building competency to serve active duty & reserve members
TRANSCRIPT

Building Competency to Serve Active Duty & Reserve Members, Veterans and Dependents. Re-Integration and Recovery.

HCHV COORDINATOR
VAAAHS
Shawn Dowling
LCDCIII, LISW-S, ACSW

PEER SUPPORT SPECIALIST
VA SUPPORTED HOUSING PROGRAM
VAAAHCS
Vincent Warren Management Specialist, U.S Navy

Understanding Military Culture
In order to effectively meet the needs of military members and their families we must understand the culture within the US Military.
Culture is defined as: The set of shared attitudes, values, goals, and practices that characterizes an institution, organization or group

What is Different for Military Members compared to Being a Civilian
Service is Generational
Lack Control Over: Location, body, clothes, etc.. Becomes a piece of Government Property
Dependents Are Not Encouraged to Ask for Help or Admit they Need it.
Constant changes in regulations, expectations, and position security
Freedom of speech limited
Cannot Advocate for a Sober Work Culture
Cannot Transfer or Quit
Violence is a Fact of Every Day Life
Can’t call in sick or take a mental health day
Confidentiality is non existent
Constant reintegration
1% of population

Common Military Behaviors
Being constantly on guard (hyper vigilant) Common practice for weapons to be present Stoic/Flat affect Recalling events repeatedly Emotional numbing/detachment Heightened response to loud noises Lack of assertiveness/speaking up Situational awareness THESE BEHAVIORS MAXIMIZED SURVIVAL
DURING ENLISTMENT, BUT CAN BE CONSIDERED DISRUPTIVE IN CIVILIAN ENVIRONMENTS

OLD WAYS OF THINKING BY THE MEMBER AND SOCIETY
Seeking help is a sign of weakness
Impacts career-deployability, promotions
Combat Veterans are all “messed up”
Service members are victims of government agenda
WWII, Korean, Vietnam veterans didn’t need help-they didn’t have problems.
If a member deploys they have PTSD, or have experienced some form of trauma
When a crime has been committed by a service member- military service is disclosed

The Current Epidemic of Suicide
20.2 per 100,000 soldiers have completed suicide-higher than current civilian rate.
32 suicides in the month of June 2011. 22 had been deployed, of those 10 had deployed 2-4x.
Males 18-24 at higher risk.
Security Forces, Maintainers and Recruiting at higher risk.
155 suicides in the first 154 days of the year-2012
Undocumented attempts
Inability to cope is interpreted as a loss of respect, dignity, lacks resiliency and purpose.

Drugs Impact Military Discipline
The abuse of alcohol, prescription drugs or the use of illicit drugs are inconsistent with the Armed Forces Values, the Warrior Ethos and the standards necessary to accomplish the mission:
• Performance
• Discipline
• Safety
• Readiness
Substance Use Disorders
Pain Medication while in the field-not prescribed when they return home.
Return home, substances are used as a tool during the reintegration period
Coping mechanism to assist with anxiety, depression, trauma, adjustment
Sleep meds prescribed due to drastic changes in sleep patterns

Times are Changing

Lt. Col. Wayne Talcott, Air Force Psychologist stated; “You maintain a jet engine so it doesn’t fall out of the sky,” he said. “We need to begin to look at where there are risks to the human weapon system and how we can build a system that protects our people.”

Mitigation Strategies
Significant Protective Factors can be Mobilized BEFORE hand that are PROVEN to work
Prevention Education
Team/Social Support
Coworker Peer Referral
Supervisor Responsiveness
Stigma Reduction
Advertising of Resources
Team Moderation in Alcohol Use
Wellness Lifestyle
Positive Policy Attitude
Significant Stress for Members Before, During, After Deployment
Accelerated Deployment Impacts Operational Readiness (Individual & Unit) Impacts: • Retention • Accidents • Mental Health & Stress Disorders • Substance Abuse • PTSD • Co morbidity of PTSD/Substance Abuse • Family Problems / Generational Impact / Community
Risk Factors Mitigation

Current Pilot Programming for Military
Needs assessment/Data collection and integration
Data visualization and data dashboard projects (DE, IA, MD, NH)
Tracking Veteran status on driver’s licenses (GA, MD, UT, WA)
Workforce development/Military culture-informed services
Hosted Operation Immersion (AZ, TN, RI)
Military cultural competency training (AZ, IA, ME, NC, OH)
Training with law enforcement and first responders (CT, ME, NC, OH)
ESGR-Employment Support for Guard and Reserve
Criminal Justice Implementation of Veterans Treatment Courts (FL, NH, ME, UT, OH)
Intimate partner violence strategic action plan (CT)
Veteran Dormitory Program in prisons and jails (FL)

Navy Capt. Robert Murphy, a medical corps officer stated that
“We’re certainly not opposed to alcohol use, but we are trying to
reduce the prevalence of alcohol abuse.”

Then VS. Now
Old Approach New Approach
Goal: Eliminate the problem Cultural change
Focus: Deterrence Prevention
Target: Service member Circle of Influence
Primary Responsibility: Service member Service member
Substance Abuse:
Abuse vs. Addiction
Individual Issues Community Issues
Approach: Punitive
Intervene to prevent substance
abuse and foster rehabilitation
Key Message:
Don’ t Get Caught
Every Service member has a duty
to intervene to prevent substance
abuse and access to rehabilitative
services with command support

Policy Academy Objectives
17
Strengthen behavioral health systems for Service Members, Veterans, & their Families
Involve Service Members, Veterans, and Families
Increase access
Close the gaps
Build capacity
Increase interagency communication/collaboration
Incorporate best practices
Plan for sustainability

Mental Health
Adjustment disorder vs. SPMI diagnosis Allowed medications Understanding needed documentation Evaluation Diagnosis/prognosis Meds prescribed Treatment Plan Regular Summaries
Acknowledge the concern they may feel that seeking treatment will impact their career.
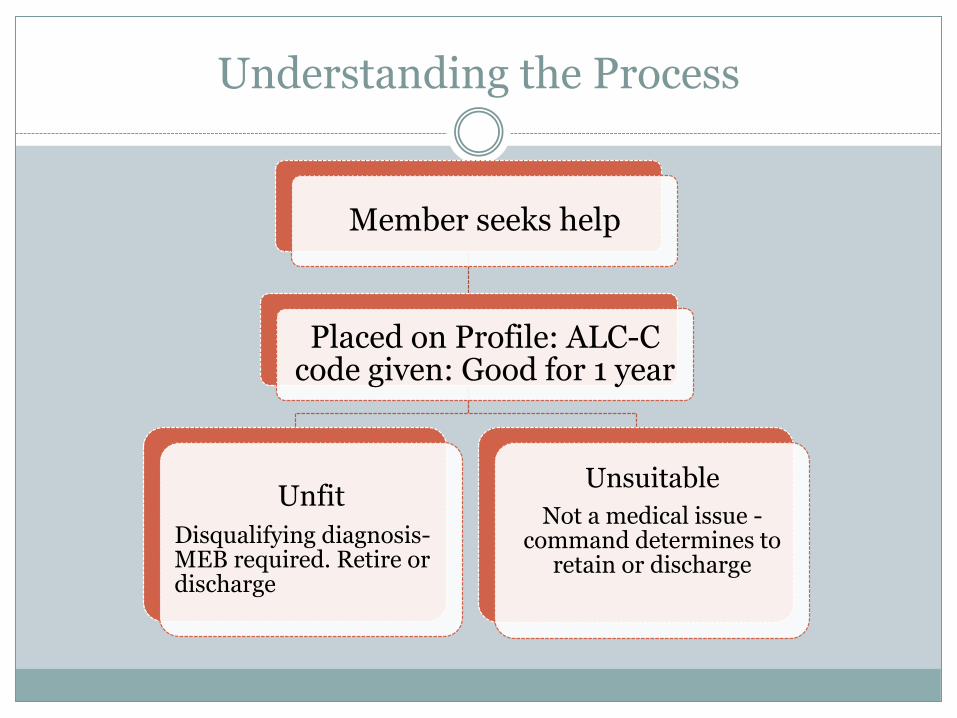
Understanding the Process
Member seeks help
Placed on Profile: ALC-C code given: Good for 1 year
Unfit
Disqualifying diagnosis-MEB required. Retire or discharge
Unsuitable
Not a medical issue -command determines to
retain or discharge
Unfitting Diagnoses’
Psychosis, unless brief and from a reversible cause
Persistent impairment (> 1 year)
Continuing psychiatric support (> 1 year)
Recurrent impairment (>1 in 1 year)
Conditions requiring use of lithium, anticonvulsants, or antipsychotics for mood stabilization

Unsuitable Diagnosis’
Personality disorders
Learning disorders
BUT ALSO:
ADHD; if medication required, WWD and waiver request from NGB/SG required
Adjustment disorders
Sexual perversions
Flying phobia
Substance use disorders

Must be seen by Military MH
Recurrent depression or anxiety disorders
Psychiatric medication for > 1 year
Hospitalized for any psychiatric condition

RECOVERY/RESTABILIZATION
It is a PROCESS not an EVENT.
Provider competency a must, without it the individual will dis-engage.
Know the SYSTEM and the INDIVIDUAL
Assist with Serving the “Whole Person” including the Dependents in a non-threatening setting that is family focused. Remember they are trained as a team work with them as such.

HELPFUL HINTS
Learn the Language: www.militaryfactory.com
Understand Rate and Rank, Medals and Awards.
Learn About the Base closest to your practice/agency
Deployment Structure-for active duty, reserve, guard.
Understand and Respect the Traditions and Expectations of the Military Culture-customs and courtesies and military bearings.

References
http://usmilitary.about.com/library/milinfo/milarticles/blalcohol.htm
http://www.ptsd.va.gov/
http://www.afterdeployment.org/
http://www/samsha.org/
http://www.vetsprevail.com