.2 Intended Educator……………………………………………… 41
4.3 Target Population………………………………………………. 41
4.4 Program Implementation Guideline Instruction………………... 41
4.5 Evidence-based Antenatal IPT Education Program Guideline
Description………………………………………………………
42
4.6 Level of Evidence and Grades of Recommendations………….. 43
4.6.1 Recommendations………………………………………. 44
Chapter 5 IMPLEMENTATION PLAN
5.1 Potential Users Communication Plan…………………….………. 47
5.1.1 Communication with Department Staff Suggestions
Committee………………………………………………
48
5.1.2 Communication with Administrative and Management
Panels……………………………………………………
48
5.1.3 Formation and Responsibilities of Steering Committee. 49
5.1.3.1 Monthly Committee Meetings……………... 49
5.1.3.2 Monthly Staff Meetings……………………. 50
5.1.4 Communication with IPT Training Centre……………... 50
5.1.5 Communication with Clinical Nursing Staff Colleagues.. 50
5.1.6 Communication with IPT Nurse Educators……………. 51

xi
5.1.7 Communication with Computer Staffs…………………. 51
5.1.8 Communication with Potential Participants……………. 51
5.2 Innovation Program Evaluation Framework…………………….. 52
5.3 Pilot test………………………………………………………….. 52
5.3.1 Pilot Test Purposes….…………………………………… 52
5.3.2 Pilot Test Staff Briefing…...…………………………….. 53
5.3.3 Pilot Test Implementation……………………………… 53
5.3.4 Pilot Test Evaluation………..………………………… .. 54
5.4 New EBP Guideline Implementation……..…………………….. 54
Chapter 6 EVALUATION PLAN
6.1 Intervention Outcome Identification…………………………… 56
6.1.1 Patient Outcomes………..……………………………. 56
6.1.2 System Outcomes…………………………………….. 57
6.1.3 Healthcare Provider Outcomes……………………….. 58
6.2 Nature of Target Participants involved………………………… 58
6.3 Determining Number of Involved Target Clients.……………... 58
6.3.1 Design……………………………….……………….. 59
6.3.2 Primary Outcomes ……………….…………………… 59
6.3.3 Secondary Outcomes…………………………………. 59
6.3.4 Analysis Methods.……………………………………. 60
6.4 Data Collection and Instruments……………………………….. 60
6.5 Data Analysis…………………………………………………… 60
6.5.1 Descriptive Statistics………………………………….. 61
6.5.2 Inferential Statistics…………………………………… 61
6.6 Effectiveness Criteria…………………………………………... 61
6.6.1 Primary Outcomes……………………………………. 61
6.6.1.1 EPDS Score………………………………… 61
6.6.1.2 GHQ Score…………………………………. 62
6.6.1.3 PSOC-E Score……………………………… 62
6.6.2 Secondary Outcomes…………………………………. 62
6.6.2.1 PND Incidence Rate and PND Management
Caseloads…………………………………..
62
6.6.3 Economic Evaluation…………………………………. 62
6.6.3.1 Cost-Benefit Analysis …………………….. 62
6.6.3.2 Cost-Effective Analysis..………………….. 63
6.7 Conclusion……………………………………………………… 64

xii
CHAPTER 7 CONCLUSION…………………………………………….. 65
REFERENCES……………………………………………………… 66-85
APPENDICES….………………………………………………....... 86-156

xiii
List of Appendices
Appendix A: IPT Theory, Principles and Applications……….. 86-92
Appendix B: Literature Searching Record & Flowcharts…….. 93-98
Appendix C: Review Literature Studies Searching Record
Table…………………………………………….
99
Appendix D: Evidence Tables………………………………… 100-107
Appendix E: SIGN Randomized Control Trial Checklist……. 108-109
Appendix F: Quality Assessment of Review Literatures…….. 110-111
Appendix G: Detailed Critique of 8 RCT Studies…………….. 112-119
Appendix H: IPT Program Intervention Compare Table……… 120-122
Appendix I: Evidence-based Antenatal IPT Education
Proposed Program ……………………………....
123
Appendix J: Flowchart of Antenatal IPT Program, title as
‘Happy Mom & Happy Family………………….
124
Appendix K: Department of Health PND Report (2011)…….. 125
Appendix L: Department of Health Approval Letter for PND
Data……………………………………………..
126
Appendix M: Comparison of Setting and Characteristic
between Reviewed Literatures and Target
MCHCs…….........................................................
127
Appendix N: Estimated Potential Participants of Innovation
Program…………………………………………
128
Appendix O: Innovation Implementation Time
Allocation………………………………………
129
Appendix P: Estimation Monthly Workload of Total Contact
Time for Innovation Program…………………..
130
Appendix Q: Nursing Staff Manpower Plan…………………. 131
Appendix R: MCHC Manpower Plan……………………….. 132
Appendix S: Estimate Cost of Innovation Program…………. 133
Appendix T: PND Management Services Cost in 2011……… 134
Appendix U: Cost-benefit Ratio in Innovation Program &
Estimate Cost Saving……………………………
135
Appendix V: Implementation Timeframe Table……………… 136-137
Appendix W: Evidence-based Antenatal Interpersonal
Psychotherapy Education Program Guideline…..
138-142
Appendix X: Antenatal IPT Program Information Sheet……...
143

xiv
Appendix Y: Antenatal IPT Program Enrollment and
Attendance Form in MCHC…………………….
144
Appendix Z: Antenatal IPT Education Program Reminder
Form…………………………………………….
145
Appendix AA: Evidence-based Antenatal IPT Education
Program Consent form………………………….
146
Appendix BB: Antenatal IPT Education Program Satisfactory
Form……………………………………………
147
Appendix CC: Key to Evidence Statements…………………… 148
Appendix DD: Grades of Recommendations…………………… 149
Appendix EE: Communication Plan Timeline…………………. 150-151
Appendix FF: Pilot Test Nurse Antenatal IPT Program
Evaluation Form ………………………………..
152
Appendix GG: Antenatal IPT Program Information Poster …… 153
Appendix HH: Framework for Program Evaluation …………… 154
Appendix II: Timeline of Pilot Test ………………………….. 155
Appendix JJ: Rundown of Outcome Measurements…………... 156

xv
Abbreviations
AN-D Antenatal Depression
CBT Cognitive Behavioral Therapy
CCDS Comprehensive Child Development Service
BDI Beck Depression Inventory
DSSC Department Staff Suggestion Committee
EBP Evidence-based Practice
EPDS Edinburgh Postnatal Depression Scale
ES Effect Size
GHQ
HDR
General Health Questionnaire
High Depression Risk
IPT Interpersonal Psychotherapy
IsIPT Internet Search of International Society of Interpersonal
Psychotherapy
MCHCs Maternal and Child Health Centers
PND Postnatal Depression
PSOC Parenting Sense of Competence Scale
PSOC-E Parenting Sense of Competence Efficacy Subscale
RCTs Randomized Control Trials
SSS Staff Suggestion Scheme

1
Chapter 1
Introduction
1.1 Background
Childbirth brings both happiness and inevitable stress to parents and families.
Nonetheless, some mothers may fails to cope with resultant stresses, suffer from
mental health illnesses (Burgess, 1997). Postnatal affective disorders include:
postnatal blues, postnatal depression (PND) and puerperal psychosis (Robertson,
Celasun & Stewart, 2003).
1.1.1 Postnatal Depression Definition
PND defined, ‘any non-psychotic depressive illness of mild to moderate
severity occurring during first postnatal year (Scottish Intercollegiate Guidelines
Network, 2002). PND symptoms include depressed mood, guilt, less
concentration, disturbed sleep, increase or decrease appetite, low self-esteem and
self-harm ideas (Najman, Andersen, Bor, O’Callaghan & Williams, 2000).
1.1.2 Epidemiology
PND evoked as a global public health problem (Almond, 2009). PND
prevalence ranges from 5% - 40% (Eastwood, Phung & Barnett, 2011; Kitamura

2
et al., 2006; O’Hara, 1995; Vigod, Villegas, Dennis & Ross, 2010). In China,
PND prevalence ranges from 14%-18% (Guo, 1993; Gao, Chan & Mao, 2009).
Underestimation may up to 60% (Halbreich & Karkun, 2006).
1.1.3 PND Health Impacts
Various PND health impacts on mothers, partners and children. 50% PND
mothers have intrusive suicide and infanticide thoughts (Barr & Beck, 2008).
Postnatal psychiatric disorders associated with higher suicide risk and 6.8%
suicides reported in first year leading to 49% maternal deaths (Appleby,
Mortensen & Faragher, 1998). Suicides account for 20% postnatal deaths (Lindahl,
Pearson & Colpe, 2005). PND associated with increase paternal depression and
paternal parenting stress, resulting less optimal infant interaction (Goodman,
2008). Untreated PND leads to martial divorce or separation (Boyce, Stubbs &
Todd, 1993; Sayer, Kohn, Fresco, Bellack & Sarwer, 2001). Some couples may
have intimate violence (Vaeth, Ramisetty-Mikler & Caetano, 2010).
PND mothers have risky parenting and less parenting activities resulting poor
parent-infant relationships (Zajicek-Farber, 2010). More punitive parenting leads
to less supportive behavior (Cornish, McMahon & Ungerer, 2008). Surkan,
Kennedy, Hurley & Black, (2011) found maternal depression is positively

3
correlated to child underweight (OR 1.5, 95% CI: 1.2-1.8, P=.001) and child
stunting growth (OR 1.4, 95% CI 1.2-1.7, P=.005).
Children up to 11 years old can have significantly lower IQ score, attention
problems, and mathematic reasoning difficulties among PND group than
non-PND group (Hay et al., 2001). Children of PND women have aggressive risk
and hyperactive and anti-social behavior (Elgar, Curtis, McGrath, Waschbusch &
Stewart, 2003). Risk of social anxiety, conduct disorder, attention deficit and
hyperactivity for children at 11 years old is four times greater for those with
depressed mothers (Pawlby, Sharp, Hay & Keane, 2008).
Untreated antenatal depression (AN-D) leads to significantly increased PND
risk, hence early detection is recommended (Cox, 1992). There was 7.4%, 12.8%,
and 12% of depression during 1st, 2
nd and 3
rd trimester pregnancy (Bennett,
Einarson, Taddio, Koren & Einarson, 2004). AN-D women are 2.4 times more
likely to have PND (RR 2.44, 95%CI 1.93-3.08)(Faisal-Cury & Menezes, 2012).
Depress pregnancy women have preterm risk (RR 1.13, 95% CI 1.66-1.21,
P<.001), low birth weight (RR 1.18, 95% CI 1.07 – 1.3, P<.001) and intrauterine
retardation (RR 1.03, 95% CI 0.99 – 1.08, P=.002) (Grote, Bridge, Gavin,
Melville & Lyengars, 2011).

4
There has suggested that pregnant women experiencing depression
symptoms should offered psychological intervention (NICE, 2007). Recently,
Clatworthy (2012) suggests early identification of HDR pregnant women,
providing antenatal evidence-based psychological interventions can effective
preventing PND and deliver early treatment for AN-D pregnant women.
1.2 Hong Kong Affirming needs
In Hong Kong PND prevalence ranges from 5% to 19.9% (Cheng, Lai & Siu,
1994; Lee et al., 1998; Lee, Yip, Chiu, Leung & Chung, 2001b; Leung, Martinson
& Arthur, 2005). Lee, Yip, Leung & Chung (2000) revealed PND psychosocial
risk factors: unsatisfactory martial relationship, poor social support, past
depression history, pregnancy depression, and finance difficulties; and stressed
the importance of early identification antenatal high depression risk factors for
provide psychiatric services. Recent, significant PND predictors found including
mother-in-law conflicts, anxiety personality and antenatal depressive symptoms
(Siu, Leung, Ip, Hung & O’Hara, 2012).
Hong Kong AN-D prevalence ranges from 6.4% (Lee et al., 2004) to 37.1%
(Lee et al., 2007). Lee et al., (2007) reported AN-D prevalence rate has a
U-shaped curve with 22.1% (95%CI 19.9-24.4%) at first trimester, drop to 18.9%

5
(95%CI 16.8-21.1%) at second trimester then rise to 21.6% (95%CI 19.4-28.9%)
at third trimester and AN-D increase PND risk (adjusted OR 3.01 95%CI 1.38-6.6)
which suggest PND prevention and recommend early detection.
Hong Kong PND screening initialed by Lee et al., (1998) and Lee, Yip, Chiu,
Leung & Chung (2001a) using Chinese version of followings: Edinburgh
Postnatal Depression Scale (EPDS); General Health Questionnaire (GHQ); Beck
Depression Inventory (BDI).
Nowadays, PND screening implemented in 31 Maternal and Child Health
Centers (MCHCs) and obstetric hospitals provide with counseling and referrals.
Legislative Council Panel Paper on Comprehensive Child Development Service
(2008) reported 12% of 29,301 mothers were probable PND whose 55% provided
with nurses counseling, 28% psychiatric counseling, 3% psychiatric referral and
28% family counsel referrals.
During motherhood transition, importance to develop well-being sense and
maternal role satisfaction to reduce PND, measured by Chinese version of EPDS
and Parent Sense of Competence Scale (PSOC) has been confirmed (Ngai & Chan,
2011).

6
Pregnant women are normally unwilling to use medication as fear of adverse
offspring exposure and they prefer psychotherapy (Kim, O’reardon & Epperson,
2010). Different psychosocial interventions reduce PND include: cognitive
behavioral therapy (CBT), non-directive counseling, psycho-education program
and interpersonal psychotherapy (IPT) (Craig & Howard, 2009). Weerasekera
(2010) reported single IPT treatment during pregnancy and postnatal had a
significantly larger effect size of 1.26, when comparing to other psychotherapies’
effect size such as CBT: 0.64; psychodynamic: 0.52; counseling: 0.41; education:
0.1. Antenatal IPT found significance effect (Gao, Chan, Li, Chen & Hao, 2010)
but not significance in other therapies include: group psycho-education (Buist,
Westley & Hill, 1999), group CBT (Austin, et al., 2008), group therapies & health
visits by health visitors (Elliott et al., 2000), cognitive problem solving and social
support in group education (Brugha et al., 2000), support group (Stamp, Williams
& Crowther, 1995), PND group midwife education (Hayes, Muller & Bradley,
2001). Hence, significance antenatal IPT is the most effective intervention for
reduce PND.
National Institute of Mental Health found IPT more effective than CBT in
treating acute depression during first 6 - 8 weeks with improve psychosocial
function after 16 weeks treatment (Elkin et al., 1989). Effective use of

7
psychotherapy and choose appropriate treatment is important after understanding
clinical problems which can help formulate comprehensive basis for collaborative
planning and treatment (Tillett, 1999). Since IPT helps depressive clients to
master social and interpersonal conflicts rather than cognitive behavior or
intra-psychic issues (Judd, Weissman & Davis, 2004) and IPT differs from other
behavioral cognitive therapies which particular concerns about interpersonal
attachment problems (Barkham & Hardy, 2001), IPT tends to more responsible to
antenatal psychosocial risk factors and relationship problems in clinical
application.
1.2.1 Interpersonal Psychotherapy
IPT initialed from interpersonal theories (Sullivan, 1953) and developed in
1970s (Evan, 1996; Stuart & Franzcp, 2003). IPT is a bio-psychosocial model of
psychological functioning with interpersonally based on attachment theory
(Bowlby, 1969), communication theory (Kiesler, 1979) and social theory (Meyer,
1958). IPT targets at improving interpersonal relationship and effective
communication skills, promoting role transition and social support networks
improvement assisting adaption of psychosocial changes and soothe interpersonal
distress (Klerman, Weissman, Rounsaville & Chevron, 1984; Stuart & Franzcp,
2003; Solen, Hobson, Leighton, Mcfarlane & Law, 2009; 唐子俊, 唐慧芳, 黃詩

8
殷 & 戴谷霖 2003). IPT sessions includes: assessment, initial, middle and
maintenance. IPT suit for problems issues: grief, role transitions, interpersonal
sensitivity and interpersonal disputes (Stuart & Franzcp, 2003). IPT theory,
principles and applications showed in Appendix A.
American Psychiatric Association, National Institute for Health and Clinical
Excellence and International Cochrane Collaboration recognize IPT as an
efficacious psychotherapy (International society for IPT, 2012). IPT found
efficacious for medical ill depression patients (Schulberg et al., 1996),
HIV-positive depression patients (Markowitz et al., 1998), depressive adolescent
(Mufson, Weissman, Moreau & Garfinkel,1999), infertile depression women
(Koszycki, Bisserbe, Blier, Bradwejn & Markowitz, 2010), AN-D women (Grote,
Bledsoe, Swartz, Frank, 2004; Lau, 2005; Spinelli, 1997; Miller, Gur, Shanok &
Weissman, 2008) and PND women (Mulcahy, Reay, Wilkinson & Owen, 2010;
O’Hara, Stuart, Gorman & Wenzel, 2000; Reay, Fisher, Robertson, Adams &
Owen, 2006; Stuart & O’Hara, 1995). Antenatal IPT Hong Kong study suggests a
great demand among HDR pregnancy women (Leung & Lam, 2012). There are
guidelines supporting antenatal IPT (NICE guideline, no. 45, 2007).
1.2.2 Study Significance

9
PND is an important public health concern. However, Hong Kong antenatal
education covers antenatal care, labor management and pain relief methods, baby
care, breastfeeding and postnatal care (Ho & Holroyd, 2002). Currently, there is
no antenatal IPT program for Hong Kong HDR pregnant women leading to a
research-practice gap in nursing.
Melnyk & Fineout-Overholt (2011) stated importance to generate new
knowledge from evidence-based practice (EBP) and translate evidence into
clinical practice to improve healthcare quality and best patient outcomes. This
program will utilize EBP process steps framework in Melnyk & Fineout-Overholt
(2011): cultivate inquiry spirit, formulate PICO questions, best evidences
searching, evidences critical appraisal, integrate literatures best evidence to
implement decision, evaluate practice outcomes change based on evidence and
disseminate evidence-based change outcomes.
This is an appropriate time to shift our client-center healthcare services from
postpartum to antepartum. MCHCs serve as a platform to early identify HDR
pregnant women and provide antenatal IPT program. Nurses can take up an
advanced public health community educator role in evolving new EBP to reduce
PND, promoting psychological well-being and maternal role competence. Urgent
affirmative needs for antenatal IPT education established in MCHCs.

10
How antenatal IPT program apply in MCHCs to reduce PND, promoting
psychological well-being and maternal role competence for high depression risk
pregnant women? Clinical Questions formulate in PICO format as following
components:
Patient: High depression risk (HDR) pregnancy women
Intervention: Antenatal interpersonal psychotherapy education program
Comparison: Routine antenatal education
Outcomes: Depressive symptoms / psychological well-being /
maternal role competence in postnatal period
1.3 Study Objectives
1.3.1 Short Term Objectives:
1.3.1.1 Develop evidence-based antenatal IPT education guidelines for HDR
pregnant women.
1.3.1.2 Gather empirical evidence on antenatal IPT education in reducing
PND and promote higher level of maternal role competence and better levels of
psychological well-being for HDR pregnant women.
1.3.2 Long Term Objectives:
1.3.2.1 To promote mental health of HDR pregnant women.
1.3.2.2 To increase maternal role competence to promote attachment bonding
and family functioning of HDR pregnant women.

11
1.3.2.3 To decrease maternal mortality related to suicides among HDR
pregnant women.
Outcome Measurement Tools
1.4.1 Depressive Measurements
1.4.1.1 Edinburgh Postnatal Depression Scale (EPDS)
EPDS, a quick and user friendly screening tool, based on 10 items self-report
rating scale with four response choices (score from 0-3): “Normal” response has a
score of “0” up to “Severe” response of “3” and question 10 of self-harm which
measure PND symptoms over past 7 days (Cox, Holden & Sagovsky, 1987) and
used during antenatal (Cox & Holden, 2003). Split-half reliability and
standardized alpha coefficients reported are 0.88 and 0.87 respectively (Cox,
Holden & Sagovsky, 1987).
The Chinese version of EPDS validated with optimal cut-off score of 9/10
with 82% sensitivity, 86% specificity, 44% positive predictive value, 97%
negative predictive value at six postpartum weeks (Lee, et al., 1998). EPDS used
in PND screening and six months follow-up which found better mental health
outcomes in MCHCs (Leung et al., 2010).
1.4.1.2 Beck Depression Inventory (BDI)

12
Beck Depression Inventory (BDI) is a 21-items tool to measure depression
severity (Beck & Beck, 1972). Its Chinese version validated with optimal cut-off
score 10/11 with 82% sensitivity, 89% specificity, 50% positive predictive value,
97% negative predictive value (Lee, et al., 2001a).
1.4.2 Psychological Well-Being Measurement
1.4.2.1 General Health Questionnaire (GHQ)
GHQ, a 12-item tool, is used to measure psychological well-being to
identifying neurotic anxiety disorders (Nott & Cutt, 1982). It uses a rating scale
with four response choices: ‘not at all’ have ‘0’ score; ‘no more than usual’ have
score of ‘1’; ‘rather more than usual’ have score of ‘2’ and ‘much more than usual’
have score of ‘3’. Its Chinese version validated with optimal cut-off score 4/5 with
88% sensitivity, 89% specificity, 52% positive predictive value ,98% negative
predictive value (Lee, et al., 2001a). There are several Hong Kong clinical studies
of GHQ application (Lee, et al., 1998; Lee, et al., 2001a; Lee, et al., 2001b; Leung,
et al., 2010).
1.4.3 Maternal Role Competence Measurement
1.4.3.1 Parenting Sense of Competence Scale (PSOC)

13
PSOC is a 17 items instrument separated into 2 subscales, i.e. Efficacy
Subscale with 8 items (PSOC-E) measuring maternal role competence level and
Maternal Role Satisfaction and Comfort Subscale with 9 items (Gibaud-Wallston
& Wandersman, 1978).
PSOC-E 8-item subscale has a 6-point scale ranging from ‘1’ being
‘strongly disagree’ to ‘6’ being ‘strongly agree’. Total scale ranges from 8 to 48,
higher scores indicating higher maternal role competence. The Chinese version of
PSOC validated with internal consistency 0.82; four weeks test-retest reliability
0.84 and PSOC-E validated with internal consistency 0.8 with significant
negatively correlated 0.31with EPDS (Ngai, Chan & Holroyd, 2007). There are
Hong Kong clinical PSOC application for maternal role measurement (Ngai &
Chan, 2011) and PSOC-E for maternal role efficacy used by Ngai, Chan & Ip
(2009).
1.4.4 Appropriateness Application of Outcome Measurement Tools
Both EPDS and BDI can use for PND screening. However, BDI for PND
detection is limited and has low ability of PND identification (Harris, Huckle,
Thomas, Johns & Fung, 1989). BDI is an insensitive detection tool for minor
depression leading to substantial false negatives (Whiffen, 1988). On the other

14
hand, EPDS can improve PND awareness of physicians and midwives by 83%;
and 92% of clients with high EPDS scores for referral (Schaper, Rooney, Kay,
Silva, 1994). EPDS is a simple and inexpensive screening tool (Lee & Chung,
1999), used extensively worldwide (Lee, et al., 2000) and acceptable to both
women and healthcare professionals (Hewitt et al., 2009). Beck & Gable (2001),
EPDS and BDI reported can identify 78% and 56% of PND, respectively. Lastly,
EPDS-GHQ double test reported increased positive predictive value up to 78%
(Lee, Yip, Chiu & Chung, 2000a). Thus, ‘EPDS & GHQ’ are used in this study.
For maternal role competence measurement, program focusing on women’s role
competence sense in efficacy, PSOC-E is suitable.
1.5 Research Hypothesis
1.5.1 HDR pregnancy women undergoing antenatal IPT program can
reduce their chance of suffering PND than those having routine
antenatal education.
1.5.2 HDR pregnancy women undergoing antenatal IPT program can have
better levels of psychological well-being than those having routine
antenatal education.

15
1.5.3 HDR pregnancy women undergoing antenatal IPT program can have
a higher level of maternal role competence efficacy level than those
having routine antenatal education.
1.6 Research Questions
1.6.1 How effectiveness of antenatal IPT program for HDR pregnancy
women as compared to routine education in reducing PND?
1.6.2 How effectiveness of antenatal IPT program for HDR pregnancy
women as compared to routine education in promote better
psychological well-being?
1.6.3 How effectiveness of antenatal IPT program for HDR pregnancy
women as compared to routine education to promote higher efficacy
level of maternal role competence?

16
Chapter 2
Critical Appraisal
To review effectiveness of antenatal IPT education, a systematic review of
relevant studies has performed for evidence-based IPT guidelines.
2.1 Literature Search and Appraisal
Randomized controlled trials (RCTs) studies on HDR pregnancy women and
antenatal IPT were targeted. Comprehensive database reviewed in University of
Hong Kong Library: PsycINFO, British Nursing Index, PubMed and the Chinese
University of Hong Kong: Maternal & Infant Care & Embase. No limitation on
publication years and language for relevant studies searching in 5 databases.
Internet searched on public domain of International Society of IPT. Keywords
using includes: ‘interpersonal psychotherapy’, ‘antenatal’, ‘postnatal’,
‘postpartum’, ‘perinatal’, ‘antepartum’, ‘prenatal’, ‘pregnancy’, ‘childbearing’
and ‘depression’.
2.2 Inclusion and Exclusion Criteria
2.2.1 Inclusion Criteria
Inclusion criteria are included:

17
i. Pregnancy women subjects with HDR.
ii. Antenatal IPT study used to reduce PND.
iii. RCTs study.
iv. Primary source studies.
2.2.2 Exclusion criteria
Exclusion criteria are included:
i. Pregnancy women subjects with current mental illness.
ii. Pregnancy women subjects with obstetric complications.
2.3 Systematic Search Results
Record of literature searches are shown in Appendix B.
2.3.1 PsycINFO
In PsycINFO, from earliest date to August 28 2012 and search used
keywords formed by combining ’interpersonal psychotherapy’ and ‘antenatal’,
‘postnatal’, ‘postpartum’, ‘perinatal’, ‘antepartum’, ‘prenatal’, ‘pregnancy’ and
‘childbearing’ separately revealed 257 relevant studies. Further combine each set
of searched results with ‘depression’ separately found 180 relevant studies.
Manual screening on titles and abstracts conducted on total 437 studies. 391
studies were excluded by adopting Exclusion Criteria. Manual screened on 46

18
relevant studies, 40 duplicated studies excluded. Finally, 6 relevant studies
selected.
2.3.2 British Nursing Index
In British Nursing Index database from 1994 to August 28, 2012 updated and
using keywords ‘interpersonal psychotherapy’ generated 52 studies, then combine
with ‘antenatal’, ‘postnatal’, ‘postpartum’, ‘perinatal’, ‘antepartum’, ‘prenatal’,
‘pregnancy’, ‘childbearing’, ‘depression’ separately that retrieved 26 studies.
Each searched results further combine with ‘depression’ separately generated 9
studies. Total of 87 studies obtained for manual screening review on titles an
abstracts.
By Exclusion Criteria mentioned, 71 studies excluded. Finally, 2 relevant
studies selected as manual screened revealed 14 duplicated studies.
2.3.3 Maternal and Infant Care
An advanced search using keywords of ‘interpersonal psychotherapy’
combined with ‘antenatal’, ‘postnatal’, ‘postpartum’, ‘perinatal’, ‘antepartum’,
‘prenatal’, ‘pregnancy’, ‘childbearing’ and ‘depression’ separately in Maternal &
Infant Care’s database from 1971 to August 28, 2012 updated revealed 77 studies.

19
By Exclusion Criteria mentioned, 55 studies excluded. Manual screening on titles
and abstracts was subsequently carried out. Finally, 4 relevant studies selected as
final manual screening discovered18 studies duplicated.
2.3.4 Embase
In Embase database from 1980 to August 28, 2012 updated, basic search of
‘interpersonal psychotherapy’ used and search in multi-field search combine with
‘antenatal’, ‘postnatal’, ‘postpartum’, perinatal’, ‘antepartum’, ‘prenatal’,
‘pregnancy’, ‘childbearing’ separately generated 148 studies. Then keyword
search of ‘depression’ with RCTs limitation revealed 130 studies.
Titles and abstracts of these 278 studies were manual screened. By Exclusion
Criteria mentioned, 254 studies excluded. Finally, 5 relevant studies selected as
revealed 19 duplicated studies.
2.3.5 PubMed
For PubMed database from 1950 to August 28, 2012 updated, ‘Interpersonal
psychotherapy’ search gave 8,223 studies. By limiting to RCTs study, 625 studies
generated and combine with ‘antenatal’ resulted in 5 studies with 5 relevant
studies; ‘postnatal’ resulted in 8 studies with 4 relevant ones; ‘postpartum’
resulted in 16 studies with 6 ones; ‘perinatal’ resulted in 2 studies with 1 relevant

20
one; ‘antepartum’ resulted in 1 relevant study; ‘prenatal’ resulted in 4 studies with
3 relevant ones; ‘pregnancy’ resulted in 14 studies with 6 relevant ones,
‘childbearing’ resulted in 4 studies with 2 relevant ones; ‘depression’ resulted in
310 studies with 6 relevant ones. One search using ‘interpersonal psychotherapy’
combined with ‘antenatal’ and ‘depression’ resulted in 13 studies with 6 relevant
ones.
Manual screened on titles and abstract of resulting 1,002 studies. By
Exclusion Criteria mentioned, 962 studies extracted. Finally, 7 studies selected as
manual screening revealed 33 duplicated studies.
2.3.6 International Society of Interpersonal Psychotherapy (isIPT)
internet searching
Titles of 125 studies reviewed in isIPT website. 123 studies excluded by
Exclusion Criteria, non-full text study, non-English and duplicated. Finally, 2
studies selected.
2.4 Final Articles Selection
In PsycINFO, British Nursing Index, Maternal & Infant Care, Embase,
PubMed and isIPT revealed 2,006 studies. 1,856 studies excluded by Exclusion
Criteria. Remaining 150 studies, 124 studies duplicated. Studies number reduced

21
to 26. These 26 studies comprises 6 from PsycINFO, 2 from British Nursing
Index, 4 from Maternal & Infant Care, 5 from Embase, 7 from PubMed, and 2
from isIPT. After removing duplications among the databases, finally 8 RCTs
studies selected for analysis. More details on studies selection are shown in
Appendix C.
2.5 EBP Guideline Development
Seven-level hierarches of evidence level (Melnyk & Fineout-Overholt, 2011)
used in this Study. After literature reviews of eight RCTs studies, relevant data
extracted and organized in Evidence Table shown in Appendix D. Evidence Table
columns cover bibliographic citation & study country, study type & evidence
level, subject characteristics, study site number, intervention, comparison, length
of follow up, outcome measurement, effect size, randomization and blinding
method.
2.6 Appraisal Strategies
2.6.1 Assess Quality Method
RCTs Checklist developed by Scottish Intercollegiate Guidelines
Network(SIGN)(2008a) for quality assessment used for this study and shown in
Appendix E which assists in objectives establishment to improve healthcare

22
quality through clinical EBP guideline development.
Review criteria are appropriateness and clarity of research questions,
randomization, concealment allocation, blinding aspect, baseline similarity
between intervention and comparison group, group difference in treatment under
investigation, validity and reliability of relevant measures outcome, dropout rate,
data analysis method of intention-to-treat, and result comparable for other sites.
Review tools: ‘well covered’, ‘adequately addressed’, ‘poorly addressed’,
‘not addressed’, ‘not reported’ and ‘not applicable’ used to ascribe quality aspects.
For level of evidence based on SIGN grading system (SIGN, 2008a), studies
fulfilling all or most criteria graded “1++”, fulfilling some criteria graded “1+” ,
and fulfilling a few or none of criteria graded ‘1-‘.
Quality assessment and detailed critique of selected literatures are shown in
Appendix F and Appendix G, respectively.
2.7 Data Summary
2.7.1 Reviewed Studies Description
Eight studies identified and appraised with above criteria with RCTs
checklist. Studies summary descriptions are bibliographic citation and study
country, number of subjects, subject characteristics, study site number, studies
result of RCTs, level of evidence, intervention, comparison group, outcome

23
measurements times, outcome measurement, effect size, randomization and
blinding method.
2.7.2 Bibliographic Citation and Study Country
Eight selected RCTs studies bibliographic presented in Table of Evidence,
cited from 2001 to 2012. Five studies conducted in U.S.A., two conducts in the
People’s Republic China and one conducted in Hong Kong.
2.7.3 Subject Numbers
Sample sizes of selected studies range 36 to 194. Three studies sample size
are ≥150 (Gao, et al., 2010; Gao, Chan & Sun, 2012; Leung & Lam, 2012). Two
studies have between 50 and 100 (Grote et al., 2009; Zlotnick, Miller, Pearlstein,
Howard & Sweeney, 2006). Three studies sample sizes are ≤50 (Crockett,
Zlotnick, Davis, Payne & Washington, 2008; Spinelli & Endicott, 2003; Zlotnick,
Johnson, Miller, Pearlstein & Howard, 2001).
2.7.4 Subject Characteristics
2.7.4.1 High Depression Risk Pregnancy Women
Some indications of HDR subjects’ characteristics include: risk factors
survey of previous depression history, poor social support, BDI >10 and recent
stressful event (Zlotnick, et al., 2001), Hamilton Depression Rating Scales >12
(Spinelli & Endicott, 2003), Cooper Predictive Index >27 (Zlotnick, et al., 2006),

24
Cooper Risk Score Index >27 (Crockett, et al., 2008), EPDS ≥12 (Grote, et al.,
2009), EPDS ≥13 (Leung & Lam, 2012) and first pregnancy (Gao, et al., 2010;
Gao, et al., 2012). Reviewed 8 studies excluded major current depression subject
under psychiatric treatment.
2.7.4.2 Age
Mean ages of all studies range 23.4 to 31.3.
2.7.4.3 Gestation weeks
All subjects gestation weeks range from 20 to 32 weeks. Details are: ≥ 28
weeks (Gao, et al., 2010; Gao, et al., 2012), 24 to 31 weeks (Crockett, et al., 2008),
20 to 22 weeks (Grote, et al., 2009; Leung & Lam, 2012; Spinelli & Endicott,
2003), 20 to 32 weeks (Zlotnick, et al., 2001) and 23 to 32 weeks (Zlotnick, et al.,
2006).
2.7.4.4 Education
Subjects’ education level are: 41.4% high school (Crockett, et al., 2008);
66% high school (Zlotnick, et al., 2006), 84.6% above college (Gao, et al., 2010);
86.5% above college (Gao, et al., 2012), 87.5% high school or above (Grote, et al.,
2009) and 52% tertiary or below (Leung & Lam, 2012).
2.7.4.5 Marital Status
Two studies recruited married subjects (Gao, et al., 2010; Gao, et al., 2012).

25
Single or cohabit subjects recruited in other studies with following percentage:
67% (Zlotnick, et al., 2006), 77% (Zlotnick, et al., 2001), 83.8% (Crockett, et al.,
2008), 37.5% (Grote, et al., 2009), 8.2% (Leung & Lam, 2012) and 51% (Spinelli
& Endicott, 2003).
2.7.4.6 Occupational Status
There are unemployed subjects in the studies: 36.1% (Crockett, et al., 2008),
63.5% (Grote, et al., 2009), 25% (Leung & Lam, 2012), 68.6% (Spinelli &
Endicott, 2003) and 0.55% unskilled (Gao, et al., 2010; Gao, et al., 2012).
2.7.4.7 Income
Three types of subjects’ income concerned: public assistance (Crockett, et al.,
2008; Zlotnick, et al., 2001; Zlotnick, et al., 2006), low income (Grote, et al., 2009;
Spinelli & Endicott, 2003) and stable income (Gao, et al., 2010; Gao, et al., 2012;
Leung & Lam, 2012).
2.7.4.8 Dropout Rate & Reasons
All studies’ dropout rate ranges from 5.26% to 24% with reasons: mastitis,
pneumonia, preterm labors, lack of time, moved out of state and loss contact.
Spinelli & Endicott (2003) stated no dropout reason.
2.7.5 Studies Result of RCTs
All selected studies used pretest-posttest control groups RCTs designed

26
comparison between IPT group and routine group. For internal validity, all studies’
research question and randomization are ‘well covered’. Randomization methods
mentioned: table of random numbers (Gao, et al., 2012), permuted block
assignment (Grote, et al., 2009) and computer generated permuted block in subset
of 4 (Leung & Lam, 2012).
Concealment methods mentioned: ‘well covered’ (Leung & Lam, 2012),
‘adequately addressed’ (Gao, et al., 2010; Gao, et al., 2012) and ‘not reported’ in
other five studies.
Blinding methods mentioned: ‘Adequate addressed’ (Gao, et al., 2010) by
blinding research assistant to treatment, collect and conduct data analysis; Leung
& Lam (2012) by blinding research staff for data collection and ‘not reported’ in
other six studies.
All studies ‘well covered’ in baseline similarity between intervention and
comparison groups, treatment under investigation, validity and reliability of
outcome measures. Five studies used intention-to-treat analysis to reduce bias
(Gao, et al., 2010; Gao, et al., 2012; Grote, et al., 2009; Leung & Lam, 2012;
Spinelli & Endicott, 2003); ‘poor addressed’ in other studies that bias might affect
results.
Data compare more than one site: 6 clinics (Leung & Lam, 2012), maternal

27
clinics (Spinelli & Endicott, 2003) and other studies conducted in one site which
‘not applicable’ reported. All studies are certainly about clinical effectiveness and
applicability to target subjects.
2.7.6 Level of Evidence
Five studies gained a grading of 1++ (Gao, et al, 2010; Gao, et al., 2012;
Grote, et al., 2009; Leung & Lam, 2012; Spinelli & Endicott, 2003) and three
studies gained grading of 1+ (Crockett, et al., 2008; Zlotnick, et al., 2001;
Zlotnick, et al., 2006).
2.7.7 Interventions
All selected studies focus on IPT problem areas: grief, interpersonal disputes,
role transition, interpersonal sensitivity shown in Appendix H. Program sessions
arranged: two 60 to 90 minutes (Gao, et al., 2010; Gao, et al., 2012), four 60 to 90
minutes (Crockett, et al., 2008; Leung & Lam, 2012; Zlotnick, et al., 2001;
Zlotnick, et al., 2006), eight 45 minutes (Grote, et al., 2009) and sixteen 45
minutes (Spinelli & Endicott, 2003). Class sizes ranged from <10 to 25. Four
studies educated by trained nurse midwife (Gao, et al., 2010; Gao, et al., 2012;
Leung & Lam, 2012; Zlotnick, et al., 2006). Three studies’ therapists were PhD or
M.D. qualifications (Crockett, et al., 2008; Grote, et al., 2009; Spinelli & Endicott,
2003). IPT educators established therapeutic relationships to develop social

28
support with communication skills. Activities include games, lectures, discussions,
role play, demonstrate and return demonstration, communication analyses,
teaching and IPT skills practice and handout issue. For subjects with postnatal
EPDS≥13 scores were referred to psychiatric service upon their consent (Gao, et
al., 2010; Gao, et al., 2012).
2.7.8 Comparison Group
All studies used routine education for their comparison groups includes:
care-as-usual pamphlets (Crockett, et al., 2008); four hours delivery and childcare
education (Gao, et al., 2010); antenatal and postnatal education covering
breastfeeding, infant care, labor process and pain relief (Gao, et al., 2012); usual
clinic education program (Grote, et al., 2009); antenatal education program
(Leung & Lam, 2012); parent education program (Spinelli & Endicott, 2003); and
standard antenatal clinic education (Zlotnick, et al., 2001; Zlotnick, et al., 2006).
2.7.9 Outcome Measurement Times
Time measurements is varied among all studies: at postnatal 6 to 8 weeks
(Gao, et al., 2010; Gao, et al., 2012; Leung & Lam, 2012); at postnatal 3 to 6
months (Gao, et al., 2012; Grote, et al., 2009; Spinelli & Endicott, 2003; Zlotnick,
et al., 2001; Zlotnick, et al.,2006).
2.7.10 Outcome Measurements

29
Outcome measurement of selected studies used EPDS (Crockett, et al., 2008;
Gao, et al., 2010; Gao, et al., 2012; Grote, et al., 2009; Leung & Lam, 2012;
Spinelli & Endicott, 2003), GHQ (Gao, et al., 2010; Gao, et al., 2012) and
PSOC-E (Gao, et al., 2012).
2.7.11 Effect Sizes
In four studies (Gao, et al., 2010; Gao, et al., 2012; Grote, et al., 2009;
Spinelli & Endicott, 2003), significant reductions in EPDS reported (-0.89 to
-3.76, P=.000). Two studies (Gao, et al., 2010; Gao, et al., 2012) reported
significance reductions in GHQ (-3.3 to -0.77, P<.01). A significance increase of
PSOC-E (2.43, P=.016) reported (Gao, et al., 2012).
2.8 Data Synthesis
All eight selected RCTs studies found evidence that antenatal IPT program
implement in maternal clinics can reduce PND; promote psychological well-being
and maternal role effectively among HDR pregnancy women. High risk
population identified by using Chinese version of EPDS ≥13 and measurement
with GHQ & PSOC-E (Gao, et al., 2010; Gao, et al., 2012; Leung & Lam, 2012).
Recruit pregnant women at gestation 20 to 32 weeks are supported by all
eight selected RCTs studies. Two studies support a 2 two hours program in group
size ≤10 can minimize barrier to care and facilitate attendance revealed (Gao, et
30
al., 2010; Gao, et al., 2012).
Four problem areas include: role transition, grief, interpersonal dispute and
interpersonal sensitivity. Other issues include IPT skills, communication skills,
motherhood transition and PND management, baby gender and martial
relationship issues, establishment of social support, conflict resolution skills and
Chinese postnatal practice.
A proposal for evidence-based antenatal IPT education program shown in
Appendix I. Trained nurses as educators is both easy and simple to program
implementation. Program includes learning activities such as games,
brainstorming, discussions, lectures, role play to motivate engagement (Gao, et al.,
2010; Gao, et al., 2012; Leung & Lam, 2012; Zlotnick, et al., 2006). The issue of
handouts definitely helps facilitate skills practice (Crockett, et al., 2008; Gao, et
al., 2012; Leung & Lam, 2012).
Postnatal measurements arranged at 6 to 8 weeks (Gao, et al., 2010; Gao, et
al., 2012; Leung & Lam, 2012) and 3 to 6 months (Gao, et al., 2012; Grote, et al.,
2009; Spinelli & Endicott, 2003; Zlotnick, et al., 2001; Zlotnick, et al., 2006).
Refer subjects with postnatal EPDS≥13 for psychiatric services upon their consent
(Gao, et al., 2010; Gao, et al., 2012).
2.9 Implications

31
PND has various health impacts. Antenatal IPT program can prevent PND;
promote psychological well-being and maternal role competence. Suggested
principles for implementation of the evidence-based IPT antenatal program
included: Early identify HDR pregnancy women by EPDS≥13; Recruit between
20 to 32 gestation weeks; Trained IPT nurse as educator; Group class size limited
≤10; Program in two 2 hours classes; Follow IPT contents with learning activities;
Psychiatric services referral if postnatal EPDS≥13; Measurement of EPDS, GHQ
and PSOC-E: baseline, 6 to 8 week and 3 to 6 months.
Finally, evidence-based antenatal IPT clinical program is likely to reduce
PND and promote joyful motherhood, resulting in happy families in Hong Kong.

32
Chapter 3
Implementation Potentials
In Chapter one, urgent needs of antenatal IPT education for HDR pregnancy
women to reduce PND and promote higher maternal role efficacy level and
psychological well-being be affirmed. This Chapter illustrates an Evidence-based
innovation and implementation potential assessments for proposed antenatal IPT
program.
3.1 Evidence-Based Innovation
Proposed innovative guidelines screen HDR pregnant women between 20 to
32 gestation weeks by EPDS ≥13 with baseline GHQ and PSOC-E obtained;
program contains two 2-hour educational in group ≤10; two postnatal
measurements of EPDS, GHQ and PSOC-E at 6 to 8 weeks and 3 to 6 months.
IPT trained nurse educator in-charge of the innovation program. Guideline
flowchart showed in Appendix J.
3.2 Assessing Implementation Potentials
To evaluate innovation EBP program implementation potentials, it is
important to consider transferability, feasibility and cost-benefit ratio (Polit &
Beck, 2008).

33
3.2.1 Transferability
3.2.1.1 Target Setting
It is a ‘window of opportunity’ for PND prevention during antenatal.
Target setting is 31 MCHCs which operate maternal shared-care program with
public hospitals, providing antenatal, postnatal care and education program for
Hong Kong pregnant women. According to Department of Health PND Report
(2011), 3883 suspected PND cases being identified in 31 MCHCs and other
services demand showed in Appendix K. Permission letter from Department of
Health approval showed in Appendix L.
3.2.1.2 Target Audiences
Target audiences are HDR pregnancy women MCHCs attendants. In
Chapter 2, 5 RCTS studies gained 1++ rating and 3 gained 1+ rating. This is a
strong indication that evidence-based innovation program in maternal clinics are
beneficially transferable to target audience in MCHCs. Pilot study is suggested
conduct in a MCHC.
Setting and characteristics shown in 8 selected studies are compared with
target MCHCs for similarities. For setting comparison, two studies conducted
Chinese population in mainland China (Gao, et al., 2010; Gao, et al., 2012) and

34
one study conducted in local MCHC (Leung & Lam, 2012). Target MCHCs
setting has 125 PND caseloads and provides maternal services, antenatal and
postnatal education; and consider similar to 8 reviewed studies which has PND 36
to 194 caseloads and provides maternal services, antenatal and postnatal
education.
For characteristics comparison, Siu, et al., (2012) provided data of target
MCHCs Chinese pregnant attendants have mean age of 28.8, gestation at 20 to 32
weeks, 74.3% secondary school level, 93.3 % married, 51.7% unemployed, public
charge services, and mean EPDS 17.8 which found comparable similar with 8
reviewed studies of 23. 4 to 31.3 mean age; gestation at 20 to 32 weeks; 41.4 to
87.5% high school level; 16% to 100% married; 36 to 68.6% unemployed; with
stable, low or no (i.e. receiving public assistance) income and mean EPDS ≥13.
Similarity between setting and characteristics of eight selected RCTs
study and target MCHCs suggest a strong transferability of innovation program.
More comparison details showed in Appendix M.
3.2.1.3 Philosophy of Care
Department of Health mission is to empower clients to improve their
health with client-focus, quality assured, evidence-based service and continuous

35
professional development and upgrade healthcare services with fostering
innovation for public health leadership (Department of Health, Family Health
Service, 2012).
Since 2005, a community-based Comprehensive Child Development Service
(CCDS) has implemented in MCHCs. CCDS aims for early identification of
various health needs of mothers, children, and family for timely referral to
appropriate services such as nurse counsel and psychiatric services (Department
of Health, Evaluation Report of Comprehensive Child Development Service,
2007).
Department of Health plan to expand CCDS to 31 MCHCs, targets to
identify at-risk pregnant women, PND mothers, and psychosocial problems
families and pre-primary children with health, developmental and behavioral
problems for appropriate healthcare referral (Legislative Council Panel Paper on
CCDS, 2012). Innovation antenatal IPT program may implement in MCHCs to
prevent PND, promote maternal role efficacy and psychological well-being
effectively.
3.2.1.4 Sufficient Patients Benefits
There were 3,883 suspected PND cases in 2011(Department of Health
PND Report, 2011). Based on 88.3 to 93% response rate reported in 8 selected

36
studies, there estimate 3,428 to 3,883 potential participants who can benefit under
innovation program. More detailed calculation shown in Appendix N.
3.2.1.5 Innovation Implementation and Evaluation Time
Innovation program includes following 3 areas:
i. Antenatal identify HDR pregnant women at 20 to 32 gestation week by 2
minutes screening of EPDS ≥13 with baseline GHQ and PSOC-E obtained.
ii. Two 2 hours education program arranged for group size ≤10, contents
including four IPT problems areas (interpersonal dispute, role transition,
grief and interpersonal sensitivity) and issues (IPT skills, interpersonal
relationship skills and PND management).
iii. Two 5-minute measurements by EPDS, GHQ and PSOC-E at postnatal 6 to 8
weeks and postnatal 3 to 6 months during attendance. Satisfactory rate
obtained after program.
It is proposed to have one-year innovative program which induces
minimal workload but has proven effective and efficient for HDR women in PND
prevention and promoting high maternal role efficacy level and psychological
well-being. It matches Department of Health, MCHCs financial and resources
situation. Innovation program time allocations details showed in Appendix O.

37
3.2.2 Feasibility
To facilitate feasibility in program implementation, barriers from
organization, nursing-profession, client-related and nurse-related should be
overcome.
Department of Health mission is to empower clients to improve their
health by providing them with cost-effective and evidence-based services, thus
enforcing its public health leader role. Innovation program is an EBP that
facilitates leadership in public health.
Gaining administrative supports for first year innovation program
implement in MCHCs, information documents will provide to Director of Health
include: additional manpower of 251.7 man-hours per month (Appendix P), 18
nurses are required (Appendix Q), 8 MCHCs manpower plan (Appendix R), IPT
program cost (Appendix S), PND management services cost (Appendix T),
cost-benefit ratio of 0.17 (Appendix U), timeframe table (Appendix V) and
evidence-based guidelines (Appendix W), facilitate ownership of ‘quality care of
service’ and EBP leadership commitment.
Monthly departmental meetings elaborate guidelines details and
improve schedule flexibility to ensure program fidelity. It is important gain

38
Director’s support for staff training, resource allocation, computer reporting
network, questionnaires license and program research approval should be obtained.
Good communications with other professionals such as medical officers and
computer network staffs and clerical staffs are necessary for enhancing adaptation,
smooth implementation and satisfactory results achievement.
To overcome barriers from nursing profession, monthly meeting
between clinical staffs and nurse educators will facilitate good communication
and improve team spirits. Provision of program flowchart, guideline details,
benefits and training opportunities can increase program acceptability to nursing
profession.
Client-related barrier can reduced or removed by assigning nurse
discussion with pregnancy women concerning program time schedule to facilitate
engagement and address their other concerns.
Staff training recruitment announced by e-mail and motivated staffs
should be given priority for training. One MCHC will implement a pilot scheme
to identify hurdles and improvement areas to ease subsequent full implementation
of the program. To ensure that program is sustainable, consideration must be
given to staff replacement and other human resources issues, result 18 nurse

39
educators training (Appendix Q). There are 4 classes monthly each with 10
attendants resulting 480 participants yearly in 8 MCHCs planned (Appendix R).
3.2.3 Cost and Benefit Ratio
3.2.3.1 Cost and Benefit Ratio of HDR Pregnancy Women
Innovation program is an educational program, considered as a safe
practice that poses no potential risk and adverse effect to pregnant women. Each
participating pregnant woman will spend 4.2 hours to prevent PND, promote
higher efficacy level of maternal role and psychological well-being.
3.2.3.2 Cost and Benefit Ratio of MCHCs
A typical program incurs IPT training course fees of $18,000; nurses
training (16 hours) cost of $67,392; screening depression risk cost of $170,270;
materials cost of $3,000 and program participant ($140 each) cost of $543,620.
Total estimated program costs are $802,282 and estimated maintenance cost is
$716,890 (Appendix S).
Department of Health provides free maternal services. But meeting
services demands implies costs. Department of Health PND report 2011 estimate
PND management services costs as follows: Nurse identifies and counseling for
3,883 cases cost of $454,311; Brief nurse follow-up cost of $75,172.5; Nurse

40
follow-up cost of $88,978.5; Medical officer counsels cost of $175,280;
Psychiatric nurse referrals cost of $3,789,240; Referral to A&E department costs
of $11,200; Total PND management services cost is $4,594,182 (Appendix T).
Cost-benefit ratio estimated to be 0.17 (Appendix U). Each PND woman
management cost is $1,183. Cost-benefit ratio of each program participant is 0.12
(Appendix U). It can calculate that innovation program can possibly save a total
PND management cost of $919, 310.8 if PND cases reduced by 20% as
innovation program implementation.
3.3 Implementation Potential Estimation
Proposed innovation program is feasible, transferable and cost-effective,
providing an “all-win” situation for Department of Health, nurses, HDR pregnant
women by reducing PND, promoting higher maternal role efficacy level and
psychological well-being. Program implementation also means compliance with
the philosophy of care, service upgrading, better professional development and
reduction in both in financial burden and management services demand.

41
Chapter 4
Antenatal IPT Education Program Guidelines
This chapter illustrates evidence-based antenatal IPT program guideline
with recommendations grading.
4.1 Program Guidelines Objectives
A set of guidelines has to be developed to guide MCHC nurse staffs in
implementing innovation program for HDR pregnant women to preventing or
reducing PND, and improve maternal role competence and psychological
well-being.
4.2 Intended Educator
Intended educators are trained nurses working in MCHCs.
4.3 Target Population
Target populations are HDR pregnant women screened with EPDS ≥ 13
in 31 MCHCs.
4.4 Program Implementation Guidelines and Instructions

42
HDR screened at 20 to 32 gestation weeks by EPDS ≥13. Invite HDR
pregnant women to join innovation program after their signing of consent form.
Follow enrolment procedures and issue education program reminder form
provided.
For refusal cases, arrange routine education. Arrange medical
assessment and referral for psychiatric services if needed.
Screened low depression risk women and arrange for them routine
education and postnatal assessment EPDS, GHQ and PSOC-E at 6 to 8 weeks and
3 to 6 months. Provide ad hoc medical officer assessment if necessary. More
details are shown in the flow chart in Appendix J.
4.5 Evidence-Based Antenatal IPT Program Guidelines
Description
As shown in Appendix W, evidence-based antenatal IPT education
program guidelines covers following 4 areas:
(i) Roles of MCHC staffs including those at head offices, clinical staff nurses,
nurse educators, medical officers and nursing officers.
(ii) Antenatal identification at 20 to 32 gestation weeks to search for those
with HDR, EPDS ≥13 being the criterion and with baseline GHQ and PSOC-E

43
kept in participants’ medical record. Recruit clients into program by providing
them with information sheet (Appendix X). Follow enrollment procedure and
issue program enrollment and attendance form (Appendix Y) and education
program reminder form provided (Appendix Z). For consenting patients (Consent
Form at Appendix AA), arrange for them two 2 hours education program in
classes ≤10 participants. Program contents should base on IPT and cover four
problem areas: role transition, grief, interpersonal dispute and interpersonal
sensitivity. Contents should also cover IPT skills, communication skills,
motherhood transition, PND management, baby gender and martial relationship
issues, establishment of social support, conflict resolution skills and Chinese
postnatal practices. Learning activities include ice-breaking games, lectures,
discussions, brainstorming, role play, communication analysis, demonstration and
return demonstration, clarifications and IPT handouts.
(iii) Administration of outcome measurement tools of EPDS, GHQ and
PSOC-E at postnatal 6 to 8 weeks and 3 to 6 months. Provide psychiatric services
referral of postnatal EPDS ≥13.
4.6 Level of Evidence and Grades of Recommendations

44
Systems of Levels of Evidence and Grades of Recommendations
designed by the Scottish Intercollegiate Guidelines Network (2008b) are shown in
Appendices CC and DD, respectively. Recommendations in the 8 selected studies
have been reviewed in accordance with above systems and results discussed in the
next Section.
4.6.1 Recommendations
A Identify HDR participants by nurse using EPDS ≥13 as a benchmark.
The Chinese version EPDS can be used to identify high depression
risk participant during antenatal (Gao, et al., 2010; Gao, et al., 2012; Leung
& Lam, 2012).
1++
A Recruitment at 20 to 32 gestation weeks by nurse during antenatal follow-up.
Program participants recruitment at 20 to 32 gestation weeks by
nurses during antenatal follow-up in MCHCs with written consent obtained
(Crockett, et al, 2008; Zlotnick, et al., 2001; Zlotnick, et al., 2006;
Gao, et al., 2010; Gao, et al., 2012; Grote, et al., 2009; Leung & Lam, 2012;
Spinelli & Endicott, 2003).
1+
1++
1++

45
A Arrange education program in two 2-hour sessions in groups ≤10 patients by
nurses using education program reminder form.
Two 2-hour sessions with an optimal class size of ≤ 10 patients will
minimize barrier to care and facilitate attendance (Gao, et al., 2010; Gao, et
al., 2012).
1++
A Trained nurse educators run IPT program with handout
Nurses with intensive IPT training for intervention deliver training
with learning activities such as games, role play, group discussions to
motivate engagement (Zlotnick, et al., 2006;
Gao, et al., 2010; Gao, et al., 2012; Leung & Lam, 2012) and provide
handout to facilitates home practices to develop IPT skills (Crockett, et al.,
2008; Gao, et al., 2012; Leung & Lam, 2012).
1+
1++
1+
1++

46
A Arrange measurement of EPDS, GHQ and PSOC-E at baseline, postnatal 6
to 8 weeks and 3 to 6 months.
It is optimal to evaluate depressive symptoms, psychological
well-being and maternal role status by the Chinese version of EPDS, GHQ
and PSOC-E at baseline, postnatal 6 to 8 weeks (Gao, et al., 2010;
Gao, et al., 2012; Leung & Lam, 2012) and postnatal 3 to 6 months (Gao, et
al., 2012; Grote, et al., 2009; Spinelli & Endicott, 2003;
Zlotnick, et al., 2001; Zlotnick, et al., 2006).
1++
1++
1++
1+
A Refer to psychiatric services as postnatal EPDS ≥13 at 6 to 8 weeks and 3 to
6 months.
Refer clients for psychiatric services if postnatal EPDS ≥13 subject to
their consent (Gao, et al., 2010; Gao, et al., 2012).
1++

47
Chapter 5
Implementation Plan
This Chapter illustrates Innovation program implementation plan with actual
timelines; stakeholders involved and communication strategies plan and pilot test
with evaluation plan.
5.1 Potential Users Communication Plan
In Hong Kong, Civil Services Bureau runs Staff Suggestion Scheme (SSS),
encouraging civil servants to make suggestions for improving services efficiency
(Civil Service Bureau Publications, 2012). Department of Health, Staff
Suggestion Committee considers suggestions for management improvement (Civil
Service Bureau Publications, 2013). Many proposals have successful adopted
through SSS, such as green management measures (Department of Health, Annual
Report 2009-2010).
Innovation Program aimed to provide quality antenatal education program
for HDR pregnant women and to boost nursing staff morale and team spirits,
implemented through SSS. Stakeholders include Departmental Staff Suggestion
Committee, administrative and management panels, IPT training course center,
nursing staffs, nurse educators, computer staffs and potential participants.

48
Implementation Timeframe Table and Communication Strategies Timeline Plan
showed in Appendix V and Appendix EE, respectively.
5.1.1 Communication with Departmental Staff Suggestions Committee
(DSSC)
Proposal will send to DSSC secretary for approval. If approved, pilot test
report, mid-term review and final report will submit as Program progresses.
5.1.2 Communication with Administrative and Management Panels
Administrative and management panels include: Director of Health, Principal
Nursing Officer and Senior Nursing Officers will notify Program SSS application.
Innovation Program provides good EBP by reducing PND management
caseloads with low cost-benefit ratio resulting save of $919,310.8 in PND
management cost with estimated 20% reduction in PND caseloads. Above figures
should ensure success in getting administrative approval.
Once approved, panels need to endorse Program guidelines, pilot test
location; 8 MCHCs sites, monitor manpower plan and services caseloads.
Pilot test report, mid-term review and final report will submit as program
progresses.

49
5.1.3 Formation and Responsibilities of Steering Committee
Steering Committee established and members include: author of the
Innovation Program (Chairman), a Senior Medical Officer (adviser), a Registered
Nurse, two computer staffs and two clerical staffs. Telephone lines provided for
members communication.
Chairman is responsible to finalize program guidelines, documents, class
timetables, briefing, staff training courses and ‘evaluator’ to report pilot test,
mid-term review (6 months) and final report (12 months) submission.
Registered Nurse responsible for: authorized approval of EPDS, GHQ and
PSOC-E questionnaires from respective questionnaires authors, resources
arrangement and collect participants’ opinions.
Computer staffs responsible for: ‘IPT Booking and Reporting’ network
system setting up, data analysis and reports preparation. Clerical staffs are
required to provide general administrative support. Committee will also oversee
staff training issues.
5.1.3.1 Monthly Committee Meetings
Steering Committee meet with 8 MCHCs in-charge nurses and 2 nurse

50
representatives monthly to prepare program guidelines and documents, booking
and data report system, resources, class schedules and activities.
5.1.3.2 Monthly Staff meetings
During implementation, Steering Committee has monthly staff meetings with
8 MCHCs in-charge nurses, educator representative and 2 nurse representatives to
discuss class schedules, resources, attendance, satisfaction, staff feedback and
review reports for program quality improvement.
5.1.4 Communication with IPT Training Centre
18 nursing staffs nominate for IPT training with fee arrangement with Hong
Kong College of Psychiatrist IPT Training Centre.
5.1.5 Communication with Clinical Nursing Colleagues
Departmental e-mail and Staff Newsletter will announce to all clinical staffs
for changes rendered necessary by current evidences, implementation plan and
recruitment of motivated staffs for training. Briefing sessions provide to 8
MCHCs staffs by Chairman. Final guidelines with logistic procedures and report
manual will provide to 31 MCHCs. Two nurse representatives will attend monthly
staff meetings. Upon request, oral presentations can provide to clinical staffs by

51
Chairman.
5.1.6 Communication with IPT Nurse Educators
Class schedules will send to nurse educators by department e-mails. Educator
representative attend staff meeting monthly. During pilot test, Educator provides
feedbacks evaluation by using 7-point scale (Appendix FF).
5.1.7 Communication with Computer Staffs
Computer staffs establish ‘IPT booking and reporting system’ and analysis
data: attendance, satisfactory rate, measurement of EPDS, GHQ, PSOC-S, PND
incidence and PND service demands. Chairman discuss with computer staffs for
preparing analysis reports. Help-desk phone service provides to 31 MCHCs.
5.1.8 Communication with Potential Participants
Steering Committee decides a survey in 2 MCHCs with convenient sampling
of 10 potential participants for their opinions in 10-point evaluation scale on
program’s information sheet (Appendix X), three questionnaires, handouts,
enrollment procedures and reminder form (Appendix Z), class schedules and
program activities. Program posters (Appendix GG) provide to 31 MCHCs and
department network. Participant satisfactory evaluation form in 7-point scales
52
provided (Appendix BB).
5.2 Innovation Program Evaluation Framework
Feasibility, propriety, acceptability and effectiveness of Program should be
evaluated. According to McKenzie & Smeltzer (2013), ‘Framework for Program
Evaluation’ with systems analysis approach, comprises six steps tailoring this
evaluation process: engaging stakeholders, describing program, focusing
evaluation design, gathering credible evidence, justifying conclusions and
ensuring use and sharing lessons learned (Appendix HH). Systems analysis of
economic evaluation determined for economic achievement.
McKenzie & Smeltzer (2013) suggests process evaluation, impact evaluation
and outcome evaluation to evaluate a program for quality improvement,
immediate changes and long term objectives achievements. These three
evaluations will be used during implementation.
5.3 Pilot Test
5.3.1 Pilot Test Purposes
To enact new changes and transform EBP, pilot testing with a small sampling
size should plan and its results reviewed for clinical applicability and feasibility

53
for successful widespread implementation (Melnyk & Fineont-Overholt, 2011).
As process evaluation aims to control and improve program quality (McKenzie &
Smeltzer, 2013), pilot test will accord first priority to evaluate on acceptability,
feasibility, logistic and identify possible problems before full implementation.
5.3.2. Pilot Test Staff Briefing
Guidelines provide to all clinical staffs by department email. Briefing session
by Chairman to pilot test MCHCs staffs on program logistics and reporting
procedures.
5.3.3 Pilot Test Implementation
A two group pretest-posttest control group with time series designed of pilot
program will conduct in one MCHC. As 40 attendants monthly planned, recruit 40
HDR participants screened at gestation 30 to 32 weeks by EPDS ≥13, enroll
willing ones in ‘program group’ and refusal ones in ‘routine group’.
Exclusion Criteria: current mental illnesses, obstetric complications and
English participants. Both groups have three-point measurements: baseline
assessment, postnatal 6-8 weeks and 12 to 16 weeks. Pilot test report plan and
implementation timeframe illustrated in Appendix II.

54
5.3.4 Pilot Test Evaluation
Pilot analysis shall use Statistical Package for Social Sciences (SPSS)
Version 21 operating on Window 7 computer. ‘Two-sample t-test’ examines
differences between three-point measurement results of EPDS, GHQ and PSOC-E
between groups. ‘Paired t-test’ examines differences between pretest and posttest
scores of EPDS, GHQ and PSOC-E of each group. ‘Analysis of variance’ used for
7-point scales of satisfaction rate and nurse educator feedback rate. Rehearsal
class checks for time management. ‘Chi-square’ analysis between groups cover
attendance rate and percentage; PND incident rate and percentage; PND
management service caseloads and percentage. Staff feedback will discuss during
monthly staff meetings.
5.4 New EBP Guideline Implementation
Evaluates EBP outcomes can reflect change impacts to best clinical practice
(Melnyk & Fineout-Overholt, 2011). Pilot test provides preliminary evidence
changes to tackle difficulties, suggestions and guidelines refinement for full
implementation in 31 MCHCs. Debriefing for enhancement with final guideline
manual provided.
Innovation Program will fully implement in 8 MCHCs by 18 nurse educators

55
providing 4 classes monthly. With Inclusive Criteria, screen for HDR participants
at 20 to 32 gestation weeks, enroll willing ones in ‘program group’ and refusal
ones in ‘routine group’. Three-point measurements (EPDS, GHQ and PSOC-E),
satisfactory rates, PND incidence and management caseloads will report through
computer network by nurses. Educator and staffs feedback discuss in staff
meeting.

56
Chapter 6
Evaluation Plan
This Chapter illustrates plan goals evaluation, outcome measurements, target
client natures and numbers, data collection and analysis instruments with effective
criteria.
According to Mckenzie & Smeltzer (2013), impact evaluation focus on
intermediate outcomes measurement of awareness, knowledge, attitudes, skills
and behaviors; outcome evaluation focus on program goals and population’s
morbidity or mortality; economic evaluation focus on cost-benefit and
cost-effectiveness.
Under ‘Framework for Program Evaluation’ with systems analysis approach
(Appendix HH), impact evaluation conduct for mid-term review in 6 months,
outcome evaluation and economic evaluation conduct final review in 12 months
to gather empirical program's ultimate evidences in reducing PND and promote
higher level of maternal role competence and psychological well-being.
6.1 Intervention Outcome Identification
6.1.1 Patient Outcomes

57
Participants outcomes include: EPDS measuring mental health outcome;
GHQ measuring psychological well-being; and PSOC-E measuring maternal role
competence level and PND incidence evaluate program effectiveness.
(a) Comparing EPDS at baseline, postnatal 6 to 8 weeks and postnatal 3 to 6
months of program group with routine group and review literatures’
effect size of EPDS.
(b) Comparing GHQ at baseline, postnatal 6 to 8 weeks and postnatal 3 to 6
months of program group with routine group and review literatures’
effect size of GHQ.
(c) Comparing PSOC-E at baseline, postnatal 6 to 8 weeks and postnatal 3 to
6 months of program group with routine group and review literatures’
effect size of PSOC-E.
(d) Comparing PND incidence percentage of program group with routine
group and department PND 2011 incidence.
6.1.2 System Outcomes
System outcomes: PND management caseloads; attendance and satisfactory
rates for evaluating program acceptance.

58
(a) Comparing PND management caseloads percentage of program group
with routine group and department PND 2011 management caseloads.
(b) Attendance rates of program group and routine group.
(c) Satisfactory rates of program group and routine group.
6.1.3 Healthcare Provider Outcomes
Educator and staff feedbacks can improve program feasibility.
6.2 Nature of Target Participants Involved
Annually, there are estimate 3,428 to 3,883 HDR participants screened by
EPDS. Program provides 3,840 enrolments. Participants screened between 20 to
32 gestation weeks by EPDS ≥13. Eligible Criteria based on review studies and
non-eligible criteria included current mental illness, obstetric complications and
English participants.
6.3 Determining Number of Involved Target Clients
Computer software ‘Java Applets’ used for power and sample size
calculation. ‘Two-sample t-test’ evaluates efficiency of program primary outcomes.
Minimal sample size of 142 participants is required to obtain power of 80% (ß =
0.2) and 95% confidence interval for ultimate effect size of 0.89 reduction in

59
EPDS, 0.77 reduction in GHQ and 2.43 increase in PSOC-E.
6.3.1 Design
A quasi-experimental non-equivalent pretest-posttest control group with time
series program designed. Participants recruit at 20 to 32 gestation weeks by EPDS
≥13, enroll willing ones in ‘program group’ and refusal ones in ‘routine group’
receive routine education. Three-point measurements of EPDS, GHQ and
PSOC-E at baseline, postnatal 6 to 8 weeks and 3 to 6 months of both groups
reported through network system. PND incidence rates and PND management
caseloads obtained through computer system.
6.3.2 Primary Outcomes
EPDS, GHQ and PSOC-E data collected from program group and routine
group analyzed by ‘two-sample t-test’ and compared with reviewed studies’ effect
sizes.
6.3.3 Secondary Outcomes
Compare PND incidence percentages and PND management caseloads
percentages in both groups analysis by ‘Chi-square test’ and Department of Health,
PND 2011 data.

60
6.3.4 Analysis Methods
‘Two-sample t-test’ with 95% confidence of statistical analysis determines
differences of EPDS, GHQ and PSOC-E from three-point measurements between
two groups and compare with reviewed literatures. ‘Paired t-test’ analysis changes
in both groups. ‘Chi-square’ tests analysis differences of PND incidence and PND
management caseloads between two groups then compare with Department of
Health PND 2011 data. Data analysis perform by computer staffs and Chairman.
6.4 Data Collection and Instruments
Three-point measurements of EPDS, GHQ and PSOC-E from baseline,
postnatal 6 to 8 weeks and 3 to 6 months conducted in both groups. All EPDS,
GHQ, PSOC-E, PND incidence and services demands reported through network
by nurses. Outcome measurements rundown is illustrated in Appendix JJ.
Attendance and program satisfactory rate report through network by nurse
educators. Staff feedbacks discuss during monthly staff meetings.
6.5 Data Analyses
Statistical Package for Social Sciences (SPSS) Version 21.0 operating on
Window 7 computer system used to analysis data by Chairman and computer

61
staffs. Statistical significance level for all inferential statistics will set at p-value
less than 0.05 (Polit & Beck, 2012).
6.5.1 Descriptive Statistics
Descriptive statistics include gestation ages and attendance percentages.
6.5.2 Inferential Statistics
‘Two-sample t-test’ compares significant differences of EPDS, GHQ and
PSOC-E between both groups then compared with reviewed studies' effect sizes
that show effects of PND, psychological well-being and maternal role.
‘Chi-square test’ compares proportion difference of PND incidences and PND
management caseloads in percentage of both groups then compare with
Department of Health PND 2011 data. Program satisfactory rates in a 7-point
scale evaluate by ‘analysis of variance’.
6.6 Effectiveness Criteria
6.6.1 Primary Outcomes
6.6.1.1 EPDS Score
Reviewed literatures advocate a significant reduction in EPDS (-0.89 to
-3.76, p =.000) as a meaningful indication. Minimum reduction of 0.89

62
EPDS in program group is indicative of primary outcome attained.
6.6.1.2 GHQ Score
Reviewed literatures advocates a significant reduction in GHQ (-3.3 to
-0.77, p<.01) as a meaningful indication. Minimum reduction of 0.77 GHQ
in program group is indicative of primary outcome attained.
6.6.1.3 PSOC-E Score
Reviewed literatures suggest a significant increase of 2.43 in PSOC-E
as a good indicator. An increase of 2.43 in PSOC-E of program group is
indicative of primary outcome attained.
6.6.2 Secondary Outcomes
6.6.2.1 PND Incidence Rates and PND Management Caseloads
Program implementation benefits are estimated to be 20% reduction in
both PND incidence and PND management costs. Such a reduction is
indicative that outcome has attained.
6.6.3 Economic Evaluations
6.6.3.1 Cost-Benefit Analysis

63
Cost-benefit analysis used to quantify health services’ costs and benefits in
monetary term and for comparison purposes (Polit & Beck, 2012). Program can
save $919, 310.8 in PND management costs with 20% PND reduction (Appendix
U), thus lightening financial burdens and reducing management services demand.
Benefit-cost ratio per program participant is $1,183/$140 or 8.45. Every $1 spent
on Program helps save $8.45. Benefits from this feasible Program outweigh costs,
rendering it a sound investment.
6.6.3.2 Cost-Effective Analysis
Cost-effective analysis compares intervention costs in monetary terms and
health outcomes in natural terms (Polit & Beck, 2012). Innovation Program costs
$802,282. Screened program participants obtained postnatal measurements are
able to gain healthy family living and enjoy motherhood role. Program can reduce
20 % PND caseloads (approximately 777 out of 3,883 estimated annual PND
incidences), and ease manpower allocation.
Innovation Program provides training opportunities facilitate pioneer role in
nursing professional development and facilitate EBP leadership role of
Department of Health in public health.

64
6.7 Conclusion
Under 'Framework of Evaluation' with a systems approach, feasibility and
ultimate effectiveness of Innovation Program has confirmed.

65
Chapter 7
Conclusions
PND is a public health issue result from high suspected PND incidence rates
and PND management caseloads. Antenatal intervention can prevent PND as early
identification of HDR pregnant women and provide evidence-based interventions
can reduce PND incidences (Clatworthy, 2012). After critical review of eight RCT
studies on EBP, an antenatal IPT program introduces to provide psychosocial
intervention to clinical practice subjects to approval from management.
Department of Health mission to provide client-focus good quality services and
MCHCs can act as platforms to provide evidence-based antenatal IPT program for
HDR pregnancy women to prevent PND and to promote their well-being and
maternal role competence.
With outcome evaluation achievement, antenatal IPT program is feasible,
transferable, and cost-benefit effective to provide an ‘all-win situation’ to clients,
nurses and Department of Health, facilitated joyful motherhood with happy
families in Hong Kong.

66
References
Almond, P. (2009). Postnatal depression: a global public health perspective.
Perspectives in Public Health, 129(5), 221-227.
Appleby, L., Mortensen, P. B. & Faragher, E. B. (1998). Suicide and other causes
of mortality after postpartum psychiatric admission. British Journal of
Psychiatry, 173, 209-211.
Austin, M. P., Frilingos, M., Lumley, J., Hadzi-Pavlovic, D., Roncolato, W.,
Acland, S., Saint, K., Segal, N. & Parker, G. (2008). Brief antenatal
cognitive behavior therapy group intervention for the prevention of
postnatal depression and anxiety: a randomized controlled trial. Journal of
Affective Disorder, 105, 35- 44.
Barkham, M. & Hardy, G. E. (2001). Counseling and interpersonal therapies for
depression: towards securing and evidence base. British Medical Bulletin,
57(1), 115-132.
Barr, J., & Beck, C. (2008). Infanticide secrets: qualitative study on postpartum
depression. Canadian Family Physician, 54, 1716-1723.
Beck, A. T. & Beck, R. W. (1972). Screening depressed patients in family practice:
a rapid technic. Postgraduate Medicine, 52, 81-85.
Beck, C. T. & Gable, R. K. (2001). Comparative analysis of the performance of
the postpartum depression screening scale with two other depression

67
instruments. Nursing Research, 50(4), 242-250.
Benette, H. A., Einarson, A., Taddio, A., Koren, G. & Einarson, T.R. (2004).
Prevalence of depression during pregnancy: systematic review. Obstetrics
Gynecology, 103, 698-709.
Boyce, P., Stubbs, J. & Todd, A. (1993). The Edinburgh postnatal depression scale:
validation for an Australian sample. Australian & New Zealand Journal of
Psychiatry, 27(3), 472-476.
Bowlby, J. (1969). Attachment. New York: Basic Books.
Brugha, T., Wheatley, S., Taub, N., Culverwell, A., Friedman, T., Kirwan, P.,
Jones, D.R. & Shapiro, D. A. (2000). Pragmatic randomized trial of
antenatal intervention to prevent post-natal depression by reducing
psychosocial risk factors. Psychological Medicine, 30, 1273-1281.
Buist, A., Westley, D. & Hill, C. (1999). Antenatal prevention of postnatal
depression. Archives of Women’s Mental Health, 1, 167-173.
Burgess, A. W. (1997). Psychiatric Nursing Promoting Mental Health, Appleton
& Lange.
Cheng, R. C., Lai, S. S. & Siu, H. F. (1994). A study exploring the risk of
postnatal depression and the help seeking behavior of postnatal women in
Hong Kong. Hong Kong Nursing Journal, 68, 12-17.

68
Civil Service Bureau Publication, Hong Kong Fact Sheets – Civil Service. (2012).
Retrieved on March, 14, 2013 from
http://www.gov.hk/en/about/abouthk/factsheets/docs/civil_service.pdf
Civil Service Bureau Publication, Guide on Staff Relation. (2013). Retrieved on
March, 14, 2013 from
http://www.csb.gov.hk/english/publication/files/sr_guide_e.pdf
Clatworthy, J. (2012). The effectiveness of antenatal interventions to prevent
postnatal depression in high risk women. Journal of Affective Disorder,
137, 25-34.
Cornish, A. M., McMahon, C., & Ungerer, J. A. (2008). Postnatal depression and
the quality of mother-infant interactions during the second year of life.
Australian Journal of Psychology, 60(3), 142-151.
Cox, J. L. (1992). Depression after childbirth. In Paykel, E. S. (Eds.), Handbook
of Affective Disorders (pp. 569-583). New York, US: Guilford Press.
Cox, J. L., Holden, J.M. & Sagovsky, R. (1987). Detection of postnatal depression:
development of the 10-item Edinburgh postnatal scale. British Journal of
Psychiatry, 150, 782-786.
Cox J. & Holden J. (2003). Perinatal Mental Health: A Guide to the Edinburgh
Postnatal Depression Scale. The Royal College of Psychiatrists.

69
Craig, M. & Howard, L. (2009). Postnatal depression. Clinical Evidence, 1, 1407.
PMC2907780. Retrieved August 2, 2012, from
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2907780/
Crockett, K., Zlotnick, C., Davis, M., Payne, N. & Washington, R. (2008). A
depression preventive intervention for rural low-income African-American
pregnant women at risk for postpartum depression. Archives of Women’s
Mental Health, 11, 319-325.
Department of Health, Annual Report (2009-2010). Retrieved on June, 5, 2013
from http://www.dh.gov.hk/english/pub_rec/pub_rec.html
Department of Health, Comprehensive Child Development Service Evaluation
Report (2007). Retrieved December 25, 2012, from
http://www.fhs.gov.hk/english/archive/files/reports/ccds_full.pdf
Department of Health, Family Health Services (2012). Mission, Vision and Values.
Retrieved December 25, 2012, from
http://www.fhs.gov.hk/english/about_us/vision/vision.html
Department of Health, Postnatal Depression Report (2011). Disclose approved
letter in Appendix L.
Eastwood, J. G., Phung, H. & Barnett, B. (2011). Postnatal depression and
socio-demographic risk: factors associated with Edinburgh Depression

70
Scale scores in a metropolitan area of New South Wales, Australia. The
Australian and New Zealand Journal Of Psychiatry, 45 (12), 1040- 1046.
Elkin, I., Shea, M. T., Watkins, J. T., Imber, S.D., Sotsky, S.M., Collins, J.F., Glass,
D.R., Pilkonis, P.A., Leber, W. R. & Docherty, J.P. (1989). NIMH
treatment of depression collaborative Research Program: general
effectiveness of treatment. Archives of General Psychiatry, 46, 971-982.
Elgar, F., Curtis, L., McGrath, P., Waschbusch, D., & Stewart, S. (2003).
Antecedent-consequence conditions in maternal mood and child
adjustment: a four year cross-lagged study. Journal of Clinical Child and
Adolescent Psychiatry, 32(3), 362-374.
Elliott, S. A., Leverton, T. J., Sanjack, M., Turner, H., Cowmeadow, P., Hopkins, J.
& Bushnell, D. (2000). Promoting mental health after childbirth: a
controlled trial of primary prevention of postnatal depression. British
Journal of Clinical Psychology, 39, 223-241.
Evans, F. B. III (1996). Sullivan H. S.: Interpersonal Theory and Psychotherapy.
Routledge, London & New York.
Faisal-Cury, A. & Menezes, P.R. (2012). Antenatal depression strongly predicts
postnatal depression in primary health care. Revista Brasileira de
Priquiatria, 34, 446-450.

71
Gao, L.L., Chan, W. C. Sally, Li, X., Chen, S. & Hao, Y.(2010). Evaluation of an
interpersonal psychotherapy oriented childbirth education program for
Chinese first time childbearing women, a randomized controlled trial.
International Journal of Nursing Studies, 47, 1208-1216.
Gao, L. L., Chan, W.C. Sally & Sun, K. (2012). Effects of an interpersonal
psychotherapy oriented childbirth education program for Chinese first time
childbearing women at 3 month follow up, a randomized controlled trial.
International Journal of Nursing Studies, 49, 274-281.
Gao, L. L., Chan, W. C. Sally & Mao, Q. (2009). Depression, perceived stress &
social support among first time Chinese mothers and fathers in the
postnatal period. Research in Nursing & Health, 32(1), 50-58.
Gibaud-Wallston, J. & Wandersman, L. P. (1978). Development and Utility of the
Parenting Sense of Competence Scale. In: Paper presented at the Meeting
of the American Psychological Association, Toronto, Canada.
Goodman, J. H. (2008). Influences of maternal postpartum depression on fathers
& on father-infant interaction. Infant Mental Health Journal, 29 (6),
624-643.
Grote, N. K., Bledsoe, S. E., Swartz, H. A. & Frank, E. (2004). Feasibility of
providing culturally relevant, brief interpersonal psychotherapy for

72
antenatal depression in an obstetrics clinic: a pilot study. Research on
Social Work Practice, 14(6), 397-407.
Grote, N. K., Swartz, H. A., Geibel, S.L., Zuckoff, A., Houch, P. R. & Frank, E.
(2009). A randomized controlled trial of culturally relevant, brief
interpersonal psychotherapy for perinatal depression. Psychiatric Services,
60, 313-321.
Grote, N. K., Bridge, J. A., Gavin, A., Melville, J. L. & Lyengars, K., (2011). A
meta-analysis of depression. During pregnancy & the risk of preterm birth,
low birth weight & intrauterine growth retardation. Archives of General
Psychiatry, 67(10), 1012-1024.
Guo, S. F. (1993). Postpartum depression. Chinese Journal of Obstetrics and
Gynaecology, (Zhonghua Fu Chan Ke Za Zhi ), 28(9), 532-533, 569.
Hay, D. F., Pawlby, S., Sharp, D., Asten, P., Mills, A. & Kumar, R. (2001).
Intellectual problems shown by 11 year old children whose mothers had
postnatal depression. Journal of Child Psychology and Psychiatry & Allied
Disciplines, 42(7), 871-889.
Hayes, B. A., Muller, R. & Bradley, B.S. (2001). Perinatal depression, a
randomized controlled trial of an antenatal education intervention for
primiparas. Birth, 28(1), 28-35.

73
Halbreich, U. & Karkun, S. (2006). Cross-cultural and social diversity of
prevalence of postpartum depression and depressive symptoms. Journal of
Affective Disorders, 91 (2-3), 97-111.
Harris, B., Huckle, P., Thomas, R., Johns, S. & Fung, H. (1989). The use of rating
scales to identify postnatal depression. British Journal of Psychiatry, 154,
813-817.
Hewitt, C., Gilbody, S., Brealey, S., Paulden, M., Palmer, S., Mann, R., Green, J.,
Morrell, J., Barkham, M., Light, K. & Richards, D. (2009). Methods to
identify PND in primary care: an integrated evidence synthesis and value
of information analysis. Health Technology Assessment, 13 (6),
doi:10.3310/hta13360. Retrieved on September 20, 2012, from
http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0015009/pdf/
Ho, I. & Holroyd, E. (2002). Chinese women’s perceptions of the effectiveness of
antenatal education in the preparation for motherhood. Journal of
Advanced Nursing, 38(1), 74-85.
Hong Kong College of Psychiatrist. Interpersonal Psychotherapy Program
Course in 2011. Retrieved December 28, 2012 from
http://www.hkcpsych.org.hk/index.php?option=com_docman&task=doc_vi
ew&gid=683&Itemid=91&lang=en

74
International Society for Interpersonal psychotherapy (IsIPT). Retrieved August
12, 2012, from http://interpersonalpsychotherapy.org/about-ipt/
Judd, F., Weissman, M. & Davis, J. (2004). Interpersonal counseling in general
practice. Australian Family Physician, 33(4), 332-337.
Kiesler, D. J. (1979). An interpersonal communication analysis of relationship in
psychotherapy. Psychiatry, 42(4), 299-311.
Kim, D.R., O’reardon, J.P. & Epperson, C. N. (2010). Guidelines for the
management of depression during pregnancy. Current Psychiatry Reports,
12, 279-281.
Kitamura, T., Yoshida, K., Okano, T., Kinoshita, K., Hayashi, M., Toyoda, N., Ito,
M., Kudo, N., Tada, K., Kanazawa, K., Sakumoto, K., Satoh, S., Furukawa,
T. & Nakano, H. (2006). Multicentre prospective study of perinatal
depression in Japan: incidence and correlates of antenatal and postnatal
depression. Archives of Women’s Mental Health, 9, 121-130.
Klerman, G. L., Weissman, M. M., Rounsaville, B. H. & Chevron, E. S. (1984).
Interpersonal Psychotherapy of Depression. Basic Book Inc., New York.
Koszycki, D., Bisserbe, J. C., Blier, P., Bradwejn, J. & Markowitz, J. (2010).
Interpersonal psychotherapy vs brief supportive therapy for depressive
infertile women: first pilot randomized control trial. Archives of Women’s

75
Mental Health, 15, 193-201.
Lau, Y. (2005). Establishing an interpersonal group program for Chinese women
with postnatal depression in Hong Kong. Hong Kong Nursing Journal,
41(2), 7-17.
Lee, A.M., Lam, S.K., Lau, M.S.M, Chong, C.S.Y., Chui, H.W. & Fong, D.Y.T.
(2007). Prevalence, course, and risk factors for antenatal anxiety and
depression. Obstetrics and Gynaecology, 110, 5, 1102-1112.
Lee, D. T.S., Yip, S. K., Chiu, H. F. K., Leung, T. Y. S., Chan, K. P. M., Chau, I. O.
L., Leung, H. C. M. & Chung, T. K. H. (1998). Detecting postnatal
depression in Chinese women. British Journal of Psychiatry, 192,
433-437.
Lee, D.T.S. & Chung, T.K.H. (1999). What should be done about postnatal
depression in Hong Kong? Hong Kong Medical Journal, 5(1), 39-42.
Lee, D. T. S., Yip, A. S. K., Leung, T. Y. S. & Chung, T. K. H. (2000). Identify
women at risk of postnatal depression. Hong Kong Medical Journal, 6(4),
349-354.
Lee, D. T., Yip, A. S., Chiu, H. F. & Chung, T. K. (2000a). Screening for postnatal
depression using the double-test strategy. Psychosomatic Medicine, 62(2),
258-263.

76
Lee, D. T. S., Yip, A. S. K., Chiu, H. F. K., Leung, T. Y. S. & Chung, T. K. H.
(2001a). Screening for postnatal depression: are specific instruments
mandatory? Journal of Affective disorder, 63, 233-238.
Lee, D. T. S., Yip, A. S. K., Chiu, H. F, K., Leung, T. & Chung, T. (2001b). A
psychiatric epidemiological study of postnatal Chinese women. American
Journal of Psychiatry, 158, 220-226.
Lee, D. T. S., Chan, S. S. M., Sahota, D. S., Yip, A. S. K., Tsui, M. & Chung, T. K.
H. (2004). A prevalence study of antenatal depression among Chinese
women. Journal of Affective Disorder, 82, 93-99.
Legislative Council Panel Paper on CCDS (2012).
Retrieved on May 15, 2013 from
http://www.legco.gov.hk/yr11-12/english/panels/ws/papers/ws0213cb2-25
93-1-e.pdf
Lenth, R. V. (2006-9). Java Applets for Power and Sample Size [Computer
software]. Retrieved on May 15, 2013, from
http://www.stat.uiowa.edu/~rlenth/Power.
Leung, S. S. K., Martinson, I. M. & Arthur, D. (2005). Postpartum depression and
related psychosocial variables in Hong Kong Chinese women: finding

77
from a prospective study. Research in Nursing & Health, 28, 27-38.
Leung, S. S. L., Leung, C., Lam, T. H., Hung, S. F., Chan, R., Yeung, T., Miao,M.,
Cheng, S., Leung, S.H., Lau, A. & Lee, D.T. (2010). Outcome of a
postnatal depression screening programme using the Edinburgh Postnatal
Depression Scale: a randomized controlled trial. Journal of Public Health,
33(2), 292-301.
Leung, S. S. K. & Lam, T. H. (2012). Group antenatal intervention to reduce
perinatal stress and depressive symptoms related to intergenerational
conflicts: a randomized controlled trial. International Journal of Nursing
Studies, 49 (11), 1391-1402.
Legislative Council Panel (2008). Welfare Services Progress report on the
implementation of comprehensive Child Development Service. Retrieved
August 2, 2012, from
http://www.legco.gov.hk/yr07-08/english/panels/ws/papers/ws0214cb2-97
7-6-e.pdf
Lindahl, V., Pearson, J. L. & Colpe, L. (2005). Prevalence of suicidality during
pregnancy and the postpartum. Archives of Women’s Mental Health, 8,
77-87.
Markowitz, J. C., Kocsis, J. H., Fishman, B., Spielman, L. A., Jocobsberg, L. B.,

78
Frances, A. J., Klerman, G. L. & Perry, S. W. (1998). Treatment of
HIV-positive patients with depressive symptoms. Archives of General
Psychiatry, 55, 452-457.
McKenzie, J. F. & Smeltzer, J. L. (2013). Planning, implementing and evaluating
health promotion programs, a primer. 3rd
ed. Pearson Education Company.
Meyer, A. (1958). Psychobiology. A Science of Man. Springfield, Illinois: Charles
C Thomas.
Miller, L., Gur, M., Shanok, A. & Weissman, M. (2008). Interpersonal
psychotherapy with pregnancy adolescents: two pilot studies. Journal of
Child Psychology and Psychiatry, 49 (7), 733-742.
Mufson, L., Weissman, M. M., Moreau, D. & Garfinkel, R. (1999). Efficacy of
interpersonal psychotherapy for depressed adolescents. Archives of
General Psyhciatry, 56, 573-579.
Mulcahy, R., Reay, R. E., Wilkinson, R. B. & Owen, C. (2010). A randomized
control trial for the effectiveness of group interpersonal psychotherapy for
postnatal depression. Archives of Women’s Mental Health, 13, 125-139.
Melnyk, B.M. & Fineout-Overholt, E. (2011). Evidence-based Practice in
Nursing and Healthcare, a guide to best practice. 2d. ed. Lippincott
Williams & Wilkins.

79
Najman, J. M., Andersen, M. J., Bor, W., O’Callaghan, M. J. & Williams, G. M.
(2000). Postnatal depression-myth and reality: Maternal depression before
and after the birth of a child. Social Psychiatry Epidemiology, 35 (1),
19-27.
Ngai, F. W., Chan, S. & Holroyd, H. (2007). Translation and validation of a
Chinese version of the Parenting Sense of Competence Scale in Chinese
mothers. Nursing Research, 56, 348-354.
Ngai, F. W., Chan, S. W. C. & Ip, W. Y. (2009). The effects of a childbirth
psycho-education program on learned resourceful, maternal role
competence and perinatal depression: a quasi-experiment. International
Journal of Nursing Studies, 46, 1298-1306.
Ngai, F. W. & Chan, S. W. C. (2011). Psychosocial factors and maternal wellbeing:
an exploratory path analysis. International Journal of Nursing Studies, 48,
725-731.
National Institute for Health & Care Excellence (NICE) clinical guideline 45
(2007). Antenatal & postnatal mental health, clinical management &
service guidance. The National Collaborating Centre for Mental Health.
Retrieved June10, 2012, from
http://guidance.nice.org.uk/CG45/NICEGuidance/pdf/English

80
Nott, P. N. & Cutts, S. (1982). Validation of the 30-item General Health
Questionnaire in postpartum women. Psychological Medicine, 12,
409-413.
O’Hara, M. W., Stuart, S., Gorman, L. L. & Wenzel, A. (2000). Efficacy of
interpersonal psychotherapy for postpartum depression. Archives of
General Psychiatry, 57, 1039-1045.
O’Hara, M. W. (1995). Introduction. In M. W. O’Hara (Ed.), Postpartum
Depression: Causes and Consequences. New York: Springer-Verlag.
Pawlby, S., Sharp, D., Hay, D. & Keane, V. O. (2008). Postnatal depression and
child outcome at 11 years: The importance of accurate diagnosis. Journal
of Affective Disorders, 107, 241-245.
Polit, D. F., & Beck, C. T. (2008). Nursing Research: principles and methods (7th
edition. ed.). Lippincott. Williams & Wilikins: Philadelphia.
Polit, D. F. & Beck, C. T. (2012). Nursing Research, generating and assessing
evidence for nursing practice. 9th
ed. Lipincott Williams & Wilkins.
Reay, R., Fisher, M., Robertson, M., Adams, E. & Owen, C. (2006). Group
interpersonal psychotherapy for postnatal depression: a pilot study.
Archives of Women’s Mental Health, 9, 31-39.
Robertson, E., Celasun, N. & Stewart, D.E. (2003). Risk factors for postpartum

81
depression. In Stewart, D.E., Robertson, E., Dennis C. L., Grace, S. L. &
Wallington, T., (2003). Postpartum Depression: Literature review of risk
factors and intervention on postpartum depression. World Health
Organization.
Sayer, C., Kohn, C., Fresco, D., Bellack, A., & Sarwer, D. (2001). Marital
cognitions and depression in the context of marital discord. Cognitive
Therapy and Research, 25(6), 713-732.
Salary Scale of Common Posts (2012). Salary scale of registered nurse and
medical officer. Retrieved December 25, 2012 from
http://www.swd.gov.hk/doc/ngo/Salary%20Scale%20of%20Common%20P
osts%20w%20e%20f%2001%2004%202012.pdf
Schaper, A. M., Rooney, B. L., Kay, N. R. & Silva, P. D. (1994). Use of the EPDS to
identify postpartum depression in a clinical setting. Journal of Reproductive
Medicine, 39 (8), 620-624.
Schulberg, H. C., Block, M. R., Madonia, M. J., Scott, C.P., Rodriguez, E., Imber,
S.D., Perel, J., Lave, J., Houck, P.R. & Coulehan, J. L. (1996). Treating major
depression in primary care practice. Archives of General Psychiatry, 53,
913-919.
Scottish Intercollegiate Guidelines Network (SIGN) (2002). Postnatal depression

82
and puerperal psychosis (SIGN Publication No. 60). Edinburgh. Retrieved
August 2, 2012, from http://www.sign.ac.uk/pdf/sign60.pdf
Scottish Intercollegiate Guidelines Network (SIGN)(2008a). Critical appraisal of
notes and methodology checklist. Retrieved June 10, 2012, from
http://www.sign.ac.uk/methodology/checklists.html
Scottish Intercollegiate Guideline Network (SIGN)(2008b). Key to evidence
statements and grades of recommendations. Retrieved December 25, 2012,
from http://www.sign.ac.uk/guidelines/fulltext/57/evidence.html
Service costs of Hospital Authority. Legislative Council Question 9 of Press
Releases on June 13, 2012. Retrieved on December 21, 2012 from
http://www.info.gov.hk/gia/general/201206/13/P201206130289.htm
Solan, G., Hobson, J. Leighton, J, Mcfarlane, B. & Law, R. (2009). An overview
and history of interpersonal psychotherapy. Nursing Standard, 23(26),
44-49.
Siu, B. W. M., Leung, S. S. L., Ip, P., Hung, S. F. & O’Hara, M. W. (2012).
Antenatal risk factors for postnatal depression: a prospective study of
Chinese women at maternal and child health centers. BioMed Central
Psychiatry, 12, 22. Doi:10.1186/1471-244x-12-22. Retrieved on December,
21, 2012 from http://www.biomedcentral.com/1471-244X/12/22

83
Spinelli, M.G. (1997). Interpersonal psychotherapy for depressed antepartum
women, a pilot study. The American Journal of Psychiatry, 154,
1028-1030.
Spinelli, M. G. & Endicott, J. (2003). Controlled clinical trial of interpersonal
psychotherapy versus parenting education program for depressed pregnant
women. American Journal Psychiatry, 160, 555-562.
Stamp, G. E., Williams, A. S. & Crowther, C. A. (1995). Evaluation of antenatal
and postnatal support to overcome postnatal depression: a randomized,
controlled trial. Birth, 22, 138-143.
Stuart, S. & Franzcp, M. R. (2003). Interpersonal Psychotherapy, a clinician
guide. Arnold, London.
Stuart, S. & O’Hara, M. W. (1995). Interpersonal psychotherapy for postpartum
depression, a treatment program. The Journal of Psychotherapy Practice
and Research, 4, 18-29.
Sullivan, H. S. (1953). The Interpersonal Theory of Psychiatry. WW Norton, New
York.
Surkan, P. J., Kennedy, C. E., Hurley, K. M. & Black, M. M. (2011). Maternal
depression and early childhood growth in developing countries: systematic
review and meta-analysis. Bulletin of the World Health Organization, 287,

84
607-615D. doi:10.2471/BLT.11.088187. Retrieved August 13, 2012, from
http://www.scielosp.org/scielo.php?pid=S0042-96862011000800013&scri
pt=sci_arttext
Tillett, R. (1999). Using psychotherapy effectively: choosing an appropriate
treatment. Advances in Psychiatric Treatment, 5, 420-426.
Weinberg, M. K. & Tronick, E. Z. (1998). The impact of maternal psychiatric
illness on infant development. Journal of Clinical Psychiatry, 59(S2),
53-61.
Weerasekera, P. (2010). Psychotherapy update for the practicing psychiatrist:
promoting evidence based practice. Clinical Synthesis, Focus, 8, 3-18.
Retrieved September 3, 2012, from
http://focus.psychiatryonline.org/journal.aspx?journalid=21
Whiffen, V. E. (1988). Screening for postpartum depression: a methodological
note. Journal of Clinical Psychology, 44, 367-371.
Vaeth, P. A., Ramisetty-Mikler, S., & Caetano, R. (2010). Depression among
couples in the United States in the context of intimate partner violence.
Journal of Interpersonal Violence, 25(5), 771-790.
Vigod, S. N., Villegas, L., Dennis, C-L & Ross, L. E. (2010). Prevalence and risk
factors for postpartum depression among women with preterm and

85
low-birth-weight infants: a systematic review. BJOG: An International
Journal of Obstetric & Gynecology, 117, 540-550.
Zajicek-Farber, M. (2010). The contributions of parenting and postnatal
depression on emergent language of children in low income families.
Journal of Child & Family Studies, 19, 257-269.
Zlotnick, C., Miller, I. W., Pearlstein, T., Howard, M. & Sweeney, P. (2006). A
preventive intervention for pregnancy women on public assistance at risk
for postpartum depression. American Journal of psychiatry, 163,
1443-1445.
Zlotnick, C., Johnson, S. L., Miller, I. W., Pearlstein, T. & Howard, M. (2001).
Postpartum depression in women receiving public assistance, a pilot study
of an interpersonal therapy oriented group intervention. American Journal
of Psychiatry, 158, 638-640.
唐子俊, 唐慧芳, 黃詩殷, 戴谷霖 (2003). 憂鬰症最新療法, 人際心理治療的
理論與實務. 心理出版社.
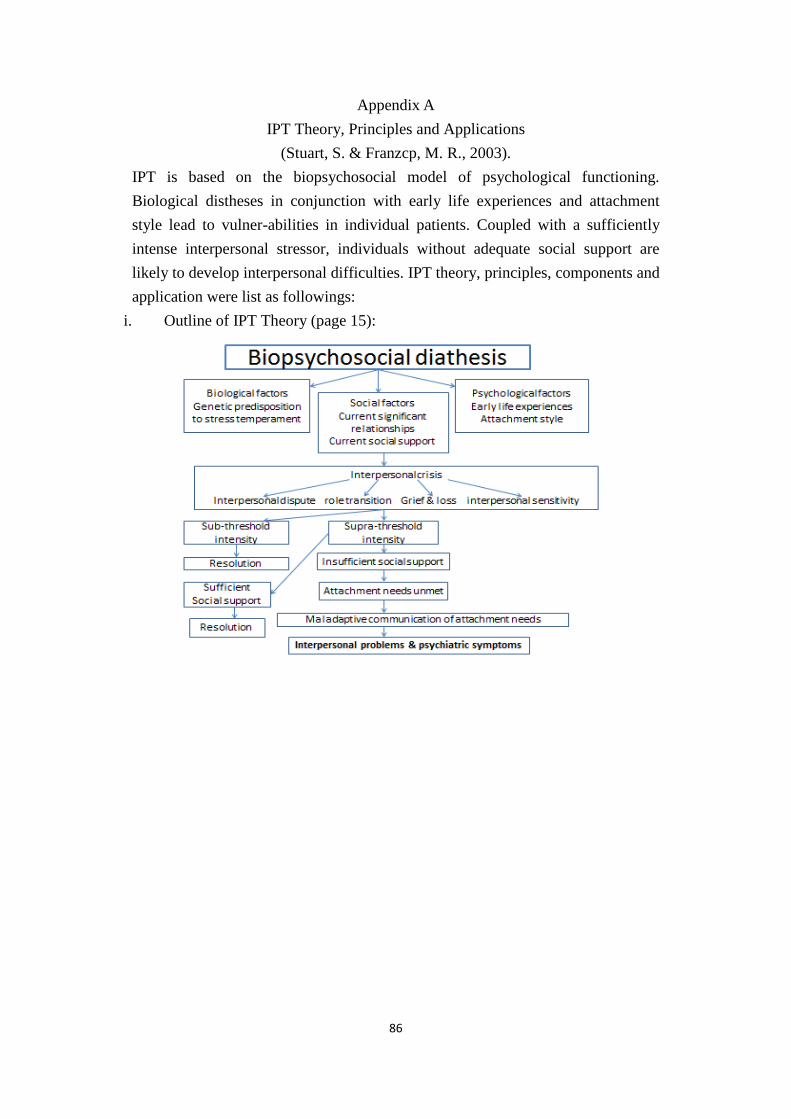
86
Appendix A
IPT Theory, Principles and Applications
(Stuart, S. & Franzcp, M. R., 2003).
IPT is based on the biopsychosocial model of psychological functioning.
Biological distheses in conjunction with early life experiences and attachment
style lead to vulner-abilities in individual patients. Coupled with a sufficiently
intense interpersonal stressor, individuals without adequate social support are
likely to develop interpersonal difficulties. IPT theory, principles, components and
application were list as followings:
i. Outline of IPT Theory (page 15):

87
ii. Components of IPT (page 39):
iii. IPT Techniques (section 3)

88
iv. IPT Four problem areas -interpersonal dispute, role transition, grief,
interpersonal sensitivity:
Interpersonal Disputes
Disagreement, arguments of relationships leading to attachment disruptions
cause distress consequence & interpersonal problems
3 stages:
Negotiation: ongoing change attempts
Impasse: resolve dispute attempts stalled
Dissolution: conflict advanced stage, ‘move on’ relationship as role
transition
6 IPT techniques:
Clarification: open-ended questions & empathic listening to identify
dispute
expression of affect: discuss relationship to help recognize emotional
reactions
communication style analysis
problem solving: collaborate to generate potential solutions to dispute,
gain mastery and develop sills to address problem
role playing: therapist gain communication style insight and give
feedback, help patient to gain insight of other’s experience and help to
develop assertiveness or communication skills
relationship appraisal: examine relationship expectations and determine
realistic of expectations, help to realistically appraise relationship
situation

89
Role Transitions
• Relationship changes occur in psychosocial contexts changes as in role
transition
• Therapist focus on patient ambivalent feelings undergoing transition, bring
attention to positive & negative reactions to change
• Defining old role: help patient to understand her circumstances, recognize
loss or anxiety, facilitate change, help to conceptualize old role & new role
in more balance & realistic way
‘What is it like to be a new parent?’
• Nature of role transitions:
Life stage : adolescence, parenthood, aging, retirement
Situational: job loss, promotion, graduation, migration
Acquisitive: career advancement, new house, financial windfall
Relationship: marriage, divorce, step-parenthood
Illness related: diagnosis of chronic illness, adaptation to pain or
physical limitations

90
Grief & Loss
Three stages:
Protest, despair & detachment
IPT goal:
help to work through stages
have a grief resolution
– Help patient develop insight and experience of loss
– Sharing experience with others
– Help to engage social support
– Diminish sense of isolation
– Develop new attachment
Basic tasks of working with grief in IPT
Identifying a grief or loss issue: relationship with loss, nature of loss,
context of loss, age of lost person, age of bereaved, absence of affect
Clarifying circumstances surrounding the loss: help to understand the
circumstances of loss
– What are your feelings about the lost individual?
– Linking loss to psychiatric onset symptoms or social dysfunction: help
to link timing of loss to onset of problems that develop a understanding
of significance of loss
– Helping patient accept painful affects associated with loss: help to
recognize affect within therapeutic relationship
– Help patient initiate new attachments & develop more effective social
supports: encourage to share experience of loss with others that help to
fulfilling some emotional, physical & social needs that met by lost
person

91
Interpersonal Sensitivity
Common factors associated with interpersonal sensitivity
Attachment style
Personality factors
Temperament
Development issues
Persisting effects of illness or mood stage
Relationships which reinforce sensitivity
Cultural factors
‘Berkson’s bias’
Assessing interpersonal sensitivity
Review of current relationships
Review old relationships
Review therapeutic relationship
Focus on three goals:
Optimizing current interpersonal functioning
Helping the patient to establish new supportive relationships
Helping to resolve the acute stressor which led to seek treatment
Encourage to broaden social network by increasing social contact
Use therapeutic relationship to improve interpersonal functioning

92
v. Maintenance Treatment
It is less frequent & less intense
Goals:
Review the state of original presenting problem & the progress the patient
continues to make
Consider new problems which do not require acute intervention
Continue to maximize patient’s interpersonal functioning over time
Provide a continuing relationship for resumption of acute treatment if
needed
• Basic techniques
No different from those used in acute treatment
Therapist stance less active
Goals to maximize patient’s independent functioning
Encouragement to know how to solve the problem

93
Appendix B
Literature Searching Record & Flowcharts
1. PsycINFO (Earliest to August 28, 2012 updated)
Keywords Results Found relevant
studies
S1 ‘Interpersonal psychotherapy’ 12993
S2 S1 AND Antenatal 14 4 [○2 ○4 ○6 ○8 ]
S3 S1 AND Postnatal 33 3 [○1 ○2 ○4 ]
S4 S1 AND Postpartum 74 6 [○1 ○2 ○4 ○6 ○7 ○8 ]
S5 S1 AND Perinatal 29 1 [○4 ]
S6 S1 AND Antepartum 9 1 [○6 ]
S7 S1 AND Prenatal 20 2 [○1 ○4 ]
S8 S1 AND Pregnancy 71 5 [○1 ○2 ○4 ○6 ○7 ]
S9 S1 AND Childbearing 7 1 [○2 ]
S10 S2 AND S3AND S4 AND S5 AND S6 AND
S7AND S8 AND S9
257
S11 S2 AND Depression 13 4 [○2 ○4 ○6 ○8 ]
S12 S3 AND Depression 13 3 [○1 ○2 ○4 ]
S13 S4 AND Depression 71 6 [○1 ○2 ○4 ○6 ○7 ○8 ]
S14 S5 AND Depression 19 1 [○4 ]
S15 S6 AND Depression 9 1 [○6 ]
S16 S7 AND Depression 9 1 [○6 ]
S17 S8 AND Depression 42 6 [○1 ○2 ○4 ○6 ○7 ○8 ]
S18 S9 AND Depression 4 1 [○2 ]
S19 S11 AND S12 AND S13 AND S14 AND S15
AND S16 AND S17 AND S18
180
S20 S1 AND S10 AND S19 13430
S21 S10 AND S19 437 Total: 46
Selected Study Code: ○1 , Crockett, et al., 2008; ○2 , Gao, et al., 2010; ○3 , Gao, et al., 2012; ○4 , Grote, et al., 2009; ○5 ,
Leung & Lam, 2012; ○6 , Spinelli & Endicott, 2003; ○7 , Zlotnick, et al., 2001; ○8 , Zlotnick, et al., 2006
First manual screening on titles and abstracts (n=437)
Second manual screening on publications (n=46)
Final included publications (n=6) ○1 ○2 ○4 ○6 ○7 ○8
Manually excluded (n=391):
- Unrelated to antenatal IPT study to reduce PND
- Not RCT study
- Not primary source study
- Pregnancy subject with current mental illness
- Pregnancy subject with complication
Manually excluded: Duplication studies (n=40)
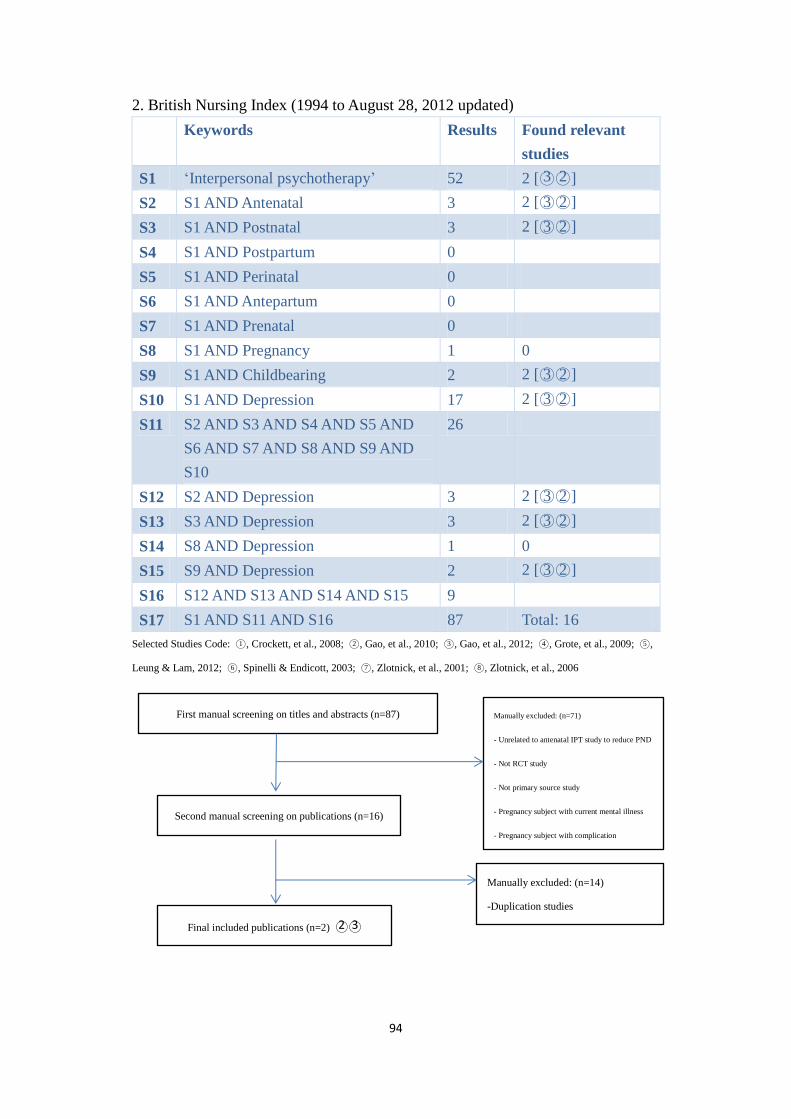
94
2. British Nursing Index (1994 to August 28, 2012 updated)
Keywords Results Found relevant
studies
S1 ‘Interpersonal psychotherapy’ 52 2 [○3 ○2 ]
S2 S1 AND Antenatal 3 2 [○3 ○2 ]
S3 S1 AND Postnatal 3 2 [○3 ○2 ]
S4 S1 AND Postpartum 0
S5 S1 AND Perinatal 0
S6 S1 AND Antepartum 0
S7 S1 AND Prenatal 0
S8 S1 AND Pregnancy 1 0
S9 S1 AND Childbearing 2 2 [○3 ○2 ]
S10 S1 AND Depression 17 2 [○3 ○2 ]
S11 S2 AND S3 AND S4 AND S5 AND
S6 AND S7 AND S8 AND S9 AND
S10
26
S12 S2 AND Depression 3 2 [○3 ○2 ]
S13 S3 AND Depression 3 2 [○3 ○2 ]
S14 S8 AND Depression 1 0
S15 S9 AND Depression 2 2 [○3 ○2 ]
S16 S12 AND S13 AND S14 AND S15 9
S17 S1 AND S11 AND S16 87 Total: 16
Selected Studies Code: ○1 , Crockett, et al., 2008; ○2 , Gao, et al., 2010; ○3 , Gao, et al., 2012; ○4 , Grote, et al., 2009; ○5 ,
Leung & Lam, 2012; ○6 , Spinelli & Endicott, 2003; ○7 , Zlotnick, et al., 2001; ○8 , Zlotnick, et al., 2006
First manual screening on titles and abstracts (n=87) Manually excluded: (n=71)
- Unrelated to antenatal IPT study to reduce PND
- Not RCT study
- Not primary source study
- Pregnancy subject with current mental illness
- Pregnancy subject with complication
Second manual screening on publications (n=16)
Manually excluded: (n=14)
-Duplication studies
Final included publications (n=2) ○2 ○3

95
3. Maternal & Infant Care (1971 to August 28, 2012 updated)
Keywords Results Found relevant
studies
S1 ‘Interpersonal psychotherapy’ 17 4 [○3 ○2 ○7 ○8 ]
S2 S1 AND Antenatal 7 3 [○2 ○3 ○8 ]
S3 S1 AND Postnatal 12 4 [○2 ○3 ○7 ○8 ]
S4 S1 AND Postpartum 11 4 [○2 ○3 ○7 ○8 ]
S5 S1 AND Perinatal 0
S6 S1 AND Antepartum 2
S7 S1 AND Prenatal 0
S8 S1 AND Pregnancy 9 3 [○3 ○7 ○8 ]
S9 S1 AND Childbearing 2 2 [○3 ○2 ]
S10 S1 AND Depression 17 2 [○3 ○2 ○7 ○8 ]
S11 S1 AND S2 AND S3 AND S4 AND
S5 AND S6 AND S7 AND S8 AND
S9 AND S10
Total:77 Total: 22
Selected Studies Code: ○1 , Crockett, et al., 2008; ○2 , Gao, et al., 2010; ○3 , Gao, et al., 2012; ○4 , Grote, et al., 2009; ○5 ,
Leung & Lam, 2012; ○6 , Spinelli & Endicott, 2003; ○7 , Zlotnick, et al., 2001; ○8 , Zlotnick, et al., 2006
First manual screening on titles and abstracts (n=77)
Manually excluded: (n=55)
- Unrelated to antenatal IPT study to reduce PND
- Not RCT study
- Not primary source study
- Pregnancy subject with current mental illness
- Pregnancy subject with complication Second manual screening on publications (n=22)
Final included publications (n=4) ○2 ○3 ○7 ○8
Manually excluded: (n=18)
-Duplication studies

96
4. Embase (1980 to August 28, 2012 updated)
Keywords Results Found
relevant
studies
S1 ‘interpersonal psychotherapy’ including
related term
16823
S2 S1 AND Antenatal 17 4 [○2 ○3 ○6 ○8 ]
S3 S1 AND Postnatal 24 4 [○2 ○3 ○4 ○6 ]
S4 S1 AND Postpartum 0
S5 S1 AND Perinatal 23 1 [○4 ]
S6 S1 AND Antepartum 11 1 [○6 ]
S7 S1 AND Prenatal 16 3 [○4 ○6 ○8 ]
S8 S1 AND Pregnancy 49 5 [○2 ○3 ○4 ○6
○8 ]
S9 S1 AND Childbearing 8 2 [○2 ○3 ]
S10 S2 AND S3 AND S4 AND S5 AND S6 AND
S7 AND S8 AND S9
148
S11 S1 AND Depression 597
S12 S11 limit to randomized control trial 130 4 [○2 ○3 ○6 ○8 ]
S13 S10 AND S12 278 Total: 24
Selected Study Code: ○1 , Crockett, et al., 2008; ○2 , Gao, et al., 2010; ○3 , Gao, et al., 2012; ○4 , Grote, et al., 2009; ○5 ,
Leung & Lam, 2012; ○6 , Spinelli & Endicott, 2003; ○7 , Zlotnick, et al., 2001; ○8 , Zlotnick, et al., 2006
First manual screening on titles and abstracts (n=278)
Manually excluded: (n=254)
- Unrelated to antenatal IPT study to reduce
PND
- Not RCT study
- Not primary source study
- Pregnancy subject with current mental
illness
- Pregnancy subject with complication
Second manual screening on publications (n=24)
Final included publications (n=5) ○2 ○3 ○4 ○6 ○8
Manually excluded: (n=19)
-Duplication studies

97
5. PubMed (1950 to August 28, 2012 update)
Keywords Results Found relevant
studies
S1 ‘interpersonal psychotherapy’ [all field] 8223
S2 S1 limited to RCT 625
S3 S2 AND antenatal [all field] 5 5 [○2 ○3 ○4 ○6 ○8 ]
S4 S2 AND postnatal [all field] 8 4[○2 ○3 ○4 ○6 ]
S5 S2 AND postpartum [all field] 16 6 [○2 ○3 ○4 ○6 ○7 ○8 ]
S6 S2 AND perinatal [all field] 2 1 [○4 ]
S7 S2 AND antepartum [all field] 1 1 [○6 ]
S8 S2 AND prenatal[all field] 4 3 [○4 ○7 ○8 ]
S9 S2 AND pregnancy [all field] 14 6 [○2 ○3 ○4 ○6 ○7 ○8 ]
S10 S2 AND childbearing [all field] 4 2 [○2 ○3 ]
S11 S2 AND depression [all field] 310 6 [○2 ○3 ○4 ○6 ○7 ○8 ]
S12 S1 AND antenatal AND depression 13 6 [○2 ○3 ○4 ○5 ○6 ○8 ]
S13 S2 AND S3 AND S4 AND S5 AND
S6 AND S7 AND S8 AND S9 AND
S10 AND S11 AND S12
1002 Total: 40
Selected Study Code: ○1 , Crockett, et al., 2008; ○2 , Gao, et al., 2010; ○3 , Gao, et al., 2012; ○4 , Grote, et al., 2009; ○5 ,
Leung & Lam, 2012; ○6 , Spinelli & Endicott, 2003; ○7 , Zlotnick, et al., 2001; ○8 , Zlotnick, et al., 2006
First manual screening on titles and abstracts (n= 1002)
Manually excluded: (n=962)
- Unrelated to antenatal IPT study to reduce
PND
- Not RCT study
- Not primary source study
- Pregnancy subject with current mental
illness
- Pregnancy subject with complication
Second manual screening on publications (n= 40)
Manually excluded: (n= 33)
-Duplication studies
Final included publications (n=7) ○2 ○3 ○4 ○5 ○6 ○7 ○8

98
6. Internet of International society of interpersonal psychotherapy (IsIPT)
on August 28, 2012 updated
Keywords Results Found
relevant
studies
S1 Study reference list of ‘interpersonal
psychotherapy’
125
S2 S1 AND Antenatal 0 0
S3 S1 AND Postnatal 1 0
S4 S1 AND Postpartum 2 0
S5 S1 AND Perinatal 3 1[○4 ]
S6 S1 AND Antepartum 0 0
S7 S1 AND Prenatal 0 0
S8 S1 AND Pregnancy 2 1[○6 ]
S9 S1 AND Childbearing 2 0
S10 S1 AND Depression 115 0
Total study reference list Total:
125
Total: 2
Selected Study Code: ○1 , Crockett, et al., 2008; ○2 , Gao, et al., 2010; ○3 , Gao, et al., 2012; ○4 , Grote, et al., 2009; ○5 ,
Leung & Lam, 2012; ○6 , Spinelli & Endicott, 2003; ○7 , Zlotnick, et al., 2001; ○8 , Zlotnick, et al., 2006
First manual screening on titles (n=125)
Second manual screening on publications (n=2)
Manually excluded: (n=123)
- Unrelated to antenatal IPT study to
reduce PND
- Not RCT study
Final included publications (n=2) ○4 ○6
Manually excluded: (n=0)
-Duplication studies

99
APPENDIX C
Review Literature Studies Searching Record Table
Database
PsyInFO British
Nursing Index
Maternal &
Infant Care
Embase PubMed IsIPT* Total
Initial screening studies 437 87 77 278 1002 125 2006
Exclusion criteria** -391 -71 -55 -254 -962 -123 -1856
Subsequent screening
studies
46 16 22 24 40 2 150
Duplication removed -40 -14 -18 -19 -33 0 -124
Selected review studies 6 2 4 5 7 2 26
Study Code^ 1,2,4,6,7,8 2, 3 2,3,7,8 2,3,4,6,8 2,3,4,5,6,7,8 4,6 1 - 8
IsIPT*: Internet of International society of interpersonal psychotherapy. Exclusion criteria**: unrelated to antenatal IPT
study to reduce PND, not RCT study, not primary study source, pregnancy subject with current mental illness, pregnancy
subject with complication. Study Code^:
1. Crockett, K., Zlotnick, C., Davis, M., Payne, N. & Washington, R. (2008). A depression preventive intervention for
rural low-income African-American pregnant women at risk for postpartum depression. Arch. Womens Mental
Health. 11, 319-325.
2. Gao, L.L., Chan, W. C. Sally, Li, X. et al. (2010). Evaluation of an interpersonal psychotherapy oriented childbirth
education program for Chinese first time childbearing women, a randomized controlled trial. International Journal
of Nursing Studies, 47, 1208-1216.
3. Gao, L. L., Chan, W.C. Sally & Sun, K. (2012). Effects of an interpersonal psychotherapy oriented childbirth
education program for Chinese first time childbearing women at 3 month follow up, a randomized controlled trial.
International Journal of Nursing Studies, 49, 274-281.
4. Grote, N. K., Swartz, H. A., Geibel, S.L., Zuckoff, A., Houch, P. R., Frank, E. (2009). A randomized controlled trial
of culturally relevant, brief interpersonal psychotherapy for perinatal depression. Psychiatric Services. 60, 313-321.
5. Leung, S. S. K. & Lam, T. H. (2012). Group antenatal intervention to reduce perinatal stress and depressive
symptoms related to intergenerational conflicts: a randomized controlled trial. International Journal of Nursing
Studies. 49(11), 1391-1402.
6. Spinelli, M. G. & Endicott, J. (2003). Controlled clinical trial of interpersonal psychotherapy versus parenting
education program for depressed pregnant women. American Journal Psychiatry. 160, 555-562.
7. Zlotnick, C. Johnson, S. L., Miller, I. W., Pearlstein, T. & Howard, M. (2001). Postpartum depression in women
receiving public assistance, a pilot study of an interpersonal therapy oriented group intervention. American Journal
of Psychiatry, 158, 638-640.
8. Zlotnick, C., Miller, I. W., Pearlstein, T., Howard, M. & Sweeney, P. (2006). A preventive intervention for pregnancy
women on public assistance at risk for postpartum depression. American Journal of psychiatry. 163, 1443-1445.

100
Appendix D Evidence Tables
Bibliographic
Citation
Country
Study Type
& Evidence
Level
Subject Characteristics &
Study Site Number
Intervention
(IG)
Comparison
(CG)
Length of
Follow Up
Outcome
measures
Effect Size Randomization,
conceal &
blinding
1.Crockett,
et al. (2008)
USA
Funding:
Klingenstein
third
Generation
Foundation
New York.
Random
ized
control
trial
(1+)
-36 African-American in a prenatal site
-Mean age: 23.4 (SD=4.98)
-24 to 31 gestation weeks
-High school, IG: 41.7%, CG: 41.2%
-College, IG 5.3%, CG 5.9%
-Single,:83.8%, married: 13.9%
-Separated: 2.8%
-36.1% unemployed, 16% full employed
-Below $10000, 47.2%
- All subject on public assistance
-Mean Cooper risk Survey 34.5 (SD=6.56)
-No current major depression disorder
-38.9% had one child
IPT class: 4 x 90 minutes, <20 in group
& 1 individual session 50 min 2 weeks
after delivery. Run by therapist (PhD or
M. Ed. Counseling)
Content: PND information, stress
management, role transition
management, develop support system,
interpersonal conflicts management skill
(N=19)
Routine:
received
care-as-usu
al
educational
pamphlets
(n=17)
(T1):
Pre-intervent
ion
(T2):
4 weeks after
intake
(T3):
PN 2-3
weeks
(T4):
PN 3 months
-Cooper
Risk Survey
>27 score.
-EPDS:≥10,
T1, 2 , 3, 4.
-SAS-SR: T
1 & T2
-PPAQ at
T3 & T4.
- PSI at T3
& T4.
-No
significant
difference
: EPDS;
PSI;
SAS-SR.
Group
assignment
randomized
with
concealment.
Blinding not
mentioned.
General comment: Dropout-5.26%, move away. Good satisfaction rate and participant willingness to accept intervention is important in implement interpersonal education.
There were not blind to therapist who administered EPDS. Good attendance rate 4.58 (SD = 4.95, mode =5).
Edinburgh Postnatal Depression Scale (EPDS), Social Adjustment Scale Questionnaire (SAS-SR), Postpartum Adjustment Questionnaire ( PPAQ), Parenting
Stress Index (PSI)

101
Bibliographic
Citation
Country
Study Type &
Evidence Level
Subject Characteristics &
Study Site Number
Intervention
(IG)
Comparison
(CG)
Length of
Follow
Up
Outcome
measures
Effect Size Randomizat
ion conceal
& blinding
2. Gao, et
al (2010)
Peoples’s
Republic
of China
Funding:
None
Randomized
controlled
study (1++)
-194 women in a regional hospital
-Mean age IG: 28.5±2.8, CG: 28.4±2.73
-First pregnancy no psychiatric disorder or
pregnancy complication, >28 weeks
-High school or below: IG: 13.5%, CG:
17.3%
- College or above: IG: 86.5%, CG: 82.7%
- All married living with husband
- Professional, IG: 34.5%, CG: 38.4%
-Semi-prof, IG: 39.1%, CG: 36.6%
-Skill, IG: 25.3%, CG: 25%
-unskilled, IG: 1.1%, CG: 0%
-Below ¥3000, IG: 35.4%, CG: 26.5%
-Above ¥3000, IG: 64.6%, CG: 73.5%
-IG, 47.9% spontaneous delivery & 47.9 %
caesarean delivery
-CG, 40.8% spontaneous delivery & 55.1%
caesarean delivery
- Newborn’s male, IG: 51%, CG: 56.1%
-Newborn’s female, IG: 49%, CG: 43.9%
IPT: 2 class, 60 min, <10 in
group
Trained midwife nurse
Content: ice-break game,
motherhood, stress coping,
communication skill, baby
gender issues, PND data,
social support , resolve
interpersonal conflict,
marital relationship, good
relationship strategies,
Chinese PN practice (n=96)
Routine
education:
(4 hours)
focus on
Delivery
education
& child
care (n=98)
-PN
Phone
FU 2
weeks
- 6
weeks
- EPPDS:
≥13
- GHQ:≥3
-SWIRS
-EPDS:-3.76, IG:
6.59 (SD 4.1) &
CG: 8.87 (SD 4.37)
( p = 0.000)*
-GHQ: -3.3,IG:
1.48 (SD 1.57) &
CG: 2.29 (SD 1.81)
(p = 0.001)*
- SWIRES: 3.25
IG: 11.03 (SD
1.55) & CG: 10.24
(SD 1.78) ( p =
0.001)*
Group
assignment
randomized.
With
concealment.
Blinded to
treatment,
collection &
analysis
General comment: Dropout -9.8%, lost contact & complication. Study limit to single teenage mother. Intention- to-treat and blinding increase study quality. * p < 0.05.
Edinburgh Postnatal Depression Scale (EPDS), General health questionnaire (GHQ), Satisfaction With Interpersonal Relationships Scale (SWIRES).

102
Bibliographic
Citation
Country
Study
Type &
Evidence
Level
Subject Characteristics &
Study Site Number
Intervention
(IG)
Comparison
(CG)
Length
of
Follow
Up
Outcome
measures
Effect Size Randomiza
tion &
conceal
method
3. Gao, et
al.,(2012)
Peoples’s
Republic
of China
Funding:
None
Rando
mized
control
trial
(1++)
-194 women in a regional hospital
-Mean age, IG: 28.5±2.8 CG: 28.4±2.73
-First pregnancy no psychiatric disorder or pregnancy complication, >28 weeks,
- High school or below, IG: 13.5%, CG: 17.3%
-College or above, IG: 86.5%, CG: 86.5%
-Married living with husband
- Professional, IG: 34.5%, CG: 38.4%
-Semi-prof, IG: 39.1%, CG: 36.6%
-Skill, IG: 25.3%, CG: 25%
-Unskilled, IG: 1.1%, CG: 0%
-< ¥6000, IG: 35.4%, CG: 26.5%
- > ¥6000, IG: 64.6%, CG: 73.5%
- IG delivery, 47.9% normal & 47.9 % caesarean
-CG delivery, 40.8% normal & 55.1% caesarean
IPT: 2 class, 90 min,
<10 in group
Trained midwife nurse
Midwife nurse (Trained)
(n=96)
Content;
-Ice break game
-Motherhood
transition
-Stress coping
-Communication skill
-Baby gender issues
-PPD sign & symptoms
-Social support source
-Skill resolve
interpersonal conflict
-Marital relationship
-Relationship strategies
-Chinese postnatal
practice
Routine
education
Content:
-Breastfeeding
-Infant care
-Labor process
- Labor pain
-Antenatal &
postnatal care
(n=98)
-PN 2
weeks
Phone
FU
-PN 6
weeks
-PN 3
months
-EPDS:
≥13
-GHQ:
≥3
-PSSS
-PSOC-E
EPDS: -0.31, IG: 6.59(SD4.1), CG 8.87 (SD4.37) (p<0.01)*
GHQ: -0.22, IG: 1.48 (SD1.57), CG: 2.29 (SD1.81)(p<0.01)*
PSOC-E: -0.37, IG 35.74 (SD 4.45) & CG:
32.43(SD6.78)(p<0.01)*
PSS: 0.25, IG: 68.76 (7.56) & CG: 62.59 (9.00) (p=0.004)*
3 months:
EPDS:-2.39, IG: 5.61 (3.33) & CG: 6.87 (SD
3.97)(p=0.018)*
GHQ: -0.77, IG:1.44(SD1.57) & CG:1.71(SD1.84)(p<0.01)*
PSOC-E: 2.43, IG: 37(5.13) & CG: 32.21
(SD5.14)(p=0.016)*
PSS: 2.33, IG: 65.92(8.1) & CG: 63.11(8.67) (p=0.021)*
Group
assignment
randomized
by table of
random
tables with
concealment
method.
Blinding not
report.
General comments: Dropout -9.8%, lost contact & complication. ITP benefit to first pregnancy. Limited to multi-parity, complicated pregnancy and social class. * p < 0.05.
Edinburgh Postnatal Depression Scale (EPDS), General Health Questionnaire (GHQ), Perceived Social Support Scale ( PSSS), Parenting Sense of Competence Efficacy Subscale (PSOC-E)

103
Bibliographic
Citation
Country
Study Type
& Evidence
Level
Subject Characteristics &
Study Site Number
Intervention
(IG)
Compari
son
(CG)
Length of
Follow Up
Outcome
measures
Effect Size Randomizat
ion &
conceal
method
4.Grote, et
al., (2009)
USA
Funding:
National Institute
of mental Health
-Staunton Farm
foundation
-National Center
for Research
Resources
Rando
mized
control
trial
(1++)
-53 women in a hospital, Mean aged, IG:24.3±5.3, CG: 24.7±5.6
-Mean gestation week, IG: 22±6.7, CG: 20.4±6.8
-High school below, IG: 8%, CG: 18%
-High school degree, IG: 24%, CG: 14%
-Above high school, IG: 68%, CG: 69%
-Single, IG: 5.6%, CG: 4.3% ; Married, IG: 8%, CG: 7%; Cohabits, IG: 36%, CG 29%
-Full time, IG: 20%, CG: 11%; part time, (IG: 24%, CG: 18%
-Unemployed, IG: 56%, CG: 71%
-< $10000, IG: 48%, CG: 68%; $10000-$20000, IG: 32%, CG: 21%,
-> $2000, IG: 20%, CG: 11%
-Baseline, IG: EPDS 18.9±3.4; BDI 24.3±10.2; BAI 14.4±11; SAS 3.1±0.8
-Baseline, CG: EPDS 18.2±3.8; BDI 25.9±11.1; BAI 16.3±10.5; SAS 3.2±0.6
-IG, 20% white; 68% African American; 8% Latina; 4% Biracial
-CG, 36% white; 57% African American; 0% Latina; 7% Biracial
IPT: 8 class 45
minutes,
maintenance up
to PN 6
months, <25 in
group
IPT trained
therapist
clinician with
doctoral-level
& master’s
level
(n=25)
Routine
education
: usual
education
program
in
obstetric
clinic
(n=28)
3 months
&
6 months
-EPDS:
≥12
-BDI
-BAI
-SAS,
cutoff
>2.2
-PPAQ
-EPDS: ES 0.71 (p<0.001)*, BDI: ES 0.33 (p=0.019)*
-BAI: ES 0.27 (p=0.051), -SAS: ES: 0.26 (p=0.63)
6 months:
-EPDS: ES 0.89 (p<0.001)*, -BDI: ES 0.47 (p=0.002)*
-BAI: ES 0.24 (p=0.88), -SAS:ES 0.46 (p=0.002)*
Secondary outcome
-IG: 95% not depression compared with CG: 58% (ES .96, p<
0.003)*.
-IG: No depression, CG: 70% in 6 months (ES 1.22, p<0.005)*.
-IG: 80% respond to treatment vs CG: 29% (ES 1.08, p<0.001)*.
-PN 6 months, IG: 88% respond to treatment, 25% of CG (ES 1.17,
p<0.001)*.
-PPAQ, IG 1.47±0.18, CG: 1.78±0.26, p<0.001)*.
-IG: high satisfaction (4.4±0.39).
Group
assignment
randomized
in permuted
block
assignment.
Concealment
not reported.
Blinding not
mention.
General comment: Dropout-18.8%, lack of time. Study relevant to culture socioeconomically disadvantage group, significant reduction in depression symptoms before and PN 6 months. Significant improvement in
social functioning at PN 6 months. Limitation was small sample size, lack of blinding which threat to internal validity. * p < 0.05.
Edinburgh Postnatal Depression Scale (EPDS), Beck Depression Inventory (BDI), Beck Anxiety Inventory (BAI), Social Adjustment Scale (SAS), Postpartum Adjustment Questionnaire ( PPAQ)

104
Bibliographic
Citation
Country
Study
Type &
Evidence
Level
Subject Characteristics &
Study Site Number
Interven
tion
(IG)
Compari
son
(CG)
Length of
Follow Up
Outcome
measures
Effect Size Randomizatio
n & conceal
method
5.Leung &
Lam (2012)
Hong Kong
Funding:
Hong Kong
Jockey Club
Charities Trust
Rand
omize
d
contr
ol
trial
(1++)
-156 in 6 MCHCs, pregnant women with grandparents involve in childcare
with no mental illness
-Mean age, IG, 31.3±4.02, CG:31.15±4.12
-Gestation week, IG:20.44±5.25, CG: 20.01±4.97
- Education < secondary, IG: 44.9%, CG: 51.3%; <Tertiary: (IG: 54.1%, CG:
48.7%
-Single, IG: 6.4%, CG: 10%; married: IG: 93.6%, CG: 90%
-Full time, IG: 69.2%, CG: 73.1%
-Housewife, IG: 28.2%, CG: 21.8; other, IG: 2.6%, CG: 5.1%
-IG: < $20,000: 0.05%; >$40,000: 41%.
-CG: < $20,000: 15.4%; >$40,000: 48.7%
-First pregnancy, IG: 73%, CG: 74%
-Second pregnancy, IG: 27%, CG: 26%
Baseline EPDS, IG: >12: 41%, CG: >12: 30%
IPT: 4
class 90
min, <12
in group
2 Trained
nurse as
therapist
(n=78)
Routine
education
:
antenatal
MCHC
routine
education
program
(n=78)
(T1)
Initial
(T2)
1 month
post IPT
(T3)
PN 6-8
weeks
-PSS
-EPDS: ≥13
& subgroup
≥12
-REM
-PAQ:
self-design
ed
-SHS
- PHS
-T2:EPDS: (p=0.18, Cohen d=0.2), T3: (p=0.72, Cohen d=0.13)
-PSS in T2 (p=0.017; Cohen d=0.38)*
- REM, T2: (p=0.3, Cohen d=0.09), T3: (p=0.85, Cohen d=0.14)
- PAQ, T2 (p=0.32, Cohen d=0.08),T3: (p=0.99, Cohen d=0.1)
- SHS, T2 (p=0.004; Cohen d = 0.41)*, T3 (p=0.67, Cohen d=0.18)
- PHS: T2 (p=0.86, Cohen d=0.16), T3 (p=0.58, Cohen d=0.26).
Subgroup analysis (>12) EPDS:
- EPDS, T2: (p=0.38, d=0.26), T3: (p=0.35, d=0.27).
- PSS, T2: (p=0.035, Cohen s= 0.61)*.
- REM in T2 (p=0.012; Cohen d=0.76)* & T3 (p=0.025; Cohen
d=0.67)*.
-PAQ in T3 (p=0.046 Cohen d= 0.59)*.
Group
assignment
randomized
with computer
generate
permuted block
(4 subsets).
Blinding of
data collect by
research staff.
General comment: Dropout -7%. .Intention-to-treat analyzed increased stronger evidence. Low dropout rate. First pioneer IPT HK program. Good quality assurance of trained therapist which increase fidelity. * p < 0.05.
Perceived Stress Scale (PSS), Edinburgh Postnatal Depression Scale ( EPDS), Relationship Efficacy Measure ( REM), Perceived Ability Questionnaire (PAQ), Subjective Happiness Scale (SHS), Perceived Health Score (PHS)

105
Bibliographic
Citation
Country
Study Type &
Evidence Level
Subject Characteristics & Study
Site Number
Intervention
(IG)
Compariso
n
(CG)
Length
of
Follow
Up
Outcome
measures
Effect Size Randomization
& conceal
method
6.Spinelli,
& Endicott,
(2003)
USA
Funding:
NIMH Research
Scientist
Development Award
for Clinicians (grant
number MH-01276).
Randomize
control trial
(1++)
-38 women in a maternal clinic
-Mean age, IG: 28.3±5.7, CG: 29.3±7.1
-Gestation week, IG: 21.5±8.3, CG: 21±6.8
-Education: no mention
- Single, IG: 42.9, CG: 58.8%
-Married or cohabits, IG: 57.1%, CG: 41.2
-Employed, IG: 28.6, CG: 29.4%
-Student, IG: 4.8%, CG: 0%
-Unemployed, IG: 66.6%, CG: 70.6%
- IG: <$15000 33%; >$15000 67%,
-CG: <$15000 41%; >$15000 59%
-Depression rating HDRS score >12
-73% history of major depression
IPT:16 class 45 minutes weekly,
<25 in group
Trained therapist M. D.
qualification
Content:
-grief
-role transition
-interpersonal deficits
-interpersonal role dispute
-pregnancy discussion (n=21)
Routine parent
education
program (45
minutes)
Focus on
pregnancy
development
stages,
delivery,
parenting and
early
childhood
(n=17)
PN 16
weeks
-EPDS
-BDI
-HDRS
-EPDS:-2.99, IG:
33.3% & CG:
11.8%
(p = 0.005)*
-BDI: 2.72, IG:
52.4% & CG:
23.5%
(p< 0.02)*
-HDRS: 2.42,
IG:52.4 & CG:
29.4% (p<0.03)*
Group
assignment
randomized
with
concealment
by table of
random
numbers.
Blinding not
report.
General comment: Dropout-24%. Significant improvement of IPT program compare with control parenting education program among antenatal women. Study limitation is small sample size. * p < 0.05.
Edinburgh Postnatal Depression Scale (EPDS), Beck Depression Inventory (BDI), Hamilton Depression Rating Scale (HDRS)

106
Bibliographic
Citation
Country
Study Type &
Evidence Level
Subject Characteristics & Study Site Number Intervention
(IG)
Comparison
(CG)
Length of
Follow Up
Outcome
measures
Effect Size Randomizati
on &
conceal
method
7.Zlotnick,
et al.,(2001)
USA
Funding:
Klingenstein
Brown
University
Random
ized
control
trial
(1+)
-35 women in a general hospital, Mean age: 23.4 ±4.41
-Gestation week: 20-32 weeks
-Education: no mention
-Single: 77%, occupation: no mention
-All subjects on public assistance
-Pre-intervention BDI: 11.06±6.84
-Mean risk factor for PND: 2.6±1.9
-IG: 77% history of depression; 47% poor social support;
71% BDI>10; 88% recent stressful event
-CG: 50% history of depression, 50% poor social support,
44% BDI score>10; 78% recent stressful event.
-46% Caucasian; 77% single; 77% high school.
-Not major depression
IPT: 4 class 60 min,
4-6 in group
No mention
therapist
Content:
role transitions &
motherhood , skills
resolving
interpersonal
conflicts (n=17)
Routine
education:
standard
antenatal
education
class in
prenatal
clinic (n=18)
3
months
-BDI:
cutoff
≥10
-3.5, IG: 8.4 (7.8) & CG:
11.3 (4.8) (p = 0.001)*.
-IG less develop PND
than CG (p = 0.02)*.
-Reliable improvement
in IG 35% than CG 11%.
-0% develop PND in IG,
33% develop in CG
Group
assignment
randomized
&
concealment
not report.
Blinding not
report.
General comment: Dropout -5.4%. High attendance rate 88% for at least 3/4 session. In group of financial disadvantage women at risk of PND, 4 session IPT program was successful in preventing PND of 3 months.
Small sample size had limitation of study’s validity. * p < 0.05.
Beck Depression Inventory (BDI)

107
Bibliographic
Citation
Country
Study Type &
Evidence Level
Subject Characteristics &
Study Site Number
Intervention
(IG)
Comparison
(CG)
Length of
Follow Up
Outcome
measures
Effect Size Randomization
& conceal
method
8.Zlotnick,
et al.,
(2006)
USA
Funding:
NIMH
Randomized
control trial
(1+)
-98 women in a prenatal clinic
-Mean age: 22.4±4.72
-Gestation: 23-32 weeks
-High school, 67%
-Single, 67%
-Occupation, no mention
-All subjects on public assistance
-Mean PND predictive index: 32.8
±4.81
-Previous major depression (n=31)
-44 Hispanic; 28 Caucasian, 17;
African American; 2 Asian & 8
other race
-All subjects not current mental
health illness.
-IPT: 4 class 60
min, 3-5 in group
by trained nurse
& one PN
individual session
(50 minutes)
Content:
-Reinforce skill for
mood changes,
-Interpersonal
difficulties,
-Newborn care
(N=53)
Routine
education:
standard
antenatal
education
class in
prenatal
clinic
(n=46)
3 months -BDI
-RIFTS
BDI - IG: 15.3
(6.96) to 9.39
(7.42) & CG: 16
(7.77) to 10.1
(9.41).
PND - IG: 4%,
CG:20% (p=0.04)*
Secondary result:
No significant
difference on BDI
or RIFS 3 months
after delivery,
controlling for
baseline scores.
Group
assignment
randomized
&
concealment
not report.
Blinding not
report.
General comment: Dropout- 13% because moved out of state that limited this study. Attendance rate 3.3 (SD = 1.97). * p < 0.05.
Beck Depression Inventory (BDI), Range of Impaired Functioning Tool (RIFTS)

108
Appendix E
Randomized Control Trials Checklist
Designed by Scottish Intercollegiate Guideline Network (SIGN) (2008a)
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Guideline topic: Key Question No:
Before completing this checklist, consider:
1. Is the paper a randomized controlled trial or a controlled clinical trial? If in doubt, check the study
design algorithm available from SIGN and make sure you have the correct checklist. If it is a
controlled clinical trial questions 1.2, 1.3, and 1.4 are not relevant, and the study cannot be rated
higher than 1+
2. Is the paper relevant to key question? Analyze using PICO (Patient or Population Intervention
Comparison Outcome). IF NO REJECT (give reason below). IF YES complete the checklist.
Reason for rejection: Reason for rejection: 1. Paper not relevant to key question □
2. Other reason □ (please specify):
Checklist completed by:
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study… In this study this criterion is:
1.1 The study addresses an appropriate and clearly
focused question.
Well covered
Adequately addressed
Poorly addressed
Not addressed
Not reported
Not applicable
1.2 The assignment of subjects to treatment groups is
randomised
Well covered
Adequately addressed
Poorly addressed
Not addressed
Not reported
Not applicable
1.3 An adequate concealment method is used
Well covered
Adequately addressed
Poorly addressed
Not addressed
Not reported
Not applicable
1.4 Subjects and investigators are kept ‘blind’ about
treatment allocation
Well covered
Adequately addressed
Poorly addressed
Not addressed
Not reported
Not applicable

109
1.5 The treatment and control groups are similar at the
start of the trial
Well covered
Adequately addressed
Poorly addressed
Not addressed
Not reported
Not applicable
1.6 The only difference between groups is the treatment
under investigation
Well covered
Adequately addressed
Poorly addressed
Not addressed
Not reported
Not applicable
1.7 All relevant outcomes are measured in a standard,
valid and reliable way
Well covered
Adequately addressed
Poorly addressed
Not addressed
Not reported
Not applicable
1.8 What percentage of the individuals or clusters
recruited into each treatment arm of the study
dropped out before the study was completed?
1.9 All the subjects are analysed in the groups to which
they were randomly allocated (often referred to as
intention to treat analysis)
Well covered
Adequately addressed
Poorly addressed
Not addressed
Not reported
Not applicable
1.10 Where the study is carried out at more than one site,
results are comparable for all sites
Well covered
Adequately addressed
Poorly addressed
Not addressed
Not reported
Not applicable
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code ++, +, or
2.2 Taking into account clinical considerations, your
evaluation of the methodology used and the statistical
power of the study, are you certain that the overall
effect is due to the study intervention?
2.3 Are the results of this study directly applicable to the
patient group targeted by this guideline?
2.4 Notes. Summarize the authors conclusions. Add any comments on your own assessment of the study, and
the extent to which it answers your question.

110
Appendix F
Quality Assessment of Review Literatures
Quality Assessment of Randomized
control Checklist,
(SIGN, 2012)
Crockett, et
al. (2008)
Gao, et al
(2010)
Gao, et al.,
(2012).
Grote, et al.
(2009)
Leung & Lam
(2012)
Spinelli, &
Endicott
(2003)
Zlotnick, et
al., (2001)
Zlotnick, et
al., (2006)
Section 1: Internal Validity 1: Well covered, 2: Adequately addressed, 3: Poorly addressed, 4: Not addressed & ignored, 5: Not report (not mentioned but insufficient detail to allow assessment to be made, 6: Not applicable
1.1 Study address appropriate and
clearly?
1 1 1 1 1 1 1 1
1.2 Random allocation? 1 1 1 1 1 1 1 1
1.3 Adequate concealment? 5 2 2 5 1 5 5 5
1.4 Double blinded? 5 2 5 5 2 5 5 5
1.5 Similar group at the start of the
trial?
1 1 1 1 1 1 1 1
1.6 Treatment is only difference? 1 1 1 1 1 1 1 1
1.7 Valid measuring tools? 1 1 1 1 1 1 1 1

111
1.8 Drop-out rate & reason? Total dropout:
5.26%, reason:
moved away.
Total dropout: 9.8%,
reasons: loss contact,
mastitis, low birth weight,
pneumonia, premature
labor.
Total dropout: 9.8%,,
reasons: loss contact,
mastitis, low birth
weight, pneumonia,
premature labor.
Total dropout:
18.8%, reason: lack of
time
Total dropout:
7%, no reason report.
Total dropout:
24%, no reason
report.
Total dropout:
5.7%, no reason
report.
Total dropout:
13%, reason:
moved out of state
1.9 Intention to treat analysis? 3 1 1 1 1 1 3 3
1.10 Comparable for all sites? 6
(conduct in a
prenatal clinic)
6
(conduct in a
regional hospital)
6
(conduct in a
regional hospital)
6
(conduct in a
hospital)
1
(conduct in
6 MCHCs)
1
(conduct in
maternal clinics)
6
(conduct in a
general hospital)
6
(conduct in a
prenatal clinic)
Section 2: Overall assessment of the study
2.1 Quality rating, Code ++,+, or - + ++ ++ ++ ++ ++ + +
2.2 Bias might affect study result? 3
No
intention-to-treat
6 6 6 6 6 3
No
intention-to-treat
3
No
intention-to-treat
2.3 Overall effect due to
intervention?
Yes Yes Yes Yes Yes Yes Yes Yes
2.4 Results directly applicable to
patient targeted by this guideline?
Yes Yes Yes Yes Yes Yes Yes Yes

112
Appendix G
Detailed Critique of 8 RCT studies
Article 1: Crockett, K., Zlotnick, C., Davis, M., Payne, N. & Washington, R. (2008). A depression preventive intervention for rural low-income African-American pregnant
women at risk for postpartum depression. Arch. Womens Mental Health. 11, 319-325.
Section 1:
internal
validity
1.1 Detailed background information was presented. Research question was not mention. Aims stated
clearly.
1.2 Assignment of subjects to treatment groups was randomized.
1.3 Concealment method not clearly reported
1.4 Blinding was not mentioned.
1.5 Similarities criteria between treatment and control groups were reported but with not equal size.
1.6 The only difference between the group might be the treatment under investigation
1.7 Valid and reliable measuring tools of EPDS, SAS-SR, PPAQ, PSI used for conduct outcomes.
1.8 Dropout rate 5.26% reported with reason reported.
1.9 Intention-to-treat was not used.
1.10 One site recruitment of a prenatal clinic in this study.
Section 2:
Overall
assessment
Dropout rate relatively low. Sample size was small in this pilot randomized control trial study. Study
was limited as not having equal groups at the onset of treatment and contamination of the
treatment-as-usual group.

113
Article 2: Gao, L.L., Chan, W. C. Sally, Li, X., Chen, S. & Hao, Y.(2010). Evaluation of an interpersonal psychotherapy oriented childbirth education program for Chinese
first time childbearing women, a randomized controlled trial. International Journal of Nursing Studies. 47, 1208-1216.
Section 1:
internal
validity
1.1 Research question was not mention. Detailed background information for affirming the needs was
presented. Aims and hypotheses were stated clearly. Randomized details mentioned.
1.2 Assignment of subjects to treatment group was randomized.
1.3 Concealment method used.
1.4 Research assistant blinded to treatment, collect data and conduct data analysis of study protocol.
1.5 Well addressed the similarities between treatment and control groups.
1.6 Only difference between groups was the treatment under investigation. There might have argued the
interaction and peer support among women group might contribute positive effect.
1.7 Measuring tools of EPDS, GHQ, SWIRS were used standard with validity.
1.8 9.8% dropout rate report with reason reported.
1.9 Intention to treat including in data analysis using SPSS.
1.10 Study recruited in a regional hospital in China.
Section 2:
Overall
assessment
High interventions to minimize bias by using randomization method with intention to treat analysis.
Researcher had minimized potential bias that may reduce reliability of finding.

114
Article 3: Gao, L. L., Chan, W.C. Sally & Sun, K. (2012). Effects of an interpersonal psychotherapy oriented childbirth education program for Chinese first time
childbearing women at 3 month follow up, a randomized controlled trial. International Journal of Nursing Studies, 49, 274-281.
Section 1:
internal
validity
1.1 Research question was not mention. Detailed background information was presented. Aims and
hypotheses were stated clearly. Randomized details mentioned.
1.2 Assignment of subjects to treatment group was randomized by table of random numbers
1.3 Concealment method used.
1.4 Blinding not report in study.
1.5 Well addressed the similarities between treatment and control group were reported.
1.6 Only difference between groups was treatment and no further treatment given.
1.7 Valid and reliable measuring tools of EPDS, GHI, PSSS, PSOC-E were used for conduct outcomes.
1.8 Dropout rate 9.8% with reason reported.
1.9 Intention-to-treat was used in data analysis with SPSS.
1.10 Study recruited in one regional hospital in China.
Section 2:
Overall
assessment
High interventions to minimize bias by using randomization method with intention to treat analysis.
Researcher had minimized potential bias that may reduce reliability of finding.

115
Article 4: Grote, N. K., Swartz, H. A., Geibel, S.L., Zuckoff, A., Houch, P. R., Frank, E. (2009). A randomized controlled trial of culturally relevant, brief interpersonal
psychotherapy for perinatal depression. Psychiatric Services. 60, 313-321.
Section 1:
internal
validity
1.1 Detailed background information was presented. Research question and hypothesize was mention
clearly. Aims stated clearly.
1.2 Assignment of subjects to treatment groups was randomized. A permuted block design for stratified
used for assigned different race in group.
1.3 Concealment method was not clearly reported.
1.4 Blinding was not mention
1.5 Similarities criteria between treatment and control groups were reported
1.6 The only difference between the group was the treatment under investigation
1.7 Valid and reliable measuring tools of EPDS, BDI, BAI, SAS, PPAQ used for conduct outcomes.
1.8 Dropout rate was 18.8% with reason reported.
1.9 Intention-to-treat was used for analysis
1.10 One site recruitment of a public obstetrics & gynecology clinic of hospital in Pennsylvania.
Section 2:
Overall
assessment
Dropout rate relatively high. Sample size was small in this randomized control trial study with
intention-to-treat was used.

116
Article 5: Leung, S. S. K. & Lam, T. H. (2012). Group antenatal intervention to reduce perinatal stress and depressive symptoms related to intergenerational conflicts: a
randomized controlled trial. International Journal of Nursing Studies, 49(11), 1391-1402.
Section 1:
internal
validity
1.1 Background information was detail reported. Hypothesized and aims were detail reported.
1.2 Assignment of subjects to treatment groups was randomized.
1.3 Concealment procedures of randomization was detail reported with computer generated permuted block
randomization in subsets of 4 was used without stratification.
1.4 Blinding was detail mentioned as patient was not possible to blind the patients. Research staff was
blinded for data collection.
1.5 Similarities criteria between treatment and control groups were reported
1.6 The only difference between the group was the treatment under investigation
1.7 Valid and reliable measuring tools of EPDS, REM, SHS, PHS used for conduct outcomes. One
measuring tool was self-designed: PAQ which was. One measuring tool of PAQ was self-designed
1.8 Dropout rate 7% with reason reported.
1.9 Intention-to-treat was used to analyze data.
1.10 Recruitment from six MCHC in four different regions in Hong Kong.
Section 2:
Overall
assessment
Dropout rate was relatively low. Researcher had used interventions of randomized control design,
blinding and intention-to-treat to minimized potential bias for increased reliability of finding.

117
Article 6: Spinelli, M. G. & Endicott, J. (2003). Controlled clinical trial of interpersonal psychotherapy versus parenting education program for depressed pregnant women.
American Journal Psychiatry. 160, 555-562
Section 1:
internal
validity
1.1 Detailed background information was presented. Research question was not mention. Aims stated
clearly.
1.2 Assignment of subjects to treatment group was randomized.
1.3 Concealment method used adequate by using table of random numbers.
1.4 Blinding not well reported.
1.5 Well addressed the similarities between the treatment and control groups were reported.
1.6 Only difference between groups was treatment and no further treatment given.
1.7 Valid and reliable measuring tools of EPDS & BDI were used for conduct outcomes.
1.8 Dropout rate 24% with no reason reported.
1.9 Intention-to-treat was performed in analysis.
1.10 Recruited from outpatient obstetric and prenatal clinics in New York.
Section 2:
Overall
assessment
High dropout rate was not acceptable. However, interventions to minimize bias were used by
randomization method with intention to treat analysis. Researcher had minimized potential bias that
may reduce reliability of finding.

118
Article 7: Zlotnick, C. Johnson, S. L., Miller, I. W., Pearlstein, T. & Howard, M. (2001). Postpartum depression in women receiving public assistance, a pilot study of an
interpersonal therapy oriented group intervention. American Journal of Psychiatry, 158, 638-640.
Section 1:
internal
validity
1.1 Detailed background information was presented. Research question was not mention. Aims stated
clearly.
1.2 Assignment of subjects to treatment groups was randomized.
1.3 Concealment method not clearly reported
1.4 Blinding was not mentioned. But all subjects understand whether or not assigned to intervention group,
they would continue to receive standard treatment.
1.5 Well addressed the similarities between treatment and control groups were reported.
1.6 The only difference between the group was the treatment under investigation
1.7 Valid and reliable measuring tools of BDI used for conduct outcomes.
1.8 Dropout rate 5.4% with no reason explained.
1.9 Intention-to-treat was not used.
1.10 One site recruitment of a prenatal clinic at a general hospital in Northeast in this study
Section 2:
Overall
assessment
The sample size was small in this pilot randomized control trial study without intention-to-treat was
resulted. But the high attendance rate and low dropout rate was successful in preventing postnatal
depression in this low income group of pregnancy women resulting high significance difference in
between group.

119
Article 8: Zlotnick, C., Miller, I. W., Pearlstein, T., Howard, M. & Sweeney, P. (2006). A preventive intervention for pregnancy women on public assistance at risk for
postpartum depression. American Journal of psychiatry. 163, 1443-1445.
Section 1:
internal
validity
1.1 Detailed background information was presented. Research question was not mention. Aims stated
clearly.
1.2 Assignment of subjects to treatment groups was randomized.
1.3 Concealment method not detail mention
1.4 Blinding was not mentioned
1.5 Well addressed the similarities between the treatment and control groups were reported.
1.6 Only difference between groups was treatment and no further treatment given.
1.7 Valid and reliable measuring tools of BDI & RIFTS were used for conduct outcomes.
1.8 Dropout rate was 13% with reason reported
1.9 Intention was not used as reduce data analysis to both intervention group & control group in 3 months
after delivery.
1.10 One site recruitment in this study
Section 2:
Overall
assessment
Sample size nearly hundred with randomization which was highly acceptable. Dropout rate was
acceptable.

120
Appendix H
IPT Program Intervention Compare Table
Group Program Class Program Content
Crockett, et al.,
(2008) Four 90 minutes
One 50 minutes PN individual
session: reinforce skill
<20
Trained IPT
therapist (PhD or
M. Ed. Of
counseling)
1. Program rational, PND & baby blues issues.
2. Manage stress & role transitions, develop support system.
3. Conflicts identify & resolve techniques.
4. Resolve conflict skill learning & material handout with assignment.
Individual session with phone FU/ visit to reinforce skills & identify problems after delivery.
Gao, et al., (2010) Two 60 minutes
One tel. FU 2 weeks
<10
Midwife nurse
educator
(IPT training)
Base on Klerman, et al., (1984), Stuart & Franzcp (2003): ice-breaking games, brainstorming, discussion,
lecture, role play, communication analysis, clarification & written pamphlet.
1. Motherhood transition & management.
2. Communication skills, baby gender issue, Chinese PND issue, social support establish & resolve
interpersonal conflict skills, marital relationship.
Gao, et al., (2012) Two 90 minutes
One tel. FU 2 weeks
<10
Midwife nurse
educator
(IPT training)
Base on Klerman, et al. ,(1984), Stuart & Franzcp (2003),
1. Role transition, communication analysis & skills, PND issues & gender issues.
2. Social support development, reduce & resolve conflict skills.
3. IPT technique & written material.
4. Phone FU reinforce skills and address mood change after delivery.

121
Grote, et al.,
(2009) Eight 45 minutes
Maintenance FU to 6 months
25
Trained IPT
therapist
(doctoral-level &
master’s level)
Focus one interpersonal problem in 3 phases:
1. Initial: review depressive symptoms, evaluate medication need & relate to interpersonal context,
identify major problem area & explain IPT concepts.
2. Intermediate: for 1 of problem area (grief, interpersonal disputes, role transition, interpersonal deficits.
3. Termination: explicit discuss & recognition of independent competence.
4. Maintenance: prevent recurrent, focus 2 problems & establish new role.
Leung & Lam,
(2012) Four 1.5 hour 12
1 trained IPT nurse
&
one therapist
Engage with video clip, role play, homework.
1. Review conflict difficulties & motivate better relationships with grandparents.
2. Poor relationship consequences & teach effective communication skills.
3. Interpersonal problem areas discuss & manage role transitions.
4. Emotional control & management.
Spinelli &
Endicott, (2003) 16 session 45 minutes 25
IPT therapist (M.D.
qualification)
Base on Klerman, et al. (1984) & Spinelli, M. A. (2001)
1. Initial: IPT rationale, past psychiatric history, interpersonal difficulties, treatment progress & focus
area, communication analysis & DSM-IV by EPDS or Hamilton rating scale & evaluate suicidal
assessment.
2. Intermediate: identify 1 or 2 problem areas (grief, role transition, role dispute, interpersonal deficits),
account role transition, beliefs & interpersonal experience, encourage feelings expression.
3. Termination: feelings discuss & develop confidence to deal with problem issues.
4. Outline contingency plans for potential problem solving.

122
Zlotnick, et al.,
(2001) Four 60 minutes 4-6
No mention 1. Program rational, PND & baby blues issues.
2. Role transition management.
3. Develop support net, conflict identify.
4. Resolve conflict skills & material handout with assignments.
Zlotnick, et al.
(2006) Four 60 minutes
One 50 minutes PN individual
session: reinforce skills
3-5
Nurse educator
with IPT training
1. Program rationale, PND & baby blues issues.
2. Role transition management.
3. Develop support net, conflict identify.
4. Resolve conflict skills & written material with assignments.
Individual session reinforced skills & address mood changes after delivery.

123
Appendix I
Evidence-based Antenatal IPT Education Proposed Program
1. Program run by IPT trained nurse in group of <10 participants
2. Learning activities: Ice-breaking games, lecture, discuss, brainstorming, role
play, communication analysis, demonstration & return demonstration,
clarification, IPT skills & handouts
3. Four hours contents based on IPT theory & applications:
1 Introduction
Understand program objectives
Manage role transition
Communication knowledge & skills
1. Games
2. Discuss Objectives
3. Motherhood transition &
management
4. Communication skills
2 Baby gender discussion
Signs & symptoms of PND
Sources of social support
Establish social support system
1. Baby gender issues
2. PND, baby blues signs &
symptoms
3. Discuss importance &
sources of social support
4. Ways to establish social
support system
3 Identify interpersonal conflict or
problems areas:
Interpersonal dispute, role
transition, grief and loss,
interpersonal sensitivity.
Discuss strategies for good
interpersonal relationship with
significant others
1. Current/ potential
interpersonal conflicts
2. Resolve interpersonal
conflict skills
3. Role play & brainstorming
strategies to facilitate
engagement, establish
good relationship with
significant others
4 Discuss strategies to manage
marriage after baby born
Discuss issues related to postpartum
1. Marital relationship after
delivery
2. Chinese practice ‘Doing
the month’

124
Appendix J
Flowchart of Antenatal IPT Program, title as ‘Happy Mom & Happy Family’
Identify high depression risk pregnant women (gestation 20 –32 weeks) by EPDS
High depression risk pregnancy
women EPDS ≥13
*Medical Officer Ad hoc assessment if necessary
ΔReporting through department computer network
YES – Program Group
1. Enrollment procedure (Appendix Y)
2. IPT program reminder (Appendix Z)
3. Sign consent form (Appendix AA)
NO – Routine Group
1. Receive routine program
Baseline Assessment:
EPDS, GHQ & PSOC-EΔ
Routine Education Program group Antenatal IPT Education Program
group, AttendanceΔ
Satisfactory surveyΔ
(Appendix BB)
Postnatal Assessment: 6 to 8 weeks
by EPDS, GHQ, PSOC-EΔ
Routine Postnatal Assessment:
6 to 8 weeks by EPDS, GHQ, PSOC-EΔ
Postnatal Assessment: 3 to 6 months
by EPDS, GHQ, PSOC-EΔ
Psychiatric Services if
EPDS ≥ 13 with consent
Low depression risk pregnancy
women EPDS ≤ 12
Exclude current have mental illness, obstetric complication & English participant
*
Invite antenatal IPT program with
information sheet (Appendix X)
Baseline Assessment:
EPDS, GHQ & PSOC-EΔ
Routine Postnatal Assessment:
3 to 6 months by EPDS, GHQ, PSOC-EΔ
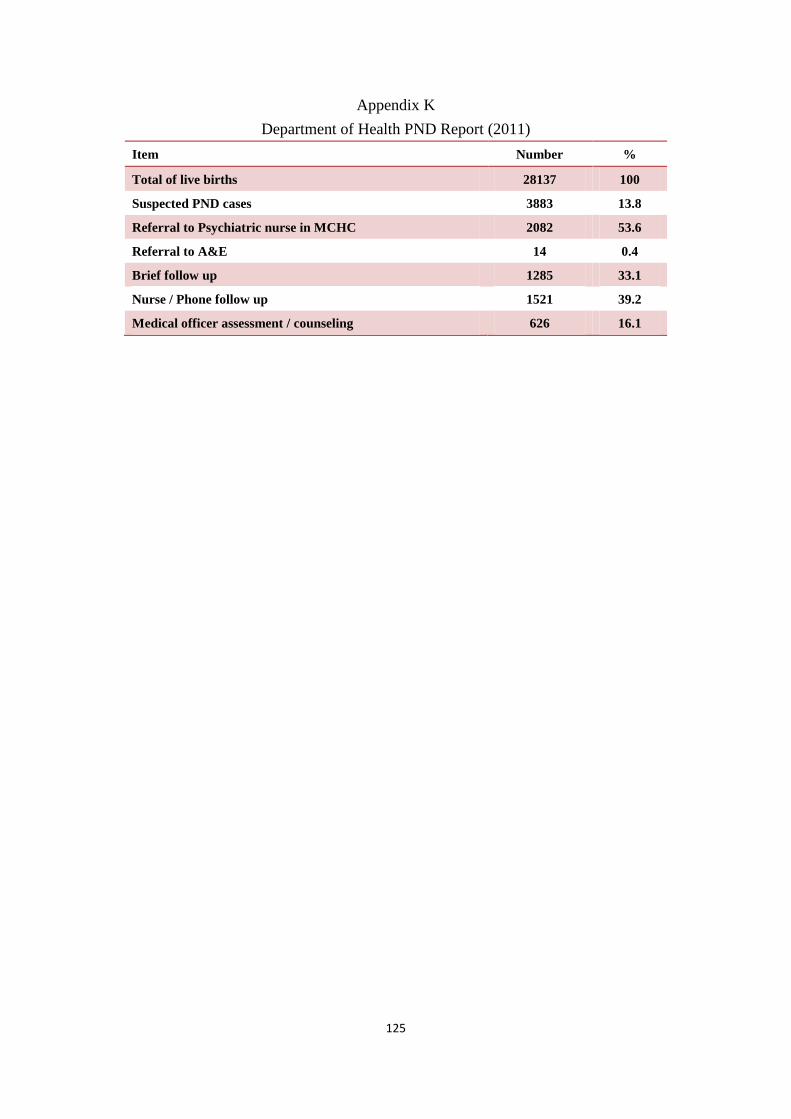
125
Appendix K
Department of Health PND Report (2011)
Item Number %
Total of live births 28137 100
Suspected PND cases 3883 13.8
Referral to Psychiatric nurse in MCHC 2082 53.6
Referral to A&E 14 0.4
Brief follow up 1285 33.1
Nurse / Phone follow up 1521 39.2
Medical officer assessment / counseling 626 16.1

126
Appendix L
Department of Health Approval Letter for PND Data

127
Appendix M
Comparison of Setting and Characteristic between Reviewed Literatures and
Target MCHCs
Setting 8 Reviewed Studies Target MCHCs
Country U.S.A., Peoples’ Republic of
China,
Hong Kong
Hong Kong
Subject number 36 - 194 125*
Setting Maternal Clinic Maternal Clinic
Comparison
education
Antenatal, postnatal Antenatal, postnatal
Characteristic 8 Reviewed Studies Target MCHCs
Mean age 23.4 – 31.3 28.8**
Gestation weeks 20 -32 20 - 32
Education Level High school 41.4 – 87.5% Secondary school 74.3%**
Marital status Married 16.2% to 100% Married 93.2%**
Occupational status Unemployed 36% - 68.6% Unemployed 51.7%**
Income Public assistance, low income,
stable income
Public service to all
Screen depression
risk
Cooper Predictive Index>27,
Cooper Risk Index >27, Frist
pregnancy, Risk factors survey,
Hamilton Depression Rating scales
>12, EPDS ≥13, EPDS ≥12
Mean EPDS 17.8**
*Department of Health PND Report (2011), 3883 /31 MCHCs =125
**Siu, Leung, Ip, Hung & O’Hara (2012) study of antenatal risk factors for PND in MCHCs.

128
Appendix N
Estimated Potential Participants of Innovation Program
Description Figures
Total of live birth of local women 28138*
Prevalence of suspected PND 13.8%*
Potential high depression risk attendant reach innovation
program will be: 28138 x 13.8%
3883
participants
Reviewed literature average response rate (n = 8) 88.3%
MCHC response rate of IPT program 93%^
Range of potential response rate of target high depression risk
attendant in proposed program:
potential reach x range of estimated response rate
3883 x 88.3% to 93%
3428 to 3883
participants
*Department of Health PND report (2011)
^Leung & Lam, (2012)

129
Appendix O
Innovation Implementation Time Allocation
Procedure Contact Time in minutes
Screening of high depression risk pregnant women by
EPDS
2
Antenatal IPT education program 240 (4 hours)
Postnatal assessment at 6-8 weeks by EPDS, GHQ,
PSOC-E
5
Postnatal assessment at 3-6 months by EPDS, GHQ,
PSOC-E
5
Total time for screening and assessment for each high
depression risk pregnant women
12 (0.2 hour)
Total contact time per high depression risk pregnant
women
252 minutes (4.2 hours)

130
Appendix P
Estimation Monthly Workload of Total Contact Time for Innovation Program
Screened low
risk women
per month
Screening
time for
low risk
women
per month
High
depression
risk women
per month
Estimate
program
response
rate
Estimate
participant
of high
depression
risk women
per month
Estimate
contact time
for screening
of high
depression
risk women
per month
Estimate
innovation
program class
in group ≤ 10
for high
depression
risk women
per month
Contact time of
innovation
program class
for high
depression risk
women per
month
Estimate
workload of
total contact
time per month
for innovation
program
(28138* –
3883* )/12
2021 x
2
minutes
3883*/
12
88.3%-
93%^
324 x
88.3% to
93%
286 x 0.2#
hour –
301.3 x
0.2 hour
286/10
-301.3/10
(31 classes x
4hours#)
60.3 hours
+124 hours
+ 67.4
hours
2021
(persons)
67.4
(hours)
324
(persons)
286-301.3
(persons)
57.2 –
60.3
(hours)
29 -31
(classes)
124(hours) 251.7
(hours)
# Total contact time per high depression risk pregnant women of antenatal IPT education program (Appendix O)
*Department of Health PND Report (2011)
^Leung & Lam (2012)

131
Appendix Q
Nursing Staff Manpower Plan
People Descriptions Calculation Data
High depression
risk pregnant
women
Potential number of high
depression risk pregnant
women
3428 to 3883
(persons)
Total contact time per high
depression risk pregnant
women
4.2 (hours)
Total contact time of low
risk pregnant women
(28138 – 3883) x 2
minutes
808.5 (hours)
Total estimated range of
contact time for all high
risk pregnant women
4.2 hours x (3428 to
3883)
13498 to 16309
(hours)
Per nursing staff
working hours
Working hours per week 44 hours per week x
44 working weeks
1936 (hours)
Minimum
training nurse for
innovation
program
Minimum training nursing
staff with consider of staff
replacement and human
factors that double number
for training are needed
(13498 to 16309
hours + 808.5 )/ 1936
hours
= 7.4 to 8.8
= 9 nurses
9 nurses x 2
= 18 nurses
18 (nurses)

132
Appendix R
MCHC Manpower Plan
Class size per
month in 1
MCHC
Total attendants per
year
Potential attendants MCHCs
10 attendants per
class x 4 classes
per month
480 attendants per
year
3883 x 0.93 response
rate = 3611
(3611 to 3883) / 480
= 7.5 - 8

133
Appendix S
Estimate Cost of Innovation Program
Item cost Description Unit price
(HK$)
Calculation Cost
IPT Program course fee Nurse training $1000/course## $1000 x 18 $18,000
Registered Nurses (RN)
for IPT program
training
44 working hours/ week,
work 44 weeks / year at
maximum salary
$234@/ working
hours
$234 x 16 hours##
x 18 RNs
$67,392
Screening of low
depression risk women
28138* – 3883* = 24255
Screen by nurse with 2
minutes EPDS
$234@ / working
hours
$234 x 0.03Hour^^
x 24255
$170,270.1
Participants Each participants cost of 4
hours program in group
class size of 10 add 0.2 hours
assessment by nurse
$234@ / working
hours
$234 x 4 hours / 10
+ $234 x 0.2 hours
$140
Subsequent materials Game materials, handout $3,000
Printout Government Logistics
Department printout
Free ----------
Machine (computer,
projector)
MCHC
Available
-----------
Reporting computer
network
Arrange by department
computer network staff
MCHC
available
-----------
Participants cost 3883 participants* $140 $140 x 3883 $543,620
Total program $802,282.1
Maintenance $716,890.1
@Estimate maximum cost of registered nurse (2012)
##Hong Kong College of Psychiatrist ITP program course fee and training hours (2011)
* Department of Health, PND Report (2011)
^^2 minutes EPDS screening time = 0.03 hour (Appendix O)

134
Appendix T
PND Management Services Cost in 2011
Services Amount Calculation Cost
Nurse identify & counsel /
PND case (30 minutes)
3883*
$234@
x 0.5 hour x 3883 $454,311
Nurse brief follow up (15
minutes)
1285* $234
@ x 0.25 hour x 1285 $75,172.5
Nurse follow up / Phone FU
(15 minutes)
1521* $234
@ x 0.25 hour x 1521 $88,978.5
Medical Officer assessment /
counseling (30minutes)
626* $560
@@ x 0.5 hours x 626 $175,280
Referral to Psychiatric Nurse
with estimate 2 follow ups
2082* $910*** x 2082 x 2 $3,789,240
Referral to A&E department 14* $800**** x 14 $11,200
Total:
$4,594,182
Each PND woman
management cost
$4,594,182 / 3883* $1,183
*Department of Health, PND Report (2011)
*** Hospital Authority service costs per specialist out-patient attendance 2010-2011 from Service costs of Hospital
Authority (2012)
****Hospital Authority service costs per A&E department attendance 2010-2011 from Service costs of Hospital Authority
(2012)
@Estimate maximum cost of registered nurse in 2012 from Salary scale of common posts (2012)
@@Estimate maximum cost of Medical officer in 2012 from Salary scale of common posts (2012)

135
Appendix U
Cost-benefit ratio in Innovation Program & Estimate Cost Saving
Item Description Calculation Cost-benefit ratio
result
Cost-benefit ratio
of innovation
program
Program Cost /
PND Management
Services Demands
$802,282.1 / $4,594,182 0.17
Cost-benefit ratio
per potential
participant in the
innovation
program
Each program
participant cost /
Each PND woman
management cost
$140 / $1,183 0.12
Item Description Calculation Estimate Cost Saving
Estimate save
PND
management cost
Estimate PND
caseload 20%
reduce
$4,594,182 – (3883* x
0.8 x $1,183‡)
$919,310.8
*Department of Health, PND Report (2011)
‡Each PND woman management cost in Appendix T

136
Appendix V
Implementation Timeframe Table
1 month 2 month
3month 4 month 5 month 6 month 7 month 8 month 9 month 10 month 11 month 12 month Till end of 12 months
Process Planning Implementation
4 programs Evaluation
Program
works
Consult
Staff
Suggestion
Scheme &
DH panel
Apply
funding
resource
Steering
committee
with Nurse
leader to
develop plan
Training
course
arrangement
Nurse IPT
training
Pilot test 1 MCHC 8 MCHCs
Monthly meeting: MCHCs In-charge, 2 clinic staffs,
others professionals, pregnancy women
Monthly staff meeting: committee members, MCHC nurse In-charge, 2 clinical staffs, nurse educator
Prepare:
guideline,
questionnaire
, handout,
computer,
reporting
network
MCHCs class
timetable &
resources
Prepare resource
for full implement
Prepare resource
for full implement
One year MCHCs class timetable &
resources maintenance

137
1 month 2 month
3month 4 month 5 month 6 month 7 month 8 month 9 month 10 month 11 month 12 month Till end of 12 months
Program
works
Staff training
recruit by
Staff email &
briefing to 8
MCHCs
Final guideline
staff briefing
with manual
Recruit
cases
3rd weeks Pilot
test recruit 40
cases
Full program
recruit cases
Evaluation
works
Baseline
assessment
(30-32
weeks)
Process Evaluation with pilot test program Pilot test
analysis &
report
-Impact Evaluation
(6Months) -Mid-term review
-Outcome Evaluation
(12Months) -Final Report
Postnatal 1st
assessment
(6-8 weeks)
Postnatal 2nd
assessment
(12-16 weeks)
1. EPDS
2. GHQ
3. PSOC-
E
After program:
1.Attendance Δ
2.Satisfactory rate Δ
3.Staff feedback ※
4.Educator feedback form □F
1.EPDSΔ
2.GHQ Δ
3.PSOC-E Δ
1.EPDSΔ
2.GHQ Δ
3.PSOC-E Δ
4.PND incidence ®
5.PND management
service demands ®
1. Attendance Δ
2. Satisfactory rate Δ
3. Staff feedback ※
4. EPDS Δ
5. GHQ Δ
6. PSOC-E Δ
7. PND incidence ®
8. PND management service demands ®
Economic evaluation: Cost-benefit / Cost-effective
Δ Report through department computer network, ※ Clinic monthly staff meeting , ® Department Report Data System, □F Fax

138
Appendix W
Evidence-based Antenatal Interpersonal psychotherapy
Education Program Guideline
This Guideline developed for implementation of antenatal interpersonal
psychotherapy (IPT) education program in MCHCs to help high depression risk
(HDR) pregnant women understand the interpersonal stress, motherhood problems
and provided IPT knowledge and skills to establish good interpersonal and
communication skills to cope with those stressful condition resulting PND
prevention, high efficacy maternal role and psychological well-being in MCHC
clients.
Role of MCHC staffs
1. Clinical staff nurse
i. Identify high depression risk (HDR) pregnant women at gestation 20 -32
weeks by EPDS ≥13 with GHQ & PSOC-E obtained that reporting
through computer network.
ii. Recruit potential participant with program information sheet (Appendix
X), arrange enroll procedure (Appendix Y) and provide program
reminder form (Appendix Z).
iii. Signed the program consent form (Appendix AA) and keep in client
medical record.
iv. Arrange routine antenatal education for refused participant.
v. Assess all participants in postnatal 6 to 8 weeks and 3 to 6 months with
EPDS, GHQ and PSOC-E and reporting through computer network by
nurse.
vi. Refer psychiatric service if postnatal assessment EPDS ≥13 with
consent
vii. Referral to medical officer Ad hoc enquiry for difficult cases.
2. Nurse trained educator
i. Educator role as designated in MCHCs antenatal IPT program.
ii. Responsible for education program and delivery the 4 hours antenatal
IPT program
iii. Attendance rate (Appendix Y) and program satisfactory form (Appendix
BB) report through computer network.
3. Medical officer
i. Provide professional support to nurse educator and clinical staff in
management of difficult cases Ad hoc enquiry.
4. Nursing officer
i. Take up the overall leading role in program implementation time

139
schedule.
ii. Monitor the workflow in collaboration with nurse educator and clinical
staff nurse.
iii. Evaluate outcome measurements and statistic entry (e.g. attendance,
satisfactory survey, staff feedback, EPDS, GHQ, PSOC-E).
5. Head office team
i. Oversee overall program implementation & quality assurance.
ii. Organize manpower and training
iii. Review program outcome measurement and statistic report (e.g. PND
incidence & management service demands, EPDS, GHQ and PSOC-E).
Content of antenatal IPT program
Two 120 minutes education program: part 1 & part 2, arranged in group ≤10 during office hours.
Part
One
60 minutes 1. Introduction of program
2. Program objectives to prevent PND, promote high efficacy level of maternal
role and psychological well-being
3. Games: ice-breaking games
4. Motherhood transition and management
5. Communication knowledge and skills
60 minutes 1. Baby gender issues discussion
2. PND signs and symptoms
3. Social support sources discussion the importance
4. Teach how to establish social support system
Summary of content & handout provided
Part
Two
60 minutes 1.Help client to identify current or potential problems:
Interpersonal conflict, role transition, grief & interpersonal sensitivity
2. Give appropriate management with IPT techniques
3. Resolve problems skills (e.g. interpersonal conflicts)
Brainstorming strategies, role play, communication analysis, demonstration &
return demonstration
4.Discuss the important of good interpersonal relationship with significant others
5.Establish good interpersonal relationship skills
60 minutes 1. Discuss strategies to manage marriage after delivery
2. Discuss postpartum Chinese practice ‘Doing the month’
Summary of program content & handout provided

140
Antenatal IPT Education Program Measurement Tools
1. Edinburgh Postnatal Depression Scale (EPDS)
EPDS is a self-report questionnaire developed by Cox, Holden & Sagovsky,
(1987) for measuring PND symptoms over past 7 days and used for antenatal
screening (Cox & Holden, 2003). Chinese version of EPDS validated with
cut-off score of 9/10 with 82% sensitivity and 86% specificity, 44% positive
predictive value, 97% negative predictive value at six postpartum (Lee, Yip,
Chiu, et al, 1998) and found useful in PND screening up to 6 months postnatal
(Leung, Leung, Lam, et al, 2010).
It contains 10 items with four response choices (scored 0-3): ‘Normal’
response: 0 up to ‘Severe’ response: 3; Q10 = self-harm question.
Total score ≥13 warrants further evaluation (Gao, et al, 2010; Gao, et al., 2012;
Leung & Lam, 2012) and introduce antenatal IPT program to prevent PND.
***In postnatal, refer psychiatric services if EPDS ≥13 with consent.
2. General Health Questionnaire (GHQ)
GHQ is a self-report questionnaire developed by Nott & Cutt, (1982) for
measuring psychological well-being. Chinese version of GHQ validated with
cut-off score 4/5 with 88% sensitivity, 89% specificity, 52% positive
predictive value, 98% negative predictive value (Lee, Yip, Chiu, et al, 2001a).
It contains 12 items with 4 health conditions (scored 0-3): ‘not at all’ have ‘0’

141
score; ‘no more than usual’ have ‘1’score; ‘rather more than usual’ have ‘2’
score; ‘much more than usual’ have ‘3’ score.
Possible PND case of total GHQ score ≥5 in postnatal (Lee, Yip, Chiu, et al,
2001a) for refer medical officer assessment Ad hoc.
Remarks: use EPDS and GHQ together can increase positive predictive value
up to 78% (Lee, Yip, Chiu, Chung, 2000a).
3. Parenting Sense of Competence Efficacy Scale (PSOC-E)
PSOC-E is a self-report questionnaire developed by Gibaud-Wallston &
Wandersman (1978) for measuring maternal role competence efficacy level.
Chinese version validated with internal consistency 0.8 and significant
negatively correlated 0.31 with EPDS (Ngai, Chan & Holroyd, 2007).
It contains 8 items with 6 point scale from 1 (strongly disagree) to 6 (strongly
agree) range from 8 to 48.
Higher scores indicated higher maternal role efficacy competence.
Reporting of measurements and program evaluation
1. All EPDS, GHQ and PSOC-E report through department computer network
by nurse.
2. Attendance and program satisfactory form (Appendix BB) will provide to
participant and report through department computer network by nurse

142
educator.
3. Educators and staffs feedback will be discuss during monthly clinic meeting
and report to head department by nursing officers.
4. Annual statistic of PND incident and services demands analysis by head
department.

143
Appendix X
Antenatal IPT Program Information Sheet
Evidence-based Antenatal IPT Education Program ‘Happy Mom, Happy Family’
(產前人際心理冶療講座)
You are cordially invited to attend the antenatal IPT education program. This
program is responsible by nurse educator in group of 10 women. Two 2
hours classes content based on IPT theory and application for sharing and
providing IPT knowledge and skills.
Program aim: maintain close interpersonal relationship, build good social
support & master motherhood to prevent PND, promote higher maternal role
competence and psychological well-being.
Learning activities: ice-breaking games, discuss, brainstorming, role play,
communication analysis & skills, demonstration & return demonstration,
clarification & IPT skills (handout provided)

144
Appendix Y
Antenatal IPT Program Enrollment and Attendance Form in MCHCs
Antenatal IPT Education Program Enrollment Form
Date :______________________Time:____________________________
___________________ MCHC
1.
Attendance 6. Attendance
2.
Attendance 7. Attendance
3.
Attendance 8. Attendance
4.
Attendance 9. Attendance
5. Attendance 10. Attendance
Nurse Educator: ______________________________
Enrollment:________
AttendanceΔ:________ (ΔReport through department computer network)

145
Appendix Z
Antenatal IPT Education Program Reminder Form
(Provided to program participants)
產前人際心理冶療講座
誠意邀請你 各位準媽媽參加講座小組
地點:__________________MCHC:____
第一堂
日期:____________________________
時間:____________________________
第二堂
日期:______________ ______________
時間:____________________________
提供產前人際心理冶療支援 輕鬆的分享
Antenatal IPT Education Program
You are cordially invited attending
Location:______________MCHC:_____
Part One
Date:_______ _____________________
Time:_________ ___________________
Part Two
Date:_____________________________
Time:_____________________________
Providing IPT program and Happy sharing
產前人際心理冶療講座
誠意邀請你 各位準媽媽參加講座小組
地
點:____________________MCHC:______
第一堂
日期:_____________________________
時間:_____________________________
第二堂
日期:_____________________________
時間:_____________________________
提供產前人際心理冶療支援 輕鬆的分享
Antenatal IPT Education Program
You are cordially invited attending
Location:______________MCHC:_____
Part One
Date:_______ _____________________
Time:_________ ___________________
Part Two
Date:_____________________________
Time:_____________________________
Providing IPT program and Happy sharing

146
Appendix AA
Evidence-based Antenatal IPT Education Program Consent form (Draft version)
Antenatal education title: Evidence-based Antenatal IPT Education Program
Program evaluator: Author of the Innovation Program (Chairman)
Description of subject population: MCHC high depression risk pregnant women.
Subject: pregnant women gestation at 20 to 32 weeks with EPDS ≥13.
Objectives: there would like to conduct an evidence-based antenatal IPT education program
among pregnant women to maintain close interpersonal relationship, build good social
support & master motherhood that reduce PND, promote high level of maternal role
competence and psychological well-being in MCHC.
Procedure: this education program requires your participation during antenatal follow-up in
MCHC for two 2 hours education classes with EPDS, GHQ and PSOC-E questionnaires
measurement at baseline, postnatal 6 -8 weeks and 3 -6 months.
Cost: this antenatal education does not involve any education fees.
Risks and discomforts: No risk and discomfort of this education program.
Benefits: this antenatal education program provide information for PND symptoms, IPT
skills and motherhood management is expected to reduce PND, promote maternal role
competence and psychological well-being among high depression risk pregnant women in
MCHC.
Confidentiality: any information and data produced in this education program will not be
given to anyone unaffiliated in a form that could identify you without your written consent.
Refusal or withdrawal of procedures: you have a right to refuse the participation or
withdraw from the program at any time without any penalty.
This education program received approval from the Department of Health and any comments or complaints
regarding the conduct of the study should be addressed initially to the Steering Working Committee, author of
innovation program (Tel: 18331844).
Consent
I confirm that the purpose of the education program research, the study procedures and the possible risks and discomforts
as well as potential benefits that I may experience have been explained to me. Alternatives to my participation in the study
have also been discussed. All my questions have been answered. I have read this study information sheet. My signature
below indicates my willingness to participate in this education program.
Signature of Subject
Name of Subject
Date
Signature of Program Chairman
(For Department of Health)
Name of Program Chairman
(For Department of Health)
Date

147
Appendix BB
Antenatal IPT Education Program Satisfactory Form
(Report through department computer networkΔ
)
Thank you for your joining Antenatal IPT Education Program. Please kindly take
your time to complete this evaluation form. Information collected will be
determine the success of the education program and facilitate future improvement
accordingly. Circle number as decided.
Item Content
內容
Very agree----------------------------very disagree
非常同意-------------------------------非常不同意
1. Program topic clear 主題清晰 1 2 3 4 5 6 7
2. Meet participant needs 切合參加者需要 1 2 3 4 5 6 7
3. Have a better understanding about IPT knowledge and skills
to deal with problems
資料是顯淺理解, 技巧可容易掌握, 用以處理問題
1 2 3 4 5 6 7
4. The handout can facilitate IPT skills practice
講義可以促進人際心理技能實踐
1 2 3 4 5 6 7
5 Role Play can facilitate IPT skills practice
角色扮演可以促進人際心理技能實踐
1 2 3 4 5 6 7
Item Educator
講者
Very agree-----------------------------very disagree
非常同意------------------------------非常不同意
1 Adequate preparation 充足預備 1 2 3 4 5 6 7
2 Express clearly 表達清楚 1 2 3 4 5 6 7
3 Friendly attitude 態度親切 1 2 3 4 5 6 7
4 Provide an answer to questions from participants 能解答參加
者提問
1 2 3 4 5 6 7
5 時間掌握恰當 proper time application 1 2 3 4 5 6 7
6 Overall, the education program is useful and worth joining
總體而言,產前人際心理冶療講座課程是實用的,值得參
與
1 2 3 4 5 6 7

148
Appendix CC
Key to Evidence Statements
Designed by the Scottish Intercollegiate Guideline Network (SIGN, 2008b)
Levels of evidence
1++ High quality meta-analyses, systematic reviews of RCTs, or RCTs with a very low risk of
bias
1+ Well-conducted meta-analyses, systematic reviews, or RCTs with a low risk of bias
1- Meta-analyses, systematic reviews, or RCTs with a high risk of bias
2++ High quality systematic reviews of case control or cohort or studies
High quality case control or cohort studies with a very low risk of confounding or bias and
a high probability that the relationship is causal
2+ Well-conducted case control or cohort studies with a low risk of confounding or bias and a
moderate probability that the relationship is causal
2- Case control or cohort studies with a high risk of confounding or bias and a significant risk
that the relationship is not causal
3 Non-analytic studies, e.g. case reports, case series
4 Expert opinion

149
Appendix DD
Grades of recommendations
Designed by the Scottish Intercollegiate Guideline Network (SIGN, 2008b)
Grades of recommendations
A At least one meta-analysis, systematic review, or RCT rated as 1++, and
directly applicable to the target population; or
A body of evidence consisting principally of studies rated as 1+, directly
applicable to the target population, and demonstrating overall
consistency of results
B A body of evidence including studies rated as 2++, directly applicable to
the target population, and demonstrating overall consistency of results; or
Extrapolated evidence from studies rated as 1++ or 1+
C A body of evidence including studies rated as 2+, directly applicable to
the target population and demonstrating overall consistency of results; or
Extrapolated evidence from studies rated as 2++
D Evidence level 3 or 4; or
Extrapolated evidence from studies rated as 2+

150
Appendix EE
Communication Plan Timeline
Time (Month)
Planning Working Phase
1 2 3$ 4 5 6# 7 8 9 10 11 12 Till
end of
12
month
s*
Communication with Secretary of Department
Staff Suggestion Committee in Department of
Health (proposal documents)
Communication with Administrative &
Management panel (Direct of Health and
Principal Nursing Officer)
Formation of Steering Committee (Author of
innovation program, 1 Senior Medical Officer, 1
Registered Nurse, 2 computer staffs, 2 clerical
staffs )
Monthly Committee Meeting with other staffs
colleagues (8MCHCs nurse in-charge, 2 nurse
clinical staffs review proposed guideline, program
class timetable schedule, questionnaire, handout,
computer booking and data reporting system and
resources)
Communication with potential participants for
opinions (Registered Nurse)
Communication with local training site (18
nursing staff IPT training program)
Communication through e-mail to nursing staffs
training (IPT training recruitment with nominate
and provide class schedule )
Communication to all clinical staffs through FHS
New-letters, e-mail and brief session to 8MCHCs:
program information and guideline (Evaluator)

151
Time (Month)
Implementation Working Phase
1 2 3$ 4 5 6# 7 8 9 10 11 12 Till
end of
12
month
s*
Communication with nurse educators by program
pilot evaluation form (Appendix FF) and class
time schedules
Communication with 31MCHCs staffs: final
version guideline (author of the innovation
program)
Monthly staff meetings with 8 MCHCs nurse
in-charge, nurse educator representative and 2
clinical nursing staff representatives (one year
class schedules, resources, monitor attendance
participant satisfaction and frontline staff
feedback)
Communication with computer staff and 8
MCHCs nurse in-charge for system maintenance
(telephone hotline)
Communication with participant by program
satisfaction form (Appendix BB)
Communication for pilot test report to
Administrative and Management panel (author of
innovation program assisting by computer staffs)
Communication for mid-term data review in 6
months (author of innovation program assisting
by computer staffs)
Communication with Administrative and
Management panel and Staff Suggestion
Committee for final report in end of 12 months
(author of innovation program assisting by
computer staffs)
Remarks: $ Program approval, # Pilot test, *Full implementation of program

152
Appendix FF
Pilot Test Antenatal IPT Program Evaluation Form
(Dedicated for Nurse)
Information and feedback collected to evaluate the feasibility of the education
program. Please kindly take your time to complete this evaluation form and sent
to antenatal IPT education program steering committee. Fax number: 12345678
Item Content
內容
Strongly Agree -------Strongly Disagree
非常同意----------非常不同意
1. Program information attractive and clear 課程資料美觀, 清晰 1 2 3 4 5 6 7
2. Program information easy to understand 課程資料容易理解及明白 1 2 3 4 5 6 7
3. Rich and diversified class 富動感的表達形式及多元化 1 2 3 4 5 6 7
4. Meet participant needs 切合參加者需要 1 2 3 4 5 6 7
5. Can educate client a better understanding about IPT knowledge and skills to
deal with problems
資料是顯淺理解, 技巧可容易掌握, 用以處理問題
1 2 3 4 5 6 7
6. Handout can facilitate IPT skills practice
講義可以促進人際心理技能實踐
1 2 3 4 5 6 7
7. Role Play can facilitate IPT skills practice
角色扮演可以促進人際心理技能實踐
1 2 3 4 5 6 7
Item Program each part allocation
環節分配
Strongly Agree--------Strongly Disagree
非常同意-----------非常不同意
1 Part 1 first unit: proper time application 第一堂第一節時間掌握恰當 1 2 3 4 5 6 7
2 Part 1second unit: proper time application 第一堂第二節
時間掌握恰當
1 2 3 4 5 6 7
3 Part 2 first unit: proper time application 第二堂第一節時間掌握恰當 1 2 3 4 5 6 7
4 Part 2 second unit: proper time application 第二堂第二節
時間掌握恰當
1 2 3 4 5 6 7
5 Part 1 first unit: practical 第一堂第一節 實用性 1 2 3 4 5 6 7
6. Part 1 second unit: practical 第一堂第二節 實用性 1 2 3 4 5 6 7
7. Part 2 first unit: practical 第二堂第一節 實用性 1 2 3 4 5 6 7
8. Part 2 second unit: practical 第二堂第二節 實用性 1 2 3 4 5 6 7
6 Overall, program teaching is not difficult
總體而言,產前人際心理冶療講座課程教學沒有困難
1 2 3 4 5 6 7

153
Appendix GG
Antenatal IPT Program Information Poster
(For MCHCs notice and internet network used)
Evidence-based Antenatal IPT Education Program ‘Happy Mom, Happy Family’
(產前人際心理冶療講座)
During antenatal visit, pregnant women at 20 to 32 gestation weeks are cordially
invited to have a screening assessment by EPDS questionnaire to improve
detection of PND in community. High risk women will receive nurse counsel and
arrange an antenatal IPT education program. This program is responsible by
trained nurse IPT educator in class group of 10 women. Two 2 hours classes
program with game activities are based on IPT theory and application for sharing
and providing IPT knowledge and skills.
Program aims are to assist pregnant women to maintain close interpersonal
relationship, build good social support and master motherhood.
For any enquiry, please contact MCHCs nursing staffs or medical staffs.

154
Appendix HH
Framework for program evaluation
Six Steps
Source: McKenzie J.F. & Smeltzer, J. L. (2013). Planning, implementing and
evaluating health promotion programs, a primer. 3rd
ed. Pearson Education
Company.
Standards:
Utility
Feasibility
Propriety
Accuracy
Engage Stakeholders
Describe the
program
Focus the evaluation
design
Gather credible evidence
Justify conclusions
Ensure use and share
lessons learned

155
Appendix II
Timeline of Pilot Test
Time (month)
Working Phase
1 2 3 4 5 6 7 8
Staff briefing of program
Recruitment of 40 cases (30-32 gestation
weeks) with baseline measurement of
EPDS, GHQ, PSCO-E
Program education group - 4 classes with
measurement of attendance, satisfactory
rate, staff feedback and educator feedback
Routine group – routine education program
Postnatal 1st assessment (6-8 weeks) of
EPDS, GHQ, PSCO-E
Postnatal 2nd
assessment (12-16 weeks) of
EPDS, GHQ, PSCO-E
Pilot test analysis and report for guideline
refinement

156
Appendix JJ
Rundown of Outcome Measurements
Data collection Baseline
measurement
Program
implement
6 to 8 weeks
postnatal
3 to 6 month
postnatal
EPDS Program group &
routine group
Program group &
routine group
Program group
& routine group
GHQ Program group &
routine group
Program group &
routine group
Program group
& routine group
PSOC-E Program group &
routine group
Program group &
routine group
Program group
& routine group
Program
attendance rate
Program
group &
routine group
Satisfactory
rate
Program
group &
routine group
PND incidence Program group
& routine group
PND
management
service
demands
Program group
& routine group