burden of serious fungal infections in dominican · pdf fileburden of serious fungal...
TRANSCRIPT
Burden of serious fungal infections in Dominican Republic1,2Harish Gugnani*, David W Denning and Carlos Rodriguez-Taveras**
*Professor of Microbiology & Epidemiology, St. James School of Medicine, Kralendjik, Bonaire (Dutch Caribbean),email: harish.gugnani@gmail **Head, Division of Infectious Diseases, Hospital Central de las Fuerzas Armadas SantoDomingo, Dominican Republic, email: [email protected] University of Manchester, Manchester Academic Health Science Centre, Manchester, U.K.
2The University Hospital of South Manchester, National Aspergillosis Centre (NAC) Manchester, U.K. in association
with the LIFE program at www.LIFE-worldwide.org
University Hospitalof South Manchester
NHS Foundation Trust
Background and Rationale
Conclusion
References
Methods
Results
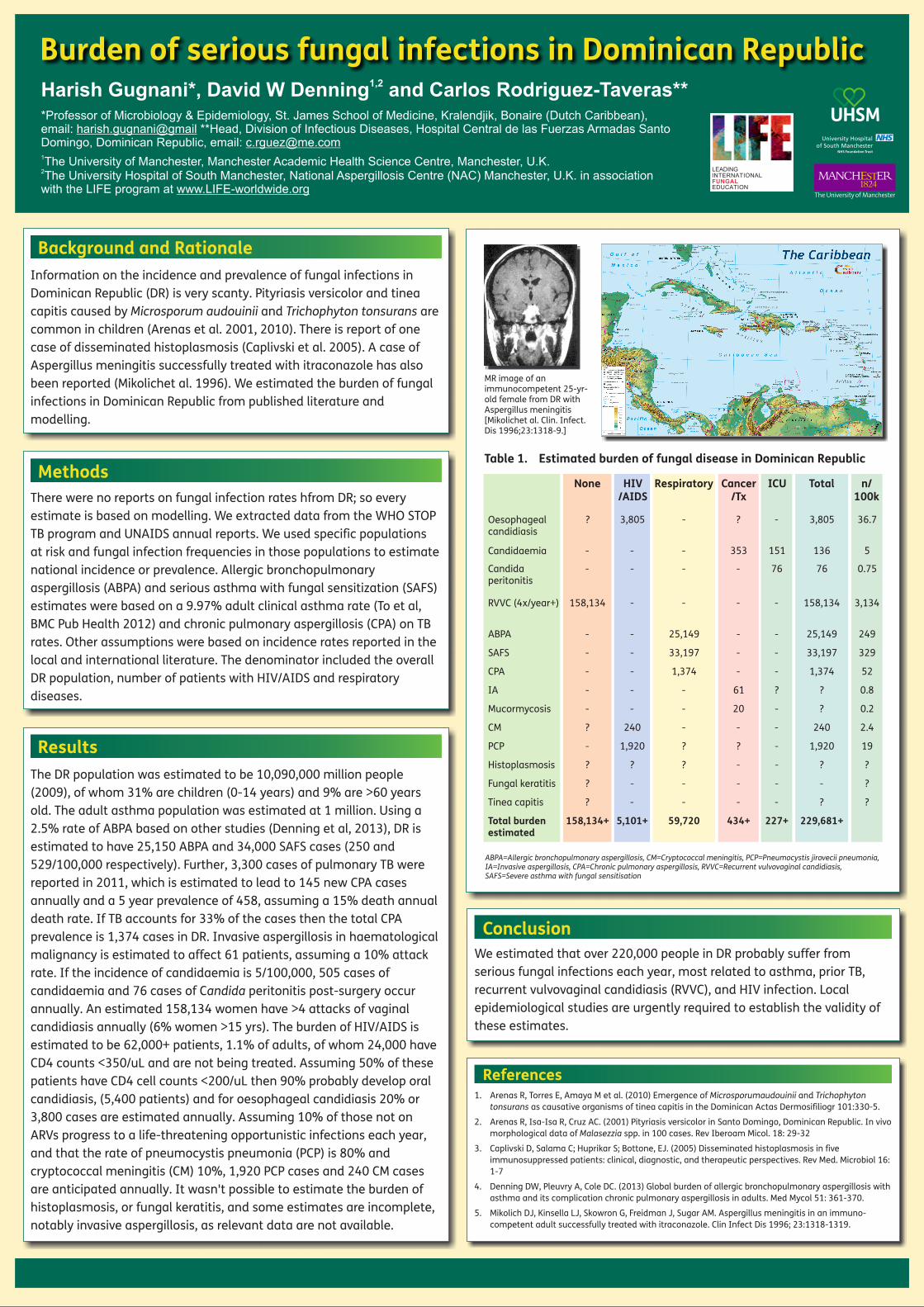
Information on the incidence and prevalence of fungal infections in Dominican Republic (DR) is very scanty. Pityriasis versicolor and tinea capitis caused by Microsporum audouinii and Trichophyton tonsurans are common in children (Arenas et al. 2001, 2010). There is report of one case of disseminated histoplasmosis (Caplivski et al. 2005). A case of Aspergillus meningitis successfully treated with itraconazole has also been reported (Mikolichet al. 1996). We estimated the burden of fungal infections in Dominican Republic from published literature and modelling.
We estimated that over 220,000 people in DR probably suffer from serious fungal infections each year, most related to asthma, prior TB, recurrent vulvovaginal candidiasis (RVVC), and HIV infection. Local epidemiological studies are urgently required to establish the validity of these estimates.
1. Arenas R, Torres E, Amaya M et al. (2010) Emergence of Microsporumaudouinii and Trichophyton tonsurans as causative organisms of tinea capitis in the Dominican Actas Dermosifiliogr 101:330-5.
2. Arenas R, Isa-Isa R, Cruz AC. (2001) Pityriasis versicolor in Santo Domingo, Dominican Republic. In vivo morphological data of Malasezzia spp. in 100 cases. Rev Iberoam Micol. 18: 29-32
3. Caplivski D, Salama C; Huprikar S; Bottone, EJ. (2005) Disseminated histoplasmosis in five immunosuppressed patients: clinical, diagnostic, and therapeutic perspectives. Rev Med. Microbiol 16: 1-7
4. Denning DW, Pleuvry A, Cole DC. (2013) Global burden of allergic bronchopulmonary aspergillosis with asthma and its complication chronic pulmonary aspergillosis in adults. Med Mycol 51: 361-370.
5. Mikolich DJ, Kinsella LJ, Skowron G, Freidman J, Sugar AM. Aspergillus meningitis in an immuno-competent adult successfully treated with itraconazole. Clin Infect Dis 1996; 23:1318-1319.
There were no reports on fungal infection rates hfrom DR; so every estimate is based on modelling. We extracted data from the WHO STOP TB program and UNAIDS annual reports. We used specific populations at risk and fungal infection frequencies in those populations to estimate national incidence or prevalence. Allergic bronchopulmonary aspergillosis (ABPA) and serious asthma with fungal sensitization (SAFS) estimates were based on a 9.97% adult clinical asthma rate (To et al, BMC Pub Health 2012) and chronic pulmonary aspergillosis (CPA) on TB rates. Other assumptions were based on incidence rates reported in the local and international literature. The denominator included the overall DR population, number of patients with HIV/AIDS and respiratory diseases.
The DR population was estimated to be 10,090,000 million people (2009), of whom 31% are children (0-14 years) and 9% are >60 years old. The adult asthma population was estimated at 1 million. Using a 2.5% rate of ABPA based on other studies (Denning et al, 2013), DR is estimated to have 25,150 ABPA and 34,000 SAFS cases (250 and 529/100,000 respectively). Further, 3,300 cases of pulmonary TB were reported in 2011, which is estimated to lead to 145 new CPA cases annually and a 5 year prevalence of 458, assuming a 15% death annual death rate. If TB accounts for 33% of the cases then the total CPA prevalence is 1,374 cases in DR. Invasive aspergillosis in haematological malignancy is estimated to affect 61 patients, assuming a 10% attack rate. If the incidence of candidaemia is 5/100,000, 505 cases of candidaemia and 76 cases of Candida peritonitis post-surgery occur annually. An estimated 158,134 women have >4 attacks of vaginal candidiasis annually (6% women >15 yrs). The burden of HIV/AIDS is estimated to be 62,000+ patients, 1.1% of adults, of whom 24,000 have CD4 counts <350/uL and are not being treated. Assuming 50% of these patients have CD4 cell counts <200/uL then 90% probably develop oral candidiasis, (5,400 patients) and for oesophageal candidiasis 20% or 3,800 cases are estimated annually. Assuming 10% of those not on ARVs progress to a life-threatening opportunistic infections each year, and that the rate of pneumocystis pneumonia (PCP) is 80% and cryptococcal meningitis (CM) 10%, 1,920 PCP cases and 240 CM cases are anticipated annually. It wasn't possible to estimate the burden of histoplasmosis, or fungal keratitis, and some estimates are incomplete, notably invasive aspergillosis, as relevant data are not available.
LEADING
EDUCATION
INTERNATIONALFUNGAL
Table 1. Estimated burden of fungal disease in Dominican Republic
Oesophagealcandidiasis
Candidaemia
Candidaperitonitis
RVVC (4x/year+)
ABPA - - 25,149 - - 25,149 249
SAFS - - 33,197 - - 33,197 329
CPA - - 1,374 - - 1,374 52
IA - - - 61 ? ? 0.8
Mucormycosis - - - 20 - ? 0.2
CM ? 240 - - - 240 2.4
PCP - 1,920 ? ? - 1,920 19
Histoplasmosis ? ? ? - - ? ?
Fungal keratitis ? - - - - - ?
Tinea capitis ? - - - - ? ?
Total burdenestimated
158,134+ 5,101+ 59,720 434+ 227+ 229,681+
None HIV/AIDS
Respiratory Cancer/Tx
ICU Total n/100k
?
-
-
158,134 - - - - 158,134 3,134
- - - 76 76 0.75
- - 353 151 136 5
3,805 - ? - 3,805 36.7
MR image of an immunocompetent 25-yr-old female from DR with Aspergillus meningitis [Mikolichet al. Clin. Infect. Dis 1996;23:1318-9.]
UHSM
ABPA=Allergic bronchopulmonary aspergillosis, CM=Cryptococcal meningitis, PCP=Pneumocystis jirovecii pneumonia, IA=Invasive aspergillosis, CPA=Chronic pulmonary aspergillosis, RVVC=Recurrent vulvovaginal candidiasis, SAFS=Severe asthma with fungal sensitisation